computerized physician order entry systems: impact on physician-nurse cooperation marie-catherine...
TRANSCRIPT

Computerized Physician Order Entry systems: impact on physician-nurse cooperation
Marie-Catherine Beuscart-Zéphir*, Françoise Anceaux**
*EVALAB, Faculty of Medicine & University Hospital, Lille, France**Percotec-LAMIH, CNRS UMR 8530, University of Valenciennes, France
PERCOTEC

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Background
• Medication ordering, dispensing & administration is a key healthcare process in the hospital setting
• But it is unfortunately not as safe as one could expect (cf. « To err is human »)– 44000 to 98000 deaths /year due to medical
errors in US hospitals– 7000 deaths related to medication errors,
increased hospital cost amounts to $2 billion

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
• Computerized Physician Order Entry (CPOE) systems proved efficient in preventing and actually reducing medication errors and Adverse Drug Events
• But they remain difficult to implement, mostly because of physicians’ reluctance to use them
• Recent survey from US Pharmacopeia demonstrated a slow but steady increase of medication errors in the hospitals using CPOE systems during last two years

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Difficulties
• Increased workload and additional time for the physicians
• Organizational changes
• Poor usability
• Negative impact on Doctor-Nurse cooperation

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Two complementary studies
• 1st study: comparative analysis of paper-based and computer-based work situations combined with a usability assessment of the HCI
• 2nd study: detailed cognitive analysis of the cooperative activities and of the individual and shared representations underlying the management of the tasks and the control of the medication process

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Focus of the 1st study
• Analysis of Doctor-Nurse communication and cooperation comparing paper-based and CPOE situations
• Usability engineering approach:– Analysis of users’ individual and collective activity
– Usability assessment of the Human Computer Interface
• Focus on the medication administration functions:– Documentation of the time for administration in the
physicians’ orders
– Nurses’ understanding of the physicians’ orders

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Content of a medication order
• Name of the drug - Lasix, Medrol, …• Pharmaceutical form - pill, powder, cream, …• Route - oral, IV, …• Concentration - 20mg, 40mg, …• Dose / Quantity – 2 tablets, 75mg, • Frequency - 3 times / day• Duration - during 5 days• Time for administration – 8am- 12 - 6pm• Conditions - if pain

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Context of the study
Three observation sites
• University hospital of Lille:– 3000 bed-capacity hospital
– Paper based situation
– Nephrology and neuro-surgery
• General public hospital (Denain, north of France):– 413 bed-capacity hospital
– Paper-based situation
– surgery, respirology and convalescents (rehab)
• Georges Pompidou University hospital (Paris)– 825 bed-capacity hospital
– CPOE situation: immunology and nephrology
– Medasys DxC@re®

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Methods

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Methods (1): activity analysis
• Semi-structured and structured interviews of the target users (physicians and nurses)
• Continuous observations, audio recording
• Document analysis (written orders)
• Self confrontation interviews (users review the records of their own activity and explain their thought processes)

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Methods (2): usability assessment
Usability assessment of the CPOE functions of DxC@re®:
• Usability inspection (3 independent evaluators, ergonomic criteria)
• On-site usability tests (real activity, portable labs)


EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Site 1
(University hospital, Lille)
Site 2
(Denain general hospital)
Site 3
(G. Pompidou University hospital)
Usability lab
Task and activity analysis
•Paper-based
•80 hours observation
•Document analysis
•Paper-based
•450 hours observation
•Document analysis
•CPOE situation
•60 hours observation
Usability assessment
•Usability test
•DxC@re CPOE
•16 hours videotaped
•Usability inspection

