communicating medical bad news: parents' experiences and preferences
TRANSCRIPT

Communicating medical Parents" experiences and
bad news: preferences
Michae l C. Sharp, MD, Ronald P. Strauss, DMD, PhD, a n d Sharon C la i re Lorch, MSW
From the Department of Pediatrics, University of North Carolina at Ch~apel Hill School of Med- icine, and the Departments of Social Medicine and Dental Ecology, University of North Caro- lina at Chapel Hill School of Dentistry
Parents (N = 189) of children enrolled in 15 developmental day care centers completed questionnaires that examined the experience of being told bad news and elicited preferences for physician behavior in a hypothetical situation (communicating the diagnosis of Down syndrome). Parents, in comparison with their experiences, preferred (p <0.001) more communication of information and feelings by their physician. Their strongest preferences were for physicians to show caring (97%), to allow parents to talk (95%), and to allow parents to show their own feelings (93%). They wanted physicians to share information (90%) and to be highly confident (89%). Most parents (87%) desired parent-to-parent refer- ral, but only a few (19%) were referred. We conclude that there is a difference between what parents experience and what they desire in physicians who com- municate bad news. Physicians control the interaction and are highly confident, but parents especially value physicians who show caring and allow parents to talk and share their feelings. (J PEDIATR 1992;121:539-46)
Physicians can remain objective and professional and still impart to others some very basic human elements: kindness, sympathy, empathy--and, above all, never, never try to take away faith or hope.--47-year-old mother/nurse of 19-year-old man with severe brain damage
Numerous authors have focused on the telling of medical bad news, 1,2 and some have suggested that it elicits an
overall negative response because of its intrinsic emotional difficulty. In testing this hypothesis, Cunningham et al. 3 found that parents appreciated an "ideal" approach and could distinguish between that and their own negative rec- ollections.
Cunningham and Sloper 4 studied parents of children with
Down syndrome and determined that parents wanted to be given the diagnosis in a realistic, sympathetic, and positive manner. The timing of imparting information was found to be critical; parents found it difficult to absorb anything but
Submitted for publication Jan. 28, 1992; accepted April 22, 1992. Reprint requests: Michael C. Sharp, MD, University of North Carolina School of Medicine, CB No. 7340, Division of Commu- nity Pediatrics, Chapel Hill, NC 27599-7340. 9 / 2 0 / 3 8 8 1 1
the most basic information at the time of diagnosis. The majority of parents wanted to be told of the diagnosis (even if only a suspicion) within the first 24 to 48 hours, and re- quested later opportunities for more intensive discussion and practical information on how to help their child. Par- ents wanted to be given bad news together, in a private set- ting, and to be able to be alone together afterward. They wanted to be able to be with their child when they are told or immediately thereafter. The few parents who were given the opportunity to meet other families of children with sim- ilar disabilities appeared to have made the best adjustment; however, about one third of the parents did not feel ready to meet other parents until several months after the birth.
According to Quine and Pahl, 5 parents value a sympa-
thetic and caring approach by physicians and say they want to be given full information about the child's condition. A high degree of physician control of the interaction was of- ten found to be a source of parental dissatisfaction. Svars- tad and Lipton 6 found parental ability to accept the diag- nosis of mental retardation to be dependent on clear and frank professional communication. Lynch and Staloch 7 suggested that parents want to know how children will function in the home, strategies for facilitating growth and
539

5 4 0 Sharp, Strauss, and Lorch The Journal of Pediatrics October 1992
development, referral to community resources, and sugges- tions on how to inform friends and family. They found that parents wanted more information from their physician than was provided. Most parents reported that the early advice given to them by physicians concerning the developmental potential or future employability of their child with Down syndrome had been too pessimistic or gloomy, and often this was a source of parental dissatisfaction. 8, 9
The literature does not provide insight into specific fac- tors that may influence parents' memories of being told bad news or their degree of satisfaction with the experience, nor does the literature indicate what constitutes caring at- tributes or behavior in this setting. Such information should assist in the preparation of physicians for delivering bad news to families. Although social class and socioeconomic factors have been discussed as potentially influencing this communication,9, 10 little is known about how these influ- ences modify parental experiences and preferences. The purpose of this study is to understand these influences and to delineate in detail the physician behaviors that parents have experienced, and those which they desire, in the tell- ing of bad news.
