community health and advocacy training in pediatrics: using asset-based community development for...
TRANSCRIPT
P
Community Health and Advocacy Training in Pediatrics: Using Asset-BasedCommunity Development for Sustainability
Su-Ting T. Li, MD, MPH1, Elizabeth M. Sterba, MS2, Elizabeth Miller, MD, PhD3, Richard J. Pan, MD, MPH4,
Albina Gogo, MD1, and Anthony F. Philipps, MD1
From the 1Department of Pediatrics and 2Office of the Vice Chancellor and Dean,University of California Davis; 3Department of Pediatrics, Children’s Hospital ofPittsburgh, University of Pittsburgh School of Medicine, Pittsburgh, PA; and
ediatricians play a critical role in promoting the health ofall children,1-4 andcommunityhealthandchildadvocacyexperiences are now a required component of pediatric
residency training.5 Since the 1999 initiation of the UniversityofCaliforniaDavis pediatric residency program’sCommunitiesand Health Professionals Together (CHPT) partnership,6-8 theCHPT’s scope has expanded to include training of residentsfrom the Departments of Family and Community Medicineand Internal Medicine, as well as students from the Schools ofNursing, Medicine, and Public Health.
Previously, CHPT was a 2-week annual experience,focused in a single community and culminating in a pro-ject.6-8 We worked collaboratively with our communitypartners to make a major curricular change based onprogram evaluations from pediatric residents andcommunity faculty. CHPT is now a 4-week, topic-based ex-perience for first-year residents, with those who elect todevelop an advocacy project receiving additional 4-week ex-periences in the second and third years (Table; available atwww.jpeds.com). Community and academic faculty devel-oped an exhaustive list of potential topics from which com-munity faculty identified their ‘‘expert’’ topic and thenworked with academic faculty to plan didactics, readings,educational activities, and reflective exercises. Here we sharelessons learned from CHPT for the sustainability of a robustcommunity health and advocacy training program applyingasset-based community development (ABCD), a strengths-based approach to building strong communities by identi-fying and mobilizing local assets.9
Identifying Local Community andInstitutional Assets
Community faculty play a vital role in teaching health profes-sionals how to engage and build partnerships with communi-ties by conveying the cultural contexts, local challenges, andcommunity assets present in the neighborhood. Ongoingidentification and recruitment of community partners is es-sential. Our community faculty includes neighborhoodleaders (eg, leader of a grassroots community-based serviceand advocacy group), local service providers (eg, physicianassistant andmidwife who founded a rural health center), ed-
ABCD Asset-based community development
CHPT Communities and Health Professionals Together
ucators (eg, school district administrator), and nonprofit or-ganization administrators. Institutional assets include anacademic faculty with interest and experience in communitypartnerships, advocacy, and community-based participatoryresearch, both within and outside our department, and edu-cational program leadership who value community and childadvocacy and provide learners dedicated time to build suc-cessful partnerships with local groups.
Nurturing Community InstitutionalPartnerships: Bridging the Cultural DivideUsing theProgramManagerasCulturalBroker
In ABCD, different community assets bring different strengthsto the partnership; however, sustaining partnerships betweenthe university and community organizations requires bridgingthe cultural differences. The role of the CHPT’s ProgramMan-ager (E.S.) is tobridge these cultural gaps to cultivate andmain-taincommunityrelationships.TheProgramManagerwashiredfromwithinthecommunityandbringsexperienceandcredibil-ity with community partners when explaining differing per-spectives and promoting collaborative problem solving toreach mutually beneficial outcomes. For example, when resi-dents accustomed to a hierarchical medical system were frus-trated with how long it was taking to make decisions onprojects and were unclear on the roles of community partners,the ProgramManager explained that, in the community, deci-sions are often made collaboratively by group consensus, andthere often is no designated leader.When community partnerswere concerned that residents were having difficulty meetingoutside of their CHPT rotation, the Program Manager insti-tuted ‘‘shadowdays,’’ duringwhich community partners couldshadowresidents tobetterunderstandtheir schedulesaddition-ally, the ProgramManager developed a CHPT dictionary thatexplains suchconcepts as ‘‘call’’ and ‘‘livingwage.’’ Communityfaculty cite the ProgramManager as key to efficacy and sustain-ability, prioritizing the ProgramManager position for resourcedevelopment rather than funding for their own roles.
