community health nursing 1 quiz
DESCRIPTION
chnTRANSCRIPT

COMMUNITY HEALTH NURSINGTEODORA J.T. MACALINCAG,R.M.,R.N., M.P.H.
Clinical Instructor

COMMUNITY
Social group determined with geographic boundaries, common values and interest.
-Its members known to interact each others
its function with a particular social structure exhibits, and create norms, values and social
institution .

HEALTH
It is a state complete physical, mental, social wellbeing not merely the absence of disease or Infirmity. (WHO)
State of well being and using power the individual possess to the fullest extent. (Nightingale)
An on going process- a way of life through which a person develops and encourages every aspects of the body, mind and feelings to interrelate harmoniously as much as possible. (Kozier)
The modern concept of health refer to optimum level of individual, families, and community.

Nursing
Is an art and science of holistic, adaptive caring and helping profession with focus centered to client concerned with health promotion, health maintenance and health restoration.

NURSING
(ADPCN) Nursing is a dynamic discipline. It is an art & science of caring for individuals, families groups & communities geared toward promotion & restoration of health, prevention of illness, alleviation of suffering & assisting clients to face death w/ dignity and peace. It is focused on assisting client as he or she responds to health –illness situations, utilizing the nursing process & guided by ethico-legal moral principles.
Art-gained frm experiences, practice
Science –scientifically tested knowledge
COMMUNITY HEALTH NURSING
Field of nursing practice where services are carried out in the community settings such as home, work place, puericulture, clinic and the like.
Scope of services covered the whole range of health promotive, preventive, curative & rehabilitative.
Special field of nursing that combines the (A) skills and knowledge of nursing, (B) public health (C) some phases of assistance and functions.
The nature of practice is comprehensive, general, continual and not episodic.
It s practice directed to individuals, families, and groups, the dominant responsibility is to the population as a whole.

PUBLIC HEALTH
Art & science of preventing disease prolonging life, promoting health, efficiency.
Services for early diagnosis & preventive treatment of disease and the development of social machinery to ensure everyone standard of living adequate for maintenance of health organizing of these benefits as to able every citizen to realize his birthright of health and longevity.
Health as Multi Factorial Phenomenon
A. PoliticalThe political climate affects health. This involves one’s leadership, howhe/she rules, manages and involves other people in decision making. Ifour leaders today did not give emphasis on the health of citizens, therewould be government funding nor would there be any government ledprograms for health. The following are subcomponents1. Safety· Is the condition of being from harm, injury or loss (Webster)If there were no laws to ensure protection from exploitative working
conditions, slavery could possibly exist and safety as a health need wouldnot be a right. Government is also expanding access to social security. Today, every Filipino has a right to obtain health benefits as a result of his/her SSS membership

Political
2. OppressionOppression is unjust or cruel exercise of
authority or power. Before the advent of a democratic way of government, people were more prone to oppression. This does not mean that oppression does not exist today it still looms in our political environment. It ultimately contributes to the poverty of citizen and in the long run the health status of the people as they are not able to purchase the necessary drugs for their illness / condition.
Political
3. Political willPolitical will is the determination to pursue
something which is in the interest of the majority. This is a quality of a democratic
government. The people are allowed to choose their representatives in congress for enactment of laws and government.

Political
4. EmpowermentEmpowerment is the ability of a person to
do something, creating the circumstances where people can use their faculties and abilities at the maximum use level in the pursuit of common goals. When one is empowered he or she feels as though they are able to make responsible choices and decide on future steps based on their needs

Cultural
B. CulturalCulture is the representation of nonphysical traits such as
values,beliefs, attitudes and customs shared by a group of people and passed from one generation to the next (Potter, 1993), these can be:
1. Practices – In health care, these are customary actions usually done to promote and maintain health like use of anting -anting or lucky charms
2. Beliefs – which is a state or habit of mind wherein a group of people place a trust into something or a person (Webster) In health care, beliefs motivate one’s behavior to achieve health. Take for example the belief that you
should not take baths on Fridays, although this not scientifically proven, people by virtue of their culture will not take baths because they believe that this could lead to sickness.

Heredity
Of course heredity also affects health status of individuals.
Heredity is the genetic transmission of traits from parents to offspring; genetically determined (Miller-Keane, 1987) Certain diseases are found to be genetically transmitted.
Environment
Environment as a factor in health is the sum total of all theconditions and elements that make up the surrounding and influence the development of an individual. (Miller -Keane, 1987)
Florence Nightingale was a pioneer who truly understood how the environment affected an individual’s health. When we discuss our health situation you will discover that most illness prevalent are truly preventable with proper environmental sanitation and hygiene

Socio-economic
Refers to the production activities, distribution and consumption of goods of an individual. Without the proper means to sustain a health lifestyle, this need becomes neglected. It is difficult to
choose between medications that must be bought today to address an illness and food that must be bought in order to survive another day.

Levels of Prevention
1. Primary level – health promotion
2. Secondary level – Preventive, PA, early detection & prompt treatment
3. Tertiary level - rehabilitation

HEALTH PROMOTION
"Health promotion is the process of enabling people to increase control over, and to improve, their health. To reach a state of complete physical, mental, and social well-being, an individual or group must be able to identify and to realize aspirations, to satisfy needs, and to change or cope with the environment. Health is, therefore, seen as a resource for everyday life, not the objective of living. Health is a positive concept emphasizing social and personal resources, as well as physical capacities. Therefore, health promotion is not just the responsibility of the health sector, but goes beyond healthy lifestyles to well-being.

OTTAWA CHARTER FOR HEALTH PROMOTION
"The fundamental conditions and resources for health are peace, shelter, education, food, income, a stable ecosystem, sustainable resources, social justice, and equity. Improvement in health requires a secure foundation in these basic prerequisites.

