complete dentures 3.history and exam
TRANSCRIPT
3. History and Exam
John Beumer III, DDS, MSand
Robert Duell, DDSDivision of Advanced Prosthodontics, Biomaterials and Hospital Dentistry
UCLA School of Dentistry
This program of instruction is protected by copyright ©. No portion of this program of instruction may be reproduced, recorded or transferred by any means electronic, digital, photographic, mechanical etc., or by any information storage or retrieval system, without prior permission.
• Medical and dental history• Orofacial exam• Prosthodontic assessment• Prognosis• Preliminary impressions• Tissue conditioning
History and Clinical Exam
Medical HistoryPotential medical emergenciesEffects on denture supporting
tissuesEffects on oral neuromuscular
control
Effects of Smoking
Predisposition to oral cancer
Predisposition to periodontal disease
Success – failure rates of osseointegrated implants
Oral Facial Exam:
Oral cancer screening exam
Exam for other pathology Local
Systemic
Prosthodontic assessment
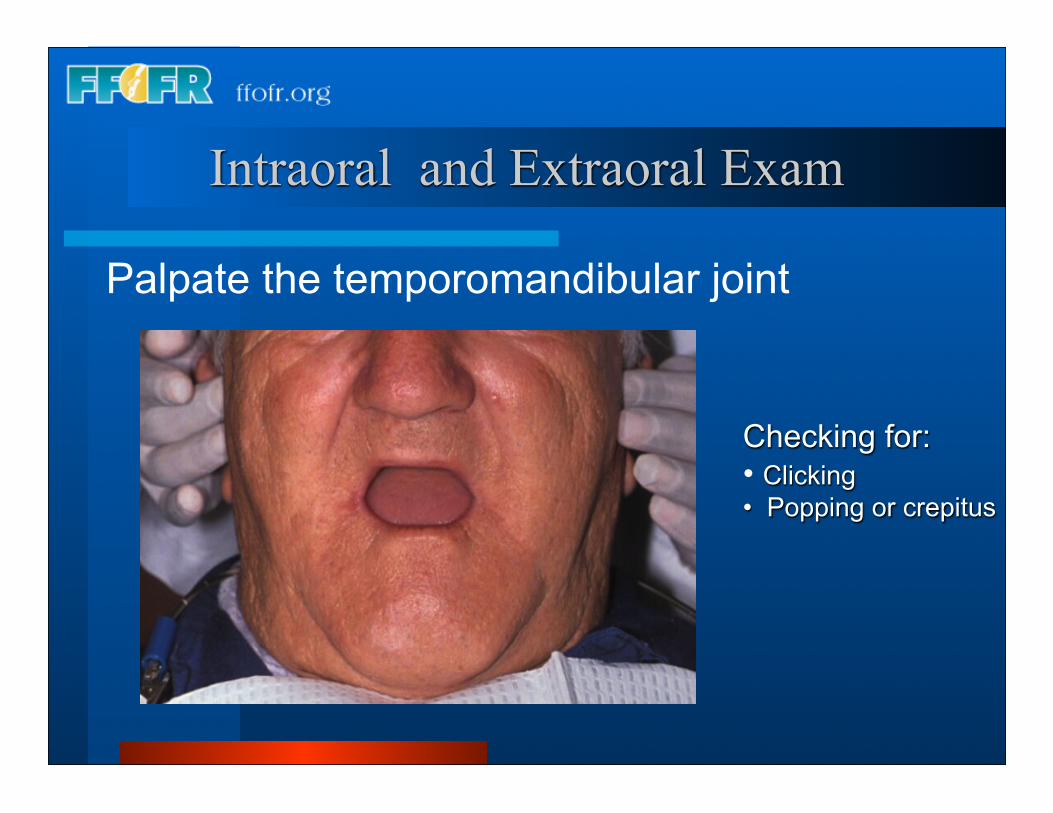
Intraoral and Extraoral Exam
Checking for:• Clicking• Popping or crepitus
Palpate the temporomandibular joint
Conduct a thorough oral cancer screening exam
• Lips and cheeks•Lateral border of the tongue•Floor of the mouth•Tonsillar region and the soft palate•Base of the tongue •Oropharynx•Neck
Intraoral and Extra Oral Exam
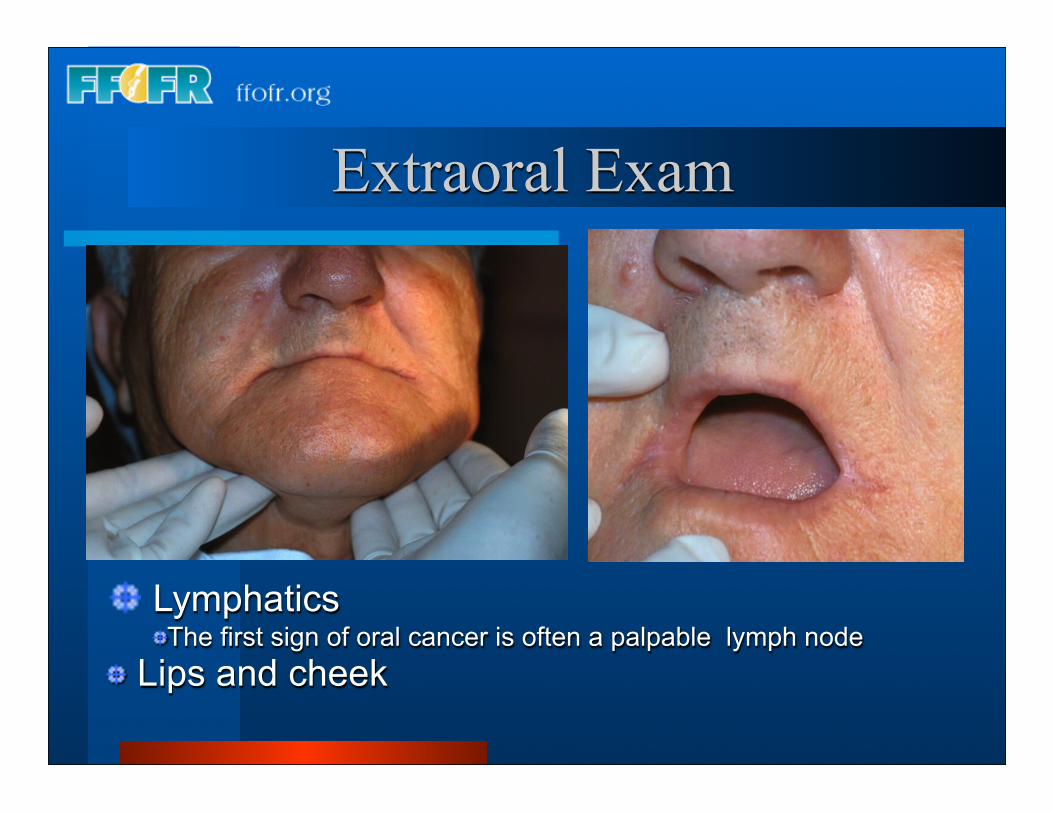
Extraoral Exam
LymphaticsThe first sign of oral cancer is often a palpable lymph node
Lips and cheek
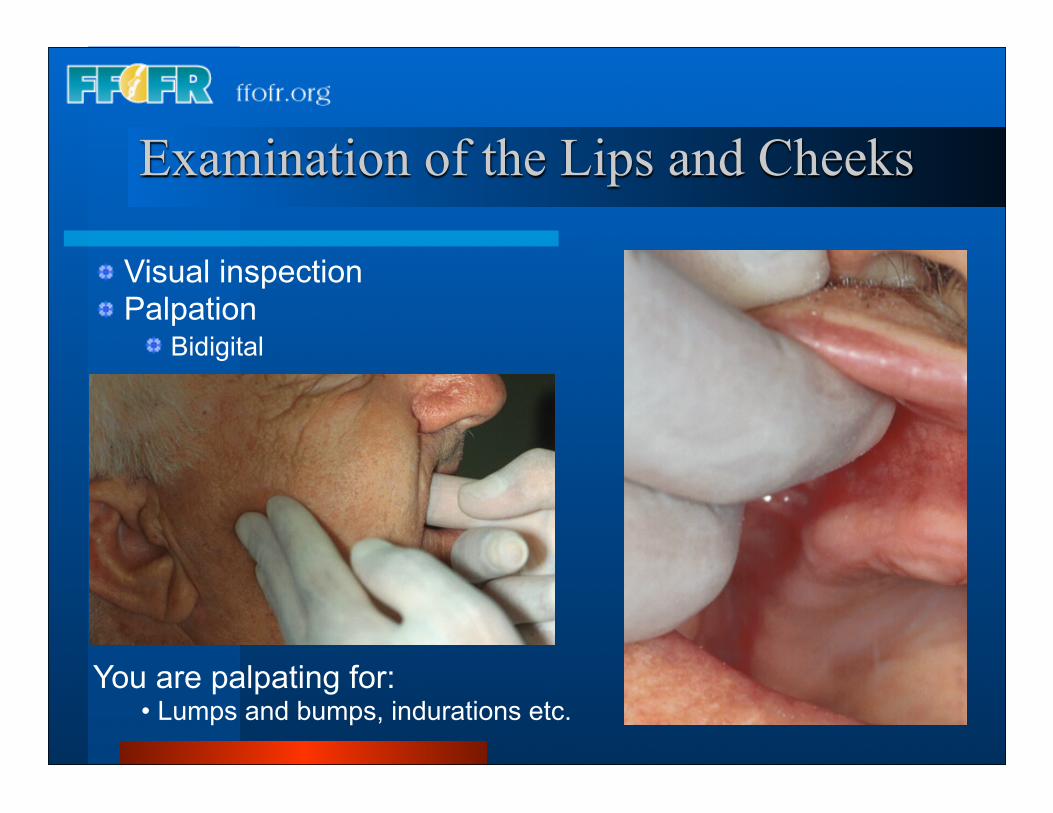
Examination of the Lips and Cheeks
Visual inspection Palpation
Bidigital
You are palpating for:• Lumps and bumps, indurations etc.
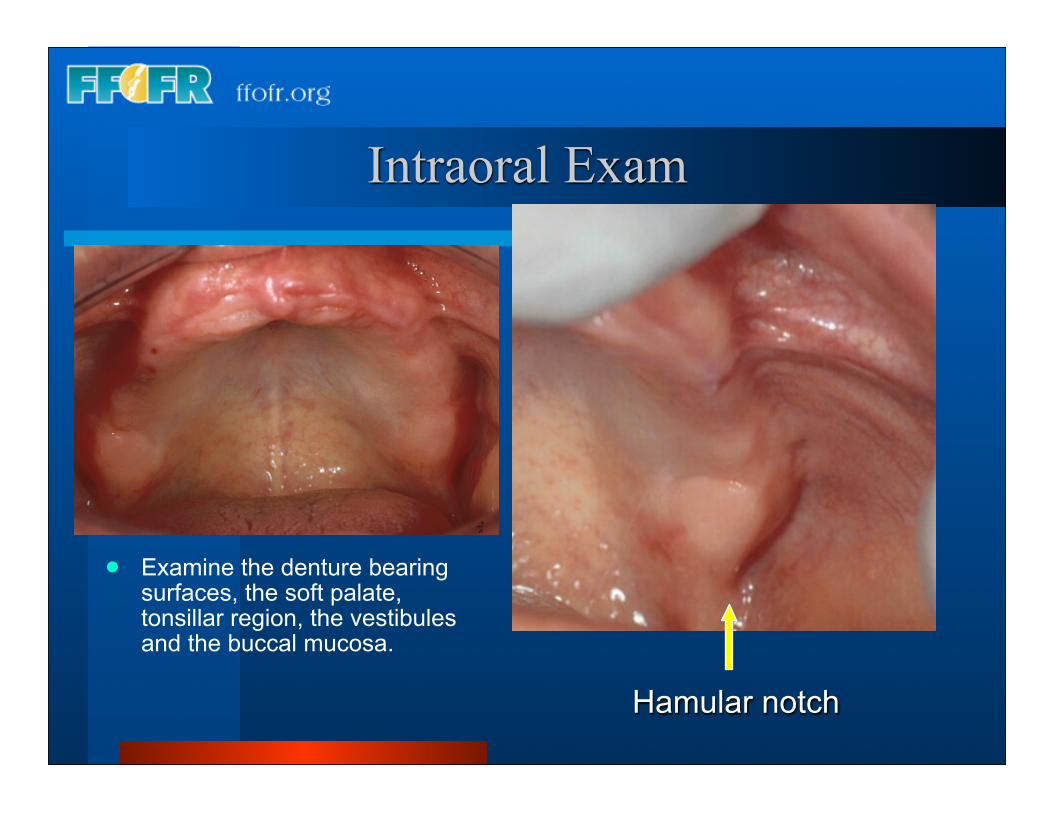
Examine the denture bearing surfaces, the soft palate, tonsillar region, the vestibules and the buccal mucosa.
Hamular notch
Intraoral Exam
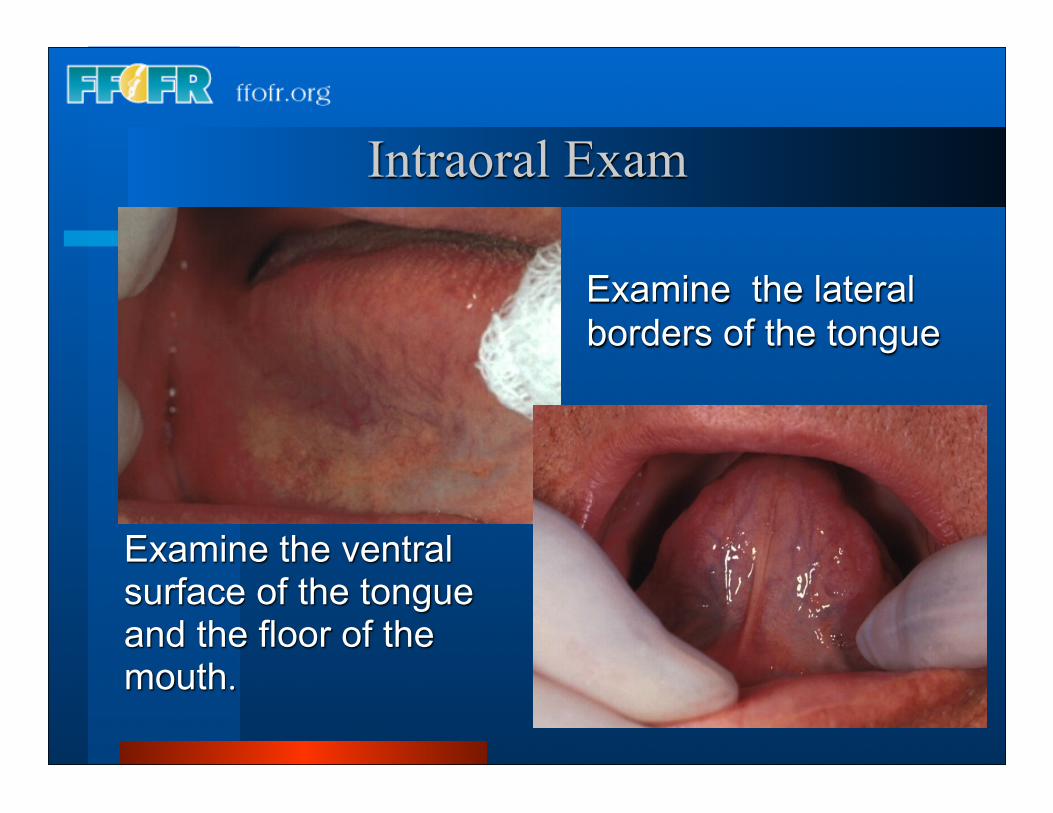
Examine the lateral borders of the tongue
Examine the ventral surface of the tongue and the floor of the mouth.
Intraoral Exam
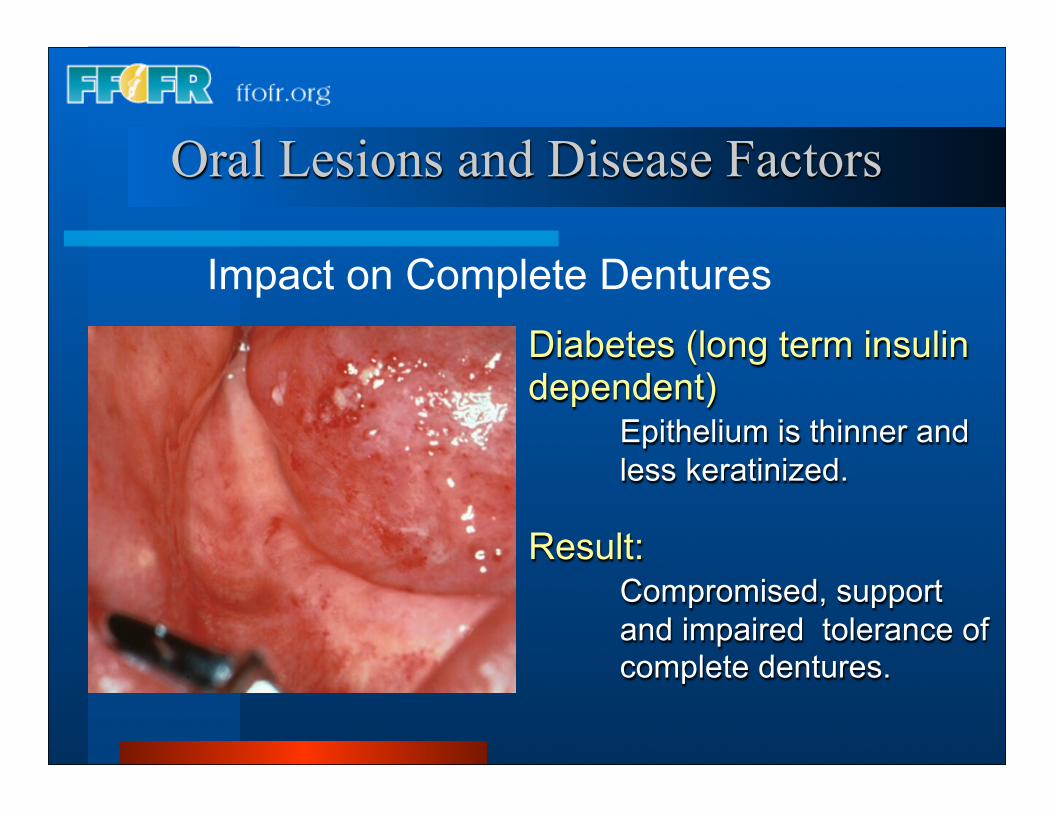
Oral Lesions and Disease Factors
Diabetes (long term insulin dependent) Epithelium is thinner and less keratinized.
Result: Compromised, support and impaired tolerance of complete dentures.
