confounding and misclassification
TRANSCRIPT

8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 1/12
A M E R I C A N J O U R N A L O F E P I D E M I O L O G Y
Copyright © 1985 by The John* Hopkins University School of Hygiene and Public HealthAll rights reserved
VoL 122, No. 3Printed in U.SJi.
CONFOUNDING AND MISCLASSIFICATION
SANDER GREENLAND1-
3AND JAMES M. ROBINS
1
Greenland, S. (UCLA School of Public Health, Los Angeles, CA 90024), and J.
M. Robins. Confounding and misd assfflcation. Am J Epidemiol 1985; 122:495-506 .
The authors exam ine som e recently proposed criteria for determining w hen to
adjust for covariates related to mlsdassification, and show these criteria to be
incorrec t In particular, they show that w hen misdassffication is present, covariate
control can sometimes increase net bias, even when the covariate would have
been a confounder under perfect classification, and even if the covariate is a
determinant of classification. Thus, bias due to misclasstflcation cannot be
adequately dealt with by the methods used for control of confounding. Theexamples presented also show that the "change-in-estimate" criterion for decid-
ing whether to control a covariate can be systematically misleading when mis-
classification is present These results demonstrate that it is necessary to
consider the degree of misdassiflcation when deciding whether to control a
covariate.
biometry; epkJemiologic methods
Most epidemiologic studies are designedto estimate the effect of some exposurefactor (or factors) on the risk of a particulardisease. Despite considerable research, theissue of when adjustment for a covariate isnecessary in this process remains contro-versial. Some recent works (1-3) have ex-plicitly or implicitly put forth recommen-dations regarding adjustment when selec-tion bias or misclassification is present in
the study. Each of these works dealt withsituations in which the covariates weretreated as confounders, i.e., variables forwhich adjustment was necessary to removebias in th e estima tor of effect. Th e pu rposeof this paper is to critically examine somerecent recom me ndations regarding ad just -
Received for publication March 8,1984 and in finalform February 20, 1985.Abbreviation: SMR, standardized morbidity ratio.1
Division of Epidemiology, UCLA School of Pu blicHe alth, Los Angeles, CA 90024.
• Occupational Health Program, Harvard School ofPublic Health, Boston, MA.
' Partially supported by NCI grant RO-CA-16042.The authors thank James Schlesselman and Alex-
ander Walker for their helpful comments.
m ent for covariates related to classification,and to offer some alternative recommen-dations.
Current writings on confounding (1-4)suggest that if no other biases are presentthe following conditions are necessary fora covariate to be a con foun der 1) it m ustbe a predictor of risk among the unexposed;2) it must be a correlate of exposure in thepop ulation serving as the source of subjects;and 3) it should not be an intermediatevariable in the causal pathway und er study.Figure la illustrates these criteria in a pathdiagram.
In case-control stu dies, the preced ing cri-teria can be broadened to allow adjustmentfor certain types of selection bias. Day etal. (1) note that if the covariate is a riskpredictor but not a correlate of exposure in
the source population (figure lb), control-ling it may still reduce bias if the covariateinfluences selection differentially with re-spect to exposure. And M iettinen and Cook(3) note that if the covariate is a correlateof exposure but not a risk predictor (figurelc), controlling it may still reduce bias if
495

8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 2/12
496 GREENLAND AND ROBINS
b) F -
d) F-
f) F-
C C
FIGURE 1. Pa th diagrams illustrating causal structure s in source populations.
the covariate influences selection differen-tially with respect to disease status. Unfor-tunately, other authors have inappro-priately extended these principles to situa-tions in which the covariate is an interme-
diate variable (figure Id) or a consequenceof exposure and disease (figure le) (5). Insuch situations, there may indeed be selec-tion bias due to the covariate, but adjust-ment for the covariate may produce a biaseven m ore severe tha n the original selectionbias (6). Thus, not all forms of selectionbias can be regarded as confounding or beadequately dealt with by covariate control.
Some authors have suggested extensions
of th e above principles to situa tion s involv-ing misclassification of exposure or disease(2, 3). We will argue below that several ofthe extensions t ha t have been proposed areincorrect. In particular, the counterexam-ples we will present will show that adjust-m en t for a deter m ina nt of classification canaggravate bias.
T he exam ples will concern epidemiologic
studies of the effect of an exposure factorF (F = 1, present; F = 0, absent) on risk ofa disease outcome D (D = 1, disease occurs;D = 0, disease does not occur) over a fixedrisk period in a well-defined population.The covariate will be denoted C (C = 1,present; C = 0, ab sen t). Th e effect of F will
be defined in terms of the rate ratio, esti-mated from case-control studies by theodds ratio. The disease will be assumed tobe "rare" over the study period to avoiddistinctions that arise in the general case.Nevertheless, all that follows applies tomore general settings involving commondiseases, multilevel factors, and measuresof association other than the rate ratio andodds ratio.
"Expected values" will be taken to belarge-sample expectations. Critical in whatfollows will be the idea of "net bias," de-fined for present purposes as the differencebetween the true effect parameter and the
expected value of the chosen estimator.(The definition of a confounder is notwell agreed upon in settings in which thetrue effect parameter cannot be unbiasedlyestimated from the observed data on F, C,and D. One might continue to define C tobe a confounder only under the above con-ditions. Instead, in this paper, we will de-fine C to be a confounder if the ne t bias ofthe crude estimator exceeds that of the
adjusted estim ator, regardless of conditions1) and 2) above. As shown below, in theabsence of inform ation on misclassificationrates, it is often impossible to determinefrom the data either the validity of condi-tions 1) and 2) or the relative bias of thecrude and adjusted estimators.)