Mediate"The prerequisites and prospects for health cannot be ensured by the health sector alone. More importantly, health promotion demands coordinated action by all concerned: by governments, by health and other social and economic sectors, by nongovernmental and voluntary organizations, by local authorities, by industry, and by the media.

People in all walks of life are involved as individuals, families, and communities. Professional and social groups and health personnel have a major responsibility to mediate between differing interests in society for the pursuit of health."Health promotion strategies and programs should be adapted to the local needs and possibilities of individual countries and regions to take into account differing social, cultural, and economic systems.“
Health Promotion Action MeansThe Charter defines health promotion in terms of the following activities: building healthy public policy in the full range of administrative and legislative action; creating supportive environments via a socio ecological approach to health; strengthening community action and democratic planning processes; developing personal skills via education; and reorienting health services toward health promotion in addition to curative services.

Moving into the Future
Citing caring, holism, and ecology as central issues, the signatories to the Charter pledged to promote health in various ways, including: advocating a clear political commitment to health and equity in all sectors; counteracting trends and products that harm health; reorienting health services toward health promotion; recognizing health and its maintenance as a major social investment.

Call for International ActionThe Charter concludes with a statement calling on the World Health Organization and other international bodies to advocate the promotion of health.

ACTION AREAS OF OTTAWA CHARTER FOR HEALTH PROMOTION
Building healthy public policy Health promotion policy combines
diverse but complementary approaches, including legislation, fiscal measures, taxation and organisational change. Health promotion policy requires the identification of obstacles to the adoption of healthy public policies in non-health sectors and the development of ways to remove them.

Creating supportive environments
The protection of the natural and built environments and the conservation of natural resources must be addressed in any health promotion strategy. Work, leisure and living environments should be a source of health for people.

Strengthening community action
Community development draws on existing human and material resources to enhance self-help and social support, and to develop flexible systems for strengthening public participation in, and direction of, health matters. This requires full and continuous access to information and learning opportunities for health, as well as funding support
Developing personal skills
Through information and education skills - enabling people to learn (throughout life) to prepare themselves for all of its stages and to cope with chronic illness and injuries is essential. This has to be facilitated in school, home, work and community settings.
Reorienting health services toward health promotion
All health services of different health agencies regardless of their status of work should promote Health.

Theories / Models of Health Promotion
Pender’s TheoryIndividual
Characteristics & Experiences
Behaviour-specific Cognitions & Affect
Behavioural Outcome
Prior related
Behaviour
Personal Factors;
Biological; Psychologic
al socio-cultural
Perceived benefit of
actionPerceived barrier of
actionPerceived self
efficacy
Interpersonal influences (family, peers, providers) norms, support
models Situational influences; options,
demand,
Activity related affect
Immediate competing demand
(low control) & preference
sCommitment to a plan of actionHealth
promoting
behaviour
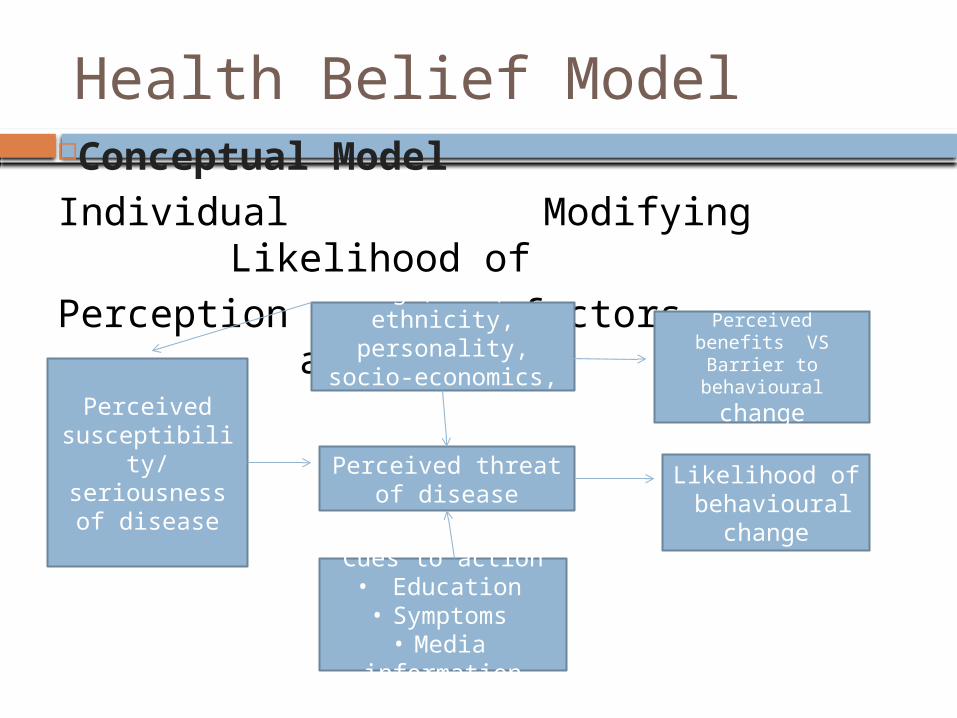
Health Belief ModelConceptual Model
Individual Modifying Likelihood of
Perception factors action
Perceived susceptibility/seriousness of
disease
Age, sex, ethnicity, personality, socio-
economics, knowledge
Perceived threat of disease
Cues to action• Education• Symptoms
•Media information
Perceived benefits VS
Barrier to behavioural
change
Likelihood of behavioural
change

Bandura Self Efficacy Self-efficacy is “the belief in one’s
capabilities to organize and execute the courses of action required to manage prospective situations”.
Self-efficacy is a person’s belief in his or her ability to succeed in a particular situation. Bandura described these beliefs as determinants of how people think, behave, and feel.
Role of Self EfficacyThe Role of Self-Efficacy Virtually all people can identify goals they want to accomplish,
things they would like to change, and things they would like to achieve. However, most people also realize that putting these plans into action is not quite so simple. Bandura and others have found that an individual’s self-efficacy plays a major role in how goals, tasks, and challenges are approached.
People with a strong sense of self-efficacy: View challenging problems as tasks to be mastered. Develop deeper interest in the activities in which they participate. Form a stronger sense of commitment to their interests and activities. Recover quickly from setbacks and disappointments.People with a weak sense of self-efficacy: Avoid challenging tasks. Believe that difficult tasks and situations are beyond their
capabilities. Focus on personal failings and negative outcomes. Quickly lose confidence in personal abilities (Bandura, 1994).

