company profile - storage.googleapis.com€¦ · company profile tim foster. tim foster...
TRANSCRIPT

Maintenance ◦ Projects ◦ Construction 2019
COMPANY PROFILE
TIM FOSTER

TIM FOSTER [email protected] Evans, GA 706.832.4340 www.timfostermpc.com
EXPERIENCE
My experience includes a vast background of various job duties within Beef Plants throughout the
country. These duties span (28) twenty-eight years.
01/2018 – Present
Nicholas Meats – Loganton, PA
Vac System Install
Hot Box Hydraulic & Process Piping Install
Basement Platform Install
Kill Floor Skinning Line Bench Install
Hot Box Steel Install
Waster Water Roto Screen Install
Shrink Tunnel Exhaust Fan Install
Post Knock Box Steel Install
Hot Box Chains Install
Hot Box 6” Drain Piping Install
Fab Pack Off Conveyor Install
180 Hydro-Therm Piping Install
01/2018 – Present
Colorado Premium Foods – Carrollton, GA
Rib Line Multivac Installation
Raw 8614 Cryovac Installation
Smoke Generators Installation
Relocation of Cryovacs
Chill Water Heat Exchanger Repairs
Install Brine Line to Relocated Injector
Relocate Rib Line Multi-Vac
Safety Guards (2) Tumbler Dumpers
Rib Rack Access Modifications
Sod and Irrigation Repair
Tempering Cooler Rack Install

TIM
FO
ST
ER
01/2018 – Present
American Beef – Chino, CA
Design Slaughter Addition
01/2018 – Present
DemKota Ranch Beef – Aberdeen, SD
Shackle Decline Modifications
Down Puller Shroud Modifications
Brisket Saw Relocation
Fab Rail Raise Index Modifications
Box Cooler Racking Install
Center Track Chain Replacement
Cold Water Tank Replacement
Repair Trolley Spreader
Repair Rail Support Steel – Break Line
Gasket Replacement for 109 Tube-Shell
Fix Bone Chute
OSHA Mandated Corrections
Auger Bearing Repair
Final Grading Area Renovations
Steam Line Modifications
Auger Bearing #9 Repair
Heat Exchanger Gasket Replacement
Meat Master Modifications
Offal Conveyor Modification
03/2018
TLI (The Livestock Institute) - Meatworks – Westport, MA
Erect Steel – Building Modifications, Install Process / Slaughter Equipment, Install Cattle Pen Barn.
04/2018
Alloy Hardfacing & Engineering Co., Inc – St. Paul and Joliet, MN
Rendering Modifications
03/2018 – 05/2018
Iowa Premium – Tama, IA
White Offal Room, Intestine and Tripe System Design and Layout.
01/2017 – 01/2018
Colorado Premium Foods – Carrollton, GA
Plant Retro-fit - Further Processing / Cooked Facility
Sous Vide Equipment Design and Installation
Boiler/Smokehouse Installation
Corn Beef Line Installation

TIM
FO
ST
ER
R&D Lab Installation
Cryovac Installation
VeMag Installation
Marination System Installation
Ground Beef Installation
Brine System Installation
Lactic Cabinet Installation
Box Conveyor Installation
Sanova System Installation
Bowl Chopper/Paddle Blender Installation
Weigh Price Labeler Installation
Relocate Slicing Line from Miami
Hot Water to Waste Water Modifications
Boning Table Extension
Relocate Miami RTE-Hot Dog Lines
Sanova Workstation Modifications
Modify Oven Ramps
Ground Beef Acid Application Installation
Install Chill Tank System
Hot Dog Ovens Installation
Install Sear Machine
Re-Pipe Air-Water Lines to Injectors
Install 2nd Pack-Off Conveyor in RTE
Brine Lines to Injections Install
Fabricate 32 Rib Racks
Fix Sous Vide Lids
Electrical System Study
Condensate Return Lines to Riser Ovens
Shrink Tunnel Guards
Remove Damaged Cooler Wall
RTE Acid Line Modifications
Flow Switches Replacement
Starter Control Panel Installation
Proteus – Install Temporary Emulsifiers
Proetus – Jacketed Tank Install
Proteus – System Installation
Proteus – Refrigeration System Install Location 1
Proteus – Glycol System Install
Proteus – Chilled Water Install
Proteus – Mix Tank Install
Proteus – Jacketed Tank Install
01/2018 – 02/2018
JBS Case Ready - Riverside, CA
Demo of Auto Product Packaging Equipment
TIM
FO
ST
ER
10/2017 – 11/2017
Nicholas Meats – Loganton, PA
Design & Build of New Fab Production Floor
Conveyor Installation
Freezer Rack Repair
Palletizer Repair
01/2017 – 12/2017
Colorado Premium Foods – Greeley, CO
Installation of Refrigeration Condenser
Design & Build Box Storage and Shipping Dock Facility
Proteus – IMP Panel Installation
Proteus – Mix Tank Installation
Proteus – Double Jacketed Tank Install
Proteus – Chilled Water Install
Proteus – Glycol System Install
11/2016 – 11/2016
Tippmann Construction/Brown Packing – Gaffney, SC
Design 80,000 SF Kill Floor and Hot Box Addition – Did not get the bid.
9/2016 – 12/2016
Passport/Tyson – Lexington, NE
Installation of Food Safety Intervention - Bovibrom
10/2016 – 11/2017
Colorado Premium Foods – Carrollton, GA
Design - Further Processing Area
12/2016 – 12/2017
DemKota Ranch Beef– Aberdeen, SD
Tripe Project
Fab Conveyor and Stand Modifications
Chute and Plow Modifications
Shackle Rail Replacement
Tripe Conveyor Modifications
Cryovac Modifications
Shackle Incline Modifications
Vacuum Pump Installation
2/2016 – Present
Colorado Premium Foods – Greeley, CO
Design Build New Construction
Combo Cooler Install

TIM
FO
ST
ER
Shipping Receiving Dock Install
Box Storage Addition
10/2015 – 12/2015
Colorado Premium Foods – Bridgeview, IL (Buedel Food’s)
Installation of Corned Beef Brisket Line
Office and Welfare Area Remodel
Installation of Chilled Brine System
10/2015 – 11/2015
Triple J Meats - Buffalo Lake, MN
Install New Rotating Kosher Box
Modify Rabbi Stand
8/2015 – 10/2015
Cimpl Meats (American Foods Group) – Yankton, SD
Assist General Contractor with Equipment Modifications (During Kill Floor Modification Shut Down)
Raise the Down-Puller
1/2015 – 06/2016
DemKota Ranch Beef (New Angus, LLC.) – Aberdeen, SD
Heat Exchanger Hot Water System and Process Piping
HVES System Installation
Carcass Wash Cabinet and System Piping Modifications
Hot Water Pasteurization System with Kosher Requirements
Processing Floor Boning Table Modifications, Bone Belt Installation, and Trim Belt Modifications
Full Box Line System Modifications
Trayformer and Case Sealer Installation
Overhead Chain Conveyor Modifications – Round Line
Boiler Economizers Installation
Ritual Slaughter Modifications – Harvest Floor
Final Acid Cabinet Relocation
HB 4 Switch and Sales Cooler Transfer
Kosher Kill Station Installation
Waste Water Cooling System Install Phase 1
Waste Water Cooling System Install Phase 2
Refrigeration Condenser Footer Steel Design
Basement Augers Installation
Screw Conveyor Shafts Installation
Classifier Installation
Lift Station Starter Repair
Cattle Chute Modifications
Acid Spray Bar Installation on Processing Trim Conveyors
Bone Belt UHMW Installation
Chilled Water Packaging System [Pac-Chill]

TIM
FO
ST
ER
Blood Drain Piping Modification
Spray Chill Level Control
Blood Pit Sump
Skinner Stands
Remove Section of Loin Trim Conveyor Modifications
HB1-2 Walking Beam Modifications
HB3-4 Walking Beam Modifications
Wing Drop Table Modifications
Relocate Acid Valves on Processing Floor Interventions
Tripe System EZ Heater Installation
Chill Water Line to Refiner
Processing Floor TM Entrance Modification
Refrigeration Condenser Stand Fabrication and Erection
Refrigeration Condenser Sump, Pumps and Piping Installation
Fabrication of Stainless Steel Sump Tank [16’ x 8’ x 10’]
Installation of Sodium Citrate Mixing System and Piping in the Knock Box and Sticking Pit Area
Trim Upgrade Modifications
Meat-Master and Reject Conveyor Installation
Intestine System Installation
Kill Floor Team Member Drop Skirt Stand Modifications
1/2015 – 3/2015
FM Meat Products – Ft. McCoy, FL
HVES Installation
USDA Stand Modifications
1/2015 – 3/2015
JBS USA – Hyrum, UT
Design Assistance of New Processing Floor
2/2014 – 7/2014
FPL Food – Augusta, GA
Fire Demolition and Kill Floor Rebuild
9/2013 – 2/2015
Creekstone Farms Premium Beef, LLC. – Arkansas City, KS
Fire Demolition and Processing Floor Rebuild
Bone Auger Project Installation
Refrigeration Replacement on Existing Processing Floor
Design of New Processing Floor
Co-Design of New Processing Building
Complete Fab Processing Installation

