contingency management motivational incentives: past, present and future maxine stitzer, ph.d. johns...
TRANSCRIPT

Contingency ManagementMotivational Incentives: Past, Present and Future
Maxine Stitzer, Ph.D.Johns Hopkins University SOM
NIDA/CTN Regional Dissemination Conference
Baltimore, MDJune 3, 2010


What you will hear today
• CM/Incentives Background – Development and efficacy research
• Effectiveness testing – National Drug Abuse Clinical Trials Network
• Implications for future – Pathway for adoption by treatment providers

Drug User’s DilemmaDrug User’s Dilemma
Get a jobTime with familyBetter health
Easy moneyHang with friendsGet high

Motivational Incentives Can Motivational Incentives Can Counteract AmbivalenceCounteract Ambivalence
Make sober living a more Make sober living a more attractive option through attractive option through positive reinforcement of positive reinforcement of abstinence and otherabstinence and otherbehavior changebehavior change


People Respond to Consequences
• Behavior can be changed by consequences– Rewards increase desired behavior– Punishment and sanctions decrease undesired
behavior

Contingency Management: Application in Drug Abuse
• Measurable target behavior
• Rewarding consequence

Application in Drug Abuse Treatment: Early Studies
• Behavioral targets:– Counseling attendance– Drug use during treatment– On-time fee payment
• Reinforcing consequences:– Money (or vouchers) – Privileges (e.g. methadone take-home doses)
Incentive Effects on Benzodiazepine Use
3-month intervention with methadone maintained benzo users; incentive is take-home or money
Percent benzo negative urines– Before incentives 9%– During incentives 53%– After incentives 11%
Stitzer et al., 1982

Voucher Reinforcement making cocaine abstinence a more
attractive option • Intensive counseling plus
• Points earned for cocaine negative urine results– Escalating schedule with reset penalty
– Trade in points for goods
– $1000 available in first 3 months Steve Higgins

Voucher Incentives in Outpatient Drug-free Treatment
0
20
40
60
80
100
2 4 6 8 10 12 14 16 18 20 22 24
BehavioralStandard
Weeks of Treatment
Perc
ent
of S
ubje
cts
Higgins et al. Am. J. Psychiatry, 1993
Cocaine negative urines

Perc
ent
Coca
ine N
egati
ve
Baseline Intervention Weeks
Control
Vouchers
0
20
40
60
80
100
2 4 6 8 10 121 2 3 4 5
** * * * *
* *
Voucher Incentives in Cocaine Abusing
Methadone Patients Silverman et al., 1996

Voucher Reinforcement
• Elegantly incorporates behavioral principles designed to initiate & sustain abstinence
• Demonstrated efficacy in controlled trials BUT• Sample sizes are small• Costs were high ($1000 per client could be earned)

$1000???
You’ve got to be kidding!!!

Nancy Petry’s Fishbowl: Intermittent Reinforcement Schedule
For cost reduction in community clinic settings
QuickTime™ and aPhoto - JPEG decompressor
are needed to see this picture.

Fishbowl Method
Incentive = draws from a bowl
- Draws earned for each negative urine or BAC- Number of draws can escalate- Bonus draws can be given for consecutive weeks of abstinence

largest chance of winning a small $1 prize
moderate chance of winning a large $20 prize
small chance of winning a jumbo $100 prize
Half the slips are winnersWin frequency inversely related to cost

Retention: Alcoholics in Outpatient Psychosocial Treatment
0
20
40
60
80
100
120
2 4 6 8
weeks
STDCM
Petry et al., 2000

Percent positive for any illicit drug
0
10
20
30
40
50
%
Intake Week 4 Week 8
STDCM
Petry et al., 2000

Efficacy of abstinence reinforcement demonstrated
Drug-free and methadone
treatment populations
Voucher and prize draw methods

Generality of Abstinence Reinforcement Effects Across Abused Substances
Cocaine (Higgins et al., 1994; Silverman et al., 1996, 2004; Petry & Martin, 2002)
Alcohol (Petry et al., 2000)
Opioids (Bickel et al., 1997; Silverman et al., 1996)
Marijuana (Budney et al., 1991, 2000, 2006)
Nicotine (Tobacco smoking) (Stitzer & Bigelow, 1984; Roll et al., 1996; Shoptaw et al., 2002)

National Drug Abuse Treatment Clinical Trials Network
Bridging the gap between research and practice
Clinicians Researchers

CTN Mission
• Conduct effectiveness research with community treatment partners– Do interventions developed and studied in research
clinics work when tested in the real world settings?– If so, how can we make these new treatments part
of usual care?