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Results (1) Activity analysis Description of the work situations
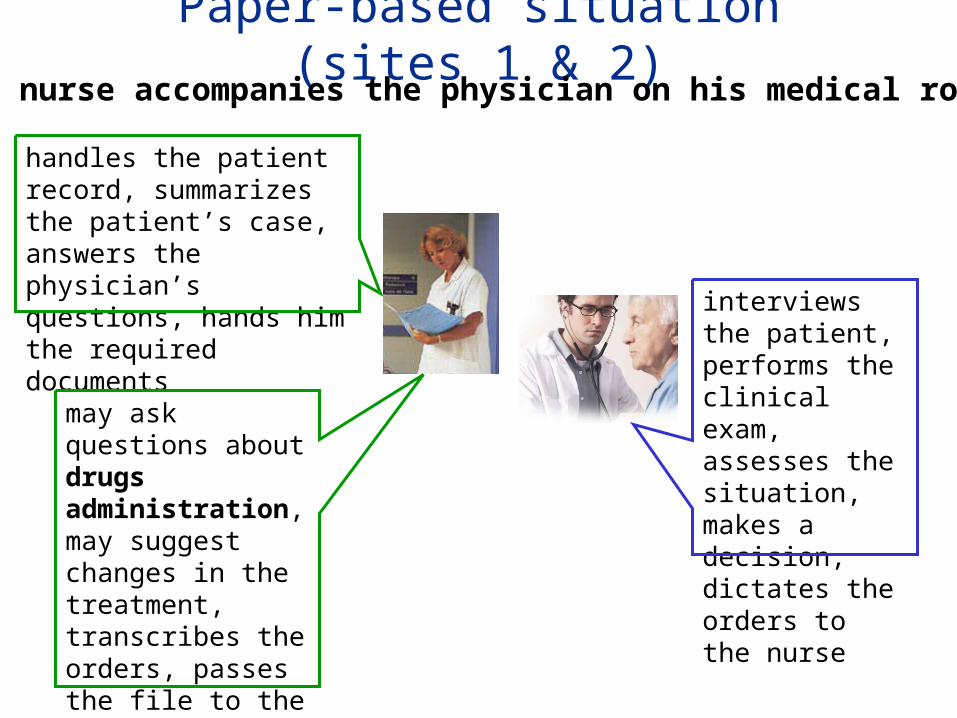
Paper-based situation (sites 1 & 2)The nurse accompanies the physician on his medical round
may ask questions about drugs administration, may suggest changes in the treatment, transcribes the orders, passes the file to the physician for signature
handles the patient record, summarizes the patient’s case, answers the physician’s questions, hands him the required documents
interviews the patient, performs the clinical exam, assesses the situation, makes a decision, dictates the orders to the nurse
Paper-based situation (sites 1 & 2)
After the rounds, the nurse copies (transcribes) the orders on her Medication Administration Record (MAR)

Computer-based (CPOE) situation (site 3)The nurse does not accompany the physician for his medical round
The physician gets the necessary medical and therapeutic information from the EPR
He interviews the patient, performs the clinical exam, assesses the situation, makes a decision about each item of the therapeutic treatment, enters each order on the computer using the CPOE
The SYSTEM (CPOE) automatically populates the nurses’ Medication Administration Record

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Documentation of the time for administration in the MAR
• CPOE situation:– The physician is constrained to enter precise orders,
including precise time for the administration– The system automatically updates the nurses’ MAR– The nurse has nothing to do
• Paper situation– The nurse has to transcribe the orders in her MAR
• Question: what is the available information / time for administration in the physician’s orders?

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
ResultsActivity analysis:
Qualitative and quantitative analysis of paper-based orders

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Analysis of the written orders• Focus on oral route orders (n = 671)
Respirology: n = 152; Surgery: n = 78; Convalescents (rehab): n = 441
• Analysis of the documentation of time for administration
• Orders written by the doctors vs. by the nurses: no difference

To copy
Nurse’s task & responsibility
FrequencyExamplesAdministration plan
(24h period)
1%(n=7)
•50 mg at 10 am.
•2 pills at 2 pm.Exact time for administration
Paper-based situation

Administration plan
(24h period)Examples Frequency
Nurse’s task & responsibility
Exact time for administration
•50 mg at 10 am.
•2 pills at 2 pm.
1%(n=7)
To copy
Approximate time for administration
•Morning, Noon, Evening
•At bedtime
•If diarrhea
•If pain
24%(n=163)
To specify the precise time for administration
Paper-based situation

Administration plan
(24h period)Examples Frequency
Nurse’s task & responsibility
Exact time for administration
•50 mg at 10 am.
•2 pills at 2 pm.
1%(n=7)
To copy
Approximate time for administration
•Morning, Noon, Evening
•At bedtime
•If diarrhea
•If pain
24%(n=163)
To specify the precise time for administration
No information / administration
schedule
•2 pills / Day
•25 mg every 2 days
75%(n=501)
To make the decision / time for administration
Paper-based situation

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Activity analysis: model of the activity

