compliance or defiance? kevin thompson. introductions who am i ? what am i doing here?
TRANSCRIPT
Compliance or Defiance?
Kevin Thompson

Introductions
Who am I ?What am I doing here?

Who are you?

What’s the aim of the session?• GOS contract compliance• The needs and wants of PCTs• Requirements of clinical
governance in enhanced service provision• To deliver a few key messages

Clinical Governance – Lets take a closer look
A systematic approach to maintaining and improving the quality of patient care withina health system

More jargon & blurb• A framework through which NHS organisations are
accountable for continually improving the quality of their services and safeguarding high standards of care by creating an environment in which excellence in clinical care will flourish.
Three key attributes:• High standards of care• Transparency and accountability and • Continuous improvement.
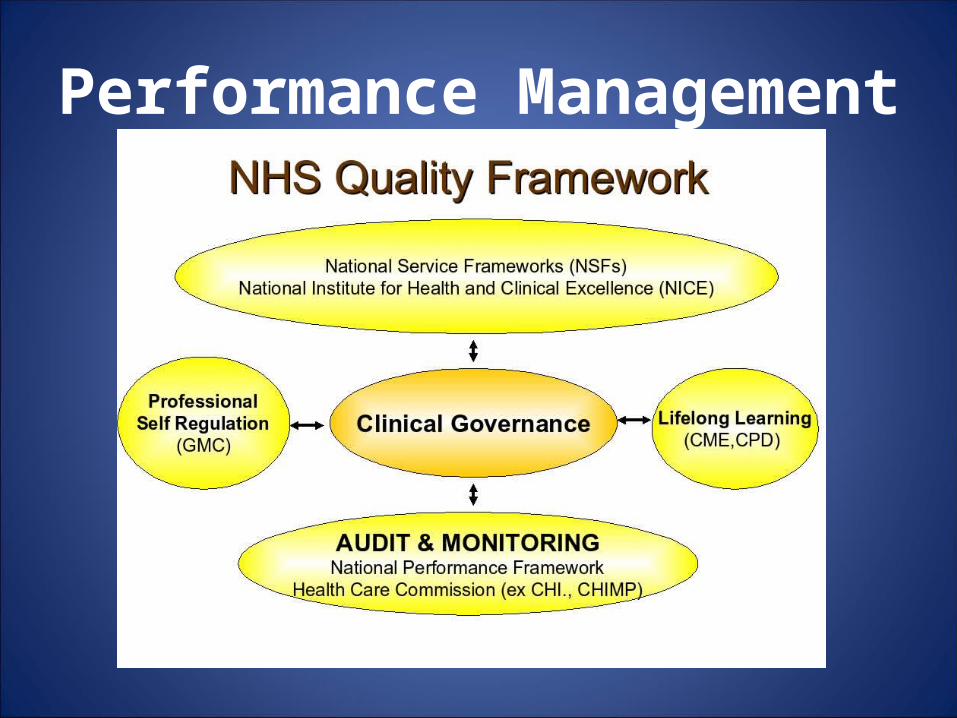
Performance Management

An NHS Invention – Which has never been a condition of our GOS contracts

Factors that have driven the CG agenda
• Secondary Care issues 1995 Bristol Babies Scandal• Social Service Review 2003 Victoria Climbie Report• Infection control MRSA, CjD, Flu Pandemics• protective legislation, health & safety and
employment law• Disabilities Act, Discrimination Act, Equalities Act• The right to complain • Ever increasing litigious society• Ever increasing risk averse society

Compare this landscape with Optics
• Competitive market place• Comparatively safe• Complaints are
negligible • We raise our own
standards

GOS is the PCTs square peg
GOS
Problem is - Expectations are now higher
• Enhanced service development has highlighted this anomaly to PCTs
• Some clinical governance MUST be implemented if you are to hold an Enhanced Service contract

Let’s get our ducks in a row
• GOS should simply require a list of policies, procedures and protocols• In 3 years time, so long as the same
procedures are in place, you are entitled to continue providing GOS services• BUT....Any introduction of CG means
demonstrating CONTINUOUS improvement
But why are PCTs so keen on CG ?• As of 1999, Trust Boards
assumed aLegal responsibility for quality of care.
• Clinical governance is the mechanismby which that responsibility is discharged.