M E T H O D S
Data collection. A questionnaire was developed to record how parents of children with developmental disabilities re- member the experience of being told the diagnosis of their child's condition. The questionnaire also assessed parents' perspectives on how the telling of bad news might be done ideally and what parents believe is common medical prac- tice. The dimensions of physician behavior chosen for study were derived from observations of unrehearsed videotapes of 48 pediatric residents practicing the telling of bad news to actor/parents. In these videos, parents were informed that their newborn infant had Down syndrome. The tapes were viewed by a group of physicians and social scientists (medical sociologist, family physician, pediatrician, social worker, medical anthropologist, and special educator) who selected nine tapes that demonstrated representative ap- proaches to this physician-patient encounter. These tapes were differentiated by the degree of control and the amount of caring displayed by the resident. The nine tapes were shown to groups of parents of children with developmental disabilities, who reacted to the content and discussed the behaviors that differentiated the residents. On the basis of their reactions, a list of important behaviors relative to the telling of bad news was genemt.ed. This process resulted in the selection of the following variables for study:
1. Degree of physician control of interaction 2. Time needed for physicians to "get to the point" 3. How much physicians care about parents" feelings 4. How much physicians allow the expression of parents" feel-
ings
5. Physicians' level of confidence in this setting 6. How much physicians show their own feelings 7. How much physicians permit parents to talk 8. How much physicians try to make the parents feel better 9. Amount of information physicians give to parents
10. How thoroughly physicians describe the likelihood of men- tal retardation
The survey's self-administered questionnaires were pre- tested with 16 parents in a Down syndrome support group to confirm the relevance of the content and determine whether such a self-administered instrument was sensitive to differences in perspective or preferences. Modified Likert scaling was chosen to allow for five-point responses to all queries. Another focus group (n = 20) in a group for par- ents of children with developmental disabilities utilized a preliminary questionnaire-rating mechanism and demon- strated their ability to respond on the Likert five-point scales. Wording and content were refined on the basis of their feedback. After the questionnaires were presented to a statewide meeting of directors of day care centers for children with developmental disabilities, the directors gave additional comments on the questionnaire.
The survey instruments were divided into three parts: ratings of how most physicians communicate, parents' rat- ings of experiences with their own child, and parents' pref- erences for how a physician should respond in a hypothet- ical situation (informing parents of a diagnosis of Down syndrome).
The tables presented in this article express the five-point Likert scale of parent ratings in trichotomized form (col- lapsing "somewhat low" and "very low" ratings into "low", and similarly for "high"; the middle category of "neither high nor low" remained unchanged). However, in the sta- tistical analysis, we used the five-point scale to compute means and perform t tests.
Social and demographic data were also collected. Many respondenSs used the comments section of the questionnaire to describe their experiences or preferences in greater detail. The parent quotes in this article were extracted from that section.
Sample characteristics. The sample studied was of par- ents who have children in developmental day care centers in North Carolina; all had experienced the communication of bad news about their child. To reach these parents, we contacted the directors of such centers at a statewide meet- ing and enlisted their participation. Of 22 developmental day care centers sent research materials, 15 (68%) partic- ipated. These centers had a total enrollment of 566 children. The participating centers were sent questionnaires, and their directors were asked to distribute and collect them from parents and return them to the investigators. One hundred eighty-nine questionnaires (33% response rate) were received, the mean being 12.6 responses per center.

Volume 121 Communicating medical bad news 54 1 Number 4
The sample was composed primarily of mothers and was largely white (Table I). Almost half of the sample had 12 or more years of education, and approximately one in five had completed college. The median age for parents was 31 years. At the time of the diagnosis, one (22%) of five par- ents was single. One fourth of the total sample had one child (26%), an additional 40% had two children, and 34% had three or more children.
Most parents were able to specify their child's diagnosis (94%); of these, many (59%) reported a single diagnosis for one child. Eleven percent indicated that they had more than one child with special needs, although their reporting was asked to be limited to the child enrolled in the developmen- tal day care program. Almost one in three of the children in this study (29%) has multiple disabilities. For the children with one disability (n = 105), the sample included children with mental retardation/developmental disability (35%), cerebral palsy (30%), Down syndrome (14%), other genetic syndromes (10%), and other disabilities (11%).
Parents were asked to remember when they were told about their child's condition, and to indicate how the doc- tor acted. Many parents were told of the diagnosis at the time of their child's birth (39%); many others learned of the diagnosis during the first year of life (37%). Twenty-four (13%) parents learned of the diagnosis when their child was between 1 and 2 years of age; only 21 parents (11%) received the diagnosis after the child was 2 years of age. An examination of the effect of the child's age at diagnosis and of the elapsed time between diagnosis and questionnaire suggested that these factors did not significantly influence parental responses in this study.
R E S U L T S
Parents' experiences of being told the diagnosis of their child's condition. The findings relative to parents' experi- ences are presented according to three dimensions of professional behavior plus information concerning socio- economic influences and referrals to other parents.
