common neck swellings m k alam almaarefa college
TRANSCRIPT

COMMONCOMMONNECK SWELLINGSNECK SWELLINGS
M K ALAMM K ALAM
ALMAAREFA COLLEGEALMAAREFA COLLEGE
ILOsILOs
At the end of this presentation students will be able to: Describe the triangles and the lymph node distribution in
the neck. Name common neck swellings according to its location in
the triangles. Outline in brief the infection, stone disease and tumors of
salivary glands. Describe aetiology, clinical presentation, investigations and
management of lymph adenopathies. Name the congenital neck swellings, its clinical features and
management. Describe the presenting feature, investigation and
management of carotid body tumor.

Neck SwellingsNeck Swellings Often a diagnostic challengeOften a diagnostic challenge
Anatomy of the neckAnatomy of the neck
History & examinationHistory & examination
InvestigationsInvestigations


HistoryHistory LocalLocal:: Onset Onset DurationDuration PainPain Difficulty in swallowing/ masticationDifficulty in swallowing/ mastication Dyspnea/ nasal obstructionDyspnea/ nasal obstruction Change of voiceChange of voice
SystemicSystemic:: Weight loss Weight loss Night sweatingNight sweating FeverFever
PMHPMH:: Surgery, liver disease, smoking etc Surgery, liver disease, smoking etc
Family historyFamily history: MTC: MTC
ExaminationExamination
LocalLocal: Solitary/ multiple: Solitary/ multiple
Solid/ cysticSolid/ cystic
Effect of swallowing/ tongue protrusionEffect of swallowing/ tongue protrusion
Complete exam: head/neck/ oral and Complete exam: head/neck/ oral and upper aero-digestive tractupper aero-digestive tract
Systemic examinationSystemic examination::

InvestigationsInvestigations
CBC, Serology, TuberculinCBC, Serology, Tuberculin
CXR, U/S, CT scan, MRI, Angio.CXR, U/S, CT scan, MRI, Angio.
FNACFNAC
Laryngoscopy, EndoscopyLaryngoscopy, Endoscopy
Open biopsyOpen biopsy

Common Neck SwellingsCommon Neck Swellings
CongenitalCongenital
Vascular/ lymphatic malformation- Vascular/ lymphatic malformation- Cystic hygromaCystic hygroma
Branchial apparatus abnormality- Branchial apparatus abnormality- Branchial cystBranchial cyst
Thyroglossal cystThyroglossal cyst
Epidermoid cystEpidermoid cyst
Dermoid cystDermoid cyst
Cervical ribCervical rib
Common Neck SwellingsCommon Neck Swellings
AcquiredAcquired
Inflammatory:Inflammatory: Acute lymphadenitis Acute lymphadenitis ( bacterial, viral)( bacterial, viral) Granulamatous- Granulamatous- TBTB, Sarcoidosis, Sarcoidosis Salivary gland infections- viral, bacterialSalivary gland infections- viral, bacterial
Traumatic:Traumatic: HematomaHematoma PseudoaneusysmPseudoaneusysm

Common Neck SwellingsCommon Neck Swellings
AcquiredAcquired
Non-neoplasticNon-neoplastic SiallithiasisSiallithiasis GoitreGoitre AneurysmAneurysm Neoplasms:Neoplasms: Benign- Benign- salivarysalivary, thyroid, , thyroid,
fibroma, fibroma, carotid body tumourcarotid body tumour Malignant- Malignant- salivarysalivary, thyroid, lymphoma, , thyroid, lymphoma,
sarcoma, sarcoma, secondary depositssecondary deposits