Medication ordering and administration process
Therapeutic decisionMedication ordering
Planning of medication administration
Drug administration
Paper-based situation

Medication ordering and administration process
Therapeutic decisionMedication ordering
Planning of medication administration
Drug administration
Makes thedecision
Gives the order: name & dosage
Schematic decision:
abstract plan
Paper-based situation

Medication ordering and administration process
Therapeutic decisionMedication ordering
Planning of medication administration
Drug administration
Makes thedecision
Gives the order: name & dosage
Schematic decision:
abstract plan
The nurse listens to the doctor-patient dialog, answers questions, asks questions
Paper-based situation

Medication ordering and administration process
Therapeutic decisionMedication ordering
Planning of medication administration
Drug administration
Makes thedecision
Gives the order: name & dosage
Schematic decision:
abstract plan
Specified plan (exact time-scheduling)
Administers the drug & documents administration
The nurse listens to the doctor-patient dialog, answers questions, asks questions
Paper-based situation

Medication ordering and administration process
Therapeutic decisionMedication ordering
Planning of medication administration
Drug administration
Schematic decision:
abstract plan
Specified plan (exact time-scheduling)
Administers the drug & documents administration
The nurse listens to the doctor-patient dialog, answers questions, asks questions
Cooperativeactivities
DistributedDecisionmaking
Paper-based situation
Makes thedecision
Gives the order: name & dosage

Medication ordering and administration process
Therapeutic decisionMedication ordering
Planning of medication administration
Drug administration
Common frame of Reference: CoFORSynchronous cooperation
The doctor-nurse dialog supports the elaboration and maintenance of a Common Frame of Reference
Coordination of actions = physician + nurse responsibility
Paper-based situation

Medication ordering and administration process
Therapeutic decisionMedication ordering
Planning of medication administration
Drug administration
Makes thedecision
Formulates the order: name & dosage
Schematic decision:
abstract plan
Specific plan (exact time-scheduling)
Administers the drug & documents administration
The nurse may ask questions of the doctor when he is available
Computer-based situation

Medication ordering and administration process
Therapeutic decisionMedication ordering
Planning of medication administration
Drug administration
Makes thedecision
Formulates the order: name & dosage
Schematic decision:
abstract plan
Specific plan (exact time-scheduling)
Administers the drug & documents administration
The nurse may ask questions of the doctor when he is available
Computer-based situation
Cooperativeactivities
DistributedDecisionmaking

Medication ordering and administration process
Therapeutic decisionMedication ordering
Planning of medication administration
Drug administration
No synchronous Doctor-Nurse dialogNo COFOR management
Coordination of actions = CPOE
Computer-based situation

Coordination of actions = CPOE
•How well does the system support the coordination of actions?•Does it help the users to understand each others actions and intentions?

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Results (2) Usability assessment


Order entry: time for administration …

Order entry: time for administration …

Selection of the pre-set schedule « morning, noon, evening, and bedtime » is automatically transcribed in « 8, 12, 18 and 21 h » in the time table (configuration depending on the time of the nurses rounds in the department)

Second solution: the physician clicks in the desired time slots and documents the dose to be delivered at that time

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Examples of problems / administration planning
• There is a problem of erroneous guidance with the time-table (ambiguous display)
• Information / times of administration can be ambiguous in the MAR


During the test, the physicians sometimes entered the wrong timings in the time table; they didn’t know what the grayish slots meant

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Examples of problems / administration planning
• There is a problem of erroneous guidance with the time-table (ambiguous display)
• Information / times of administration can be ambiguous in the MAR


During the test, the nurses interpreted the orders and made assumptions. When confronted with « bizarre » timings, the nurses made the corrections in their Medication Administration Record without asking the physician

