congreso europeo de autonomia personal y dependencia mérida /spain 9. - 10. märz 2009 the many...
Post on 18-Dec-2015
213 views
TRANSCRIPT

CONGRESO EUROPEO DE AUTONOMIA PERSONAL Y DEPENDENCIAMérida /Spain • 9. - 10. März 2009
The many faces of ageing:A challenge for the politicians of the
European countries
Prof. Dr. Dr. h.c. Ursula LehrDepartment of Gerontology, University of Heidelberg

It is not only important to add years t o live
but also to add life to years.
Our life expectancyis dependent from our life style.
It does not only count how old one will be, but how one will get old.

AGEING has many faces:
The competent and wise senior
who is able to manage his/ her own life
and the helpless and dependent senior
who needs help and support
Chronological age is a very problematic criterion upon which to base political measures

AGEING has many faces:
The competent and wise senior
who is able to manage his / her own life
and the helpless and dependent senior
who needs help and support
Chronological age is a very problematic criterion upon which to base political measures

Politicians and Scientists of all disciplines and faculties,
administrators and practionners, too,
have to discuss the question of longevity combined with a state of psychophysical wellbeing,
the question of an Ageing Society.

What can be done to assure
a healthy and competent ageing?
What can be done to assure quality of life in old age?
What can be done to prevent illness, diseases and dependency?
What can be done to assure a high quality of life in old age – also for disabled and frail dependents?

The demographic change
I. The demographic change1. the rise of the individual life expectancy;
- the greying society2. the necessity for a preventive environment:
age-friendly cities and products
II. Ageing and dependency1. the change in the household-structure2. number of people needing long-term-care3. the limitation of family care,
the need of ambulant services and institutions
III. A policy for healthy ageing 1. prevention and rehabilitation
2. long- term- care

63,168,0 69,6
77,975,1
81,677,7
83,8
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
90,0
1950 2000 2025 2050
1950-2050
€ € €€
Life expectancy in Europe

Life expectancy at birth in the European countries in the year 2003
Eurostat Database 2005
74,8 75,1 74,975,5 75,4
77,2
75,875,2
76,9
74,1
76,1 76,0
74,075,1
77,9
76,2
78,777,8
81,1 81,1
79,5
81,380,7
83,782,9
80,3
82,9
80,8 80,881,8
80,581,8
82,4
80,7
82,5 83,0
60,0
65,0
70,0
75,0
80,0
85,0
90,0
EU BE DK DE GR ES FR IRL IT LU NL AT PT FIN SE GB IS CH
Life Expectancy Females
Life Expectancy Males