But why are PCTs so keen on CG ?• Trusts must prepare an
Annual Review ofClinical Governance toreport on quality of careand its maintenance
SO IT REALLY IS AN IMPORTANTBOX TICKING EXERCISE
Who sets the standards?

Standards for Better Health
• A set of standards set out by the Department of Health in 2004. (Pillars – then Domains)
• NHS trusts must declare their level of compliance with these standards as part of their Annual Health Check.

Level 1 Level 2 Level 3
Key issue in L3 is demonstrating compliance

However• Although the Care Quality Commission
is the new independent regulator of health and social care in England
• The Dept of Health has specifically excluded primary ophthalmic services from the remit of the CQC

So here we go............

Key Message Number 1• GOS is a centrally negotiated, centrally funded
national contract• Compliance should NOT under ANY circumstances
be seen as being subject to local conditions at the whim of an individual/PCT
• GOS does NOT include payment for Clinical Governance
• LOCs MUST be empowered to defend their members right to hold a national contract using nationally agreed guidelines.

Don’t keep stepping back

RememberAs an LOC you have safety in numbers
Please share your issues with others

So what is ?
To achieve any standardSomeone has to set the goalposts

There must be an agreed minimum baseline standard
Why is QiO unique?
All about being SAFE !

IT committee

Description of QiO Levels
Level 1• Is a mirror image of the GOS contract
monitoring form to enable compliance.• This defines advice on SAFE practice
• This is the AGREED baseline

Level 1Safe Practice
What we are supposed to doWhat we say we do
What we ACTUALLY do

Level 2
Picks up other standardsthat may be required in
enhanced service provision

Level 2Good Practice – Enhanced Services

Level 3
Deals with more aspirational standards for practice
development
Level 3 – Best Practice

What are the interactive audits?Currently 3 Audits
• Record keeping• Infection control• Information governanceDo I have to complete them for GOS
compliance?• NO................BUT.......................

Are we contortionists ?

Beware of Clause 100
The most commonly used clause to over regulate is clause 100
100. The contractor shall comply with all relevant legislation and have regard to all relevant guidance
issued by the PCT, the SHA, or the Sec. of State.• QiO is not just a help tool for contractors
• It is intended to help OAs and PCTs understand the environment that we work in and the risks attached
• The audits simply highlight aspects of Level 1 GOS compliance that relate to an area of specific subject matter to demonstrate their relevance.

Record Keeping AuditTHIS IS NOT A CLINICAL AUDIT
IT IS A DATA AUDIT
WARNING
• Erroneous clinical findings can lead to complicity
• Unless concerns have been raised about performance, there is no reason why you should be scrutinised on your clinical performance and decision making
• This measures ability to RECORD only

How’s my driving?

It’s a friendly reminder

Before this...........
Or this..............