TIM
FO
ST
ER
4/2014 – 9/2014
JBS USA – Tolleson, AZ
Lid Stock Line Installation
Sales Cooler Modification Installation
9/2013 – 12/2013
JBS USA – Tolleson, AZ
Wendy’s Patty Line Installation
Tripe/Omasum Design and Installation
5/2013 – 6/2013
Proteus Industries – Boston, Mass
Engineering Services Protein Process
Equipment Skid Design
4/2013 – 5/2013
Buffalo Lake, MN – Triple J / Alle Processing
Installation of a Double Kosher Box
Fabrication and Installation of the Rabbi Stand and Lung Station
Fabrication and Installation of the Operator Stand
Electrical Service and Operator Controls
Hydraulic System Installation
4/29/2011 – 6/7/2013
Northern Beef Packers – Aberdeen, SD
Coordination & Management of the Plant Installations of all Utilities, Services, Equipment
and Processes.
Commission & Startup of all Processes
New Plant Construction (420,000 sf)
3/17/2009 – 3/10/2011
Tyson / IBP – Complex Engineer - Garden City, KS
Leadership of Maintenance Department(s) / Management of Maintenance Engineer(s)
Project Manager of all on-site Company Projects
Project List:
Replacement of 20” Underground Effluent Line
Batch Cooker replacements
Replacement of Condensate Return System
Rebuild of TASCO Wastewater Cells
Installation of Wastewater Roto-Screen
Numerous Auger Replacements
Installation of Tallow Filtering System
Installation of REB-1200, Tallow {Vertical Separation}
Replacement of Boiler Feed Water Pumping System

TIM
FO
ST
ER
Replacement of High Pressure Water Sanitation System
Replacement of Carcass Wash Pumps and Piping System
Replacement of 200 HP Air Compressors
Replacement of 700 HP Sullair NH3 Compressors
Installation of 600 HP Mycom NH3 Compressor
Replacement of Pumper Drums of House Accumulators
Replacement of 70 Hot Box Evaporators (in process)
Installation of 70 new NH3 Control Banks (in process)
Installation of new roof mounted NH3 Headers (in process)
Installation of new beams and 162 Cooler Rail Switches
Installation of New Slaughter Trayformers (in process)
Installation of Air Compressor Water Recirculation System
Installation of new NH3 Liquid Pumps
Installation of Dual VBS Hot Scales
Installation of HB2 (bromine-based, liquid antimicrobial) System
Installation of Finalyse - Pre-Harvest Cattle Spray System
Installation of Complete Re-Wiring of Processing Floor
Installation of New Cryovac Machines on Processing
Installation of new Test and Hold Combo Cooler
Installation of New Sortation Coolers (Retro)
Installation of (2) New Kill Floor AMU’s (in process)
Installation of numerous Power 90’s (MH)
Installation of new 10,000 box Flow Thru System
9/30/2005 – 3/1/2009
FPL Food LLC – VP of Engineering - Augusta, GA
Leadership of Maintenance Department(s)
Management of Maintenance Manager(s)
Management of Rendering Operations
Management of Wastewater Operations
Project Manager of all Company Projects
Project List:
Termet Spinal Vacuum System
Installation of IMS Down-puller / Jarvis Hock Restrainer
Installation of Multiple Systems Side Puller.
1st Leg Bench Renovation
Blood Chain and Head Chain Conveyor
Installation of VBS Live Scale
Installation of Carcass Tracking System
In-Floor Blood Pit Installation
Blood Pit Stimulator Installation
Offal Tri-Web Project design and Installation
Fab Floor Trim Belt Modifications.
Fab Floor Full Box Line Renovation.
Fab Floor Box Shipping – Flow thru Racking System
TIM
FO
ST
ER
Steak Addition – Project Design
Installation of KP Chub Line #2
Installation of Frozen Block Grinders (2)
Further Processing – Refrigeration Upgrade
Installation of 5# Patty Line “C”
Installation of Beef Crumbles Line
AccuPump Upgrade
Co-Design of New Further Processing Facility
Installation of Chub Lines
Installation of Chub Grinding System
Installation of Frozen Patty System
11/16/2004 – 9/5/2005
Maintenance Projects and Construction L.L.C
7/22/2005 – 9/5/2005
FPL Food LLC / Further Processing Facility – Augusta, GA
Management of Maintenance Department
Training of Company New Hire Maintenance Manager
1/17/2005 – 07/21/2005
Sunterra Meats – Alberta Canada
Installation of 45 Head / hour Beef Kill Floor (Complete)
Installation of 60 Head / hour Beef Fab Floor (Complete)
11/16/2004 – 10/28/2005
Rolandia Brazil - Corol / Prestcott Plant
Co-Design 150 head / hour Kill Floor
Co-Design Grinding System and Patty Line
Co-Design Cook / Marinate System
8/6/2004 – 12/31/2004
Shapiro Packing / FPL Food LLC – VP of Engineering
FPL Food LLC / Packing Company – Augusta, GA
Transfer of Ownership and Operations Startup
Grading Area Addition
AMR Area Addition
Fabrication Area Modification Design
Chuck Chain Installation Design
Grinding System and Chub Packaging Design
4/17/2003 – 8/6/2004
Maintenance Projects and Construction L.L.C. - Owner
Shapiro Packing Company – Augusta, GA
OSHA Abatement Issues
In term Plant Engineer
TIM
FO
ST
ER
Implementation of PMC
Implementation of MLS – Maintenance Labor System
Daily Maintenance Operations
Coordination with USDA and Plant QA personnel
Kill Floor Design Team Coordination
Ground Beef Maintenance
Ground Beef Projects
Frigorífico Santos Lugares – Montevideo, Uruguay
Engineering Adviser – Facility and Equipment Status
Frigorífico La Caballada – Salto, Uruguay
Engineering Adviser – Facility Construction
Beef Kill Renovations
Lamb Kill Renovations
Processing / Packaging Renovations
Building Improvements
Food Safety Interventions
Design Kosher Salt / Soak System and Building Addition
12/02/2002 – 4/10/2003
Iowa Quality Beef - Plant
Engineer/Project Engineer / Project Manager
Total Facility Remodel
Live Scale Installation
Crowd Pen and Serpentine Design and Installation
Restrainer Building Addition
Kill Floor Revision
Offal Area Revision
Fab Floor Design and Installation
Shipping Dock Building Addition
Packaging Design and Installation
Refrigeration System Revision
Hot Water System Design and Installation
High Pressure Sanitation System Design and Installation
Inedible Collection and Loadout System
Electrical System upgrade and MCC Addition
Pre-Evisceration Wash and Acid Rinse Installation
High Pressure Wash and Pasteurization System Installation
Head and Offal Acid Rinse Installation
Final Carcass Acid Rinse Installation
10/2001 – 12/1/2002
Future Beef Operations – Corporate Engineering - Director of Maintenance
Assist in the coordination, design, and construction of new facilities
Define, develop and implement the Direction of Engineering for multiple plant sites

TIM
FO
ST
ER
Define, develop, implement, and maintain the MLS (Maintenance Labor System) for multiple sites
Define, develop and implement a company wide Maintenance Training Program
Define, develop and implement a company wide Contractor Training Program
Define, develop and implement a company wide Attendance Policy
Promote, teach and believe that Safety is first
Define capital budget; develop capital requests forms, manage and coordinate all capital projects
Insure the Plant is constructed and maintained in a manner to prevent injuries
As of 11/2001- assume all roles and responsibilities of Future Beef Plant - Arkansas City
Plant Engineer (Business Unit Leader)
Manage and develop (2) Maintenance Engineers, (1) Process Controls Engineer, (7) Maintenance
Supervisors, (1) Wastewater Pre-treatment Environmental Engineer, (1) WWTP Lab Supervisor,
(1) Warehouse/Supply Manager, (1) Purchasing Supervisor, (1) Buyer, (1) Safety Director, (2) Health
Service Techs, and (12) Security Guards
Retention of (95) total maintenance department employees
To manage total facilities’ maintenance department. Coordinate with Operations, USDA, and FBO
Corporate personnel. Duties to include leadership, planning, budgeting, goal setting and reporting for all
aspects of the maintenance department
Project List:
Assist in the Cattle Dehair Revision
Edible Foot Operation High Voltage Stimulator
6/1999 – 10/2001
ConAgra Beef – Omaha Plant (Northern States)
Plant Engineer
Promote, teach and believe that Safety is first
Insure the Plant is maintained in a manner to prevent injuries.
Retention of (56) total maintenance employees.
Manage and develop (2) Maintenance Superintendents and (7) Maintenance Supervisors
Manage all aspects of the Maintenance Department to include (3) minutes or less per day of
maintenance downtime per department, maintain R&M, supply and labor budgets
Management of Maintenance Labor System (MLS) – Preventive and Predictive Maintenance.
Develop and administer a Skills Based Maintenance Training Program
Maintain a daily Energy Management System.
Define Capital Budget; submit requests and Manage all plant Capital Projects
Project List:
Plant Coordination of Kill Floor
Skinning Line Addition
Tripe Room Conversation
Mountain Chain Area Addition
Dressing Line Revision
Dressing Line Lighting Revision
Paunch Press and Load out Addition