How do abstinence incentives fit into the clinical picture?
• Add-on to counseling as usual– Special intervention to enhance motivation for
sustained abstinence – Focuses on the positive to recognize and celebrate
success– Allows counselors to work on life-style changes
that can sustain abstinence beyond incentives

CTN MIEDAR StudyCTN MIEDAR Study
Participants = 800 stimulant users (cocaine or methamphetamine)
Conducted in:
6 methadone and
8 drug-free programs

Random Assignment
• Usual care
• Usual care enhanced with abstinence incentives
• 3-month evaluation

Sample CollectionSample CollectionTwice WeeklyTwice Weekly

Intermittent Reinforcement Schedule:Intermittent Reinforcement Schedule: Draws from the Abstinence BowlDraws from the Abstinence Bowl
Good
JobGood
Job
Good Job
Small Small
Small
Large
Large
Jumbo
Good Job
Good Job
Good Job
Good Job
Good Job
Small
Good Job
Small

Draws Escalate with Draws Escalate with Stimulant- and Alcohol-Free Test ResultsStimulant- and Alcohol-Free Test Results
Weeks Drug Free
# Draws
1
2
4
5
3

Bonus Draws for Bonus Draws for Opiate and Marijuana AbstinenceOpiate and Marijuana Abstinence
Weeks Drug Free
# Draws2 2 2 2 2

Half the chips are winners Half the chips are winners Examples of PrizesExamples of Prizes
SMALLSMALL ($1-$5 items)($1-$5 items)
LARGELARGE($20 items)($20 items)
JUMBOJUMBO($80-$100 items)($80-$100 items)
42% 8%

Total Earnings
• $400 in prizes could be earned on average– If participant tested negative for all targeted
drugs over 12 consecutive weeks

MIEDAR: Who participated and how did it turn out?

PATICIPANT DEMOGRAPHICS
METH PSYCH
(N=388) (N=415)
FEMALE (%) 45 55MINORITY (%) 49 58AGE (mean yrs) 42 36EDUC (mean yrs) 12 12EMPLOYED (%) 32 35PROB/PAROLE (%) 16 36METH DOSE(mg) 86 ---TIME IN TX (mos) 9 1

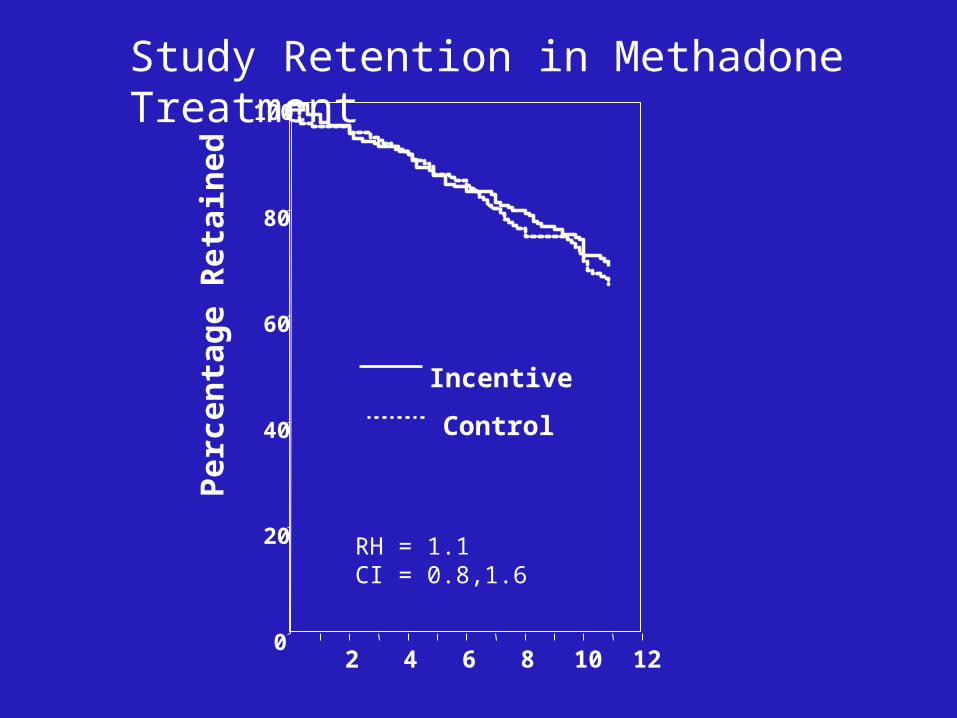
METHADONE PROGRAM STUDY RESULTS
Per
cen
tage
Ret
ain
ed
0
20
40
60
80
100
2 4 6 8 10 12
RH = 1.1 CI = 0.8,1.6
Study Retention in Methadone Treatment
Control
Incentive

Percent Stimulant Negative Urines
0
20
40
60
80
100
1 3 5 7 9 11 13 15 17 19 21 23
Study Visit
Per
cen
tag
e o
f st
imu
lan
t n
egat
ive
uri
ne
sam
ple
s
Abstinence IncentiveUsual Care
OR=1.91 (1.4-2.6)

Individual Subject Performance
21% Incentive vs
8% control
had prolonged abstinence outcome (19-24 Stimulant Negative Urines)