I am very pleased with my children's doctor. He has been their doctor since birth, and he really gets to the point when he finds something and he gives me a chance to talk and ask questions, and even comment on some little thing that my children may have done or said. He's really got a sense of humor, too, and I think that helps lighten the mood under most circumstances. I wouldn't trade my children's pediatrician for anything.--26-year-old mother of a 7-year-old child with mental retardation
The doctor came into the recovery room and all he said was, "Hey, man, I hate to lay this thing on you now, but your child is Down syndrome. She probably won't even be able to do any more than dress herself." I do know I will never forget the way he told us. It is burned into my memory forever.--39-year-old mother of a 4-year-old girl with Down syndrome
Among the parents (n--- 156) who specified whether
Table I. Sample characteristics
Characteristic % No.
Race White 64.9 122 African-American 28.2 53 Other 6.9 13
Education --<9 yr 10.9 20 10-12 yr 41.8 77 >12 yr 47.3 87
Gender Women 93.0 174 Men 7.0 13
Age of parent <25 yr 14.0 26 25-30 yr 28.5 53 31-35 yr 26.3 49 ~36 yr 31.2 58
anyone else was in the room at the time of diagnosis, some were alone (30%), some were with their spouse (45%), and some had other persons present (26%). Parents were most likely to be informed by a pediatrician (31%), neonatologist (18%), or another physician (12%); other professionals composed the remainder. Most of the informing profes- sionals .were male (79%).
Elements o f interaction
I was never asked how I felt. The whole conversation was about Travis.--39-year-old mother with 22-month-old son who is hear- ing impaired and has a speech delay
Most parents found that the physician had a high degree of control over the interaction during which the family was informed about their child's diagnosis (Table II). Such lev- els of professional control did not seem to diminish parental perceptions of their ability to contribute to the conversation. Most parents held that the physician gave them a consid- erable chance to talk. However, fewer than half (47%) of the parents believed that the physician gave them much oppor- tunity to show their feelings. Nearly as many parents (41%) believed that the physician made little effort to make them feel better. When the means of the variables describing the parents' experiences in the interaction were listed from highest to lowest, "doctors' control of conversation" was highest, followed by physicians' "allowing parents to talk" and "show feelings." Efforts to "make the parents feel bet- ter" were ranked lower.
Information management
I don't want them to unnecessarily scare the hell out of me--but I hate the feeling of being in the dark. Especially when a new prob- lem appears with a medical name a mile long, I don't know the "right" questions to ask.--29-year-old mother of 4-year-old child with spastic diplegia
5 4 2 Sharp, Strauss, and Lorch The Journal of Pediatrics October 1992
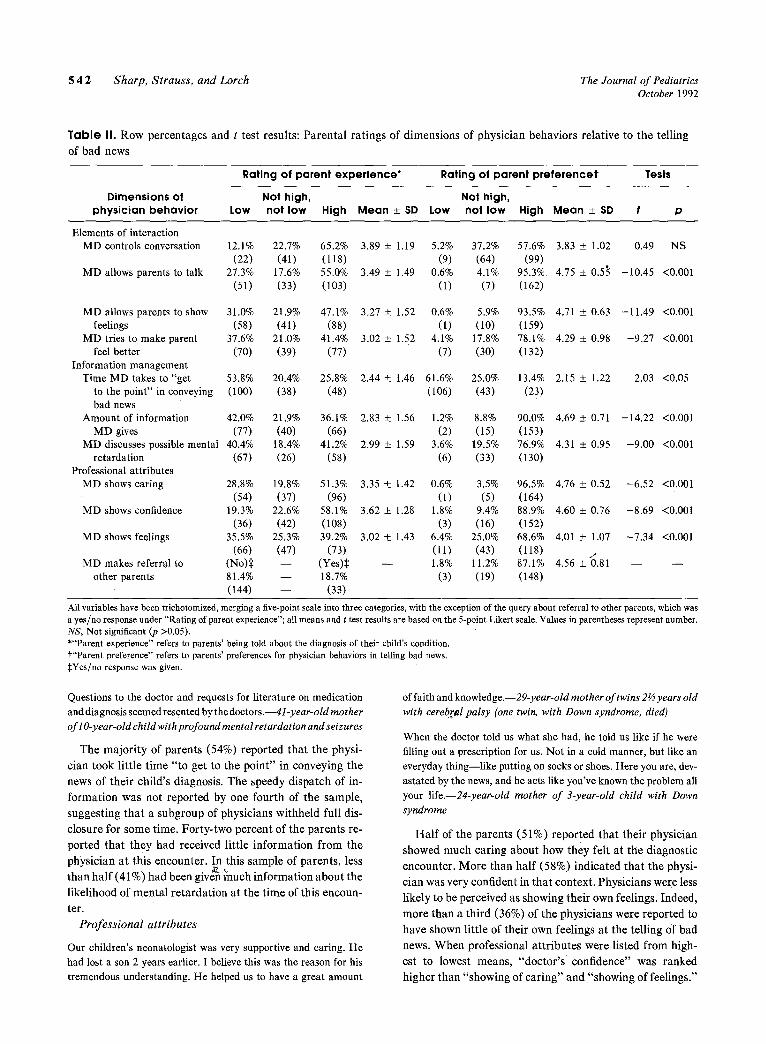
T a b l e II. Row percentages and t test results: Paren ta l ra t ings of dimensions of physician behaviors relat ive to the telling
of bad news
Rating of parent experience* Rating of parent preferencet Tests
Dimensions of Not high, Not high, physician behavior Low not low High Mean _+ SD Low not low High Mean +_ SD t p
Elements of interaction MD controls conversation
MD allows parents to talk
12.1% (22)
27.3% (51)
MD allows parents to show 31.0% feelings (58)
MD tries to make parent 37.6% feel better (70)
Information management Time MD takes to "get 53.8%
to the point" in conveying (100) bad news
Amount of information 42.0% MD gives (77)
MD discusses possible mental 40.4% retardation (67)
Professional attributes MD shows caring 28.8%
