conservative treatment of liver metastasis alvydas cesas md, head of chemotherapy department...
TRANSCRIPT

Conservative treatment of liver metastasis
Alvydas Cesas MD, head of chemotherapy department
Klaipeda Hospital
Frequency of Liver Metastasesof Colorectal Cancer
30 - 40% of colorectal primaries
Steele Jr G et al., Ann Surg, 1989


COLORECTAL CANCERLIVER METASTASES
Survivalbenefit
30%at 5 years
Resectable 10-20% Non resectable 80-90%
IV Chemo IA Chemo Others
Goal of chemotherapy for colorectal cancer liver metastases
• Management palliation and control symptoms
• Control tumor growth• Attempts to lengthen progression-free and
overall survival• Extreme care (chemotherapy) must be
taken to adequately assess each individual’s potential for both benefit and harm from chemotherapy

Goal of chemotherapy for colorectal cancer liver metastases
• Quality-of-life issues must be frankly and objectively discussed with patients about expectations can be within a realistic framework
• Keep in mind that virtually all of the clinical trials involving patients with metastatic disease were restricted by design to patients who were in good overall general condition.

Unresectable liver metastasis before treatment
Liver metastasis after 6 months treatment

The effects of chemotherapy for MCRC
• Objective response rates
• Time to disease progression
• Overall survival
• Quality of life

Chemotherapy Plus BSC Versus BSC Alone: Meta-analysis
Jonker W et al. Br Med J 2000;82:1789–94
Hine
Rougier
NGTATG
Scheithauer
Hafstrom
Allen-Mersh
Glimelius
Pooled
Relative risk (95% CI)
1.0 (0.41–2.45)
0.64 (0.46–0.92)
0.72 (0.54–0.95)
0.64 (0.44–0.93)
0.58 (0.34–0.99)
0.75 (0.53–1.06)
0.78 (0.40–1.53)
0.69 (0.60–0.81)
0.1 0.2 0.5 1 2 5 10
Risk ratio 1-year mortality
Favourschemotherapy
Favourscontrol

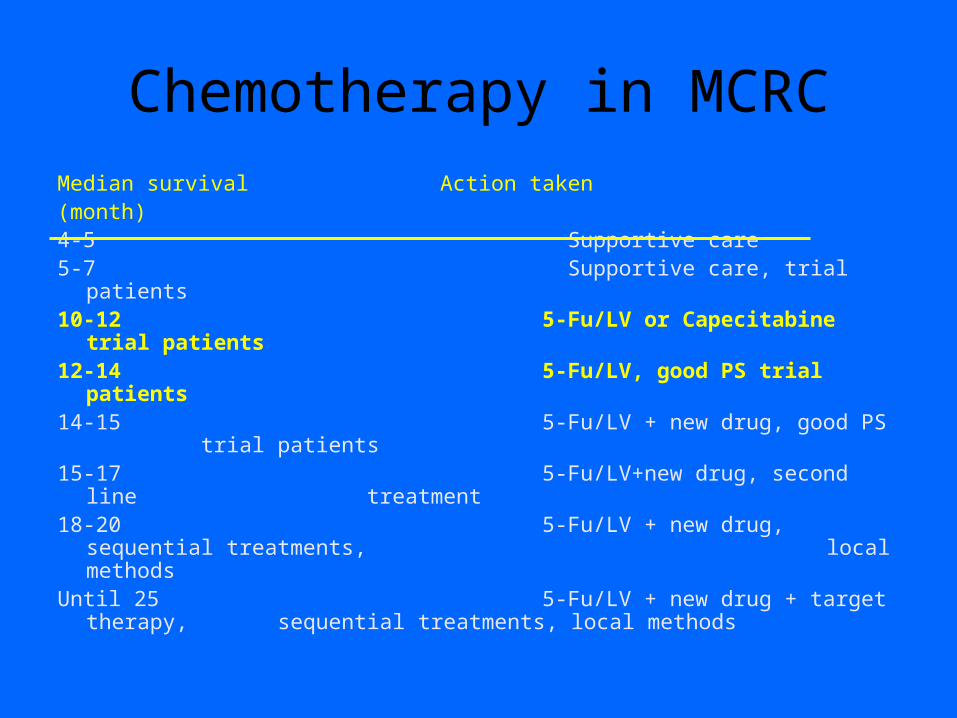
Chemotherapy in MCRC
Median survival Action taken(month)4-5 Supportive care5-7 Supportive care, trial patients10-12 5-Fu/LV, trial patients12-14 5-Fu/LV, good PS trial patients14-15 5-Fu/LV + new drug, good PS
trial patients15-17 5-Fu/LV+new drug, second line
treatment18-20 5-Fu/LV + new drug, sequential treatments,
local methodsUntil 25 5-Fu/LV + new drug + target therapy,
sequential treatments, local methods