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Conclusion of the 1st study

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
EFFERALGAN 500MG CPR BLANC
Horaire de prise : Matin Midi Soir Coucher
8
2118
12
Avt pansement
Si douleurs A la demande
EFFERALGAN 500MG Moment(s) :
couchersoirmidimatin
123
EFFERALGAN 500MG CPR BLANC
Horaire de prise : Matin Midi Soir Coucher
8
2118
12
ORALE
Avt pansement
Si douleurs A la demande
123
EFFERALGAN 500MG CPR BLANC
Horaire de prise : Matin Midi Soir CoucherHoraire de prise : Matin Midi Soir Coucher
8
2118
12
8
2118
12
ORALE
Avt pansement
Si douleurs A la demandeSi douleurs A la demande horaire exact
Fréquence :
unités ttes les (h) à partir de
Gestion par le patient
Condition(s) d’administration :
Traitement à domicile
Unité prescription
Voie administration orale
comprimé
8
2118
12
EFFERALGAN 500MG CPR BLANC
Horaire de prise : Matin Midi Soir CoucherHoraire de prise : Matin Midi Soir Coucher
8
2118
12
8
2118
12
Avt pansement
Si douleurs A la demandeSi douleurs A la demande
EFFERALGAN 500MG Moment(s) :
couchersoirmidimatin
123
EFFERALGAN 500MG CPR BLANC
Horaire de prise : Matin Midi Soir Coucher
8
2118
12
ORALE
Avt pansement
Si douleurs A la demande
123
EFFERALGAN 500MG CPR BLANC
Horaire de prise : Matin Midi Soir CoucherHoraire de prise : Matin Midi Soir Coucher
8
2118
12
8
2118
12
ORALE
Avt pansement
Si douleurs A la demandeSi douleurs A la demande horaire exact
Moment(s) :
couchersoirmidimatin
123
EFFERALGAN 500MG CPR BLANC
Horaire de prise : Matin Midi Soir Coucher
8
2118
12
ORALE
Avt pansement
Si douleurs A la demande
123
EFFERALGAN 500MG CPR BLANC
Horaire de prise : Matin Midi Soir CoucherHoraire de prise : Matin Midi Soir Coucher
8
2118
12
8
2118
12
ORALE
Avt pansement
Si douleurs A la demandeSi douleurs A la demande horaire exact
Fréquence :
unités ttes les (h) à partir de
Fréquence :
unités ttes les (h) à partir de
Gestion par le patient
Condition(s) d’administration :
Gestion par le patient
Condition(s) d’administration :
Traitement à domicile
Unité prescription
Voie administration orale
compriméUnité prescription
Voie administration orale
comprimé
8
2118
12
8
2118
12

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Questions and problems• The cognitive task and activity analysis
uncovered important underlying variables– Synchronous or asynchronous cooperation– Distributed or individual decision making– Individual and / or shared representations of the
medication decision process
• Impact on:– The control of the medication process– The prevention of new risks in the process

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Focus of the second study
• Individual and shared representations underlying (supporting) the management of the tasks and the control of the medication process:– Content of the Common Frame of Reference?
• Important variable: type of cooperation, synchronous vs. asynchronous– Preliminary results in the paper-based synchronous
situation

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Analysis of physician – nurse dialogs:verbal protocol analysis

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Methods
• Detailed observation of the physician-nurse dialog during the medical rounds– Audio-taped, detailed observation grid
• Transcription: detailed verbal (& behavioral) protocols
• Protocol analysis: coding scheme
• Analysis of the coded communication units

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Protocol analysis
• A coding scheme is necessary to code the cooperation units in the doctor-nurse dialogs recorded during the medical rounds
• This analysis relies on a model of cognitive architecture of cooperation (Millot & Hoc 97; Hoc 2001)
EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Cognitive architecture of cooperation
• On a cognitive point of view, cooperation can be described as the management of interferences
• Interference: the effects of the action(s) of one agent are relevant for the goals of another agent, either to favor it (positive interference) or to threaten it (negative interference) (Castelfranchi 98; Hoc 2001)
• Interference management requires the sharing of task representations, of partners’ activities, and of the goal to be reached.
• The COmmon Frame Of Reference (COFOR) is the shared representation that supports interference management

Cooperation cognitive architecture (Hoc, Helie & Loiselet, 2000)
Meta Cooperation
Cooperationin planning
Cooperationin action

Cooperation cognitive architecture (Hoc, Helie & Loiselet)
Meta Cooperation
Cooperationin planning
Cooperationin action Interference management (coordination of actions)

Cooperation cognitive architecture (Hoc, Helie & Loiselet)
Meta Cooperation
Cooperationin planning
Cooperationin action
Agent A’s Current Representation
Interference management (coordination of actions)

Cooperation cognitive architecture (Hoc, Helie & Loiselet)
Meta Cooperation
Cooperationin planning
Cooperationin action
Agent A’s Current Representation
Agent B’s Current Representation
Interference management (coordination of actions)

