comparing two fronto-orbital advancement strategies to treat trigonocephaly in metopic synostosis
TRANSCRIPT
Accepted Manuscript
Comparing Two Fronto-orbital Advancement Strategies to Treat Trigonocephaly inMetopic Synostosis
Philipp Metzler, MD,DMD Harib H. Ezaldein, BS John A. Persing, MD Derek M.Steinbacher, MD, DMD
PII: S1010-5182(14)00129-2
DOI: 10.1016/j.jcms.2014.04.006
Reference: YJCMS 1782
To appear in: Journal of Cranio-Maxillo-Facial Surgery
Received Date: 2 March 2014
Revised Date: 11 April 2014
Accepted Date: 15 April 2014
Please cite this article as: Metzler P, Ezaldein HH, Persing JA, Steinbacher DM, Comparing Two Fronto-orbital Advancement Strategies to Treat Trigonocephaly in Metopic Synostosis, Journal of Cranio-Maxillofacial Surgery (2014), doi: 10.1016/j.jcms.2014.04.006.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Comparing Two Fronto-orbital Advancement Strategies to Treat Trigonocephaly in
Metopic Synostosis
Philipp Metzler (MD,DMD), Harib H Ezaldein (BS); John A Persing (MD).; Derek M
Steinbacher (MD, DMD)
Plastic and Reconstructive Surgery
Yale University School of Medicine
330 Cedar St, BB 3rd Floor
New Haven, CT 06520
Corresponding author:
Derek M. Steinbacher MD, DMD
Plastic and Craniomaxillofacial Surgery, Yale University School of Medicine
330 Cedar St, BB 3rd Floor
New Haven, CT 06520
Tel.: +1 (203) 785 4559
Fax: +1 (203) 785 7514
E-mail address: [email protected]

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
1
Summary
Background: Trigonocephalic treatment entails frontoorbital reshaping of the forehead,
increasing bitemporal dimensions, and advancing lateral orbits. Various techniques can achieve
this, but no consensus exists regarding effects on long-term skull growth. Overcorrecting
forehead dimensions is one strategy though preserving a vascularized fronto-orbital bar can
influence future growth. We therefore seek to craniomorphologically compare fronto-orbital
advancement (FOA), using bandeau widening and advancement, to a pedicled “tilt” procedure to
assess whether adequate 3D remodeling is achieved.
Methods: Demographic and computed tomographic data was recorded. Pre-and post-
craniometric measurements were performed for the endocranial bifrontal angle, orbital plane
angle, anterior advancement and the interzygomaticofrontal suture distance.
Results: 40 CT scans were analyzed, with similar demographics. No perioperative complications
were encountered. The endocranial bifrontal angle increased in the FOA (p=0.00026) and tilt
groups (p=0.00297), along with the orbital plane angles (FOA, p=0.020498; tilt, p=0.07371), the
anterior advancement (FOA, p=0.00932; tilt, p=0.05823), and the interzygomaticofrontal suture
distance(FOA, p=0.001241; tilt, p=0.07811).
Conclusions: Both techniques improve frontoorbital dimensions for correction of metopic
synostosis. In severe trigonocephaly phenotypes, the FOA allows a greater magnitude of
expansion and overcorrection, but compromises preservation of a vascularized leash. The “tilt”
procedure possesses the benefit of near-anatomic bandeau remodeling, while potentially
improving long-term growth.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
2
Keywords
Tilt procedure, fronto-orbital advancement, trigonocephaly, metopic, suture, metopic synostosis,
cranial vault remodeling.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
3
Level of Evidence: LEVEL II (PRS, Comparison with gold-standard
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
4
Introduction
Treatment goals for metopic synostosis include expansion and advancement of the supralateral
bandeau, widening of the temporal dimensions, and rounding the forehead. Several techniques
have been espoused to achieve these objectives, and have evolved over time (Tessier, 1967;
Tessier, 1971; Hoffman and Mohr, 1976; Marchac, 1978; Marchac and Renier, 1979;
Obwegeser, 2009). In addition to aesthetic correction, a marked increase of the endocranial
volume within the anterior cranial fossa occurs (Renier et al., 1982; van der Meulen, 2012). This
allows expansion of the brain into the area, with an increased blood supply and mitigation of
intracranial hypertension providing a corollary benefit to brain development and psychomotor
abilities (Renier et al., 1982; Sidoti et al., 1996; Schaller et al., 2012). However, traditional
expansion techniques have shown a tendency toward the original deformity with long-term
surveillance (Cohen et al., 1991; Fearon et al., 2009). This subsequent supralateral orbital rim
restriction is thought secondary to diminished intrinsic growth, inadequate surgical expansion,
and devascularization of segments at the time of advancement or some combination (McCarthy
et al., 1990; Cohen, 1996; Losken et al., 1996). Overcorrection has been advocated to account for
the anticipated relapse or growth restriction (Fearon, 2008; Fearon et al., 2009). Another
strategy suggested is to maintain a vascularized pedicle to the advanced bandeau while “tilting”
the segment forward (Hoffman and Mohr, 1976; Patel et al., 2012).