Results of chemotherapy effects
• Until the very end of the 1980s there was no firm evidence that treatment had any meaningful influence on the well-being of many patients
• In 1989, two large randomised trials comparing 5-Fu alone and 5-Fu with biochemically modulated, reported slightly prolonged survival (median about 3 months) and QoL by the combined regimen.
NGTATG J Clin Oncol 1989,7:1437-1446; Poon MA et all J Clin Oncol 1989,7:1407-1418Borner MM et al Ann Oncol 1998,9:535-541Shmoll HJ et al Proc Am Soc Clin Oncol 2000,19:Abstr935

5-Fu regimes and leucovorin doses
• No firm evidence showing that any of the modulated 5-Fu regimens is superior to the others¹
• Low leucovorin dose is to be preferred for routine use since regimens using higher leucovorin doses are not superior²
¹Glimelius EJC Vol I;2003,6:173-180
²Sobrero AF et al J Clin Oncol 1997,15:808-815

Advanced CRC Meta-Analysis Project. J Clin Oncol 1992;12:960–9
TrialGITSGNCOGGOIRCGISCADGenovaTorontoCity of HopeRPCIBologna
Overall
Response rateodds ratio (95% CI)
Overall survivalodds ratio (95% CI)
0 0.5 1.0 1.5 2.0 0 0.5 1.0 1.5 2.05-FU + LV better/5-FU + LV worse5-FU + LV better/5-FU + LV worse
0.45(0.34–0.60)
0.97(0.86–1.09)
Meta-analysis: What is impact of 5-FU modulation with LV?
Chemotherapy in MCRC
Median survival Action taken(month)4-5 Supportive care5-7 Supportive care, trial patients10-12 5-Fu/LV or Capecitabine trial patients12-14 5-Fu/LV, good PS trial patients14-15 5-Fu/LV + new drug, good PS
trial patients15-17 5-Fu/LV+new drug, second line
treatment18-20 5-Fu/LV + new drug, sequential treatments,
local methodsUntil 25 5-Fu/LV + new drug + target therapy,
sequential treatments, local methods