Cooperation cognitive architecture (Hoc, Helie & Loiselet)
Meta Cooperation
Cooperationin planning
Cooperationin action
COFORElaboration Maintenance
Agent A’s Current Representation
Agent B’s Current Representation
CommonFrame ofReference
Interference management (coordination of actions)

Cooperation cognitive architecture (Hoc, Helie & Loiselet)
Meta Cooperation
Cooperationin planning
Cooperationin action
COFORElaboration Maintenance
Anticipative management of interferences
When local management is not efficient or sufficient
Agent A’s Current Representation
Agent B’s Current Representation
CommonFrame ofReference
Interference management (coordination of actions)

Cooperation cognitive architecture (Hoc, Helie & Loiselet)
Meta Cooperation
Cooperationin planning
Cooperationin action
Elaboration of compatible
representations
Elaboration of a mental model of self and a mental
model of others
Elaboration of a common code ofcommunication
COFORElaboration Maintenance
Anticipative management of interferences
When local management is not efficient or sufficient
Agent A’s Current Representation
Agent B’s Current Representation
CommonFrame ofReference
Interference management (coordination of actions)

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Verbal protocol analysis: example of coding of verbal exchanges during the
medical round

Nurse : 25, we can leave him on that Physician : no, we’re going to stop it entirelyNurse : it’s up to you.
Physician : OK,your temperature did’nt go up again?Patient : NoNurse : Since we stopped the Claforan, he’s doing betterPhysician : yeah, yeah
(he picks up the temperature chart from the foot of the bed) Physician : artificial tears, vitamin A, Medrol, Omeprazole…ok.
Nurse : and the Médrol does he still need it? We’re at post-op day ... I can’t remember
Nurse : What dose was he on??Physician : (he picks up the temperature chart from the foot of the bed )
50, post-op day 10 we can stop it
Physician : Did we get an inflammation order set with a CRP?Nurse : yesterday
Physician : yesterday…(the nurse hands him the results and he reads them) Physician : He’s getting Medrol, eh?Nurse : mmmm
Physician : CRP below 3
Physician : yeah, but if we stop it ... Yeah, you’re right

COFOR Management
maintenance
elaboration
Nurse : 25, we can leave him on that Physician : no, we’re going to stop it entirelyNurse : it’s up to you.
Physician : OK,your temperature did’nt go up again?Patient : NoNurse : Since we stopped the Claforan, he’s doing betterPhysician : yeah, yeah
(he picks up the temperature chart from the foot of the bed) Physician : artificial tears, vitamin A, Medrol, Omeprazole…ok.
Nurse : and the Médrol does he still need it? We’re at post-op day ... I can’t remember
Nurse : What dose was he on??Physician : (he picks up the temperature chart from the foot of the bed )
50, post-op day 10 we can stop it
Physician : Did we get an inflammation order set with a CRP?Nurse : yesterday
Physician : yesterday…(the nurse hands him the results and he reads them) Physician : He’s getting Medrol, eh?Nurse : mmmm
Physician : CRP below 3
Physician : yeah, but if we stop it ... Yeah, you’re right

COFOR Management
maintenance
elaboration
Nurse : 25, we can leave him on that Physician : no, we’re going to stop it entirelyNurse : it’s up to you.
Physician : OK,your temperature did’nt go up again?Patient : NoNurse : Since we stopped the Claforan, he’s doing betterPhysician : yeah, yeah
(he picks up the temperature chart from the foot of the bed) Physician : artificial tears, vitamin A, Medrol, Omeprazole…ok.
Nurse : and the Médrol does he still need it? We’re at post-op day ... I can’t remember
Nurse : What dose was he on??Physician : (he picks up the temperature chart from the foot of the bed )
50, post-op day 10 we can stop it
Physician : Did we get an inflammation order set with a CRP?Nurse : yesterday
Physician : yesterday…(the nurse hands him the results and he reads them) Physician : He’s getting Medrol, eh?Nurse : mmmm
Physician : CRP below 3
Physician : yeah, but if we stop it ... Yeah, you’re right
Interference detection
Interference creation