8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 3/12
CONFOUNDING AND MISCLASSIFICATION 497
C O V A R I A T E S U N R E L A T E D T O
CLASSIFICATION
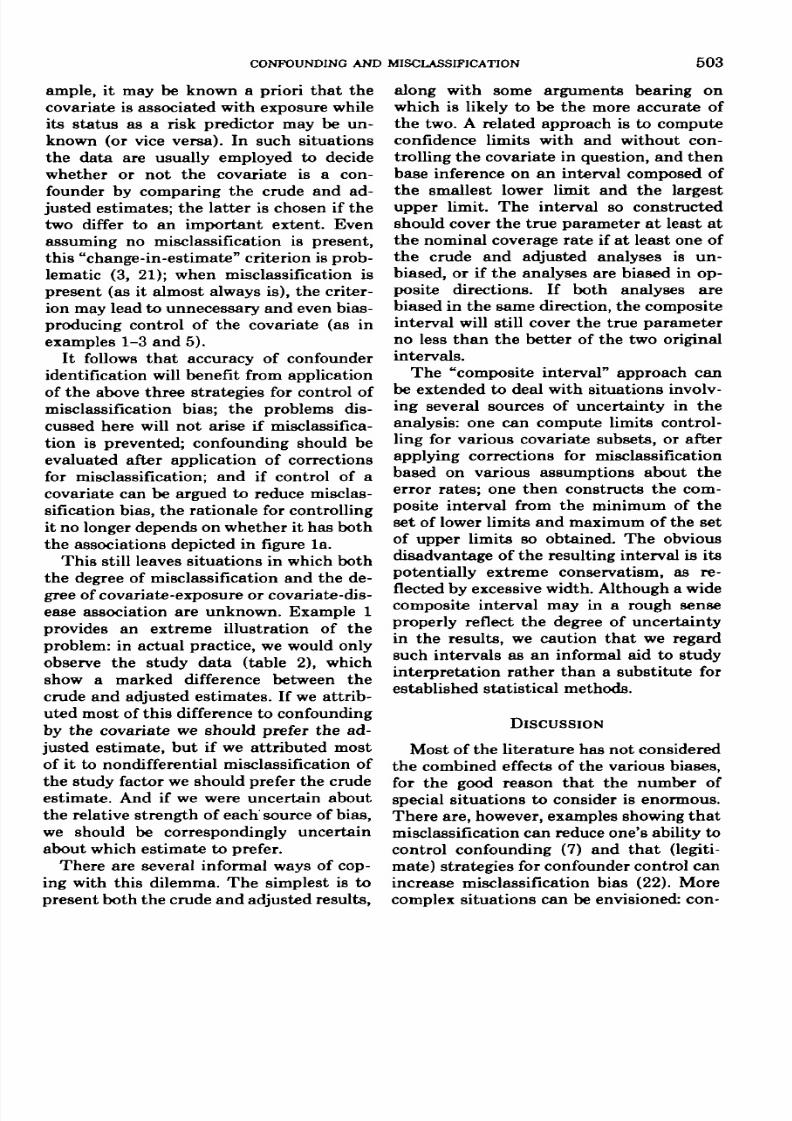
Consider a situation in which the covar-iate is associated with exposure but not a
risk predictor (as in figures lc or If ). It h asbeen suggested that the situation shown infigure If "may lead to genu ine confoundingwhen the variables are measured with er-ror" (2, p. 106) and the following examplewas used to illustrate this assertion.
Example 1
Suppose th at th e underlying source pop-
ulation structure is as in table 1. A case-control study tak ing all cases and an equalnum ber of con trols, bu t nondifferentiallymisclassifying F 10 per cent of the time(i.e., sensitivity and specificity for measure-ment of F equals 0.9 across all levels of Cand D) will have expected data as in table2, where F* = 1 for sub jects classified as
UF
present" and F* = 0 for subjects classifiedas
UF absent." (To illustrate the construc-
tion of table 2, note that the upper lefthand cell of table 2 is 0.9 (90) + 0.1 (1) =
T A B L E 1
Source population structure for examples 1 and 2
Expected no. of
incident cases
Population at
risk
Rate ratio
parameters
C
F-l
90
9,000
= 1
F = 0
1
10,000
100
C - 0
F-l F-0
10 9
1,000 90,000
100
Crude rate ratio parameter, 100.
T A B L E 2
Expected data for example 1 (case-control study of
population in table 1 with sensitivity and specificity of
measure ment of F having constant sensitivity = 0.90
and specificity = 0.90)
CasesControls
Expected oddratio*
f* =
819
C - 1
1 F
9
1010
0 F- -
1010
C -
1
9
0
F*-0
981
Expected crude odds ratio, 23.
F* , measured value of F.
81 when rounded to the n earest whole num-ber.) We can see from table 1 that, in theabsence of other biases, the tru e effect cor-responds to a rate ratio of 100. In contrast,
the expected crude rate ratio estimate fromth e study (table 2) is 23, bu t the expectedadjusted rate ratio estimate is 9, even morebiased.