5-Fu bolus vs. infusional
• High-dose infused regimens with modulated 5-Fu are likely superior to conventional bolus regimens, since they result in more tumour regressions, longer times to disease progression, less toxicity and/or longer overall survival.
Schmoll et al Proc Am Soc Clin Oncol 2000, 19:abst 935 de Gramont A et al J Clin Oncol 1997, 15: 808-815 Aranda E Ann Oncol 1998, 9:727-731 Weh HJ Oncologie 1998,21 403-407
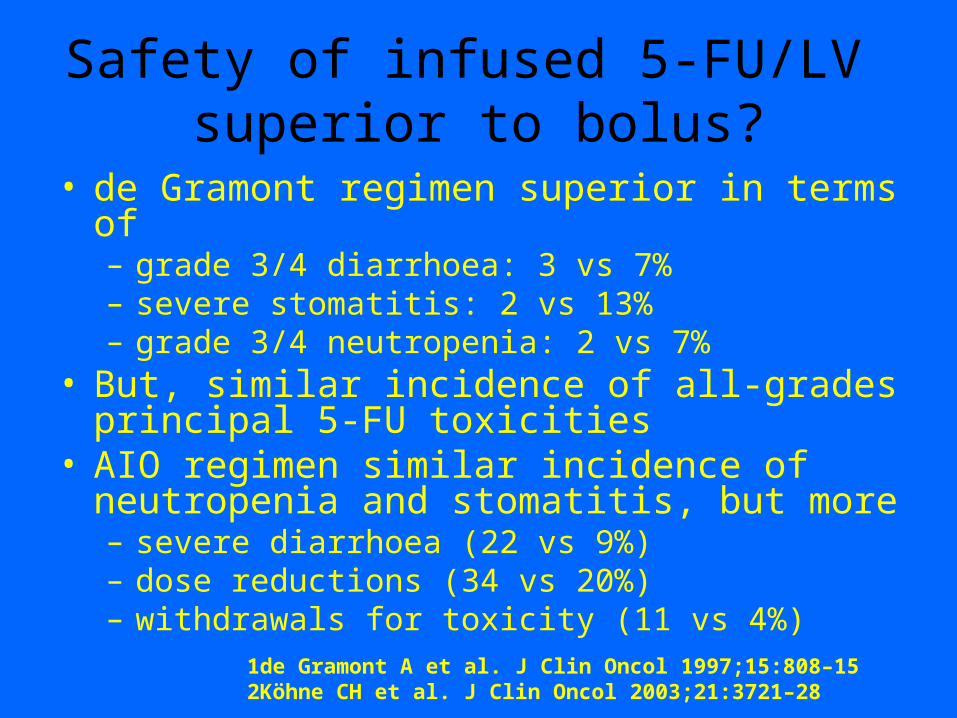
Safety of infused 5-FU/LV superior to bolus?
• de Gramont regimen superior in terms of – grade 3/4 diarrhoea: 3 vs 7%– severe stomatitis: 2 vs 13%– grade 3/4 neutropenia: 2 vs 7%
• But, similar incidence of all-grades principal 5-FU toxicities
• AIO regimen similar incidence of neutropenia and stomatitis, but more– severe diarrhoea (22 vs 9%)– dose reductions (34 vs 20%)– withdrawals for toxicity (11 vs 4%)
1de Gramont A et al. J Clin Oncol 1997;15:808–152Köhne CH et al. J Clin Oncol 2003;21:3721–28

How different are the 5-FU regimens?
1.0
0.8
0.6
0.4
0.2
0
de Gramont
Mayo Clinic
Time (months)
13.0 14.2
1.0
0.8
0.6
0.4
0.2
00 5 10 15 20 25 30 35 40
EORTC AIO
EORTC AIO
Mayo Clinic
12.0 13.212.5
0 5 10 15 20 25 30 35 40
Time (months)
Est
imat
ed p
rob
abili
ty
RR TTP
Mayo Clinic 14% 5.0 mo
de Gramont 33% 6.3 mo
RR TTP Mayo Clinic 12% 4.1 moAIO 9% 4.4 moAIO/LV 21% 6.4 mo

Pooled data of two identical phase III trials in first-line MCRC
First-line MCRC
Prior adjuvant >6 months ago
Capecitabine(n=603)
Bolus 5-FU/LV(n=604)
Twelves C. Eur J Cancer 2002;38(Suppl. 2):S15–S20
• Endpoints – ORR – PFS – overall survival – tolerability – pharmacoeconomics

Capecitabine in first-line MCRC: Pooled data of two phase III trials
• Endpoints – ORR +– PFS =– overall survival =– tolerability +
• pharmacoeconomics +
First-line MCRC
Prior adjuvant >6 months ago
Capecitabine(n=603)
Bolus 5-FU/LV(n=604)
Twelves C. Eur J Cancer 2002;38(Suppl. 2):S15–S20