Sources of Self-Efficacy1. Mastery Experiences
The most effective way of developing a strong sense of efficacy is through mastery experiences," Bandura explained (1994). Performing a task successfully strengthens our sense of self-efficacy. However, failing to adequately deal with a task or challenge can undermine and weaken self-efficacy.
2. Social ModelingWitnessing other people successfully completing a task is another important source of self-efficacy. According to Bandura, “Seeing people similar to oneself succeed by sustained effort raises observers' beliefs that they too possess the capabilities master comparable activities to succeed” (1994).
3. Social PersuasionBandura also asserted that people could be persuaded to belief that they have the skills and capabilities to succeed. Consider a time when someone said something positive and encouraging that helped you achieve a goal. Getting verbal encouragement from others helps people overcome self-doubt and instead focus on giving their best effort to the task at hand.
4. Psychological ResponsesOur own responses and emotional reactions to situations also play an important role in self-efficacy. Moods, emotional states, physical reactions, and stress levels can all impact how a person feels about their personal abilities in a particular situation. A person who becomes extremely nervous before speaking in public may develop a weak sense of self-efficacy in these situations. However, Bandura also notes "it is not the sheer intensity of emotional and physical reactions that is important but rather how they are perceived and interpreted" (1994). By learning how to minimize stress and elevate mood when facing difficult or challenging tasks, people can improve their sense of self-efficacy.
Quiz
What are the component of political factor in health? (1-4) What is this health factors that determine the sum total of
all the condition& elements that makes up the surroundings? (5)
It an art & science of preventing disease, prolonging life and promoting health.(6)
Identify what level of preventions are the following activities. (7-16)
a. Biopsy d. scrotal examb. Diabetes awareness e. tooth brushing drillc. Application of braces for scoliosis

f. Immunizationg. Toilet constructionh. Proper Hand washing techniquei. Removal of tumor in abdomenj. Physical therapy

Define Health. Define nursing according to ADPCN.
Define community. Define community health nursing.
DOH ROLES & FUNCTIONS
1. LEADERS IN HEALTH 2. ENABLE AND CAPACITY BUILDER 3. ADMINISTRATOR OF SPECIFIC
SERVICES

III Phil. Health Care Delivery System
DOH Mission Guarantee equitable,
sustainable and quality health for all Filipinos, especially the poor, and to lead the quest for excellence in health.
VISSION The Leader of Health for All in the Philippines.

HSRA GOAL
SUPPORT MECHANISM WILL BE THROUGH SOUND ORGANIZATIONAL DEVELOPMENT, STRONG POLICIES SYSTEM AND PROCEDURE CAPABLE HUMAN RSOURCES AND ADEQUATE FINANCIA RESOURCES
Fourmula one for Health
Better health outcome More responsive health system Equitable health care financing ELEMENTS Health financing Health regulation Health service delivery Good governnce

Primary Health Care
Primary Health Care: as a philosophical approach to health and health care
This approach is characterised by an holistic understanding of health as wellbeing, rather than the absence of disease. The presence of good health is dependent upon multiple determinants; health services are important but so too are housing, education, public works, industry, agriculture, communication and other services. The health status of communities is both a function of and a reflection of development in those communities. The locus of control is important in PHC; health services should reflect local needs and involve communities and individuals at all levels of planning and provision of services. Services and technology should be affordable and acceptable to communities. Through health promotion and preventive care, PHC aims to eliminate causes of ill health. Equity is a crucial part of PHC; health services must strive to address inequity and prioritise services to the most needy. Finally, PHC should be based upon social, biomedical and health services research in order to provide effective health care.
PHC History
Alma Ata international conference on PHC in Sept. 12, 1978, the WHO and UNICEF proposed new concept of PHC. This conference proved to be a turning point in the history of health care policy. Backed by the fundamental tenet that health is a basic human right for which disparities or inequalities should not allowed, it culminated with a call for citizen led activities at the regional level in public hygiene, health education, MCHC, FP. Accepting that challenge, in 1981 the 34th WHO General conference drew up a set of global targets aimed at improving health for all by the year 2000.
PHC Philosophy
holistic understanding of health recognition of multiple determinants of
health community control over health services health promotion and disease prevention equity in health care research-based methods accessible, acceptable, available,
affordable technology

PHC Strategies
needs-based planning decentralised management education Inter-sectoral coordination and
cooperation balance between health promotion,
prevention and treatment multi-disciplinary health workers
PHC Services
locally based affordable and accessible , available,
acceptable well integrated health care teams health promotion disease prevention illness treatment rehabilitation services
PHC Elements/ Components
E-Education for Health L- Local Endemic Disease Control E- Expanded Program on Immunization M- Maternal & Child Care E- Essential Drugs N- Nutrition T- Treatment of communicable diseases S- Safe Water and Sanitation