Impact on Complete Dentures
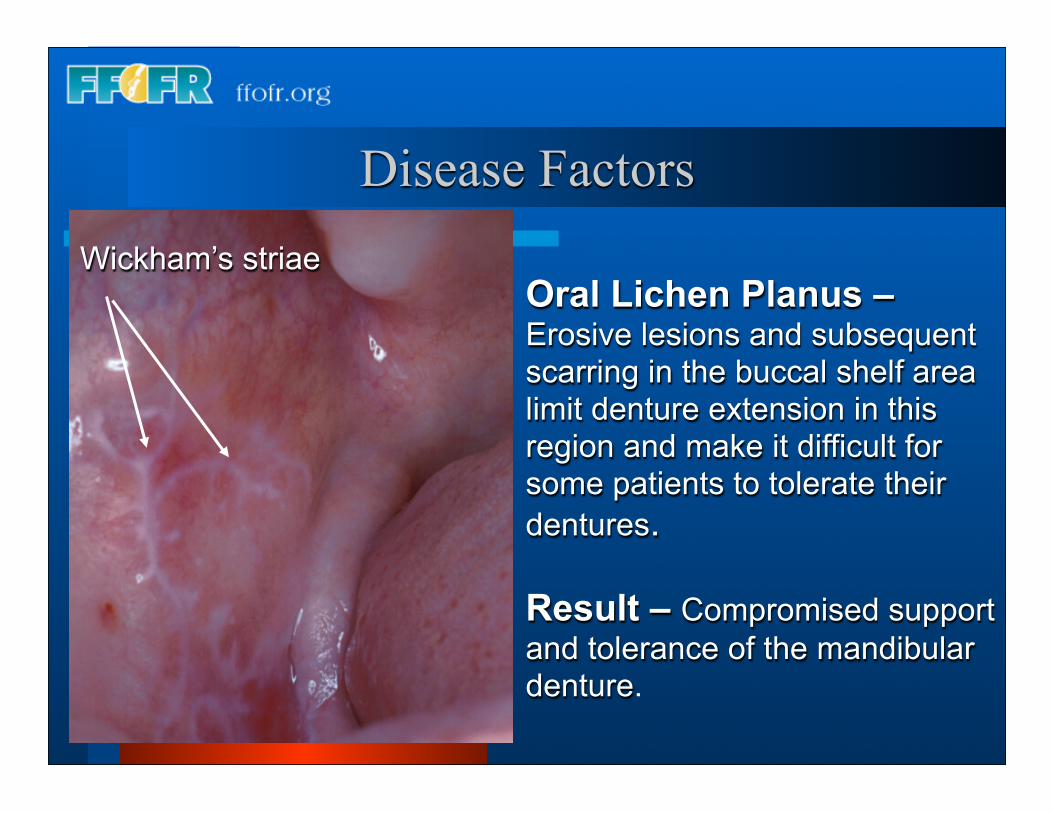
Oral Lichen Planus – Erosive lesions and subsequent scarring in the buccal shelf area limit denture extension in this region and make it difficult for some patients to tolerate their dentures.
Result – Compromised support and tolerance of the mandibular denture.
Disease FactorsWickham’s striae
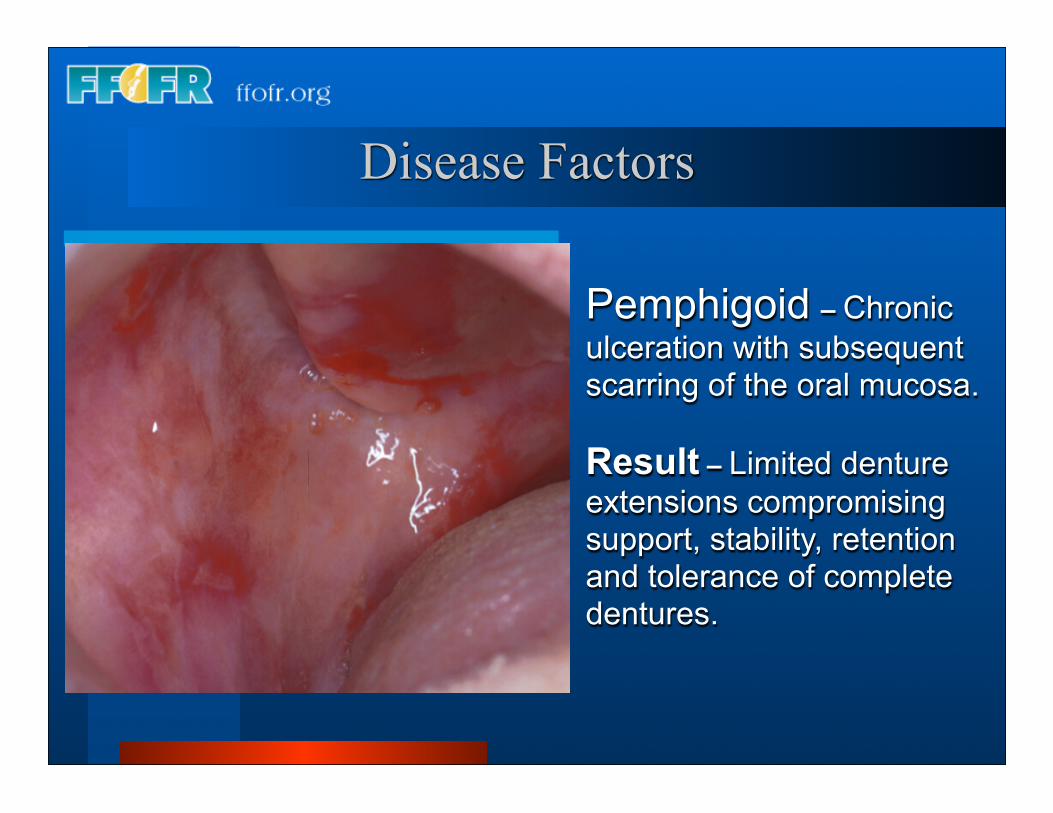
Pemphigoid – Chronic ulceration with subsequent scarring of the oral mucosa.
Result – Limited denture extensions compromising support, stability, retention and tolerance of complete dentures.
Disease Factors
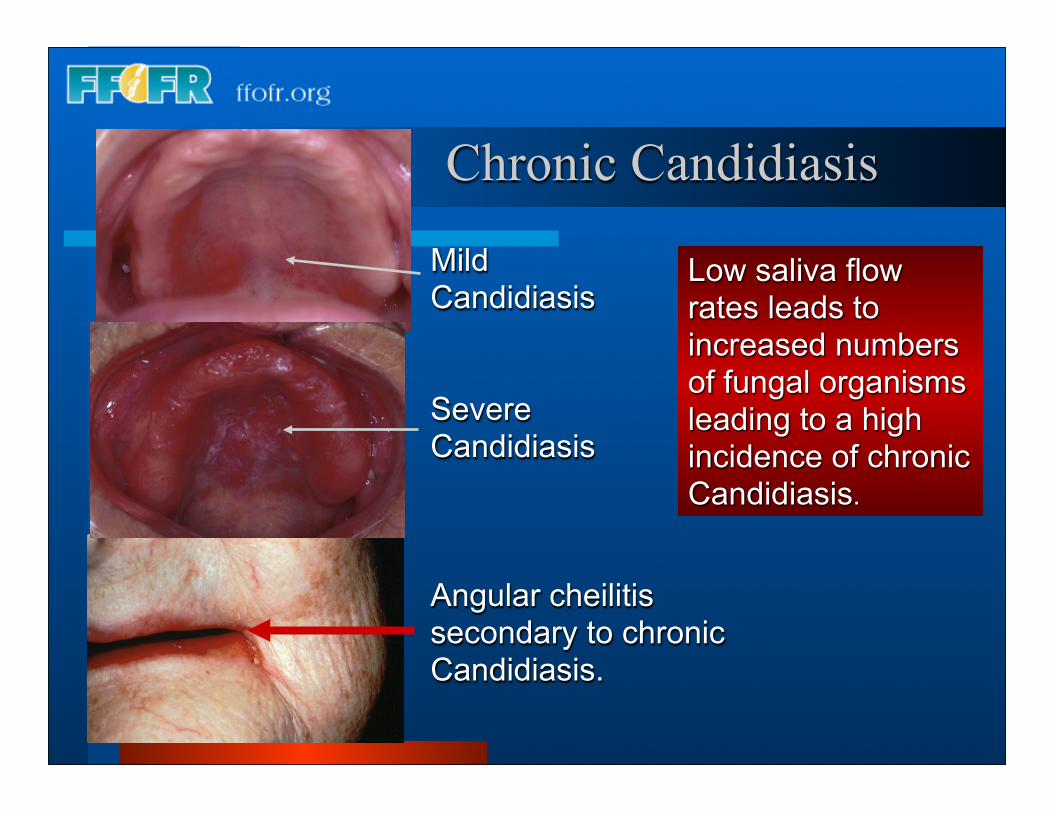
Low saliva flow rates leads to increased numbers of fungal organisms leading to a high incidence of chronic Candidiasis.
MildCandidiasis
SevereCandidiasis
Angular cheilitissecondary to chronicCandidiasis.
Chronic Candidiasis
Clinical Manifestations
Burning and irritation of the denture bearing mucosa, making tolerance of complete dentures difficult. In addition the fungus is keratolytic, further compromising support and tolerance.
Treatment
Topical antifungal therapy followed by relining of the dentures (Nystatin is the drug of choice. It can be dispensed as a cream, a powder or an oral lozenge).
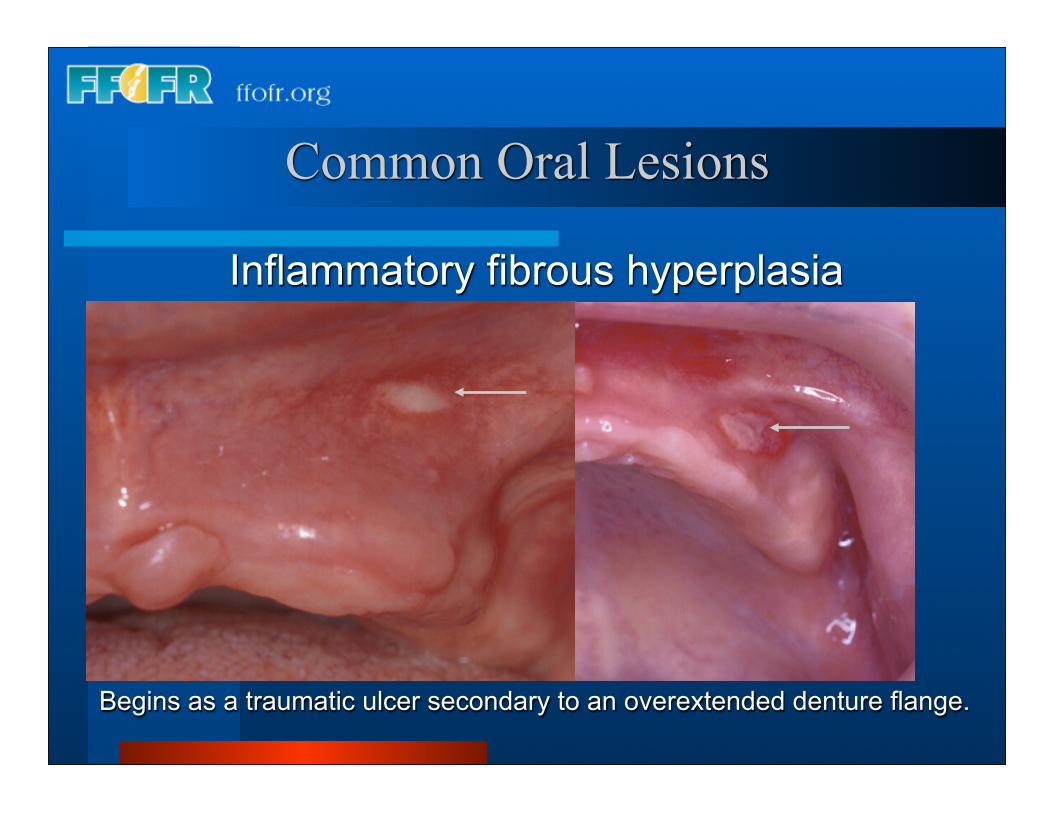
Begins as a traumatic ulcer secondary to an overextended denture flange.
Common Oral Lesions
Inflammatory fibrous hyperplasia
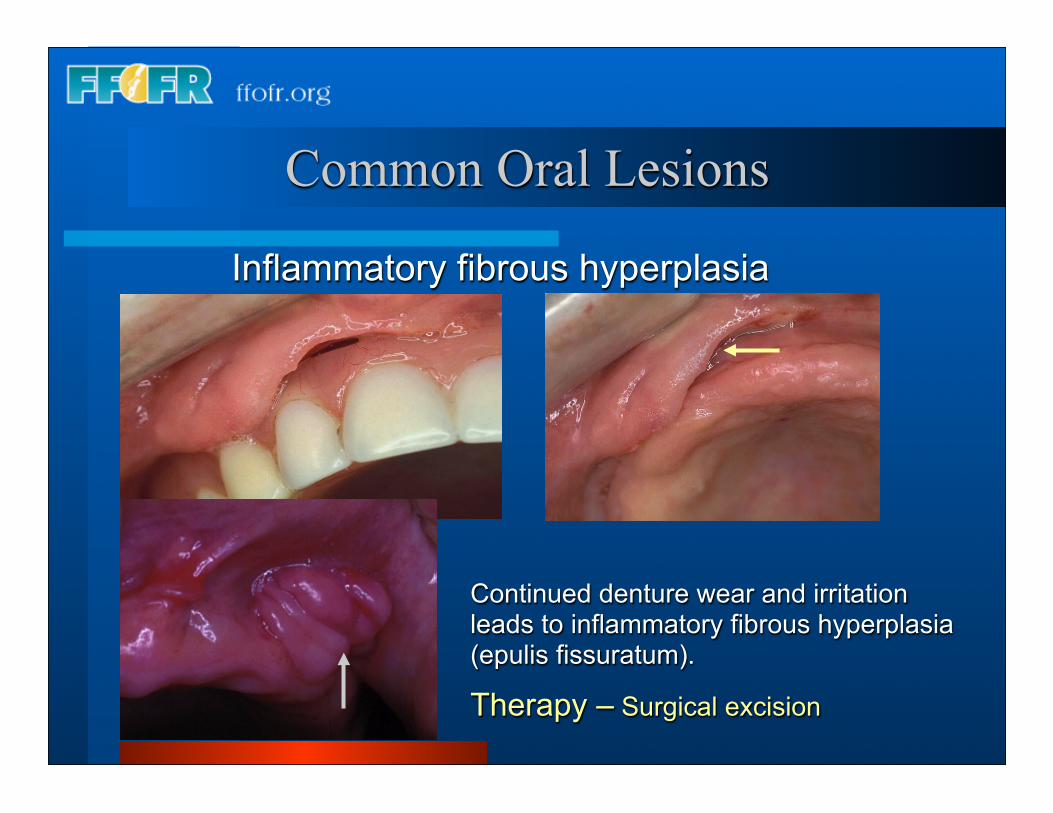
Continued denture wear and irritation leads to inflammatory fibrous hyperplasia (epulis fissuratum).
Therapy – Surgical excision
Common Oral Lesions
Inflammatory fibrous hyperplasia
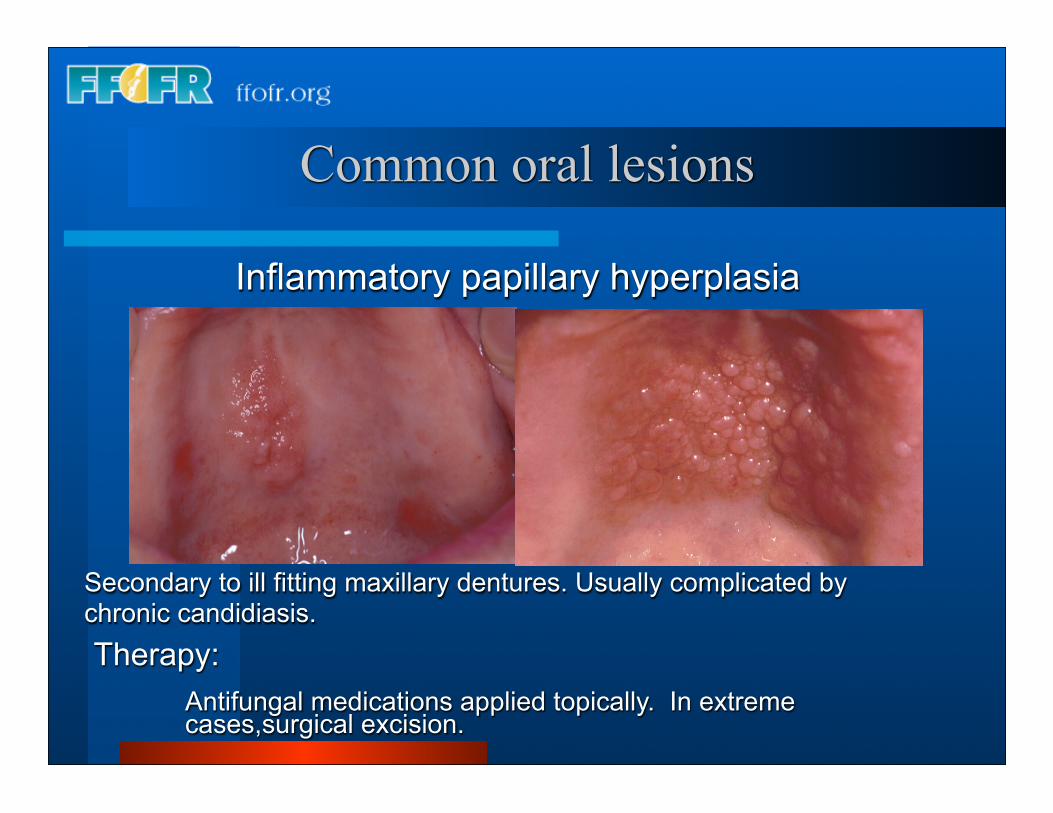
Common oral lesions
Secondary to ill fitting maxillary dentures. Usually complicated by chronic candidiasis.
Inflammatory papillary hyperplasia
Therapy: Antifungal medications applied topically. In extreme cases,surgical excision.
Therapeutic Approaches – Palatal Papillary Hyperplasia**with Associated Candida Albicans
Antifungal therapy*a) Reline or remake dentureb) Nystatin powder (100,000 units per gram) Apply to undersurface of denture
three times per day for 3-4 weeksc) Nystatin cream – Best used for lesions associated with the corners of the
mouthd) Reline denture with temporary reline material
Surgical excision with electrosurgery (when antifungal therapy has reached an end point)
*Nystatin rinse is generally ineffective. Nystatin oral or vaginal suppositories used as an oral lozenge are reserved for fungal infestations that extend beyond the denture bearing surfaces.