COFOR Management
maintenance
elaboration
Nurse : 25, we can leave him on that Physician : no, we’re going to stop it entirelyNurse : it’s up to you.
Physician : OK,your temperature did’nt go up again?Patient : NoNurse : Since we stopped the Claforan, he’s doing betterPhysician : yeah, yeah
(he picks up the temperature chart from the foot of the bed) Physician : artificial tears, vitamin A, Medrol, Omeprazole…ok.
Nurse : and the Médrol does he still need it? We’re at post-op day ... I can’t remember
Nurse : What dose was he on??Physician : (he picks up the temperature chart from the foot of the bed )
50, post-op day 10 we can stop it
Physician : Did we get an inflammation order set with a CRP?Nurse : yesterday
Physician : yesterday…(the nurse hands him the results and he reads them) Physician : He’s getting Medrol, eh?Nurse : mmmm
Physician : CRP below 3
Physician : yeah, but if we stop it ... Yeah, you’re right
Interference detection
Interference resolution
Interference creation

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
• This typical excerpt demonstrates – the importance of COFOR management in the
dialogs– The important part played by the nurse in the
medication decision making

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
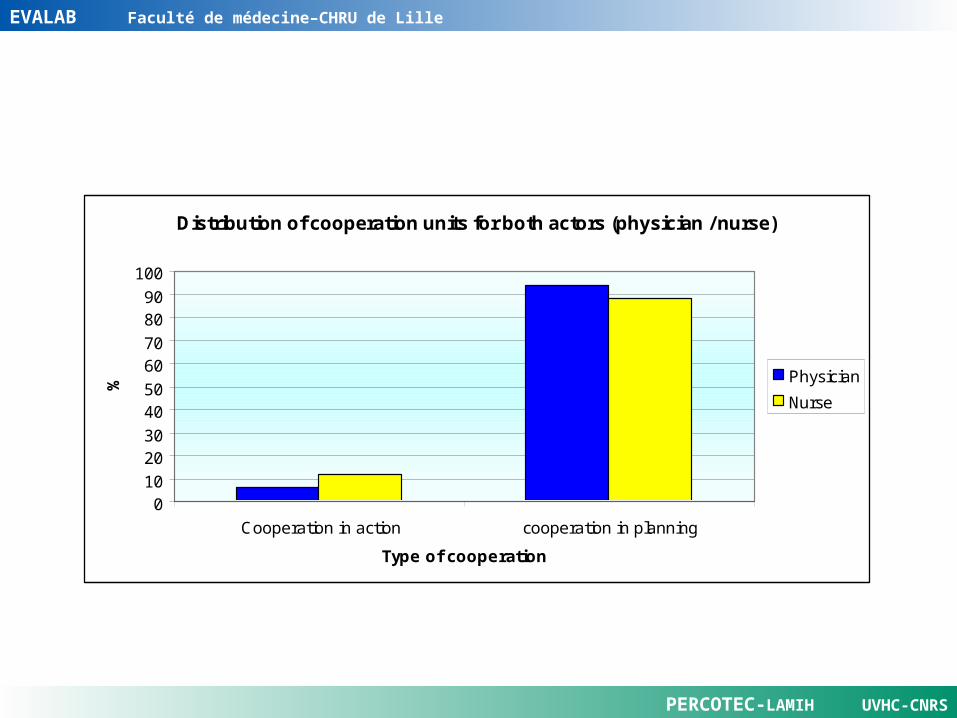
Preliminary results
• Two rounds, 30 patients (11 + 19), 1h53mn recorded
• Total number of communication units: 790
• Total number of physician-nurse communication units: 417
EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Distribution of cooperation units for both actors (physician / nurse)
010
2030
4050
6070
8090
100
Cooperation in action cooperation in planning
Type of cooperation
%
Physician
Nurse

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
distribution of Physician Nurse cooperation units
0
5
10
15
20
25
Requirementfor
information
Answer /requirement
forinformation
Transmissionof information(comments onone's actions)
Decisionmaking(order)
Suggestion
Functions of communication units
%
Physician
Nurse

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Discussion, conclusion
EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Impact for the design of CPOE systems
• Normative model: the physician is responsible for the decision making and for medication ordering he is solely responsible for orders entry
• Observed activity in the paper-based situations (5 departments, 2 hospitals): the nurses play an important part in the decision making part of the process, they are often in charge of orders entry

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
• Not only a design issue: also an organizational issue and a safety issue
• Can we (must we) imagine systems implementing a cooperative model of the medication ordering process and supporting a distributed decision making process?
Impact for the design of CPOE systems