Rationale for PHC
Many people die w/o seeing by the health care provider.
Communicable disease are still dominant cause of illness and death among all age group
Rapid population growth rate. Poor environmental sanitation. Lack of basic health knowledge Thousands allied professionals were registered but
prefer to work in secondary or tertiary level High cost of medical services now a days. Budgetary allocation for health care institution are
not enough to sustain the health of the population

DOH PROGRAMS
MATERNAL AND CHILD HEALTH Maternal care: 1. Ante- natal care – registration, visits 2. tetanus toxoid immunization 3. micronutrient supplementation 4. tx of other diseases and conditions 5. clean and safe delivery- use of partograph 6. Post partum care 7. family planning program

CHILD CARE
Infant and child feeding Newborn screening EPI Management of childhood illnesses Micronutrient supplementation Dental health Early child development Child health injuries
HEALTH SERVICES FOR NEWBORN, INFANT AND CHILD
Newborn resuscitation Newborn routine eye prophylaxis Prevention & mgt of hypothermia of
newborn Immediate & exclusive BF Complimentary feeding at six mos. Birth registration Birth weight & monitoring Full immunization

HEALTH SERVICES FOR NEWBORN, INFANT AND CHILD
Micronutrient supplementation Dental care Developmental milestone screening Advice on psychosocial stimulation Growth monitoring and promotion Nutritional screening Disability detection IMCI First aid
REPRODUCTIVE HEALTHELEMENTS:
FP MCH &Nutrition Prevention & mgt of RTI, STI & HIV/AIDS Prevention & mgt of abortion & its complication Prevention & mgt of breast & repro CA other
gynecological conditions Education & counselling on sexuality & sexual
health, men’s reproductive health & involvement Violence against women & children Prevention & mgt of infertility & sexual
dysfunction

Herbal Medicines
Akapulko (Cassia alata) a medicinal plant called "ringworm bush or schrub" and "acapulco" in English, this Philippine herbal medicine is used to treat tinea infections, insect bites, ringworms, eczema, scabies and itchiness.
Ampalaya (Momordica charantia) Common names include "bitter melon " or "bitter gourd " in English. This Philippine herbal medicine has been found to be effective in the treatment of diabetes (diabetes mellitus), hemofrhoids, coughs, burns and scalds, and being studied for anti-cancer properties.
Bawang (Allium sativum) Common name in english is "Garlic". Bawang is a used in Philippine herbal medicine to treat infection with antibacterial, antiinflammatory, anti-cancer and anti-hypertensive properties. It is widely used to reduce cholesterol level in blood.
Bayabas (Psidium guajava) - "Guava" in English. A Philippine herbal medicine used as antiseptic, anti-inflammatory, anti-spasmodic, antioxidant hepatoprotective, anti-allergy, antimicrobial, anti-plasmodial, anti-cough, antidiabetic, and antigenotoxic in folkloric medicine.
Lagundi (Vitex negundo) - known as "5-leaved chaste tree" in english is used in Philippine herbal medicine to treat cough, colds and fever. It is also used as a relief for asthma & pharyngitis, rheumatism, dyspepsia, boils, and diarrhea.

Niyog-niyogan (Quisqualis indica L.) - is a vine known as "Chinese honey suckle". This Philippine herbal medicine is used to eliminate intestinal parasites.
Sambong (Blumea balsamifera)- English name: "Ngai camphor or Blumea camphor" is a Philippine herbal medicine used to treatkidney stones, wounds and cuts, rheumatism, anti-diarrhea, anti spasms, colds and coughs and hypertension
Tsaang Gubat (Ehretia microphylla Lam.) - English :"Wild tea" is a Philippine herbal medicine taken as tea to treat skin allergies including eczema, scabies and itchiness wounds in child birth
Ulasimang Bato | Pansit-Pansitan(Peperomia pellucida) is a Phillipine herbal medicine known for its effectivity in treating arthritis and gout.
Yerba Buena (Clinopodium douglasii) - commonly known as Peppermint, is used in Philippine herbal medicine as analgesic to relive body aches and pain due to rheumatism and gout. It is also used to treat coughs, colds and insect bites

Health related laws in the Phil. Republic Act 349 – Legalizes the use of
human organs for surgical, medical and scientific purposes
Republic Act 1080 – Civil Service Eligibility
Republic Act 1082 – Rural Health Unit Act
Republic Act 1136 – Act recognizing the Division of Tuberculosis inthe DOH
Republic Act 1891 – Act strengthening Health and Dental services in the rural areas.
Republic Act 2382 – Philippine Medical Act which regulates the practice of medicines in the Philippines
Republic Act 3573 – Law on reporting of Communicable Diseases Republic Act 4073 – Liberalized
treatment of Leprosy Republic Act 6425 – Dangerous Drug Act
of 1992

Republic Act 6675 – Generics Act of 1988 Republic Act 7160 – Local Government
Code Republic Act 7170 – Law that govern organ
donation Republic Act 7277 – Magna Carta of
Disabled Persons Republic Act 7305 – The Magna Carta of
public Health Workers Republic Act 7432 – Senior Citizen Act

Republic Act 7600 – Rooming In and Breastfeeding Act of 1992
Republic Act 7719 – National Blood Service Act of 1994
Republic Act 7883 – Barangay Health workers Benefits and Incentives Act
Republic Act 8172 – Asin Law Republic Act 8423 – Philippine Institute
of Traditional and Alternative Medicine