(54) MD shows confidence 19.3%
(36) MD shows feelings 35.5%
(66) MD makes referral to (No):~
other parents 81.4% (144)
22.7% 65.2% 3.89 _+ 1.19 5.2% 37.2% 57.6% 3.83 _+ 1.02 0.49 NS (41) (118) (9) (64) (99)
17.6% 55.0% 3.49 +_ 1.49 0.6% 4.1% 95.3% 4.75 _+ 0.53 -10.45 <0.001 (33) (103) (1) (7) (162)
21.9% 47.1% 3.27 -+ 1.52 0.6% 5.9% 93.5% 4.71 + 0.63 -11.49 <0.001 (41) (88) (1) (10) (159)
21.0% 41.4% 3.02 -+ 1.52 4.1% 17.8% 78.1% 4.29 _+ 0.98 -9.27 <0.001 (39) (77) (7) (30) (132)
20.4% 25.8% 2.44 +_ 1.46 61.6% 25.0% 13.4% 2.15 +_ 1.22 2.03 <0.05 (38) (48) (106) (43) (23)
21.9% 36.1% 2.83 -+ 1.56 1.2% 8.8% 90.0% 4.69 + 0.71 -14.22 <0.001 (40) (66) (2) (15) (153)
18.4% 41.2% 2.99 -+ 1.59 3.6% 19.5% 76.9% 4.31 + 0.95 -9.00 <0.001 (26) (58) (6) (33) (130)
19.8% 51.3% 3.35 -2-_ 1.42 0.6% 3.5% 96.5% 4.76 + 0.52 -6.52 <0.001 (37) (96) (1) (5) (164)
22.6% 58.1% 3.62 + 1.28 1.8% 9.4% 88.9% 4.60 _+ 0.76 -8.69 <0.001 (42) (108) (3) (16) (152)
25.3% 39.2% 3.02 ___ 1.43 6.4% 25.0% 68.6% 4.01 _+ 1.07 -7.34 <0.001 (47) (73) (11) (43) (118) t - - (Yes)~ - - 1.8% 11.2% 87.1% 4.56 + 0.81 - - - - - - 18.7% (3) (19) (148) - - (33)
All variables have been trichotomized, merging a five-point scale into three categories, with the exception of the query about referral to other parents, which was a yes/no response under "Rat ing of parent experience"; all means and t test results are based on the 5-point Likert scale. Values in parentheses represent number. NS, Not significant (p >0.05). *"Parent experience" refers to parents' being told about the diagnosis of their child's condition. t"Parent preference" refers to parents' preferences for physician behaviors in telting bad news. :~Yes/no response was given.
Questions to the doctor and requests for literature on medication and diagnosis seemed resented by the doctors.--41-year-old mother of l O-year-old child with profound mental retardation and seizures
The major i ty of parents (54%) reported tha t the physi-
cian took li t t le t ime " to get to the point" in conveying the
news of their child's diagnosis. The speedy dispatch of in-
format ion was not reported by one four th of the sample,
suggesting t ha t a subgroup of physicians withheld full dis-
closure for some time. Forty-two percent of the parents re-
ported tha t they had received little informat ion f rom the
physician at this encounter. In this sample of parents , less �9 , ~ . .
than ha l f (41%) had been gtven much mformat ton about the
likelihood of menta l re tardat ion at the t ime of this encoun-
ter.
Professional attributes
Our children's neonatologist was very supportive and caring. He had lost a son 2 years earlier. I believe this was the reason for his tremendous understanding. He helped us to have a great amount
of faith and knowledge.--29-year-old mother of twins 2�89 years old with cereb!M palsy (one twin, with Down syndrome, died)
When the doctor told us what she had, he told us like if he were filling out a prescription for us. Not in a cold manner, but like an everyday thing--like putting on socks or shoes. Here you are, dev- astated by the news, and he acts like you've known the problem all your life.--24-year-old mother of 3-year-old child with Down syndrome
Hal f of the parents (51%) reported tha t their physician
showed much caring about how they felt at the diagnostic
encounter. More than hal f (58%) indicated tha t the physi-
cian was very confident in t ha t context. Physicians were less
likely to be perceived as showing thei r own feelings. Indeed,
more than a th i rd (36%) of the physicians were reported to
have shown litt le of their own feelings at the telling of bad
news. W h e n professional a t t r ibutes were listed from high-
est to lowest means, "doctor ' s confidence" was ranked
higher than "showing of car ing" and "showing of feelings."
