considerations for food contact materials for foods for infants susceptible populations food...
TRANSCRIPT
Considerations for Food Contact Materials for Foods for Infants
Susceptible Populations Food Advisory Committee Meeting
Tuesday, December 16th, 2014
April P. Neal Kluever, Ph.D., D.A.B.T.ToxicologistFDA/CFSAN/OFAS/DFCN
Today’s Presentation:Special Considerations for Infants in the Context of Food Packaging
• Exposure considerations• Biological considerations• Safety assessment considerations
Conclusions
2

Special Considerations for Infants in the Context of Food Packaging
1. Exposure considerations
3

Infants experience a unique exposure scenario
1. American Academy of Pediatrics recommends that infant formula or breast milk be the sole source of nutrition for the first 6 months after birth
2. Infants consume more food per kg bodyweight per day compared to adults
Together, there is potential for elevated exposure to food packaging migrants for infants aged 0-6 months
4

Infant Dietary Intake• NHANES food-intake data (2005-2010) was used to determine
values for both body weight and infant food consumption for infants 0-6 months
• Values indicative of the highest food intake to body weight ratio were used to represent potential worst-case exposure scenarios
5
Infant body weight: 6.3 kg
Infant formula intake:
140 g/kg bw/d (900 g/infant/d)
General dietary intake:
50 g/kg bw/d (3000 g/person/d; 60 kg person)
Special Considerations for Infants in the Context of Food Packaging
1. Exposure considerations
2. Biological considerations
6

Potential for elevated exposure to food contact substances occurs during period of
development
Developing systems:– Reproductive– Endocrine– Neurological– Skeletal– Immunological
Developing Physiology:– Absorption– Distribution– Metabolism– Excretion
7
For in-depth review, see Neal-Kluever et al, 2014, Food and Chem. Toxicol. 70: 68-83

Developing Physiology: Infant Pharmacokinetics (or Toxicokinetics)• Highly variable• Rapid changes in the first 6 months after birth• Altered absorption, distribution, metabolism,
excretion, and storage of xenobiotics• Altered PK/TK can have a large impact on the
toxicity of a chemical and infant susceptibility
8
Developing Systems: Reproductive• Male
– The developing testis is particularly sensitive during the early postnatal period
• Female– Developmentally-sensitive windows for female
reproductive organs occur prenatally or later in development (around puberty)
– Possibility remains that developmental exposures may have latent effects not detectable until reproductive maturation
9

Developing Systems: Endocrine Hypothalamic-Pituitary-Adrenal (HPA) Axis
Transient activity in perinatal period before entering the “juvenile pause”
Influences:• Initiation of puberty• Stress response• Behavior
Hyman SE (2009) Nat Neurosci. 12:241-243
Hypothalamus

Developing Systems: Endocrine Hypothalamic-Pituitary-Gonadal (HPG) Axis
Transient, pulsate activity in immediate postnatal period before entering the “juvenile pause”
Influences:• Reproductive organ maturation • Initiation of puberty• Sexual behavior
11Pinilla L (2012) Physiol Rev 92:1235-1316

Developing Systems: Skeletal
• Neonatal bone is remodeled extensively during the first few postnatal years
• Several important milestones are achieved during the first 6 months after birth involving bone ossification, growth, and vascularity
• Stunted skeletal growth can predispose infants to increased fracture risk later
12