4California Legislature, Sacramento, CA
Initially funded by the Dyson Foundation and Sierra Health Foundation. The authorsdeclare no conflicts of interest.
0022-3476/$ - see front matter. Copyright ª 2012 Mosby Inc.
All rights reserved. 10.1016/j.jpeds.2011.10.032
183

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. 160, No. 2
Building Capacity
Community PartnersCommunity faculty bring invaluable experience with commu-nity health issues. We build on their experience through theCHPT Academy, an annual series of workshops that providesthemwith a common venue and format to discuss communityhealth and advocacy with our residents. The CHPT Academyprovides community faculty and local partners an opportunityto discuss ABCD, social capital, determinants of health,patient-centered medical home, and program planning andevaluation. In addition, because teaching residents is oftena new experience for community faculty, we also discusshow to apply adult learning principles tomake residents’ com-munity experiences explicitly relevant to them.
Academic FacultyUntil recently, a single academic faculty member (R.P.) pri-marily ran our CHPT rotation at the university. But sustain-ing teaching in community health and advocacy requiresa village. We identified additional faculty, community andacademic pediatricians, and pediatric subspecialists whowere also involved with the community to speak to residentsat orientation about their experiences. This allowed us tohighlight to residents the importance of community pediat-rics to all pediatricians, introduce different role models,and recast faculty’s image of themselves to include commu-nity. We then identified academic faculty with expertise indifferent areas of community health and advocacy and incor-porated them into our required CHPT rotation to provideaccess to content experts, help residents reflect on their com-munity experiences and incorporate what they learned intobecoming better pediatricians.
Look Beyond PediatricsWe expanded on community health teaching efforts in otherdisciplines (Family and Community Medicine in 2006 andInternal Medicine in 2007) to develop collaboration acrossdifferent programs. By 2010, what was originally Communi-ties and Physicians Together became CHPT, with significantinput from community faculty to reflect the multiprofes-sional, interdisciplinary focus of community health and ad-vocacy education.
Developing Shared Vision by Documentingand Sharing Outcomes
CHPT builds on the broad expertise and assets in communityhealth and advocacy within the University of California DavisHealth System, the opportunities for collaboration withuniversity academic departments and outside academicprograms, and a range of partnerships with community collab-oratives and agencies inorder tobuild an educational, research,and innovative services program that supports the emergenceof healthy communities. CHPT offers learners at differentstages of development the opportunity to engage inmeaningfullearning and exchange with diverse community partners.
