complete remission of ovarian cancer induced intractable malignant ascites with intraperitoneal...
TRANSCRIPT
SHORT REPORT
Complete remission of ovarian cancer induced intractablemalignant ascites with intraperitoneal bevacizumab.Immunological observations and a literature review
Filippo Bellati & Chiara Napoletano & Ilary Ruscito &
Maria Pastore & Milena Pernice & Morena Antonilli &Marianna Nuti & Pierluigi Benedetti Panici
Received: 23 September 2009 /Accepted: 28 October 2009 /Published online: 24 November 2009# Springer Science + Business Media, LLC 2009
Summary Malignant ascites resistant to conventionaldrugs frequently affects ovarian cancer patients at the endof life. Here we report the case of a patient who benefitedfrom complete resolution of ascites after low dose intraper-itoneal administration of bevacizumab. Immunologicalanalyses showed an initial increase in proportion andfunction of CD8+ effector T cells and a reduction ofcirculating Treg cells. A review of the current literatureregarding bevacizumab in ovarian cancer is reported.Bevacizumab has shown a high efficacy in the treatmentof ovarian cancer. Intraperitoneal administration induces animmune activation and appears promising in the treatmentof malignant ascites.
Keywords Ascites . Bevacizumab . Intraperitoneal .
Lymphocyte . Ovarian Cancer
Introduction
Patients affected by platinum refractory ovarian cancerremain the greatest problem faced by Gynecologic Oncol-ogists in developed countries [1]. These women suffer froma dismal prognosis associated with severely impairedquality of life. In their last period of life, malignant ascitesresistant to conventional drugs affects 28% of thesepatients. Symptoms include abdominal swelling (55%),abdominal pain (53%), nausea (37%), anorexia (36%),vomiting (25%), and fatigue (17%) [2, 3]. Several medicalstrategies can be attempted, but most patients will in anycase require repeated paracentesis or permanent drains.
Drugs that have been investigated and that are commonlyadopted in the treatment of malignant ascites include diuretics,cytokines and cytotoxic agents administered intraperitoneally(ip). Diuretics have demonstrated to achieve high responserates in particular subsets of oncology patients, although theirefficacy in women with peritoneal carcinomatosis has beenquestioned [4]. Intraperitoneal administration of Interferon-alpha 2b has been attempted by a series of authors withcomplete response rates ranging from 10% to 30% [5–7].This treatment requires frequent repeated administrations [7]and is associated with nausea, dyspepsia, abdominal disten-sion and flu like symptoms. Intraperitoneal chemotherapyhas been used for the treatment of malignant ascites andrecent randomized studies have demonstrated its superiorityin terms of survival to conventional intravenous administra-tion as primary treatment of ovarian cancer [8]. This
Condensation Intraperitoneal Bevacizumab induces an immuneactivation and is highly effective in the treatment of refractorymalignant ascites in ovarian cancer.
Filippo Bellati and Chiara Napoletano have contributed equally to thiswork.
F. Bellati :M. Pastore :M. Pernice :M. Antonilli :P. Benedetti PaniciInstitute of Gynecology and Obstetrics, Sapienza University,Rome, Italy
F. Bellati : C. Napoletano : I. Ruscito :M. NutiDepartment of Experimental Medicine, Sapienza University,Rome, Italy
F. Bellati (*)Department of Gynecology and Obstetrics,University of Rome Sapienza,viale del Policlinico,Rome 155-00161, Italye-mail: [email protected]
Invest New Drugs (2010) 28:887–894DOI 10.1007/s10637-009-9351-4

therapeutic strategy yields its best results in patients in whomtumor has shown to be responsive to earlier systemictherapies [9] and nodules have greatest size inferior to 1 cm.
Bevacizumab is a dimeric monoclonal antibody directedagainst Vascular Endothelial Growth Factor (VEGF), current-ly under evaluation in ovarian cancer by several internationalgynecologic oncology groups. Intravenous administration hasbeen shown to induce chylous ascites in some patients,although the precise mechanism that justifies this side effectremains unknown [10]. Some authors have reported a highefficacy of intraperitoneal bevacizumab for the treatment ofmalignant ascites [11, 12]. We report the third case of aplatinum refractory ovarian cancer patient, who experienceda complete resolution of malignant ascites, after intraperito-neal administration of bevacizumab. Since recent evidencehas demonstrated that the therapeutic effect of oncologytreatments can be greatly ascribed to an immune activation[13, 14], we also describe the immunological changes inducedby this monoclonal antibody. A review of the literature aboutthe role of bevacizumab in ovarian cancer is presented.
Patient’s history
In 2005, after two years of negative follow up, a 55 years oldwomen with a history of stage IIIC serous G3 ovarian cancercame at our institution with CA125 of 234 UI/mL and a CTscan showing a single hepatic recurrence. The patient had beenpreviously treated with primary cytoreduction with no residualdisease and adjuvant carboplatin and paclitaxel. She wassubjected to a diagnostic laparoscopy which confirmed thesuperficial hepatic lesion, but showed carcinomatosis notamenable of optimal debulking. Consequently, she wasaddressed to six cycles of platinum and taxane chemotherapy.At the end of treatment, the patient showed a complete clinicalresponse, but 5 months later CA125 increased again. Sheunderwent six subsequent cycles of III line chemotherapy withdoxil, which was successively switched to topotecan fordisease progression. After the third cycles of the lattertreatment, she started complaining abdominal distension anddyspnea. Trans-abdominal ultrasound showed ascites anddifferent abdomino-pelvic lesions. A paracentesis was carriedout removing 5 litres. It was decided to attempt palliative careof ascites with the administration of intraperitoneal cisplatin75 mg/mq. The patient benefited from a 3-week period withoutascites, after which she complained abdominal bloating.Treatment with intraperitoneal cisplatin was repeated afterascites removal for six cycles and additional paracentesis werecarried in between cycles on patient’s need. At the end of thesixth cycle, she started complaining weekly severe abdominalbloating, with partial gastrointestinal occlusion and dyspnea,which rapidly improved after peritoneal drainage. Each para-centesis removed between 3 and 5 litres of volume.