**Is this a premalignant lesion? No!!!!
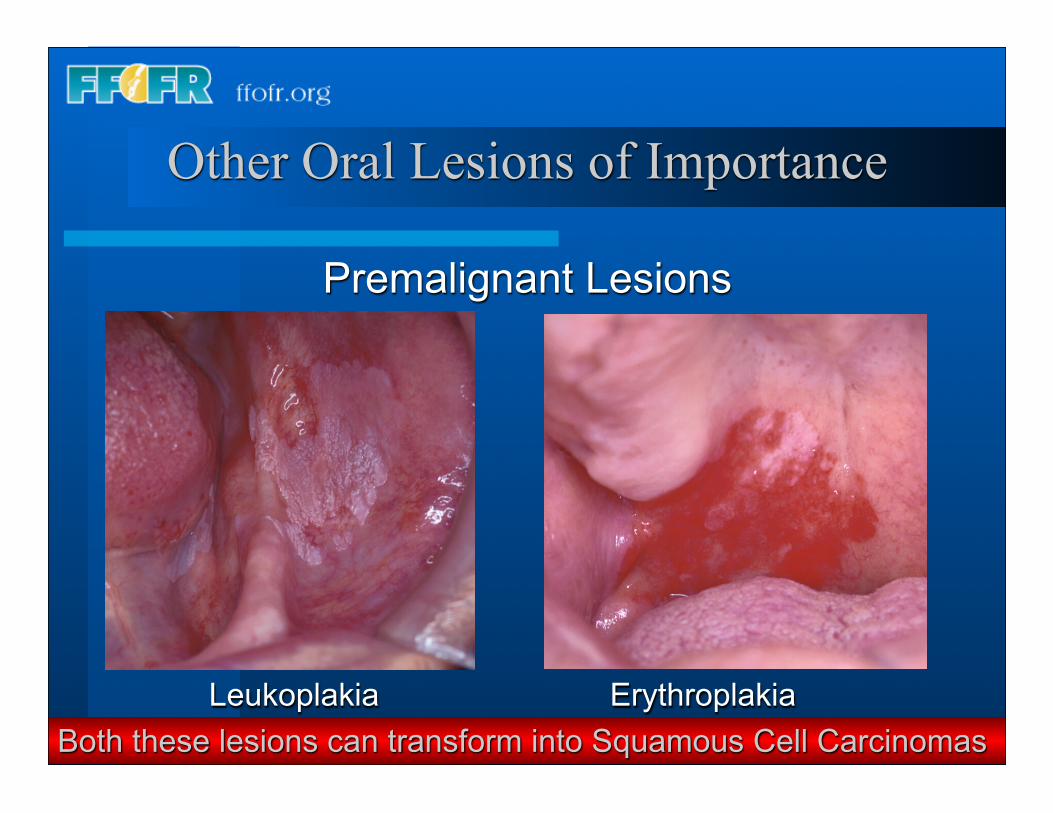
Other Oral Lesions of Importance
Premalignant Lesions
Both these lesions can transform into Squamous Cell CarcinomasLeukoplakia Erythroplakia
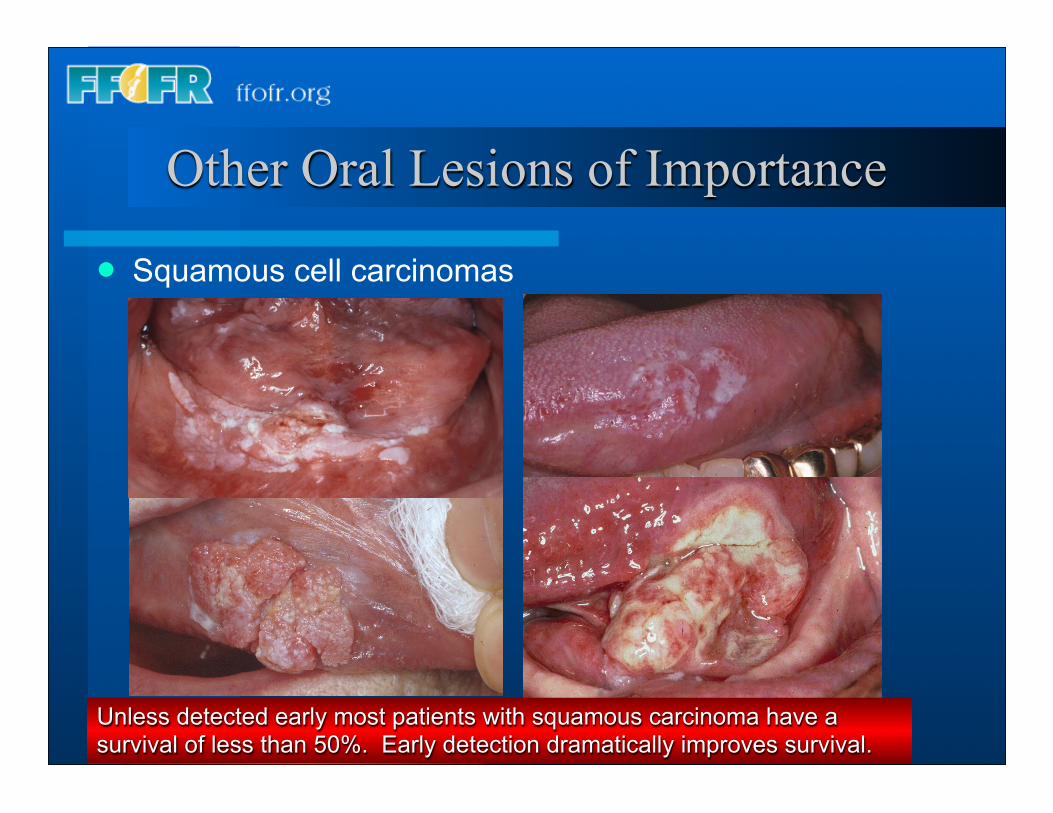
Other Oral Lesions of Importance
Squamous cell carcinomas
Unless detected early most patients with squamous carcinoma have a survival of less than 50%. Early detection dramatically improves survival.
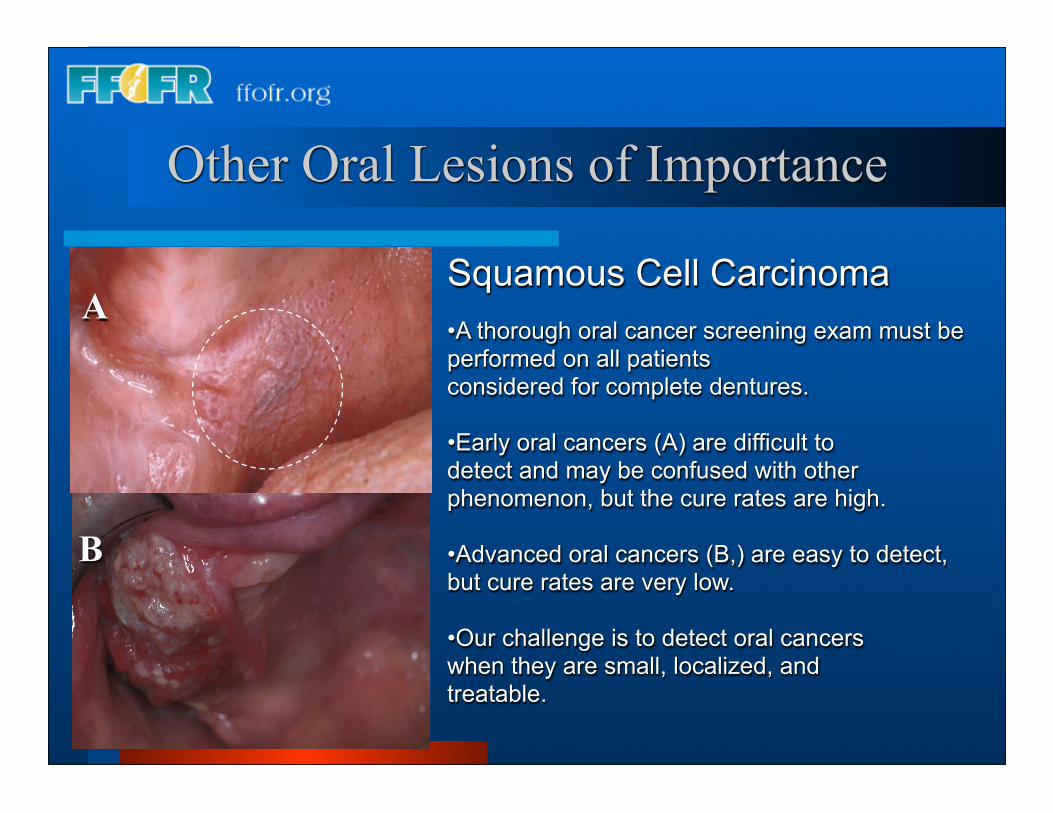
Squamous Cell Carcinoma•A thorough oral cancer screening exam must be performed on all patientsconsidered for complete dentures.
•Early oral cancers (A) are difficult todetect and may be confused with otherphenomenon, but the cure rates are high.
•Advanced oral cancers (B,) are easy to detect, but cure rates are very low.
•Our challenge is to detect oral cancerswhen they are small, localized, andtreatable.
A
B
Other Oral Lesions of Importance
Oral Exam
Clinical Factors Influencing Stability, Retention, and Support of
Complete Dentures
Definitions – Removable Prosthodontics
Retention – Resistance to vertical displacement of the denture away from the denture bearing surface during.
Stability – Resistance to lateral displacement of the denture during function.
Support – Resistance to vertical forces of occlusion. Factors of the bearing surface that resist or absorb occlusal loads during function.
What factors associated with the denture bearing tissues influence the quality of retention, stability, and support provided the complete denture?
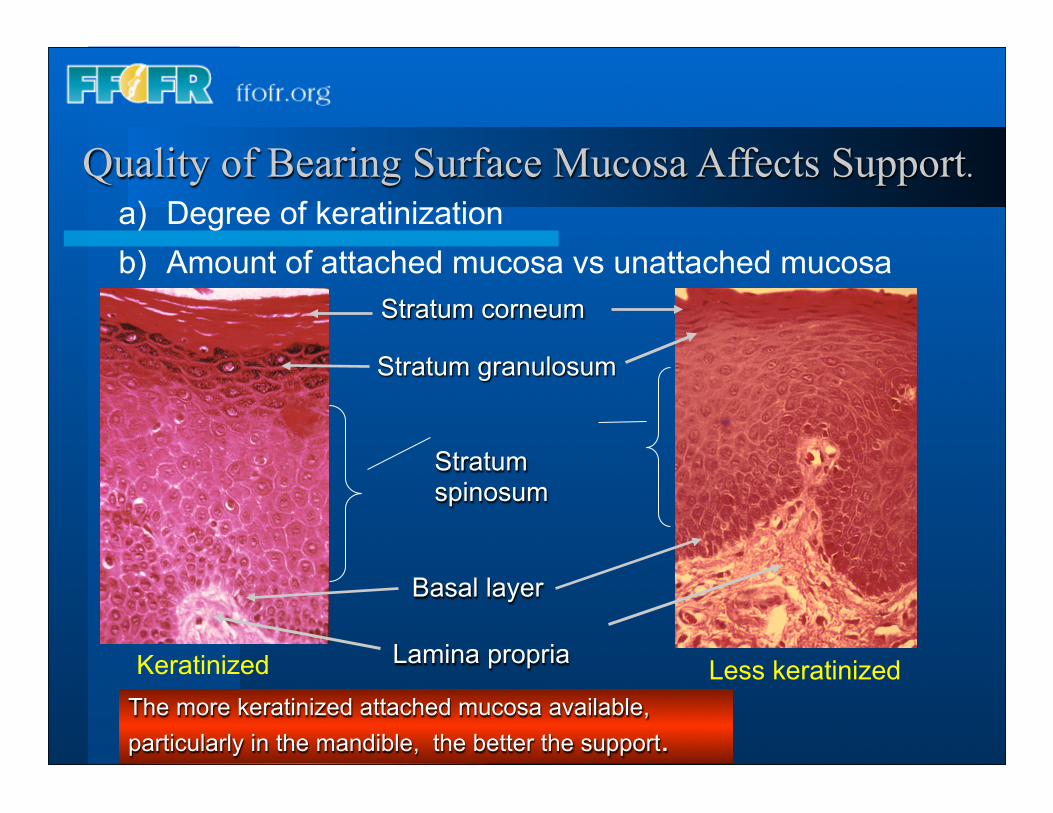
Quality of Bearing Surface Mucosa Affects Support.
The more keratinized attached mucosa available, particularly in the mandible, the better the support.
Stratum corneum
Stratum granulosum
Stratumspinosum
Basal layer
Lamina propriaKeratinized Less keratinized
a) Degree of keratinizationb) Amount of attached mucosa vs unattached mucosa
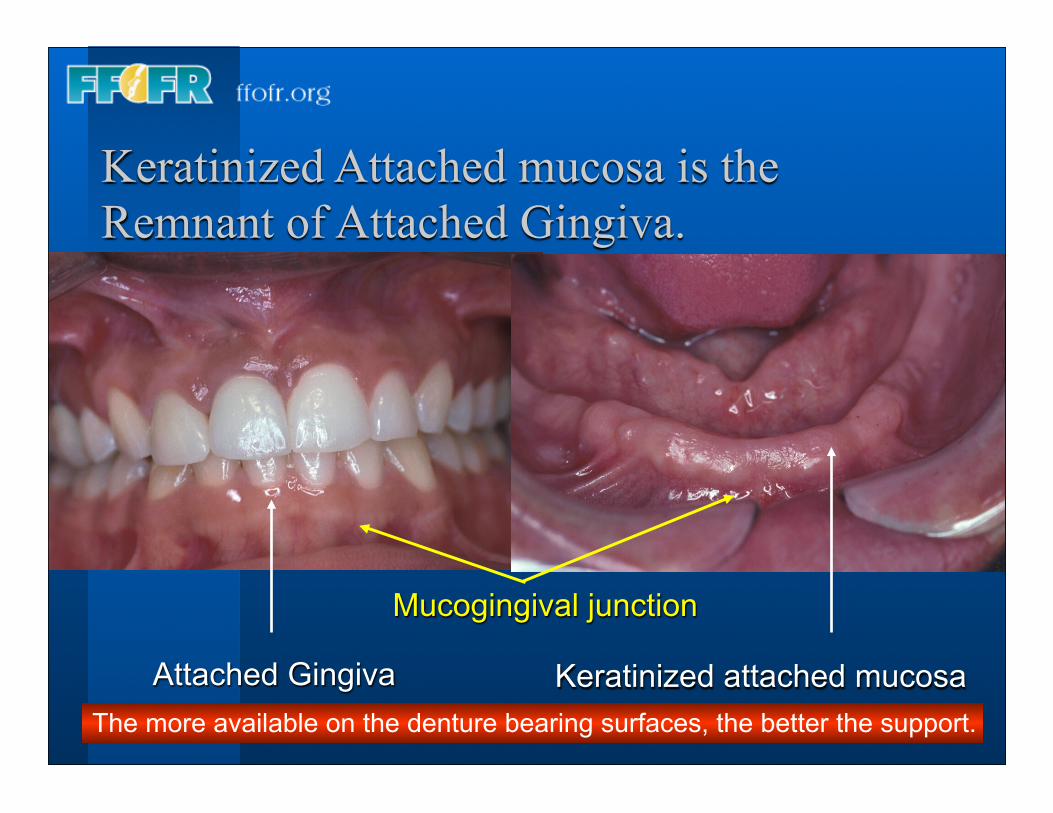
Keratinized Attached mucosa is the Remnant of Attached Gingiva.
Attached Gingiva Keratinized attached mucosa
Mucogingival junction
The more available on the denture bearing surfaces, the better the support.
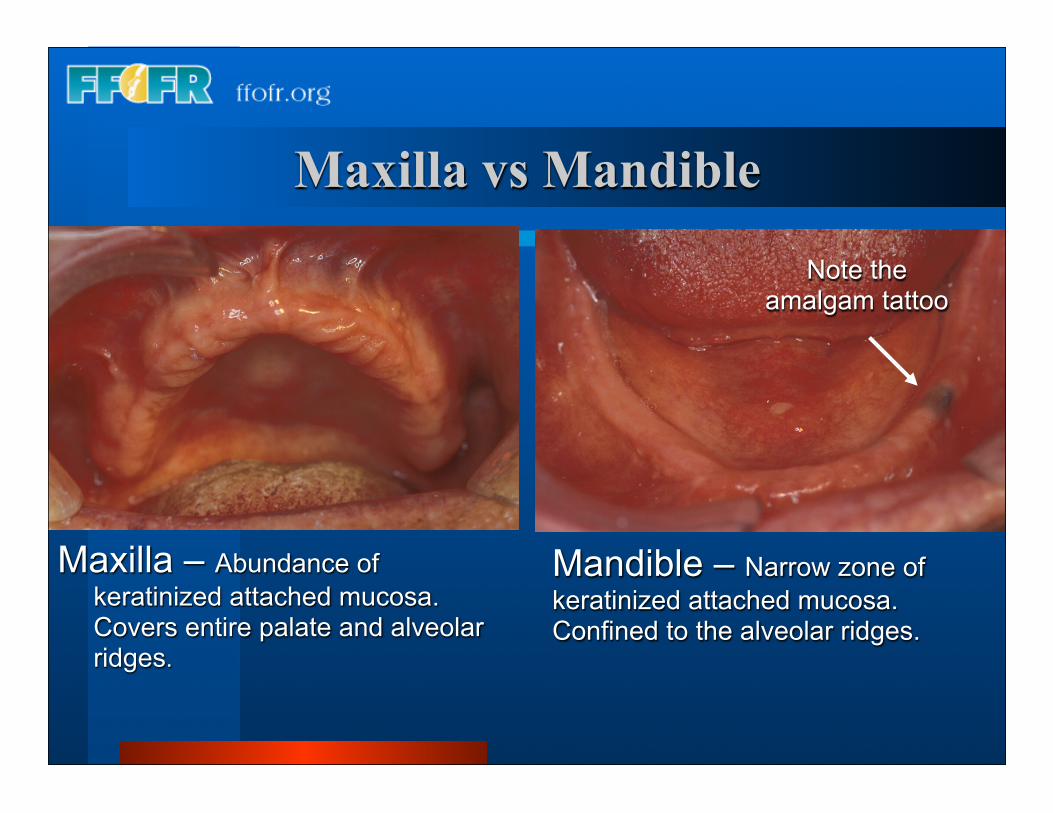
Maxilla – Abundance of keratinized attached mucosa. Covers entire palate and alveolar ridges.
Mandible – Narrow zone of keratinized attached mucosa. Confined to the alveolar ridges.
Note the amalgam tattoo
Maxilla vs Mandible
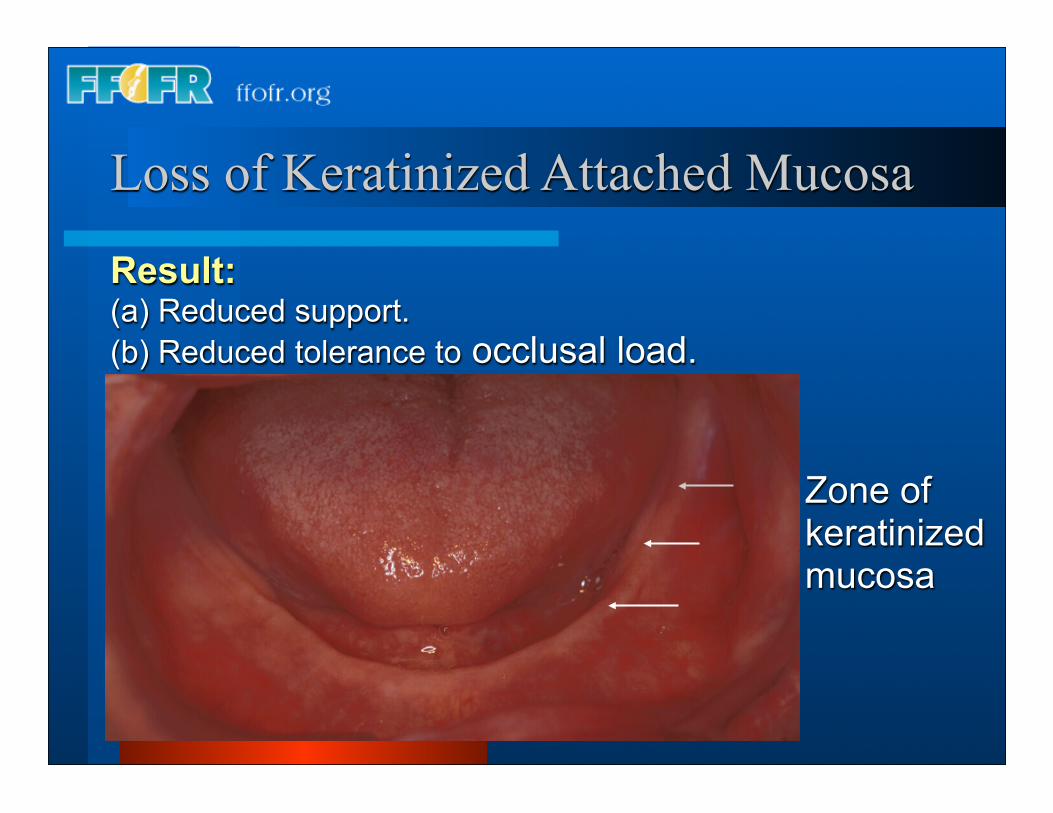
Loss of Keratinized Attached Mucosa Result:(a) Reduced support.(b) Reduced tolerance to occlusal load.
Zone of keratinized mucosa
What is the impact of bone resorption on retention, stability,
and support?
All three are negatively impacted.
