community paramedicine pilot program - healthforce.ucsf.edu · community paramedicine 2 a locally...
TRANSCRIPT

Community Paramedicine Pilot Program Summary and Two Year Evaluation
University of California, San FranciscoPhilip R. Lee Institute for Health Policy Studies and
Healthforce CenterJanet Coffman, MPP, PhD
Lead Evaluator
California Emergency Medical Services AuthorityHoward Backer, MD, MPH, FACEP
PI for HWPP #173
Lou MeyerProject Manager

Working Definition of Community Paramedicine
2
A locally determined community-based, collaborative model of care that leverages the skills of paramedics and EMS systems to address care gaps identified through a community-specific health care needs assessment.�New models of community-based health care that bridge primary care and emergency care
�Utilizes paramedics outside their traditional emergency response and transport roles

Why Paramedics?�Trusted and accepted by the public�In most communities--inner city and rural�Work in home and community-based settings �Licensed personnel that operate under medical control as part of a system of care�Trained to make health status assessments, recognize and manage life-threatening conditions outside of the hospital�Always available (24 / 7 / 365)
3

Community Paramedicine Concepts� Post hospital discharge short-term follow-up� Frequent EMS user case management� Directly Observed Therapy for tuberculosis: public
health department collaboration � Hospice support� Alternate destination to mental health crisis center� Alternate destination to sobering center� Alternate destination to urgent care center (Cancelled)
4
Methods�Evaluation period 24 to 28 months except for alternate destination to sobering center (depending on project start time between June 2015-October 2015)� Outcomes assessed across three domains
• Safety• Effectiveness• Potential savings accrued by other parts of the health
care system
5

Cumulative Patients Enrolled by Conceptthrough September 2017*
Concept # EnrolledPost-Discharge Short-term Follow-Up 1,401Frequent EMS Users 103Directly Observed Therapy for Tuberculosis 42Hospice 270Alternate Destination – Mental Health 251Alternate Destination –Sobering Center 400Alternate Destination – Urgent Care 48§
All Projects 2,515
6
* 24 to 28 months for individual projects, depending on start date except for alternate destination to sobering center§ Pilot projects for alternate destination urgent care cancelled

Enrolled Patients’ Payer Types –Through September 2017
46%
34%
9%
11%
MedicareMedi-CalUninsuredPrivate Insurance
7
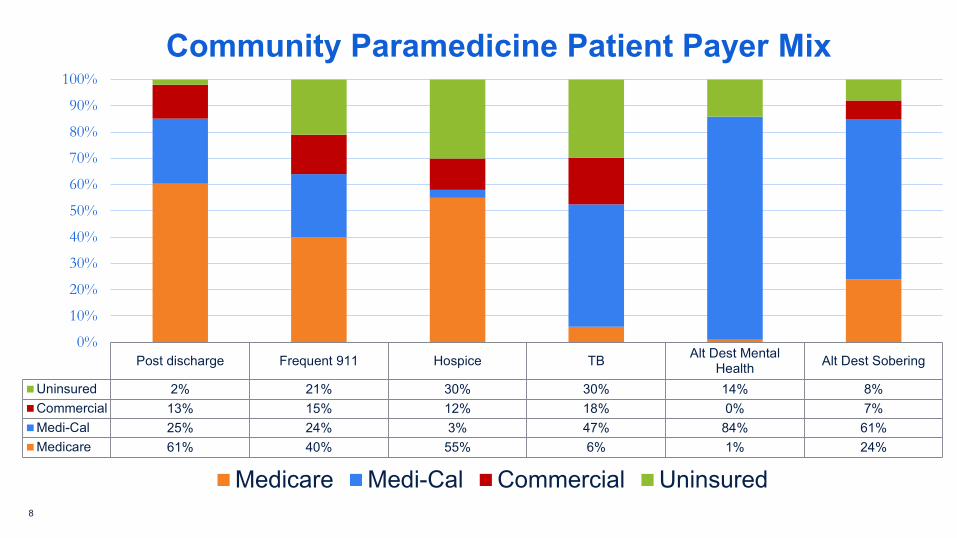
Post discharge Frequent 911 Hospice TB Alt Dest MentalHealth Alt Dest Sobering
Uninsured 2% 21% 30% 30% 14% 8%Commercial 13% 15% 12% 18% 0% 7%Medi-Cal 25% 24% 3% 47% 84% 61%Medicare 61% 40% 55% 6% 1% 24%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Community Paramedicine Patient Payer Mix
Medicare Medi-Cal Commercial Uninsured8
Post-Discharge Short-term Follow-Up �Decreased hospital readmissions within 30 days for at least one diagnosis at all sites�CPs identified 229 patients (16%) who misunderstood how to take their medications or had duplicate medications and were at risk for adverse effects.�All five post-discharge projects achieved potential cost savings for payers, primarily Medicare and Medi-Cal.
9

Project Impact on 30 Day Hospital Readmission Rate
24.4 22.5 23.1 23.1 22.117.2 16.8
19.4 18.9 20.1
6.5
28.4
7.7 8.6 8.510.7
0
16.7
8.1
13.6
051015202530
UCLA CHFButte CHF* AlamedaCHF
SanBernardino
CHF
SolanoCHF
Butte MI AlamedaMI
AlamedaCOPD
SolanoCOPD
Alamedapneumonia
Historical vs Project Readmission Rate (%)
Historical Project
10
*All projects except Butte CHF and Alameda COPD showed statistically significant reduction in the readmission rate for enrolled patients relative to the partner hospitals’ historical readmission rates (p value < 0.05). Alameda COPD had no statistically significant difference. Butte CHF had a higher readmission rate than the historical rate.
Frequent EMS Users �Reductions in numbers of 911 calls, ambulance transports, and ED visits among enrolled patients. �Assisted patients in obtaining housing and other non-emergency services that met the physical, psychological, and social needs that led to their frequent EMS use �EMS collaboration with many other community organizations
11