After a careful counselling and patient’s refusal ofintraperitoneal indwelling catheter, it was decided to begintreatment with intraperitoneal bevacizumab at 5 mg/kg everythree weeks [12]. The patient was subjected to paracentesiswith removal of 5 litres of ascites and intraperitonealinfusion of bevacizumab diluted in 250 ml of saline solution.After the first administration, she benefited from a generalclinical improvement without any complaint or side effect.Treatment was repeated four times with the patient reportinga highly improved quality of life. Throughout treatmentCA125 levels remained high showing a stable disease [15],but she deceased before the fifth administration. The familyreported that, for a few days before exitus, the patient hadsuffered from a progressive loss of appetite and fatigue. Thepatient’s family informed us that she had died during thenight for respiratory failure.
Immunological changes during intraperitonealbevacizumab
In order to evaluate if the beneficial effects of bevacizumabcould be partially ascribed to an immune effect, changes inthe different lymphocyte subsets were analyzed in periph-eral blood and ascite before treatment (time 0) and only inperipheral blood after 21 days before three successiveadministrations (time 1, time 2 and time 3).
Due to the complete remission of the peritoneal effusion,a more accurate analysis of the local effect of bevacizumabwas not possible.
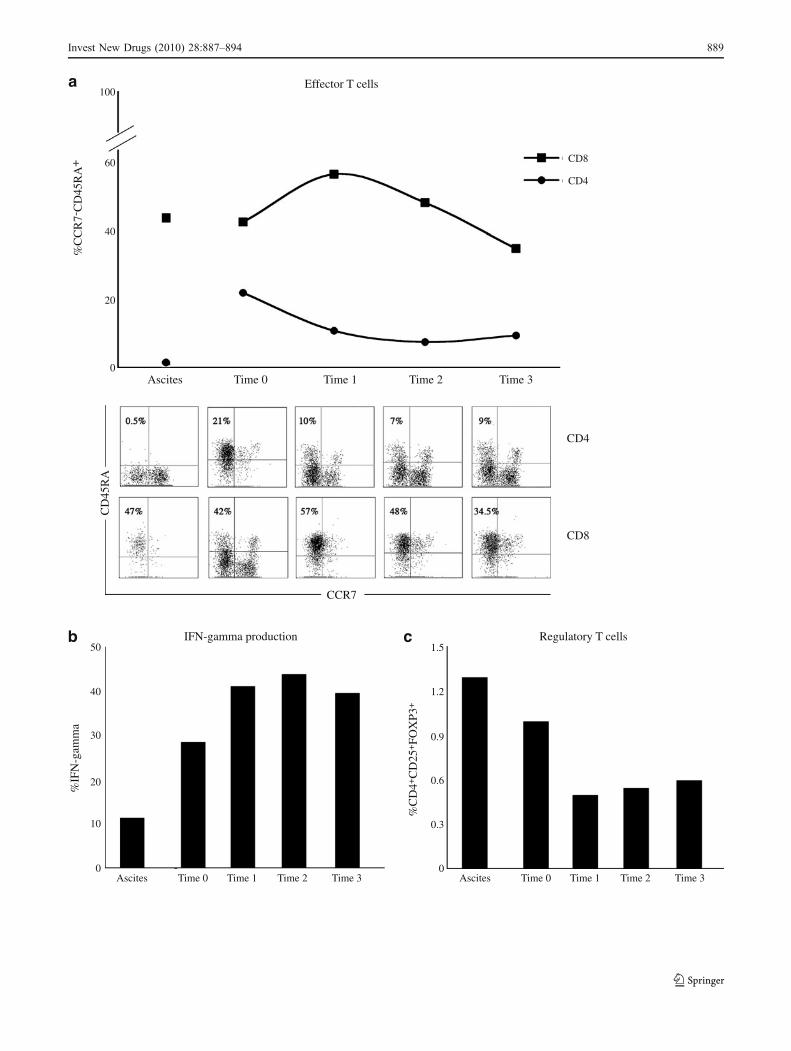
CD4+ and CD8+ lymphocyte subsets were analyzed bycytofluorimetry for the expression of CD45RA and CCR7markers. The percentage of CD8+ effector T cells(CD45RA+CCR7-) in peripheral blood and ascites wascomparable at time 0. In peripheral blood, the firstadministration of bevacizumab increased the amount ofCD8+ effector cells from 42% (time 0) to 57% (time 1), butthis effect did not persist in successive administrations (time2: 48%, time 3: 34,5%). Different results were obtained in theCD4+ effector T cells. The percentage of CD4+ effectorlymphocytes in peripheral blood was 21%, while in asciteswas 0,5% at time 0. Drug administrations reduced the amountof CD4+ effector T cells from 21% to 9% at time 3 (Fig. 1a).