Contrary to the implication of the quotecited above, it is evident that adjustmentfor the covariate in example 1 dramaticallyincreases the net bias, rather than reducesit. Thus, the covariate is not a genuineconfounder in this situation. The example
also demonstrates the pitfall of using theobserved study data to judge whether con-founding is present: misclassification caneasily distort the apparent degree of con-founding or effect modification by a thirdvariable. This point has been made beforeby one of the present authors (7).
Example 1 turn s out to be an illustrationof a more general feature of nondifferential
misclassification of exposure (proven in theAppendix): if the odds ratios are constantacross strata, the covariate is associatedwith exposure but not classification or dis-ease, and sensitivity and specificity sum tomore than 1.0, then the misclassificationbias in the standardized odds ratio will begreater tha n th at in the crude (unless thereis no association of exposure with disease,in which case neither estimate will be
biased). As discussed in the Appendix, thistheorem extends to cohort studies. Thetheorem also extends to case-control stud-ies of populations in which the disease(rather than exposure) is nondifferentiallymisclassified and t he cova riate is associatedwith disease (instead of exposure). If, how-ever, only one of exposure and disease aremisclassified, the misclassification is non-differential, and the covariate is associatedonly with the correctly classified variable,then both the standardized and crude oddsratios will be equally biased towards thenull (this follows directly from a theoremof Ko rn (8)); furtherm ore, nondifferentialmisclassification of a nonconfounding co-

8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 4/12
498 GREENLAND AND ROBINS
variate will produce no bias in either thestandardized or crude odds ratio.
In example 1, nondifferen tial misclassi-fication of the exposure generated the spu-
rious appearance of confounding by a co-variate (in the sense that the crude andadjusted values differ), and nondifferentialmisclassification of the disease can do so aswell. As the following example shows, dif-ferential misclassification of a noncon-founding covariate can also generate thespurious appearance of confounding.
Example 2
Consider again the case-control study ofthe source population described in example1 and table 1, but with C rather than Fmeasured with error. Specifically, supposethe presence of C is detected with perfectspecificity but with a sensitivity of 0.98among cases and 0.90 among noncases (asmight occur, for example, if the covariaterepresented an event for which the caseshad better recall). The expected data wouldthen be as in table 3. The expected crudeodds ratio differs from the expected stan-dardized morbidity ratio (SMR) estimate(9, 10) and the expected Mantel-Haenszelestimate (2, 4), yet it is the crude (ratherthan any adjusted value) that equals thecorrect population rate ratio. This occursfor two reasons: first, since F and D are notmisclassified, th e expected crude odds ra tioequals the crude rate ratio parameters, andsecond, the crude parameter equals the
TABLE 3
Expected data for example 2 (case-txntrol study of
population in table 1 with differential misclassification
of C: sensitivity = 0.98 among cases and 0.90 among
controls, specificity = 1.00 in both groups)
CasesControls
Expected oddsratios
C -
F-l
888
99
1
F = 0
19
C * -
F = l
122
61
• 0
F - 0
991
stratum-specific values. (The misclassifi-cation has also generated a spurious ap-pearance of odds ratio heterogeneity.)
PR E DIC T OR S OF E XPOSUR E
CLASSIFICATION
It has been suggested th at in case-controlstudies "study procedures that bear on theaccuracy of information on ex po su re ... areconfounders if they are distributed differ-ently between the index (case) and refer-ence [control] series" (3, p. 598). The fol-lowing example shows that this claim isfalse as a general principle.
Example 3
Suppose the correctly classified expecteddata in a case-control study are as given intable 4, and that these numbers perfectlyreflect the magnitude of the effect of thestudy factor on incidence. Let C = 1 indi-cate that the exposure information was ob-tained by direct interview with subject, andC = 0 that the subject had died before aninterview could be performed (so informa-tion was obtained from next-of-kin). Notethat a higher proportion of controls weredirectly interviewed. Suppose that inter-views of next-of-kin of deceased subjects(C = 0) always had a sensitivity (for expo-sure) of 0.75 and a specificity of 0.85, whiledirect interviews of subjects (C = 1) alwayshad a s ensitivity of 0.90 and a specificity of
0.95. The expected misclassified data wouldthen be as in table 5; we see that the crudeodds ratio is 1.8, closer to the correct valueof 2 than any of the adjusted or stratum-specific values. Thus, adjustment for the
TABLE 4
Expected correctly classified data for example 3.
(C •= 1 if subject directly interviewed,
C-0 otherwise.)
Expected crude odds ratio, 100.Expected SMR estimate (9,10), 92 .Expected Mantel-Haenszel odds ratio (2, 4, 18), 73.C*, measured value of C.
CasesControls
Correct oddsratios
C - 1
F-*l F-0
20 80100 800
2.00
C - 0
F - l F = 0
120 48040 320
2.00
Correct crude odds ratio, 2.00.

8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 5/12
CONFOUNDING AND MISCLASSIFICATION 499
TA B LE 5
Expected data under misclassification, example 3(case-control study of subjects in table 4, with C a
determinant of exposure classification: sensitivity =
0.90 and specificity = 0.95 when C = 1, sensitivity =
0.75 and specificity = 0.85 when C = 0)
CasesControls
Expected oddsratios
C - l
F*-l F* = 0
22 78130 770
1.67
F* =
162
78
C - 0
1 F* = 0
438282
1.34
Expected crude odds ratio, 1.80.Expected SM R estimate, 1.37.Expected Mantel-Haenszel odds ratio, 1.39.F*, measured value of F.
