confocal application in practice no relevant thanks to ... · confocal application in practice...
TRANSCRIPT

7/18/2018
1
Confocal Application in Practice
Everyday (CAPE) AAD F023: Imaging in Chicago 7/28/2018
Jane M. Grant-Kels, MD
Founding Chair Emeritus Department of Dermatology
Professor of Dermatology, Pathology, & Pediatrics
Director of Cutaneous Oncology Center & Melanoma Program
Univ of CT
Health Ctr [email protected]
Dermpath Lab
No Relevant
Conflict of Interest
Thanks to
Harold
Rabinovitz, MD &
Margaret
Oliviero, NP Confocalist
• Skin cancer epidemic
– Patients do not consider biopsies trivial!
• New available technology to help dx skin
cancers in vivo & reduce unnecessary bx’s
Why this is important? From: Analysis of Trends in US Melanoma Incidence and Mortality
Glazer, et al. Analysis of Trends in US Melanoma Incidence and Mortality. JAMA
Dermatol. 2017;153(2):225-226
Lifetime Risk of Developing Invasive MM in US
Changes in
annual lifetime
risk of
developing
invasive MM in
US: 1930 to
2016
Glazer, et al. Analysis of Trends in US Melanoma Incidence and Mortality
JAMA Dermatol. 2017;153(2):225-226.
US Annual Deaths From Melanoma
Est’d # of
annual
deaths from
MM in US:
2009 to
2016
Thin Melanoma Mortality • Greatest # of deaths from MM 1992-2013
from T1 MMs
• Prognosis (risk for death w/in 10 yrs): worse for
0.01-0.25mm thick MMs than from 0.26-0.50mm
thick!(not explained by ulceration)
• Prognosis worsened for MM > 0.51mm deep
• EARLY DETECTION (in situ) IS IMPORTANT! Landow, et al. Mortality burden & prognosis of thin melanomas overall & by
subcategory of thickness, SEER registry data, 1993-2013. JAAD 2017;76:258-
263.

7/18/2018
2
Skin Cancer
Deaths USA
• BCC: 4.3 million
cases/yr 3,000
deaths
• SCC: > 1 million
cases/yr 15,000
deaths https://www.cancer.org/cancer/basal-and-
squamous-cell-skin-cancer/about/what-is-
basal-and-squamous-cell.html
Devices currently available to
enhance clinical dx of melanoma • Full body photography
• Dermoscopy - NNT (# pig lesions bx’d to dx MM):
184.3 Carli, et al. Br J Dermatol 2004;150:687-92.
- Skin Ca Ctr using dermoscopy:
76,783 nevi excised to dx 9,910 MMs Argenziano, et al. JAAD 2012;67:54-9.
- RCM
What is confocal microscopy? Confocal microscope is a high
resolution, non-invasive imaging
device Visualization on a cellular level
comparable to histopathology:
• Epidermis
• Dermo-epidermal junction
• Dermis RCM in Dermatology: Fundamentals and Clinical Application. Editor: S.
Gonzalez. 2011
Stratum corneum
Stratum granulosum
Stratum spinosum
Dermoepidermal junction
Papillary dermis
Reticular dermis
Biopsy is performed
Histopathology Skin is sectioned in a
vertical plane: allows for
evaluation <2% of lesion
Histopathology

7/18/2018
3
Horizontal sectioning:
optical images with a field
of view up to 8X8 mm
RCM
More of the lesion is able to be
evaluated!
ZERO adverse events reported
How does RCM Work?
RCM uses a diode
laser (830nm)
• Penetrates into the
skin illuminating a
tiny point inside the
tissue.
Technical Principles of RCM
Detector Pinhole
Laser
• Reflected light
then passes
through a pinhole.
• Light collected by
the detector is
converted to pixels
to form an image.
Technical Principles of RCM
Detector Pinhole
Laser
• The image is
displayed on a
computer monitor
in real-time
• Relies on inherent diff refractive index of structures: melanocytes, keratinocytes… Psaty, Halpern. Clinics in Dermatol 2009;27:35
• Max depth of imaging 200-300 um usually @ level of papillary dermis
Superficial Dermis
Dermal-Epidermal
Junction
Stratum Corneum
(surface)