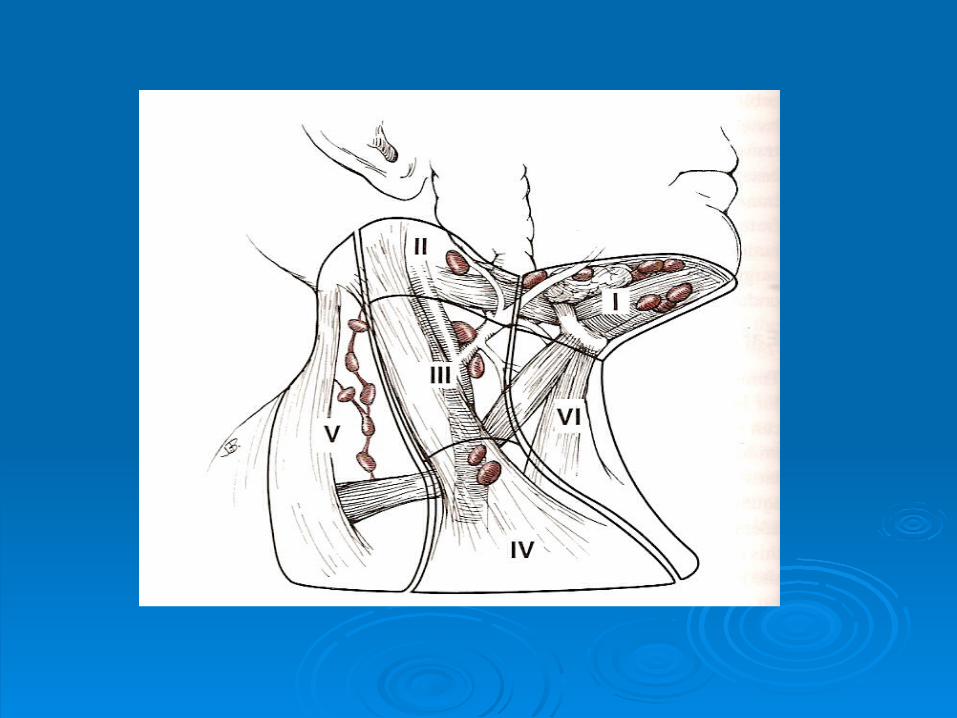
Location of common neck swellings
• Mid-line: Dermoid cyst, thyroglossal cyst
• Anterior triangle: Thyroid, lymph nodes, branchial
cyst, carotid body tumour, submandibular salivary gland
enlargement
• Posterior triangle: Lymph nodes, cystic hygroma
lymphadenopathy
• Throat infection: Upper deep cervical, usually discrete, size 1-2 cm, mildly tender, inflamed tonsil
• Tuberculous: Upper & middle cervical, discrete or matted, mildly tender, firm to cystic, overlying skin- normal temp., purplish or normal color
• Primary neoplasms: Ant./post. triangles, smooth, discrete, non-tender, rubbery, not fixed
• Metastatic: Discrete, hard, non-tender, tethered,
Acute lymphadenitisAcute lymphadenitis
Usually follow tonsillitis, throat infection, Usually follow tonsillitis, throat infection,
scalp or face infection, dental abscess scalp or face infection, dental abscess
Lymph node enlarged and tenderLymph node enlarged and tender
Pyrexia, general malaisePyrexia, general malaise
Antibiotic and treatment of primary sourceAntibiotic and treatment of primary source

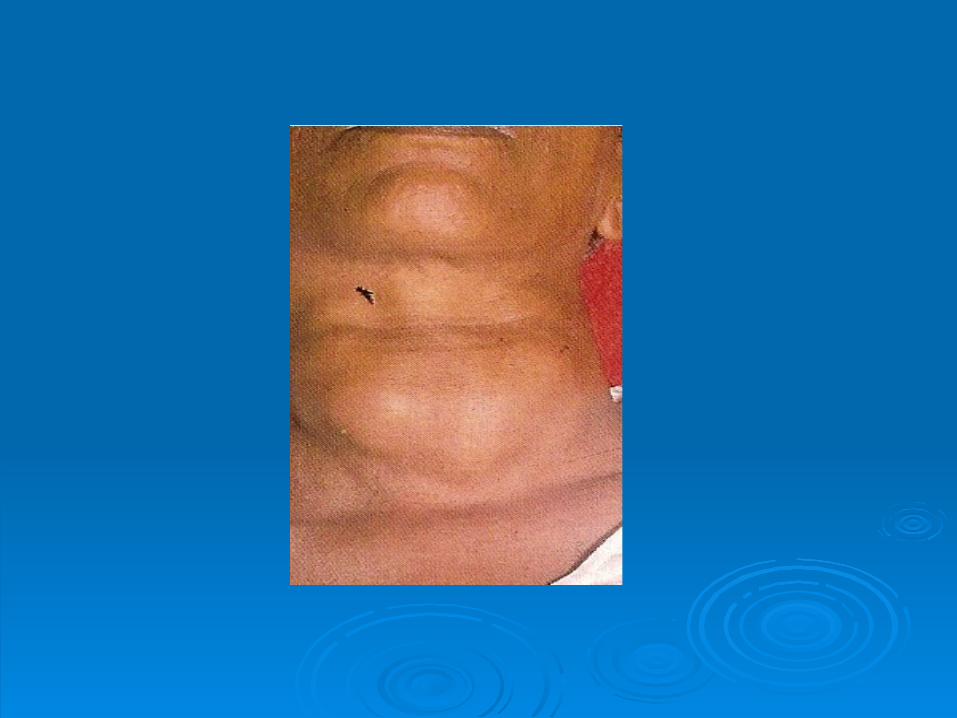
TB lymphadenitisTB lymphadenitis
Human & bovine TB bacillusHuman & bovine TB bacillus
Upper deep cervical groups commonly affectedUpper deep cervical groups commonly affected
Painless, initially firm swelling, later may become soft (cold Painless, initially firm swelling, later may become soft (cold
abscess), matted, discharging sinusabscess), matted, discharging sinus
Evening temperature, night sweats, weight loss, anorexiaEvening temperature, night sweats, weight loss, anorexia
Diagnosis: FNA, aspirate for AFB, culture, PCR, biopsyDiagnosis: FNA, aspirate for AFB, culture, PCR, biopsy
Treatment: Anti-tuberculous drugsTreatment: Anti-tuberculous drugs



