communication and patient interviewing
DESCRIPTION
Communication and Patient Interviewing. Introduction to Primary Care: a course of the Center of Post Graduate Studies i n FM. PO Box 27121 – Riyadh 11417 Tel: 4912326 – Fax: 4970847. Land. Working. Man. Women. Family. Chatting . Aim. - PowerPoint PPT PresentationTRANSCRIPT

1
Communication and Communication and Patient InterviewingPatient Interviewing
Introduction to Primary Care: a course of the Center of Post Graduate Studies in FM
PO Box 27121 – Riyadh 11417Tel: 4912326 – Fax: 4970847

2
Land Working Man Women
Family
Chatting

3
• Aim: At the end of this session, the participants are expected to have knowledge on communication skills and patient interviewing.
• Objectives:– Knows basic principles of communication– Knows the place of verbal and nonverbal
communication in patient interview– Is aware of the importance of nonverbal clues– Know the importance of hidden agenda – Can explain the interview process
Aim
4
• A process of production and submission of knowledge/symbols, which are received and interpreted by the other party.
• Sharing
What is communication?
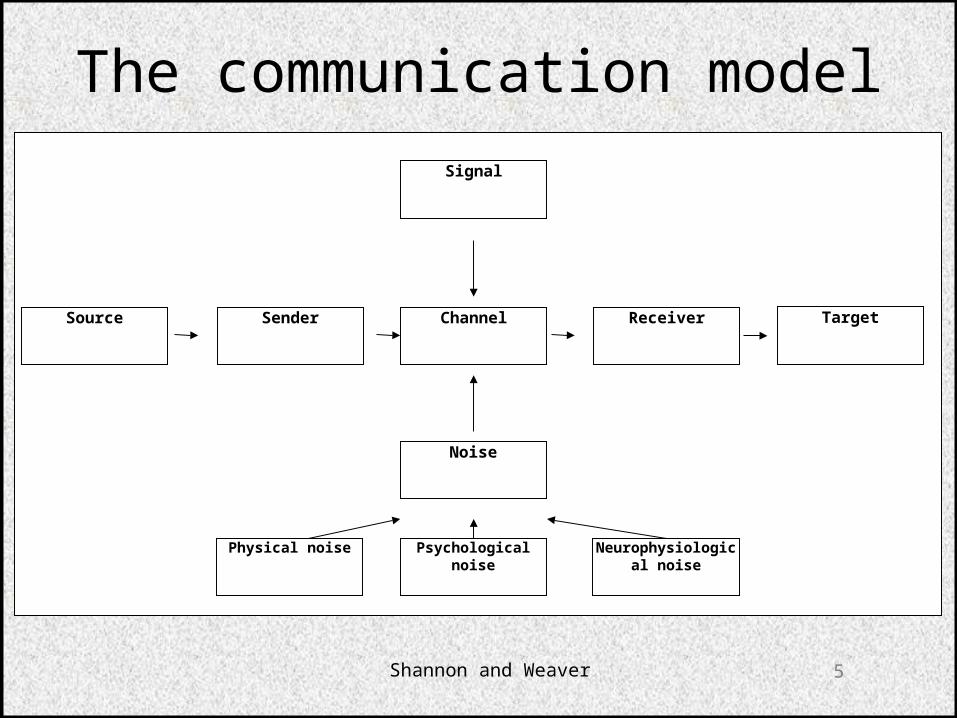
5Shannon and Weaver
Signal
Source Sender Channel Receiver Target
Noise
Physical noise Psychological noise Neurophysiological noise
The communication model

6
• 70% of the patients can be diagnosed by only communication
• Doctors who are good communicators are less suited by their patients
• Patient satisfaction increases when he/she can have a good communication with the doctor.