184
Harnessing institutional support also drew on the ABCDapproach, emphasizing assets and strengths within the healthcare system related to community health and advocacy andencouraging collaboration across disciplines and programs.We celebrate our successful joint projects and partnershipduring our annual symposium for community partners, res-idents, and faculty. Highlighting CHPT through awards, em-phasizing multiprofessional education, and coordinatingwith other residency programs beyond the institution in-creases institutional, multidepartmental support.We have highlighted CHPT accomplishments locally and
nationally with support from the Department Chair andDean’s Office for nominations for awards that demonstratethe health system’s longstanding history of community en-gagement, partnership building, and community health edu-cation. The 2009 Gold Country Champions for Changeaward (local), the 2005 Community Campus Partnershipsfor Health award (national), and the 2007 Ehrlich FacultyService Learning Award (national) are examples of awardsthat have allowed CHPT not only to increase its visibilityin our university, but also to be relevant to its mission.Since 2009, we have participated in a statewide collabora-
tive of residency programs engaged in teaching communitypediatrics and advocacy, the California Community Pediat-rics and Legislative Advocacy Training Collaborative. Partic-ipation in this collaborative has increased the visibility ofCHPT beyond University of California Davis and providednew opportunities to showcase community pediatrics toa wider audience, while underscoring the broad institutionalsupport for community pediatrics and advocacy educationacross several residency programs.Finally, institutional support can be sustained only if there
is ongoing ‘‘product,’’ whether through awards, communitybenefit, or publications. Specifically, CHPT has participatedin both process and outcomes evaluations over the past de-cade, publishing results in peer-reviewed journals.6-8
Discussion
ABCD builds on existing strengths in the community tosustainably address community challenges. We emphasizeto our trainees that the most successful projects involvepartnering with the community, building capacity, and de-veloping a project that can be sustained by the community,even after the resident has graduated. Similarly, the mostsuccessful community health and advocacy training pro-grams involve identifying and nurturing community andinstitutional partnerships; building capacity in communitypartners, faculty, and institution; and documenting andsharing outcomes to harness institutional support for asustainable program. n
Reprint requests: Su-Ting T. Li, MD, MPH, Department of Pediatrics,
University of California Davis, 2516 Stockton Blvd, Room 220, Sacramento,
CA 95817-2233. E-mail: [email protected]
References available at www.jpeds.com
Li et al
February 2012 NOTES FROM THE AMSPDC
References
1. AmericanAcademyofPediatrics,CommitteeonCommunityHealthServices.
The pediatrician’s role in community pediatrics. Pediatrics 1999;103:1304-7.
2. Rushton FE Jr. The pediatrician’s role in community pediatrics. Pediatrics
2005;115:1092-4.
3. American Academy of Pediatrics. Community pediatrics: health equity.
Available from: http://www.aap.org/commpeds/resources/health_equity.
html. Accessed November 22, 2011.
4. AmericanAcademyofPediatrics. Policy statement: thepediatrician’s role in