Fig. 1 Lymphocyte subset and IFNγ production analyses. Panel ashows the percentage of CD4 and CD8 effector T cells in ascites andblood reported as CCR7-CD45RA+ cells (at the top) and thecytofluorimetric analysis of CD45RA and CCR7 in CD4 and CD8 Tcells (below). Panel b represents the intracellular staining of IFNγproduced by T cells purified from ascites and peripheral blood after theaddition of PMA and Ionomycin. Results are reported as percentage ofIFNγ. Panel c depicts the percentage of Treg cells isolated from ascitesand peripheral blood of at different time points. Treg cells were markedusing anti-CD4, anti-CD25 and anti-FOXP3 antibodies
�
888 Invest New Drugs (2010) 28:887–894
100
60
40
20
0
%C
CR
7-C
D45
RA
+ CD8
CD4
Ascites Time 0 Time 1 Time 2 Time 3
CD4
CD8
CD
45R
A
CCR7
Effector T cells
50
40
30
20
10
0
1.2
1.5
0.9
0.6
0.3
0Ascites Time 0 Time 1 Time 2 Time 3 Ascites Time 0 Time 1 Time 2 Time 3
%IF
N-g
amm
a
%C
D4+
CD
25+FO
XP3
+
IFN-gamma production Regulatory T cells
a
b c
Invest New Drugs (2010) 28:887–894 889
In order to study the lymphocyte polarization (TH1, TH2,TH17), T cells were stimulated with PMA (25 ng/ml) andIonomycin (250 ng/ml) in presence of Brefeldin (10 μg/ml)for 16 hours and the release of IFNγ, IL-4 and IL-17 wasanalyzed by cytofluorimetry. Results showed a prevalenceof IFNγ producing cells in both blood and ascites. Inparticular, the amount of IFNγ in the blood was 28,7% attime 0, while in ascites was 11,3%. The percentage of thiscytokine increased after the first dose of bevacizumab(41,5%) and remained stable during the other administra-tions (time 2: 42%, time 3: 40%) (Fig. 1b). IL-4 was notproduced, while IL-17 was present only in ascites (3,3%).
Regulatory T cells (Treg) (CD4+CD25+FOXP3+) werealso analyzed in blood and ascites. The level of thislymphocyte subset was similar in peripheral blood andascites at time 0. Bevacizumab decreased the percentage ofcirculating Treg cells from 1% (time 0) to 0,5% (time 1).This reduction remained stable after each administration(Fig. 1c).
Finally, the levels of NK (CD3-CD16+CD56+) and NKT(CD3+CD16+CD56+) cells were analyzed. The amount of
NK and NKT cells in peripheral blood was highercompared to that analyzed in the ascites (NK: blood 18%vs ascites 6,3%; NKT: blood 22% vs ascites 3,1%). Thepercentage of these two populations did not change duringtreatment.
Comment
Ascites represents a major issue in patients affected byrecurrent ovarian cancer. Ascites has an important effect onwomen’s quality of life [16] and survival [17]. The directcorrelation between the presence of ascites and advancedand/or disseminated intraperitoneal disease can partiallyjustify the dismal prognosis observed in these patients,although ascites itself could play a direct role on the historyof the disease. Ascites contains elevated concentration ofseveral growth factors and immunosuppressive cytokines,such as VEGF, IL-10 and TNFα [18, 19]. The feeling ofmechanical distension and abdominal bloating reducesappetite and can cause partial bowel obstruction. On the
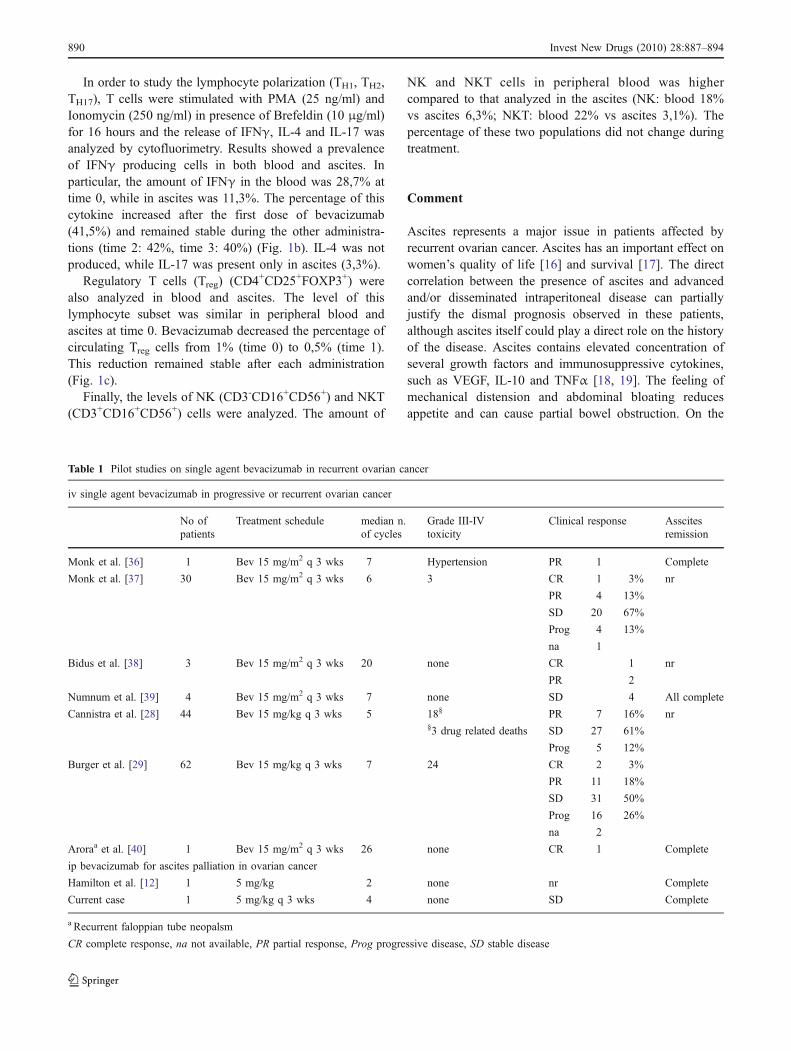
Table 1 Pilot studies on single agent bevacizumab in recurrent ovarian cancer