Outpatient Psychosocial Clinics: Contrasting Outcomes

Percent Stimulant Negative Urines
0
20
40
60
80
100
1 3 5 7 9 11 13 15 17 19 21 23
Study Visit
Per
cen
tag
e o
f st
imu
lan
t n
egat
ive
uri
ne
sam
ple
s
Abstinence Incentive
Usual Care
Study Week
Per
cen
tage
Ret
ain
ed
0
20
40
60
80
100
2 4 6 8 10 12
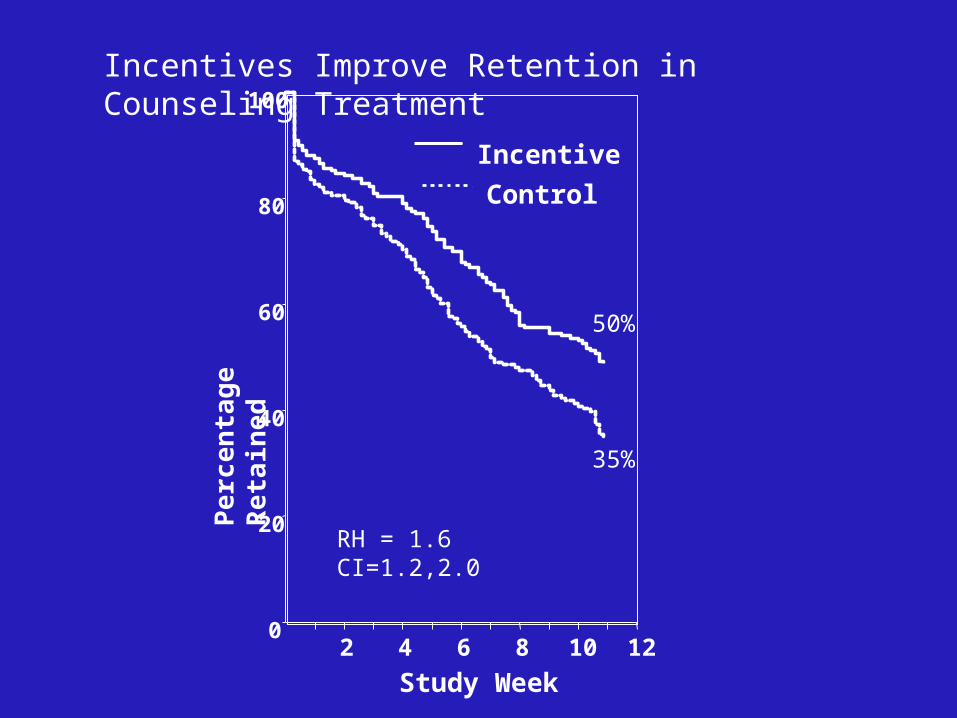
RH = 1.6 CI=1.2,2.0
Incentives Improve Retention in Counseling Treatment
Control
Incentive
50%
35%
Psychosocial Site Differences: Raising Performance
• Abstinence incentives worked best in clinics with lower retention – Control mean = 3.6 - 6.8 weeks
• Clinics where clients were usually retained for 8 weeks didn’t show improved retention with incentives
Individual Subject Performance
19% incentive vs 5% control had 12 weeks of stimulant negative samples

RESEARCH CONCLUSIONS
Incentives can improve client outcomes on retention and drug use when implemented in community treatment programs

Dissemination/Adoption
• Clearly recognized as one evidence-based practice advocated by program funders and licensers
• 1/4 - 1/3 of clinics are currently using incentives- mostly to reinforce attendance (Roman et al., 2010)
• Information on what it is and how to do it increasingly available– e.g. PAMI materials at www.nattc.org– programs such as this one today

Should Kids Be Bribed To Do Well In School?
TIMEMAGAZINE
April 8, 2010
Why Adopt Motivational Incentives?
from Kellogg et al., Something of Value, JSAT, 2005

49
Counselors Come to Understand Reinforcement
• “We came to see that we need to reward people where rewards in their lives were few and far between
• We use the rewards as a clinical tool – not as
bribery, but for recognition • The really profound rewards will come later”

50
Clients Like it• “Clients are proud and are having fun • Early in treatment, when their name is called out,
they are feeling good that they are being acknowledged
• For once in their life, they are being rewarded for
something”

51
Contributes to Positive Clinician-Client Interaction
• When patients publicly, and sometimes tearfully, acknowledged the counselor’s help in public, the staff felt a sense of gratitude
• “In the last two award ceremonies, clients said, ‘I want to thank the staff….’ That sounded real good – we felt appreciated”

Looking Into the Future
Peace, Prosperity and…
Prizes in every clinic!

Motivational Incentive Workshops

QuickTime™ and aPhoto - JPEG decompressor
are needed to see this picture.
Fourth Visit
Date:
Second Visit
Date:
Third Visit
Date:
Task:
3 NegativeUAs
First VisitDate:
Task:
ProbationOfficeVisit
Task:
Negative UA
Task:
Negative UA14 DayAnniversary!
Christine HigginsDissemination SpecialistCTN Mid Atlantic Node
Incentive Approaches for Clinicians

Ashli Sheidow, Ph.D.Associate Professor PsychiatryFamily Services Research CtrMedical Univ South Carolina
Incentive Contracting for Adolescents

QuickTime™ and aPhoto - JPEG decompressor
are needed to see this picture.
QuickTime™ and aPhoto - JPEG decompressor
are needed to see this picture.
Jim BeitingExecutive DirectorCommunity Behavioral HealthHamilton, Ohio
Incentive Implementation for Administrators
Salon A