Developing Systems: Nervous
• Many important developmental processes are ongoing in the early postnatal period (synaptogenesis, myelination, etc)
• Neurotoxicity during this period can result in latent and long-lasting effects on behavior, cognition, and other neurological functions
13
Developing Systems: Immunological
Immune system= innate and adaptive immunityInnate immunity (non-specific; phagocytes and soluble factors)
• Deficient in infants
Adaptive ImmunityHumoral (B cells; antibody-dependent)
• Deficient in infants
Cell-mediated (T-lymphocyte dependent)• Different in infants (Th2 vs Th1 bias)
14
Special Considerations for Infants in the Context of Food Packaging
1. Exposure considerations
2. Biological considerations
3. Safety assessment considerationsa) Safety testing tiers
b) Toxicological information useful for infant safety assessment
15
Safety Testing Tiers• The level of safety testing that is recommended
to support the safety of an FCS is largely determined by the cumulative estimated daily intake (CEDI) of the FCS.
• The CEDI is the sum of the estimated daily intakes (EDIs) of the FCS that may result from the application of the substance described in the notification and any other regulated food uses of the substance.
16
Safety Testing Tiers
17
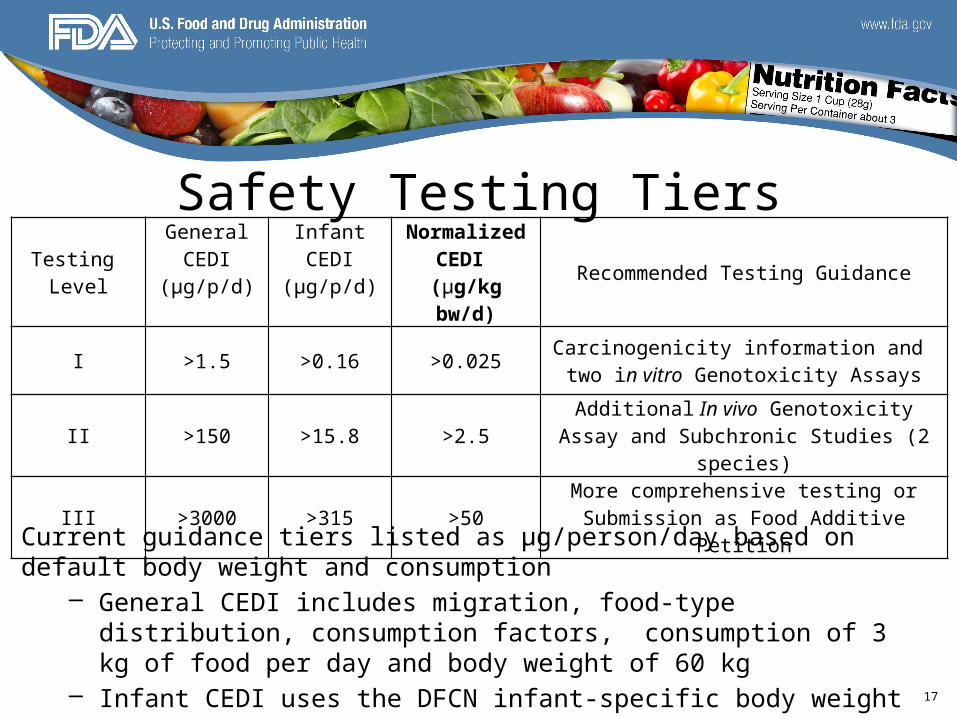
Testing Level
GeneralCEDI
(µg/p/d)
InfantCEDI
(µg/p/d)
Normalized CEDI
(µg/kg bw/d) Recommended Testing Guidance
I >1.5 >0.16 >0.025 Carcinogenicity information and two in vitro Genotoxicity Assays
II >150 >15.8 >2.5 Additional In vivo Genotoxicity Assay and Subchronic Studies (2 species)
III >3000 >315 >50 More comprehensive testing orSubmission as Food Additive Petition
Current guidance tiers listed as μg/person/day based on default body weight and consumption
– General CEDI includes migration, food-type distribution, consumption factors, consumption of 3 kg of food per day and body weight of 60 kg
– Infant CEDI uses the DFCN infant-specific body weight and intake
Toxicological Considerations in Infant Safety Assessment
• Do the available toxicity data or chemical structure suggest a concern for developmental toxicity, e.g., neurotoxicity, immunotoxicity, reproductive/endocrine toxicity, or other endpoints?
• Would any endpoints identified in a juvenile or adult animal toxicity study be expected to result in a different effect or change in magnitude or sensitivity of effect in a neonate or preweaned animal?
18

Toxicological Considerations in Infant Safety Assessment
• What other data may be useful to inform age- or species-dependent differences, e.g., ADME, MOA, PK/PD, TK/TD?
• Do the available data/testing address the concern identified? Can the available information address the variability or differences between infants and adults?
19
Conclusions• Infants can be a sole-source consuming
population with different physiology than adults.• Developing organ systems and different
physiology may alter susceptibility to toxicants
20
Conclusions• Normalizing dietary exposure to body weight
allows categorical classification into safety assessment tiers
• Careful consideration of the toxicity profile of potential food migrants is needed to determine whether additional testing for infant safety is needed.
21
Questions
22