Eurostat Database 2005
68,9
76,1
72,0
65,3
68,4
65,566,3
75,9
70,5
67,5
69,9
72,7
75,6
81,0
78,577,1 76,7 76,7
77,7
81,0
78,9
74,9
77,8
80,5
60,0
65,0
70,0
75,0
80,0
85,0
90,0
Bulgaria
Cypru
s
Czech
Rep
Estonia
HungaryLatv
ia
Lithuan
iaMalt
a
Poland
Romania
Slovakia
Slovenia
Life Expectancy Males
Life Expectancy Females
Life expectancy at birth in the new European countries in 2003
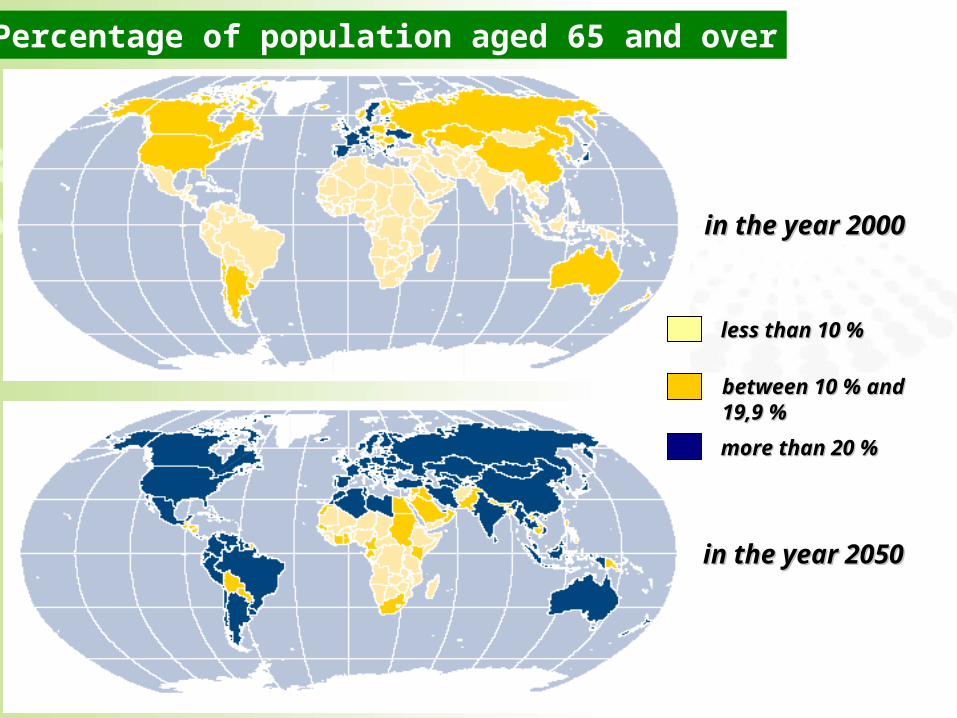
in the year in the year 20002000
in the year in the year 20502050
less than 10 less than 10 %%
between 10 % and between 10 % and 19,9 %19,9 %
more than 20 more than 20 %%
Percentage of population aged 65 and over

Percentage of persons 60 +in some European countries
0
5
10
15
20
25
30
35
40
45
50
D E I A CH F
%
1950 1975 2000 2025 2050
Quelle: UN (2002), World Population Ageing 1950-2050

Percentage of people 60 +
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
40,0
45,0
1950200020252050
%
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
40,0
45,0
50,0

in some European countries
0
2
4
6
8
10
12
14
16
D E I A CH F
%
1950 1975 2000 2025 2050
Quelle: UN (2002), World Population Ageing 1950-2050
Percentage of people 80 +

1950200020252050
0,0
2,0
4,0
6,0
8,0
10,0
12,0
14,0
16,0
0,0
2,0
4,0
6,0
8,0
10,0
12,0
14,0
16,0
%
Percentage of people 80 +

Percentage of people 90 plusand 100 plus in Germany
501300
10000
1047000
44000
2100000
114700
2000 2020 2050
über 90 Jahre über 100 Jahre
Quelle: UN (2002), World Population Ageing 1950-2050

1745 18271959
2164
25152756
2948 2843
3483
3883 38834122
48365120
5480
4360
2333
3098
0
1000
2000
3000
4000
5000
6000
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
number of people in Germany, which celebrated their 100. birthday in the years…

Number of people 105 years and olderin Germany
Gesamt Frauen Männer
bis 1990: BRDab 1991: BRD und ehemalige DDR
0 516
24
61 6353
73 73
99
131 133
154165 163
196205 206
217
243
274
316
1965
1970
1975
1980
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
364
2005
385
2006
443
2007

Fertility Rate in EU- countries 1950-2000
0,00,51,01,52,02,53,03,54,04,5
Belgien
Bulgarien
Dänem
ark
Deutsc
hland
Estlan
d
Finnland
Frankre
ich
Griech
enlan
dIrla
ndIta
lien
Lettlan
d
Litauen
Luxemburg
Malta
0,00,51,01,52,02,53,03,54,04,5
Niederl
ande
Österre
ichPolen
Portugal
Rumänien
Schwed
en
Slowakei
Slowenien
Spanien
Tsch.R
ep.
Ungarn
UKingdom
Zypern
195019752000

33%
11%
The percentage of childless womenin Germany (cohort 1950,1960 and 1965)
21%
1950 Geborene 1960 Geborene 1965 Geborene(Schätzung)

The decrease of the birth rate can be stopped only by the
chance of combining job and family.
It is necessaryfor women and men
to include job and familyin their future planning.