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
• The physician and the nurse are in charge – of the coordination of their actions – of the control of the process.
• They share part of their individual representations, and their control of the process overlap.
• The nurse can control the whole process at a high level (tactical survey)
Paper-Based situation

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
CommonFrame ofReference
Medication
Planning ordering administration
Physician’s control
of the processNurse’s control of
the processShared control

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
• The system is in charge – of the coordination of the actions – of the overall control of the medication ordering
and administration process.
• This control and the actions performed by the system are not always visible to the users.
• The nurse controls a smaller part of the process, only on an operational level.
CPOE situation

Medication
Planning ordering administration
Physician’s control
of the processNurse’s control of
the process
CPOE’s Control of the
process

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Next steps
Paper-based CPOE
Synchronous cooperationCommon rounds
FrequentAnalysis in process
??????
Asynchronous cooperation
No common rounds
Less frequentAnalysis in process
FrequentAnalysis in process
EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Thank you for your attention
Questions?

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Documents analysis
• Extensive quantitative and qualitative analysis of a sample of 818 written orders– site 1 Neurosurgery, 109 orders for 20 patients
mean length of stay = 6 days– site 2 Respirology 292 orders, 42 patients,
mean length of stay = 9 days– and site 2 Convalescents 417 orders, 38
patients, mean length of stay = 17 days

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
• Name of the drug - Lasix, Medrol, …• Pharmaceutical form - pill, powder, cream, …• Route - oral, IV, …• Concentration - 20mg, 40mg, …• Dose / Quantity – 2 tablets, 75mg, • Frequency - 3 times / day• Duration - during 5 days• Time for administration – 8am- 12 - 6pm• Conditions - if pain

Percentage of available data elements in 818 medication orders (oral route)
0 20 40 60 80 100
ca
teg
ori
es
of
av
aila
ble
da
ta e
lem
en
ts
percentages
Site 2 Convalescents
Site 2 Respirology
Site 1 Neurosurgery

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Patterns of missing information
Total Daily Dose 0 0 0 1 0 1 1Concentration of medication per tablet 0 0 0 0 0 1 1Total number of tablets per day 0 0 1 0 1 1 1Number of tablets per administration 0 0 0 0 1 0 1Frequency of administration 0 1 0 0 1 0 1Patterns P1 P3 P4 P5P2
Legend: 0 = missing data; 1 = available data

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Distribution of the patterns within the 818 orders from the three departments of the two hospitals
0
5
10
15
20
25
30
35
40
P1 P2 P3 P4 P5
Patterns
%
Neuro surgery
Respirology
Convalescents

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Self Confrontation interviews (Nurses)
• Exploratory study: 2 nurses, Neurosurgery• Confronted with orders representing patterns
1 tà 4• Asked to explain how they would carry out
the orders (what, and when) and on which knowledge they would rely on to fill in the missing data
• Content analysis: 217 information units identified and categorized

Cooperation level
Categories of knowledge ExamplesObserved frequency
Meta-cooperation
Knowledge on her own competencies
“I haven’t enough information to execute this order” 8%
Knowledge on nurses strategies “A nurse would have to phone the doctor” 10%
Knowledge on partners “The anaesthetist always documents his orders this way” 10%
Cooperation in planning
Knowledge on the patient’s case and his particular context
“He [the patient]’s already on medication at home, he needs his usual meds” 13%
Knowledge on the medical decision making
“This treatment depends on two parameters, when they are met, we may suggest a shift from the intravenous to the oral route”
2%
Contextual knowledge, exceptions: when rules don’t apply
“The patient is NPO [fasting] so should not get it [the medication] orally, but the anaesthetist explicitly ordered it, so it’s OK”
6%
Knowledge on medication: usual dosage, rules of administration
“It is always one dose in the morning”
“It is always 100 mg pills that we divide in two or four”
31%
Knowledge on orders documentation: usual codes for notation and transcribing
“We would have written it in the MAR”
20%

EVALAB Faculté de médecine–CHRU de Lille
PERCOTEC-LAMIH UVHC-CNRS
Distribution of the categories of knowledge necessary to administer medication orders according to two patterns of
missing data
0 10 20 30 40 50 60 70
K / own competencies
K / nurses strategies
K / partners
K / patient's case
K / medication
K / writing & transcribing codes
Exceptions
Pattern
s
%
P4
P1
Pattern 1: « lasix »; Pattern 4: « Lasix 20mg, 2 X Day »