Ridge Resorption
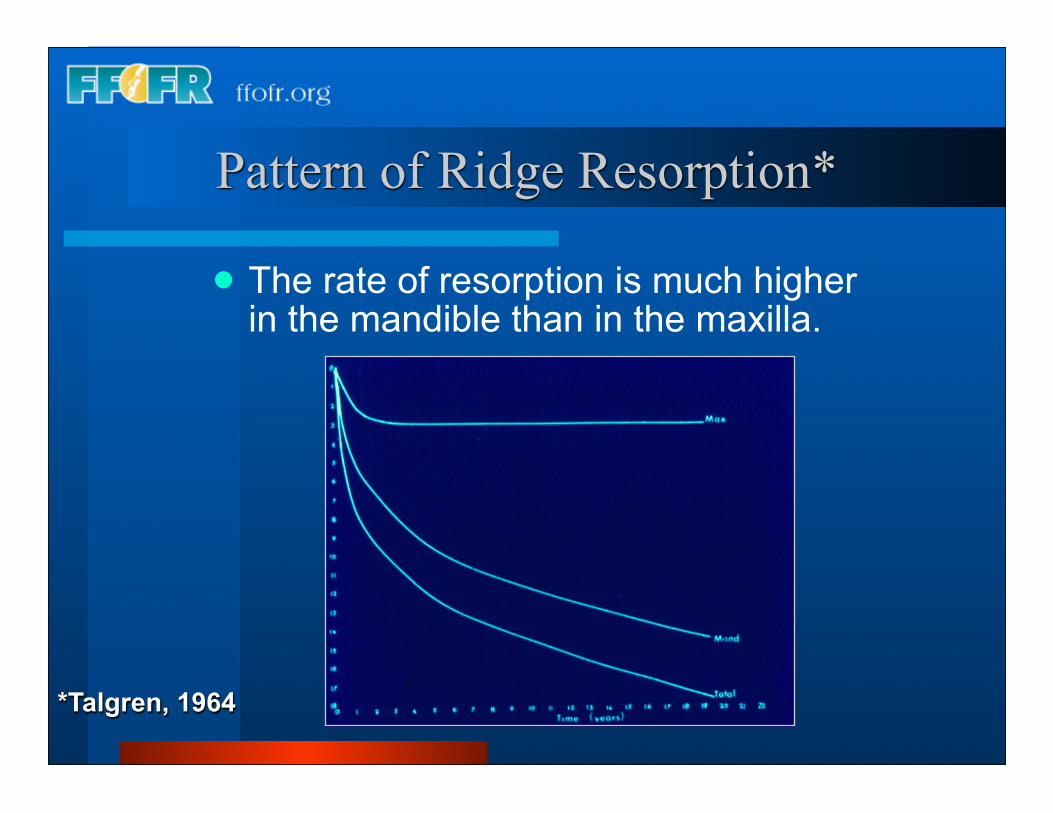
Pattern of Ridge Resorption*
The rate of resorption is much higher in the mandible than in the maxilla.
*Talgren, 1964
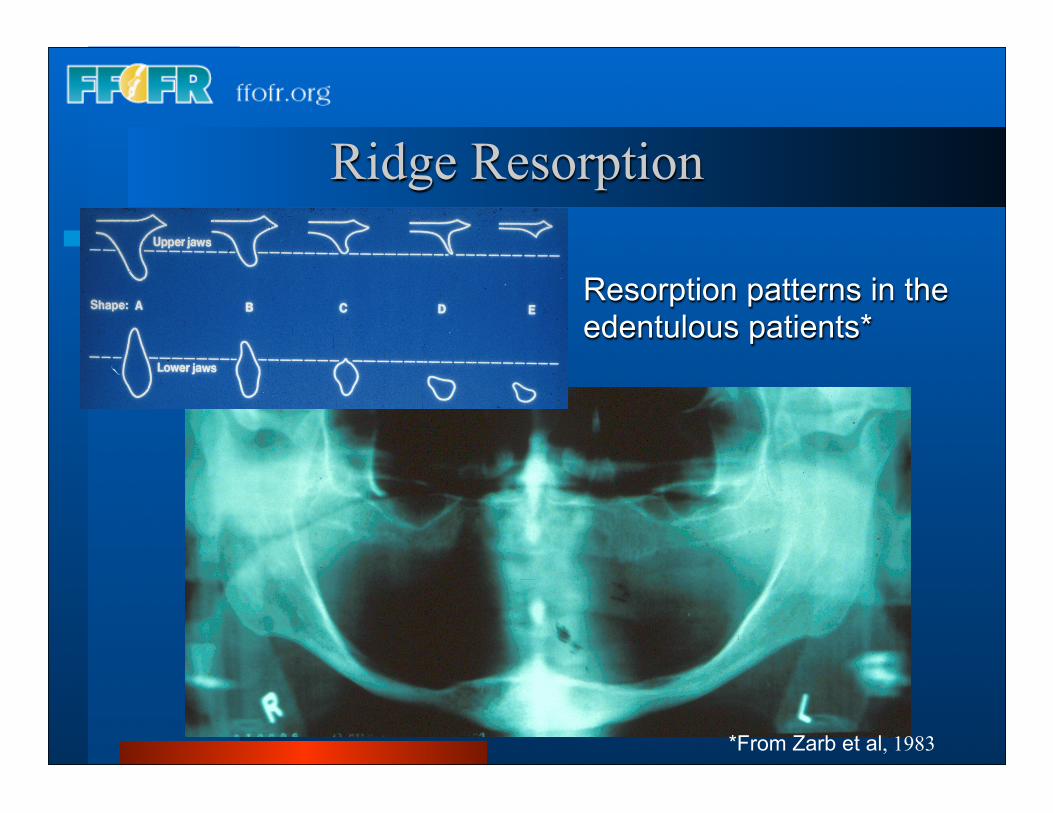
Resorption patterns in the edentulous patients*
Ridge Resorption
*From Zarb et al, 1983
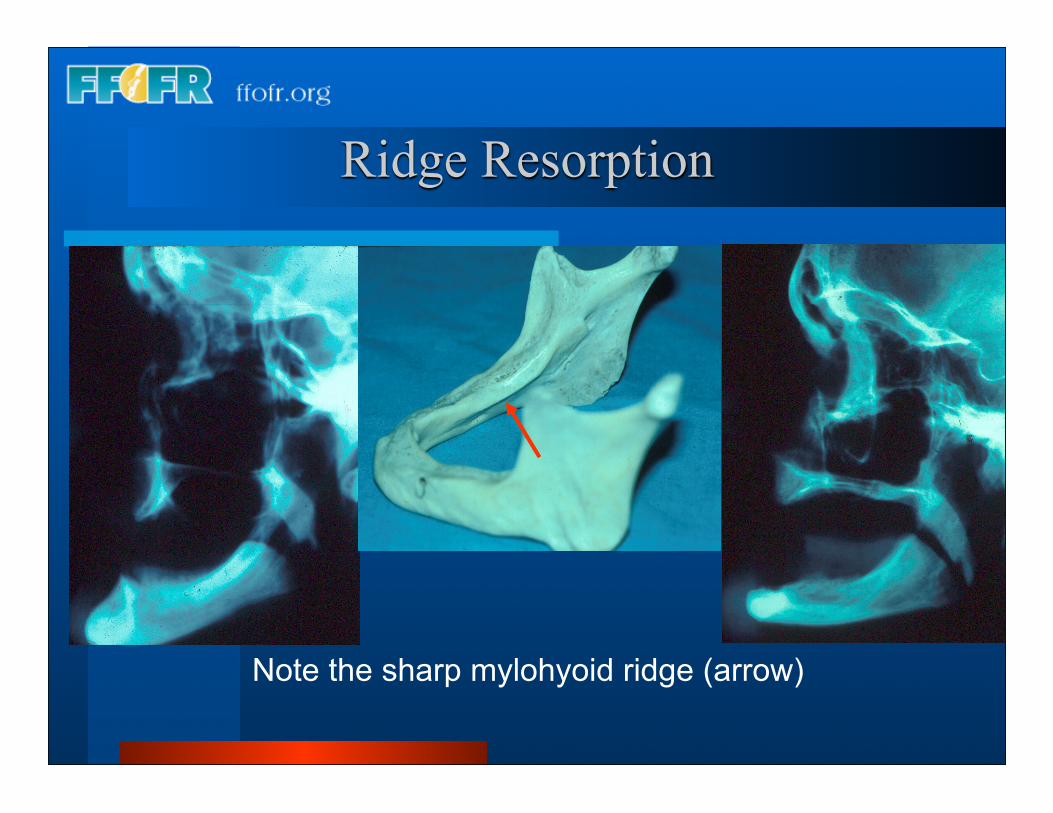
Ridge Resorption
Note the sharp mylohyoid ridge (arrow)
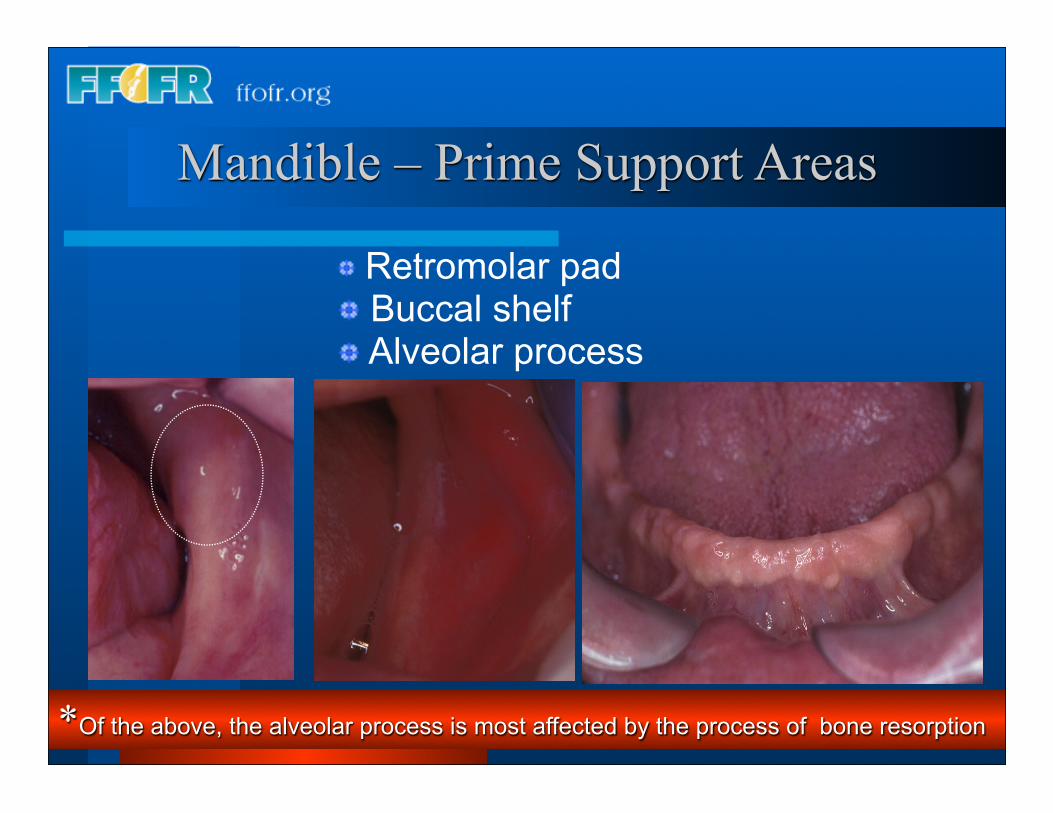
Mandible – Prime Support Areas
*Of the above, the alveolar process is most affected by the process of bone resorption
Retromolar pad Buccal shelf Alveolar process
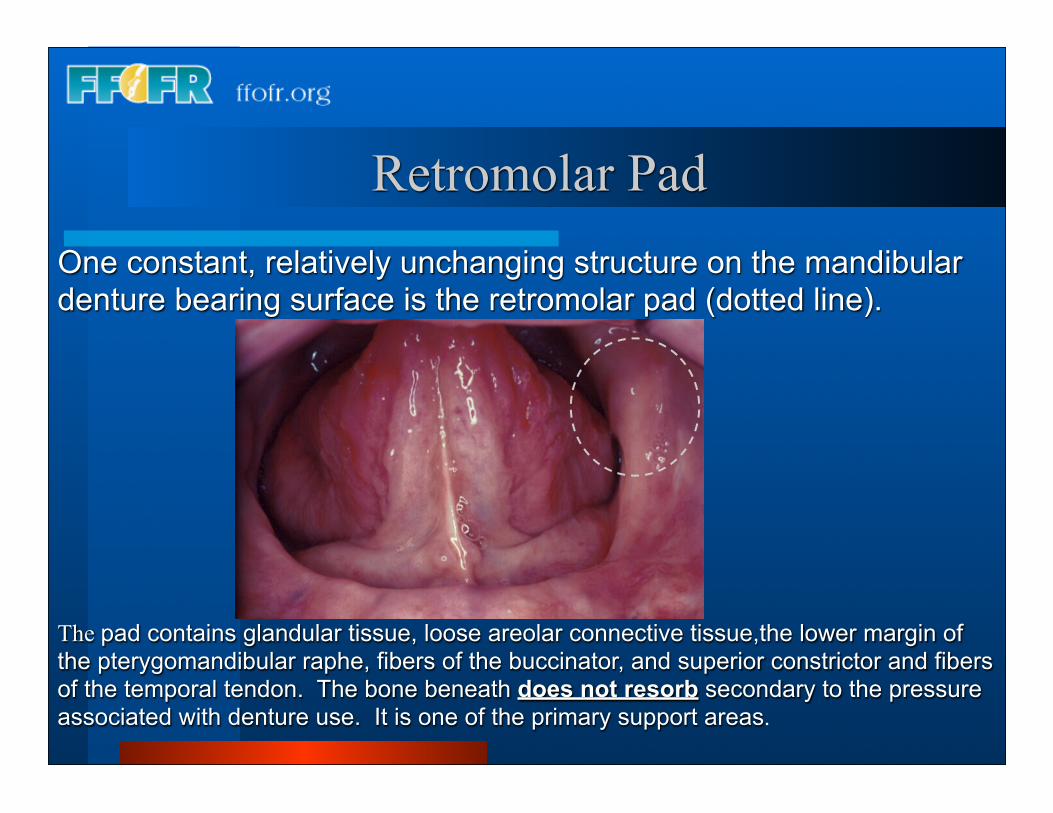
The pad contains glandular tissue, loose areolar connective tissue,the lower margin of the pterygomandibular raphe, fibers of the buccinator, and superior constrictor and fibers of the temporal tendon. The bone beneath does not resorb secondary to the pressure associated with denture use. It is one of the primary support areas.
Retromolar PadOne constant, relatively unchanging structure on the mandibular denture bearing surface is the retromolar pad (dotted line).
Buccal Shelf
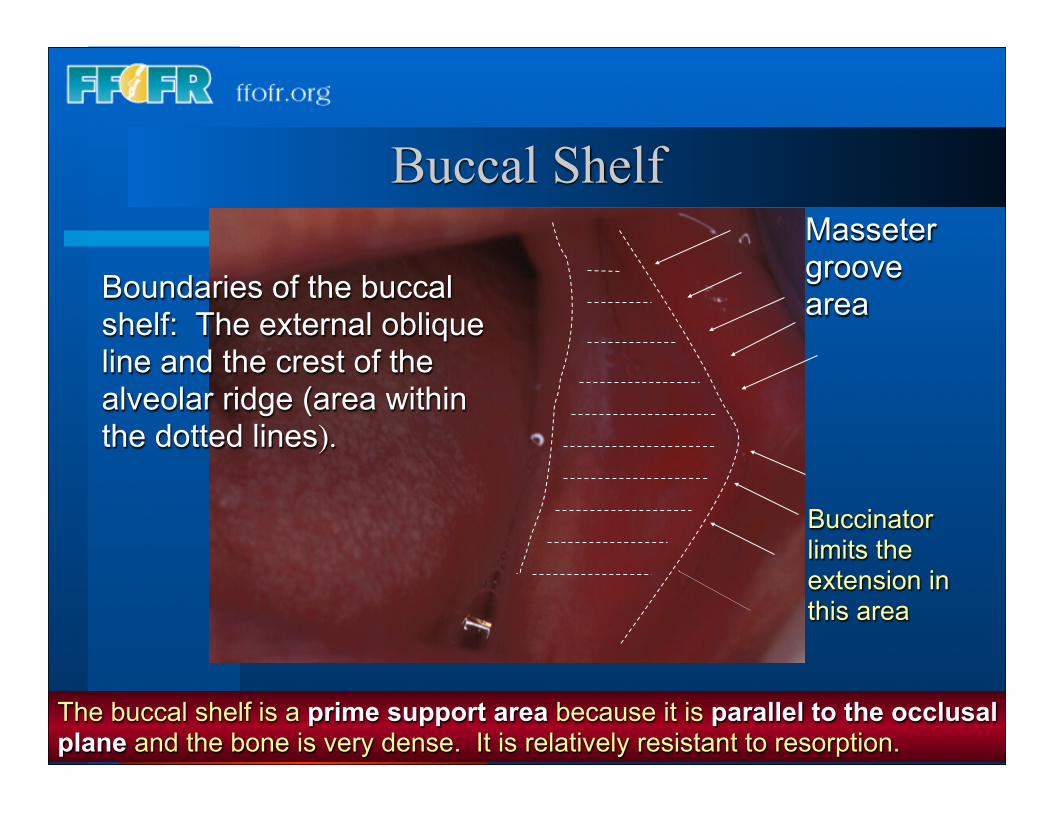
Boundaries of the buccal shelf: The external oblique line and the crest of the alveolar ridge (area within the dotted lines).
The buccal shelf is a prime support area because it is parallel to the occlusal plane and the bone is very dense. It is relatively resistant to resorption.
Masseter groove area
Buccinator limits the extension in this area
Buccal Shelf
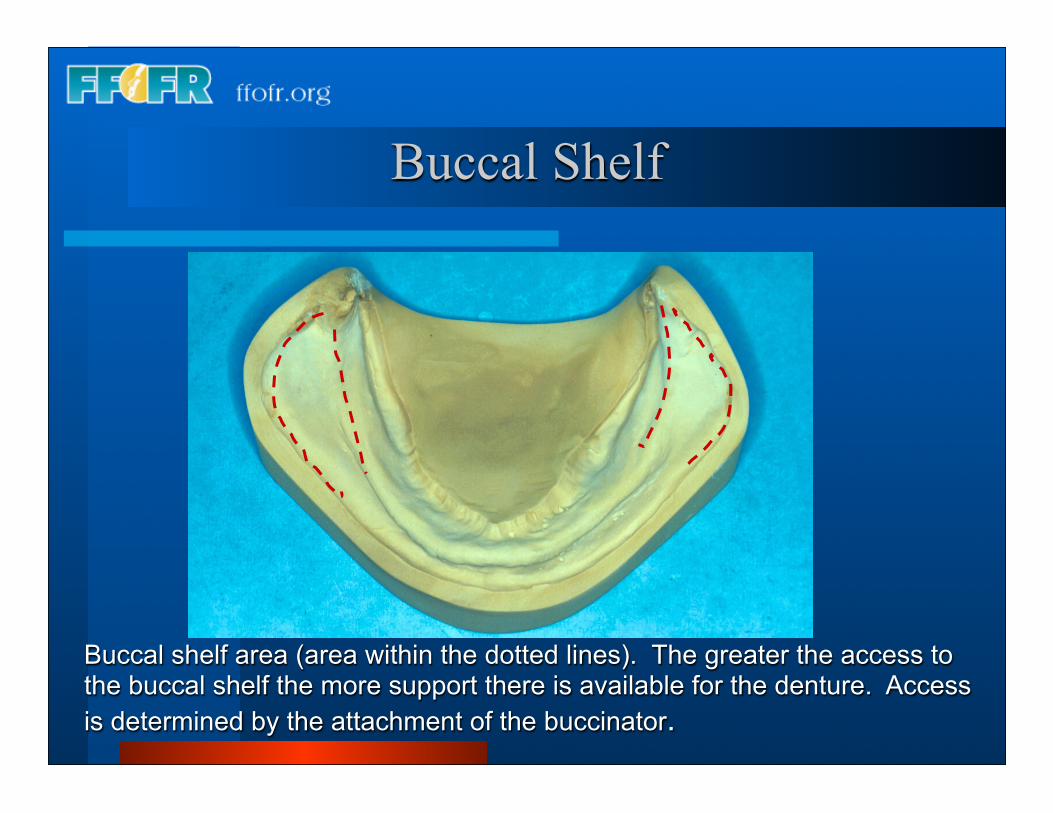
Buccal shelf area (area within the dotted lines). The greater the access to the buccal shelf the more support there is available for the denture. Access is determined by the attachment of the buccinator.