TIM
FO
ST
ER
Fab Floor Revision
Packaging Revision
Ground Beef Revision
MAP (Modified Atmosphere Packaging) Line Revision
Bone Pre-breaker and Screw Transfer System
Welfare Building Addition
Air Compressor Building Addition
Offal Dock Addition
Boiler and Building Addition
Hot Water Storage Tank Addition
Blood Collection System
Phone System
Rendering Buss Duct Revision
Production Ethernet Network – Fiber Optics
Bone Cannon Addition
Mexican Export Requirements
24” Inedible Auger System to Rendering
Rendering System Upgrades
Raw Product Bin and System
Epoxy Flooring - Fab – Ground Beef
140 and 180 degree Water Systems
High Pressure Sanitation System
Pro-Man System Revisions
11/98 – 6/99
ConAgra Beef – Greeley Plant (Monfort Beef)
Project Engineer
Define Capital Budget; submit requests and manage all plant Capital Projects
Project List:
Pro-Man Addition
Fab Floor Gas Fired Air Make-up System
700 hp Ammonia Compressor(s) Installation
Evap-Condenser(s) System Installation
Fab Packaging Revision
Epoxy Flooring – Fab and Shipping Dock
Trim Upgrade Area Addition
11/1995 – 11/1998
ConAgra Beef – Corporate Engineering (Monfort Beef)
Corporate Energy Director
Indirectly manage and develop the (4) Beef Plant Energy Coordinators.Implement the Monfort Energy
Management Program in the (4) beef plants
Indirectly manage and develop the (4) beef plant Boiler and Refrigeration Departments
Manage the shrink program
Provide startup support during major capital projects

TIM
FO
ST
ER
Manage and co-manage capital projects
Project List:
Kill Floor Construction/Renovations
WWTP Construction/Renovations
Rendering (Inedible, Edible, Gel Bone, Blood Drying) Construction/Renovations
Chill Coolers Construction/Renovations
Pasteurization Systems Design and Installation
Hot Water Storages Systems Ammonia Refrigeration Systems
6/1994 – 11/1995
ConAgra Beef – Greeley Plant (Monfort Beef)
Plant Energy Coordinator
Implement the Monfort Energy Management Program
Manage and co-manage capital energy saving projects
Indirectly manage and develop the plant Boiler and Refrigeration Department
Project List:
Tank(s) Insulation and Steam / Condensate Revision.
Hot Water Storage Tanks
10/1991 – 6/1994
ConAgra Beef – DesMoines Plant (Monfort Beef)
Environmental Supervisor
Management of EPI Wastewater System
Management of (3) Wastewater Operators
Management of all City, County, and State Permits
Management of the By-Product Recovery System
Management of Rendering Odor Control System
Management of Paunch Land Application
Project List:
EPI – Wastewater System Revision
Cattle Pen High Pressure Wash-down System
180 degree Pick Heater Addition
6/1990 - 10/1991
ConAgra Beef – DesMoines Plant (Monfort Beef)
Wastewater Operator
Operations and maintenance of the EPI Wastewater System
2/1990 – 6/1990
ConAgra Beef – DesMoines Plant (Monfort Beef)
Hides Production EmployeeDrop Tank
Trim face plates
Fleshing Machine Operator

TIM
FO
ST
ER
10/1989 – 2/1990
ConAgra Beef – DesMoines Plant (Monfort Beef)
Kill Floor Production Employee
Hock cutter
Bung Dropper
AREA OF CONCENTRATION AND EXPERTISE
• HR (Value of Team Members)
• HACCP
• Food Safety Programs
• Food Safety Interventions
• USDA Coordination
• Safe Work Areas
• Team Member Safety
• Humane Handling
• Carcass Tracking
• Slaughter Operations
• Kosher Operations
• Refrigeration Systems
• Carcass Chilling
• Shrink Management
• Carcass Sortation
• Processing
• Further Processing
• Ground Beef
• Material Handling
• Hides
• Rendering
• Wastewater
• Lagoon Operations
• Tripe Wash and Refine
• Offal Operations
• Water Heating and Chilling
• Boiler Operations
OTHER AREAS OF EMPHASIS
• Management of Hourly Mechanics, Maintenance Superintendents and Supervisors
• Cost Management
• Budget Definition and Management
• Energy Management
• Cost Savings Initiatives
• Value Engineering & Project Management
MPC is registered with the following Safety programs:
http://www.safetyservicescompany.com/
Safety Services Company is North America’s leading provider of safety and compliance training products and services.
Safety Services Contact Info: Paul Martinez Account Executive Global Compliance Solutions Safety Services Company a Div. of SSC (T) 888-519-6556 (F) 866-285-0140 2626 S. Roosevelt St. Suite #2 Tempe, AZ 85282 [email protected] www.safetyservicescompany.com
https://www.isnetworld.com/
ISN is the global resource for connecting corporations with safe, reliable contractors and suppliers from capital-intensive and public sector industries.
https://www.asme.org/
ASME is a not-for-profit membership organization that enables collaboration, knowledge sharing, career enrichment, and skills development cross all engineering disciplines, toward a goal of helping the global engineering community develop solutions to benefit lives and livelihoods.

ISN – Rating for MPC:
“A” – Grade Level
Grade Since 08/21/2013
Grade Component Status Points
Contractor Safety Information Exceptional 20 / 20
Safety Statistics Superior 25 / 25
RAVS Safety Program RAVS score is 100 30 / 30
Insurance Insurance Documents are Accepted 0 / 0
EMR Letters Rate is Verified - Not Qualified 5 / 5
Acknowledgement Form Chemical Process Safety Awareness
Grade Acknowledged 10 / 10
Subcontractor Management
Program Acceptable to use subcontractors. 5 / 5
Ammonia Awareness Program Acceptable to work with Ammonia. 5 / 5
Total 100 / 100

MPC Safety Programs Table of Contents:
*All program details available upon request. [Or visit www.timfostermpc.com – Safety
Programs tab]
1. Company Safety Policies and Procedures
2. Safety Committees
3. General Safety Rules and Code of Safe Practices
4. Accident Investigation Plan
5. Assured Equipment Grounding Conductor Program & Ground Fault Circuit
Interrupters – (GFCI)
6. Bloodborne Pathogens
7. Disciplinary Programs
8. Electrical Safety: Qualified and Non-Qualified
9. Fall Protection
10. Fire Protection
11. First Aid & CPR
12. Hand & Power Tools
13. Hazard Communication – HAZCOM
14. Ladder & Stairway Safety
15. Lockout-Tagout: Control of Hazardous Energy
16. Noise Exposure – Hearing Conservation
17. Personal Protective Equipment – Assessments – PPE
18. Respiratory Protection Program
19. Rigging Equipment for Material Handling
20. Scaffolds
21. Trenching, Shoring, & Excavations
22. OSHA Inspections, Log 300, & Posting Requirements
23. Safety Meeting Minutes
24. Behavior Based Safety Program – (BBS)
25. Short Service Employee Policy – (SSE)
26. Subcontractor Management Plans & Management of Change
27. Ammonia Awareness
28. Gaseous Chlorine Awareness
29. Process Safety Management

MPC Injury & Illness Prevention Program
Table of Contents:
*All program details available upon request. [Or visit www.timfostermpc.com – Safety
Programs tab]
1. Safety & Health Program Summary
2. General Safety Rules
3. Safety Committee Policy
4. Job Hazard Analysis
5. Accident Investigation
6. Fire Prevention & Emergency Action Plans
7. Medical Services & First Aid
8. Workplace Violence Prevention
9. Slips, Trips & Falls
10. Office Safety
11. General Electrical Safety
12. Bloodborne Pathogens
13. Personal Protective Equipment
14. Manual Material Handling
15. Hazard Communication
16. Driver Safety
17. New Hire Orientation
18. Appendix Chapter - HAZWOPER