iv single agent bevacizumab in progressive or recurrent ovarian cancer
No ofpatients
Treatment schedule median n.of cycles
Grade III-IVtoxicity
Clinical response Asscitesremission
Monk et al. [36] 1 Bev 15 mg/m2 q 3 wks 7 Hypertension PR 1 Complete
Monk et al. [37] 30 Bev 15 mg/m2 q 3 wks 6 3 CR 1 3% nr
PR 4 13%
SD 20 67%
Prog 4 13%
na 1
Bidus et al. [38] 3 Bev 15 mg/m2 q 3 wks 20 none CR 1 nr
PR 2
Numnum et al. [39] 4 Bev 15 mg/m2 q 3 wks 7 none SD 4 All complete
Cannistra et al. [28] 44 Bev 15 mg/kg q 3 wks 5 18§ PR 7 16% nr§3 drug related deaths SD 27 61%
Prog 5 12%
Burger et al. [29] 62 Bev 15 mg/kg q 3 wks 7 24 CR 2 3%
PR 11 18%
SD 31 50%
Prog 16 26%
na 2
Aroraa et al. [40] 1 Bev 15 mg/m2 q 3 wks 26 none CR 1 Complete
ip bevacizumab for ascites palliation in ovarian cancer
Hamilton et al. [12] 1 5 mg/kg 2 none nr Complete
Current case 1 5 mg/kg q 3 wks 4 none SD Complete
a Recurrent faloppian tube neopalsm
CR complete response, na not available, PR partial response, Prog progressive disease, SD stable disease
890 Invest New Drugs (2010) 28:887–894
Tab
le2
Pilo
tstud
ieson
combinatio
ntreatm
entswith
bevacizumab
inov
ariancancer
Com
binatio
ntherapieswith
bevacizumab
inprogressiveor
recurrentovariancancer
Noof
patients
Treatmentschedule
Mediann.
ofcycles
Grade
III–IV
toxicity
Clin
ical
response
Ascitesremission
Monket
al.[37a]
2Bev
15mg/m
2q3wks
+5F
U/leu+Oxal
orBev
15mg/m
2q3wks
+Cyclo
6none
Prog
2nr
Cohnet
al.[31]
10Bev
10mg/kg
q2wks
+Taxane
40–7
0mg/m
2p1q7
4none
PR
889%
2Cr
SD
111%
2Pr
na1
Wrightet
al.[41]
23Bev
5mg/kg
q1or
2wks
with
Cyclo
15(65%
)7
11§
PR
835%
nr
5FU
6(26%
)§2drug
relateddeaths
dueto
bowel
perforation
SD
1044%
Gem
+Doxil
1(4%)
Prog
522%
Doce
1(4%)
Kesterson
etal.[42]
1Bev
15mg/kg
q3wks
+paclitaxel
80mg/m
2plq7
8none
CR
1Cr
Garciaet
al.[32]
70Bev
10mg/kg
q2wks
+Cyclo
50mg/day
583
PR
1724%
nr
SD
4463%
Prog
913%
Azadet
al.[34]
13Bev
5–10
mg/kg
q3wks
+Sorafenib
200mgtwicedaily
4ç2
PR
646%
nr
SD
754%
Nim
eiriet
al.[35]
13Bev
15mg/kg
q3wks
+Erlotinib
150mg/day
610
§CR
17%
nr
PR
17%
§2drug
relateddeaths
dueto
bowel
perforation
SD
754%
Prog
43%
Schultheiset
al.[33]
70Bev
10mg/kg
q1or
2wks
+Cyclo
50mg/day
nrnr
PR
12175
nr
SD
3347%
Prog
812%
na17
Com
binatio
ntherapieswith
bevacizumab
inprim
aryovariancancer
Micha
etal.[43]
20prim
ary
neoplasm
Bev
15mg/kg
q3wks
+paclitaxel
175mg/m
2+carboplatin
(AUC=5)
plq21
618
neutopenia
CR
633%
nr
2hypetension
PR
1055%
1Neurologicaltoxicity
SD
16%
nr2
astud
yalso
includ
edpatientssubjectedto
bevacizumab
sing
leagentfollo
wed
bytheotherdrug
sin
combinatio
n.These
patientshave
been
dscribed
inTable
1bRecurrent
fallo
pian
tube
neop
lasm
Bev
Bevacizum
ab,CRcompleterespon
se,Cyclo
Cycloph
osph
amide,DoceDocetaxel,5FU
5-fluo
rouracil,
Gem
gemcitabine,Leu
lecovo
rin,
nano
tavailable,nr
notrepo
rted,OxalOxalip
latin
e,PRparial
respon
se,Progprog
ressivedisease,
SDstable
disease
Invest New Drugs (2010) 28:887–894 891

other hand, ascites contains high concentrations of nutrientsuch as proteins [20], fat-soluble vitamins and carotenoids[21], which are lost during paracentesis or permanentdrainage thereby contributing to cachexia.