In our unit, both surgical techniques, the modified “fronto-orbital advancement” and the “tilt-
procedure” are routinely used for metopic synostosis correction (Selber et al., 2007; Patel et al.,
2012). The purpose of this study is to objectively analyze the frontoorbital morphology achieved
comparing these two distinct techniques.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
5
Materials and Methods
This is a retrospective analysis performed in concordance with the Yale University Institutional
Review Board (protocol: HIC# 1101007932). Consecutive infants with metopic synostosis who
underwent treatment by the senior authors (J.A.P. or D.M.S.) at Yale were included.
Demographic and surgical data were tabulated, computed tomographic scan information were
obtained for both patients groups (fronto-orbital advancement (FOA, figure 1) and tilt procedure
(TP, figure 2). Technical details of each procedure is described in Figures 1 and 2, based on
previous descriptions (Tessier, 1967; Hoffman and Mohr, 1976; Marchac, 1978; Patel et al.,
2012). CT scan images were digitized from pre- and postoperative timepoints for each group and
analyzed using a surgical planning program (SurgiCase; Materialise, Leuven, Belgium).
Anatomic landmarks, measurements, and angles are shown in Table 1 and Figure 3. Percentages
of intra- and intergroup analysis were calculated (Tessier, 1967; Hoffman and Mohr, 1976;
Marchac, 1978; Patel et al., 2012). Statistical analysis involved the paired two-sample t-test. A
significant difference was noted with p-values <0.05.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
6
Results
Demographic data
Exactly 40 CT scans were included for analysis, 10 pre- and postoperative scans for the fronto-
orbital advancement and 10 pre- and postoperative scans for the tilt procedure. The FOA group
had 8 males and 2 females, with mean pre-op and post-op ages of 8 and 9.6months respectively.
The tilt group had 7 males and 3 females, with mean pre-op and post-op ages of 5 and 7.9
months. The average follow up time for the FOA and tilt groups is 1.5 months and 2.85 months
correspondingly. Post-operatively, all patients showed uneventful healing.
Endocranial bifrontal angle (ECA)
The endocranial bifrontal angle averaged 127.0° pre-op and 151.2° post-op, with a mean percent
change of 19.0% for the FOA group (p=0.00026). It averaged 129.3° preoperatively and 143.9°
post-operatively with a mean percent change of 11.3% for the tilt group (p=0.00297)(see Table
2).
Orbital plane angle (OPA)
The orbital plane angle in the FOA group measured on average 121.7° preoperatively and 132.0°
postoperatively, with an average 19 % change (p=0.020498). For the tilt procedure group, the
preoperative angle averaged at 119.8° and 129.9° postoperatively with an average correction of
11.3% (p=0.07371)(see Table 3).
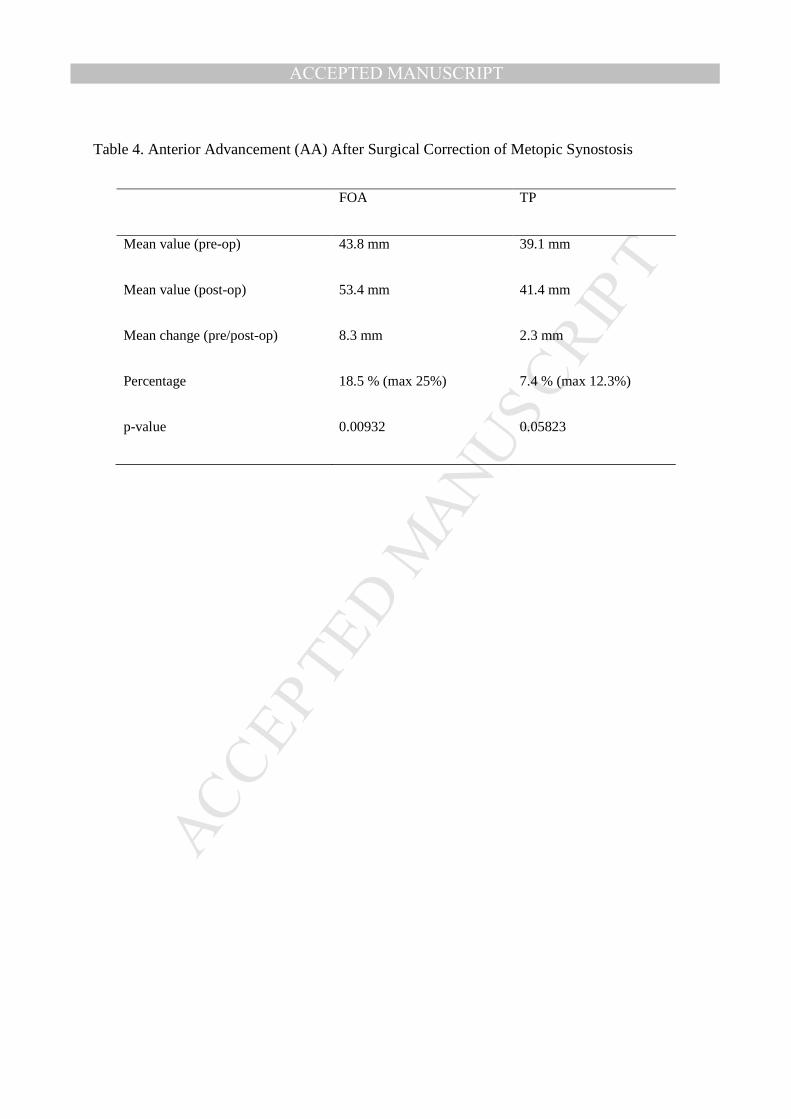
Anterior advancement (AA)
The anterior advancement distance for the FOA group averaged at 43.8 mm preoperatively and
53.4 mm postoperatively, with an average percent change of 18.5 % (p=0.00932). The mean

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
7
preoperative AA in the tilt group is 39.1 mm and 41.4 mm, postoperatively, with an average
percent change of 7.4 % (p=0.05823) (see Table 4).
