collaborating for outcomes - university of alabama at birmingham · collaborating for outcomes shae...
TRANSCRIPT
2/23/2015
1
Collaborating for Outcomes
Shae Rogers, RN BSNAssistant Nurse Manager, Labor and Delivery
UAB Hospital
Laura Money, RN MSNNurse Manager, Labor and Delivery
UAB Hospital
Collaborating for Outcomes
DO NOT have a financial interest/arrangement or affiliation with any organi ations that could be perceivedany organizations that could be perceived as a real or apparent conflict of interest in
the context of the subject of this presentation
Educational Objectives
• Discuss contributing factors to medical errors in the OB setting
• Review best practices to optimize team ll b i / i i i i i
Page 3
collaboration/communication to minimize errors in the OB area
2/23/2015
2
Medical Errors
Frequency of Hospital associated events1. Adverse drug events2. Catheter‐associated urinary tract infection3. Central line‐associated bloodstream infection4 Injury from falls and immobility
Page 4
4. Injury from falls and immobility5. Obstetrical adverse events6. Pressure ulcers (bed sores)7. Surgical site infections8. Venous thrombosis (blood clots)9. Ventilator‐associated pneumonia
Distribution of RN Legal Cases by Practice
Page 5
Most Common OB Litigations
In a 2005 Survey conducted by ACOG related to OB claims:2,564 claims were included in the survey
29% were for neurologically impaired infant21% cases noted FM as the primary concern
Page 6
% cases noted FM as the primary concern14% were for stillbirth or neonatal death15% were for shoulder dystocia/brachial plexus injury
Over 90% of all litigations noted an associated factor was electronic fetal monitoring

2/23/2015
3
Most Common cause of Errors
ACOG, AWHONN, TJC, AHRQ (Agency for Health Care Research and Quality), HHS (US Department of Health and Human Services, AACN (Association of Critical Care Nurses) ETC…… All Agree
Page 7
g
The #1 cause of medical errors is …….
COMMUNICATION
Fetal Monitoring
We are not going to talk:
Accel
Decel
Base Line
Page 8
Category 1
Category 2
Category 3
Interpretation is no longer the issue!
How we communicate better at UAB in 2015!
Interdisciplinary Rounds
High Risk Planning
I t di i li Si l ti
Page 9
Interdisciplinary Simulations

2/23/2015
4
Interdisciplinary Rounds
Interdisciplinary meeting at the start of every shift to discuss current patients and scheduled cases (20 minute maximum time frame)
Attended by Faculty Physicians (OB and Anesthesia), residents, nursing representatives from various areas (L&D, OR, RNICU, triage)
Page 10
, , g )
Plans of care for each patient is reviewed, questions and concerns are discussed
Admissions and OR schedule is reviewed and a final timeline agreed upon by the team
Patient throughput is reviewed and any challenges proactively managed
Challenges
Identify Key people needed
Attendance‐ finding an appropriate time
Communicating the start of the meeting to all team members
Page 11
members
Collaborative planning not teaching meeting
Keeping the meeting to less than 20 minutes
Outcomes
Fosters a team approach to all plans of care
Ensures continuity of care
Proactively addresses concerns or conflicts in the plan of care
Page 12
Adjusts the Admission and OR schedule to promote safe patient care and patient satisfaction
Allows “down stream” units to proactively plan and coordinate patient flow and staffing

2/23/2015
5
Case Study
Patient with Oxytocin infusing 23 hrs and AROM 15 hrs
Patient with no pain control after epidural and multiple doses of IV medications
Page 13
Patient with no epidural and NRFHT’s
Multiple NICU admissions
1 LR open with non laboring patients in rooms
Tools ‐ AgendaAGENDA AND PROCEDURES FOR DAILY MULTIDISCIPLINARY HANDOFF The L&D ANM with broadcast announcing the “Rounding Team Meeting” at 0715 and 1915 Monday‐Friday and at 0800 and 2000 on Saturday and Sunday. 1. Introduction of each team member participating by name not just title. 2. Start with review of patients on the L&D Board
The handoff on each patient should brief, formal, focused and professional consisting of:
Patient room number, name, age, gestational age
Current diagnoses and issues including fetal status assessment
Discussion of labor progress and identification of possible need for cesarean
Obstetric management plan and anesthesia management plan; discussion of nursing
Page 14
Obstetric management plan and anesthesia management plan; discussion of nursing concerns
Opportunity for questions 3. Review the OR schedule briefly to recap the 0700 meeting and confirm workflow and order of
cases
At the evening meeting, this step can be omitted if no cases waiting for the OR. 4. Review patients in the MEU and briefly review plan of care 5. Review status, location and plan of care for any off‐service, antepartum OB patients 6. Review status and plan of care for any patients on HRO likely to be transferred to L&D or
potential complicated C/S 7. Discuss any potential patient throughput issues on the MBU, HRO and L&D This meeting should be completed within 10‐15 minutes of its initiation.