Year
City State
(A) (B) (C) (D) (E) (F)
(M)
(G) (H) (I) (J) (K) (L) (1) (2) (3) (4) (5)
Page totals 0 0 0 0 0 0 0 0 0 0 0
Page 1 of 1 (1) (2) (3) (4) (5)
OSHA's Form 300 (Rev. 01/2004)
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Log of Work-Related Injuries and Illnesses
Attention: This form contains information relating to
employee health and must be used in a manner that
protects the confidentiality of employees to the extent
possible while the information is being used for
occupational safety and health purposes. U.S. Department of LaborOccupational Safety and Health Administration
2010
You must record information about every work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment beyond first aid. You must also record significant work-related injuries and illnesses that are diagnosed by a physician or licensed health care professional. You must also record work-related injuries and illnesses that meet any of the specific recording criteria listed in 29 CFR 1904.8 through 1904.12. Feel free to use two lines for a single case if you need to. You must complete an injury and illness incident report (OSHA Form 301) or equivalent form for each injury or illness recorded on this form. If you're not sure whether a case is recordable, call your local OSHA office for help.
Describe injury or illness, parts of body affected,
and object/substance that directly injured or made
person ill (e.g. Second degree burns on right
forearm from acetylene torch)
Employee's Name Job Title (e.g.,
Welder)
Where the event occurred (e.g.
Loading dock north end)
Respirato
ry
Conditio
n
Respirato
ry
Conditio
n
On job
transfer or
restriction
(days)Job transfer
or restriction
Pois
onin
gP
ois
onin
g
Hearing L
oss
Inju
ry
Other record-
able cases
Identify the person Describe the case
Date of
injury or
onset of
illness
Inju
ry
Death(mo./day)
Form approved OMB no. 1218-017
Evans
Establishment name
CHECK ONLY ONE box for each case based on the
most serious outcome for that case:
Enter the number of
days the injured or ill
worker was:
Check the "injury" column or choose one
illness:
Tim Foster-dba MPC (Maintenance Projects Construction)
GA
Hearing L
oss
Classify the case
Days away
from workRemained at work
Away
From
Work
(days)
Skin
Dis
ord
er
Skin
Dis
ord
er
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Case
No.

Year 2010
Street
City Zip 30809
0 0 0 0
(G) (H) (I) (J) OR
5 4 1 3 3 0
0 0(K) (L)
Total number of… Knowingly falsifying this document may result in a fine.
(M)
(1) Injury 0 (4) Poisoning 0
(2) Skin Disorder 0 (5) Hearing Loss 0
(3) Respiratory
Condition 0 (6) All Other Illnesses 0
Industry description (e.g., Manufacture of motor truck trailers)
Post this Summary page from February 1 to April 30 of the year following the year covered by the form
All establishments covered by Part 1904 must complete this Summary page, even if no injuries or illnesses occurred during the year. Remember to review the Log to verify that the entries are complete
Using the Log, count the individual entries you made for each category. Then write the totals below, making sure you've added the entries from every page of the log. If you had no cases write "0."
Employees former employees, and their representatives have the right to review the OSHA Form 300 in its entirety. They also have limited access to the OSHA Form 301 or its equivalent. See 29 CFR 1904.35, in OSHA's Recordkeeping rule, for further details on the access provisions for these forms.
Total number of
cases with days
away from work
Total number of cases
with job transfer or
restriction
Total number of
days away from
work
Total number of days of
job transfer or restriction
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Injury and Illness Types
U.S. Department of Labor
OSHA's Form 300A (Rev. 01/2004)
Summary of Work-Related Injuries and IllnessesOccupational Safety and Health Administration
Form approved OMB no. 1218-0176
Title
Date
Owner
7/16/2013
Establishment information
Total number of
deaths
Number of Cases
Total number of
other recordable
cases
Number of Days
Total hours worked by all employees last
year
Standard Industrial Classification (SIC), if known (e.g., SIC 3715)
Annual average number of employees
North American Industrial Classification (NAICS), if known (e.g., 336212)
1
706-832-6719
Tim Foster
Phone
Company executive
I certify that I have examined this document and that to the best of my knowledge the entries are true, accurate, and
complete.
50
Tim Foster - dba MPC (Maintenance Projects & Construction)
Sign here
State
Employment information
Evans
Your establishment name
1198 Newport Trail
GA
Year
City State
(A) (B) (C) (D) (E) (F)
(M)
(G) (H) (I) (J) (K) (L) (1) (2) (3) (4) (5) (6)
Page totals 0 0 0 0 0 0 0 0 0 0 0 0
Page 1 of 1 (1) (2) (3) (4) (5) (6)
All
oth
er
illnesses
Away
From
Work
(days) All
oth
er
illnesses
Skin
Dis
ord
er
Skin
Dis
ord
er
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Case
No.
GA
Hearing L
oss
Classify the case
Days away
from workRemained at work
Form approved OMB no. 1218-0176
Evans
Establishment name
CHECK ONLY ONE box for each case based on the
most serious outcome for that case:
Enter the number of
days the injured or ill
worker was:
Check the "injury" column or choose one type of
illness:
Tim Foster dba MPC (Maintenance Projects and Construction)
Identify the Describe the case
Date of
injury or
onset of
illness
Inju
ry
Death(mo./day)
Pois
onin
gP
ois
onin
g
Hearing L
oss
Inju
ry
Other record-
able cases
You must record information about every work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment beyond first aid. You must also record significant work-related injuries and illnesses that are diagnosed by a physician or licensed health care professional. You must also record work-related injuries and illnesses that meet any of the specific recording criteria listed in 29 CFR 1904.8 through 1904.12. Feel free to use two lines for a single case if you need to. You must complete an injury and illness incident report (OSHA Form 301) or equivalent form for each injury or illness recorded on this form. If you're not sure whether a case is recordable, call your local OSHA office for help.
Describe injury or illness, parts
of body affected, and
object/substance that directly
injured or made person ill (e.g.
Second degree burns on right
forearm from acetylene torch)
Employee's
Name
Job Title (e.g.,
Welder)
Where the event
occurred (e.g.
Loading dock north
end)
Respirato
ry
Conditio
n
Respirato
ry
Conditio
n
On job
transfer or
restriction
(days)Job transfer
or restriction
Attention: This form contains information relating to
employee health and must be used in a manner that
protects the confidentiality of employees to the extent
possible while the information is being used for
occupational safety and health purposes. U.S. Department of LaborOccupational Safety and Health Administration
2011OSHA's Form 300 (Rev. 01/2004)
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office
Log of Work-Related Injuries and
Year 2011
Street
City Zip 30809
0 0 0 0
(G) (H) (I) (J) OR
5 4 1 3 3 0
0 0(K) (L)
Total number of… Knowingly falsifying this document may result in a fine.
(M)
(1) Injury 0 (4) Poisoning 0
(2) Skin Disorder 0 (5) Hearing Loss 0
(3) Respiratory
Condition 0 (6) All Other Illnesses 0
Industry description (e.g., Manufacture of motor truck trailers)
Post this Summary page from February 1 to April 30 of the year following the year covered by the form
All establishments covered by Part 1904 must complete this Summary page, even if no injuries or illnesses occurred during the year. Remember to review the Log to verify that the entries are complete
Using the Log, count the individual entries you made for each category. Then write the totals below, making sure you've added the entries from every page of the log. If you had no cases write "0."
Employees former employees, and their representatives have the right to review the OSHA Form 300 in its entirety. They also have limited access to the OSHA Form 301 or its equivalent. See 29 CFR 1904.35, in OSHA's Recordkeeping rule, for further details on the access provisions for these forms.
Total number of
cases with days
away from work
Total number of cases
with job transfer or
restriction
Total number of
days away from
work
Total number of days of
job transfer or restriction
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Injury and Illness Types
U.S. Department of Labor
OSHA's Form 300A (Rev. 01/2004)
Summary of Work-Related Injuries and IllnessesOccupational Safety and Health Administration
Form approved OMB no. 1218-0176
Title
Date
Owner
7/10/2013
Establishment information
Total number of
deaths
Number of Cases
Total number of
other recordable
cases
Number of Days
Total hours worked by all employees last
year
Standard Industrial Classification (SIC), if known (e.g., SIC 3715)
Annual average number of employees
North American Industrial Classification (NAICS), if known (e.g., 336212)
1
(706) 832-6719
Tim Foster
Phone
Company executive
I certify that I have examined this document and that to the best of my knowledge the entries are true, accurate, and
complete.
1860.5
Tim Foster - dba MPC (Maintenance Projects & Construction)
Sign here
State
Employment information
Evans
Your establishment name
1198 Newport Trial
GA