2,03,63,22,4
One person 75 and older in relation to younger persons
Quelle: Statistisches Jahrbuch 2006, 1: Schätzung aufgrund der 10. koordinierten Bevölkerungsvorausberechnung2: Schätzung aufgrund der 11. koordinierten Bevölkerungsvorausberechnung
0-20 20-40 40-60 60-75
36
23
15
5
25
22
15
5
14
15
11
5
11
10
10
4
46
7
8
3,90
20
40
60
80
1890 1925 1939 1950 1970 2006 2015 2040 2050
79
67
45
35
25
8,46,21
3,92
11,2
1,62,92,31,7
1,42,01,61,2
4,72

Quelle: Statistisches Bundesamt (2002).Statistisches Jahrbuch 2002 (ab 2001 inkl. Neue Länder) Bundesamt für Statistik (BFS) (2003), Demografisches Portrait der Schweiz 2002Statistik Austria (2005). Statistisches Jahrbuch 2003. Statistisches Bundesamt (2001). 9. Koordinierten Bevölkerungsvorausberechnung
Anzahl der jüngeren Personen
79
67
45
35
25
14,8 12,46,2
88
51
39
28
78
64
46
31
2115 12,6
7
68
15,513,1
7,5
0
10
20
30
40
50
60
70
80
90
100
1880 1923/25 2001* 20401934/39 1950/51 1970/71 1991/94
One person 75 and older in Germany, Austria and Switzerlandin relation to younger persons

Mobility (walking impairment: arthrosis, arthritis, osteoporosis)
Fine motor skills (decreased sensitivity of skin, limited mobility of hands and joints)
Sensory properties (problems with eyes, variation of the vision of coloures, reduction of the field of view, hearing problems etc.)
Sensitivity (decreased sensation of touch)
Limitations regarding physical strength and endurance
75 years old are not yet in need of care, but there might be some physical impairments

The demographic change
I. The demographic change1. the rise of the individual life expectancy;
- the greying society2. the necessity for a preventive environment:
age-friendly cities and products
II. Ageing and dependency1. the change in the household-structure2. number of people needing long-term-care3. the limitation of family care,
the need of ambulant services and institutions
III. A policy for healthy ageing 1. prevention and rehabilitation
2. long- term- care

With increasingly poor health the environment, ecological factors, gains more influence.
Very often ecological variables (housing situation, rural or urban environments, transportation system etc.) will determine the degree of dependency.
Favourable ecological conditions extend the life space, unfavourable may result in a restriction and a loss of abilities and skills.Often an adaptation of the home to the specific needs of a person will contribute to more independence of a handicapped elderly

The Madrid- and the Leòn- Conference in 2007
also discussed the image of the aged,
their competencies, potentials and human
capital, but also their problems
and the necessity to adapt the environment to
this growing group of the elderly.
The WHO has created a model-programme of
“age-friendly cities”.

To create an environment
that is acceptable and human for the elderly,
is a challenge in our time of an ageing society.
It is necessary to create “age friendly cities!”

In order to prevent frailness and care dependencywe need a
„preventive environment“
On the one hand• barriers needs to be recognized and
removed,
On the other hand
• the living environment needs to be arranged in a way that may motivate psysical, mental and social activity

to cross the road safely:
traffic light with visual and auditory signals
and longer periods
Age-friendly cities

Town planning the condition of pavements influences walking in the lokal area (narrow, uneven, cracked, glittering looking or glassy) makes the (elderly) people unsecure and produces falls, produces dependency
cobbled pavement (wheelchairs, Rollatoren, Kinderwagen)

stairs (for bridges and tunnels): an elevator is necessary!
stairs must have railings on both sides; the first and the last steps must be marked
(visual problems)
public toilets, conveniently locateds
street signs
and house numbers
Town planning