Volume 121 Communicating medical bad news 5 4 3 Number 4
Socioeconomic effects and parental memories. Paren t
educat ion and race were examined with chi-square analysis
to de te rmine their influence on parenta l experience. On
most of the ra t ing variables there was no significant effect
(p <0 .05) of educat ion or race. Significant effects of both
parent educat ion and race were found only on parent rat-
ings of how much the physician allowed them to ta lk and
how much informat ion he or she gave at the t ime of diag-
nosis.
Paren t s with less than college educat ion (63%) were more
likely (p = 0.05) to perceive tha t the physician gave them
a chance to talk, in comparison with those who had college
educat ion (48%). Minor i ty parents (69%) were also more
likely (p = 0.05) than white parents (49%) to feel t ha t the
physician gave them a chance to talk a t the t ime of diagno-
sis.
Paren t s with less than college educat ion (46%) were more
likely (p = 0.03) to perceive tha t the physician gave them
a lot of informat ion than were those with college educat ion
(25%). Minor i ty parents (56%) were also more likely
(p = 0.003) than white parents (26%) to believe t ha t the
physician gave them a lot of informat ion at the t ime of di-
agnosis.
Pa ren t education, bu t not race, was significantly associ-
ated (p = 0.03) with the physician's show of feelings. Par-
ents with less than college educat ion (47%) were more likely
to find the physician touched or moved by the i r situation,
than were college-educated parents (32%).
Race, but not parent education, was significantly related
(p = 0.004) to the perception of the physician 's a t t empt to
help the parents feel better. Minor i ty parents (61%) were
more likely to perceive the physician as trying to help them
feel be t te r than were white parents (32%).
Referral to other parents
There was so much negativity thrown at us on top of all the rest of our problems and worries about her. No one told us how much love and happiness she would bring in our lives. What we needed was other people to talk with who had been there, firsthand. Not pro- fessionals, but parents--loving, caring people. We didn't meet oth- ers until she was about 6 months old. That's a long time to find out that we were not alone. Also that it's not the end of the world to have a special needs child.--36-year-old mother of 6-year-old girl with chromosomal abnormality
Parents were asked whether " the doctor put them in
touch with other parents with a child like their own." Few
parents (19%) reported tha t such a referral was init iated. Of
the 74 families who learned the diagnosis at the child's bir th,
only 6 (8%) were referred to another parent.
Pa ren ta l preferences for how a physician should commu-
nicate
I feel the doctors, all doctors, should be more willing to listen to what we, as parents, have to say. After all, we are with our children
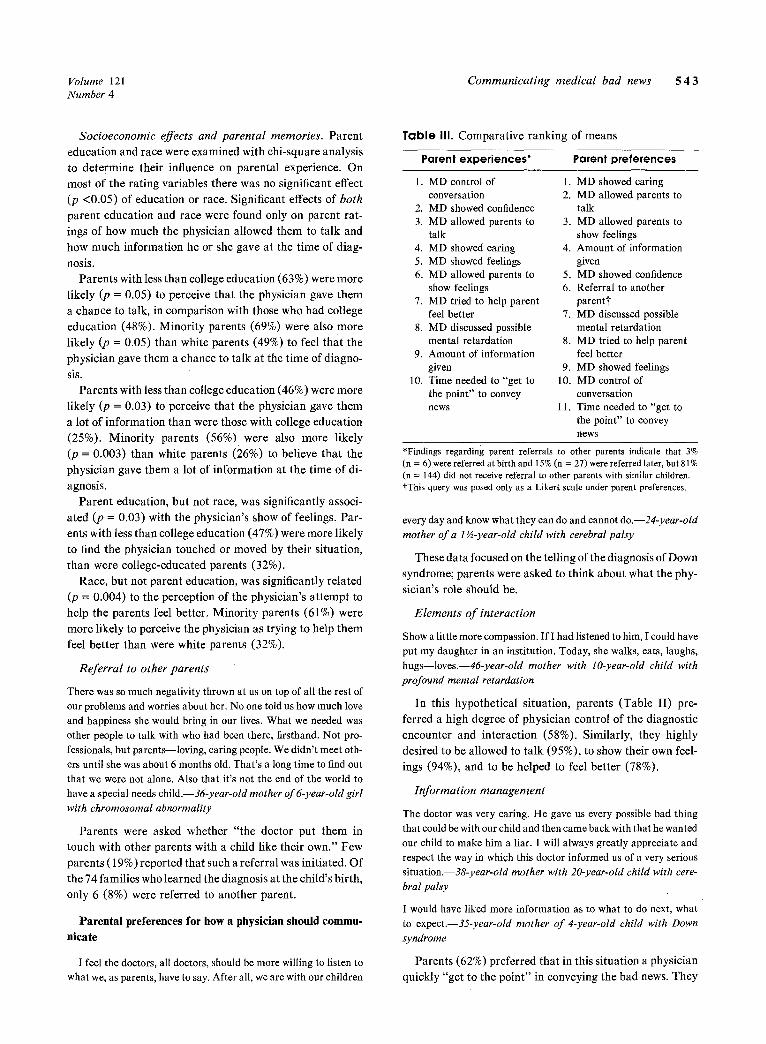
Table III. Compara t ive rank ing of means
Parent experiences* Parent preferences
1. MD control of 1. MD showed caring conversation 2. MD allowed parents to
2. MD showed confidence talk 3. MD allowed parents to 3. MD allowed parents to
talk show feelings 4. MD showed caring 4. Amount of information 5. MD showed feelings given 6. MD allowed parents to 5. MD showed confidence
show feelings 6. Referral to another 7. MD tried to help parent parentt
feel better 7. MD discussed possible 8. MD discussed possible mental retardation
mental retardation 8. MD tried to help parent 9. Amount of information feel better
given 9. MD showed feelings 10. Time needed to "get to 10. MD control of
the point" to convey conversation news 11. Time needed to "get to
the point" to convey news