Expected crude odds ratio under matching onC, 1.37.
source of information is unnecessary in th isexample, and in fact harmful in that itincreases net bias.
Suppose in the above example one hadmatched the controls to cases on source ofinformation (C), so the same proportion ofcontrols as cases (14 per cent) had been
directly interviewed. The expected adjustedodds ratios would then be about the sameas before, but the expected crude odds ratiowould now be only 1.4. Thus, matching onsource of information would also be harm-ful in this example.
Note that the covariate in example 3 wasnot actually related to the exposure withineither the case series or the control series
(table 4). Thus, a covariate need not berelated to the exposure in order to spu-riously mimic a confounder through its ef-fects on exposure classification. Example 1illustrates that if a covariate is related toexposure, it need not be related to diseaseor classification in order to spuriouslymimic a confounder.
Exam ple 3 illustrates a failure of the oft-repeated validity criterion of comparability
of measurement (11, 12): in the example,focusing the analysis within groupingsbased on measurement comparability led toless valid results than simple pooling ofsubjects without regard to measurementcomparability. Even restriction of the anal-ysis to the subjects with the most accurate
measurem ents (stratum C = 1) producedless valid results than a crude analysis ofall subjects. Nevertheless, this comparabil-ity criterion may have its origin in examples
such as the following, which parallels ex-ample 3 yet illustrates a general situationin which adjustment for a determinant ofexposure classification reduces bias.
Example 4
Suppose the correctly classified expecteddata in a case-control study are as given intable 6, and that these numbers perfectlyreflect the magnitude of the effect of the
study factor on incidence (note in particu-lar tha t the re is no effect). L et C be definedas in example 3, and the sensitivities andspecificities within levels of C be as in ex-ample 3. The expected misclassified datawould then be as in table 7. We see thatthe crude odds ratio is biased away fromthe correct value of 1.00, whereas the str at-ified odds ratios are not. Thus, in this ex-ample, adjustment for the source of infor-mation (indicated by C) is essential forvalidity.
TABLE 6
Expected correctly classified data for example 4
Expected no. ofincident cases
Population at risk
Correct oddsratios
C
F - 1
10
100
- 1
F-0
80
800
1.00
C - 0
F-1 F-0
60 480
40 320
1.00
Correct crude odds ratio, 1.00.
TABLE 7
Expected data under misclassification, example 4
(case-control study of subjects in table 6, with C a
determinant of exposure classification: sam e
classification rates as example 3)
CasesControls
Expected oddsratios
I
F*-
13130
C-l1 F'-O
77770
1.00
f -
11778
C = 01 F*-0
423282
1.00
Expected crude odds ratio, 1.32.F* , measured value of F.

8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 6/12
500 GREENLAND AND ROBINS
The effect of covariate adjustment on netbias in example 4 was opposite to that inexample 3. Consequently, one cannot stateth a t in general a predictor of exposure clas-sification should or should not be treatedas a confounder. Nevertheless, example 4illustrates a general principle of hypothesistesting: suppose that no other biases arepresent, and within levels of the covariatemisclassification of exposure is nondiffer-entia l an d there is no true exposure-diseaseassociation; then the true large-sample al-pha level (type I error rate) of any of theusual stratified tests of association (e.g.,
Mantel-Haenszel (4)) will not exceed theirnominal alpha-level (8). And (except forsome special cases of unusual structure) ifthe covariate is both a predictor of the(nondifferential) exposure classification er-rors and associated with disease, stratifi-cation on the covariate will be necessary toproduce a test of size within the nominalalpha -level (this is because ex posure will bedifferentially misclassified within the crude
table). "Comparability of measurement"therefore remains a valid criterion for hy-pothesis testing. Although forcing "com-parab ility of measu remen t" also guaranteesthat the measurement bias in point esti-mation will be towards the null, example 3demonstrates that the net bias can some-times be greatly increased by such action.
PREDICTORS O F DIAGNOSTIC ERROR
Misclassification of disease status is of-ten referred to as misdiagnosis or diagnos-tic error. It has been stated that confoun-ders "are predictors (determinants) of di-agnosing the illness—by being either riskindicato rs or determina nts of diagnostic er-rors—in the type of setting represented bythe study" (3, p. 594). The following ex-ample shows that (contrary to the preced-
ing quote) a determ inant of diagnostic errormay be associated with the stud y factor an dyet no t be a true confounder.
Example 5
Sup pose our source population is actuallyas in table 8 (showing a true effect param-
eter of rate ratio = 2.00 and an associationof C with F), and C is a determinant ofdiagnostic errors as shown in the table: inthe population w ith C pres ent, d iagnosis ofdisease takes place with a 95 per cent sen-sitivity and a 0.08 per cent false positiverate over the study period, while in thepopulation with C absent, diagnosis of dis-ease take s place with 90 per cent sensitivityand 0.06 per cent false positive rate. If wedo a follow-up study of the entire popula-tion and expend no additional case-findingor case-screening efforts, our expected d atawill be as in table 9: the expected crude rate
ratio estimate is 1.67, while the expectedadjusted estimates are around 1.56. Thus,adjustment for the determinant of diagnos-tic error is unnecessary in this example,and in fact harmful in that it increases netbias. As in the last two examples, the ad-justed estimators are more biased than thecrude, so that, despite its association withexposure and its influence on diagnosticerrors, the covariate is not a true con-
founder. Note also that adjustment for thecovariate would produce bias in a case-control study of this population.