Record keeping auditLevel 1 – Q13.5-13.7
Records should be:•Fully maintained•Accurate•contemporaneous•Informative•legible
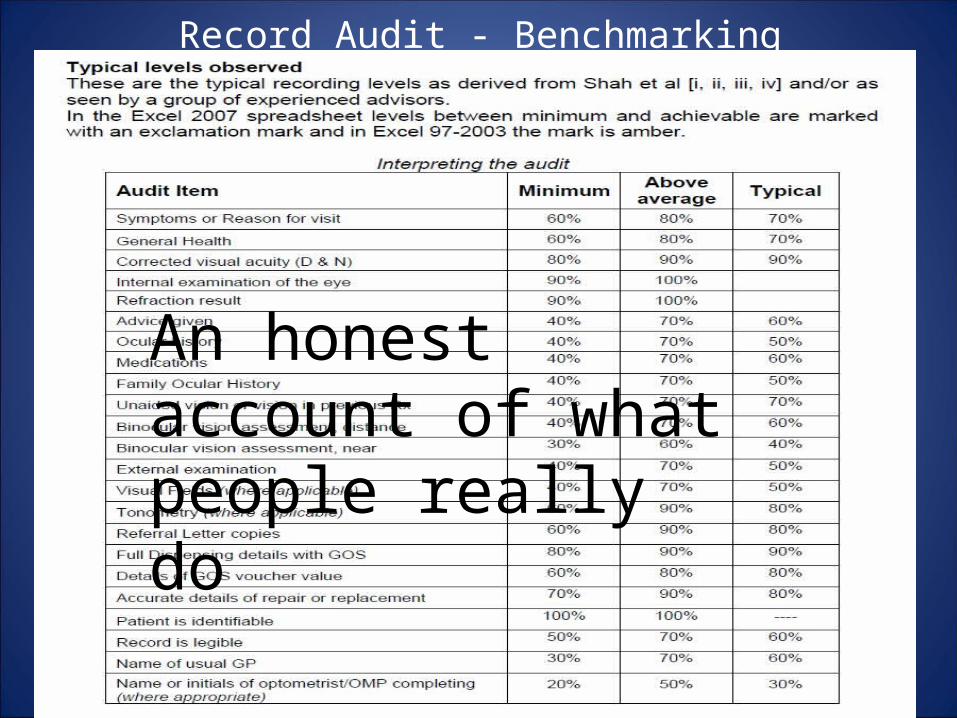
Record Audit - Benchmarking
An honest account of what people really do
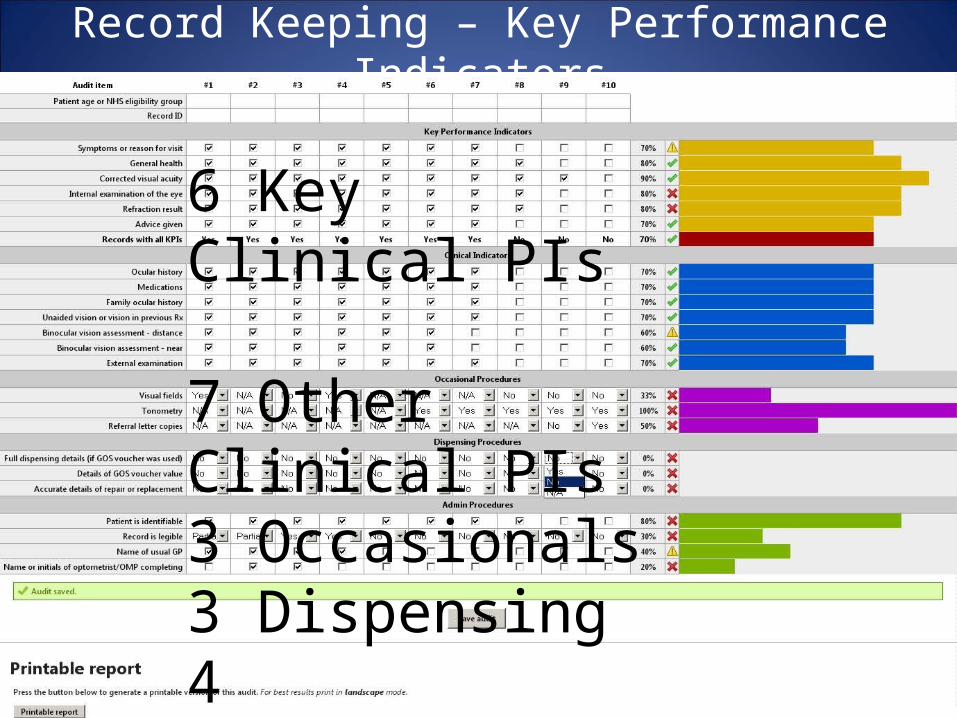
Record Keeping – Key Performance Indicators
6 Key Clinical PIs
7 Other Clinical PIs3 Occasionals3 Dispensing4 Administrative
Top 6 KPIs to remember
Is anything in life 100% perfect?
Why are they here?Are they alive?Can they see?Is it alright in there?Do they need specs?Did I remember to speak at any point?