community pediatrics. Reaffirmed January 2010. Pediatrics 2010;125:e978.
5. Accreditation Council for Graduate Medical Education. ACGME pro-
gram requirements for graduate medical education in pediatrics, effective
July 1, 2007. Available from: http://wwwacgmeorg/acWebsite/downloads/
RRC_progReq/320_pediatrics_07012007pdf. Accessed January 27, 2011.
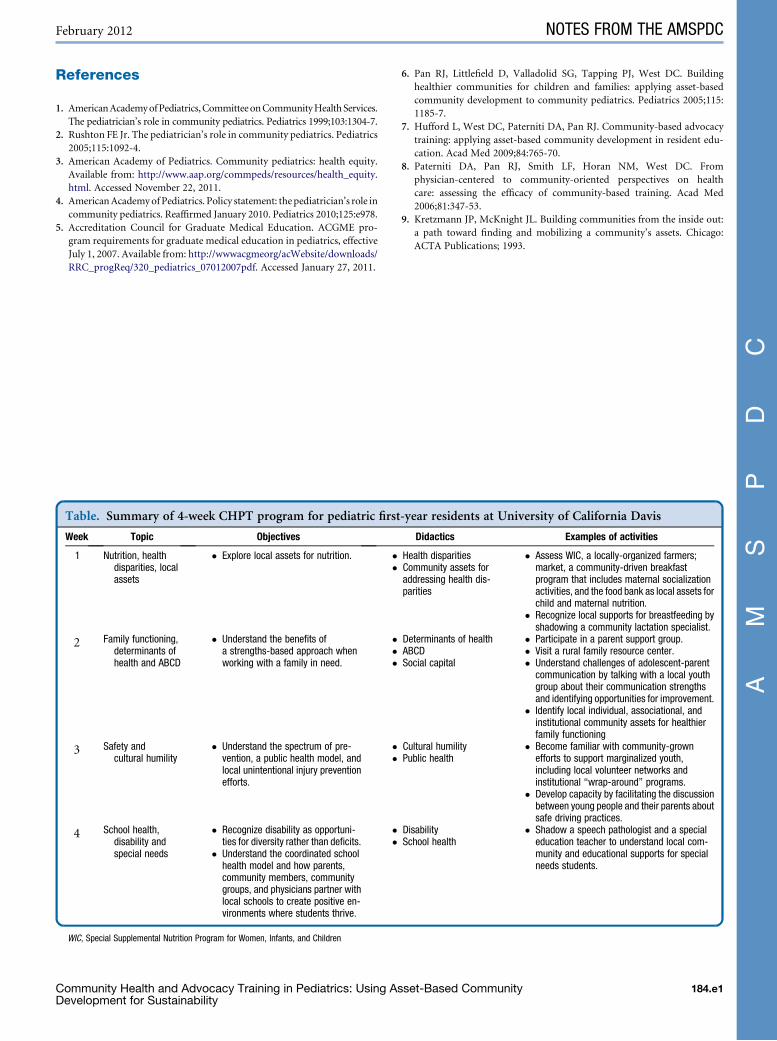
Table. Summary of 4-week CHPT program for pediatric first
Week Topic Objectives
1 Nutrition, healthdisparities, localassets
� Explore local assets for nutrition. ��
2 Family functioning,determinants ofhealth and ABCD
� Understand the benefits ofa strengths-based approach whenworking with a family in need.
���
3 Safety andcultural humility
� Understand the spectrum of pre-vention, a public health model, andlocal unintentional injury preventionefforts.
��
4 School health,disability andspecial needs
� Recognize disability as opportuni-ties for diversity rather than deficits.
� Understand the coordinated schoolhealth model and how parents,community members, communitygroups, and physicians partner withlocal schools to create positive en-vironments where students thrive.
��
WIC, Special Supplemental Nutrition Program for Women, Infants, and Children
Community Health and Advocacy Training in Pediatrics: Using AsDevelopment for Sustainability
6. Pan RJ, Littlefield D, Valladolid SG, Tapping PJ, West DC. Building
healthier communities for children and families: applying asset-based
community development to community pediatrics. Pediatrics 2005;115:
1185-7.
7. Hufford L, West DC, Paterniti DA, Pan RJ. Community-based advocacy
training: applying asset-based community development in resident edu-
cation. Acad Med 2009;84:765-70.
8. Paterniti DA, Pan RJ, Smith LF, Horan NM, West DC. From
physician-centered to community-oriented perspectives on health
care: assessing the efficacy of community-based training. Acad Med
2006;81:347-53.
9. Kretzmann JP, McKnight JL. Building communities from the inside out:
a path toward finding and mobilizing a community’s assets. Chicago:
ACTA Publications; 1993.
-year residents at University of California Davis
Didactics Examples of activities
Health disparitiesCommunity assets foraddressing health dis-parities
� Assess WIC, a locally-organized farmers;market, a community-driven breakfastprogram that includes maternal socializationactivities, and the food bank as local assets forchild and maternal nutrition.
� Recognize local supports for breastfeeding byshadowing a community lactation specialist.
Determinants of healthABCDSocial capital
� Participate in a parent support group.� Visit a rural family resource center.� Understand challenges of adolescent-parentcommunication by talking with a local youthgroup about their communication strengthsand identifying opportunities for improvement.
� Identify local individual, associational, andinstitutional community assets for healthierfamily functioning
Cultural humilityPublic health
� Become familiar with community-grownefforts to support marginalized youth,including local volunteer networks andinstitutional ‘‘wrap-around’’ programs.
� Develop capacity by facilitating the discussionbetween young people and their parents aboutsafe driving practices.
DisabilitySchool health
� Shadow a speech pathologist and a specialeducation teacher to understand local com-munity and educational supports for specialneeds students.
set-Based Community 184.e1