The belief that pure determinants of di-agnosis should be treated as confoundersmay have its origin in exam ples such as th efollowing, which parallels example 5 yetillustrates a general situation in which ad-justment for a determinant of diagnostic
error reduces bias.
Example 6
Suppose the source population structurewas as in table 10, with C a determinant ofdiagnostic errors as shown: F and C havethe same association as in example 5, andthe sensitivity and false positive rate ofdisease diagnosis is also the same as in
example 5. Th e only difference is that , un -like in example 5, F has no effect. If we doa follow-up study of the entire populationand take as cases all and only those diag-nosed as such, our expected data will be asin table 11. We see th at the crude rate ratiois biased away from the correct value of

8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 7/12
CONFOUNDING AND MISCLASSIFICATION 5 0 1
T A B L E 8
Source population structure for examp le 5
Expected no. of
Diagnosed cases
Undiagnosed cases
Expected no. of noncases diagnosed
as cases
Population at risk
True rate ratio parameters (based on
true cases only)
F - 1
76
4
32
40,000
C o l
F = 0
19
1
16
20,000
2.00
F-1
32
8
12
20,000
C - 0
F-0
32
8
24
40,000
2.00
Apparent cases
Population at risk
Expected rate
ratio estimates
C
F = 1
10 8
40,000
- 1
F-0
3520,000
1.54
C
F = 1
4420,000
- 0
F-0
5640,000
1.57
Crude rate ratio parameter (based on true case s onl y), 2.00.
TABLE 9 Th e effect of covariate adjustm ent on ne tExpected data for exam ple 5 (follow-up study of bias in example 6 was oppos i te to that in
population in table 8 using aUdiagnos& l persons as e x a m p l e g . There fo re , One can no t s t a te th a tcases, C a determinant of disease diagnosis) , .. . . .
in general a predictor of diagnostic errors
should or should not be treated as a con-
founder. Nevertheless, example 6 illus-trate s a general principle parallel to the one
given after example 4: suppose that noother biases are present, and within covar-
Expected crude rate ratio ertimate, i.67. ia te leve ls th e re is n o t n i e exp osu re -d is easeExpected SMR estimate, 1.66. associa t ion and d iagnos t ic er rors are non-Expected Mantei-Haenszei rate ratio ertimat., 1.56. dif ferent ia l ; then the t rue large-sample a l -
ph a level of an y of th e usu al s t ra t i f ied tes t s
of association will not exceed their nominal
1.00 (albeit slightly), whereas the stratified alpha-level (8). And (except for some spe-rate ratios are not. Th us , in this example, cial cases of unusua l structu re) if the co-adjustment for the diagnostic predictor was variate is both a predictor of the (nondif-
app ropriate for validity. ferential) diagnostic erro rs an d associated
T A B L E 10
Source population structure for example 6
Expected no. of
Diagnosed cases
Undiagnosed cases
Expected no. of noncases
diagnosed as cases
Population at risk
True rate ratio parameters
(based on true cases only)
C - 1
F-1
38
2
32
40,000
1.00
F-0
19
1
16
20,000
F-1
18
2
12
20,000
C - 0
F-0
36
4
24
40,000
1.00
Crude rate ratio parameter (based on true cases only), 1.00.

8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 8/12
502 GREENLAND A ND ROBINS
TA B LE 11
Expected data for example 6 (follow-up study for
population in table 10 using all diagnosed persons as
cases, C a determinant of disease diagnosis)
Apparent casesPopulation at risk
Expected rateratio estimate*
C
F- 1
7040,000
= 1
F-0
3620,000
1.00
C
F - 1
3020,000
= 0
F - 0
6040,000
1.00
Expected crude rate ratio estimate, 1.06.
with the exposure, stratification on the co-
variate will be necessary to produce a testof size within the nominal alpha-level
(again, because the diagnostic errors will bedifferential within the crude table). Predic-tors of diagnostic accuracy may thus be
treated as confounders in hypothesis test-ing. But example 5 demonstrates that con-
trol of such predictors can sometimesgreatly increase net bias in point estima-tion.
IMPLICATIONS FOR THE CONTROL OF
MISCLASSIFICATION BIAS
The above examples show that, despiteconjectures to the contrary, predictors of
classification or diagnosis cannot be ade-
quately dealt with in the same frameworkas predictors of risk. In particular, a co-
variate can be a determinant of exposureclassification or disease diagnosis but it
may nevertheless be detrimental to adjustfor the covariate. This appears to run
counter to usual epidemiologic intuitions(cf., 11, 12), and yet the above examplesought to be sufficient to rule out a simpleparallelism between confounder controland misclassification control. Furthermore,the misclassification rates employed aboveare not numerically extreme, making it
doubtful that the hoped-for parallelismmight hold approximately: for example,Copeland et al. (13, table 2) reviewed re-
ported sensitivities and specificities ofseven measurements and found four in-
stances in which sensitivity was below 60
per cent or specificity was below 75 per
cent. More recent studies have found under80 per cent agreement between interview
responses and medical records for certaintypes of drug history items (14-16) (low
agreement necessarily implies high errorrates for one or both of the sources); differ-ential recall was indicated in some in-
stances (16). Even when the error ratesappear "low," errors can produce sizeabledistortions if the presence or absence of theexposure or disease is "rare" (as in example4 or the real data reported by Schulz et al.