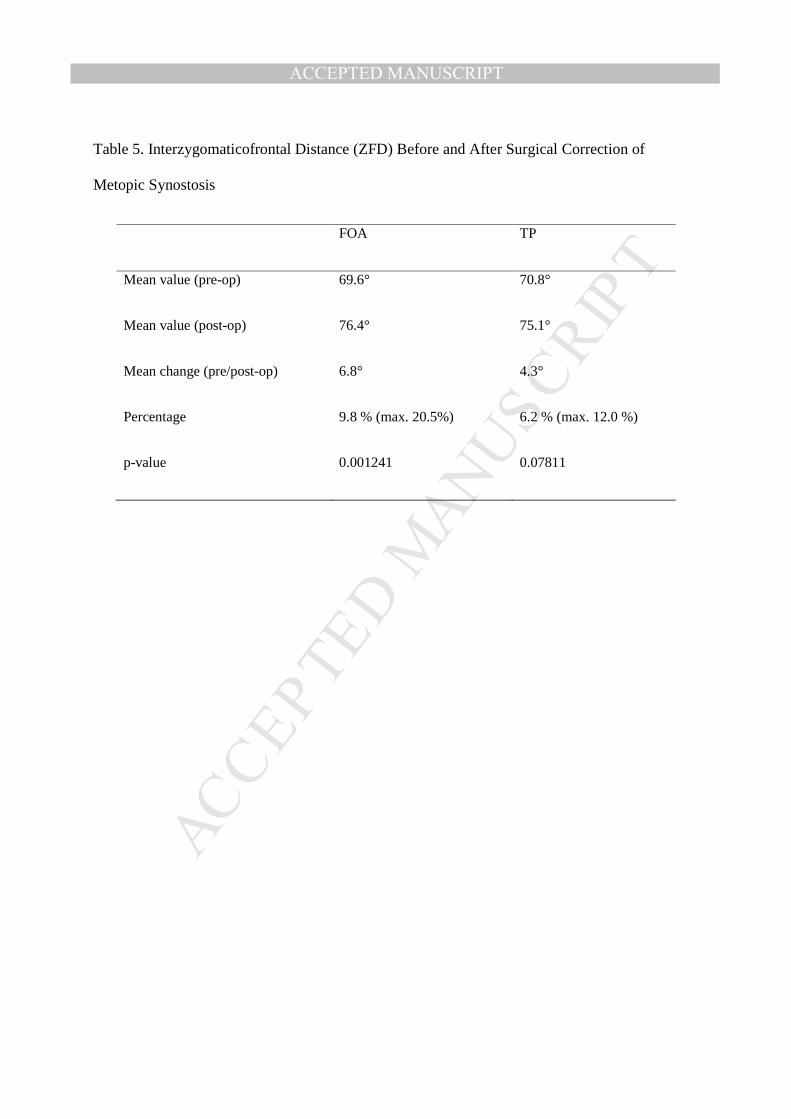
Interzygomaticofrontal suture distance (ZFD)
The interzygomaticofrontal suture distance (ZF-ZF) distance for the FOA group averaged at
69.55 mm preoperatively and 76.38 mm postoperatively, with an average percent change of
9.81% (p=0.001241). The mean preoperative inter-ZF distance in the tilt group is 70.78 mm and
75.14 mm, postoperatively, with an average percent change of 6.16% (p=0.07811). These values
are listed in Table 5
Statistical evaluation showed in all measurements (ECA, OPA, AA, ZFD) significant higher (p ≤
0.05) postoperative changes in the FOA than in the Tilt group.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8
Discussion
A variety of surgical strategies have been proposed to correct the characteristic trigonocephalic
stigmata seen in metopic synostosis. Advancing the supralateral orbit, expanding the temporal
dimensions, and rounding the forehead are the critical features of most techniques. In 1967,
Tessier et al. introduced the fronto-orbital advancement as the key procedure to correct forehead
dysplasia (Tessier, 1967; Tessier, 1971). Evolution and modification of this original technique
has been reported with excellent results (Hoffman and Mohr, 1976; Persing et al., 1990; Jimenez
et al., 2002; Knoll et al., 2005; Fearon, 2008; Shah et al., 2012). Nevertheless, hollowing, and
contour irregularities, as a function of return to original deformity, occur requiring revisions
(Cohen et al., 1991; Fearon et al., 2009; Steinbacher et al., 2011). The principle strategy to
minimize secondary procedures is to overexpand and overcorrect the supralateral dimensions
(Fearon, 2008; Fearon et al., 2009). The concept of maximizing perfusion of osseous segments
while limiting soft tissue forces and tension is also important (McCarthy et al., 1990; Cohen,
1996; Losken et al., 1996).