Preventive environment:
to motivate physical and mental activity

niedrige Sitzgelegenheit ohne Armlehne
schlecht lesbare Mini-Bildlegenden

“Geronto-Ökologie”, a gerontological-ecological and
environmental approach, designed also for an
elderly population, has to be developed.
We need a “design for all” , an “universal design”.
Our industry has to realize the population change,
too: Easier handling of ticket machines, light switch,
armatures, telephone keyboard, the caps of jars and
bottles; video players must become easier to handle,
mobile phones should be more legible, PCs, etc.

The industrial sector needs to realize that society is ageing and have to change
some of its products

The industrial sector needs to realize that society is ageing and have to change some of its products
NährwertangabenSpeisequark 20 % Fett
100 g enthalten durchschnittlich:

Design for all ???

Einkaufen aus dem Blickwinkel reifer Kunden
www. Age-Explorer.de

Der Age Explorer® als Innovationsquelle
www. Age-Explorer.de

It is necessary to enable the society to meet the demographic change!
To change their attitude toward the aged,
to create a more positive image;- to change something in the environment
(city-planning, traffic system, to secure a greater mobility;)
- architects and designers need to adjust to an aging world.
Industry and factory have to realize the aging society and change some of their products to guarantee elderly people an independent life and social participation.

Ageing and dependency
I. The demographic change1. the rise of the individual life expectancy;
- the greying society2. the necessity for a preventive environment:
age-friendly cities and products
II. Ageing and dependency1. the change in the household-structure2. number of people needing long-term-care3. the limitation of family care,
the need of ambulant services and institutions
III. A policy for healthy ageing 1. prevention and rehabilitation
2. long- term- care

We have a trend from the three-generation-household over the two-generation-household to the one-generation-household - and from here to the
one-person-household.
Living-arrangements of the elderly together with their children are extremely rarely in many of the regions of Europe and will be reduced in the future.
This will have consequences for the potential care-givers, if they are needed.
More ambulant services and homes for the aged will be needed


In former times:Grandparents with many,many grandchildren
today:the only one grandchild with 4 grandparents and sometimes2 great-grandparents

7,1
44,4
19,416,1
36
4,4
0
5
10
15
20
25
30
35
40
45
50
1-Personen-Haushalte 5 und mehr Personen-Haushalte
%
1900 1950 2000
Quelle: Bundeszentrale für politische Bildung: Datenreport (2002), S.39
Changes in the household-structure in Germany (1900, 1950, 2000)

Percentage of persons (65+)living in an One-Person-Household in Germany
Quelle: Microcensus 2002; Altenbericht 2006, S. 176
65 - 69 70 - 74 75 - 79 über 80
19,1 23
35,9
50,3
65
87,4
34,9
16,9
0
10
20
30
40
50
60
70
80
90
100
FrauenMänner
%
% %% %

35,2%
14,9% 14,4%
31,0%
24,3%
30,3%
0%
5%
10%
15%
20%
25%
30%
35%
40%
Deuts
chla
nd
Spanie
n
Portugal
Frankr
eich
Italie
n
Öster
reic
h
Percentage of the Single-Households in other countries of the EU (2000)

Ageing and dependency
I. The demographic change1. the rise of the individual life expectancy;
- the greying society2. the necessity for a preventive environment:
age-friendly cities and products
II. Ageing and dependency1. the change in the household-structure2. number of people needing long-term-care3. the limitation of family care,
the need of ambulant services and institutions
III. A policy for healthy ageing 1. prevention and rehabilitation
2. long- term- care

Independent living ambulant care
and living in homes for the aged
81,1
63,2
40
12,4
21,7
30,7
6,5
15
28,6
80-85 years 85-90 years über 90 years
Percentage of people in Germany (2007)

Percentage of people with cognitive impairements
2,8%
6,0%
13,3%
23,9%
34,6%
1,2%
65 - 69 70 - 74 75 - 79 80 - 84 85 - 89 > 90
Alter in Jahren
Die Gesamtzahl der demenziell erkrankten Menschen liegt bei 800.000 – 1,2 Mio. (geschätzt). Etwa 50% der Demenzen werden dem Typ Alzheimer zugeordnet.