B
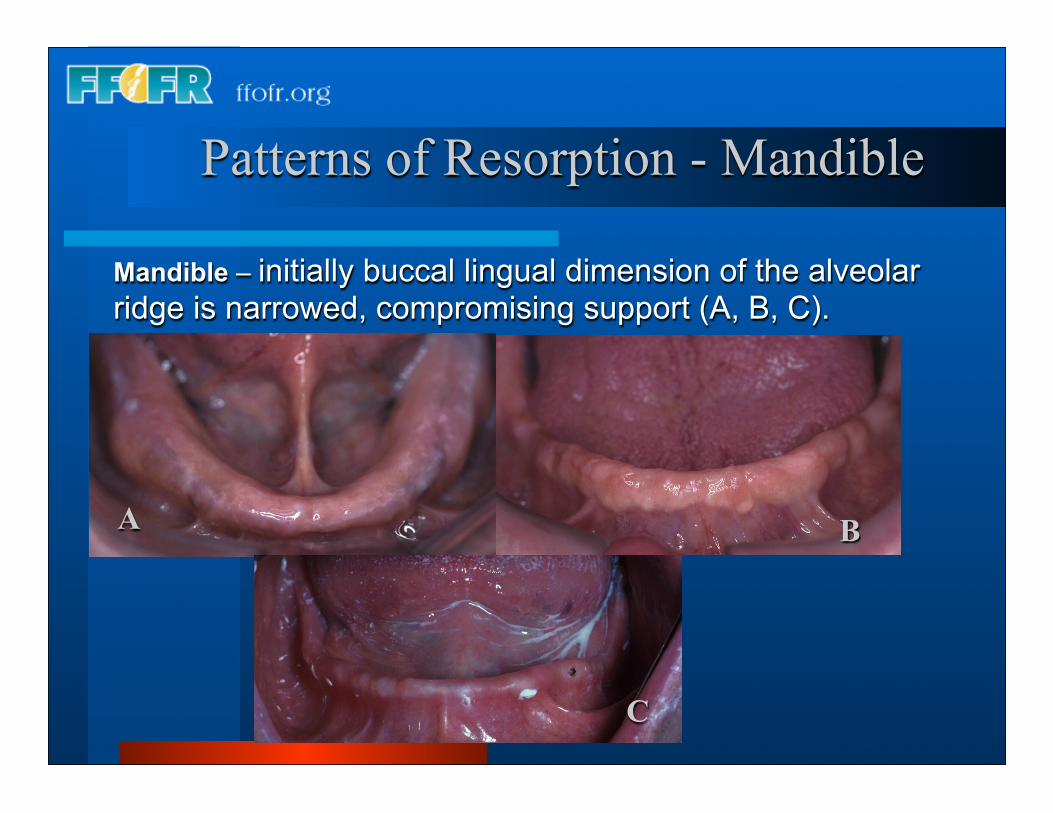
Mandible – initially buccal lingual dimension of the alveolar ridge is narrowed, compromising support (A, B, C).
A
Patterns of Resorption - Mandible
C
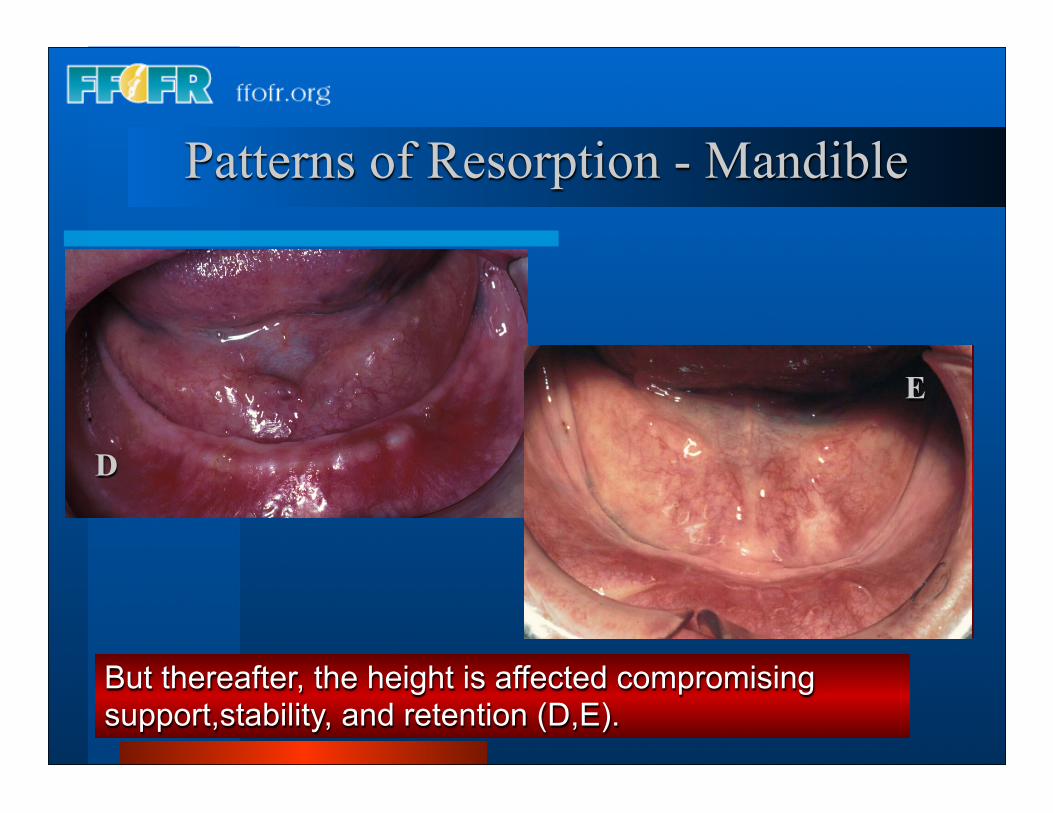
But thereafter, the height is affected compromising support,stability, and retention (D,E).
D
Patterns of Resorption - Mandible
E
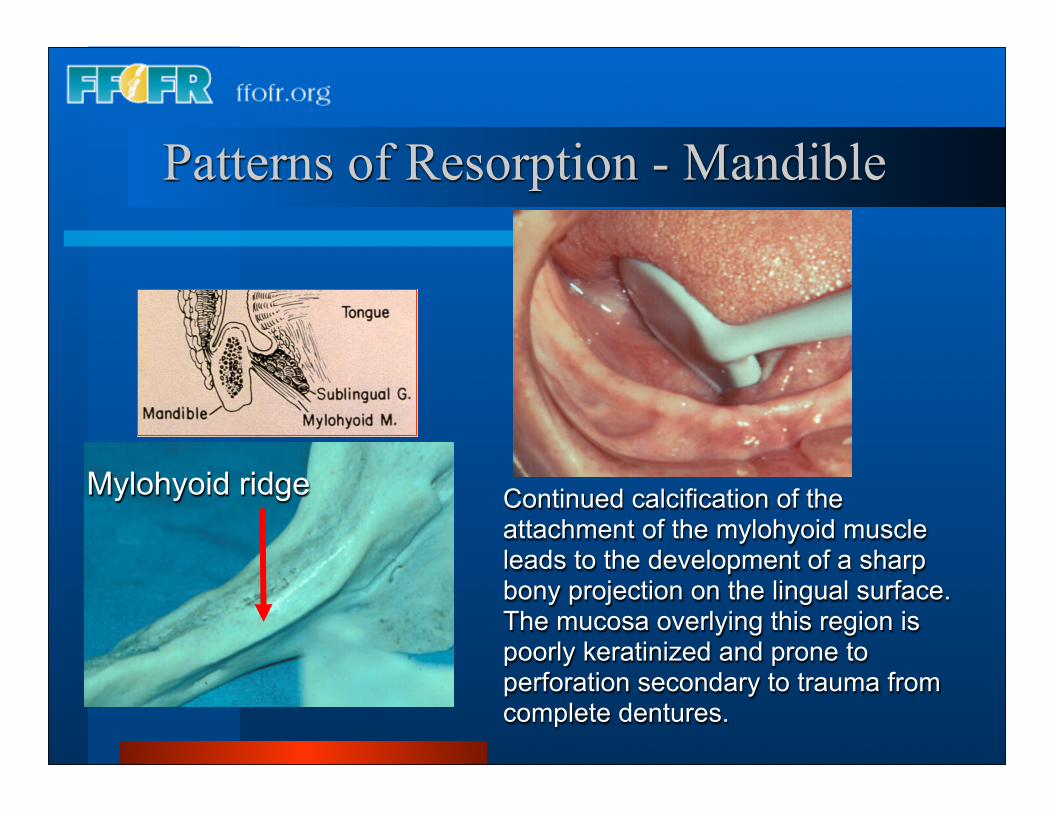
Continued calcification of the attachment of the mylohyoid muscle leads to the development of a sharp bony projection on the lingual surface. The mucosa overlying this region is poorly keratinized and prone to perforation secondary to trauma from complete dentures.
Mylohyoid ridge
Patterns of Resorption - Mandible
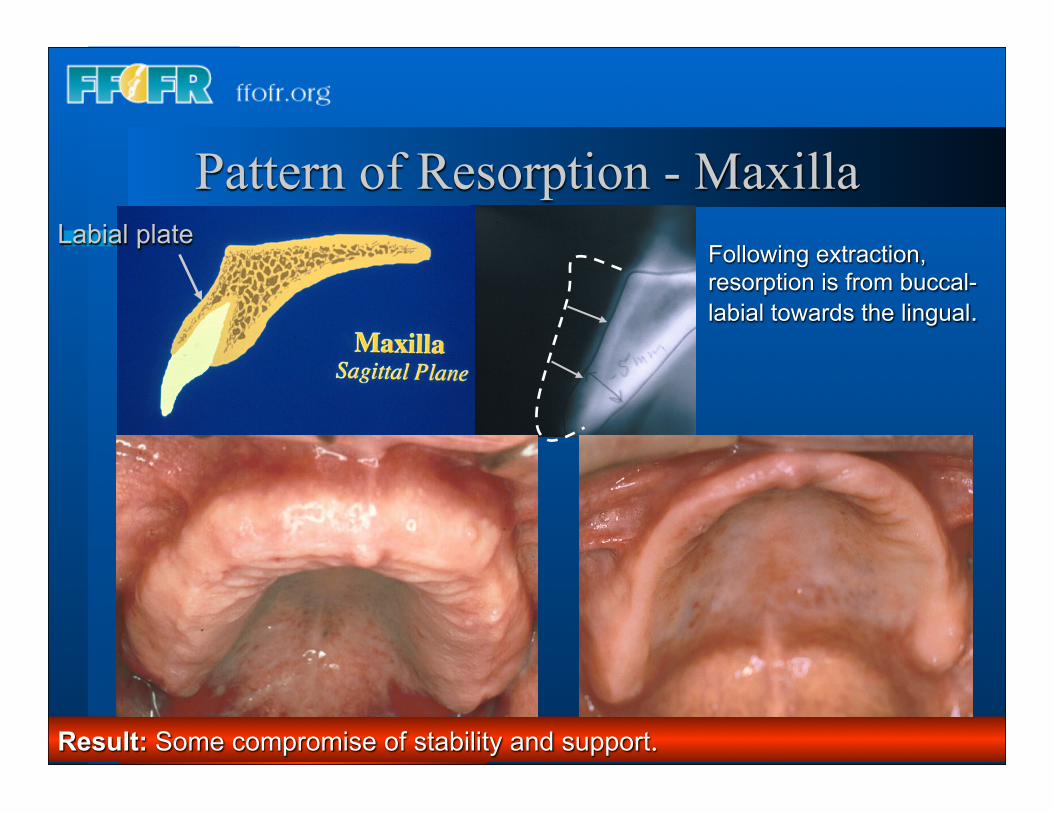
Following extraction, resorption is from buccal-labial towards the lingual.
Labial plate
Result: Some compromise of stability and support.
Pattern of Resorption - Maxilla
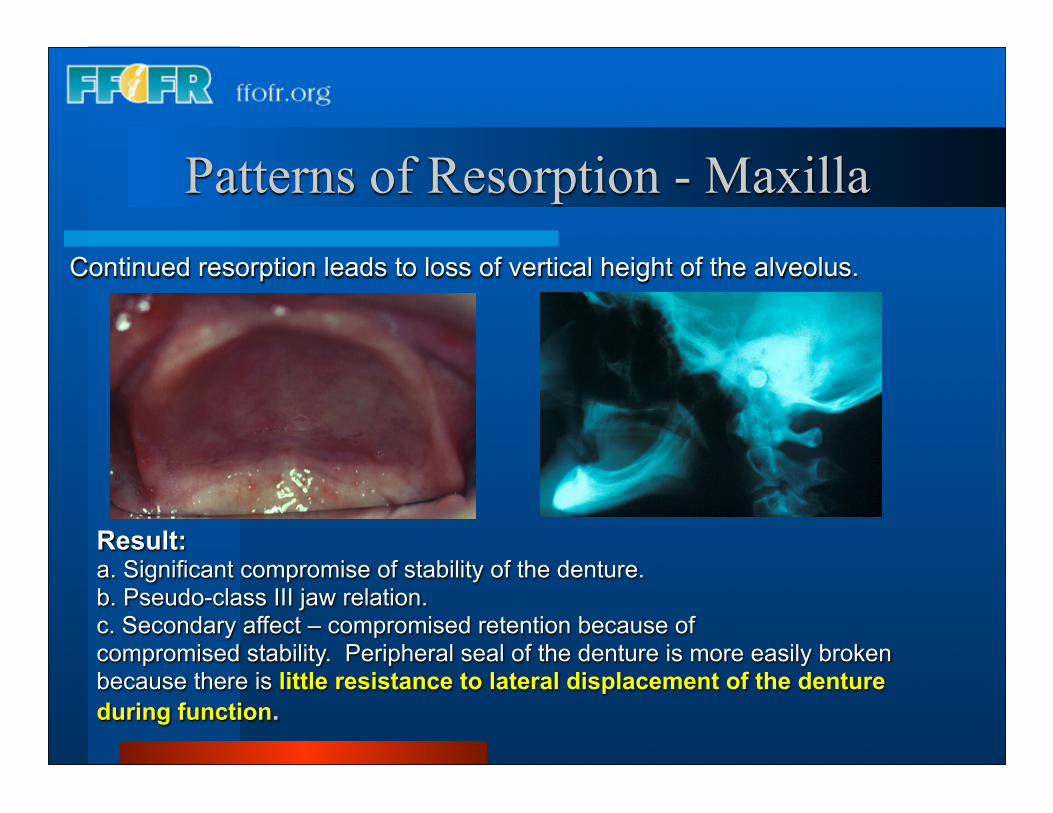
Continued resorption leads to loss of vertical height of the alveolus.
Result:a. Significant compromise of stability of the denture.b. Pseudo-class III jaw relation.c. Secondary affect – compromised retention because ofcompromised stability. Peripheral seal of the denture is more easily broken because there is little resistance to lateral displacement of the denture during function.
Patterns of Resorption - Maxilla
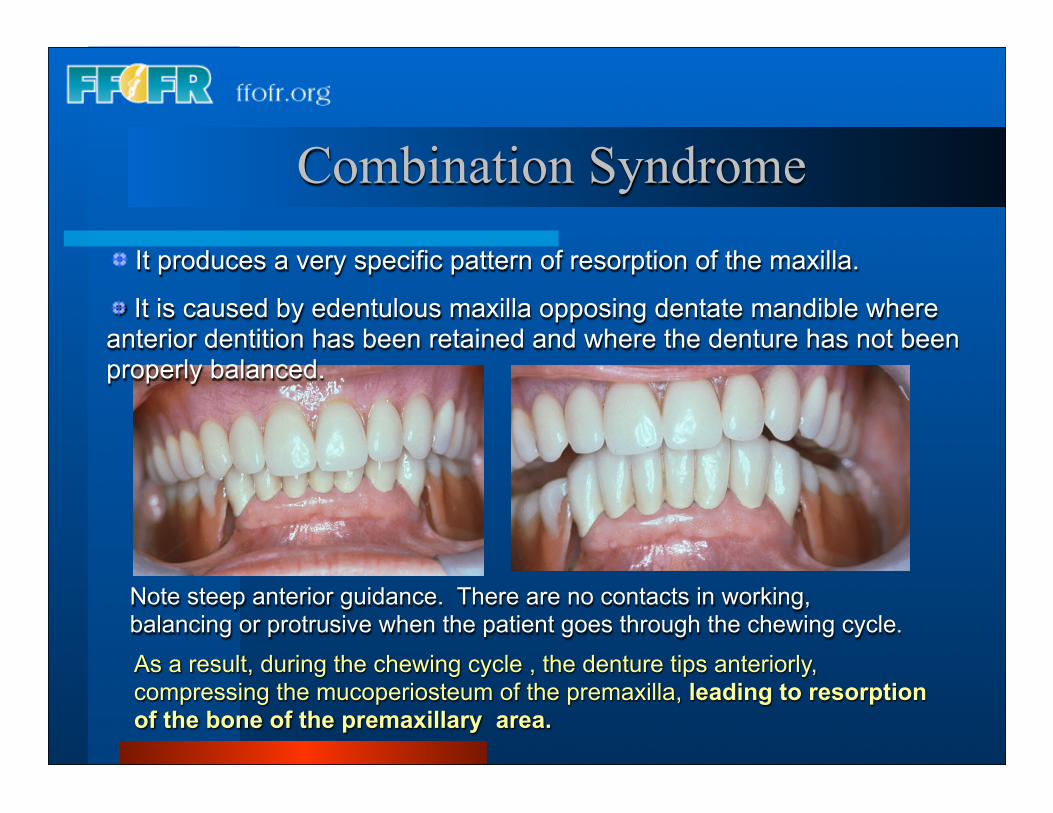
Note steep anterior guidance. There are no contacts in working, balancing or protrusive when the patient goes through the chewing cycle.
As a result, during the chewing cycle , the denture tips anteriorly, compressing the mucoperiosteum of the premaxilla, leading to resorption of the bone of the premaxillary area.
Combination Syndrome It produces a very specific pattern of resorption of the maxilla.
It is caused by edentulous maxilla opposing dentate mandible where anterior dentition has been retained and where the denture has not been properly balanced.
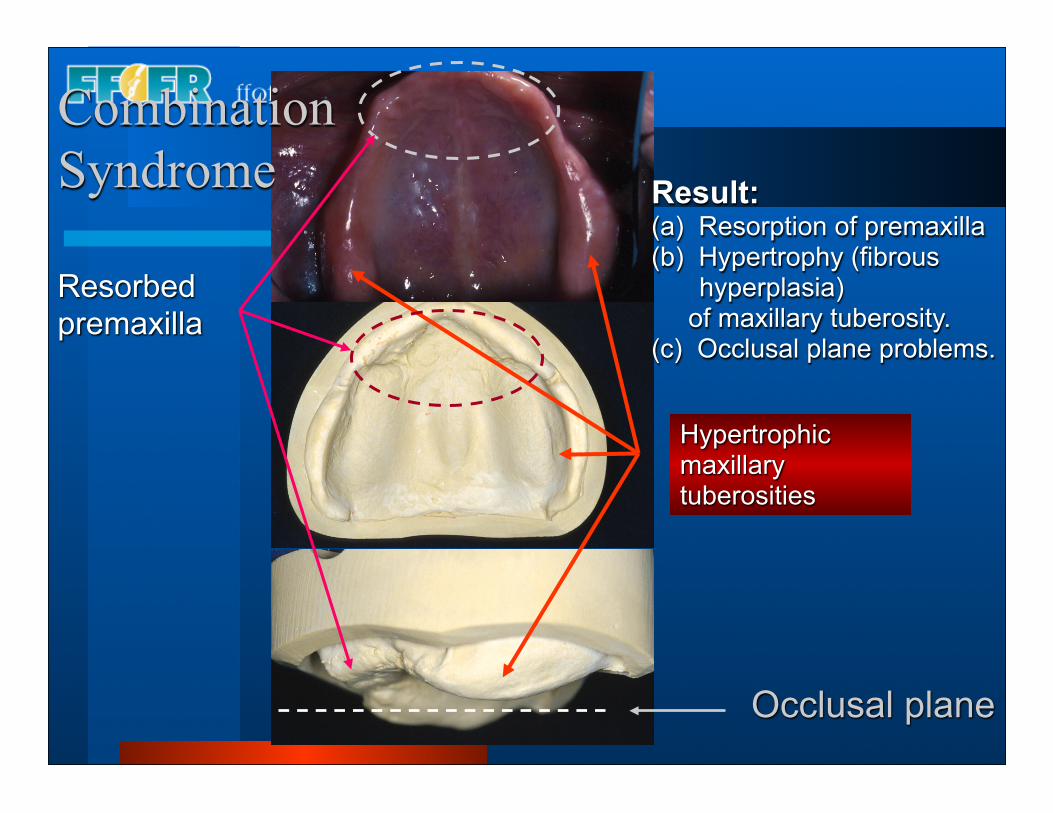
Result:(a) Resorption of premaxilla(b) Hypertrophy (fibrous
hyperplasia) of maxillary tuberosity.(c) Occlusal plane problems.