Patient communication
Lussier MT. Doctor-Patient Communication. Canadian Family Physician. 2006;52:1401-1402
7
• Percentage of doctors interrupting patients speech within the first 18 seconds:– 69%
• Proportion from these patients who didn’t even express their reason for encounter:– 77%
However
Beckman HB, Frankel RM. The effect of physician behavior on the collection of data. Ann Intern Med 1984;101:692-6
8
• Percentage of patients leaving doctors office who do not have enough information on their illness: – 50%
• Percentage of patients who do not know how to use their medication:– Around 50%
• Percentage of patients not adhering to the suggestions of their doctor:– 22-70%
Moreover
9
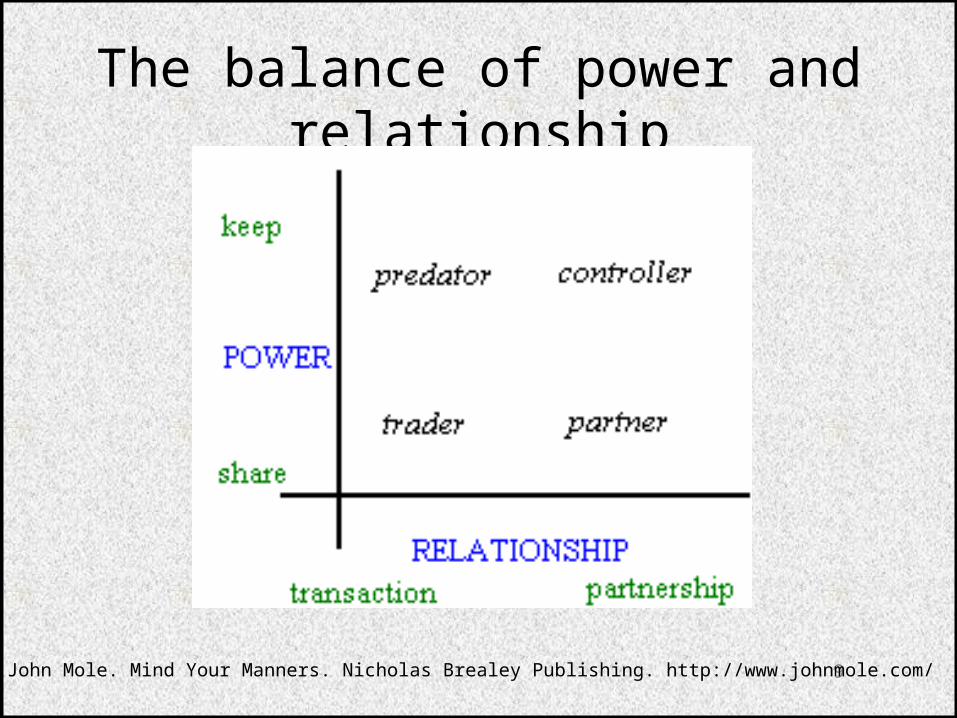
The balance of power and relationship
John Mole. Mind Your Manners. Nicholas Brealey Publishing. http://www.johnmole.com/
10
• Verbal (% 7)
• Paralanguage (% 38)
• Body language (% 55)
Components of face to face communication
11
• Things spoken• Things not spoken• Stumbling• Indecision• Hesitation• Avoidance• Whethering• Reflection• Hidden (masked) communication