An ideal technique achieves both near anatomical correction and overcorrected dimensions to
account for future growth impairment (Fearon, 2008; Metzler et al., 2013). Further, the
technique should encourage brain-expansion and - growth. Beyond creating an excess of space
for the brain to expand, vascular preservation of the fronto-orbital bar may exhibit a major
influence on promotion e.g. growth and development and the brain-endocranial interface (Cohen,
1996; Losken et al., 1996; Francis et al., 2011).
The classic one-piece fronto-orbital advancement has long been the most common technique
used to correct metopic craniosynostosis and is still considered the gold standard. Evolution of

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
9
this technique has involved a two-piece split, with intervening midline bone graft, and bone
shims placed from the orbital roof to the anterior cranial fossa (Selber et al., 2007; Francis et al.,
2011).
A number of craniometric analyses have been performed to shed insight on both the abnormal
findings characterizing metopic synostosis and the surgical morphological goals that should be
achieved with correction (Posnick et al., 1994; Havlik et al., 1999; Pearson et al., 2008; Beckett
et al., 2012; Kellogg et al., 2012). Three-dimensional planning and analysis has been proposed as
an effective means to achieve an ideal result, based on objective angles and parameters (Diluna
and Steinbacher, 2012; Shah et al., 2012). Similarly, an “average” frontoorbital bandeau guide
has been developed, based on a series on unaffected infants, and may be used to gauge treatment
(Burge et al., 2011). There is no consensus as to the ideal parameters of expansion and
positioning of the frontoorbital bandeau. Certainly with the advent of limited suturectomy
techniques and springs, there is no emphasis on temporal expansion and advancement, relying
solely on future brain growth. Most would agree that severe trigonocephaly, as classified by
Beckett et al., require a more complete, 3-dimentional remodeling technique involving fronto-
orbital bandeau repositioning (Francis et al., 2011; Beckett et al., 2012).
Accepting the tenet that in moderate-severe trigonocephaly, the angle of the frontoorbital bar
needs to be opened and the temporal aspects widened, we sought to investigate morphologic
differences between two techniques developed conserving these goals. To the authors’
knowledge, no study exists comparing various surgical techniques for trigonocephaly correction
in current literature. Therefore, the aim of this study was to compare the data of metopic
synostotic patients following the modified “fronto-orbital advancement” and the” tilt procedure”.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
10
Statistical analysis of both techniques showed significant differences between the pre- and
postoperative measurements focusing the fronto-orbital rim correction. Both techniques enable
the surgeon to positively influence the characteristic trigonocephalic stigma in all patients.
Within the FOA group, a large magnitude of correction is possible, consistent with the strategy
of overcorrection to account for future diminished growth. However, this is at the expense of
stripping all vascularized attachments to the bone. Inherently, because the tilt procedure
preserves the integrity of the fronto-nasal suture, the amount of sagittal correction is limited.
However, the amount of advancement required at the nasofrontal region is typically minimal.
Additionally, the tilt maneuver obviates an osseous step off above the nose, which may limit the
need for postoperative esthetic correction in this area. Another advantage of the ‘tilt procedure’
is the possibility for synchronous correction of zygomatic hypoplasia (Persing et al., 1990).
Technically, the tilt procedure, maintains the medial and lateral attachments of the frontonasal
and zygomaticofrontal sutures, and blood supply from the supraorbital and supratrochlear
arteries, and anterior branch of the superficial temporal artery. The superior and inferior latero-
orbital blood supply is maintained with periosteal preservation and connections of the deep
supraorbital and temporal with the zygomaticofacial and temporal arteries (Rene, 2006). The
preserved vascularization of this fronto-orbital segment may play a pivotal role in frontal sinus
development and function. McCarthy and colleagues noted a significant failure of the frontal
sinus development after FOA and complete periosteal stripping (McCarthy et al., 1990).