Occlusal plane
Hypertrophic maxillary tuberosities
Resorbed premaxilla
Combination Syndrome
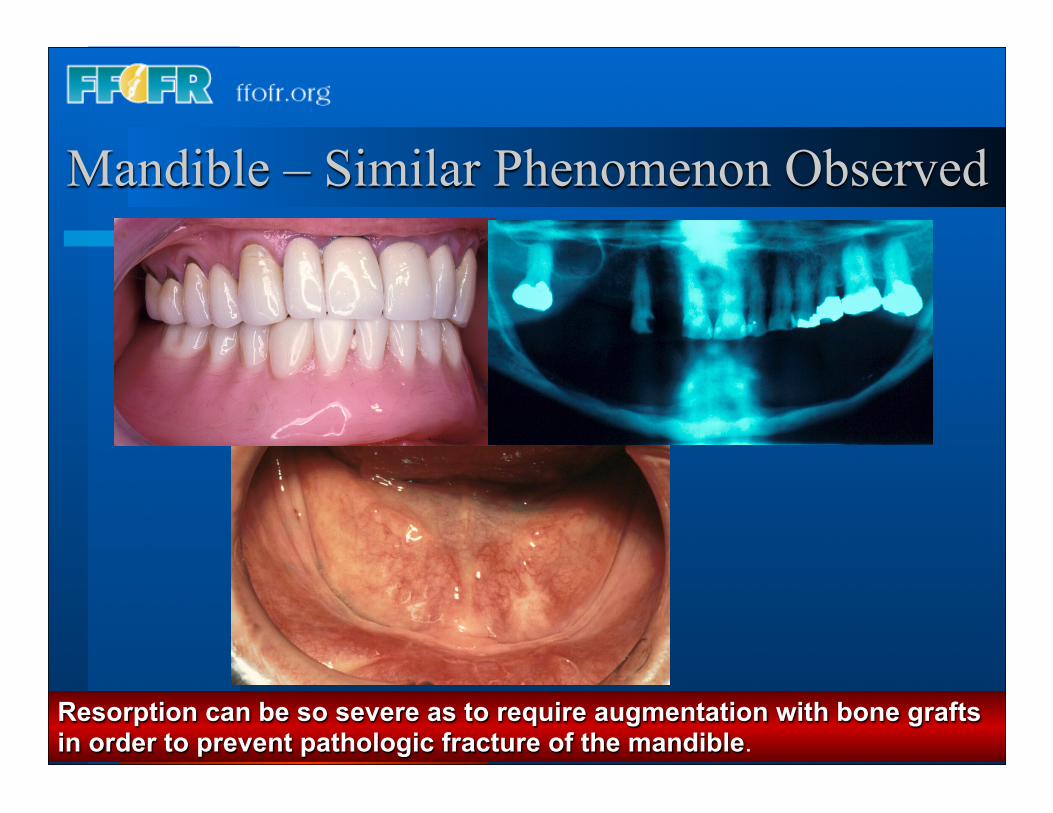
Mandible – Similar Phenomenon Observed
Resorption can be so severe as to require augmentation with bone grafts in order to prevent pathologic fracture of the mandible.

Measures to Prevent or Slow Resorption.1. Well adapted and properly extended dentures with properly designed and executed occlusion.2. Retention of residual tooth roots in key locations.
3. Use of osseointegrated implants
Retained roots and osseointegrated implants are useful because they absorb much of the occlusal load locally, thereby preventing compression of the periosteum and in turn preventing resorption of the adjacent bone.
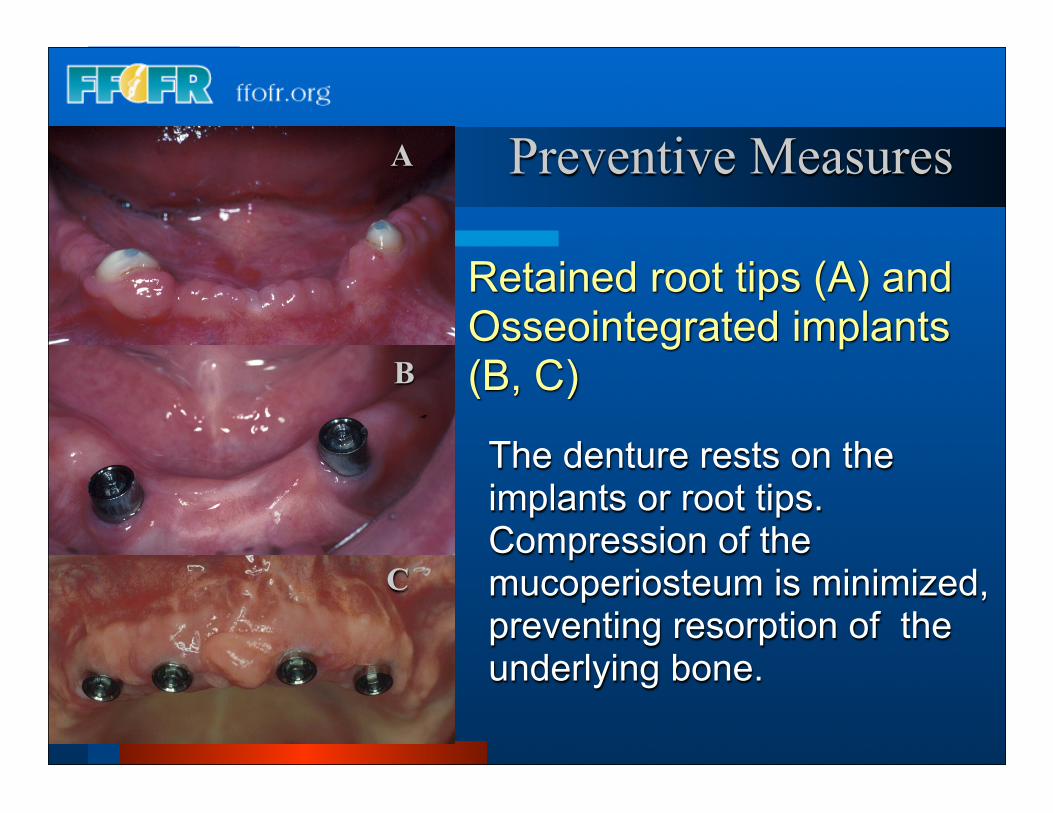
Retained root tips (A) andOsseointegrated implants (B, C)
A
B
C
The denture rests on the implants or root tips. Compression of the mucoperiosteum is minimized, preventing resorption of the underlying bone.
Preventive Measures
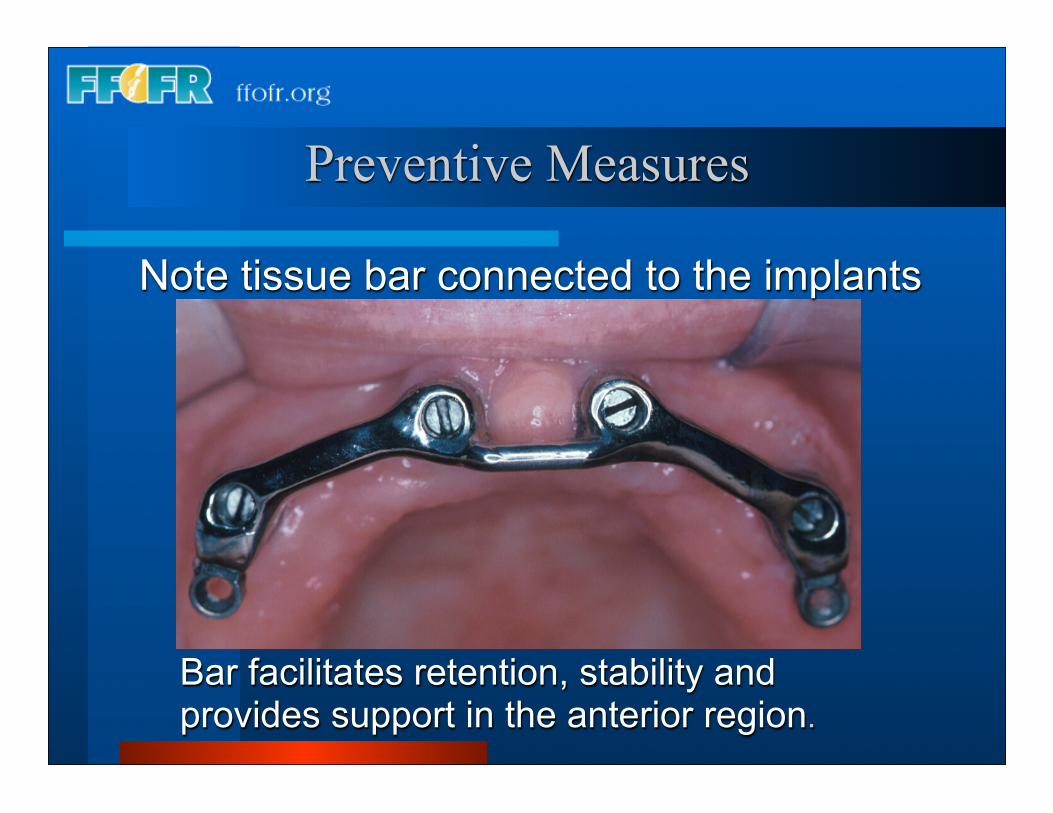
Note tissue bar connected to the implants
Bar facilitates retention, stability and provides support in the anterior region.
Preventive Measures
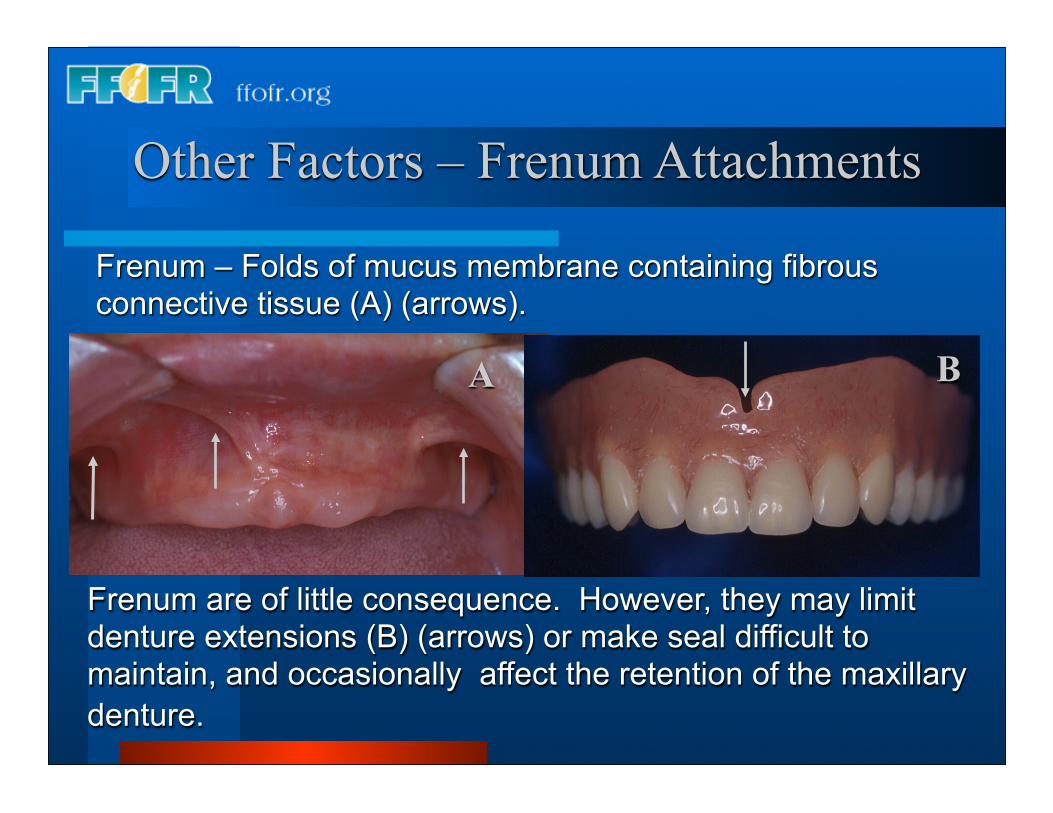
Frenum – Folds of mucus membrane containing fibrous connective tissue (A) (arrows).
A
Frenum are of little consequence. However, they may limit denture extensions (B) (arrows) or make seal difficult to maintain, and occasionally affect the retention of the maxillary denture.
B
Other Factors – Frenum Attachments
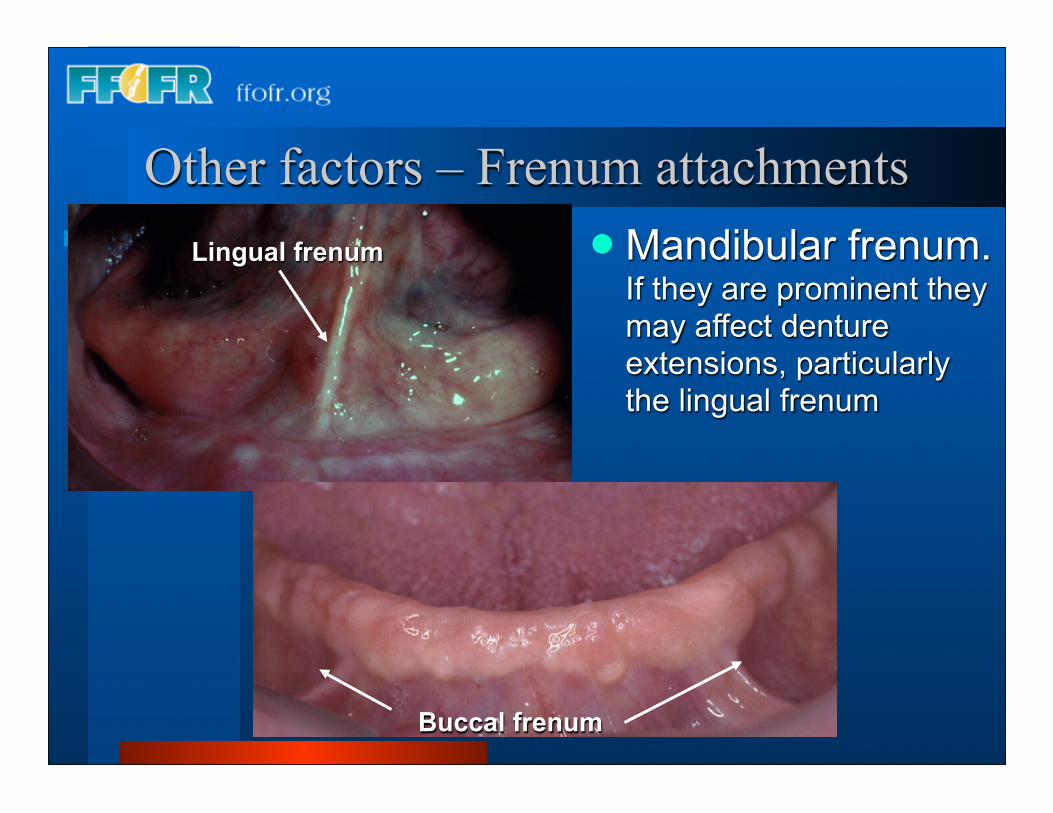
Other factors – Frenum attachments Mandibular frenum.
If they are prominent they may affect denture extensions, particularly the lingual frenum
Buccal frenum
Lingual frenum
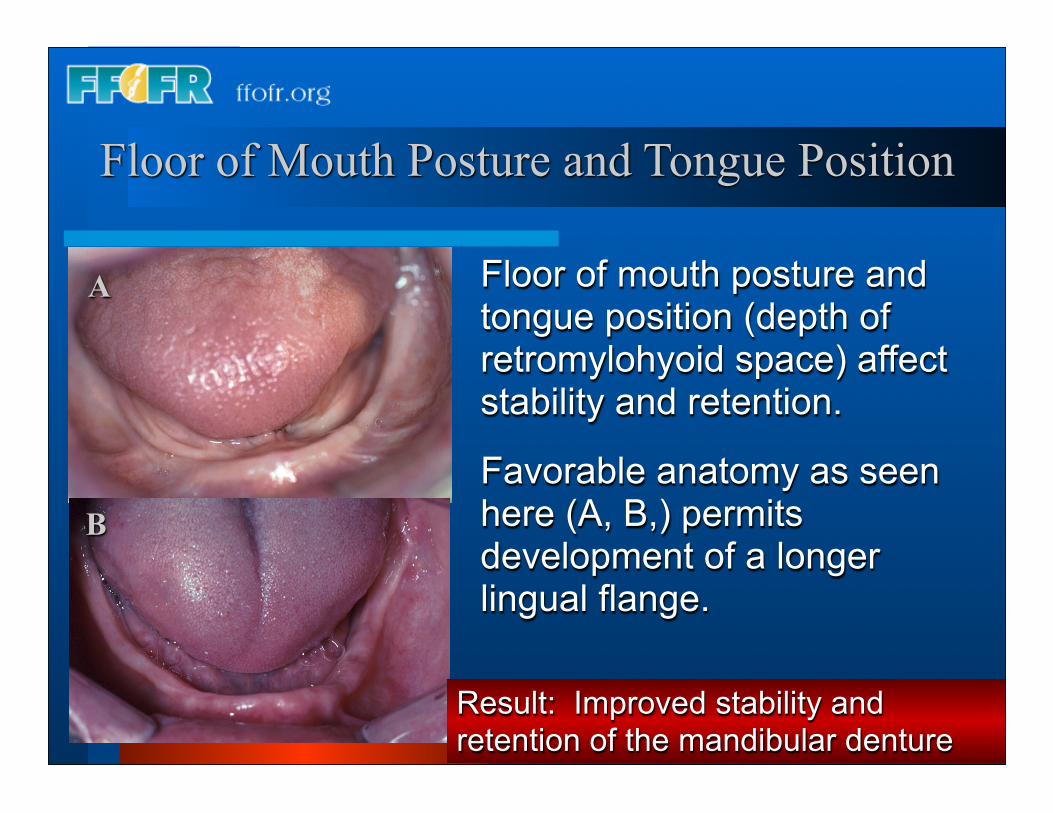
Floor of mouth posture and tongue position (depth of retromylohyoid space) affect stability and retention.
Favorable anatomy as seen here (A, B,) permits development of a longer lingual flange.