New AOP information documentReplaces Sight Test Resource Pack
“In Practice” section of AOP web site

Infection Control Audit
Our “patients” tend NOT to be sick
Much of this is simply about good housekeeping

We accept that if an enhanced service were developed that dealt with a greater number of
sick people, more onerous conditions may need to be attached
Proportionate to the risk
Appropriate to the
profession

Infection Control Audit
The audit has been carefully worded as a training tool, to be used as a statement
for all staff to sign up to as a demonstration of compliance
38 Questions4 Sections
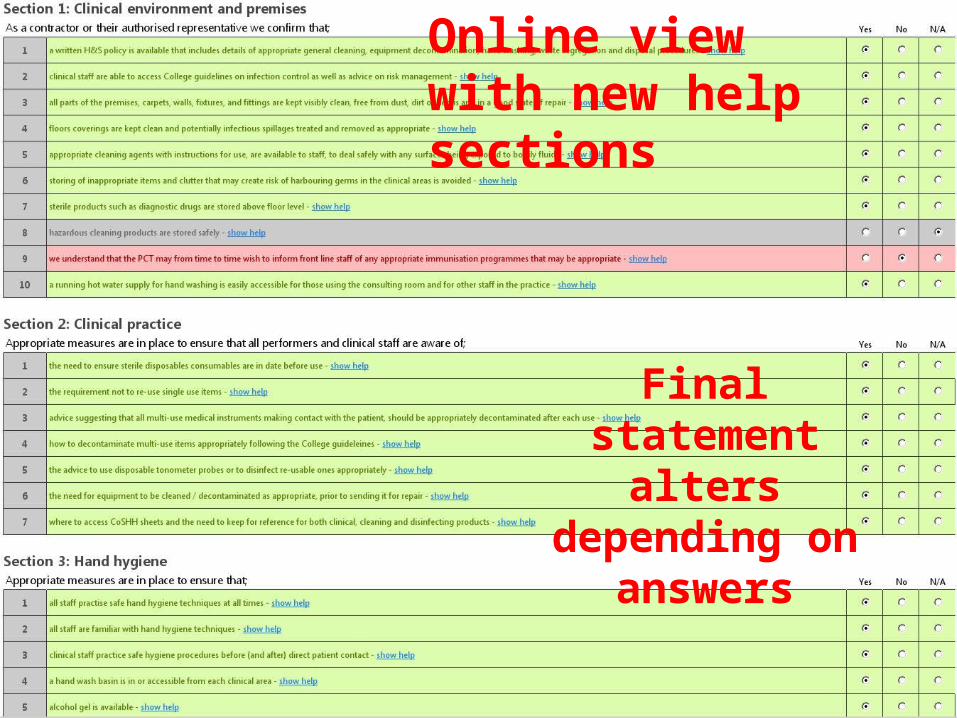
Final statement alters depending
on answers
Online view with new help sections
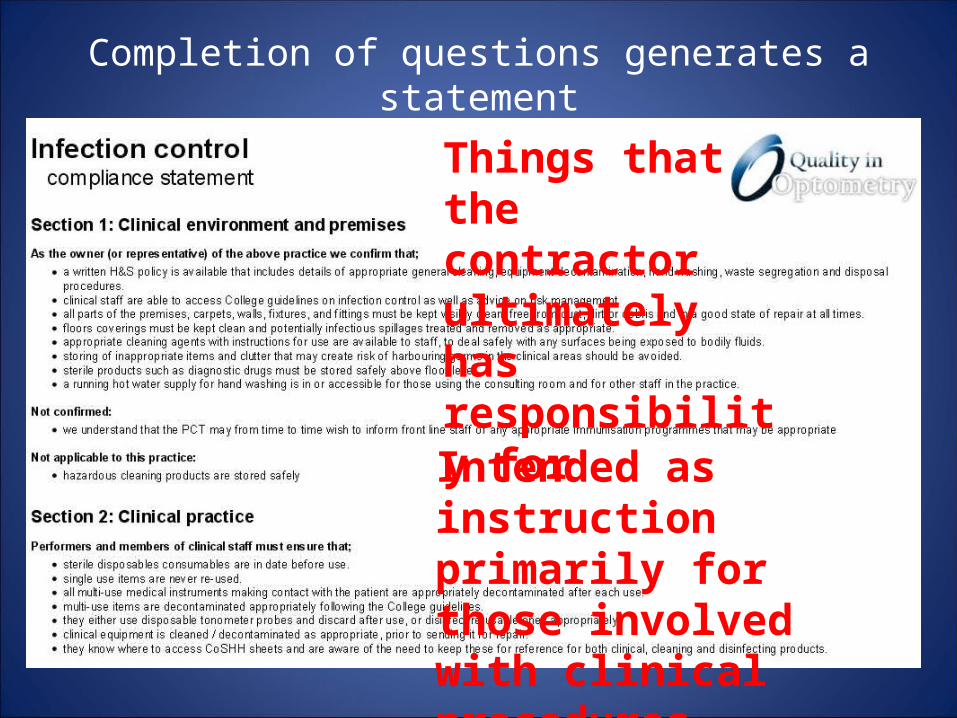
Completion of questions generates a statement
Things that the contractor ultimately has responsibility for
Intended as instruction primarily for those involved with clinical procedures