Tools ‐ Sign in Sheet
Page 15

2/23/2015
6
Team‐ Picture
Page 16
Interdispinary Rounds- how it really works
Page 17
High Risk Patient Planning
Monthly meeting to discuss pregnant patients with varying cardiac diseases
Attended by Cardiology, MFM, Anesthesia, and Nursing
Page 18
Patients presented and POC proactively discussed and changed based on recommendations from all disciplines throughout the continuum of prenatal care

2/23/2015
7
Challenges
Knowledge deficit by all team members based on specialty
Consulting teams with a lack of opportunity for care collaboration based on specialty
Page 19
p y
Limited knowledge by the inpatient staff of plans of care related to non OB complications
Trust in team members to provide expected care
Outcomes Increased knowledge by nursing staff for cardiac complications (cardiac staff provided educational inservices, memo, references)
Teams now plan care after discussing interrelated complications (ie pain management, coagulation plans, pacemaker management in the OR, monitoring, IV drips, etc)
Page 20
etc)
All care team members; prenatal providers, cardiac team, and L&D inpatient staff are proactively aware of the on going plan made by the team as the patient progresses in her pregnancy
Knowledge based on each discipline's specialty is shared and discussed in the meeting building trust in competence throughout the team
Case Study
Induction
3 k
PATIENT INFO
LT Age: 24 DOB: X/X/XXXX MRN: XXXXXX EDD: 10/28/14 GP: G1P0 Cards/OB: Cantu, Colvin
DIAGNOSES
1. ccTGA, VSD, Coarct 2. PA band, Coa repair 1mo 3. VSD closure 2yrs 4. Systemic tricuspid valve replacement 6yrs 5. Chronic Coumadin --currently on 4mg daily (INR 2.99 on 8/14)
ECHOCARDIOGRAM
Echo 6/24/2013: 1. No Coa or VSD 2. TVR: good fxn (mn gradient 10) 3. Good ventricular fxn 4. Nl estimated PA pressures Echo 5/12/2014: no sig change 1. Mild flow acceleration across coarct repair (12mmHg gradient) Echo 7/23/2014: 1. Good bi-V function 2. TVR: mn gradient 12-17
MRI/OTHER
AntiCoagulation Plan: LMWH with tight levels --> transition to Coumadin at 14 wks --> transition back to LMWH at 34-35 wks --> IOL at 36-37 wks with transition to UFH on L&D until cervix 6+cm then discontinue -- resume 4-6 hours after vaginal delivery. For C-section, resume UFH 12 hours post delivery.