The number of people 80+ and 90+ will rise in all European Countries. The number of people needing help and care could increase - although it it expected that dependency and helplesness will start at an later age, fostered by a healthier life-style,by prevention and rehabilitation.
„The need for care will rise, but probably not in the high values projected under the constant-caring scenario…. Education promotes a healthy life style….However, the absolute and relative numbers of old people who need care are going to expand over the following decades.
At the same time, the proportion of middle-aged people who can provide care, decrease“
(Vaupel & Kistowski, 2008)

0
500
1000
1500
2000
2500
3000
3500
4000
4500
Pflegebedürftige 2040 2080 2360 2830 4100
Pflegeheimplätze 604 640 781 1122 2426
1 2 3 4 52001 2003 2010 2020 2050
Estimated number of dependent elderly people in Germany; the need for institutional care
Quelle: Institut der Deutschen Wirtschaft 2005
* in Tausend
*
*
im Jahr

Ageing and dependency
I. The demographic change1. the rise of the individual life expectancy;
- the greying society2. the necessity for a preventive environment:
age-friendly cities and products
II. Ageing and dependency1. the change in the household-structure2. number of people needing long-term-care3. the limitation of family care,
the need of ambulant services and institutions
III. A policy for healthy ageing 1. prevention and rehabilitation
2. long- term- care

1. the rising age of the person needing care
2. the rising age of the potential care-giver
3. family care is daughter care, the daughter is very often a grandmother herself
4. more women in the labor force
5. many elderly persons don‘t have children
Limitation and problems of family care

6. the number of children decreased; care cannot be shared by several
siblings
7. very often the one or two children are living far away from their parents - a necessity in industrial societies
8. the older generation is not too enthusiastic about living in a three-generation-household
9. there is an increasing divorce-rate (and women will not take care for their ex-mothers in law)
Limitation and problems of family care

"Families are less willing to care for older relatives than they used to be"
71
73
62
64
76
84
78
55
78
67
66
83
72
30
28
38
37
24
17
24
44
23
31
33
19
39
EUR 12
Belgium
Denmark
Germany
Greece
Spain
France
Ireland
Italy
Luxembourg
Netherlands
Portugal
United Kingdom
10 30 50 70 90
Agree Disagree
%
People aged 60+
Source: Walker, Maltby (1997): Ageing Europe

Families caring for an aged person should be supported;
We need a network of services for older people, living in their homes, - well distributed throughout the city;
We have an increased need of high qualified professional help and ambulant services;
We have to support voluntary organizations, where also the „young old“ can be active;
We need a well-developed volunteer infrastructure

The solution of the problems of the frail and dependent elderly person, the problem of ambulant services for the elderly, the problems of housing conditions and
the problems of caring are a challenge of our time of demographic change and increasing longevity!
What can be done to prevent dependency?

A policy for healthy ageing
I. The demographic change1. the rise of the individual life expectancy;
- the greying society2. the necessity for a preventive environment:
age-friendly cities and products
II. Ageing and dependency1. the change in the household-structure2. number of people needing long-term-care3. the limitation of family care,
the need of ambulant services and institutions
III. A policy for healthy ageing 1. prevention and rehabilitation
2. long- term- care

1. Maintaining and increasing the competence of the elderly in order to prevent dependency, to secure a healthy ageing with a high degree of quality of life
2. Extending and improving rehabilitation measures in order to re-enable the elderly to lead an independent life
3. Finding a solution to the problem of the dependent and frail elderly and the problems of providing adequate care for them
A policy for senior citizens