Chemotherapy in MCRCMedian survival Action taken(month)
4-5 Supportive care5-7 Supportive care, trial patients10-12 5-Fu/LV, trial patients12-14 5-Fu/LV, good PS trial patients14-15 5-Fu/LV + new drug, good PS
trial patients15-17 5-Fu/LV+new drug, second line
treatment18-20 5-Fu/LV + new drug, sequential
treatments, local methodsUntil 25 5-Fu/LV + new drug + target therapy,
sequential treatments, local methods
Combination Therapy
• Irinotecan improves RR, TTP and survival
– in first line (with 5-FU/LV)1,2
– in second line polychemotherapy1 and monotherapy3
• Oxaliplatin with 5-FU/LV
– improves RR and TTP in first line4,5
– is effective in 5-FU resistant disease in second line6
1Douillard JY et al. Lancet 2000;
2Saltz LB et al. N Engl J Med
20003Rougier P et al. Lancet 1998;
4de Gramont A et al. J Clin Oncol
20005Giacchetti S et al. J Clin Oncol 2000;
6André T et al. Ann Oncol
1999

Combination Therapy
Irinotecan/5-FU/FA is more active than 5-FU/FA in metastatic CRC, offering improved tumour control and prolonged survival with a manageable adverse event profile and can therefore be considered as a standard treatment
Bolus & Infusional regimens of 5-FU/FA/irinotecan are safe and have a manageable toxicity pattern. Infusional regimens may have a better risk/benefit ratio than bolus 5-FU/FA/irinotecan regimens

Combination Therapy
• Addition of oxaliplatin to 5-FU/LV – improves all efficacy outcomes in first line (1-3)– is effective in irinotecan-pretreated patients in
second line (4,6)• Addition of irinotecan to 5-FU/LV improves efficacy in
first line (6,7) • Combinations with infused 5-FU favoured in Europe
while bolus preferred in USA
1de Gramont A et al. J Clin Oncol 2000;18:2938–47; 2Giacchetti S et al. J Clin Oncol 2000;18:136–473Goldberg R et al. Proc Am Soc Clin Oncol 2003;22:252 (Abst 1009)4Rothenberg ML et al. J Clin Oncol 2003;21:2059–695Rothenberg ML et al. Proc Am Soc Clin Oncol 2003;22:252 (Abst 1011)6Douillard JY et al. Lancet 2000;355:1041–7; 7Saltz LB et al. N Engl J Med 2000;343:905–14

1st line 5-FU/LV +/– irinotecan
Regimen
Responserate (%)
PFS(months)
Median survival(months)
Bolus(USA)1
Irinotecan/5-FU/LV
5-FU/LV
Irinotecan
39*
21
18
7.0*
4.3
4.2
14.8*
12.6
12.0
Infused(Europe) 2
Irinotecan/5-FU/LV
5-FU/LV
35*
22
6.7*
4.4
17.4*
14.1
Combineddata 3
Irinotecan/5-FU/LV
5-FU/LV
37*
21
6.9*
4.3
15.9*
13.3
*p<0.05 (vs 5-FU/LV)
1Saltz LB et al. N Engl J Med 2000;343:905–142Douillard JY et al. Lancet 2000;355:1041–7
3Saltz LB et al. Proc Am Soc Clin Oncol 2000;19:242a (Abst 938)

0
20
40
60
80
100
0 1 2Years
Aliv
e (%
)
IFL
FOLFOX
IROX
IFL vs FOLFOX p=0.0001 IFL vs IROX p=0.04FOLFOX vs IROX p=0.09
Goldberg RM, et al. Proc Am Soc Clin Oncol 2003;22:252 (abst 1009)
Addition of oxaliplatin later shown also to prolong survival 1st line

XELOX compares favourablywith FOLFOX
1Van Cutsem E et al. Proc Am Soc Clin Oncol 2003;22 (Abst 1023)2Goldberg R et al. Proc Am Soc Clin Oncol 2003;22:252 (Abst 1009)
3de Gramont A et al. J Clin Oncol 2000;18:2938–47
XELOX (n=96) 1
FOLFOX4 (n=267) 2
FOLFOX4 (n=210) 3
PR + CR (%) 55 45 50
PFS (months) 7.6 8.7 8.2
OS (months) 19.5 19.5 16.2

Chemotherapy in MCRCMedian survival Action taken(month)
4-5 Supportive care5-7 Supportive care, trial patients10-12 5-Fu/LV, trial patients12-14 5-Fu/LV, good PS trial patients14-15 5-Fu/LV + new drug, good PS
trial patients15-17 5-Fu/LV+new drug, second line
treatment18-20 5-Fu/LV + new drug, sequential treatments,
local methodsUntil 25 5-Fu/LV + new drug + target therapy,
sequential treatments, local methods