Year
City State
(A) (B) (C) (D) (E) (F)
(M)
(G) (H) (I) (J) (K) (L) (1) (2) (3) (4) (5) (6)
Page totals 0 0 0 0 0 0 0 0 0 0 0 0
Page 1 of 1 (1) (2) (3) (4) (5) (6)
OSHA's Form 300 (Rev. 01/2004)
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office
Log of Work-Related Injuries and
Respirato
ry
Conditio
n
Respirato
ry
Conditio
n
On job
transfer or
restriction
(days)Job transfer
or restriction
Attention: This form contains information relating to
employee health and must be used in a manner that
protects the confidentiality of employees to the extent
possible while the information is being used for
occupational safety and health purposes. U.S. Department of LaborOccupational Safety and Health Administration
2012
Pois
onin
gP
ois
onin
g
Hearing L
oss
Inju
ry
Other record-
able cases
Describe injury or illness, parts
of body affected, and
object/substance that directly
injured or made person ill (e.g.
Second degree burns on right
forearm from acetylene torch)
Employee's
Name
Identify the Describe the case
Date of
injury or
onset of
illness
Inju
ry
Death(mo./day)
Job Title (e.g.,
Welder)
Form approved OMB no. 1218-0176
Evans
Establishment name
CHECK ONLY ONE box for each case based on the
most serious outcome for that case:
Enter the number of
days the injured or ill
worker was:
Check the "injury" column or choose one type of
illness:
Tim Foster dba MPC (Maintenance Projects and Construction)
GA
Hearing L
oss
Classify the case
Days away
from workRemained at work
You must record information about every work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment beyond first aid. You must also record significant work-related injuries and illnesses that are diagnosed by a physician or licensed health care professional. You must also record work-related injuries and illnesses that meet any of the specific recording criteria listed in 29 CFR 1904.8 through 1904.12. Feel free to use two lines for a single case if you need to. You must complete an injury and illness incident report (OSHA Form 301) or equivalent form for each injury or illness recorded on this form. If you're not sure whether a case is recordable, call your local OSHA office for help.
Where the event
occurred (e.g.
Loading dock north
end)
All
oth
er
illnesses
Away
From
Work
(days) All
oth
er
illnesses
Skin
Dis
ord
er
Skin
Dis
ord
er
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Case
No.

Year 2012
Street
City Zip 30809
0 0 0 0
(G) (H) (I) (J) OR
5 4 1 3 3 0
0 0(K) (L)
Total number of… Knowingly falsifying this document may result in a fine.
(M)
(1) Injury 0 (4) Poisoning 0
(2) Skin Disorder 0 (5) Hearing Loss 0
(3) Respiratory
Condition 0 (6) All Other Illnesses 0
Employment information
Evans
Your establishment name
1198 Newport Trial
GA
Tim Foster - dba MPC (Maintenance Projects & Construction)
Sign here
State
Company executive
I certify that I have examined this document and that to the best of my knowledge the entries are true, accurate, and
complete.
3200
(706) 832-6719
Tim Foster
Phone
Total hours worked by all employees last
year
Standard Industrial Classification (SIC), if known (e.g., SIC 3715)
Annual average number of employees
North American Industrial Classification (NAICS), if known (e.g., 336212)
1
Total number of
other recordable
cases
Number of Days
Establishment information
Total number of
deaths
Number of Cases
Form approved OMB no. 1218-0176
Title
Date
Owner
7/10/2013
U.S. Department of Labor
OSHA's Form 300A (Rev. 01/2004)
Summary of Work-Related Injuries and IllnessesOccupational Safety and Health Administration
Total number of
days away from
work
Total number of days of
job transfer or restriction
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Injury and Illness Types
Industry description (e.g., Manufacture of motor truck trailers)
Post this Summary page from February 1 to April 30 of the year following the year covered by the form
All establishments covered by Part 1904 must complete this Summary page, even if no injuries or illnesses occurred during the year. Remember to review the Log to verify that the entries are complete
Using the Log, count the individual entries you made for each category. Then write the totals below, making sure you've added the entries from every page of the log. If you had no cases write "0."
Employees former employees, and their representatives have the right to review the OSHA Form 300 in its entirety. They also have limited access to the OSHA Form 301 or its equivalent. See 29 CFR 1904.35, in OSHA's Recordkeeping rule, for further details on the access provisions for these forms.
Total number of
cases with days
away from work
Total number of cases
with job transfer or
restriction

Year
City State
(A) (B) (C) (D) (E) (F)
(M)
(G) (H) (I) (J) (K) (L) (1) (2) (3) (4) (5)
Page totals 0 0 0 0 0 0 0 0 0 0 0
Page 1 of 1 (1) (2) (3) (4) (5)
Away
From
Work
(days)
Skin
Dis
ord
er
Skin
Dis
ord
er
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Tim Foster-MPC
GA
Hearing L
oss
Case
No.
Classify the case
Days away
from workRemained at work
Form approved OMB no. 1218-017
Evans
Establishment name
CHECK ONLY ONE box for each case based on the
most serious outcome for that case:
Enter the number of
days the injured or ill
worker was:
Check the "injury" column or choose one
illness:
Other record-
able cases
Identify the person Describe the case
Date of
injury or
onset of
illness
Inju
ry
Death(mo./day)
Pois
onin
gP
ois
onin
g
Hearing L
oss
Inju
ry
Describe injury or illness, parts of body affected,
and object/substance that directly injured or made
person ill (e.g. Second degree burns on right
forearm from acetylene torch)
Employee's Name Job Title (e.g.,
Welder)
Where the event occurred (e.g.
Loading dock north end)
Respirato
ry
Conditio
n
Respirato
ry
Conditio
n
On job
transfer or
restriction
(days)Job transfer
or restriction
Attention: This form contains information relating to
employee health and must be used in a manner that
protects the confidentiality of employees to the extent
possible while the information is being used for
occupational safety and health purposes. U.S. Department of LaborOccupational Safety and Health Administration
2013
You must record information about every work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment beyond first aid. You must also record significant work-related injuries and illnesses that are diagnosed by a physician or licensed health care professional. You must also record work-related injuries and illnesses that meet any of the specific recording criteria listed in 29 CFR 1904.8 through 1904.12. Feel free to use two lines for a single case if you need to. You must complete an injury and illness incident report (OSHA Form 301) or equivalent form for each injury or illness recorded on this form. If you're not sure whether a case is recordable, call your local OSHA office for help.
OSHA's Form 300 (Rev. 01/2004)
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Log of Work-Related Injuries and Illnesses
Year 2013
Street
City Zip 30809
0 0 0 0
(G) (H) (I) (J) OR
5 4 1 3 3 0
0 0(K) (L)
Total number of… Knowingly falsifying this document may result in a fine.
(M)
(1) Injury 0 (4) Poisoning 0
(2) Skin Disorder 0 (5) Hearing Loss 0
(3) Respiratory
Condition 0 (6) All Other Illnesses 0
Industry description (e.g., Manufacture of motor truck trailers)
Post this Summary page from February 1 to April 30 of the year following the year covered by the form
All establishments covered by Part 1904 must complete this Summary page, even if no injuries or illnesses occurred during the year. Remember to review the Log to verify that the entries are complete
Using the Log, count the individual entries you made for each category. Then write the totals below, making sure you've added the entries from every page of the log. If you had no cases write "0."
Employees former employees, and their representatives have the right to review the OSHA Form 300 in its entirety. They also have limited access to the OSHA Form 301 or its equivalent. See 29 CFR 1904.35, in OSHA's Recordkeeping rule, for further details on the access provisions for these forms.
Total number of
cases with days
away from work
Total number of cases
with job transfer or
restriction
Total number of
days away from
work
Total number of days of
job transfer or restriction
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Injury and Illness Types
U.S. Department of Labor
OSHA's Form 300A (Rev. 01/2004)
Summary of Work-Related Injuries and IllnessesOccupational Safety and Health Administration
Form approved OMB no. 1218-0176
Title
Date
Owner
1/27/2014
Establishment information
Total number of
deaths
Number of Cases
Total number of
other recordable
cases
Number of Days
Total hours worked by all employees last
year
Standard Industrial Classification (SIC), if known (e.g., SIC 3715)
Annual average number of employees
North American Industrial Classification (NAICS), if known (e.g., 336212)
1
706-832-6719
Tim Foster
Phone
Company executive
I certify that I have examined this document and that to the best of my knowledge the entries are true, accurate, and
complete.
2306.5
Tim Foster - MPC
Sign here
State
Employment information
Evans
Your establishment name
1198 Newport Trl
GA