Neoplastic ascites contains, in addition to malignantcells, a great variety of immune cells including NK,Cytotoxic T Lymphocytes (CTL) and regulatory T cells,which are selectively recruited in the peritoneal cavity [22].
Intraperitoneal administration of monoclonal antibodieshas not yet been thoroughly investigated, but preliminarystudies have mostly given promising results. Excludingintraperitoneal radioimmunotherapy [23], some clinicalstudies have been conducted on trifunctional antibodies.Catumaxomab, a rat/murine hybrid, trifunctional, bispecificantibody (anti-epithelial cell adhesion molecule, anti-EpCAM, and anti-CD3) has been adopted for the treatmentof ascites. Intraperitoneal catumaxomab has a systemic effecton tumor cells [24] and enhances antitumor immunity [25].
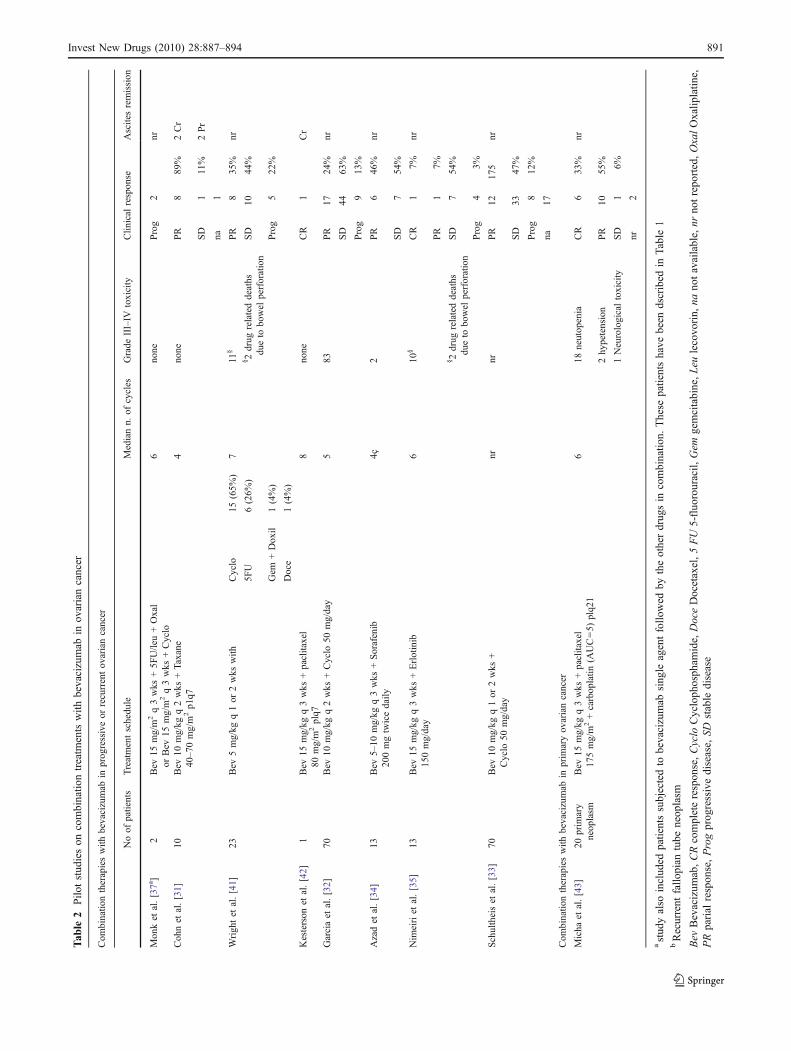
Bevacizumab has given important results in colorectalcancer [26, 27] and is currently under thorough investiga-tion in women affected by ovarian neoplasms. In patientswith platinum resistant chemotherapy, who had failed atleast two lines of chemotherapy, iv bevacizumab as singleagent achieved response rates ranging from 16% to 21%[28, 29]. In an important study in mice models, bevacizu-mab showed to have a strong synergic effect with cisplatin,possibly due to a re-establishment of sensitivity to platinumagents [30]. Higher response rates were observed incombination regimens with metronomic administration oftraditional drugs [31–33] and novel target therapies [34, 35],but frequent severe side effects including bowel perforation,hypertension and fatigue [28, 29] have been reported. TheMedical Research Council has recently launched a largephase III trial with the objective of evaluating the possibleaddition of bevacizumab to standard first line chemotherapy(NCT00483782). A review of available data and ongoing
phase III randomized trials on bevacizumab in ovariancancer patients are shown in Tables 1, 2 and 3.
The primary intention of blocking VEGF is to inhibittumour vasculogenesis [44, 45] although new mechanismthrough which this cytokine can favour cancer progressionare being found. Recently, it has been shown that VEGF isable to induce a immunosuppressive milieu. It has beendemonstrated that VEGF interferes with dendritic cellsmaturation [46] and can induce and/or maintain Tregs incancer patients [47, 48].