DIAGNOSTICS
Fetal Echo 5/12, 7/14, 7/23: normal Targeted US 6/2: normal
APPOINTMENTS
1. Hospital: UAB 2. Unit: L&D 3. Mode: Vaginal 4. Monitoring: Tele 5. Other: If pt desires epidural, may be done w nl PTT, UFH off, & pt in active labor -- pull PRIOR to restarting UFH
Page 21
37 weeks
Medication recommendations
Challenges
Labs
Unexpected diagnosis
Collaboration
Outcomes
Delivery
Follow up
2/23/2015
8
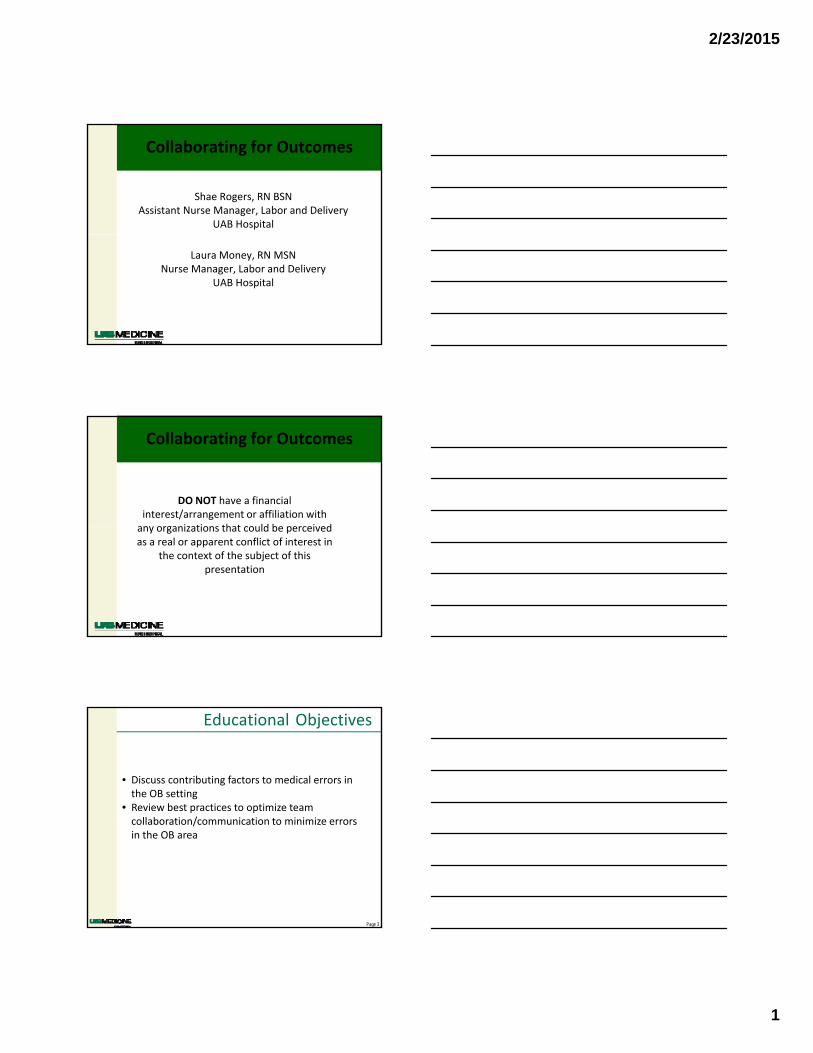
Tools – planning sheetPatient Info Diagnoses Echocardiogram MRI/Other Other
diagnostics PLAN Appointments
Miscellaneous
BC Age: 24 DOB: 1/19/1990 MRN: XXXXXXX EDD: 1/9/15 GP: G1P0 Cards/OB: Colvin, Comp
1. Tetralogy of Fallot s/p repair and PV replacement 2. Non‐sustained VT with + EPS s/p AICD
Echo 6/3/2014: 1. Very mild PS and PI 2. Good RV function 3. Normal LV function (EF 60%) Echo 12/15/2014: 1. LVEF 50%
ICD Information: Model: Boston Scientific Incepta Tachycardia Detect: VT: 165 bpm ‐‐ No therapy VT: 190 bpm ‐‐ Burst pacing VF: 210 bpm Pacing Mode: DDD. Lower rate 50 bpm NOTE: Magnet will disable shock and anti‐tachycardia pacing therapies
GXT 6/23: normal Fetal Echo 8/11: no defect seen Targeted U/S 8/11: no defect seen Fetal Echo 10/6: wnl AICD chk 12/15: 2 brief episodes of Sinus tach
1. Hospital: UAB 2. Unit: L&D 3. Mode: 4. Monitoring: Tele ‐‐ In the event of C‐section, place magnet over ICD
1. Continue MFM care ‐‐ last seen on 12/15 2. Colvin f/u 2‐3 months after delivery
CC Age: 28 DOB: 12/27/85 MRN: XXXXXXX EDD: 1/16/15 GP: G3A1P1 Cards/OB: Cribbs, MFM
1. Endocarditis of MV (2006) 2. MVR (2006) 3. Drug, EtOH, Tob abuse now on Methadone 4. Hx Csection 9/22/10 5. Endocarditis (2011) s/p IV abx x 6wks
Echo 8/18/2011: 1. Nl biV function 2. MVR with 8mmHg gradient (stable) 3. No MR 4. 7x3mm mobile mass on ventricular side of valve Echo 10/27/2014:
AntiCoagulation Plan: Previously on Warfarin 7.5mg ‐‐ stopped at 5wks. Continue LMWH until delivery due to poor compliance (unlikely to follow multiple daily dosing with heparin in 3rd trimester). Admit to HRO prior to C‐section to keep as inpatient Will
Anti‐Xa 11/14: 0.7 (Peak) dose increased from 60 to 65mg BID
1. Hospital: UAB 2. Unit: L&D 3. Mode: repeat CS 4. Monitoring: Tele 5. Other: Pt desires BTL at Csection 6
1. Continue MFM care ‐‐ last seen on 12/12 2. Cribbs f/u 12/19 3. OB Anesthesia consult done on 11/26
Page 22
abx x 6wks 6. NON‐COMPLIANCE 7. Clot on mechanical mitral valve
Echo 10/27/2014: 1. Nl function 2. Mitral stenosis (Peak and mean 20 and 8.5mmHg) 3. Thrombis 1.8 x 2.4mm on atrial aspect of MV prolapses into LV Echo 11/26/2014: 1. MV thrombis smaller and gradient decreased to peak 13mmHg
section to keep as inpatient. Will check anti‐Xa upon admission to confirm patient has been using Lovenox. If anti‐Xa negative, proceed with C‐section, otherwise, wait until 24 hours after last dose to deliver. Start heparin gtt (without bolus) 12 hours after C‐section unless bleeding complications. Transition to Coumadin after delivery AS AN INPATIENT.