Completion of questions generates a statement
Intended as instruction for all
staff – general health & safety
and good housekeeping

Completion of questions also generates a form for all staff to sign
Demonstrates an element of training and
understanding of everyone’s obligations

Information Governance Audit
Summer 2010Connecting for Health launch Eyecare Toolkitentirely inappropriate for optical sector
No connectivity
to NHS IT

Lack of NHS connectivity •Highly unlikely that there will be any form of connectivity for GOS in next few years
•We recognise that there may be some instances of connectivity in ES (Scotland perhaps?)
•QiO audit is aimed at PCTs who are raising the issue of the CfH toolkit

Information Governance Audit
• 13 areas of “compliance” dealt with• lots of overlap and repetition• prints off a compliance statement for
staff to sign• grading is based on the CfH toolkit
grading levels

Completion of questions generates statement and form for all staff to sign
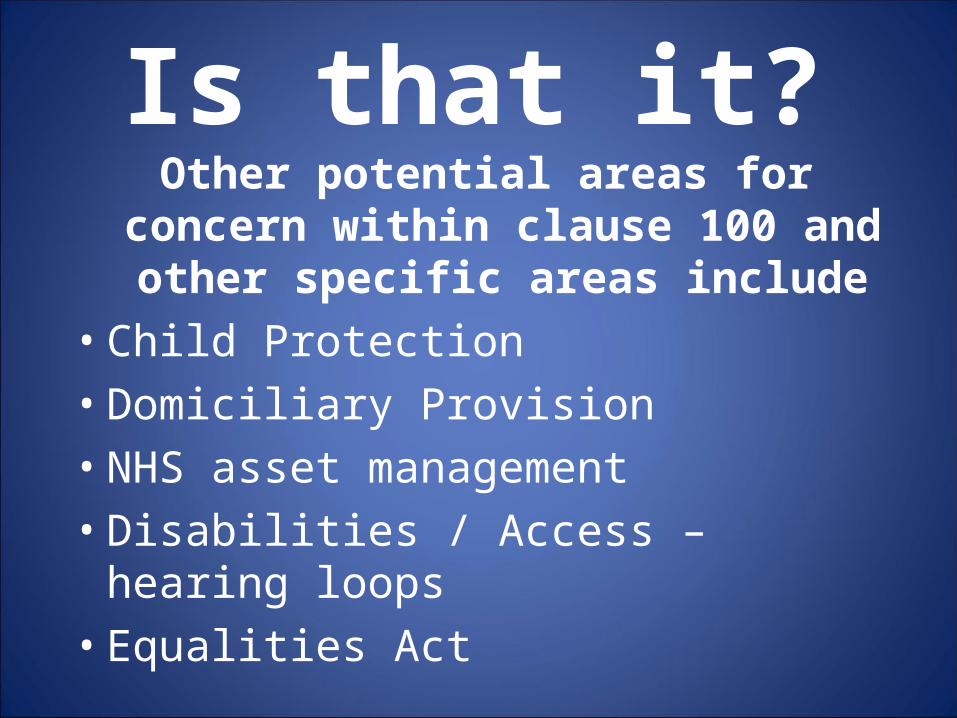
Is that it?Other potential areas for concern within
clause 100 and other specific areas include
• Child Protection• Domiciliary Provision• NHS asset management • Disabilities / Access – hearing loops• Equalities Act