7/18/2018
4
RCM Mosaic • Individual
500μm×500μm images
stitched together like a
quilt to form a large field-
of-view
• Images captured in a
single, horizontal plane
• Mosaics can be up to
8 mm x 8 mm square
• Multiple mosaics are
captured at diff levels in
the skin
Horizontal section
CONFOCAL HISTOLOGY In-Vivo
Confocal vs.
H&E
Horizontal
sections
Rajadhyaksha M. JID 1999
Melanin back scattered the light = bright cells
Keratinocytes:
10 to 30µm bright
polygonal
structures w/ dark
outlines
Stratum Corneum 15-20 µm below skin
surface: Keratinocytes
25 - 35µm in diameter w/
bright, granular cytoplasm
& dark oval nuclei
Honeycombed pattern
Stratum Granulosum
20-100 µm below stratum
corneum: Honeycombed
pattern c/o 15 - 25µm cells
w/ bright cytoplasm & dark oval-round nuclei
Stratum Spinosum 50-100 µm below stratum
corneum (location
depends on epid
thickness):
Suprabasalar
Layer
Single layer of refractive
cells corresponds to
horizontal sectioning @
suprapapillary plates
7/18/2018
5
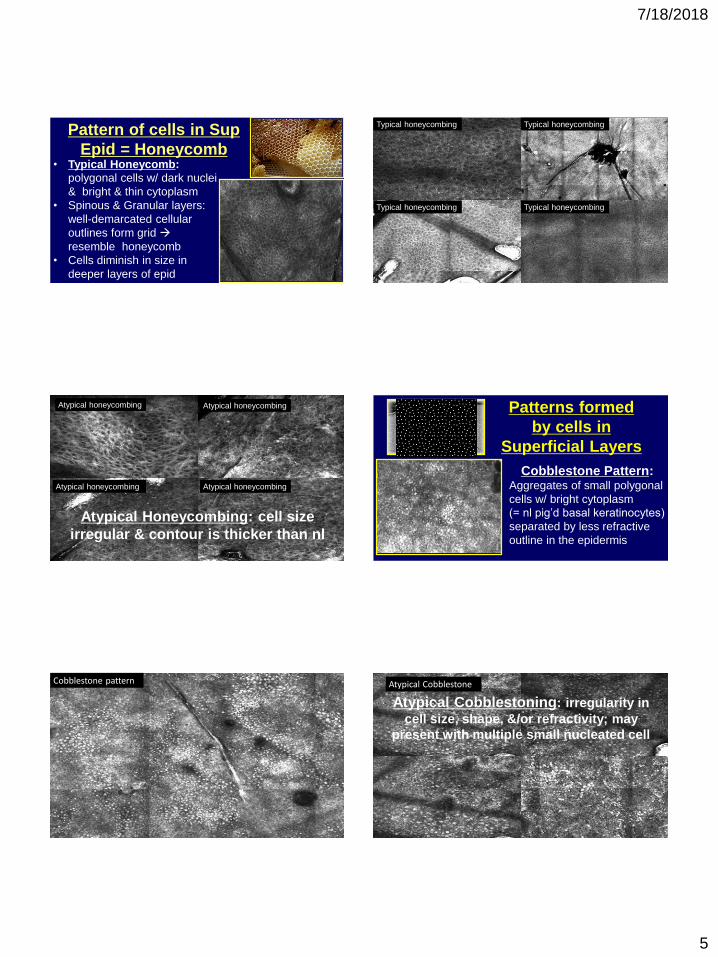
• Typical Honeycomb:
polygonal cells w/ dark nuclei
& bright & thin cytoplasm
• Spinous & Granular layers:
well-demarcated cellular
outlines form grid
resemble honeycomb
• Cells diminish in size in
deeper layers of epid
Pattern of cells in Sup
Epid = Honeycomb
Typical honeycombing Typical honeycombing
Typical honeycombing Typical honeycombing
Atypical honeycombing
Atypical honeycombing Atypical honeycombing
Atypical honeycombing
Atypical Honeycombing: cell size
irregular & contour is thicker than nl
Cobblestone Pattern: Aggregates of small polygonal
cells w/ bright cytoplasm
(= nl pig’d basal keratinocytes)
separated by less refractive
outline in the epidermis
Patterns formed
by cells in
Superficial Layers
Cobblestone pattern Atypical Cobblestone
Atypical Cobblestoning: irregularity in
cell size, shape, &/or refractivity; may
present with multiple small nucleated cell

7/18/2018
6
• Absence of honeycomb or cobblestone pattern
• Disarray of nl architecture of sup layers w/ unevenly distributed bright granular particles & cells
Patterns formed by cells in the
Superficial Layers
Disarranged pattern:
Disarranged pattern Disarranged
pattern
Disarranged pattern Disarranged pattern
Edged papilla • Demarcated rim of bright
confluent basal cells
• Dark holes in epid =
opening of dermal papillae
Pattern formed @ DEJ
Edged papillae
Non-edged papillae • Dermal papilla w/o
demarcated rim of
bright cells but
separated by a series
of large reflecting
cells.
Pattern formed at the DEJ
Non-edged papillae
Non-edged papillae