1st line Irinotecan/5FU/LV ± bevacizumab
No Bevacizumab Past
Disease Progression
May Receive Bevacizumab
Past Disease Progression
May Receive Bevacizumab
Past Disease Progression
IFL: bolus 5-FU 500 mg/m2
leucovorin 20 mg/m2
irinotecan 125 mg/m2
5-FU/LV: bolus 5-FU 500 mg/m2
leucovorin 500 mg/m2
BV: 5 mg/kg
Previously Untreated
Metastatic CRC
IFL + BV(N = 403)
5-FU/LV + BV(N = 110)
IFL + Placebo
(N = 412)
Hurwitz H, et al. N Engl J Med 2004;350:2335–42

Effect on overall survival of adding bevacizumab to 1st line
IFL
Pro
bab
ilit
y o
f su
rviv
al
1.0
0.8
0.6
0.4
0.2
00 10 20 30 40
Survival (months)
IFL + placebo
IFL + bevacizumab
Median survival (months)IFL + placebo: 15.6 (95% CI: 14.3–17.0) vsIFL + Avastin: 20.3 (95% CI: 18.5–24.2)HR=0.66 (95% CI: 0.54–0.81)p<0.001
Kaplan-Meier curve Hurwitz H, et al. N Engl J Med 2004;350:2335–42

Phase III trial of IFL ± Avastin in metastatic CRC (AVF2107g): progression-free survival
Median progression-free survival (months)IFL + placebo: 6.2 (95% CI: 5.6–7.7)IFL + Avastin: 10.6 (95% CI: 9.0–11.0)HR=0.54 (95% CI: 0.45–0.66) p<0.001
Pro
babili
ty o
f bein
g p
rogre
ssio
n-f
ree
1.0
0.8
0.6
0.4
0.2
00 10 20 30
Progression-free survival (months)
6.2 10.6
IFL + Avastin
IFL + placebo
Hurwitz H, et al. N Engl J Med 2004;350:2335–42

Improvements in the RR of MCRC to 1st line infusional 5-FU based chemotherapy
0
10
20
30
40
50
60
70
5-FU 5-FU/FA FOLFIRI, FOLFOX (inf),
Bevacizumab + IFL Cituximab + IRI / 5-FU/FA
(inf)
RR (%)

Overall survival: first-line fluoropyrimidine combination
regimens5-FU/LV (Saltz)
5-FU/LV (Douillard)
5-FU/LV (de Gramont)
0 5 10 15 20 25Median OS (months)
IFL (Goldberg)
IFL (Saltz)
FOLFIRI (Douillard)
FOLFOX (de Gramont)
FOLFOX (Goldberg)
IFL+ Avastin

FOLFOX4 after failure of irinotecan/5-FU/LV (IFL) 2nd line
Rothenberg M, et al. Proc Am Soc Clin Oncol 2003;22:252 (abst 1011)
Pro
bab
ilit
y
1.0
0.8
0.6
0.4
0.2
00 5 10 15 20
Months
5.62.6
1.9 FOLFOX4Eloxatin®
LV5FU2
RR TTP OS
FOLFOX4 9.6% 5.6 mo 9.8 moLV5FU2 0.7% 2.6 mo 8.7 mo Eloxatin® 1.5% 1.9 mo 8.1 mo

Mono ComboNo. 111 218
Survival(months) 6.9 8.6 P = NS
11 23 P < 0.05
HR (95% CI): 0.54 (0.42; 0.71)log rank p-value < 0.0001
0
0.2
0.4
0.6
0.8
1
0 2 4 6 8 10 12
Pro
po
rtio
n
Cetuximab +/- irinotecan 2nd lineafter irinotecan failure
Time to progression (months)
Response Rate (%)
Cunningham, Van Cutsem et al 2003 Proc Am Soc Clin Oncol 22: Abstract 1012