*Findings regarding parent referrals to other parents indicate that 3% (n = 6) were referred at birth and 15% (n = 27) were referred later, but 81% (n = 144) did not receive referral to other parents with similar children. tThis query was posed only as a Likert scale under parent preferences.
every day and know what they can do and cannot do.--24-year-old mother of a 1�89 child with cerebral palsy
These data focused on the telling of the diagnosis of Down
syndrome; parents were asked to th ink about what the phy-
sician's role should be.
Elements of interaction
Show a little more compassion. If I had listened to him, I could have put my daughter in an institution. Today, she walks, eats, laughs, hugs--loves.--46-year-old mother with lO-year-old child with profound mental retardation
In this hypothet ical si tuation, parents (Table II) pre-
ferred a high degree of physician control of the diagnostic
encounter and interact ion (58%). Similarly, they highly
desired to be allowed to ta lk (95%), to show their own feel-
ings (94%), and to be helped to feel be t ter (78%).
Information management
The doctor was very caring. He gave us every possible bad thing that could be with our child and then came back with that he wanted our child to make him a liar. I will always greatly appreciate and respect the way in which this doctor informed us of a very serious situation.--38-year-old mother with 20-year-old child with cere- bral palsy
I would have liked more information as to what to do next, what to expect.--35-year-old mother of 4-year-old child with Down syndrome
Parents (62%) preferred tha t in this si tuation a physician
quickly "get to the point" in conveying the bad news. They

5 4 4 Sharp, Strauss, and Lorch The Journal of Pediatrics October 1992
strongly (90%) indicated a desire for a lot of information at this encounter. Furthermore, parents preferred (77%) being told in detail about the possibility of mental retardation at the first encounter.
Professional attributes
The doctor simply stated the diagnosis, handed us some papers with general information,.., told us to institutionalize him, and walked out the door. We would like to have been treated like human be- ings.--32-year-old mother of 4-year-old child with cerebral palsy
Our doctor that diagnosed our son could not have handled our "bad news" conversation better. He was caring, sympathetic (even tears in his eyes), direct, to the point without rushing. He answered our questions "straight"--no sugarcoating, but not total gloom and doom either.--39-year-old mother with 2-year-old with Cornelia de Lange syndrome
Nearly all parents preferred a physician to show a high degree of caring in this setting (97%). Most parents wanted physicians to show strong confidence (89%) and to show
much of their ow n feelings (69%). Socioeconomic influences on parents" preferences. Sig-
nificant effects of parent education and race as tested by chi-square analysis (p <0.05) were generally limited to the queries about parents' preferences for physicians' informa- tion management. Parents with less than college education (97%) were more likely than college-educated parents (82%) to want a great deal of information at the time of di- agnosis (p = 0.05). Minority parents were also more likely than white parents to desire a lot of information at this en- counter (p -- 0.04). Parents with less than college education (83%) in comparison with college-educated parents (69%) desired much information about the possibility of mental retardation (p = 0.02). Minority parents were similarly more desirous than white parents of such information (t9 = 0.006). Parents with less than college education (17%) (p = 0.04) and minority parents (20%) (p = 0.02) were more likely than college-educated parents (9%) or white parents (10%) to desire a physician to take a long time to "get to the point". Most parents did not want the physicians to delay in telling the bad news.