Republic Act 8749 – The Philippine Clean Air Act of 1999
Republic Act 9165 – Comprehensive Dangerous Drugs Act 2002
Republic Act 9173 – Philippine Nursing Act of 2002
Republic Act 9288 – Newborn Screening Act Presidential Decree 147 – Declares April & May as National Immunization
Day
Presidential Decree 491 – Nutrition Program Presidential Decree 996 – Provides for
compulsory basic immunization for children and infants below 8 years of age
Presidential Decree 856 – Code of Sanitation Executive Order 51 – The Milk Code Administrative Order 114 – Revised/updated
the roles and functions of theMunicipal Health Officers, Public Health Nurses andRural Midwives
Community Organization
A process, mechanism or means of attaining goal of community development
Deals with problem solving Begins as a response to the need or
problems Seek a social change Bringing people together who have similar
needs or interest In small task oriented-groups with certain
defined objectives and activities

co
In complex form, it requires bringing together various sectors of the population, relevant government and non-government agencies and institution

Community Organizing
A continuous and sustained process of:
Guiding people to understand the existing condition of their own community
Organizing people to work collectively and efficiently on their immediate and long term problems
Community Organizing
Mobilizing people Develop their capacity Readiness to respond Take action on their immediate and
l longterm needsCOPAR- Community organizing
participatory action research A social development approach that aims to
transform the apathetic, individualistic and voiceless poor into dynamic participatory & politically responsive community.
COPAR A collective, participatory,
transformative, liberalative, sustained and systematic process of building peoples organization by mobilizing & enhancing the capabilities & resources of the people for the resolution of their issues & concerns toward effective change in their existing oppressive & exploitative condition
(1994 National Rural CO Conference).

IMPORTANCE OF COPAR Tool for the community development &
people empowerment as this helps the community workers to generate community participation in development activities.
Prepares people to eventually take over the management of development program in the future.
Maximizes community participation and involvement: Community resources are mobilized for health development services.

PRINCIPLES OF COPAR People, especially the most oppressed,
exploited & deprive sectors are open to change, have the capacity to change & are able to bring about change.
COPAR, should based on the interest of the poorest sectors of the society.
COPAR, should lead to self reliant community and society.

METHOD USED IN COPAR A progressive cycle action- reflection action, w/c
begin with small, local & concrete issues, identified by the people & the evaluation and reflection of and on the action taken by them.
Consciousness-raising, through experiential learning is central to the COPAR process because it place emphasis on learning that emerges from concrete action & w/c encircle succeeding action.
COPAR is participatory and massed-based, because it is primarily directed towards & based in favor of the poor, the powerless & the oppressed.
COPAR is grouped centered & not leader certered. Leaders are identified emerge & are tested through action rather than appointed or selected external force
Process/Phases of COPAR Pre-entry phase – conduct of preliminary social
analysis of the community is needed to be able to plan the most effective way of entering the community
Preparation of staff Do you like working for the people? Do you believe on people’s capacity to change? Do you believe that people have the potentials to
contribute to their own development? Do you believe that people should be empowered to
make decision on matters affecting them? Will you support people’s decision? Are you committed to serving people’s interest?

Pre-entry
Site collection – steps Developing the criteria for site collection Identifying potential municipality/
catchment area Identifying potential barangay Choosing the final project village/
barangay Identification of the host family

Process/ Phases of COPAR
Entry phase- immersion phase Community integration Participating in community activities Conversing with people in places where
they usually converge Conducting house to house visit or social
calls Social investigation Collecting Synthesizing Collating Analyzing data

Process / Phases of COPAR Core group formation- the core group
will be a training ground for developing leaders in:
Democratic & collective leadership Planning & assuming task for formation
of a community wide organization Handling & resolving group conflicts Critical thinking & decision making
process

Task of core group
Integration with the core group members
Deeper social investigation
Training and education
Mobilizing the core group

Process / Phases of COPAR
Organization – Building Phase – it signaled the start of the community management of any development program. The ultimate aim was to form a structure or organization that would coordinate & become responsible for community wide health & development activities

Organization-Building phase Activities pre-organization building activities Listing of speakers, task of core group Possible issues that may arise & how to
respond them Organizing & setting the committee Legal & technical recruitment By laws, registration Training & education of the organization Income generating project. Mobilization of the health organization

Process / Phases of COPAR
Consolidation & Expansion phase or sustenance & Strengthening phase it is a process molding the community
organization into cohesive unit & strengthening the leadership group & uniting the membership.
Consolidation & Expansion phase
Strategies : education & training Networking & linkaging Conduct of mobilization of livelihood &
related development Development of secondary leaders Evaluation

Family
Basic unit of the society Types : Conjugal (nuclear) familyThe term "nuclear family" is commonly used, to
refer to conjugal families. A "conjugal" family includes only the husband, the wife, and unmarried children who are not of age. Sociologists distinguish between conjugal families (relatively independent of the kindred of the parents and of other families in general) and nuclear families (which maintain relatively close ties with their kindred).
Matrifocal family (solo or single parent)
A "matrifocal" family consists of a mother and her children. Generally, these children are her biological offspring, although adoption of children is a practice in nearly every society. This kind of family is common where women have the resources to rear their children by themselves, or where men are more mobile than women.
Extended family The term "extended family. This term has two
distinct meanings. First, it serves as a synonym of "consanguinal family" (consanguine means "of the same blood"). Second, in societies dominated by the conjugal family, it refers to "kindred" who do not belong to the conjugal family. These types refer to ideal or normative structures found in particular societies. Any society will exhibit some variation in the actual composition and conception of families.

Blended family Male same-sex couple with a child The term blended family or stepfamily describes
families with mixed parents: one or both parents remarried, bringing children of the former family into the new family. traditional family refers to "a middleclass family with a bread-winning father and a stay-at-home mother, married to each other and raising their biological children," and non traditional to exceptions from this rule.
Principles of family nursing care plan
The nursing care plan focuses on actions which are designed to solve or minimize existing problem. The plan is a blueprint for action. The core of the plan are the approaches, strategies, activities, methods and materials which the nurse hopes will improve the problem situation.
The nursing care plan is a product of a deliberate systematic process. the planning process is characterized by logical analyses of data that are put together to arrive at rational decisions. The interventions the nurse decides to implement are chosen from among alternatives after careful analysis and weighing of available options.
The nursing care plan, as with all plans, relates to the future. It utilizes events in the past and what is happening in the present to determine patterns. It also projects the future scenario if the current situation is not corrected.