Importantly, the “pedicled” fronto-orbital segment may have a beneficial impact on long-term
growth results (Cohen, 1996; Losken et al., 1996; Patel et al., 2012).
The tilt procedure carries benefit when applied to younger infant, as this group has malleable
osseous segments, allowing greenstick. However, earlier surgical intervention is typically

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
11
associated with a worsened degree of growth restriction. The preserved vascular supply in this
technique may offset this concern, not to mention the likely benefit of earlier surgery on
neuropsychiatric outcomes (Kapp-Simon, 1994). The degree of surgical correction achievable
using the tilt would certainly be well applied to the mild and moderate metopic synostosis. In
severe trigonocephalic phenotypes, the larger magnitude of movement possible with the FOA,
may allow for distinct 3D correction and overcorrection. Long-term analysis is necessary to fully
vet the concepts of over-expansion, growth promotion, and secondary deformities comparing the
two techniques.
Future work will focus on meticulous documentation of surgical age, phenotypic classification,
technique and magnitidue of correction, followed by close, long-term anthropometric analysis
shed further insight into the disease process and treatment strategies in metopic synostosis
(Metzler et al., 2013).
Conclusions
Two techniques for correction of trigonocephaly are compared. Both the tilt and FOA effectively
achieve surgical goals of frontoorbital expansion and advancement. The FOA allows for
overcorrection, with larger magnitude of advancement and expansion. Conversely the tilt
preserves osseous blood supply, which may portend improved growth outcomes. Future work is
geared toward longitudinal follow-up of these patients in relation to morphology and growth
outcomes
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
12
Conflict of Interest Statement:
None of the authors has any financial or commercial interest in any aspect of this article.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
13
References
Beckett JS, Chadha P, Persing JA and Steinbacher DM: Classification of trigonocephaly in metopic
synostosis. Plastic and reconstructive surgery 130: 442e-447e, 2012.
Burge J, Saber NR, Looi T, French B, Usmani Z, Anooshiravani N, et al.: Application of CAD/CAM
prefabricated age-matched templates in cranio-orbital remodeling in craniosynostosis. The
Journal of craniofacial surgery 22: 1810-1813, 2011.
Cohen SR: Vascularized fronto-orbital advancement. The Journal of craniofacial surgery 7: 228, 1996.
Cohen SR, Kawamoto HK, Jr., Burstein F and Peacock WJ: Advancement-onlay: an improved technique of
fronto-orbital remodeling in craniosynostosis. Child's nervous system : ChNS : official journal of
the International Society for Pediatric Neurosurgery 7: 264-271, 1991.
Diluna ML and Steinbacher DM: Simulated fronto-orbital advancement achieves reproducible results in
metopic synostosis. The Journal of craniofacial surgery 23: e231-234, 2012.
Fearon JA: Beyond the bandeau: 4 variations on fronto-orbital advancements. The Journal of craniofacial
surgery 19: 1180-1182, 2008.
Fearon JA, Ruotolo RA and Kolar JC: Single sutural craniosynostoses: surgical outcomes and long-term
growth. Plastic and reconstructive surgery 123: 635-642, 2009.
Francis CS, Shetty A, Frank R, Meltzer HS and Cohen SR: In situ fronto-orbital advancement with medial
orbital osteotomies for trigonocephaly-associated hypotelorism. The Journal of craniofacial
surgery 22: 281-284, 2011.
Havlik RJ, Azurin DJ, Bartlett SP and Whitaker LA: Analysis and treatment of severe trigonocephaly.
Plastic and reconstructive surgery 103: 381-390, 1999.
Hoffman HJ and Mohr G: Lateral canthal advancement of the supraorbital margin. A new corrective
technique in the treatment of coronal synostosis. Journal of neurosurgery 45: 376-381, 1976.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
14
Jimenez DF, Barone CM, Cartwright CC and Baker L: Early management of craniosynostosis using
endoscopic-assisted strip craniectomies and cranial orthotic molding therapy. Pediatrics 110: 97-
104, 2002.
Kapp-Simon KA: Mental development in infants with nonsyndromic craniosynostosis with and without
cranial release and reconstruction. Plastic and reconstructive surgery 94: 408-410, 1994.
Kellogg R, Allori AC, Rogers GF and Marcus JR: Interfrontal angle for characterization of trigonocephaly:
part 1: development and validation of a tool for diagnosis of metopic synostosis. The Journal of
craniofacial surgery 23: 799-804, 2012.