The only other parent preference influenced by parent race (although not by education) was the degree of confi- dence shown by the physician. Minority parents (95%) had a greater preference than white parents (86%) for their physician to show a high degree of confidence (p = 0.02).
Referral to other parents
It would have been nice to be put in touch with other parents of a child with Joubert syndrome.--29-year-old mother of a l 6-month- old child with Joubert syndrome
On a five-point Likert scale, parents had a strong (87%) preference for physicians to "put parents in touch with other
parents with a similar child." Few parents (2%) had a low desire for such a referral.
Parents' preferences compared with their experience
It took a pediatrician, willing to admit the limitations of doctors, willing to cry and share his own feelings with us, to change our minds and seek the second opinion that saved our son's life! He be- came an equal with us in caring about the future of our child and family.--44-year-old mother of 12-year-old child with spina bifida and hydrocephalus
The doctor who first saw Karen's problem was.. , so horrible in handling us we tried to not pay his bill! He was terribly abrupt, businesslike, no compassion. I've had many bad experiences with doctors and rarely have met any who considered parents' opinions valuable. I feel they must have been taught in "med" schools to detach--stay distant and controlling.--37-year-old mother of 5- year-old child with autism and mental retardation
A comparison was performed between parental experi- ences and parental preferences (Table II). A significant difference existed for nine of ten comparisons; parents gen- erally prefered more interaction, information, and emo- tional content than was their experience. Table III shows a comparative ranking of means. The leading parental pref- erences were to have a physician who shows caring and who allows parents to talk and to show their own feelings. Phy- sician control of the conversation ranked highest in parent memory and nearly lowest in parent preference. In spite of its relatively low comparative ranking, physician control of the interaction was still preferred by the majority of respondents. Parents recall getting relatively little informa- tion at the time of their child's diagnosis, but rank this as highly preferred.
D I S C U S S I O N
This study provides insight into the relative importance of specific physician behaviors in the telling of bad news to parents. Previous studies have identified important features associated ~ t h parental satisfaction with the communica- tion of bad news. 4-9 This study should help physicians un- derstand what behaviors are most important to parents who are hearing bad news.
Parental memories may transform the reality of experi- ence, especially given the emotional nature of hearing bad news. It is possible that parents may recollect poor experi- ences more clearly than positive ones, or that dissatisfied parents are more likely to respond in studies such as this. There was no means in this retrospective study to provide documentation of actual physician behaviors, although we are convinced that parental recollections are a critical out- come measure. The comments and responses from parents indicated that the memories of "being told" are often etched into their consciousness on a permanent basis. Many parents wrote extensive commentaries on the back of the

Volume 121 Communica t ing medical bad news 545 Number 4
questionnaire forms and sometimes expressed the unful- filled desire to communicate once again with the physician who told them of their child's condition. The response rate to the questionnaire in this study limits the ability to gen- eralize, although the sample provides insights into the ex- periences of a group of parents.
The physician was often perceived as in control, confi- dent, and able to allow the parents to talk, although less likely to allow the parents to show feelings. Parents remem- ber receiving little information at this encounter, including little information about the likelihood of mental retarda- tion. Parents most value the physician's ability to show car- ing, and to allow time for parents to talk and show feelings. Parents experienced significantly fewer of these desired be- haviors in the physicians who told them bad news. Nearly all parents desired referral to other parents, but only one in five had received such a referral.
Less educated and minority parents were more likely to report having been given sufficient information and an ad- equate opportunity to talk during the initial encounter. When asked about their preferences, however, less educated and minority parents desired even more information, com- pared with others. It is possible that minority parents, or those with less education, more strongly perceive a need for information because they may know less about medical conditions and may have less access to sources of informa- tion aside from the physician.
Little is known about how physicians are prepared to perform one of their most difficult professional roles, the telling of bad news. Some medical schools v use videotaped role-playing techniques as a training tool, but most medical students learn these skills by either observation or trial and error. Rarely are parents in a position to provide feedback to the conveyer of bad news, because they are generally ab- sorbed in the process. The findings from this study may help inform educators about what behaviors and communicative approaches should be taught to physicians relative to the telling of bad news. Although personality plays a role in the ability of physicians to project to another's situation and then develop a relationship, studies indicate that physicians in training are capable of learning new techniques. 12
Physicians evaluate their effectiveness partly by their ability to heal their patients and make them feel better. Faced with a lifelong diagnosis for a newborn child, the physician may feel ineffectual. Physicians who believe that they cannot help may avoid dealing with the issues or en- gaging with parents. There may also be a concern that op- ening communication will encourage an endless demand from the family for support. Physicians may put a dispro- portionate emphasis on treating the child, rather than on allowing the parents to talk or to reveal their feelings. Phy- sicians sometimes place a high value on intellect and may find it difficult to understand that a cognitively limited child
may be wanted, may enhance the life of a family, and may lead a worthy life.