7/18/2018
7
Ring
Pattern
• Histopath: pred junctional
nevi w/ a lentiginous prolif
of melanocytes
• Bright peripheral rim =
single melanocytes & small
nests at DEJ
• Holes = dermal papillae
Meshwork Pattern • Round & oval shaped structures
= melanocytic nests located at
tips of rete (junctional nests) • Junctional thickening =
elongated rete ridges filled w/
melanocytes
Congenital nevus Superficial type
Junctional thickening
Dermis W/in dermis diff
structures can be
visualized:
• Nests
• Bright cells
• Collagen fibers
• Blood vessels
Bright cells
Collagen Vessels
Dermis: Nest (cluster or clod)
• Dermal melanocytic
nests w/in papillae
w/o connection to
epid
Dermal nests
• Oval to round bright
aggregate w/ well-
defined borders, c/o
clustered cells, freq
large & highly
refractive
Junctional nest
• Nests connected
w/ epidermal
basal cell layer
& bulge into dermal papillae
• Irregularly
shaped, w/ ill-
defined borders
• No visible
nucleus
• = melanophages
Dermis: Plump Bright Cells

7/18/2018
8
Collagen • Bright elongated
fibrillar
structures/bundles
w/ no cellular
component, no
visible nucleus, &
no visible
movement
• Distributed side by
side thru out dermis
Collagen
Distributed as coils
or rings in papillary
dermis
Distributed as
parallel bundles in
reticular dermis
Blood vessels Linear or canalicular
vessels parallel to
horizontal plane
Vessels traversing
thru papillae
perpendicular to
horizontal plane
Why Confocal?
The Future is NOW
• Help w/ DDX
• Confocal makes me better @ DP: horizontal view
• Convince resistant pt of need for biopsy/surgery
• Avoid bx if benign. Go directly to Rx if malignant – Pts do not consider a skin bx trivial: @U CONN 60% bxs
– Cosmetic sites, sites w/ delayed healing (legs)
• ID lesion to bx in pt w/ many atypical nevi
• ID site for surgery after bx
RCM Workflow:
1. Dermoscopy • Dermoscopic
imaging device
part of RCM
• Dermoscopy &
RCM combined:
sensitivity of 98%
• Dermoscopy
image 10 x 10 mm Guitera, et al. J Invest Dermatol 2009;129(1):131-8.
2. RCM
Imaging
• After dermoscopy
RCM images
acquired: ~4-6
mosaics w/in epid
& sup dermis
• Images reviewed
at bedside or
transferred via
internet for review
by remote MD

7/18/2018
9
Confocal Near: At the Bedside • Obtain image at exam table & evaluate while
obtaining image or immed after
• Immed answer avoid bx if benign or
proceed to definitive therapy if malignant
Remote Reading
Image captured by confocalist & read at bedside
or transmitted electronically to DP for sign out
Home Screen: Patient list
Lists completed & uncompleted evaluations
Select patient case • Access to clinical information
• Access to all images as thumbnails
(dermoscopy & RCM)
• Each clicked & expanded for SO