Knoll BI, Shin J and Persing JA: The bowstring canthal advancement: a new technique to correct the
flattened supraorbital rim in unilateral coronal synostosis. The Journal of craniofacial surgery 16:
492-497, 2005.
Losken HW, Pollack IF and Singhal VK: Vascularized fronto-orbital advancement. The Journal of
craniofacial surgery 7: 107-110, 1996.
Marchac D: Radical forehead remodeling for craniostenosis. Plastic and reconstructive surgery 61: 823-
835, 1978.
Marchac D and Renier D: [The "floating forehead". Early treatment of craniofacial stenosis]. Annales de
chirurgie plastique 24: 121-126, 1979.
McCarthy JG, Karp NS, LaTrenta GS and Thorne CH: The effect of early fronto-orbital advancement on
frontal sinus development and forehead aesthetics. Plastic and reconstructive surgery 86: 1078-
1084, 1990.
Metzler P, Zemann W, Jacobsen C, Gratz KW and Obwegeser JA: Cranial vault growth patterns of
plagiocephaly and trigonocephaly patients following fronto-orbital advancement: A long-term
anthropometric outcome assessment. Journal of cranio-maxillo-facial surgery : official
publication of the European Association for Cranio-Maxillo-Facial Surgery 2013.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
15
Obwegeser JA: [The range of craniosynostosis - timing and techniques of craniofacial repair]. Praxis 98:
1007-1014, 2009.
Patel A, Chang CC, Terner JS, Tuggle CT and Persing JA: Improved correction of supraorbital rim
deformity in craniosynostosis by the "tilt" procedure. The Journal of craniofacial surgery 23: 370-
373, 2012.
Pearson GD, Havlik RJ, Eppley B, Nykiel M and Sadove AM: Craniosynostosis: a single institution's
outcome assessment from surgical reconstruction. The Journal of craniofacial surgery 19: 65-71,
2008.
Persing JA, Jane JA, Park TS, Edgerton MT and Delashaw JB: Floating C-shaped orbital osteotomy for
orbital rim advancement in craniosynostosis: preliminary report. Journal of neurosurgery 72: 22-
26, 1990.
Posnick JC, Lin KY, Chen P and Armstrong D: Metopic synostosis: quantitative assessment of presenting
deformity and surgical results based on CT scans. Plastic and reconstructive surgery 93: 16-24,
1994.
Rene C: Update on orbital anatomy. Eye 20: 1119-1129, 2006.
Renier D, Sainte-Rose C, Marchac D and Hirsch JF: Intracranial pressure in craniostenosis. Journal of
neurosurgery 57: 370-377, 1982.
Schaller BJ, Filis A, Merten HA and Buchfelder M: Premature craniosynostosis--the role of skull base
surgery in its correction. A surgical and radiological experience of 172 operated infants/children.
Journal of cranio-maxillo-facial surgery : official publication of the European Association for
Cranio-Maxillo-Facial Surgery 40: 195-200, 2012.
Selber J, Reid RR, Gershman B, Sonnad SS, Sutton LN, Whitaker LA, et al.: Evolution of operative
techniques for the treatment of single-suture metopic synostosis. Annals of plastic surgery 59: 6-
13, 2007.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
16
Shah A, Patel A and Steinbacher DM: Simulated frontoorbital advancement and intraoperative
templates enhance reproducibility in craniosynostosis. Plastic and reconstructive surgery 129:
1011e-1012e, 2012.
Sidoti EJ, Jr., Marsh JL, Marty-Grames L and Noetzel MJ: Long-term studies of metopic synostosis:
frequency of cognitive impairment and behavioral disturbances. Plastic and reconstructive
surgery 97: 276-281, 1996.
Steinbacher DM, Wink J and Bartlett SP: Temporal hollowing following surgical correction of unicoronal
synostosis. Plastic and reconstructive surgery 128: 231-240, 2011.
Tessier P: [Total facial osteotomy. Crouzon's syndrome, Apert's syndrome: oxycephaly, scaphocephaly,
turricephaly]. Annales de chirurgie plastique 12: 273-286, 1967.
Tessier P: Relationship of craniostenoses to craniofacial dysostoses, and to faciostenoses: a study with
therapeutic implications. Plastic and reconstructive surgery 48: 224-237, 1971.