A policy for the elderly has to be more than just a policy for pensions systems and a policy for care – although they are very important - and has to include also other aspects than financial ones.
Maintaining and increasing the competence of
the elderly in order to prevent dependency is a
life-long process:
- To optimize development;
education and life-long learning
- to force prevention, preventive behaviour, healthy life-style
- to create an age-friendly environment

Health and well-being do`nt decrease with increasing age,
but you can find health only there,
where you are fighting for them everyday
(v. Weizsäcker)

not only by the absence of diseases
not only by psychophysical and psychosocial wellbeing
(WHO-Definiton)
Healthy ageing includes the ability to cope adequately with stress, health-problems, limitations and handicaps and to continue an enjoying life.
Healthy ageing is to be defined

Healthy ageing –a life-long process
Gerontology of intervention is based on
1. OPTIMIZATION 2. PREVENTION
3. REHABILITATION 4. MANAGEMENT
Schaffung günstiger Entwicklungsbedingungen in Kindheit
und Jugend
Vorbeugung von Krankheiten, Verhinderung von Abbau- und
Verlusterscheinungen
Weitestmögliches Rückgängigmachen von Störungen
"Management" von Situationen bei bleibenden Einschränkungen,
Zurechtkommen mit irreversiblen Problemsituationen, Sicherung des
Erreichten
WHO: HEALTHY AGEING IS ACTIVE AGEÌNG.

WHO-Modell: Healthy Ageing
Healthy Ageing
EnvironmentSystem Level
Social ecology economic culture political (in peace) health care system social security
PersonIndividual Level
mental physical functional capacity coping style / personality spiritual autonomy dignity interdependance optimalization / compensation

The importance of physical, mental and social activity must be made clear from childhood on.
It is also necessary to maintain a high degree of physical, social and mental activity in men and women during the years of adulthood.

PHYSICAL ACTIVITY is a prerequisit for healthy ageing.
Age-determined physical changes – such as
FUNCTIONAL IMPAIRMENTS OF THE ORGANS; CHANGES IN THE MOTOR-SYSTEM AND MUSCULAR SYSTEM AS WELL AS CHANGES IN THE RESPIRATORY ORGANS
are similar to the effect of lack of exercise.
The young physical inactive individual seems old-
Just as the old but active individual seems young.

Many studies have found, that mentally more active people, individuals with a higher range of interests, a father reaching future time perspective and a greater number of social contacts reach old age with greater feelings of psycho-physical wellbeing.
Cognitive activity is essential for healthy ageing.
Elderly persons must be given mental tasks; they must be challenged to mental activity. Reduction in mental activity can speed up the process of ageing.
Functions, which are not used, are decreasing
Mental ativity is a prerequisit of healthy ageing, too

Life-long learning
Age: Today and in the future
former times:
Old age
Adult
hood
young
leisuretime
work
educationB
ild
ung
Arb
eit
Fre
izei
t
nach Riley & Riley, 1992

A policy for the aged, however, should not be determined only by the question:
„What can we do for the aged?“
It also should be asked:
„What can the aged do for the society? “
Integration and participation of the elderly are a prerequisite for the quality of life of the elderly, for health and productivity; – but it is helpful also for the society.

A policy for healthy ageing
I. The demographic change1. the rise of the individual life expectancy;
- the greying society2. the necessity for a preventive environment:
age-friendly cities and products
II. Ageing and dependency1. the change in the household-structure2. number of people needing long-term-care3. the limitation of family care,
the need of ambulant services and institutions
III. A policy for healthy ageing 1. prevention and rehabilitation
2. long- term- care

Report by the European Commission: Employment, Social Affairs and Equal Opportunities DG (2008)
Reports on National Policy Developments (p16-34)
„EU Member States are strongly committed to ensuring access for all, to adequate health care and long-term care…….Long-term care does not refer to the same range of services in all countries. Some countries focus on the medical component, separating medical from social care.The provision of integrated services for dependent is not available everywhere.Many Member States wish to promote rehabilitative care;Often elements of medical and social care provided to dependent are not covered by the basic insurance packages….
Long-term Care in the European Union