(17)).This leaves three strategies for the con-
trol of misclassification bias: 1) preventionof misclassification through improved
measurement m ethods; 2) algebraic correc-tion for misclassification (which requires a
source of error-rate estimates, such as a
validation substudy); and 3) control of
those covariates for which con trol could be
argued to reduce misclassification bias in
the specific analysis being performed. The
first two strategies have been extensivelydiscussed in a number of recent publica-tions (e.g., 13, 17-20), while the third ap-
pears to have been either ignored or mis-perceived. With regard to the third strat-egy, a general principle was illustrated by
examples 3-6: if misclassification is non-
differential within levels of a covariate but
varies across levels of the covariate, then,in the absence of other sources of bias,control for the covariate will in generalimprove the validity of the test of associa-tion of factor and disease; nevertheless,
control of the covariate may in some in-
stances increase the net bias in estimation(cf., example 3, 5). In this case, the soleadvantage of the adjusted point estimate is
tha t the direction of its misclassificationbias is known a priori (i.e., it is towards the
null); if the misclassification is differential,however, this advantage is lost.
IMPLICATIONS FOR IDENTIFICATION OF
CONFOUNDING
Th e above examples also show how studydata can be systematically deceptive as to
whether or not a covariate is a confounder(in the sense of requiring control). For ex-
8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 9/12
C O N F O U N D I N G A N D M I S C L A S S I F I C A T I O N 503
ample, it may be known a priori that thecovariate is associated with exposure whileits status as a risk predictor may be un-known (or vice versa). In such situations
the data are usually employed to decidewhether or not the covariate is a con-founder by comparing the crude and ad-justed estimates; the latter is chosen if thetwo differ to an important extent. Evenassuming no misclassification is present,this "change-in-estimate" criterion is prob-lematic (3, 21); when misclassification ispresent (as it almost always is), the criter-ion may lead to unnecessary and even bias-
producing control of the covariate (as inexamples 1-3 and 5).
It follows that accuracy of confounderidentification will benefit from applicationof the above three strategies for control ofmisclassification bias; the problems dis-cussed here will not arise if misclassifica-tion is prevented; confounding should beevaluated after application of corrections
for misclassification; and if control of acovariate can be argued to reduce misclas-sification bias, the rationa le for con trollingit no longer depends on whether it has boththe associations depicted in figure la.
This still leaves situations in which boththe degree of misclassification and the de-gree of covariate-exposu re or co variate-dis-ease association are unknown. Example 1provides an extreme illustration of theproblem: in actual practice, we would onlyobserve the study data (table 2), whichshow a marked difference between thecrude and adjusted estimates. If we attrib-uted m ost of this difference to confoundingby the covariate we should prefer the ad-justed estimate, but if we attributed mostof it to nondifferential misclassification ofthe study factor we should prefer the crude
estimate. And if we were uncertain aboutthe relative stre ng th of each source of bias,we should be correspondingly uncertainabout which estimate to prefer.
There are several informal ways of cop-ing with this dilemma. The simplest is topresent both th e crude and adjusted results,
along with some arguments bearing onwhich is likely to be the more accurate ofthe two. A related approach is to computeconfidence limits with and without con-
trolling the cov ariate in question, and the nbase inference on an interval composed ofthe smallest lower limit and the largestupper limit. The interval so constructedshould cover the true parameter at least atthe nominal coverage rate if at least one ofthe crude and adjusted analyses is un-biased, or if the analyses are biased in op-posite directions. If both analyses arebiased in the same direction, the composite
interval will still cover the true parameterno less than the better of the two originalintervals.
The "composite interval" approach canbe extended to deal with situations involv-ing several sources of uncertainty in theanalysis: one can compute limits control-ling for various covariate subsets, or afterapplying corrections for misclassificationbased on various assumptions about theerror rates; one then constructs the com-posite interval from the minimum of theset of lower limits and maximum of the setof upper limits so obtained. The obviousdisadvantage of the resulting interval is itspotentially extreme conservatism, as re-flected by excessive w idth. Although a widecomposite interval may in a rough senseproperly reflect the degree of uncertainty
in the results, we caution that we regardsuch intervals as an informal aid to studyinterpretation rather than a substitute forestablished statistical methods.
DISC USSION
M ost of the literature ha s not consideredthe combined effects of the various biases,for the good reason that the number of
special situations to consider is enormous.The re a re, however, examples showing t h atmisclassification can reduce on e's ability tocontrol confounding (7) and that (legiti-mate) strategies for confounder control canincrease misclassification bias (22). Morecomplex situations can be envisioned: con-

8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 10/12
504 GREENLAND AND ROBINS
sider, for example, a matched-pair case-con trol study in which a confounder is usedas a matching factor but is routinely mis-classified during selection, resulting in theselection of mismatched con trols. As a con-sequence, either the study results will re-main confounded by the confounder or, ifth e confounder is correctly measured in th eanalysis, many of the subjects will be leftunmatched; loss of validity or efficiency isthus inevitable in this situation.
In most epidemiologic studies, all sourcesof bias will variously cancel and interact ina m an ne r too complex for accurate analysis.
It is perhaps for this reason that someauthors criticize overemphasis of formalstatistical results in drawing and present-ing conclusions from epidemiologic data.But granting that formal methods do notadequately address these problem s, numer-ical reasoning can still be emp loyed to eval-ua te th e likely im pact of various sources ofbiases on the study data at hand, and tocheck on the validity of any general rec-
ommendations that appear in the methodo-logic literature .