Cituximab as single agent in 2nd line treatment of irinotecan-refractory
mCRC
* ~ 40% of pts received cituximab as a 3rd or higher line treatment
Pts RR Dis Con mTTP mS
Saltz 2002 57 11% 34% 1.4 mths 6.4 mths
Cunningham 2003*
111 11% 34% 1.5 mths 6.9 mths

Cituximab plus irinotecan is active 2nd line in irinotecan-refractory mCRC
Saltz et al 2001 Proc Am Soc Clin Oncol 20: Abstract 7
Efficacy results
PR 27 / 120 (23%)
Disease control 36 / 120 (30%)
Median duration of response (MDR) 6.2 mths

HAI and systemic chemotherapy in randomized studies
Response rate 2-years survival
No. pts. HAI SYS p HAI SYS p
MSKCC 162 53 21 .001 17 12 -
NCI 64 62 17 .003 47 13 -
French 163 49 14 NS 22 10 .02
German 168 43 20 - 12,7 17,6 -
CALGB 135 48 25 .009 22,7 19,8 .027

Drugs for HAI Drug Half-life (min) Estimated Increased Exposure
bay HAI
5-Fluoruracil 10 5-10 foldFloxuridine <10 100-400 foldCarmustine < 5 6-7 foldMitomycin C <10 6-8 foldCisplatin 20-30 4-7 foldAdriamycin 60 2 fold
Vincent T. De Vita Cancer principles and practice of oncology 2005 7-th

Survival after Adjuvant Therapy Subsequent to liver resection with HAI and systemic therapy versus systemic therapy alone
Survival rate HAI+SYS
Comparison (n=74) SYS (n=82) P value
2-Y survival 85% 69% .02
2-Y hepatic DFS 89% 57% .00001
2-Y DFS 57% 41% .07
Kemeny MM et al N Engl J Med 1999:341-2039

Time from Second Progression to Death
• MST from 2nd line 9-10 months • TTP 2nd line 3- 4 months• Time from 2nd P to death 6 months
– From Cunningham and Rougier 1999
• MST folfiri folfox 21 months• TTP 1st + 2nd line 14 months• Time from 2nd P to death 7 months
– From Tournigand ASCO 2001
WHY NOT THIRD LINE CT ?

Where are we now?In the metastatic setting…….1. Addition of bevacuzimab to bolus 5-FU/irinotecan
prolongs survival as 1st line therapy2. After irinotecan failure, addition of cetuximab is an
alternative to FOLFOX as 2nd line treatmentBut • Unclear yet if both agents also effective with 5-FU
alone, Xeloda alone or oxaliplatin combinations• Optimal sequence not known• Don’t know how to tailor treatments to specific patients

Patient selection: Trials and the real world
Trials patients
1. Young and fit
2. Normal liver and renal function
3. Limited other medication
4. Treated at specialist units
5. Specific tumourand drug free!

Patient selection: Trials and the real world
Trials patients
1. Young and fit
2. Normal liver and renal function
3. Limited other medication
4. Treated at specialist units
5. Specific tumourand drug free!
Clinic patients
1. Older and less fit
2. Liver/renal function often abnormal
3. Many of them on other drugs
4. Treated by general oncologists
5. Variety of tumours?and drug costs money
Potential Prognostic Subgroups
• Older patients (>65 years old)• Poor performance status (>0)• >1 metastatic site• Prior adjuvant therapy with 5-FU/LV• Elevated LDH, alkaline phosphatase,
WBC

Prognostic Factors for Advanced CRC
AP = alkaline phosphatase
ECOG performance status
>1 0–1
WBC No. of sites
>10K <10K >1 1
No. of sites AP
>1 1 >300 <300
MST = 6 months MST = 10 months MST = 15 months
From Koehne, Ann. Oncol 2001
Conclusion Active drugs have had a dramatic impact on the treatment of colorectal cancer metastases:
• Capecitabin (tolerability), • Cetuximab (time to progression),• Irinotecan, oxaliplatin, bevacuzimab (survival)• HAI + Systemic chemotherapy improved
survival and hepatic DFS
Future improvements are probable using a multididciplinary approach, together with a hope that new treatments, based upon recent tumor-biological knovledge, will eventualy yield clinically meaningful effects.