Reports on National Policy Developments (p16-34)
„Spain is planning the implementation of a uniform basket of long-term-care services across the autonomous regions making long-term care accessibility a priority for social inclusion policy. The newly launched „Autonomy and Dependency Care System“ was designed to guarantee care for dependent and promote their autonomy. It provides for a wide range of care services both at home and in care centers, and for financial and every-day support to their families. 100% coverage by 2015 is the target“ (p.18)Many countries are firmely focussed on enhancing tailor-made home and community care services and moving away from institutional care… The goal is to help individuals to remain at home for as long as possible, while providing institutional care when needed.
Long-term Care in the European Union

Reports on National Policy Developments (p16-34)
> The quality of long-term care services varies widely both between and within countries
> Some Member States have introduced regulations and legislation for assessing and enhancing the quality of long-term care services
> The increased demand for long-term care services represents a policy challenge for many countries as current supply is considered to be insufficient and inadequate in terms of meeting current and especially future needs
Long-term Care in the European Union

founded in 2005North Rhine Westphalia (Germany)Andalucia + Extremadura (Spain)Burgenland (Austria)Gelderland + Limburg (The Netherlands)Lower Silesia (Poland)Mid-East-Region + Midland Region (Ireland)Scotland + West-Midlands (United Kingdom)
Silver Economy network of European regions

Silver Economy networkof European regions
The partners will develop a coordinated programme, which engage with a variety of players and stakeholders, will be tailored to specific regional requirements.…considering ways to improve the qualities ranging from services, tourism, culture, wellness and health to products of services which help support independent living.A checklist on “Minimum requirements for home-based services for older people” was developed

In 1995 introduced by law
82 million inhabitants – 2.1 million need care,(more than 80% of them are older than 60 years)
1.4 mill. are living in their own private home (68%) 0.7 mill are living in homes for the aged, (32%)
The LTCI is financed by a deduction directly from the salaries of those who are in the workforce and of the pensions of the retirees. Family members, who are not in the workforce, are included in the insurance of spouses or parents. – Employers and employees both pay half. The contribution rate was 1.7% in 1995 – but now it is 1.95% for persons with children and 2.2% for childless persons
Long-term Care Insurance in Germany

In 1995 introduced by law three different types of benefit:
- home care benefits - institutional care or nursing home benefits - other benefits, such as social security insurance for caregivers or modification for the private home
care level 1: 215.--€ 420.--€ 1.023.-- € monthly care level 2: 420.--€ 980.--€ 1.279.--€ care level 3: 675.--€ 1470.--€ 1.470.--€
Level 1: more than 45 minutes care and 45 minutes housekeeping
Level 2: two hours personal care and one hour housekeeping
Level 3: mire than 4 hours personal care, one hour housekeeping und help at night
Long-term Care Insurance in Germany

Independent living ambulant care
and living in homes for the aged
81,1
63,2
40
12,4
21,7
30,7
6,5
15
28,6
80-85 years 85-90 years über 90 years
Percentage of people in Germany (2007)

Armin LASCHET (2008):
“In any political debate demographic change and
ageing are commonly regarded as a treat. What
is required, however, is a shift in both, focus and
approach: we need to consider demographic
change and the ageing of our society as a
challenge and as a opportunity for both,
economic growth and improving Europe’s
competitiveness. In the ‘Silver economic network
of European regions’ we emphasise the
economic opportunities inherent in this
demographic change:”

Old age, longevity, should not be seen as a problem but as a chance and challenge – a challenge for everyone: for the aging individual, for his/her family and for our society.
We should not only ask for the problems and deficits of aging and old age. We have to ask for the resources, the new potentials of the aged, also for the competencies and potentials of the very old persons.
We have to see the aged of the 21st century as human capital.