Intraperitoneal therapy with bevacizumab has been recent-ly suggested as treatment of malignant ascites [11, 12].El-Shami et al. [11] reported nine patients, one affected byovarian cancer, in whom ascites resolved with low dosebevacizumab administered monthly. Accurate data regardingthis initial experience are currently unavailable. Hamiltonet al. [12], reported a case of an elderly patient with platinumrefractory ovarian cancer who refused surgery, second linetherapy and consequently addressed to palliative care. After athree month interval, the patient suffered from ascites andlower limbs edema which rapidly recurred after an initialparacentesis. Treatment with bevacizumab 5 mg/kg repeatedafter 24 days was able to resolve ascites and correlatedsymptoms and the patient deceased peacefully in her sleep. Itis unknown if traditional second line cytotoxic drugs couldhave achieved a palliative beneficial effect.
In this case, the patient had been subjected to multiple linesof chemotherapy including rechallenging with platinumregimens, pegilated liposomal doxorubicin and topotecan.Furthermore, attempts of palliation with intraperitonealcisplatin had been carried out. After paracentesis and a singleadministration of intraperitoneal low dose bevacizumab, thepatient benefited from a complete resolution of ascites andcorrelated symptoms. The patient referred a great improvementin her quality of life. This clinical and symptomatic improve-ment supported our decision to continue treatment for
Table 3 Ongoing phase III randomized trials
Sponsor and collaborators Protocol ID Treatment N. ofpatients
FIGO disease stage Estimated dateof closureStudy chair
Gynecologic oncology group NCT00262847 Bev iv Carboplatin iv + Paclitaxel iv 2000 Stage III–IV ClosedBurger RA
Genetech NCT00434642 Bev iv Carboplatin + Gemcitabine 450 Platinum sensitiverecurrence
June 2010Hua M.
Gynecologic oncology group NCT00565851 Bev iv Carboplatin + Taxane 660 Platinum sensitiverecurrence
December 2009Coleman RL.
Medical research council NCT00483782 Bev iv Carboplatin + Paclitaxane 1,520 Stage I–IV na
Gynecologic oncology group NCT00951496 Bev iv + Paclitaxel iv (paclitaxel ip,Carboplatin iv or ip, Cispatin ip.)
1,100 Stage II–III January 2016Walker JL
Bev Bevacizumab, ip intraperitoneal, iv intravenous, na not applicable
Data collected from NCI (cancer.gov, August 2009)
892 Invest New Drugs (2010) 28:887–894

successive cycles. The patient deceased at home in the absenceof pain, several weeks after the last drug administration forrespiratory arrest. This time interval between the last drugadministration and death makes the hypothesis of a iatrogenicside effect extremely unlikely. The extent of the disease and thecompromised clinical conditions of the patient before thebeginning of treatment makes any conclusion on an effect onthe history of the disease speculative.
Recent findings have shown that treatment with bev-acizumab is associated with a reduction in VEGF levels,but this change does not correlate with clinical outcome[32]. In this patient, we investigated the role that ipbevacizumab had on the immune system. It is not possibleto draw conclusions on a single case, but some preliminaryobservations can be drawn. Studies on other monoclonalantibodies adopted in oncology have shown that theimmune system gives a crucial contribution to the anti-tumour effects [49]. Circulating lymphocytes were able tosecrete IFNγ in a higher proportion as compared tolymphocytes recruited in ascitic fluid. In peripheral blood,this capability increased and remained high during treat-ment with bevacizumab. Ip bevacizumab temporarilyincreased effector CD8+ cells, whereas CD4+ effector cellsremained low. In vivo, CD4+ effector cells are pivotal formaintaining an adequate number and function of cytotoxicT lymphocytes by cytokine secretion. Circulating Tregshalfened after drug administration and remained low. NKand NKT proportion were not influenced by the ipadministration of bevacizumab. Overall, the early cellularchanges show the beginning of an activation of the immunesystem. This positive initial effect gradually aborted withtreatment continuation. Possible explanations could be animmunological impairment due to several previous lines ofchemotherapy and the high tumor burden or alternativelythe induction of human anti-mouse antibodies. Futurebiological studies on larger number of patients will benecessary to confirm these immunological observations andbetter understand the complex mechanism that underlaysthe therapeutic effect of bevacizumab. Analyses on lessheavily pre-treated women will show if bevacizumab isable to induce a more prolonged immune activation.
In conclusion, although only few cases have beenreported, the exceptional results and the complete absenceof side effects observed in this and other reported casesstrongly warrant future trials to investigate the role thatintraperitoneal bevacizumab can have both as palliativetreatment of refractory ascites and as salvage therapy inovarian cancer.
Acknowledgements This work was supported by AssociazioneItaliana Ricerca contro il Cancro, Ministero della Salute/RegioneLazio, Ministero dell’Istruzione dell’Università e della Ricerca. ChiaraNapoletano was supported by Associazione Italiana Ricerca contro ilCancro.