We need you to alert us before you go into overload

Beware the dangers of Enhanced Service Provision
Golden opportunity for PCTs to
pull optometry
into line
LOCs negotiating MUST agree reasonable
terms
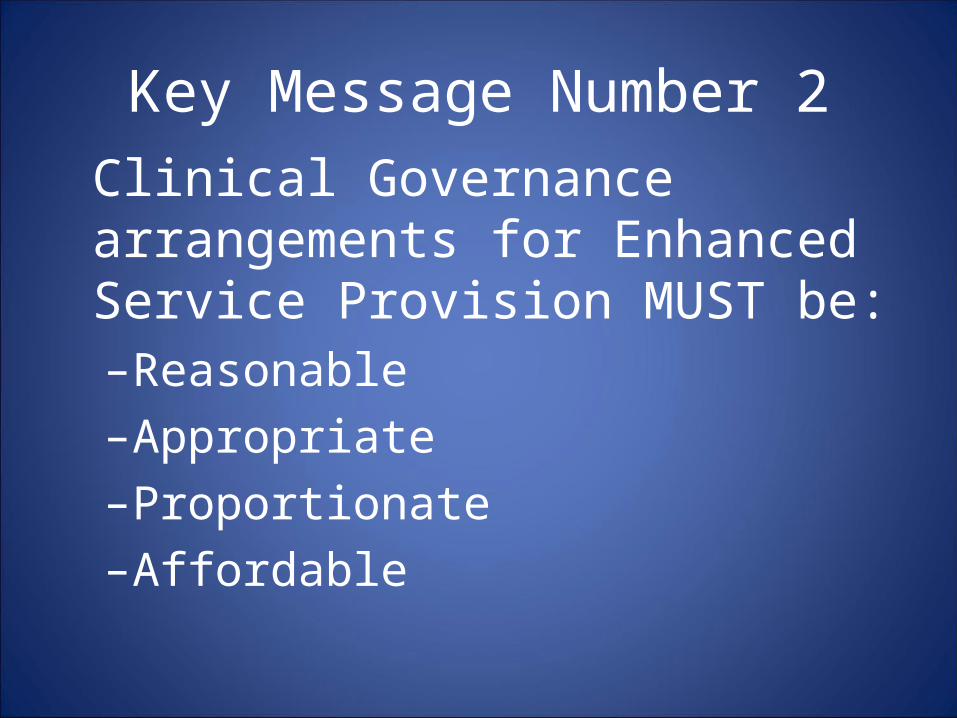
Key Message Number 2Clinical Governance arrangements for Enhanced Service Provision MUST be:–Reasonable–Appropriate–Proportionate–Affordable
LOCs MUST look for the hidden detail that may come back and bite
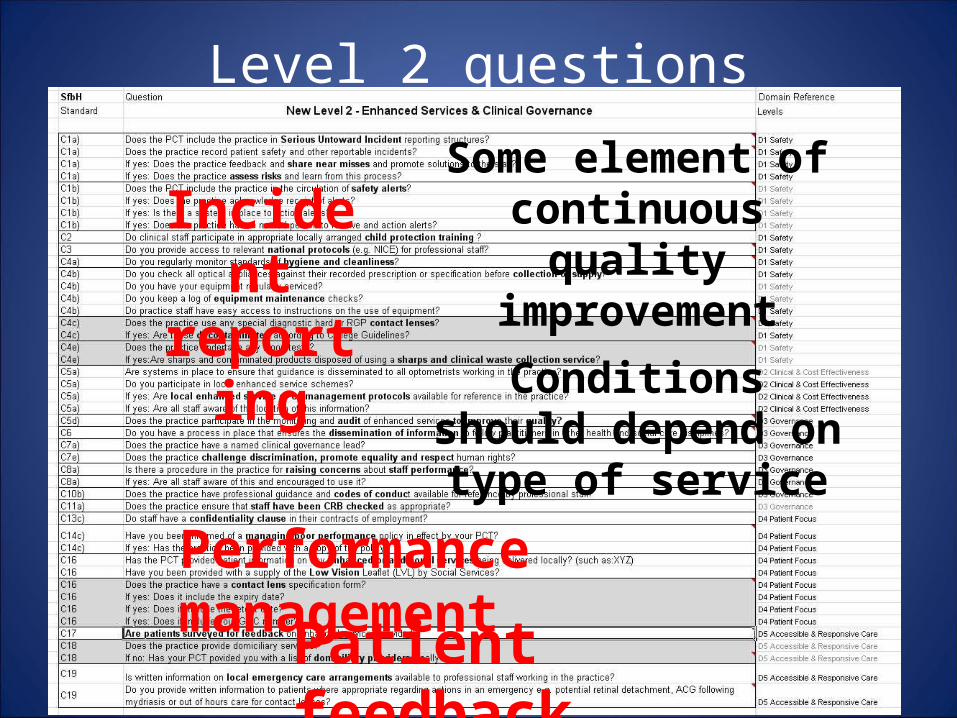
Level 2 questions
Some element of continuous quality
improvement
Conditions should depend on type of
service
Incident reporting
Performance management
Patient feedback

Level 3 questions – a lot of tough stuff

Key Message Number 3
• Do NOT get conned into delivering clinical governance for a one-off sum.• It will require all 3 levels of QiO (SfBH)• It is not a one-off process • Fees MUST be adequate and ongoing

We tend to want to tick all the boxes
more questions?

But just for once
OF LEVEL 3 !!

Is there a benefit to me if I try to implement clinical governance??

Are there personal benefits?

Improving internal standards• Customer care• Auditing• Incident reporting• Safer environment
for everyone

Not just about patient safetyMore about your own safety
BUT..............• If PCT driven• Look closely at poor performance
policy• Most are punitive rather than
supportive• Other professions have MUCH more
support
So if you are going to expose yourselfIt’s best not to do it in public !
Key Message Number 4
• Developing performance management procedures can actually be beneficial to the success of your business
• But beware of punitive PCT measures within performance policies

Compliance or Defiance?Summary of Key Messages
• LOCs should promote QiO• Beware the hidden cost of ES• Do not get conned into delivering CG
simply for the benefit of a PCT• If you DO implement PERFORMANCE
MANAGEMENT, use it to your own advantage

Stand your ground
Discussion – Is there anything more QiO & LOCSU can help you with?