A
B
Result: Improved stability and retention of the mandibular denture
Floor of Mouth Posture and Tongue Position
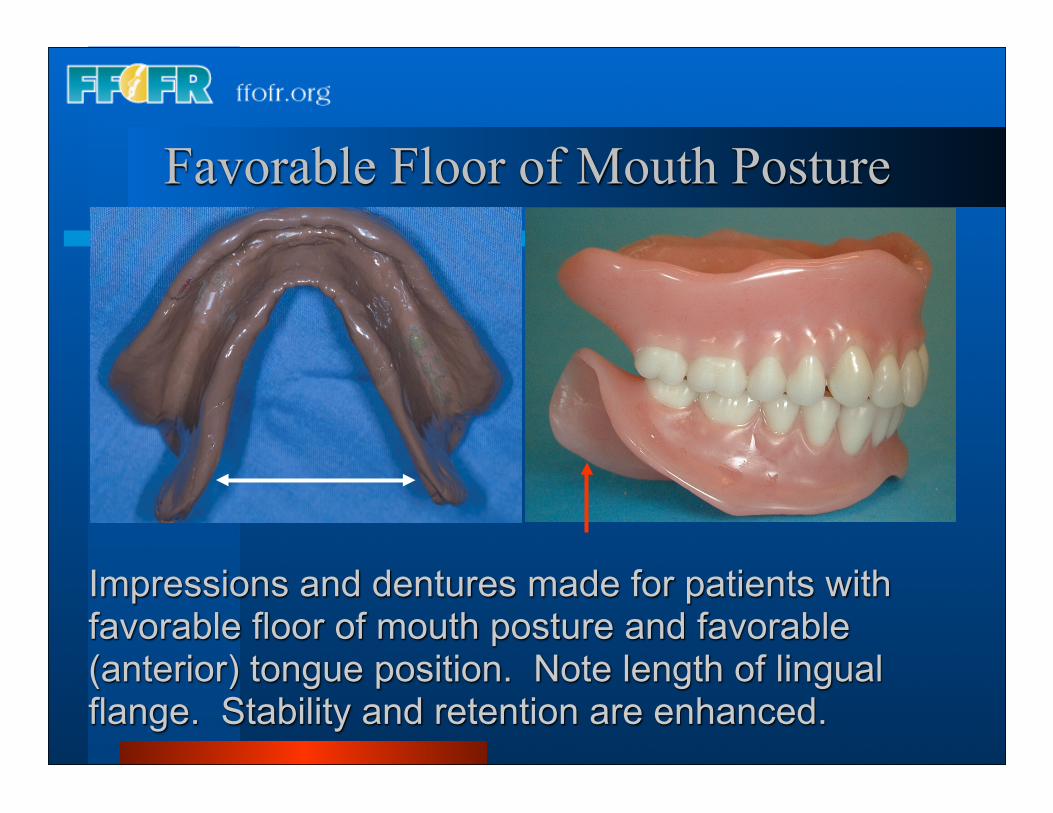
Impressions and dentures made for patients with favorable floor of mouth posture and favorable (anterior) tongue position. Note length of lingual flange. Stability and retention are enhanced.
Favorable Floor of Mouth Posture
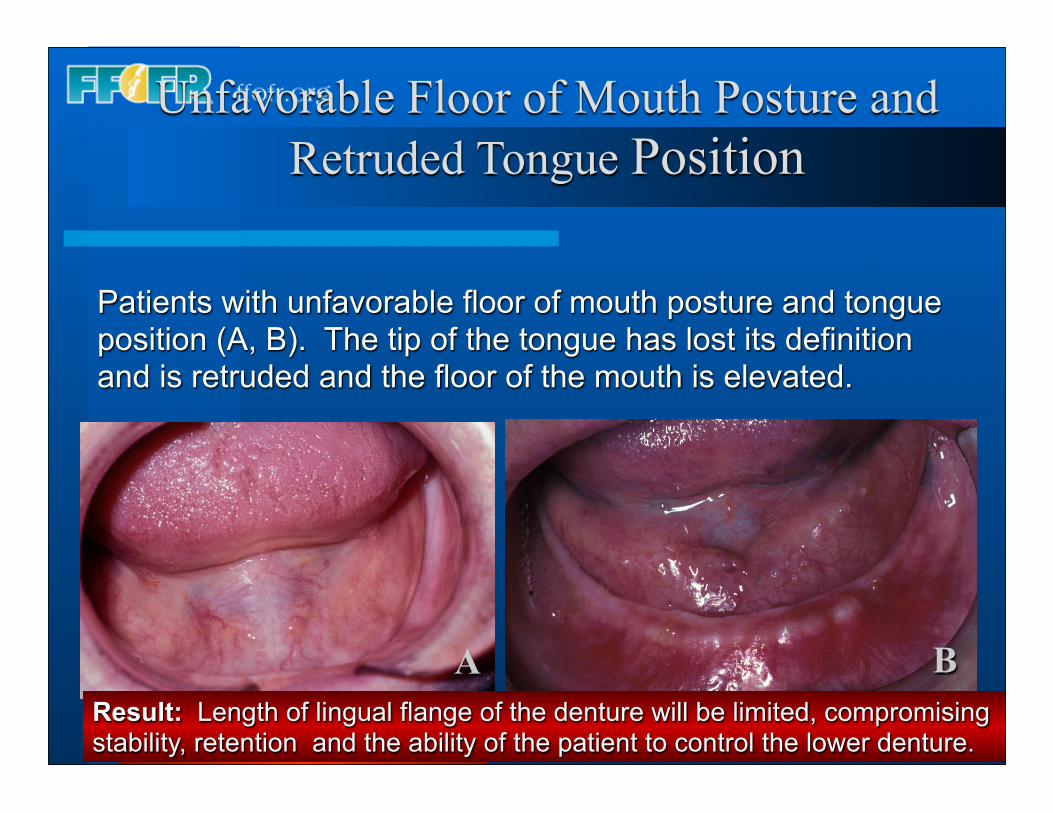
Patients with unfavorable floor of mouth posture and tongue position (A, B). The tip of the tongue has lost its definition and is retruded and the floor of the mouth is elevated.
Result: Length of lingual flange of the denture will be limited, compromising stability, retention and the ability of the patient to control the lower denture.
A B
Unfavorable Floor of Mouth Posture and Retruded Tongue Position
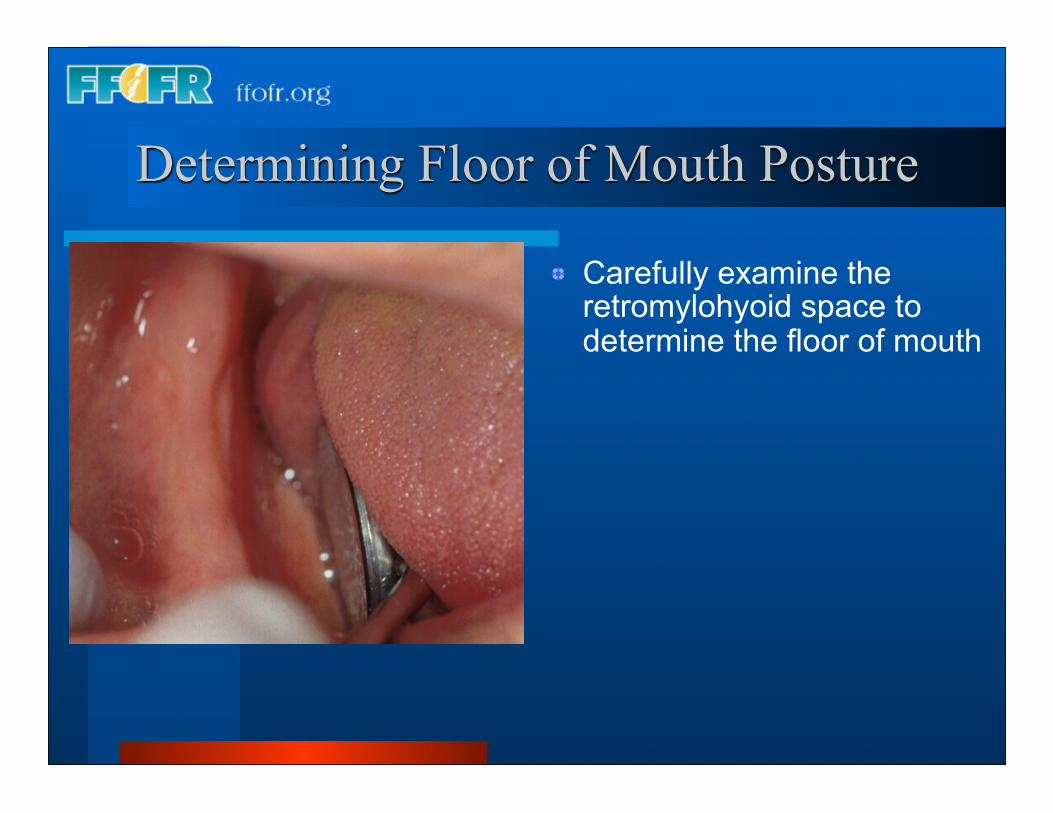
Carefully examine the retromylohyoid space to determine the floor of mouth
Determining Floor of Mouth Posture
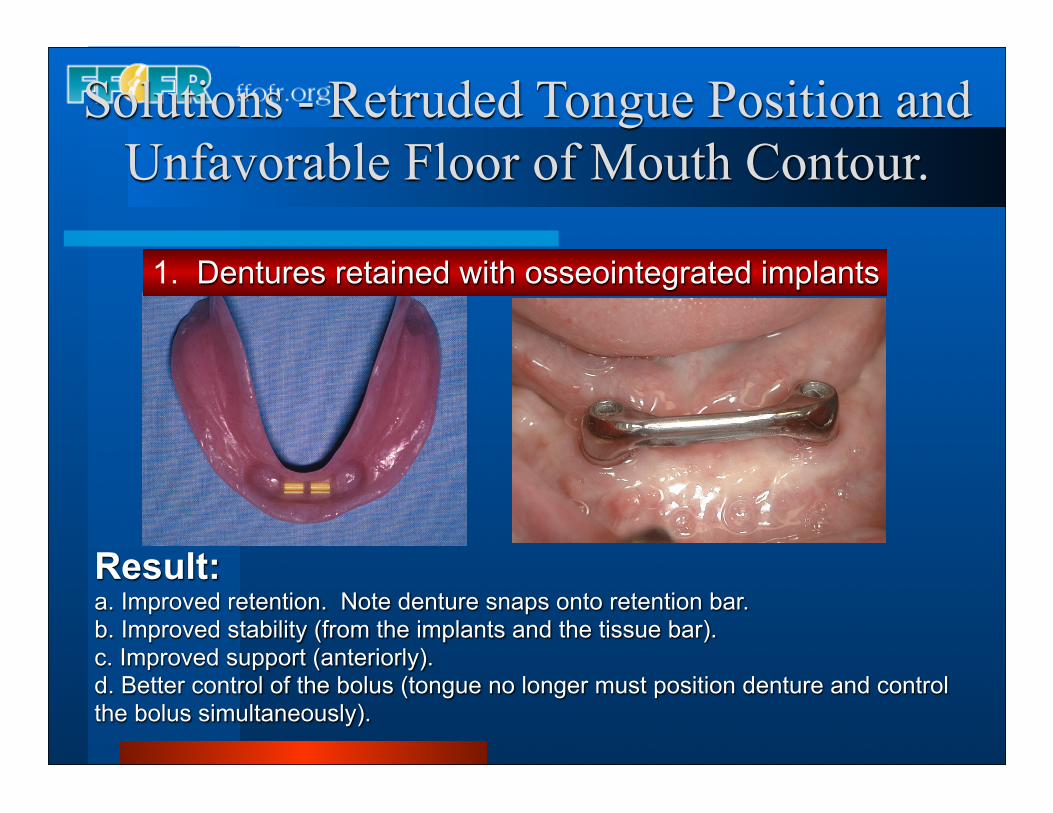
Result:a. Improved retention. Note denture snaps onto retention bar.b. Improved stability (from the implants and the tissue bar).c. Improved support (anteriorly).d. Better control of the bolus (tongue no longer must position denture and control the bolus simultaneously).
Solutions - Retruded Tongue Position and Unfavorable Floor of Mouth Contour.
1. Dentures retained with osseointegrated implants
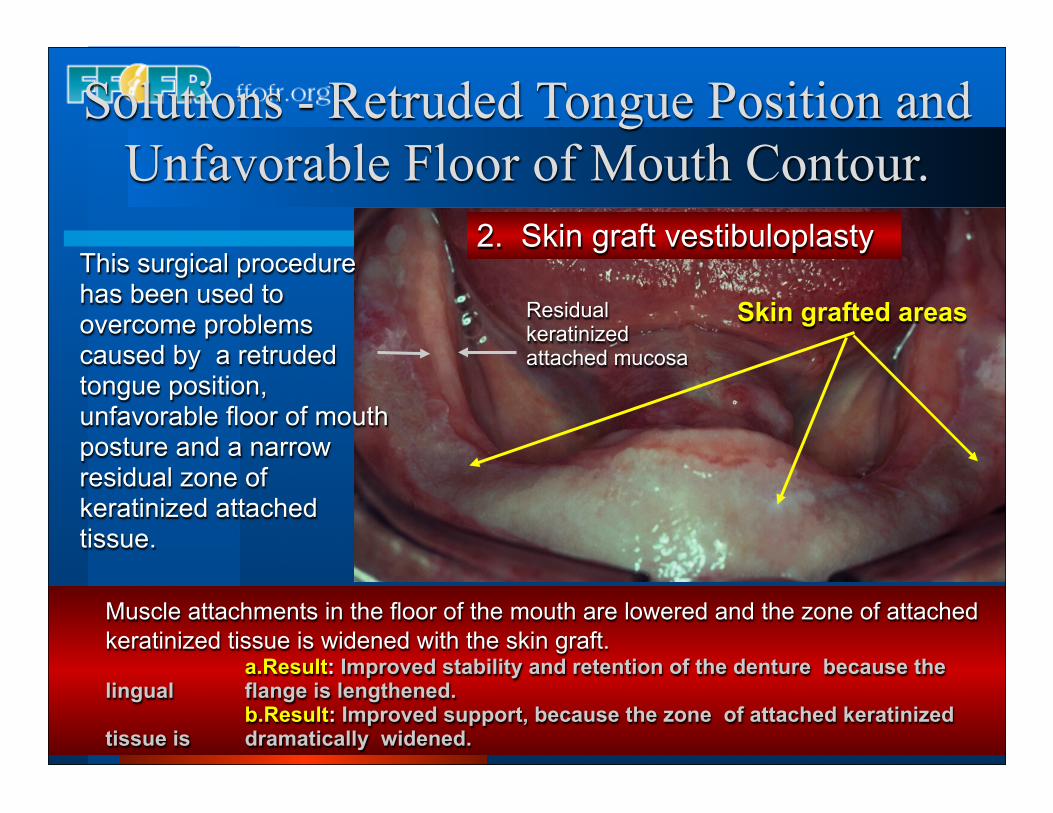
This surgical procedure has been used to overcome problems caused by a retruded tongue position, unfavorable floor of mouth posture and a narrow residual zone of keratinized attached tissue.
Muscle attachments in the floor of the mouth are lowered and the zone of attached keratinized tissue is widened with the skin graft.
a.Result: Improved stability and retention of the denture because the lingual flange is lengthened.
b.Result: Improved support, because the zone of attached keratinized tissue is dramatically widened.
2. Skin graft vestibuloplasty
Skin grafted areas
Solutions - Retruded Tongue Position and Unfavorable Floor of Mouth Contour.
Residual keratinizedattached mucosa
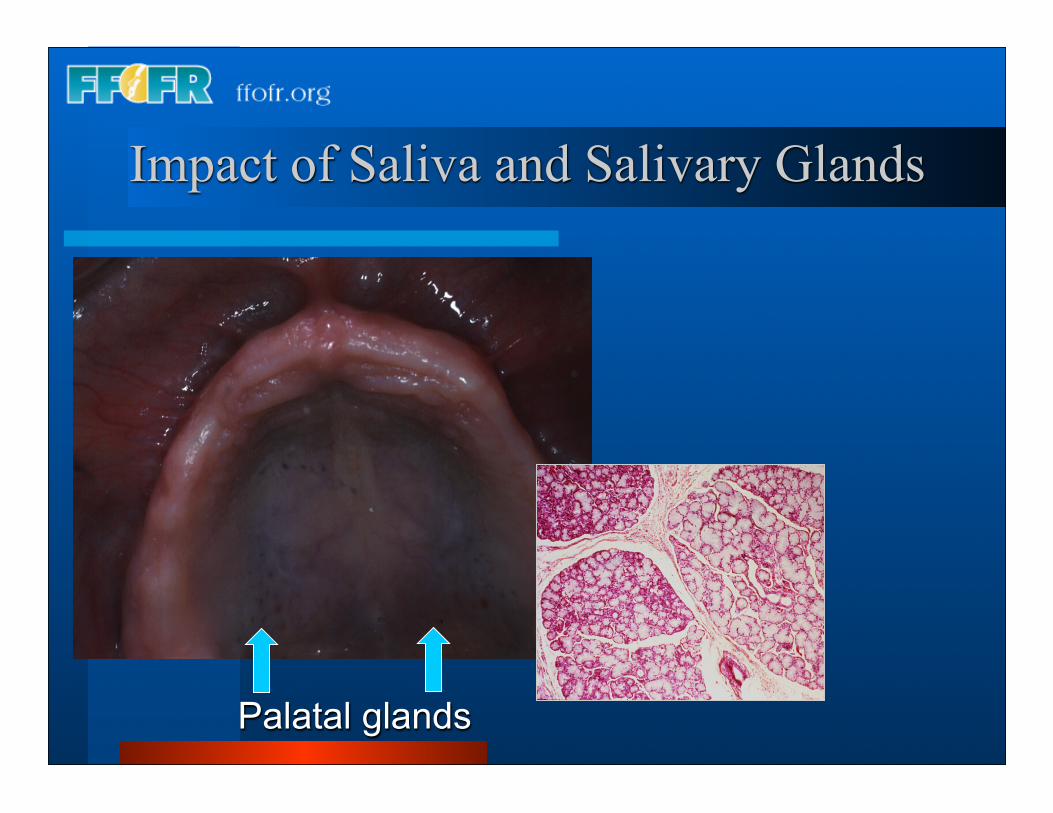
Impact of Saliva and Salivary Glands
Palatal glands
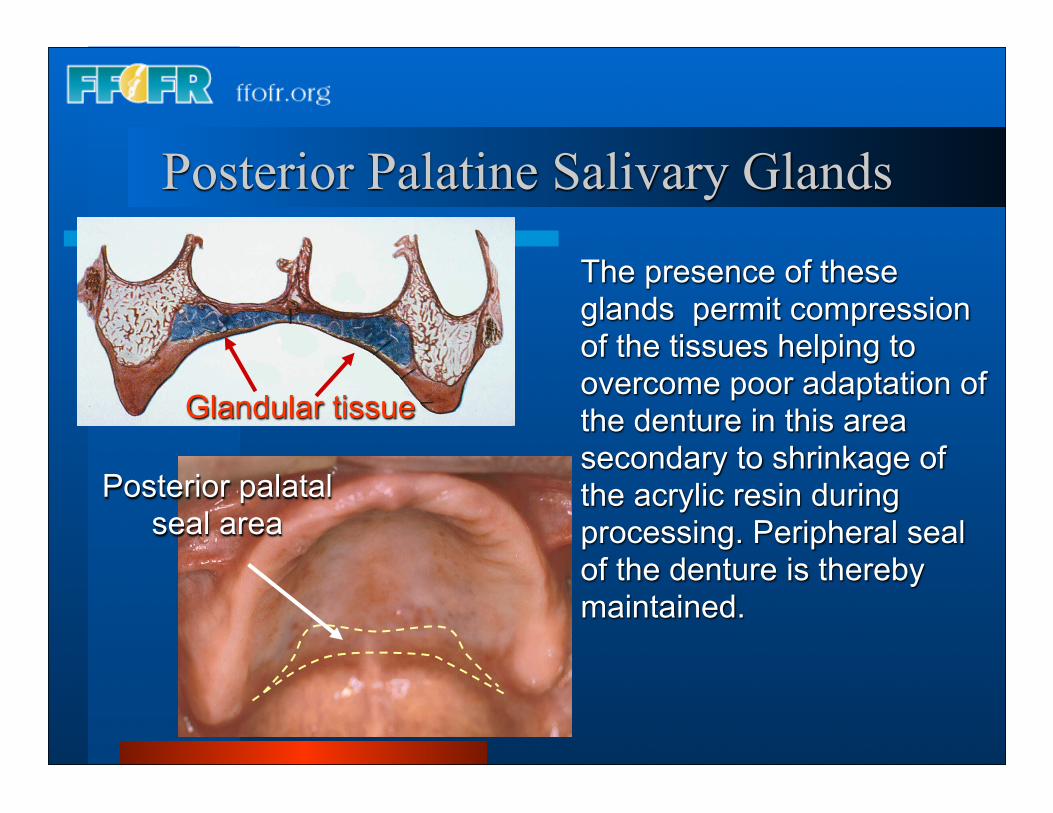
Glandular tissue
Posterior palatal seal area
The presence of these glands permit compression of the tissues helping to overcome poor adaptation of the denture in this area secondary to shrinkage of the acrylic resin during processing. Peripheral seal of the denture is thereby maintained.