References
1. Jemal A, Siegel R, Ward E et al (2008) Cancer statistics, 2008.CA Cancer J Clin 58:71–96
2. Herrinton LJ, Neslund-Dudas C, Rolnick SJ et al (2007)Complications at the end of life in ovarian cancer. J PainSymptom Manage 34:237–43
3. Ayantunde AA, Parsons SL (2007) Pattern and prognostic factorsin patients with malignant ascites: a retrospective study. AnnOncol 18:945–49
4. Pockros PJ, Esrason KT, Nguyen C, Duque J, Woods S(1992) Mobilization of malignant ascites with diuretics isdependent on ascitic fluid characteristics. Gastroenterology103:1302–06
5. Bezwoda WR, Seymour L, Dansey R (1989) Intraperitonealrecombinant interferon-alpha 2b for recurrent malignant ascitesdue to ovarian cancer. Cancer 64:1029–33
6. Stuart GC, Nation JG, Snider DD, Thunberg P (1993) Intraper-itoneal interferon in the management of malignant ascites. Cancer71:2027–30
7. Sartori S, Nielsen I, Tassinari D, Trevisani L, Abbasciano V,Malacarne P (2001) Evaluation of a standardized protocol ofintracavitary recombinant interferon alpha-2b in the palliativetreatment of malignant peritoneal effusions. A prospective pilotstudy. Oncology 61:192–6
8. Armstrong DK, Bundy B, Wenzel L et al (2006) Intraperitonealcisplatin and paclitaxel in ovarian cancer. N Engl J Med 354:34–43
9. Adam RA, Adam YG (2004) Malignant ascites: past, present, andfuture. J Am Coll Surg 198:999–1011
10. Wright JD, Secord AA, Numnum TM et al (2008) A multi-institutional evaluation of factors predictive of toxicity andefficacy of bevacizumab for recurrent ovarian cancer. Int JGynecol Cancer 18:400–6
11. El-Shami K, Elsaid A, El-Kerm A (2007) Open-label safety andefficacy pilot trial of intraperitoneal bevacizumab as palliativetreatment in refractory malignant ascites. J Clin Oncol 25:9043(ASCO Meeting Abstracts)
12. Hamilton CA, Maxwell GL, Chernofsky MR, Bernstein SA,Farley JH, Rose GS (2008) Intraperitoneal bevacizumab for thepalliation of malignant ascites in refractory ovarian cancer.Gynecol Oncol 111:530–32
13. Zitvogel L, Apetoh L, Ghiringhelli F, Kroemer G (2008)Immunological aspects of cancer chemotherapy. Nat Rev Immu-nol 8:59–73
14. Bellati F, Visconti V, Napoletano C et al (2009) Immunology ofgynecologic neoplasm: analysis of the prognostic significance ofthe immune status. Curr Cancer Drug Targets 9:541–65
15. Rustin GJS, Quinn M, Thigpen T et al (2004) Re: New Guidelinesto Evaluate the Response to Treatment in Solid Tumors (OvarianCancer). J Natl Cancer Inst 96:487–488
16. Rosenberg SM (2006) Palliation of malignant ascites. Gastro-enterol Clin North Am 35:189–99
17. Berek JS, Hacker NF, Lagasse LD, Nieberg RK, Elashoff RM(1983) Survival of patients following secondary cytoreductivesurgery in ovarian cancer. Obstet Gynecol 61:189–93
18. Curiel TJ, Coukos G, Zou L et al (2004) Specific recruitment ofregulatory T cells in ovarian carcinoma fosters immune privilegeand predicts reduced survival. Nat Med 10:942–49
19. Bamias A, Koutsoukou V, Terpos E et al (2008) Correlation ofNK T-like CD3 + CD56+ cells and CD4 + CD25 + (hi) regulatoryT cells with VEGF and TNFalpha in ascites from advancedovarian cancer: Association with platinum resistance and progno-sis in patients receiving first-line, platinum-based chemotherapy.Gynecol Oncol 108:421–27
Invest New Drugs (2010) 28:887–894 893
20. Tamsma JT, Keizer HJ, Meinders AE (2001) Pathogenesis ofmalignant ascites: Starling's law of capillary hemodynamicsrevisited. Ann Oncol 12:1353–57
21. Schweigert FJ, Raila J, Sehouli J, Buscher U (2004) Accumulationof selected carotenoids, alpha-tocopherol and retinol in humanovarian carcinoma ascitic fluid. Ann Nutr Metab 48:241–45
22. Bamias A, Tsiatas ML, Kafantari E et al (2007) Significantdifferences of lymphocytes isolated from ascites of patients withovarian cancer compared to blood and tumor lymphocytes.Association of CD3 + CD56+ cells with platinum resistance.Gynecol Oncol 106:75–81
23. Meredith RF, Buchsbaum DJ, Alvarez RD, LoBuglio AF (2007)Brief overview of preclinical and clinical studies in the develop-ment of intraperitoneal radioimmunotherapy for ovarian cancer.Clin Cancer Res 13:5643s–5645s
24. Wimberger P, HeubnerM, Lindhofer H, JägerM, Kimmig R, Kasimir-Bauer S (2009) Influence of catumaxomab on tumor cells in bonemarrow and blood in ovarian cancer. Anticancer Res 29:1787–91
25. Ströhlein MA, Siegel R, Jäger M, Lindhofer H, Jauch KW, HeissMM (2009) Induction of anti-tumor immunity by trifunctionalantibodies in patients with peritoneal carcinomatosis. J Exp ClinCancer Res 28:18
26. Grothey A, Sugrue MM, Purdie DM et al (2008) Bevacizumabbeyond first progression is associated with prolonged overallsurvival in metastatic colorectal cancer: results from a largeobservational cohort study (BRiTE). J Clin Oncol 26:5326–34
27. Wagner AD, Arnold D, Grothey AA, Haerting J, Unverzagt S(2009) Anti-angiogenic therapies for metastatic colorectal cancer.Cochrane Database Syst Rev. CD005392.