Year
City State
(A) (B) (C) (D) (E) (F)
(M)
(G) (H) (I) (J) (K) (L) (1) (2) (3) (4) (5)
Page totals 0 0 0 0 0 0 0 0 0 0 0
Page 1 of 1 (1) (2) (3) (4) (5)
Away
From
Work
(days)
Skin
Dis
ord
er
Skin
Dis
ord
er
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Tim Foster - MPC
GA
Hearing L
oss
Case
No.
Classify the case
Days away
from workRemained at work
Form approved OMB no. 1218-017
Evans
Establishment name
CHECK ONLY ONE box for each case based on the
most serious outcome for that case:
Enter the number of
days the injured or ill
worker was:
Check the "injury" column or choose one
illness:
Other record-
able cases
Identify the person Describe the case
Date of
injury or
onset of
illness
Inju
ry
Death(mo./day)
Pois
onin
gP
ois
onin
g
Hearing L
oss
Inju
ry
Describe injury or illness, parts of body affected,
and object/substance that directly injured or made
person ill (e.g. Second degree burns on right
forearm from acetylene torch)
Employee's Name Job Title (e.g.,
Welder)
Where the event occurred (e.g.
Loading dock north end)
Respirato
ry
Conditio
n
Respirato
ry
Conditio
n
On job
transfer or
restriction
(days)Job transfer
or restriction
Attention: This form contains information relating to
employee health and must be used in a manner that
protects the confidentiality of employees to the extent
possible while the information is being used for
occupational safety and health purposes. U.S. Department of LaborOccupational Safety and Health Administration
2014
You must record information about every work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment beyond first aid. You must also record significant work-related injuries and illnesses that are diagnosed by a physician or licensed health care professional. You must also record work-related injuries and illnesses that meet any of the specific recording criteria listed in 29 CFR 1904.8 through 1904.12. Feel free to use two lines for a single case if you need to. You must complete an injury and illness incident report (OSHA Form 301) or equivalent form for each injury or illness recorded on this form. If you're not sure whether a case is recordable, call your local OSHA office for help.
OSHA's Form 300 (Rev. 01/2004)
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Log of Work-Related Injuries and Illnesses

Year 2014
Street
City Zip 30809
0 0 0 0
(G) (H) (I) (J) OR
5 4 1 3 3 0
0 0(K) (L)
Total number of… Knowingly falsifying this document may result in a fine.
(M)
(1) Injury 0 (4) Poisoning 0
(2) Skin Disorder 0 (5) Hearing Loss 0
(3) Respiratory
Condition 0 (6) All Other Illnesses 0
Industry description (e.g., Manufacture of motor truck trailers)
Post this Summary page from February 1 to April 30 of the year following the year covered by the form
All establishments covered by Part 1904 must complete this Summary page, even if no injuries or illnesses occurred during the year. Remember to review the Log to verify that the entries are complete
Using the Log, count the individual entries you made for each category. Then write the totals below, making sure you've added the entries from every page of the log. If you had no cases write "0."
Employees former employees, and their representatives have the right to review the OSHA Form 300 in its entirety. They also have limited access to the OSHA Form 301 or its equivalent. See 29 CFR 1904.35, in OSHA's Recordkeeping rule, for further details on the access provisions for these forms.
Total number of
cases with days
away from work
Total number of cases
with job transfer or
restriction
Total number of
days away from
work
Total number of days of
job transfer or restriction
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instruction, search and gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Injury and Illness Types
U.S. Department of Labor
OSHA's Form 300A (Rev. 01/2004)
Summary of Work-Related Injuries and IllnessesOccupational Safety and Health Administration
Form approved OMB no. 1218-0176
Title
Date
Owner Operator
1/7/2015
Establishment information
Total number of
deaths
Number of Cases
Total number of
other recordable
cases
Number of Days
Total hours worked by all employees last
year
Standard Industrial Classification (SIC), if known (e.g., SIC 3715)
Annual average number of employees
North American Industrial Classification (NAICS), if known (e.g., 336212)
1
706-832-6719
Tim Foster
Phone
Company executive
I certify that I have examined this document and that to the best of my knowledge the entries are true, accurate, and
complete.
2730
Tim Foster - MPC
Sign here
State
Employment information
Evans
Your establishment name
1198 Newport Trl
GA

Year
City State
(A) (B) (C) (D) (E) (F)
(M)
(G) (H) (I) (J) (K) (L) (1) (2) (3) (4) (5) (6)
- - - - - - 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
Page totals 0 0 0 0 0 0 0 0 0 0 0 0
Page 1 of 1 (1) (2) (3) (4)
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time
to review the instruction, search and gather the data needed, and complete and review the collection of information.
Persons are not required to respond to the collection of information unless it displays a currently valid OMB control
number. If you have any comments about these estimates or any aspects of this data collection, contact: US
Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do
not send the completed forms to this office.
Log of Work-Related Injuries and Illnesses
Attention: This form contains information relating
to employee health and must be used in a manner
that protects the confidentiality of employees to the
extent possible while the information is being used
for occupational safety and health purposes. U.S. Department of LaborOccupational Safety and Health Administration
2015
You must record information about every work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment
beyond first aid. You must also record significant work-related injuries and illnesses that are diagnosed by a physician or licensed health care professional. You must also record work-related
injuries and illnesses that meet any of the specific recording criteria listed in 29 CFR 1904.8 through 1904.12. Feel free to use two lines for a single case if you need to. You must complete
an injury and illness incident report (OSHA Form 301) or equivalent form for each injury or illness recorded on this form. If you're not sure whether a case is recordable, call your local OSHA
office for help.
Employee's Name Job Title (e.g.,
Welder)
Where the event occurred (e.g.
Loading dock north end)
Identify the person Describe the case
OSHA's Form 300 (Rev. 01/2004)
Job transfer
or restriction
Date of
injury or
onset of
illnessDeath(mo./day)
Days away
from work
Inju
ry
Hearing L
oss
Remained at work
Respirato
ry
Conditio
n
Respirato
ry
Conditio
n
On job
transfer or
restriction
(days)
Describe injury or illness, parts of body affected,
and object/substance that directly injured or made
person ill (e.g. Second degree burns on right
forearm from acetylene torch)
Form approved OMB no. 1218-0176
Evans
Establishment name
CHECK ONLY ONE box for each case based on
the most serious outcome for that case:
Enter the number of
days the injured or ill
worker was:
Check the "injury" column or choose one type of
illness:
Tim Foster dba MPC
GA
Classify the case
All
oth
er
illnesses
Away
From
Work
(days)
All
Oth
er
Illn
esses
Skin
Dis
ord
er
Skin
Dis
ord
er
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Case
No.
Pois
onin
gP
ois
onin
g
Hearing L
oss
Inju
ry
Other record-
able cases

Year 2015
Street
City Zip 30809
0 0 0 0
(G) (H) (I) (J) OR
5 4 1 3 3 0
0 0(K) (L)
Total number of… Knowingly falsifying this document may result in a fine.
(M)
(1) Injury 0 (4) Poisoning 0
(2) Skin Disorder 0 (5) Hearing Loss 0
(3) Respiratory
Condition 0 (6) All Other Illnesses 0
North American Industrial Classification (NAICS), if known (e.g., 336212)
Employment information
Evans
Your establishment name
1198 Newport Trl
GA
(706) 832-6719
Tim Foster
Phone
Company executive
I certify that I have examined this document and that to the best of my knowledge the entries are
true, accurate, and complete.
Total number of
other recordable
cases
Number of Days
All establishments covered by Part 1904 must complete this Summary page, even if no injuries or
illnesses occurred during the year. Remember to review the Log to verify that the entries are complete
Total hours worked by all employees last
year
Annual average number of employees 1
Tim Foster dba MPC
State
Establishment information
Total number of
deaths
Number of Cases
Using the Log, count the individual entries you made for each category. Then write the totals below,
making sure you've added the entries from every page of the log. If you had no cases write "0."
Employees former employees, and their representatives have the right to review the OSHA Form 300 in
its entirety. They also have limited access to the OSHA Form 301 or its equivalent. See 29 CFR
1904.35, in OSHA's Recordkeeping rule, for further details on the access provisions for these forms.
Total number of
cases with days
away from work
Total number of cases
with job transfer or
restriction
2,820
Sign here
Standard Industrial Classification (SIC), if known (e.g., SIC 3715)
Form approved OMB no. 1218-0176
Title
Date
Owner
January 20, 2016
Engineering Services
Total number of
days away from
work
Total number of days of
job transfer or restriction
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instruction, search and
gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it
displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department
of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Injury and Illness Types
Industry description (e.g., Manufacture of motor truck trailers)
Post this Summary page from February 1 to April 30 of the year following the year covered by the form
U.S. Department of Labor
OSHA's Form 300A (Rev. 01/2004)
Summary of Work-Related Injuries and IllnessesOccupational Safety and Health Administration
Year
City State
(A) (B) (C) (D) (E) (F)
(M)
(G) (H) (I) (J) (K) (L) (1) (2) (3) (4) (5) (6)
- - - - - - 0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
Page totals 0 0 0 0 0 0 0 0 0 0 0 0
Page 1 of 1 (1) (2) (3) (4)
All
oth
er
illnesses
Away
From
Work
(days)
All
Oth
er
Illn
esses
Skin
Dis
ord
er
Skin
Dis
ord
er
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Case
No.
Pois
onin
gP
ois
onin
g
Hearing L
oss
Inju
ry
Other record-
able cases
Form approved OMB no. 1218-0176
Evans
Establishment name
CHECK ONLY ONE box for each case based on
the most serious outcome for that case:
Enter the number of
days the injured or ill
worker was:
Check the "injury" column or choose one type of
illness:
Tim Foster dba Maintenance Projects & Construction
GA
Classify the case
Respirato
ry
Conditio
n
Respirato
ry
Conditio
n
On job
transfer or
restriction
(days)
Describe injury or illness, parts of body affected,
and object/substance that directly injured or made
person ill (e.g. Second degree burns on right
forearm from acetylene torch)
OSHA's Form 300 (Rev. 01/2004)
Job transfer
or restriction
Date of
injury or
onset of
illnessDeath(mo./day)
Days away
from work
Inju
ry
Hearing L
oss
Remained at work
Employee's Name Job Title (e.g.,
Welder)
Where the event occurred (e.g.
Loading dock north end)
Identify the person Describe the case
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time
to review the instruction, search and gather the data needed, and complete and review the collection of information.
Persons are not required to respond to the collection of information unless it displays a currently valid OMB control
number. If you have any comments about these estimates or any aspects of this data collection, contact: US
Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do
not send the completed forms to this office.
Log of Work-Related Injuries and Illnesses
Attention: This form contains information relating
to employee health and must be used in a manner
that protects the confidentiality of employees to the
extent possible while the information is being used
for occupational safety and health purposes. U.S. Department of LaborOccupational Safety and Health Administration
2016
You must record information about every work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment
beyond first aid. You must also record significant work-related injuries and illnesses that are diagnosed by a physician or licensed health care professional. You must also record work-related
injuries and illnesses that meet any of the specific recording criteria listed in 29 CFR 1904.8 through 1904.12. Feel free to use two lines for a single case if you need to. You must complete
an injury and illness incident report (OSHA Form 301) or equivalent form for each injury or illness recorded on this form. If you're not sure whether a case is recordable, call your local OSHA
office for help.