Principles of FNCP
The nursing care plan is based upon identified health and nursing problems. The problems are the starting points for the plan, and the foci of the objectives of care and intervention measures.
The nursing care plan is a means to an end, not an end in itself. The goal in planning is to deliver the most appropriate care to the client by eliminating barriers to family health development.
Nursing care planning is a continuous process, not a one-shot-deal. The results of the evaluation of the plan’s effectiveness trigger another cycle of the planning process until the health and nursing problems are eliminated.

FAMILY ASSESSMENT
A good family assessment requires astute observation skills and the ability to be an active listener. Assessment data can be obtained anytime health care professionals interact with patients and families. Gathering information about family structure, function, and needs does not have to be restricted to structured interviews. Anytime the family is present; you can obtain more information about the family and their role in the patient’s health care management. Informal conversations with the patient and family while you are passing medications, adjusting an intravenous rate, or giving a tube feeding can yield data that will help you complete the family picture.

Areas of Family Assessment
What is the family like? Who is considered part of the family? What is the patient’s position and role in the
family? Who has most influence on the patient? What are the ages and sex of the family
members? What are their occupations? What is the health status of family members? Are there physical limitations that would affect a
family member’s ability to help with care needs?

Areas of Family assessment
What resources are available to the family? Can the family provide for the patient’s physical
needs? What is the patient’s home like? Does it provide
sufficient safety and comfort features? What is the patient’s ability to perform self-care? What are the health insurance resources? What neihgborhood or community resources are
available? What connections does the family have with friends,
neighbors, church, community organizations?

Areas of Family Assessment
What are the family’s educational background, lifestyle, and beliefs?
What is the level of education of the family members and their attitudes toward learning?
Do all family members have basic literacy skills? Are there language barriers to verbal communication? What is the family’s lifestyle and cultural background? Does the family have any folk medicine beliefs? Are there potential conflicts between cultural beliefs and the
recommendations of health professionals? What are the family’s normal dietary patterns? Does the family seem to be able to take in new information easily
and apply what was taught? Does the family seem overwhelmed as a result of the need to learn
new skills?
Areas of Family Assessment
What is the family’s understanding of the current health care problem?
What do they think has caused the health care problem? Why do they think the problem occurred now? What do they think the illness does to the patient? How severe do they believe the illness is? What kind of treatment do they think the patient should
receive? What are the most important results they think the patient
should obtain from the treatment? What are the major problems the illness has caused for the
family? What do they fear most about the situation?
Areas of Family Assessment
How does the family seem to function? Do family members seem to be sensitive to the patient and to
each other? Do family members appear to be able to communicate
effectively with each other? Does the family indicate that they have the ability to accept
help from others when it is needed? How open does the family seem to teaching? Do key family members have the ability to make effective
decisions? What experience does the family have in handling crisis
situations? How did the family react to crises in the past and what
resources did they use to help them?

Areas of Family Assessment
What is the family’s understanding of the current health care problem?
What do they think has caused the health care problem? Why do they think the problem occurred now? What do they think the illness does to the patient? How severe do they believe the illness is? What kind of treatment do they think the patient should
receive? What are the most important results they think the patient
should obtain from the treatment? What are the major problems the illness has caused for the
family? What do they fear most about the situation?

Areas of Family Assessment
What are the patient and family’s teaching needs? What do the patient and family think are the most
important things they need to know? Do the patient and family know others with the same
health care problem? Do the patient and family understand and agree with the
treatment plan? Are there any physical or cognitive limitations that will be
barriers to learning? Are the patient and family willing to negotiate goals with
the health care team? Are the patient’s perceptions about what to do similar to
the family’s point of view?

Assessment Initial data base (IDB)
A. Family structureB. Socio-economic & cultural characteristicC. Home & environmentD. Health status of family members of the
familyE. Values habit, practices on health
promotion, maintenance of disease prevention

2. Data analysis
Sort data Cluster/ group related data Identify pattern (e.g. Function,
Behaviour, lifestyle) Compare pattern w/ norm/ standard Interpret result Make inferences/ draw conclusion

3. Health conditions/problems and family nursing diagnosis
1st level define health conditions/problems A. wellness state B. health deficit C. health threats D. foreseeable crisis 2nd level- define the family nursing problems
diagnosis as: family’s inability to perform health task on each health condition/problems specifying the barrier to performance or reason for non performance of family health task

Developing a Family Nursing Care Plan
Component: 1. Prioritization of conditions/ problems knowledge , technology, &
intervention to enhance wellness Resources of family, nurse community 2. Goals and objective of nursing care 3. Plan of intervention 4. Plan for evaluating care