We have seen that misclassification bias(including biases arising from diagnosticerrors) cannot in general be controlled bythe same basic methods used to controlconfounding or some forms of selectionbias. If we have accurate estimates of theclassification probabilities, corrections for
misclassification are possible (13, 18-20,22). Nevertheless, the true classificationrates are virtually never known, and esti-mates of them will usually be subject toconsiderable error so that the "corrected"estimates will not be fully corrected formisclassification bias. It is also known th a trelatively modest degrees of misclassifica-tion can produce large amounts of bias (7,13 , 22). These observations taken together
indicate that , similarly to m any othe r prob-lems, prevention of misclassification bias issuperior to any analytic cure.
The contingency-table results presentedhere and elsewhere (7, 8, 13, 18, 22) haveimmediate consequences for binary regres-
sion methods, such as logistic regression.Most importantly, we note that misclassi-fication of a regressor can bias the coeffi-cient estim ates for othe r regressors, even ifthe misc lassification is nondifferen tial (cf.,example 1) or even if the t ru e coefficient ofthe misclassified regressor is zero (cf., ex-ample 2); misclassification of a regressorcan also bias interaction estimates (cf., ex-amples 2 and 3, and reference 7). Theseobservations poin t out the necessity of con-sidering the measurement quality of allvariables entered in a model, even whenonly certain effects within the model are
the object of study. Similar conclusionshave been reached by Kupper (23) in thecase of ordinary regression. Exam ples 3 and5 also imply that the addition of "dataquality" indicators to models (such as avariable indicating whether data were ob-tained from the subject or from a surrogate(24)) can sometimes increase bias in someor all of the risk factor coefficients.
R E F E R E N C E S
1. Day NE, Byar DP, Green SB. Overadjustment in
case-control studies. Am J Epidemiol 1980;
112:696-706.
2. Breslow NE, Day NE. Statistical methods in can-
cer research. Volume 1. The analysis of case-
control studies. IARC Scientific Publication No.
32 . Lyon: International Agency for Research on
Cancer, 1980.
3 . Miettinen OS, Cook EF. Confounding: essence
and detection. Am J Epidemiol 1981;114:593-603.
4. Schlesselman JJ. Case-control studies: design,
conduct, analysis. New York: Oxford UniversityPress, 1982.
5. Horwitz RI, Feinstein AR. Alternative analytic
methods for case-control studies of estrogen and
endometrial cancer. N Engl J Med 1978;299:
1980-94.
6. Greenland S, Neu tra RR. An analy sis of detectio n
bias and proposed corrections in the study of
estrogens and endometrial cancer. J Chronic Dis
1981;34:433-8.
7. Greenland S. T he effect of misclass ification in the
presence of covariates. Am J Epidemiol 1980;
112:564-9.
8. Korn EL. Hierarchical log-linear mode ls no t pre-served by classification error. J Am Stat Assoc
1981;76:110-13.
9. Miettinen OS. Standardization of risk ratios. Am
J Epidemiol 1972^6:383-8.
10. Greenland S. Interpretation and estimation of
summary ratios under heterogeneity. Stat Med
1982;l:217-27.
8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 11/12
CONFOUNDING AND MISCLASSIFICATION 505
11. MacMahon B, Pugh TF. Epidemiology: principles 18. Kleinbaum DG, Kupper LL, Morgenstern H. Ep-and methods. Boston: Little, Brown, 1970. idemiologic research: principles and quantitative
12. Miettinen OS. The "case-control" study: valid se- methods. Belmont, CA: Lifetime Learning, 1982.lection of subjects. J Chronic Dis 1985 (in press). 19- Fleiss JL. Statistical methods for rates and pro-
13. Copeland KT, Checkoway H, McMichael AJ, et portions. 2nd ed. New York: John Wiley and Sons,
aL Bias due to misclassification in the estimation 1981.of relative risk. Am J Epidemiol 1977;105:488-95. w- Greenland S, Kleinbaum DG. Correcting for mis-14. Brody DS. An analysis of patient recall of their classification in two-way tables and matched-pair
past therapeutic regimens. J Chronic Dis O1 Btuies. IntJ Epidemiol 1983;12^3-7.1980-33
-57-63 Robins J, Morgenstern H. Confounding and prior
15. Paganini-HillA, Ross RK. Reliability of drug n&Ox**'{AbStmCt)
- **J E
Pidemio1 1 9 8 3 ;
£ * f " ^ a o ^Tn***infonnation
- ^J
22. Greenland S. The effect of misclassification inEpidemiol 1982;116:114-22 matched-pair case-control studies. Am J Epide-
16. Rosenberg MJ, Layde PM, Ory HW, et al. Agree- ^ j i982;116:402-6.ment between women's histories of oral contra- 23. Kupper LL. Effects of the use of unreliable sur-ceptive use and physician records. Int J Epidemiol I0geLte variables on the validity of epidemiologic1983;12:84-7. research studies. Am J Epidemiol 1984;12(h643-8.
17. Schulz KF, Cates W, Grimes DA, et aL Reducing 24. Pickle LW, Greene MH, Ziegler RG, et al. Colo-
classification errors in cohort studies. Stat Med rectal cancer in rural Nebraska. Cancer Res1983;2:25-31. 1984;44:363-9.