Verbal communication
12
• S (smile)
• O (open posture)
• F (forward lean)
• T (touch)
• E (eye contact)
• N (nod)
Nonverbal communication
13
Hand shaking
14
Forward lean
15
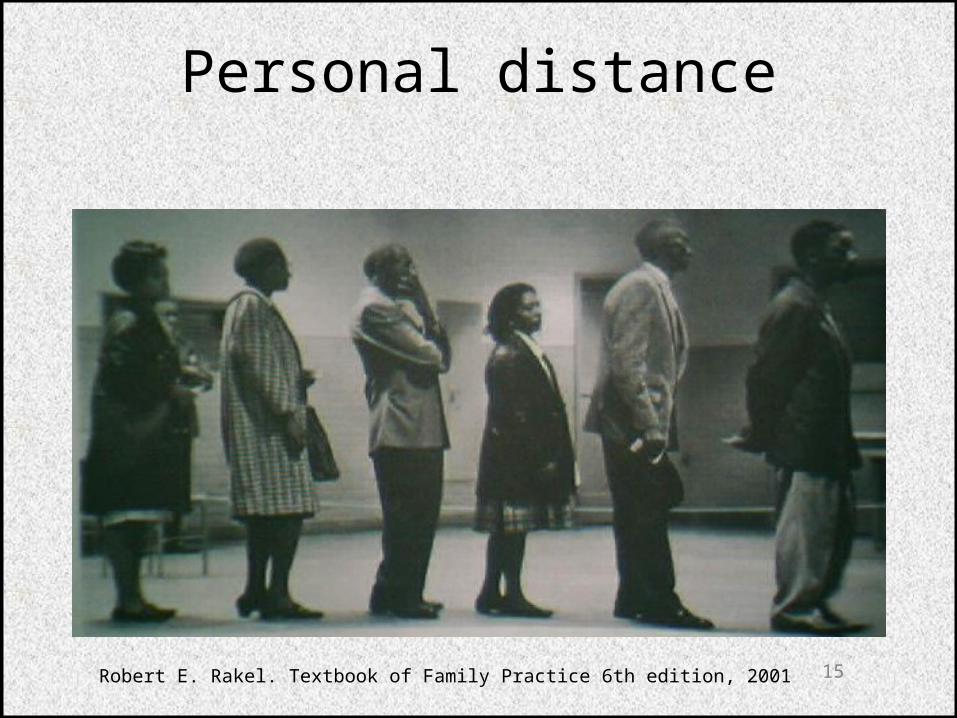
Personal distance
Robert E. Rakel. Textbook of Family Practice 6th edition, 2001

16
46 cm 1.2m 1.2-3.6m 3.6m
Intimate Personal Social Common
Personal distance

17
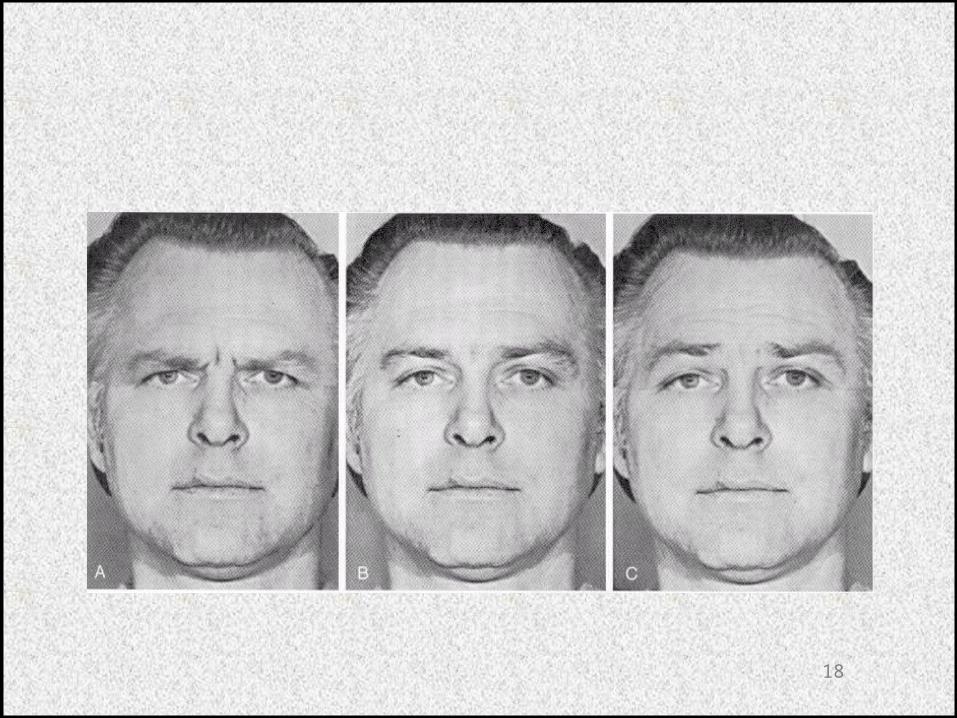
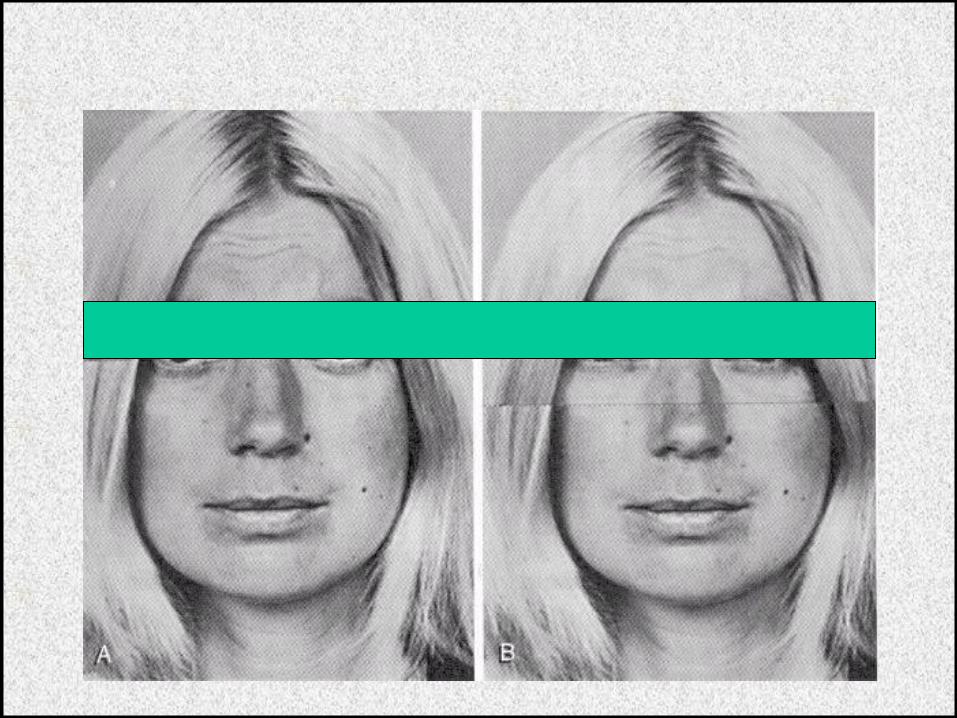
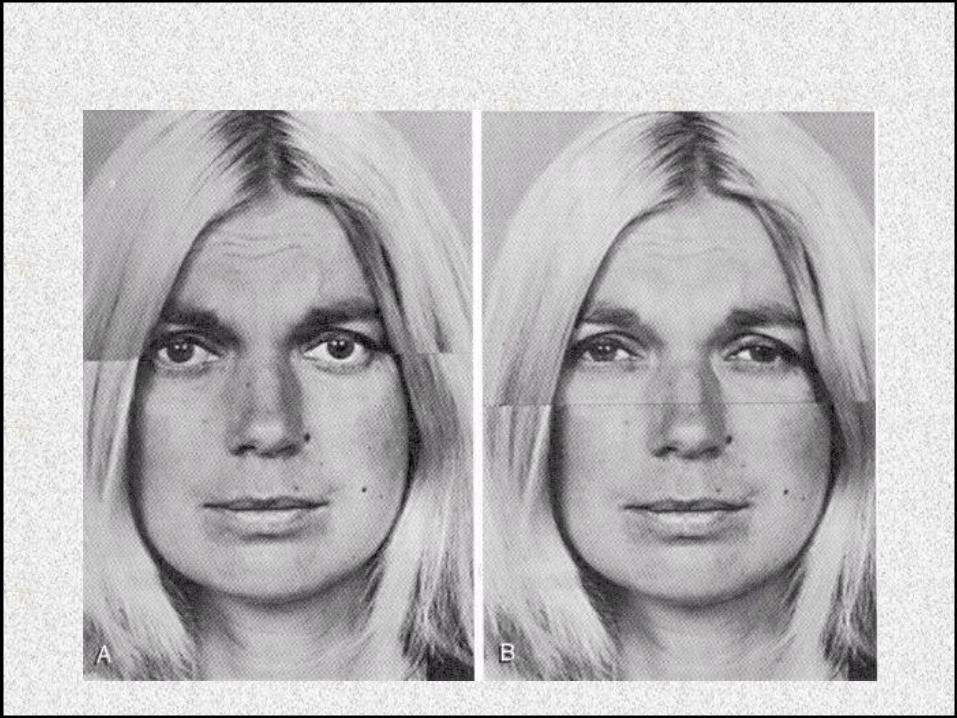
Mimics
18
19
20
21
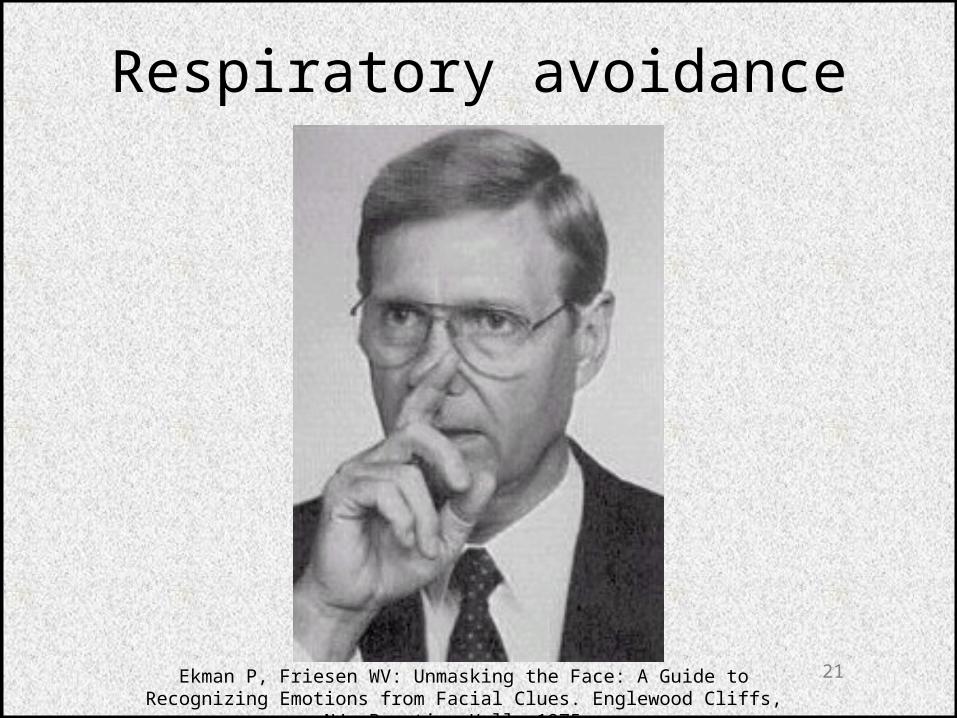
Respiratory avoidance
Ekman P, Friesen WV: Unmasking the Face: A Guide to Recognizing Emotions from Facial Clues. Englewood Cliffs, NJ, Prentice-Hall, 1975.
22
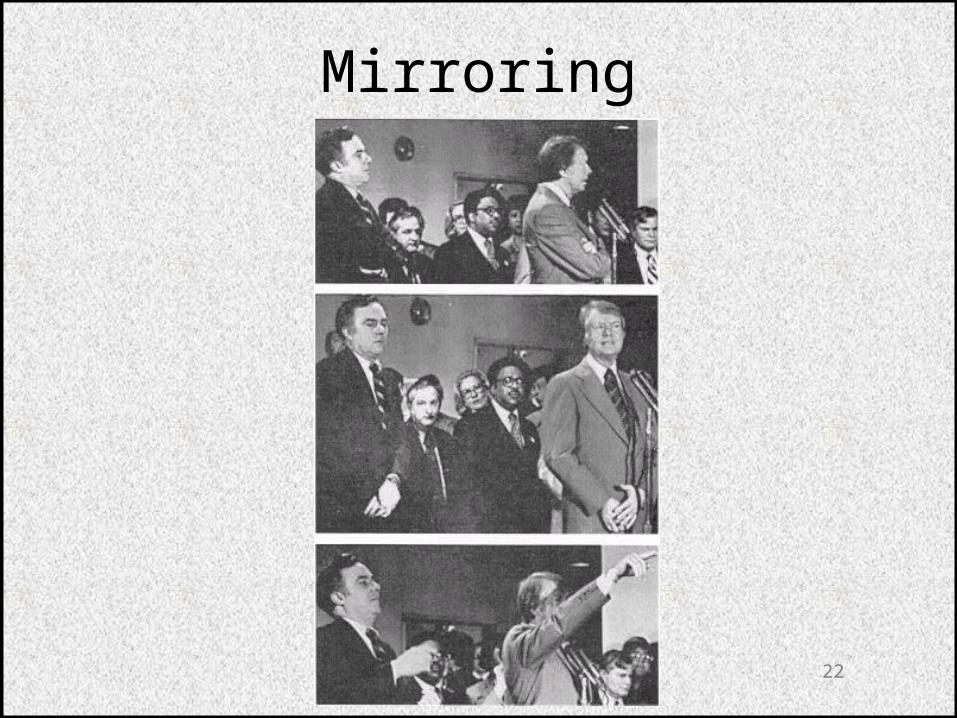
Mirroring

23
Father: How does his heart sound?Doctor: Sounds pretty good. He’s got a little murmur there. I’m not sure what it is. It’s … it uh … could just be a little hole in his heart.Mother: Is that very dangerous when you have a hole in your heart?Doctor: No, because I think it’s the upper chamber, and if it’s the upper chamber