Year 2016
Street
City Zip 30809
0 0 0 0
(G) (H) (I) (J) OR
5 4 1 3 3 0
0 0(K) (L)
Total number of… Knowingly falsifying this document may result in a fine.
(M)
(1) Injury 0 (4) Poisoning 0
(2) Skin Disorder 0 (5) Hearing Loss 0
(3) Respiratory
Condition 0 (6) All Other Illnesses 0
U.S. Department of Labor
OSHA's Form 300A (Rev. 01/2004)
Summary of Work-Related Injuries and IllnessesOccupational Safety and Health Administration
Form approved OMB no. 1218-0176
Title
Date
Owner
January 24, 2017
Engineering Services
Total number of
days away from
work
Total number of days of
job transfer or restriction
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instruction, search and
gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it
displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department
of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Injury and Illness Types
Industry description (e.g., Manufacture of motor truck trailers)
Post this Summary page from February 1 to April 30 of the year following the year covered by the form
Establishment information
Total number of
deaths
Number of Cases
Using the Log, count the individual entries you made for each category. Then write the totals below,
making sure you've added the entries from every page of the log. If you had no cases write "0."
Employees former employees, and their representatives have the right to review the OSHA Form 300 in
its entirety. They also have limited access to the OSHA Form 301 or its equivalent. See 29 CFR
1904.35, in OSHA's Recordkeeping rule, for further details on the access provisions for these forms.
Total number of
cases with days
away from work
Total number of cases
with job transfer or
restriction
2,390
Sign here
Standard Industrial Classification (SIC), if known (e.g., SIC 3715)
Total number of
other recordable
cases
Number of Days
All establishments covered by Part 1904 must complete this Summary page, even if no injuries or
illnesses occurred during the year. Remember to review the Log to verify that the entries are complete
Total hours worked by all employees last
year
Annual average number of employees 1
Tim Foster dba Maintenance Projects & Construction
State
(706) 832-6719
Tim Foster
Phone
Company executive
I certify that I have examined this document and that to the best of my knowledge the entries are
true, accurate, and complete.
North American Industrial Classification (NAICS), if known (e.g., 336212)
Employment information
Evans
Your establishment name
1198 Newport Trl
GA

Year
City State
(A) (B) (C) (D) (E) (F)
(M)
(G) (H) (I) (J) (K) (L) (1) (2) (3) (4) (5) (6)
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
0 0 0 0 0 0 0 0 0 0 0 0
Page totals 0 0 0 0 0 0 0 0 0 0 0 0
Page 1 of 1 (1) (2) (3) (4)
All
oth
er
illn
esse
s
Away
From
Work
(days)
All
Oth
er
Illn
esse
s
Skin
Dis
ord
er
Skin
Dis
ord
er
Be sure to transfer these totals to the Summary page (Form 300A) before you post it.
Case
No.
Po
iso
nin
gP
ois
on
ing
He
ari
ng
Lo
ss
Inju
ry
Other record-
able cases
Form approved OMB no. 1218-0176
Evans
Establishment name
CHECK ONLY ONE box for each case based on
the most serious outcome for that case:
Enter the number of
days the injured or ill
worker was:
Check the "injury" column or choose one type
of illness:
Tim Foster - MPC
GA
Classify the case
Re
sp
ira
tory
Co
nd
itio
n
Re
sp
ira
tory
Co
nd
itio
n
On job
transfer or
restriction
(days)
Describe injury or illness, parts of body affected,
and object/substance that directly injured or
made person ill (e.g. Second degree burns on
right forearm from acetylene torch)
OSHA's Form 300 (Rev. 01/2004)
Job transfer
or restriction
Date of
injury or
onset of
illnessDeath(mo./day)
Days away
from work
Inju
ry
He
ari
ng
Lo
ss
Remained at work
Employee's Name Job Title (e.g.,
Welder)
Where the event occurred (e.g.
Loading dock north end)
Identify the person Describe the case
Public reporting burden for this collection of information is estimated to average 14 minutes per response, including time
to review the instruction, search and gather the data needed, and complete and review the collection of information.
Persons are not required to respond to the collection of information unless it displays a currently valid OMB control
number. If you have any comments about these estimates or any aspects of this data collection, contact: US
Department of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do
not send the completed forms to this office.
Log of Work-Related Injuries and Illnesses
Attention: This form contains information relating
to employee health and must be used in a manner
that protects the confidentiality of employees to the
extent possible while the information is being used
for occupational safety and health purposes. U.S. Department of LaborOccupational Safety and Health Administration
2017
You must record information about every work-related injury or illness that involves loss of consciousness, restricted work activity or job transfer, days away from work, or medical treatment
beyond first aid. You must also record significant work-related injuries and illnesses that are diagnosed by a physician or licensed health care professional. You must also record work-related
injuries and illnesses that meet any of the specific recording criteria listed in 29 CFR 1904.8 through 1904.12. Feel free to use two lines for a single case if you need to. You must complete an
injury and illness incident report (OSHA Form 301) or equivalent form for each injury or illness recorded on this form. If you're not sure whether a case is recordable, call your local OSHA office
for help.
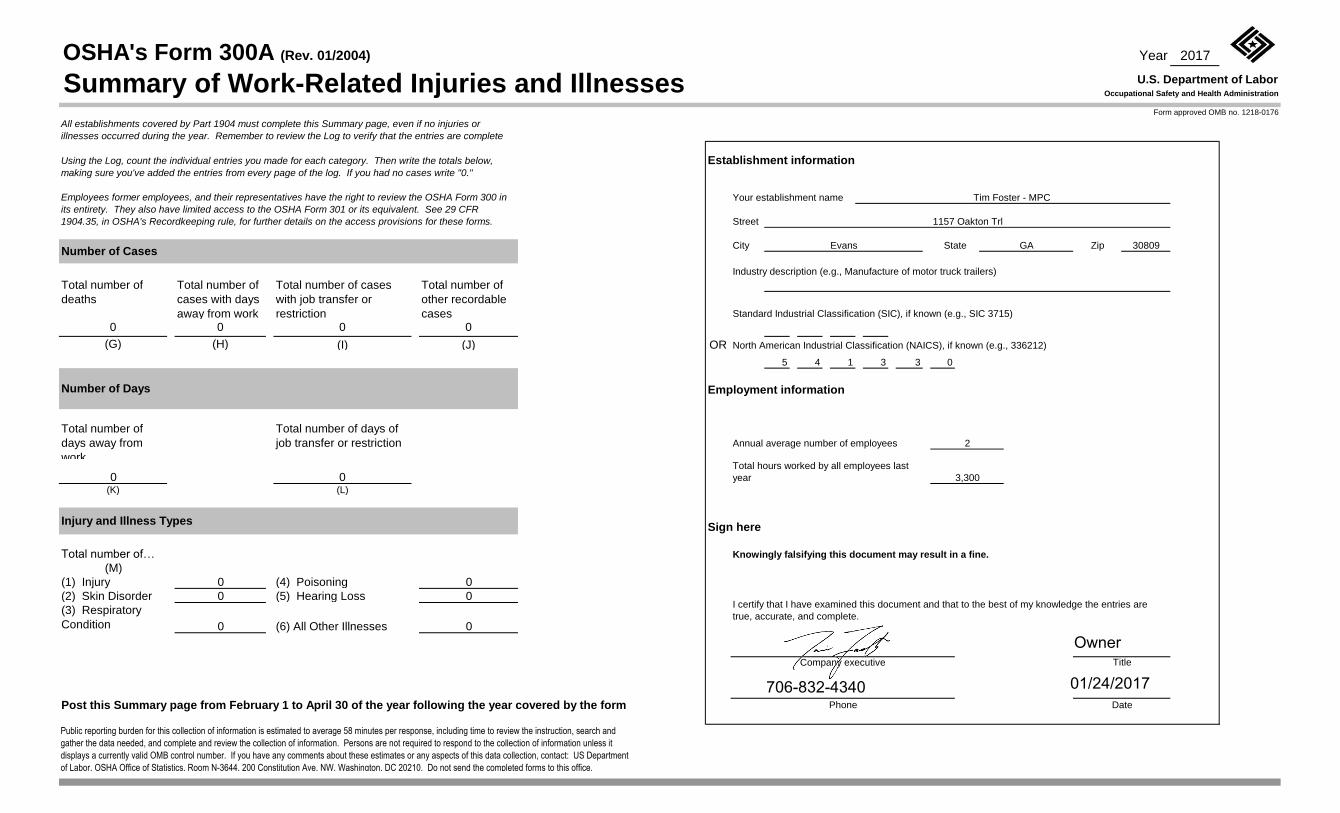
Year 2017
Street
City Zip 30809
0 0 0 0
(G) (H) (I) (J) OR
5 4 1 3 3 0
0 0(K) (L)
Total number of… Knowingly falsifying this document may result in a fine.
(M)
(1) Injury 0 (4) Poisoning 0
(2) Skin Disorder 0 (5) Hearing Loss 0
(3) Respiratory
Condition 0 (6) All Other Illnesses 0
U.S. Department of Labor
OSHA's Form 300A (Rev. 01/2004)
Summary of Work-Related Injuries and IllnessesOccupational Safety and Health Administration
Form approved OMB no. 1218-0176
Title
Date
Total number of
days away from
work
Total number of days of
job transfer or restriction
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instruction, search and
gather the data needed, and complete and review the collection of information. Persons are not required to respond to the collection of information unless it
displays a currently valid OMB control number. If you have any comments about these estimates or any aspects of this data collection, contact: US Department
of Labor, OSHA Office of Statistics, Room N-3644, 200 Constitution Ave, NW, Washington, DC 20210. Do not send the completed forms to this office.
Injury and Illness Types
Industry description (e.g., Manufacture of motor truck trailers)
Post this Summary page from February 1 to April 30 of the year following the year covered by the form
Establishment information
Total number of
deaths
Number of Cases
Using the Log, count the individual entries you made for each category. Then write the totals below,
making sure you've added the entries from every page of the log. If you had no cases write "0."
Employees former employees, and their representatives have the right to review the OSHA Form 300 in
its entirety. They also have limited access to the OSHA Form 301 or its equivalent. See 29 CFR
1904.35, in OSHA's Recordkeeping rule, for further details on the access provisions for these forms.
Total number of
cases with days
away from work
Total number of cases
with job transfer or
restriction
3,300
Sign here
Standard Industrial Classification (SIC), if known (e.g., SIC 3715)
North American Industrial Classification (NAICS), if known (e.g., 336212)
Total number of
other recordable
cases
Number of Days
All establishments covered by Part 1904 must complete this Summary page, even if no injuries or
illnesses occurred during the year. Remember to review the Log to verify that the entries are complete
Total hours worked by all employees last
year
Annual average number of employees 2
Tim Foster - MPC
State
Phone
Company executive
I certify that I have examined this document and that to the best of my knowledge the entries are
true, accurate, and complete.
Employment information
Evans
Your establishment name
1157 Oakton Trl
GA
Owner
706-832-4340 01/24/2017