Csection 6. Deliver at ~36 wks EGA ‐‐ admit Sunday, 12/21/14 for elective repeat CS and BTL on 12/22/14
JD Age: 21 DOB: 2/18/1993 MRN: XXXXXX EDD: Late Jan, '15 GP: G2A1P1 Cards: McElderry, MFM
1. Cardiomyopathy LVEF 20% (?PPCM) 2. Recurrent syncope with frequent ventricular ectopy ‐‐ Now on beta‐blocker & life‐vest (ICD after pregnancy) 3. Hx Tob and THC abuse ‐ quit early this pregnancy 4. Admitted to UAB on 11/12/14 with progressive SOB
Echo 8/2014: LVEF 15% Echo 9/21/2014: 1. Borderline dilated LV with LVEF 40‐45% 2. Mild to moderate MR Echo 11/11/2014: LVEF 40‐45%
None EEG 9/23: nl 1. Hospital: UAB 2. Unit: L&D 3. Mode: vaginal 4. Monitoring: Tele, A‐line 5. Other: Birth control undecided; Pt desires BTL
1. MFM and Cards (EP) f/u ‐‐ last seen on 12/3 and next for 1/16/15 2. Needs OB Anesthesia consult ‐‐ EP notified but no appt made yet ‐‐ was to be sent to MEU on 12/3 for OB Anesthesia consult
High Risk Planning Team‐ Pic
Page 23
Page 24

2/23/2015
9
6 Months Later
Page 25
Interdisciplinary Scenarios
Developed a team approach to simulation training
Conduct interdisciplinary OB simulations on the unit on a regular basis
Page 26
Implemented consistent clinical practice and communication processes for OB emergency
Challenges
Timing
Developing consistent communication and clinical practices for nurses and physicians
Page 27
Clear focus for each discipline’s learning needs
Respect and safety in a learning environment across multiple disciplines
Appropriate and timely debrief

2/23/2015
10
Outcomes
More confident staff
More trusting relationship between disciplines
Improved understanding of each staff members role
Page 28
role
Improved documentation, management, and outcomes especially for Shoulder Dystocia
Fetal Monitoring‐ improved communication regarding those category 2 tracings
Case Study
Simulation: Shoulder Dystocia
RN staff were able to clearly communicate and demonstrate the use of appropriate interventions
RNs and MDs recognized the importance of continuous communication‐ improved communication related to times and manuevers
Page 29
and manuevers
RNs and MDs became aware of the need to educate and reassure family members
Practice makes perfect (or at least better)! Scenarios have given staff members more confidence in providing safe patient care during real situations
Simulation toolOB simulation SHOULDER DYSTOCIA LEARNERS: OB physicians / ANESTHESIA physicians / NURSING STAFF
Prebrief: 32 yowf,PARA 3012, 38 wk 3 days SROM clear fluid, DM Class R, EFW 4000gm, Patient weight 285#, 5' tall
Epiidural placed at 5 cm. Prolonged stage one labor, patient labored down for 1 1/2 hours
MD in to evaluate readiness to begin pushing 2 hours ago. progress,C/C/+3, FHT's 150's shows mild to moderate variables, ctx q 2‐3 min
Patient states " I'm tired! I give up! The baby's head comes out and then goes back! I just want a C/S!"