Reduction in Emergency Services: Frequent 911 Users
955
131
625
1100
200
400
600
800
1000
1200
San Diego 911 calls Alameda 911 callsBaseline Post Intervetion
35% Reduction
16% Reduction
12 Note: 24 months of operation for San Diego, 28 months for Alameda

Directly Observed Therapy for Tuberculosis
�Dispensed appropriate doses of tuberculosis (TB) medications and monitored side effects and symptoms that could necessitate a change in treatment regimen �CPs achieved better compliance (99.9%) than community health workers (93.3%) and provided care to patients that CHW could not reach�Demonstrates capability for collaborative work with public health
13

Hospice Support�Provided hospice patients and their families with psychosocial support and administered medications in consultation with a hospice nurse, until nurse could arrive� In accordance with patient wishes, reduced rates of ambulance transports to an ED�Potential savings for Medicare and other payers by reducing unnecessary ambulance transports, ED visits, and hospitalizations
14

Percent of 911 Calls for Hospice Patients Resulting in Transport to ED
1/23/201715
(26 months data; N=270 hospice patient calls to 911 )80%
30%
0%10%20%30%40%50%60%70%80%90%
Prior to the pilot (all hospice calls) During the pilot (911 calls forpatients of partner hospices)

Alternate Destination – Mental Health � Performed medical screening of patients to determine whether they
could be safely transported directly to a mental health crisis center
� 96% of patients enrolled were evaluated at the mental health crisis center without the delay of a preliminary ED visit.
�Over study period (24 months), 4% of patients required subsequent transfer to the ED (9 patients)
� Potential savings for payers, primarily Medi-Cal, due to reduced ED visits and subsequent transfer to mental health center
� Strongly supported by law enforcement because reduces the amount of time required for mental health calls
16

Alternate Destination—Mental Health
251
252
389
5423
Number of Enrolled, Eligible, and Ineligible PatientsN=969 patients evaluated over 24 months
Enrolled-transportedEligible-not enrolled due to lack of capacity or insurance typeIneligible-Intoxicated, medicalIneligible-Prior disruptive behaviorDid not consent
17

Alternate Destination-Sobering� Performed medical screening of patients to determine whether they
could be safely transported directly to a sobering center
� Enrolled and transported 400 patients in first 8 months.
� Ten patients (2.5%) were transferred to an ED within six hours of admission to the sobering center due to medical complaints
• 9/10 complaints developed after admission to sobering center
• 7 subsequently treated and released, 2 transferred for psych eval, 1 left ED without being seen
� Potential savings for payers, primarily Medi-Cal, due to reduced ED visits
18

Alternate Destination – Urgent Care� Insufficient data to make firm conclusions about this model�No patients experienced an adverse outcome, although two patients were transferred to an ED following admission to an urgent care center �Nine patients were rerouted to an ED because the urgent care center declined to accept �Projects closed: Multiple barriers to this model in California, although successful in other states
19
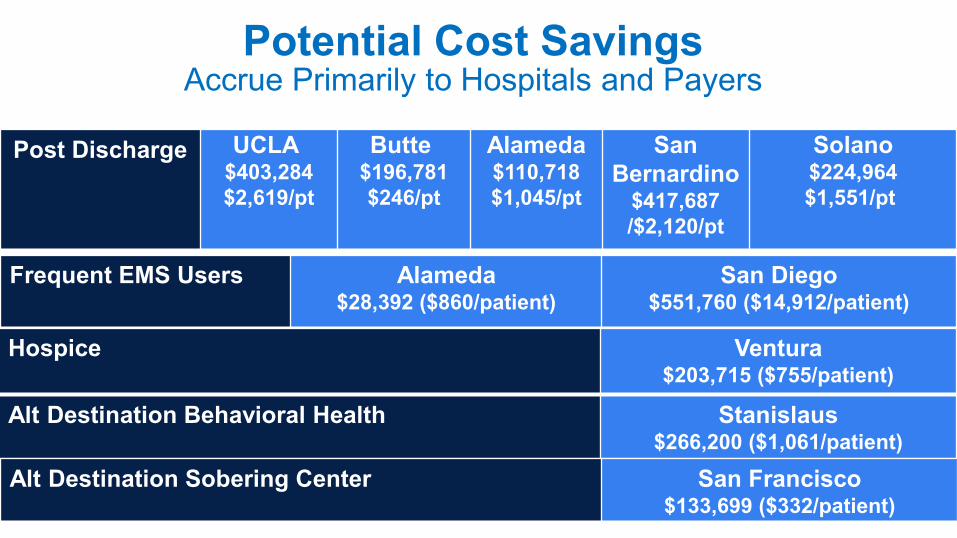
Potential Cost Savings Accrue Primarily to Hospitals and Payers
Post Discharge UCLA$403,284$2,619/pt
Butte$196,781$246/pt
Alameda$110,718$1,045/pt
San Bernardino
$417,687/$2,120/pt
Solano$224,964$1,551/pt
20
Frequent EMS Users Alameda$28,392 ($860/patient)
San Diego$551,760 ($14,912/patient)
Hospice Ventura$203,715 ($755/patient)
Alt Destination Behavioral Health Stanislaus$266,200 ($1,061/patient)
Alt Destination Sobering Center San Francisco$133,699 ($332/patient)

Conclusion�Specially trained paramedics can provide services beyond their traditional and current statutory scope of practice in California�Projects have improved patients’ well-being�No adverse outcomes for patients�No other health professionals displaced� In most cases, yielded savings for health plans and hospitals
21