Community Health Nursing Process Assessment of community health needsComponents: a. health status b. health resources c. health action potentials Community diagnosis (community dx ppt) Community Planning (principles) Intervention- action, strategies, activities to
be done as solution to the problems identified Evaluation
Elements of community planning process
Needs assessment: identifying the needs and assets of the community or neighborhood and the particular health concerns and disparities,
Strategic planning: clarifying vision, goal, and directives, establishing decision making processes and criteria, fostering sustainability, and ensuring that resources are being appropriately used.
Building understanding about multiple determinants of health : raising awareness about what contributes to good health and fostering buy-in into a preventive approach to improving health and safety outcomes
Partnership and coalition building: determining and engaging the support of key stakeholders and decision makers, including community engagement
Prioritization: selecting the appropriate factors and combination of factors
Comprehensive approaches: implementing multifaceted activities to achieve desired outcomes
Evaluation: ongoing assessment and evaluation of community efforts
VITAL STATISTICS
Population natural increase:Formula: Number of births – Number of deaths
Rate of natural increase= CBR – CDR
Absolute increase per year= Pt –Po tPt= population size at a later yearPo= population size at earlier timet = number of years between time o and time t
Population Increase
Relative increase= Pt_- Po_ PoPopulation Composition:Sex Ratio= Number of males X Number of femalesFertility rates: CBR= number of live births X
1000 Midyear population
Vital Statistics
General fertility rates = number of live births X 1000 Midyear population of women 15-44
yrsCDR = Number of deaths X 1000 Midyear populationIMR=number of deaths < 1yr X1000 Number of live births

Epidemiology
The study of the distribution of diseases in populations and of factors that influence the occurrence of disease. Epidemiology examines epidemic (excess) and endemic (always present) diseases; it is based on the observation that most diseases do not occur randomly, but are related to environmental and personal characteristics that vary by place, time, and subgroup of the population. The epidemiologist attempts to determine
who is prone to a particular disease; where risk of the disease is highest;
when the disease is most likely to occur and its trends over time; what exposure its victims have in common;
how much the risk is increased through exposure; and how many cases of the disease could be avoided by eliminating
the exposure

n the course of history, the epidemiologic approach has helped to explain the transmission of communicable diseases, such as cholera and measles, by discovering what exposures or host factors were shared by individuals who became sick. Modern epidemiologists have contributed to an understanding of factors that influence the risk of chronic diseases, particularly cardiovascular diseases and cancer, which account for most deaths in developed countries today. Epidemiology has established the causal association of cigarette smoking with heart disease; shown that acquired immune deficiency syndrome (AIDS) is associated with certain sexual practices; linked menopausal estrogen use to increased risk of endometrial cancer but to decreased risk of osteoporosis; and demonstrated the value of mammography in reducing breast cancer mortality. By identifying personal characteristics and environmental exposures that increase the risk of disease, epidemiologists provide crucial input to risk assessments and contribute to the formulation of public health policy.

Descriptive Epidemiology
Descriptive epidemiologic studies provide information about the occurrence of disease in a population or its subgroups and trends in the frequency of disease over time. Data sources include death certificates, special disease registries, surveys, and population censuses; the most common measures of disease occurrence are (1) mortality (number of deaths yearly per 1000 of population at risk); (2) incidence (number of new cases yearly per 100,000 of population at risk); and (3) prevalence (number of existing cases at a given time per 100 of population at risk). Descriptive measures are useful for identifying populations and subgroups at high and low risk of disease and for monitoring time trends for specific diseases. They provide the leads for analytic studies designed to investigate factors responsible for such disease profiles.

Analytic Epidemiology
Analytic epidemiologic studies seek to identify specific factors that increase or decrease the risk of disease and to quantify the associated risk. In observational studies, the researcher does not alter the behavior or exposure of the study subjects, but observes them to learn whether those exposed to different factors differ in disease rates. Alternatively, the researcher attempts to learn what factors distinguish people who have developed a particular disease from those who have not. In experimental studies, the investigator alters the behavior, exposure, or treatment of people to determine the impact of the intervention on the disease. Usually two groups are studied, one that experiences the intervention (the experimental group) and one that does not (the control group). Outcome measures include incidence, mortality, and survival rates in both the intervention and control groups.
COMMUNITY
The people in a given geographical location, the word can really refer to any group sharing something in common. This may refer to smaller geographic areas -- a neighborhood, a housing project or development, a rural area -- or to a number of other possible communities within a larger, geographically-defined community.
TYPES OF COMMUNITY
Geographic communities share physical space, so that residents come into contact with each other by virtue of proximity, rather than intent. However, to be a "real" community, residents must feel a sense of belonging and hold at least some values and symbols in common.
Communities of interest are sometimes referred to as "communities within communities".
Virtual communities are groups of people that primarily interact via communication media rather than face to face.[3] If the mechanism is a computer network, it is called an online community.

TYPES OF COMMUNITY
Interest. Communities of people who share the same interest or passion.
Action. Communities of people trying to bring about change.
Place. Communities of people brought together by geographic boundaries.
Practice. Communities of people in the same profession or undertake the same activities.
Circumstance. Communities of people brought together by external events/situations.

CHARACTERISTICS OF COMMUNITY
Has one or more roles that define its identity within society.
Has a set of goals - provides a sense of direction.
Is organised within a set of formal/informal beliefs, values, expectations and behaviours that defines the boundary of the community.
The boundary may be explicit (physical) or implicit (defined by the
shared characteristics of its members).
Has ownership of it's members.
There is some form of communication between members.

CHARACTERISTICS OF A COMMUNITY
Has skills and resources that are shared between the members.
Balance the needs of the community with the needs of its members.
Often has clubs, teams, groups etc. within the community.