7/18/2018
10
Does RCM Work?
• 748 lesions: 629 cases (84.1%) benign no bx
• 119 cases (15.9%) bx’d: 44 concerns of ca: 38 malig & 6 benign 69 for atypical features on RCM: benign w/ atypia 6 due pts’ concerns or cosmetic: all benign
• 75 true neg results: 69 lesions bx’d for atypical RCM features + 6 lesions bx’d bc of pt concerns
• Sensitivity 100%; specificity 92.6% Giambrone, et al. (Rao). The dxic accuracy of in vivo confocal
microscopy in clinical practice. JAAD 2015;73:317-319.
Others Experience with RCM • RCM sensitivity for melanocytic lesions:
– 68-99% sensitivity
– 66-99% specificity
– Positive predictive value of 97.5%
– Negative predictive value of 99%
– Rare but not impossible to miss melanoma Binder, et al. Arch Dermatol 1995;131:286 // Argenziano, et al. Arch Dermatol 1998;134:1563 //
Piccolo, et al. Br J Dermatol 2002;147:481 // Carli, et al. J Eur Acad Dermatol Venereol 2002;16: 339
// Gerger, et al. Br J Dermatol 2008;158:329 // Rajpara, et al. Br J Dermatol 2009;161:591 //
Pellacani, et al. BJD 2014;171:1044 // Farnetani, et al. JAMA Derm 2015;151:1075 // Pellacani, et al.
JEADV 2016;30:413 // Borsari, et al JAMA Derm 2016;152:1093 // Menge, et al. JAAD 2016;74:
1114 // Song, Grant-Kels, et al. JAAD 2016;75:1187
ARTICLES LESION SENS SPECIFICITY
Nori, et al. JAAD 2004;51:923 BCC 100% 95.7%
Guitera, et al. JID 2012;132:2386 (Reduced 68% of bx’s)
BCC MM
100% 87.6%
88.5% 70.8%
Guitera, et al. JAMA Derm 2013; 149:692 LM 93% 76%
Rao, et al, JAAD 2013;69:e295 Mixed >90% >60%
Pellacani, et al. BJD 2014;171:1044 Mixed 76.3%
Farnetani, et al. JAMA Derm 2015;151:1075
Mixed 88.9% 79.3%
Pellacani, et al. JEADV 2016;30:413 (Reduced >70% of bx)
Mixed
Borsari, et al JAMA Derm 2016;152:1093 Mixed 95.3% 83.9%
Menge, et al. JAAD 2016;74:1114 LM 100% 71%
Song, Grant-Kels, et al. JAAD 2016;75:1187 (Reduced 60% of bx)
Mixed 85.7% 71.4%
UCONN Experience
Prospective:RCM Vs MDSLAMultispectral digital skin lesion analysis
• Pts scheduled for bx of clinical &/or dermoscopically
atypical pigmented lesions but NOT obviously MM
• Lesions evaluated w/ RCM & MDSLA prior to bx
• 55 lesions evaluated: MDSL Sens 71% Specificity 25%
RCM Sens 86% Specificity 67%
• RCM recommended bx for 22 lesions (40%)
– Path: 4 MMIS, 3 severely DN, 4 Atypical mel lesions
• 60% spared bx bc RCM benign!Song,Grant-Kels, et al.JAAD 2016;75:1187

7/18/2018
11
Imaging Mode: Mosaic Images can be scanned horizontally, with small quadratic fields-of-view forming a
square mosaic of contiguous 500 by 500 images: the RCM mosaic μm μm
Imaging Mode: stack Field of view:
500 μm by 500 μm
RCM 1500 Codes
3 Scenarios Possible • 96931 & 96934: YOUR staff capture
the image & you read it
• 96932 & 96935: YOUR staff capture the
image & someone else reads it.
• 96933 & 96936: Someone else captures it &
YOU read it. Thanks to AAD RUC team,
Dan Siegel &
Harold Rabinovitz
Cut Biopsy 11100, 11101
RCM Image Acquisition
Only
96932, 96935
RCM Interpretation
Only 96933, 96936
PathPC
88305
RCM Imaging &
Interpretation 96931, 96934
Path(TC+ PC)
88305
PathTC
88305
RVU First Lesion 2.93 2.92 1.28 1.11 4.51 1.94 0.83
RVU Each Additional Lesion 0.93 0.98 1.22 1.11 2.32 1.94 0.83
Medicare National Payment Rate $ First Lesion* $104.82 $104.46 $45.79 $39.71 $161.35 $69.40 $29.69
Medicare National Payment Rate $ Each
Additional Lesion* $33.27 $35.06 $43.65 $39.71 $83.00 $69.40 $29.69
*These rates are adjusted for cost-of-living variances, so your actual payment
maybe different from this number.
2017 Medicare National Payment Rates
$172.03
$75.58
$124.89
$35.63 $39.95
$41.75
2018
Handheld RCM 3000 • Introduced to clinical practice in 2011
• Small, portable & more accessible
for application on curved facial
surfaces
• A faster procedure
• Imaging of several lesions
simple, faster & simple
• No CPT code yet
Vivascope 1500
Vivascope 3000 Handheld RCM Traditional RCM
• ~25-30minutes
• Field of view = 8X8mm
• Viva stack capability
• Mosaic formation
• CPT code
• ~10 minutes
• Field of view = 0.9mm
• VivaStack capability
• No mosaics
• No CPT code
Vivascope 1500 Vivascope 3000

7/18/2018
12
Accuracy of in vivo RCM for dx of BCC: Comparative
study between handheld & wide-probe RCM
Castro, Stephens, Fraga-Braghiroli, Oliviero, Rezze, Rabinovitz , Scope .
J Eur Acad Dermatol Venereol. 2015; 29(6):1164-9.
54 BCC imaged with both RCM devices
Sensitivity
Specificity
100% 93%
78% 78%
Vivascope
1500 Vivascope
3000