then it means nothing.Mother: Oh.Doctor: Otherwise they just grow up and they repair them.Mother: What would cause the hole in his heart?Doctor: H’m?Mother: What was it that caused the hole in his heart?Doctor: Doctor: It’s cause … uh … just developmental, when their uh …Mother: M-h’mDoctor: There’s a little membrane that comes down, and if it’s the upper chamber, there’s a membrane that comes down, one from each direction. And sometimes they don’t quite meet, and so there’s either a hole at the top or a hole at the bottom and then … it’s really uh … uh … almost never causes any trouble.
24
Mother: Oh.Doctor: It’s uh … one thing that they never get SBE from … it’s the only heart lesion in which they don’t.Mother: Uh-huh.Doctor: And uh … they grow up to be normal.Mother: Oh, good.Doctor: And uh … if anything happens they can always catheterize them and make sure that’s what it is, or do heart surgery.Mother: Yeah.Doctor: Really no problem with it. They almost never get into trouble so …Mother: Do you think he might have developed the murmur being that my husband and I both have a murmur?Doctor: No.Mother: No. Oh, it’s not hereditary, then?Doctor: No.Mother: Oh, I see. [Someone whistling in the room]
25
Doctor: It is true that certain people … tendency to rheumatic fever, for instance.Mother: H’mm.Doctor: There is a tendency for the abnormal antigen-antibody reaction to be inherited, and therefore they can sometimes be more susceptible.Mother: Oh, I see. That wouldn’t mean anything if uh … I would … I’m Rh negative andhe’s positive. It wouldn’t mean anything in that line, would it?Doctor: Uh-huh.Mother: No? Okay.Doctor: No. The only thing you have to worry about is other babies.Mother: M’h’m.Doctor: Watch your Coombs’ and things.Mother: Watch my what?Doctor: Watch your Coombs’ and things.Mother: Oh, yeah.Doctor: Your titres, Coombs’ titres. (p 68)

26
The body language
27
• Sometimes what hte patient says at the door is his/her real reason for coming.
• The door is safe; patient can leave easily if refused.
• Ask at the end: “Is there anything we have not covered or anything else you would like to ask me?”
Hand-on-the doorknob syndrome
Quill TE: Recognizing and adjusting to barriers in doctor-patient communication.
Ann Intern Med 111:51, 1989.
28
• Summary sentences
• Recognize deviations in perception/expectations
• Patient empowerment
• Patient participation
• Attentive listening
Patient interview
29
• Direct questions
• “Why” questions
• Guiding questions
• Yes-No questions
• Sudden topic changes
• Loss of eye contact
• Loss of feedback
Traps in the interview
30
• Defensive patient
• Anxious patient
• Angry patient
• Selfish and demanding patient
Problem patients
31
• It is possible to change the process and initiate a new behavior– How did I interpret the patient’s statements or
behavior to make myself angry?– Is there another way to interpret the patient’s
behavior?
Changing reactions to problem patients
32
• What is communication? • What models of communication do you know?• 1/2 of communication is by body language• The best doctor-patient interview is by sitting on
both sides of the table• Nonverbal messages are produced intentionally• In which body position is the patient most
receiving if you give some kind of education?
Summary