Primary malignant tumours of lymph nodesPrimary malignant tumours of lymph nodes
Hodgkin's disease, Hodgkin's disease,
lymphosarcomalymphosarcoma


Secondary deposits in lymph Secondary deposits in lymph nodesnodes
Primary tumour sitePrimary tumour site: Nasopharyngeal area, : Nasopharyngeal area,
tongue, oral cavity, thyroidtongue, oral cavity, thyroid
Affected lymph nodes are hard and fixedAffected lymph nodes are hard and fixed
Diagnosis: Diagnosis: Assessment of primary, FNA & biopsyAssessment of primary, FNA & biopsy
Treatment: Block dissection of the neckTreatment: Block dissection of the neck



Inflammatory disorders (Salivary)
Viral infections (Mumps)
• Common among children.• Usually affects parotid, submandibular
occasionally• Painful swelling, fever and headache. • Resolves in 5-10 days.• Treatment- symptomatic
Bacterial infections (Salivary)
• Common in elderly, also seen in fit and young
• Dehydration results in ascending infection via parotid duct
• Painful, more on eating/ drinking,
• tender parotid swelling with fever and malaise
• Pus exuding from duct papilla
• Staph. aureus, Strep. viridans
• Early cases: antibiotics, oral hygiene
• Late cases: abscess drainage

Calcular disease (Sialothiasis)• Painful swelling of submandibular gland during
eating
• Swelling resolves/ reduces 1-2 hours after meals
• Enlarged submandibular gland on bimanual examination
• Stone in the duct- palpable in the floor of mouth
• Treatment: Stone in the duct- extraction by direct incision over the
duct Stone in the gland- excision of the gland
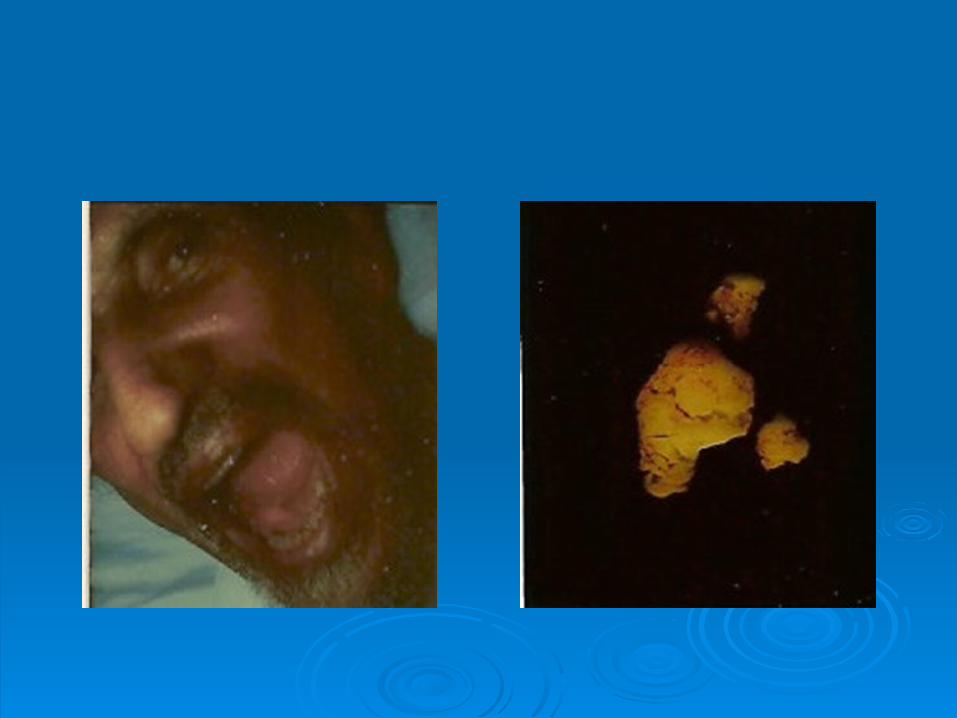
Salivary GlandsSalivary Glands
Neoplasms (Benign)
Pleomorphic adenoma
Warthins tumour
Oncocytoma,
Basal cell adenoma,
Intraductal papilloma