van der Meulen J: Metopic synostosis. Child's nervous system : ChNS : official journal of the International
Society for Pediatric Neurosurgery 28: 1359-1367, 2012.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Tables
Table 1. Craniometric Parameters
Abbreviation Parameter Description
ECA Endocranial bifronal angle Angle of the frontal bone in a single axial plane at the level of the
superior-most aspect of the crista galli with the vertex (CG)
located on the endocranial side of the frontal bone at the metopic
suture and terminal points at the lateral borders of the respective
orbital apertures (OA right, OA left)
OPA Orbital plane angle Angle of both planes of the orbital aperture (supraorbital notch
(SON), zygomaticofrontal suture (ZF), zygomaticomaxillary
suture (ZM)
AA Anterior advancement Distance between the Clinoid (C) and the Glabella (G)
ZFD Interzygomaticofrontal suture
distance
Distance between zygomaticofrontal sutures (ZF)

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 2. Endocranial Bifrontal Angle (ECA) Before and After Surgical Correction of Metopic
Synostosis
FOA TP
Mean value (pre-op) 127.0° 129.3°
Mean value (post-op) 151.2° 143.9°
Mean change (pre/post-op) 24.18° 14.6°
Percentage 19.0% (max. 48.3 %) 11.3% (max. 18.2 %)
p-value 0.00026 0.00297

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 3. Orbital Plane Angle (OPA) Before and After Surgical Correction of Metopic Synostosis
FOA TP
Mean value (pre-op) 121.7° 119.8°
Mean value (post-op) 132.1° 129.9°
Mean change (pre/post-op) 10.4° 10.1°
Percentage 19.0 % (max. 26.5%) 11.3 % (max. 23.5%)
p-value 0.00026 0.00297
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 4. Anterior Advancement (AA) After Surgical Correction of Metopic Synostosis
FOA TP
Mean value (pre-op) 43.8 mm 39.1 mm
Mean value (post-op) 53.4 mm 41.4 mm
Mean change (pre/post-op) 8.3 mm 2.3 mm
Percentage 18.5 % (max 25%) 7.4 % (max 12.3%)
p-value 0.00932 0.05823
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 5. Interzygomaticofrontal Distance (ZFD) Before and After Surgical Correction of
Metopic Synostosis
FOA TP
Mean value (pre-op) 69.6° 70.8°
Mean value (post-op) 76.4° 75.1°
Mean change (pre/post-op) 6.8° 4.3°
Percentage 9.8 % (max. 20.5%) 6.2 % (max. 12.0 %)
p-value 0.001241 0.07811

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Captions to Illustrations
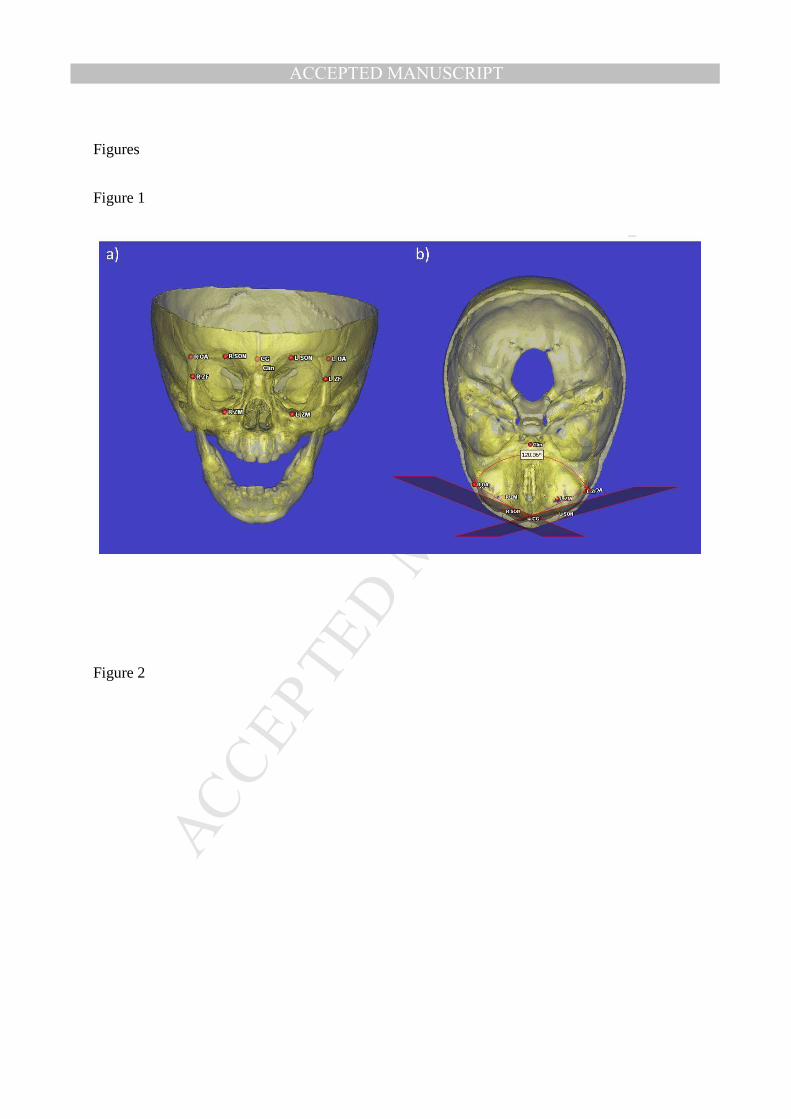
Figure 1
Pre-operative 3-D computed tomography scan of an eight months old patient with metopic
synostosis.