Posterior Palatine Salivary Glands
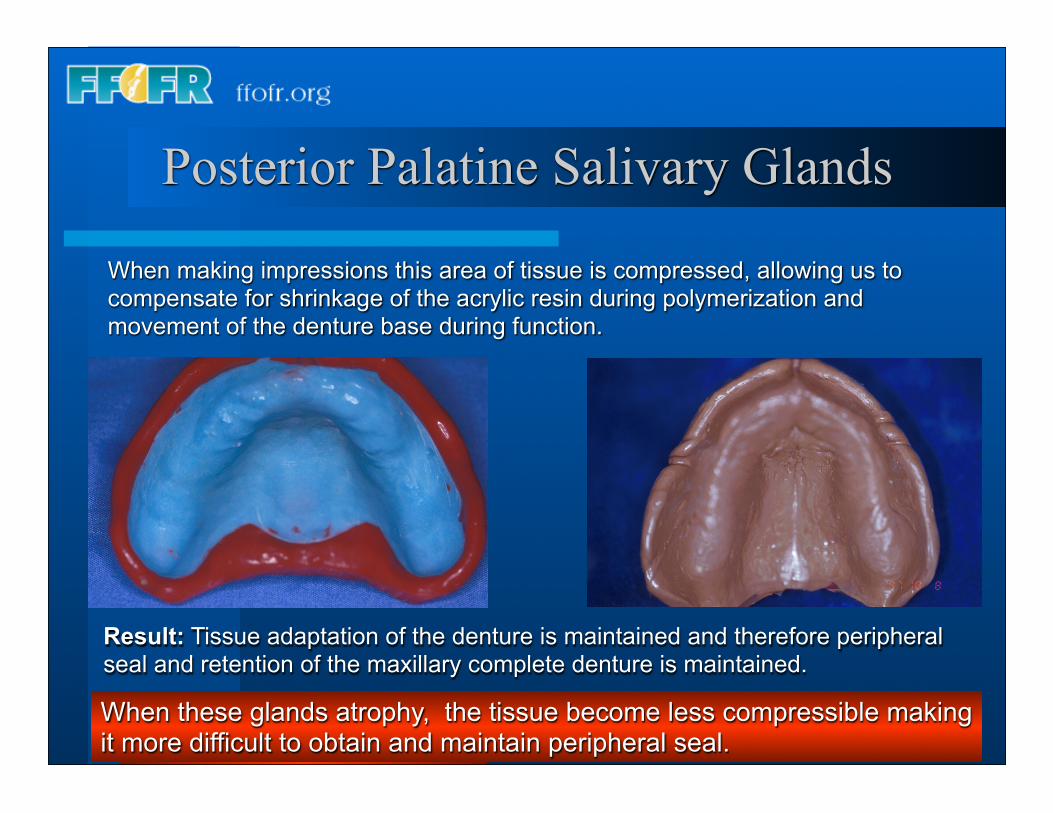
When making impressions this area of tissue is compressed, allowing us to compensate for shrinkage of the acrylic resin during polymerization and movement of the denture base during function.
Result: Tissue adaptation of the denture is maintained and therefore peripheral seal and retention of the maxillary complete denture is maintained.
When these glands atrophy, the tissue become less compressible making it more difficult to obtain and maintain peripheral seal.
Posterior Palatine Salivary Glands
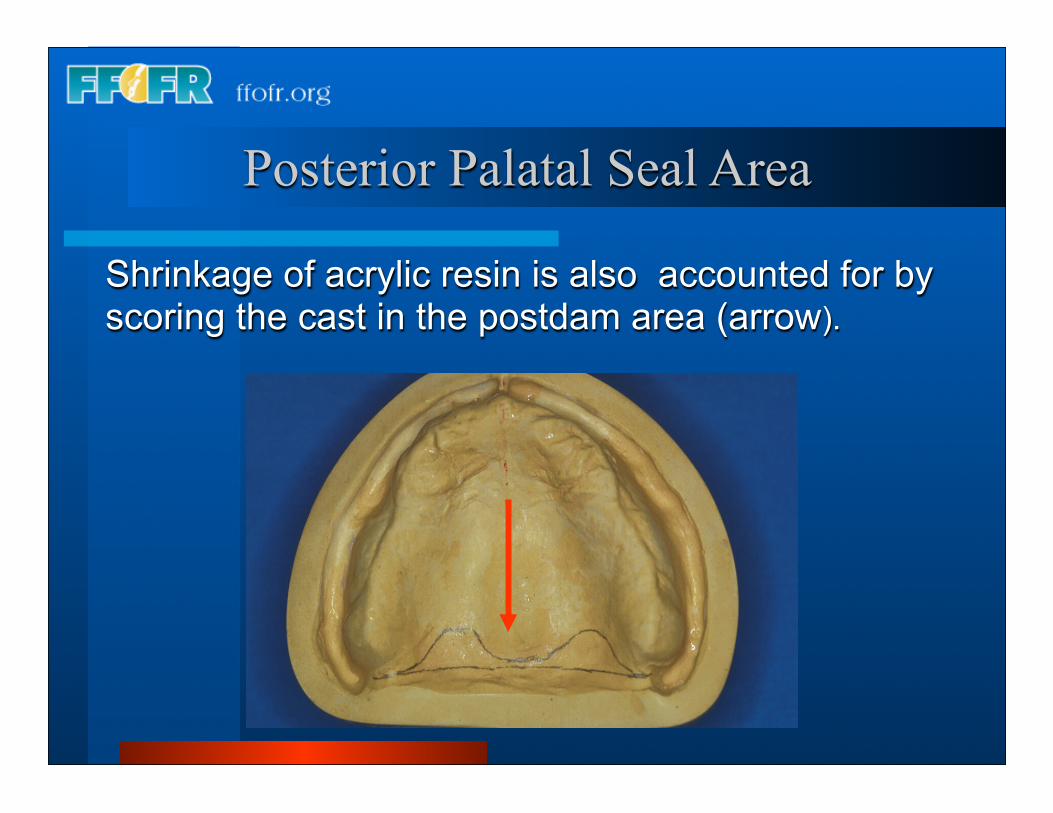
Shrinkage of acrylic resin is also accounted for by scoring the cast in the postdam area (arrow).
Posterior Palatal Seal Area
Salivary Flow and Retention
Low flow rates• Difficult to achieve and maintain peripheral seal of the maxillary denture• Compromised adhesion and cohesion.
Saliva as a Lubricant
Low flow rates• Primarily affects the mandibular denture
bearing surfaces.• Results in more friction at the mucosa-
denture interface as the mandibular denture slips and slides over the denture bearing surface during function.
Neuromuscular Control
• Some patients have the ability to manipulate their lower denture and control the bolus simultaneously, regardless of the quality of the design and construction of the denture. • Many patients with good neuromuscular control can overcome unfavorable bearing surface contours and anatomy and chew efficiently with their complete dentures and the converse is also true.
Tissue Factors Affecting Support
Mandible:• Retromolar pad• Alveolar ridge contours (the broader the more support)• Amount of attached keratinized mucosa (the more present the better the support)• Buccal shelf area (the more access and the greater the surface area the better the support
Maxilla:• Amount of keratinized mucosa• Alveolar ridge contours• Palatal shelf area and contour
Tissue Factors Affecting Stability
Mandible:• Alveolar ridge height• Floor of mouth contour (favorable vs. unfavorable)• Tongue position (anterior vs. retruded)• Neuromuscular control• Presence of flabby, moveable denture bearing surface tissues.
Maxilla:
• Alveolar ridge height• Presence of well formed maxillary, moveable denture bearing surface tissues tuberosities• Presence of flabby
Tissue Factors Affecting Retention
Mandible:
Primary Factors:• Tongue position• Floor of mouth posture• Neuromuscular control
Secondary Factors• Peripheral seal• Adhesion• Cohesion
Maxilla:• Shape of the palatal vault (peripheral seal)• Drape of the soft palate - House classification (peripheral seal)• Quality and quantity of saliva (peripheral seal)• Compressibility of posterior palatal seal area (peripheral seal)• Presence of well shaped tuberosities• Height of alveolar ridge (resistance to lateral displacement)
Clinical exam - Prosthodontic Assessment
Assessment of existing dentures• Retention• Stability• Vertical dimension of occlusion• Centric relation• Esthetics
Prosthodontic Assessment
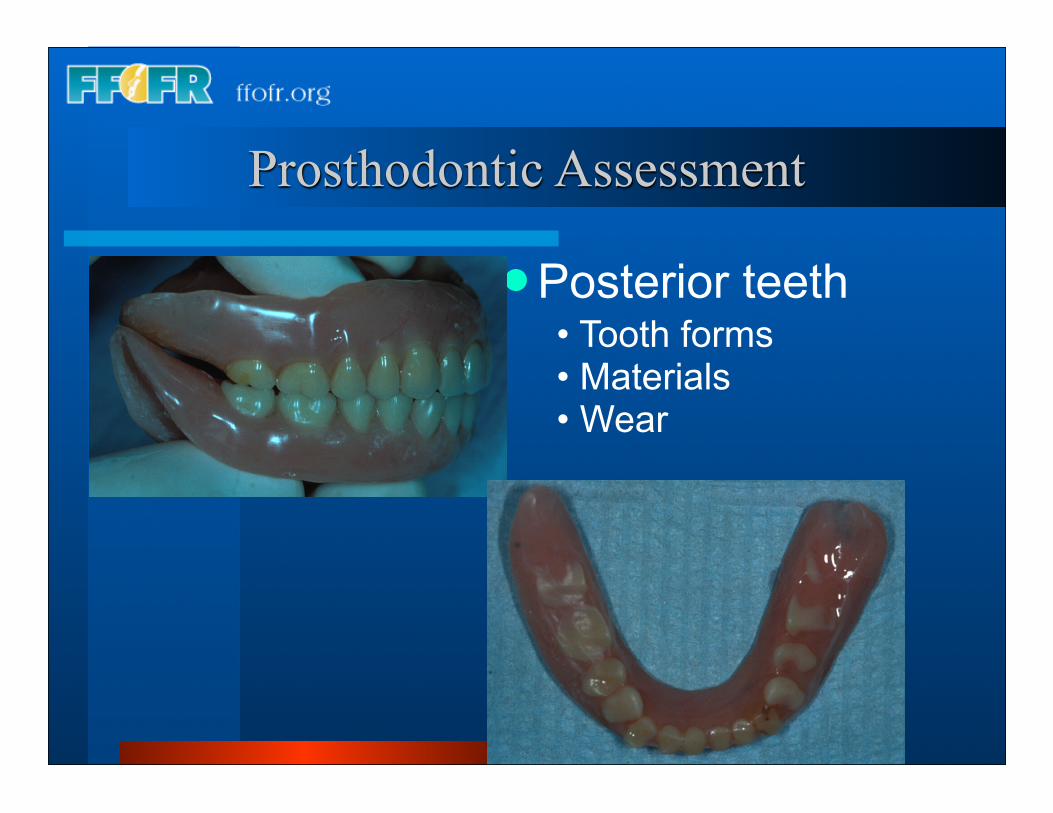
Posterior teeth• Tooth forms• Materials• Wear
Prosthodontic Assessment
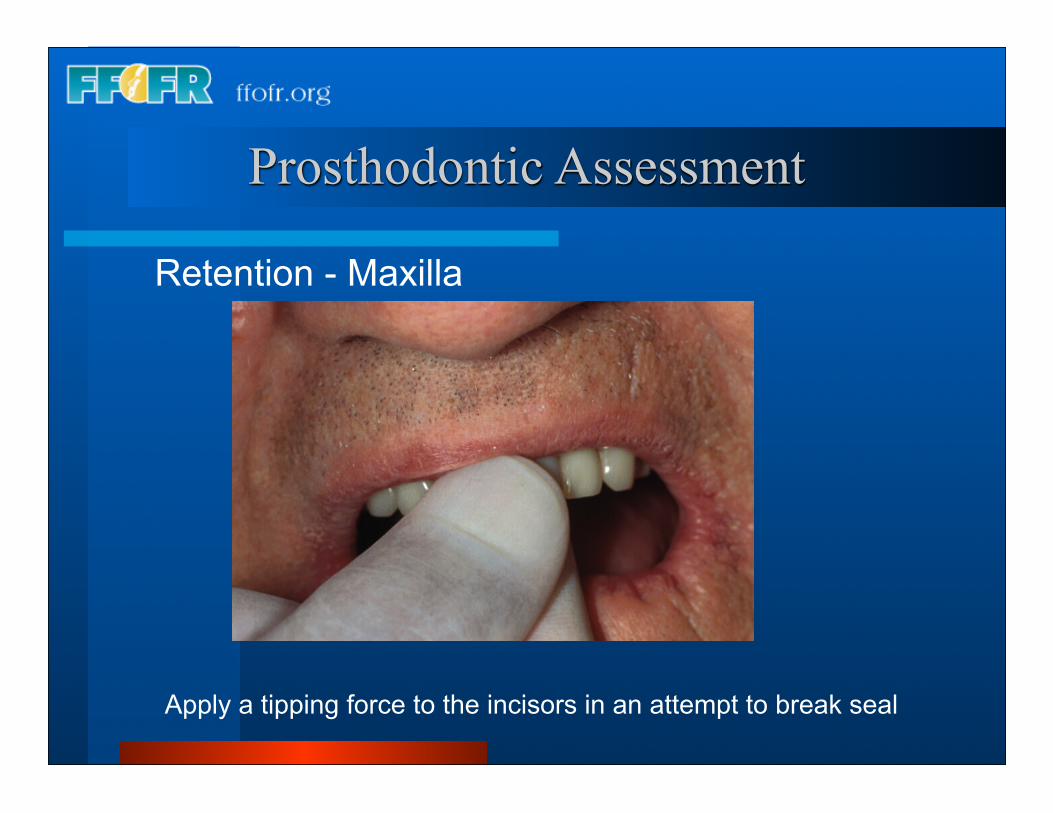
Retention - Maxilla
Apply a tipping force to the incisors in an attempt to break seal
Prosthodontic Assessment
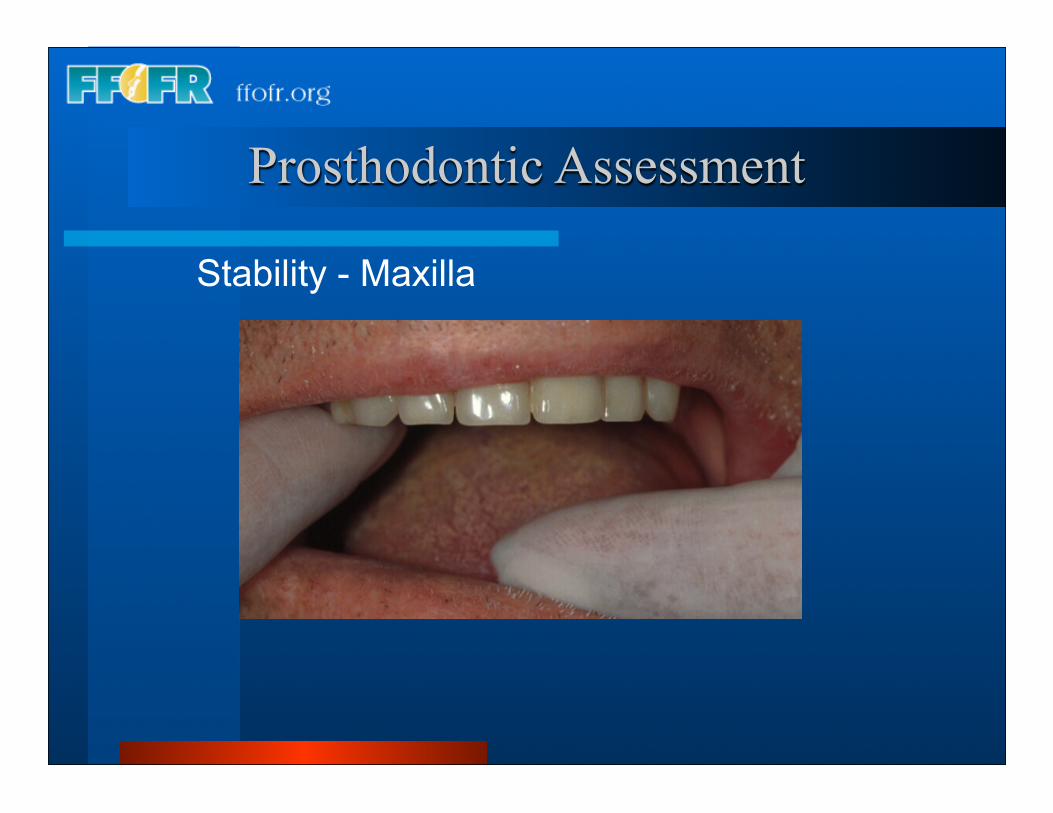
Stability - Maxilla
Prosthodontic Assessment
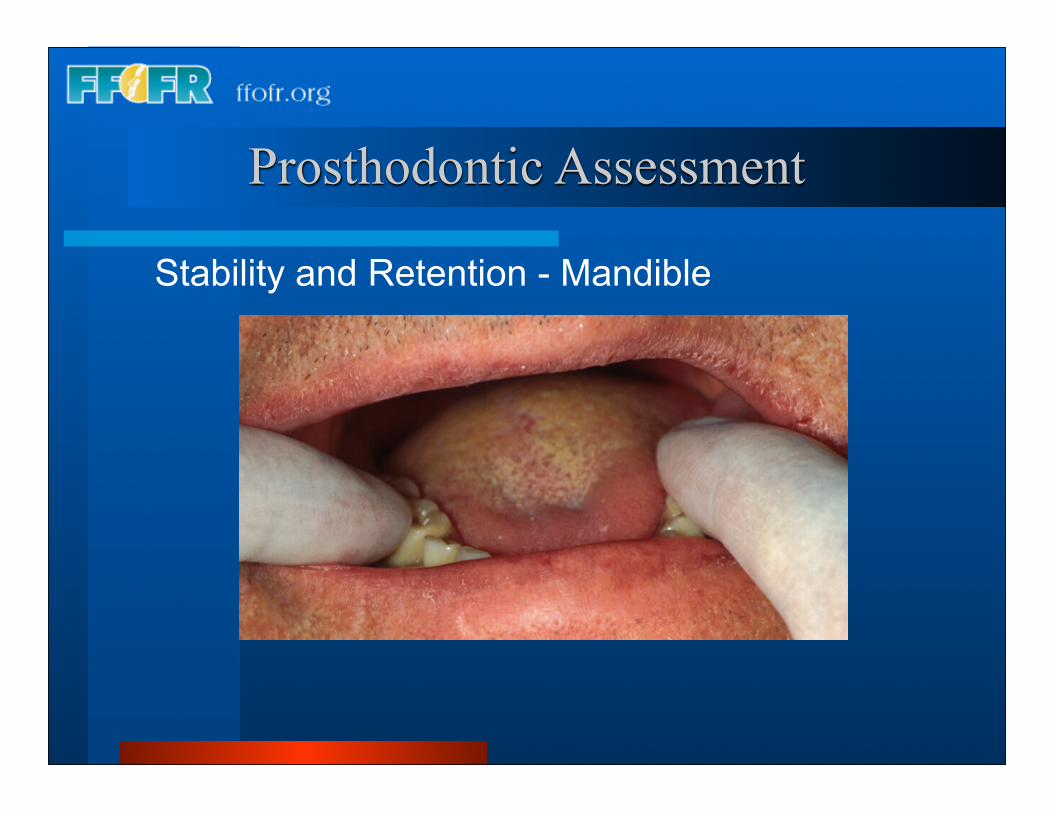
Stability and Retention - Mandible
Prognosis based upon:
• Bearing surface anatomy, tongue position and floor of mouth posture
• Neuromuscular control• Denture history
• Psychological classification
Visit ffofr.org for hundreds of additional lectures on Implant Dentistry, Removable Partial Dentures, Esthetic Dentistry and Maxillofacial Prosthetics.
The lectures are free and available upon registering for the site.
Our objective is to create the best and most comprehensive online programs of instruction in Prosthodontics on the internet.