28. Cannistra SA, Matulonis UA, Penson RT et al (2007) Phase IIstudy of bevacizumab in patients with platinum-resistant ovariancancer or peritoneal serous cancer. J Clin Oncol 25:5180–86
29. Burger RA, Sill MW, Monk BJ, Greer BE, Sorosky JI (2007)Phase II trial of bevacizumab in persistent or recurrent epithelialovarian cancer or primary peritoneal cancer: a gynecologiconcology group study. J Clin Oncol 25:5165–71
30. Mabuchi S, Terai Y, Morishige K et al (2008) Maintenancetreatment with bevacizumab prolongs survival in an in vivoovarian cancer model. Clin Cancer Res 14:7781–89
31. Cohn DE, Valmadre S, Resnick KE, Eaton LA, Copeland LJ,Fowler JM (2006) Bevacizumab and weekly taxane chemotherapydemonstrates activity in refractory ovarian cancer. Gynecol Oncol102:134–9
32. Garcia AA, Hirte H, Fleming G et al (2008) Phase II clinical trialof bevacizumab and low-dose metronomic oral cyclophosphamidein recurrent ovarian cancer: a trial of the California, Chicago, andPrincess Margaret Hospital phase II consortia. J Clin Oncol26:76–82
33. Schultheis AM, Lurje G, Rhodes KE et al (2008) Polymorphismsand clinical outcome in recurrent ovarian cancer treated withcyclophosphamide and bevacizumab. Clin Cancer Res 14:7554–63
34. Azad NS, Posadas EM, Kwitkowski VE et al (2008) Combinationtargeted therapy with sorafenib and bevacizumab results inenhanced toxicity and antitumor activity. J Clin Oncol 26:3709–14
35. Nimeiri HS, Oza AM, Morgan RJ et al (2008) Efficacy and safetyof bevacizumab plus erlotinib for patients with recurrent ovarian,primary peritoneal, and fallopian tube cancer: a trial of theChicago, PMH, and California Phase II Consortia. Gynecol Oncol110:49–55
36. Monk BJ, Choi DC, Pugmire G, Burger RA (2005) Activity ofbevacizumab (rhuMAB VEGF) in advanced refractory epithelialovarian cancer. Gynecol Oncol 96:902–5
37. Monk BJ, Han E, Josephs-Cowan CA, Pugmire G, Burger RA(2006) Salvage bevacizumab (rhuMAB VEGF)-based therapyafter multiple prior cytotoxic regimens in advanced refractoryepithelial ovarian cancer. Gynecol Oncol 102:140–4
38. Bidus MA, Webb JC, Seidman JD, Rose GS, Boice CR, Elkas JC(2006) Sustained response to bevacizumab in refractory well-differentiated ovarian neoplasms. Gynecol Oncol 102:5–7
39. Numnum TM, Rocconi RP, Whitworth J, Barnes MN (2006) Theuse of bevacizumab to palliate symptomatic ascites in patientswith refractory ovarian carcinoma. Gynecol Oncol 102:425–8
40. Arora N, Tewari D, Cowan C, Saffari B, Monk BJ, Burger RA(2008) Bevacizumab demonstrates activity in advanced refractoryfallopian tube carcinoma. Int J Gynecol Cancer 18:369–72
41. Wright JD, Viviano D, Powell MA et al (2006) Bevacizumabcombination therapy in heavily pretreated, recurrent cervicalcancer. Gynecol Oncol 103:489–93
42. Kesterson JP, Mhawech-Fauceglia P, Lele S (2008) The use ofbevacizumab in refractory ovarian granulosa-cell carcinoma withsymptomatic relief of ascites: a case report. Gynecol Oncol111:527–29
43. Micha JP, Goldstein BH, Rettenmaier MA et al (2007) A phase IIstudy of outpatient first-line paclitaxel, carboplatin and bevacizu-mab for advanced-stage epithelial ovarian, peritoneal, andfallopian tube cancer. Int J Gynecol Cancer 17:771–76
44. Presta LG, Chen H, O’Connor SJ et al (1997) Humanization of ananti-vascular endothelial growth factor monoclonal antibody forthe therapy of solid tumors and other disorders. Cancer Res57:4593–99
45. Ferrara N, Hillan KJ, Novotny W (2005) Bevacizumab (Avastin),a humanized anti-VEGF monoclonal antibody for cancer therapy.Biochem Biophys Res Commun 333:328–35
46. Alfaro C, Suarez N, Gonzalez A et al (2009) Influence ofbevacizumab, sunitinib and sorafenib as single agents or incombination on the inhibitory effects of VEGF on humandendritic cell differentiation from monocytes. Br J Cancer100:1111–19
47. Osada T, Chong G, Tansik R et al (2008) The effect of anti-VEGFtherapy on immature myeloid cell and dendritic cells in cancerpatients. Cancer Immunol Immunother 57:1115–24
48. Wada J, Suzuki H, Fuchino R et al (2009) The contribution ofvascular endothelial growth factor to the induction of regulatoryT-cells in malignant effusions. Anticancer Res 29:881–8
49. Kute TE, Savage L, Stehle JR Jr et al (2009) Breast tumor cellsisolated from in vitro resistance to trastuzumab remain sensitive totrastuzumab anti-tumor effects in vivo and to ADCC killing.Cancer Immunol Immunother 58:1889–98
894 Invest New Drugs (2010) 28:887–894