a) Coronal view, showing the craniocephalic landmarks used for antropometric
measurements
b) Axial view, showing the pre-operative measurements (endocranial bifrontal angle (ECA);
orbital planes angle (OPA))
Figure 2
Fronto-orbital Advancement (FOA)
A classical osteotomy was performed for fronto-orbital bar mobilization. For hypotelorism
correction, a two- piece opening and expansion of the supraorbital bar using an interpositional
bone graft was done.
a) Coronal view, showing the osteotomy lines and anterior advancement (medial and lateral
of the fronto-orbital segment) after remodeling.
b) Axial view, showing the complete mobilization (osteotomy line and advancement within
the frontal skull base) of the fronto-orbital segment.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
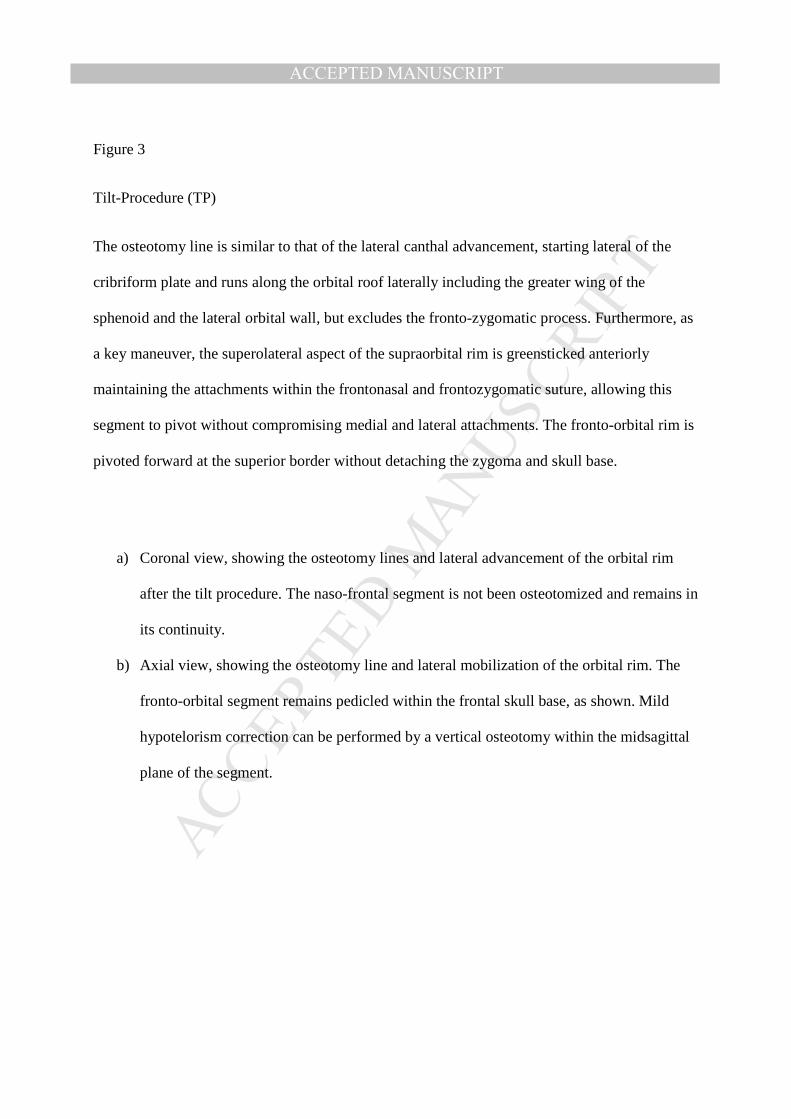
Figure 3
Tilt-Procedure (TP)
The osteotomy line is similar to that of the lateral canthal advancement, starting lateral of the
cribriform plate and runs along the orbital roof laterally including the greater wing of the
sphenoid and the lateral orbital wall, but excludes the fronto-zygomatic process. Furthermore, as
a key maneuver, the superolateral aspect of the supraorbital rim is greensticked anteriorly
maintaining the attachments within the frontonasal and frontozygomatic suture, allowing this
segment to pivot without compromising medial and lateral attachments. The fronto-orbital rim is
pivoted forward at the superior border without detaching the zygoma and skull base.
a) Coronal view, showing the osteotomy lines and lateral advancement of the orbital rim
after the tilt procedure. The naso-frontal segment is not been osteotomized and remains in
its continuity.
b) Axial view, showing the osteotomy line and lateral mobilization of the orbital rim. The
fronto-orbital segment remains pedicled within the frontal skull base, as shown. Mild
hypotelorism correction can be performed by a vertical osteotomy within the midsagittal
plane of the segment.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figures
Figure 1
Figure 2

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 3