The crisis of hearing bad news evokes discomfort. The knowledge that bad news is likely to initiate parental exPression of emotions such as crying and anger may make physicians uncomfortable. Physicians may identify with the parents' plight and fear their own emotions. On the other hand, experienced physicians may see so much pain and suffering that they insulate themselves.
More needs to be learned about the value system of phy- sicians and how they develop caring attitudes about paren- tal needs. Medical education is generally oriented toward teaching factual and objective material, with less emphasis on emotional and sociocultural content. What factors influence medical students' and residents' abilities to com- municate in a caring manner? Are physicians convinced by their training that parental perspectives have importance and can help educate clinicians? Are they encouraged to express their own feelings about their patients?
The moment of being told bad news is critical for several reasons. It is the time at which the "ideal" wanted child ceases to exist and the new "special," and often unexpected, child becomes real. At this moment the family's life is changed on a permanent basis. Parents, often young, may lack experience in handling such news, and may feel lost, inadequate, or fearful. This encounter initiates the process of adapting to the new child, and the quality of the inter- action may affect how the family "sees" or accepts the child and his or her special needs. The person who tells bad news takes on an important position by virtue of providing the family's introduction to the child's future. If the physician's behavior inspires trust, the family may be able to enter the future more readily. If the physician is perceived as behav- ing in ways that increase the family's discomfort, then the parents may have difficulty accepting the child and being hopeful. The conveyer of bad news must be skilled at inspiring trust and able to communicate effectively with
parents.
We acknowledge the insight and assistance of Dr. Susan Schooley and the parent-to-parent groups that participated in the initial phases of this project. We are grateful to the parents who shared their feelings and experiences and to the directors of the de- velopmental day care centers that participated.
R E F E R E N C E S
1. Pueschel SM, Murphy A. Assessment of counseling practices at the birth of a chilffwith Down's syndrome. American Jour- nal of Mental Deficiency 1976;81:325-30.
2. Gayton WF, Walker L. Down syndrome: informing the parents. Am J Dis Child 1974;127:510-2.
3. Cunningham CC, Morgan PA, McGucken RB. Down's syn- drome: is dissatisfaction with disclosure of diagnosis inevita- ble? Dev Med Child Neurol 1984;26:33-9.

5 4 6 Sharp, Strauss, and Lorch The Journal of Pediatrics October 1992
4. Cunningham CC, Sloper T. Parents of Down's syndrome ba- bies: their earlier needs. Child Care Health Dev 1977;3:325- 47.
5. Quine L, Pahl J. First diagnosis of severe mental handicap: characteristics of unsatisfactory encounters between doctors and parents. Soc Sci Med 1986;22:53-62.
6. Svarstad BL, Lipton HL. Informing parents about mental re- tardation: a study of professional communication and parent acceptance. Soc Sci Med 1977;11:641-5.
7. Lynch EC, Staloch NH. Parental perceptions of physicians' communication in the informing process. Merit Retard 1988;26:77-81.
8. Springer A, Steele MW. Effects of physicians' counseling on rearing of Down syndrome children. American Journal of Mental Deficiency 1980;85:1-5.
9. Lipton HL, Svarstad B. Sources of variation in clinicians' communication to parents about mental retardation. Ameri- can Journal of Mental Deficiency 1977;82:155-61.
10. McDonald AC, Carson KL, Palmer D J, Slay T. Physicians' diagnostic information to parents of handicapped neonates. Merit Retard 1980;20:12-4.
11. Wolraich ML, Albanese M, Reiter-Thayer S, Barratt W. Teaching pediatric residents to provide emotion-ladened in- formation. Journal of Medical Education 1981;56:438- 40.
12. Wolraich ML, Albanese M, Reiter-Thayer S, Barratt W. Factors affecting physician communication and parent-physi- cian dialogues. Journal of Medical Education 1982;57:631- 25.
BOUND VOLUMES AVAILABLE TO SUBSCRIBERS
Bound volumes of the 1992 issues of THE JOURNAL OF PEDIATRICS are available to subscribers (only) from the Publisher, at a cost of $58.00 for domestic, $78.06 for Canadian, and $74.00 for international subscribers, for Vol. 120 (January-June) and Vol. 121 (July-December), shipping charges included. Each bound volume contains subject and author indexes, and all advertising is removed. Copies are shipped within 60 days after publication of the last issue in the volume. The binding is durable buckram, with the Journal name, volume number, and year stamped in gold on the spine. Ph'yment must accompany all orders. Contact Mosby-Year Book, Inc., Subscrip- tion Services, 1 t830 Westline Industrial Dr., St. Louis, MO 63146-3318, USA/800-325-4177, ext. 4351, or 314-453-4351.
Subscriptions must be in force to qualify. Bound volumes are not available in place of a regular Journal subscription.