Pleomorphic AdenomaPleomorphic Adenoma
• Most common neoplasm, parotid most common site
• M=F, 3-5 decade
• Slow growing, painless mass/ mild discomfort
• Risk of malignant change- 1.5% in 5 years
• FNA- most helpful
• CT, MRI rarely needed
• Treatment: Superficial parotidectomy / Total parotidectomy
Enucleation not recommended Submandibular: Total gland excision



Salivary glandsSalivary glands
Neoplasms (Malignant) Mucoepidermoid carcinoma* Acinic cell carcinoma Adenoid cystic carcinoma Basal cell carcinoma Low grade adenocarcinoma Mucinous adenocarcinoma Malignant pleomorphic tumour Lymphoma Secondary deposits

Malignant tumoursMalignant tumours
• Swelling of the affected gland
• Rapid growth
• Painful
• Lymphadenopathy
• Fixity, skin attachment
• Nerve palsy, paresthesia
• No particular feature of histological subtype

Malignant tumoursMalignant tumours
• FNA
• CT, MRI
• Staging:
T1: Tumour less than 2 cm
T2: Tumour 2-4 cm T3: Tumour more than 4 cm T4: Any size with evidence of extension

Treatment- malignant salivary tumours
• Parotid: En-bloc excision. Preserve facial if not involved
• Submandibular/Sublingual: En-bloc excision• Post-op radiotherapy: High grade, local extension, perineural extension
• Neck dissection: High grade mucoepidemoid tumours
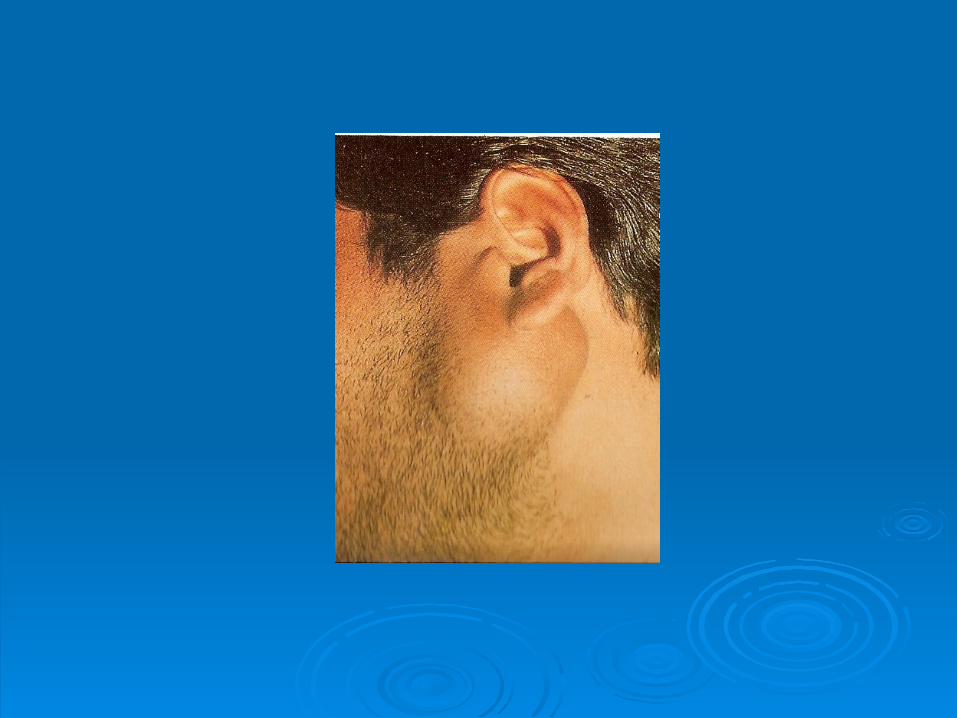
Thyroglossal cystThyroglossal cyst
• Persistent of part of thyroglossal ductPersistent of part of thyroglossal duct
• Midline swelling just above thyroid cartilageMidline swelling just above thyroid cartilage
• Moves up on tongue protrusionMoves up on tongue protrusion
• Cyst contains mucoid materialCyst contains mucoid material
• Cyst is in intimate relation with hyoid boneCyst is in intimate relation with hyoid bone
• Surgical excision (Sistrunk operation)- Excising whole Surgical excision (Sistrunk operation)- Excising whole
cyst, wedge of hyoid and duct up to the base of tonguecyst, wedge of hyoid and duct up to the base of tongue