A P P E N D I X
Proof of theorem corresponding to example 1
Suppose a covariate is associated with exposure but not associated with classification or the disease, theexposure is nondifferentially misclassified with sensitivity Q and specificity P (and P + Q > 1), and the truestratum-specific odds ratio R for the exposure-disease association is constant across the covariate levels. Thenthe misclassification bias in the standardized morbidity ratio (SMR) estimate ("internally" standardized oddsratio, weighting the odds ratios based on the covariate distribution in the exposed controls) (9, 10) will begreater than the misclassification bias in the crude odds ratio (unless R •» 1, in which case neither are biased).
In particular, if SMR and Rc represent the large-sample expectations of the standardized and crude estimators,we have that R < 1 impliesR<R C< SMR< 1 and R > 1 implies ft > ft, > SMR > 1.
Proof: For statum t of the covariate letXi •=» expected true number of unexposed controls,T( = expected exposure odds among controls (T, 'A Tj for some i, j)
S = expected case-control ratio among the unexposed (S is constant across strata since the covariate is not arisk factor).
Then TtX( = expected number of exposed controls,SXt " expected number of unexposed cases, andRSTiXj = expected number of exposed cases.
Also, the apparent numbers expected after misclassification will beAt = SXAQRTi + (1 — P)) = apparent number of exposed cases,Bt = SXAP + (1 — Q)RTt) •• apparent number of unexposed cases,Cj = XAQTj + (1 - P)) = apparent number of exposed controls, andDi = XAP + (1 — Q)Ti) •= apparent number of unexposed controls.
We will prove the theorem only for the case R > 1, T\ < To, as proofs for the other three cases follow bysymmetrical arguments.
For the binary case (i = 0 or 1 only), proof proceeds by the following lemmas:
Lemma 1. If R > 1 and 7\ < To, then BiD0 < BoDx.
Proof: By direct algebra, B^Do - BoD, - P(l - Q)(l - R)S(T0 -
1 - R is the only negative term in the right hand product, hence both sides of the equation are negative.
Lemma 2. If T, < To and P + Q > 1, then CtD0 < CoDi.
Proof: By direct algebra, CJ)l - C,D0 = (P + Q - 1)(TO - T,)X,.Xo.
All the terms in the right hand product are positive, hence both sides of the equation are positive.Lemma 3. If R > 1, 7\ < To, and C,D0 < CoDi, then SMR < fl,.
Proof: By Lemma 1 B,D0 - B<lD l < 0.Hence

8/2/2019 Confounding and Misclassification
http://slidepdf.com/reader/full/confounding-and-misclassification 12/12
5 0 6 GREENLAND AND ROBINS
C1D0(BlDB - BoD,) > CoD 1(B 1D 0 -
yielding
then
BjdDo7
+ BoCoD,1
> B,CoDiDc, +
Adding (B1C1 + Bt/Co)DiDo to both sides of the last inequality and factoring, we obtain
(fl,C,A> + BcCoDtHDt + D o) > (B, + flo)(C, + Co)Z),A,,
then
B . d / D , + BcCo/Do > (Bi + Bo)(C, + C)/^ + A,).
Dividing both sides of the last inequality into Ai + Ac, yields
SM R B<A/A>) (Bi + Bo)(C, + Co)
It is well known (e.g., see references 12, 13, and 18) tha t (within s tra ta) nondifferential misclassificationproduces bias towards the null, hence ft > SMR > 1; unrelatedness of the covariate to classification impliesthat the misclassification is also nondifferential in the crude table and hence ft > fle. The theorem now followsfor binary covariates from Lemmas 1-3. Extension to the case of a covariate with K levels follows bymath ematical induction: Suppose the theorem holds for K — 1 levels. Let SMR and ft ̂be the expected internallystandardized and crude odds ratios obtained from all K covariate st rata, SMR* and ft«* the correspondingexpected values obtained from the first K - 1 strata only, and let S MR . be the standardized odds ratio obtainedby collapsing the first K — 1 levels of the covariate before adjustme nt (Le., coding the co variate as "level K ornot-K"). Finally, let A*, B*, C*, and D* be the sum of the corresponding cells in the first K - 1 strata, and
W* = ]
Since SMR* = A'/W* < A*D*/B*C = ft/, we have B*C*/D* < W*, hence
SMR - WAI B Z D K < * - c v £ t - '" = SMR"
Th e binary case yields ftc > SMR,., hence i t > S MR . As before, we have R> R* and SMR > 1 as well, provingthe theorem.
Using argumen ts symm etrical to those given above, the theorem extends to the case in which the unexposedserve as the source of standardization weights (i.e., the "externally" standardized odds ratio), as well as anyaverage of the exposed and unexposed weightings (such as weighting based on the combined distribution). Thetheorem also extends to cohort studies by letting ft be the risk ratio, S the incidence in the unexposed, SMRthe usual cohort standardized morbidity ratio, and X, T, C, an d D refer to quantities in the total cohort (ra thertha n the c ontrols). Finally, the theorem extends to case-control studies of populations with nondifferentialmisclassification of disease by letting Q an d P refer to th e disease sensitivity and specificity, and mumming th atthe covariate is unassociated with exposure (instead of disease) and that no refinement of diagnosis is made forthe study. We note, however, that the assumption of a constant odds ratio (in case-control studies) or risk ratio(in cohort studies) is necessary for the above results: examples show that under heterogeneity the misclassifi-cation bias in the crude ratio can sometimes exceed that in the standardized ratio. Such an example can beconstructed by modifying example 1 (tables 1 and 2) so tha t th e true numb er of cases at F •=• C •» 1 ia 1.