U.S. Department of LaborOccupational Safety and Health Administration
OSHA’s Form 300A (Rev. 01/2004)Year 20__ __
Summary of Work-Related Injuries and IllnessesForm approved OMB no. 1218-0176
Total number ofdeaths
__________________
Total number ofcases with daysaway from work
__________________
Number of Cases
Total number of days awayfrom work
___________
Total number of days of jobtransfer or restriction
___________
Number of Days
Post this Summary page from February 1 to April 30 of the year following the year covered by the form.
All establishments covered by Part 1904 must complete this Summary page, even if no work-related injuries or illnesses occurred during the year. Remember to review the Log
to verify that the entries are complete and accurate before completing this summary.
Using the Log, count the individual entries you made for each category. Then write the totals below, making sure you’ve added the entries from every page of the Log. If you
had no cases, write “0.”
Employees, former employees, and their representatives have the right to review the OSHA Form 300 in its entirety. They also have limited access to the OSHA Form 301 or
its equivalent. See 29 CFR Part 1904.35, in OSHA’s recordkeeping rule, for further details on the access provisions for these forms.
Establishment information
Employment information
Your establishment name __________________________________________
Street _________________________ _______
City ____________________________ State ______ ZIP _________
Industry description ( )
_______________________________________________________
Standard Industrial Classification (SIC), if known ( )
____ ____ ____ ____
North American Industrial Classification (NAICS), if known (e.g., 336212)
e.g., Manufacture of motor truck trailers
e.g., 3715
(I ee the
Worksheet on the back of this page to estimate.)
_____________________
OR
____ ____ ____ ____ ____ ____
Annual average number of employees ______________
Total hours worked by all employees last year ______________
f you don’t have these figures, s
Sign here
Knowingly falsifying this document may result in a fine.
I certify that I have examined this document and that to the best of myknowledge the entries are true, accurate, and complete.
___________________________________________________________
___________________________________________________________
Company executive Title
Phone Date( ) - / /
Public reporting burden for this collection of information is estimated to average 58 minutes per response, including time to review the instructions, search and gather the data needed, andcomplete and review the collection of information. Persons are not required to respond to the collection of information unless it displays a currently valid OMB control number. If you have anycomments about these estimates or any other aspects of this data collection, contact: US Department of Labor, OSHA Office of Statistical Analysis, Room N-3644, 200 Constitution Avenue, NW,Washington, DC 20210. Do not send the completed forms to this office.
Total number of . . .
Skin disorders ______
Respiratory conditions ______
Injuries ______
Injury and Illness Types
Poisonings ______
Hearing loss
All other illnesses ______
______
(G) (H) (I) (J)
(K) (L)
(M)(1)
(2)
(3)
(4)
(5)
(6)
Total number ofcases with jobtransfer or restriction
__________________
Total number ofother recordablecases
__________________
0
Tim Foster - MPC
5997
1157 Oakton Trl
0
0
Evans
0
GA
0
0
18
0
3
30809
25 192
3 3 0
0
0
0 0
5
0
4 1
706-832-4640
Owner

MPC REFERENCES/COLLEAGUES: Imagine That Engineering
RGV, Inc.
DKC Services Inc.
Packers Hydraulic Solutions
IEServices
Quality Piping & Fabricating
Creekstone Farms Premium Beef, LLC.
FPL Foods
JBS
New Angus LLC.
Northern Beef Packers
Sunterra Meats
Tyson Foods Inc.

All Power Inc.
Artic Insulation
ASKSteve Inc.
BIRKO/CHAD Equipment
BETTCHER Industries
Brookside & Lane Associates
DORAL
E&T Electric, LLC
Economical Design Solutions
Elanco
Food Safety Net Services
Frontline Industrial
IEH Laboratories and Consulting
InPwr Inc.
IMS Texas
Jarvis
JKMI
Kornex
Kusel Equipment

Mallot Creek Group
MBA Suppliers
McNeil Refrigeration
Mid States Supply Company
Midlands Mechanical
Midwest Metal Craft
Millard Manufacturing Corp
Multiple Systems
PB Metal Fab LLC
PhD Consulting
Preston Refrigeration
Prestressed Concrete, Inc.
Proteus Industries
Quality Metal Supply
Reiser
SB Packing House Equipment
SBI General & Mechanical
Schmeeckle Bros. Construction Co.
Schneider Structural Engineering
SFK LEBLANC

SCR
Tippmann Group
Vande Berg Scales
VCP&A
Woodruff & Howe
Environmental Engineering