Branchial cyst
• Remnant of 2nd branchial cleft
• Painless
• Site: Behind the anterior edge of upper 1/3rd of
sternomastoid muscle bulging forward
• Ovoid shape, size 5-10 cm, smooth surface
• Cystic (fluctuates)
• Transillumination: opaque
• Tender and red if infected
• Treatment; Surgical excision



Carotid body tumour
• Tumour of chemoreceptor tissue in carotid body• Painless, slow growing • Site: Anterior triangle, within carotid bifurcation, at the level
of hyoid bone• Spherical, non-tender, firm/hard• Pulsatile, moving in horizontal plane• Investigation: CT (splaying of carotid vessels), MRI, Investigation: CT (splaying of carotid vessels), MRI,
angiography angiography• No FNANo FNA• Treatment: Surgical excisionTreatment: Surgical excision


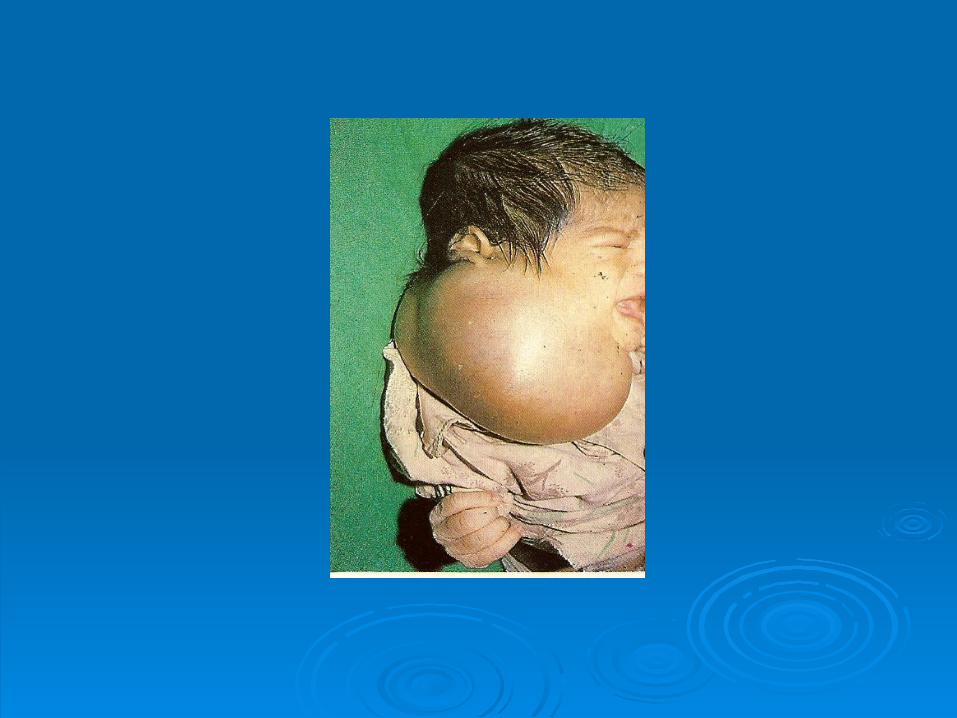
Cystic hygroma
• Collection of lymphatic sacs• Congenital• From birth to within few years• Site: base of the neck in post. triangle• Subcutaneous• Variable size• Soft, cystic , brilliantly trans illuminates