ASSESSMENT RN INTERVENTIONS INTERVENTIONS‐RESIDENT PROFESSIONALISM
RISK FACTORS
Delivery imminent use HELPER neumonic Recognition of Shoulder Dystocia Leader Established
Medical History
H Call for help
McRoberts Maneuver Team communications
Diabetes E Evaluate for episiotomy SP pressure Chain of Command implemented
Fetal Macrosomia L Legs (MacRoberts Maneuver) Confirmation of pt. not pusing 1st year notify upper level
Previous shoulder dystocia TIME BEGINS WHEN PATIENT BEGINS PUSHING Bladder Drained Anesthesia notified timely
Abnormal pelvic anatomy START TIMER (CALL OUT EACH MINUTE TO 5 MIN) Rotational Maneuvers Attending notified
Short stature P Suprapubic (not fundal) pressure to disengage Episiotomy
Page 30
Short stature P Suprapubic (not fundal) pressure to disengage Episiotomy
Protracted Labor the anterior shoulder‐confirm the pt. is not pushing Posterior Arm Delivery
Turtle Sign E Enter rotational maneuvers Aware of elapsed time‐5 min limit
Pushing 2 hours R Remove posterior arm
MONITOR FETAL HEARTRATE‐CALL OUT TO TEAM
RECOGNITION/ PLANNING
Stools in place IV lines are labeled and free/ prep trasnport to the OR
Notify ANM
Prepare for vaginal delivery
Prepare for Operative delivery
COMMUNICATION COMMUNICATION COMMUNICATION COMMUNICATION
SBAR to team SBAR to Interdisiplinary team‐include OR team/Peds Announcemen to IDT of Shoulder RN establish Team (call for help)
Notify MD Patient education‐support‐encouragement Dystocia SBAR Interdisiplinary team
Notify OR team Family informed during procedure Patient and family informed of Patient education
Notify Peds procedures/maneuvers Family support‐ empathy
2/23/2015
11
Simulation tool
Scenerio Assessment Coordinator / Participant Notes: Resources Required for simulation
Assessment complete Yes / No Person to act as patient
Risk factors Patient gown
noted? Yes / No IV fluids‐plain
communicated? Yes / No IV fluids‐Pitocin/postpartum
Interventions IV tubing
implemented Yes / No Tape to place IV on patient arm
correct Yes / No Hemipelvis with fetus
missed interventions Yes / No if yes which one(s) Fetal Monitor
Communication Fetal Monitor tracing
SBAR Yes / No Stools in room
Team Yes / No Pillows/extra linen for staging
close loop Yes / No
Profesionlism Yes / No
Page 31
Scenrio Debrief
Facts of the case breifly reviewed by the sim coordinators
Participants please provide the following information
How did you feel during the scenerio?
What went well?
What do you think we could do better
Was this simulation helpful yes / No
Will this simulation change anything about your previous practice? Yes / No
What?
Collaborating for Outcomes- It Makes a Difference
Page 32
Kachalia A, Kaufman SR, Boothman R, Anderson S, Welch K, Saint S, et al. Liability claims and costs before and after implementation of a medical error disclosure program. Ann Intern Med 2010;153:213–21.
AHRQ's Patient Safety Initiative: Building Foundations, Reducing Risk. December 2003. Agency for Healthcare Research and Quality, Rockville, MD. http://archive.ahrq.gov/research/findings/final-reports/pscongrpt/psini2.html
Page 33
reports/pscongrpt/psini2.html
Cathy Tokarski. Better Communication Needed to Reduce Medical Errors. Medscape. Jan 27, 2005Communication, Teams, and Medical Mistakes. Moorman, DW. Ann Surg. Feb 2007; 245(2): 173–175.
20 tips to Help Prevent Medical Errors: Patient Fact Sheet. December 2014. Agency for Health Research and Quality. Rockville MD. http:/www.ahrq.gov/patients-consumers/care-planning/errors/ 20tips/index.html