COMPONENT OF A COMMUNITY
CORE- PEOPLE HOUSING ENVIRONMENTAL SERVICES FIRE AND SAFETY PEACE & ORDER HEALTH SERVICES EDUCATION SOCIAL SERVICES ECONOMICS- BUSINESSES, RECREATION COMMUNICATION POLITICS- LEADERSHIP

ELEMENTS OF HEALTHY COMMUNITY
A healthy community: Meets the basic needs of its residents. Promotes health and wellness. Creates quality education and learning opportunities for all ages. Ensures a vibrant and diversified economy. Provides broad access to arts and culture. Fosters strong and connected neighborhoods
and communities. Protects and stewards its natural environment.
FACTORS AFFECTS HEALTH
Income and social status - higher income and social status are linked to better health. The greater the gap between the richest and poorest people, the greater the differences in health.
Education – low education levels are linked with poor health, more stress and lower self-confidence.
Physical environment – safe water and clean air, healthy workplaces, safe houses, communities and roads all contribute to good health. Employment and working conditions – people in employment are healthier, particularly those who have more control over their working conditions

FACTORS AFFECTS HEALTH
Social support networks – greater support from families, friends and communities is linked to better health. Culture - customs and traditions, and the beliefs of the family and community all affect health.
Genetics - inheritance plays a part in determining lifespan, healthiness and the likelihood of developing certain illnesses. Personal behaviour and coping skills – balanced eating, keeping active, smoking, drinking, and how we deal with life’s stresses and challenges all affect health.
Health services - access and use of services that prevent and treat disease influences health
Gender - Men and women suffer from different types of diseases at different ages.

COMMUNITY DEVELOPMENT
A group of people in a community reaching a �decision to initiate a social action process (that is, planned
intervention) to change their economic, social, cultural, or environmental situation.
Christenson and Robinson, 1978 Collective » Agency
Collective agency -believe working together can make a difference -organize to address their shared needs
collectively

Key Qualities of Community Dev.
It is always purposive � Its purpose is always positive � It exists in the efforts of people and �
not necessarily in goal achievement.
Trying is enough to qualify as community
development It is structure-oriented�

Reason For Community Dev.
Expand participation� Reaction against some proposed change �
in the local area that is deemed as having negative consequences on residents’ quality of life
Modify severe social, economic or �environmental problems in the community
Satisfy missing needs or resources�

3 APPROACHES TO CD
� Technical Assistance
Conflict Approach �
Self-Help Approach�
Technical Assistance Characteristics
If residents wish to participate, they �must study and understand a great deal of complex information
Local citizens are defined as �consumers of such development - not participants in it
The most frequent employers of the �technical assistance model is government
Technical Assistance Characteristics
Usually involves the delivery of programs of services to a local area by some agency or organization It is often a “top-down” approach that �
involves the use of experts The focus is mainly on the task to be � performed Assumes that answers to community � problems can be arrived at scientifically

Problems w/ this Approach
Local community participation is �downplayed due to a greater interest in realizing efficiency rather than access on the part of citizens
Some question as to whose values are �influencing development decisions; often are guided by middle class values of the government officials and consultants
The assisting group does not always have �a full understanding of the community

CONFLICT APPROACH
Primary focus is upon the deliberate use �or creation of confrontation by professional organizers
The goal is to redistribute power A major � �organizing tool is to confront those forces seen as blocking efforts to solve problems
In this approach, there is a deep �suspicion of those who have formal community power
CONFLICT APPROACH
This perspective assumes that power is �never given away, that it has to be taken.
Goal is to build a people’s organization �to allow those without power to gain it through direct action. Their strength is in numbers -- people working collectively.

STEPS IN THE CONFLICT APPROACH
An outside organizer enters the �community, usually at the request of a local group wanting change. Outside person usually informs the local leaders, analyzes the power structure, and assesses what the major problems are
The organizer and the local allies seek �to build a people’s organization
STEPS IN THE CA
The coalition engages in direct action – traditional power structure is confronted through direct action involving a large number of people
• publicity or threat: press conferences, advertising, public hearing
• action: courts, lobbying, sit-ins, strikes, demonstrations • pressure: boycott of goods or facilities People’s organization is then formulized by � developing a permanent organizational structure (although not always)
CRITISISM OF THIS APPROACH
Maintenance of effort: once problem is solved, �hard to maintain commitment
Burn-out: key organizers and volunteer staff �often become burnt out after their initial organizational efforts
Loss of leaders: professional organizer often �leave after the issue has been addressed; leaders who remain get tempted to seek local or external positions in government/corporations
Finance: hard to keep a reliable source of funds �available to support the group’s work

SELF-HELP APPROACH
Emphasis is on process -- people within �the community working together to arrive at group decisions and taking actions to improve their community
Based on the principle that people can �collaborate in a community to provide important needs and services
The process is more important than any �particular task or goal

IN THE SELF-HELP APPROACH
Want to institutionalize a process of change based on building community institutions and strengthening community relationships, rather than to achieve any particular objective
Key Features of the Self-Help Approach
Project is community controlled� Local needs are clearly defined and action is �
initiated by the community Effective leadership and skills are present; �
effective use of volunteers Good efforts to secure financial resources� Significant cooperation and integration of �
people and organizations in the effort Access to outside support, as needed� Self-sustaining enterprises that can spur other �
community improvement efforts

Factors in Effective Change
Linkages� – Vertical • Limited by cutbacks – Horizontal • “Lateral Learning” Planning� – Each approach views planning
differently

Community vs. Economic Development
Community development is much broader than �economic development
Unlike CD, economic development does not �necessarily involve local citizen action, and it may not result in an improvement in the quality of life
If economic development is undertaken without �much community involvement, than there is no community development
Economic development for community �development has distinctive features that economic development alone might not have

Community vs. Economic Development
It seeks to increase the resources for �people to meet their needs
It encourages the development of jobs �services, facilities, and groups that are needed by the whole community
It seeks to reduce inequality It provides � �for and depends upon local community action and involvement
Examples of CD Efforts That Embody the Self-Help Approach
Strengthening and expanding the pool of �leaders at the local level
Facilitating job training and retraining �activities
Enhancing the capacity of local �government officials
Providing needed information to help �facilitate sound decision making (such as needs assessment, surveys, socioeconomic data)
Examples of CD Efforts Using Self-Help Approach
Community Asset Mapping
Conflict Mediation�
Public Issues Education