cognitiveoutcomes ofdifferentsurgicalapproaches ... · assessment and how neuropsychological test...
TRANSCRIPT
do
i:10.
1684
/ep
d.2
013.
0587
E
CCDUS5<
Review articleEpileptic Disord 2013; 15 (3): 221-39
Cognitive outcomesof different surgical approachesin temporal lobe epilepsy
Christoph HelmstaedterDepartment of Epileptology, University of Bonn, Germany
Received March 22, 2013; Accepted June 12, 2013
ABSTRACT – Epilepsy surgery is a successful treatment option forpharmacoresistant focal symptomatic epilepsies. However, cognitiveimpairment is very common in epilepsy patients and may be negativelyor positively affected by surgery. Amidst the long-standing discussion ofwhether a particular surgical approach for temporal lobe epilepsy patientsmay be superior with regards to seizure control, a recent meta-analysisindicated that this is the case for more extended resections. Larger tem-poral lobe resections, however, raise concerns that more unaffected andfunctional tissues may be involved, thus causing worse cognitive outcome.This review is based on published reports collected over a long period,with changing diagnostics and surgical methods, and focuses mainly onthe experiences of one epilepsy centre. The review highlights the effectsof standard versus selective surgery, the different surgical approaches inselective surgery, determinants other than surgery which may affect cog-nitive outcome, and the methodologically-important question of outcomeassessment and how neuropsychological test selection may bias the result.Overall, from a neuropsychological point of view, individual and selectivesurgery is preferred in which the aim is to achieve seizure control with min-imal effect on the functional integrity of tissues or fibre tracts. Cognition
ryday life and this should be kept inrgery is preferred.
selective surgery, standard surgery,
with temporal lobe epilepsy (TLE),successful seizure control wasachieved in 58% operated versus8% medically-treated patients in
is important for the functions of evemind, irrespective of which kind of su
Key words: temporal lobe epilepsy,outcome, cognition, memory
The cognitive outcomeof temporal lobe epilepsysurgery
pileptic Disord, Vol. 15, No. 3, September 2013 221
orrespondence:hristoph Helmstaedterepartment of Epileptology,niversity of Bonn,igmund Freud Str 25,3105 Bonn, [email protected]>
Epilepsy surgery represents a verysuccessful treatment option forpatients with focal symptomaticepilepsies. By comparing surgicalversus conservative medical treat-ment in 80 randomised patients
a 12-month observation period(Wiebe et al., 2001). This corres-ponds to what was found in ourown non-randomised longitudinal2-10-year follow-up study of 102medically- (12% seizure-free) versus147 surgically- (63% seizure-free)

2
C
tcabeSesasemtTfew1iarmohmterdlmwsfTml(avgctpwacl4castwra
Twam(sRsgidrsfi(rtt2wStrlnfmpifretb(
Da
Toma(ccer
. Helmstaedter
reated patients with TLE (Helmstaedter et al., 2003). Inonclusion, and without any further characterisation,bout two thirds of operated patients with TLE mayecome (permanently) seizure-free (Tellez-Zentenot al., 2010).eizure control is clearly the primary aim ofpilepsy surgery. Successful seizure control under-tandingly reduces behavioural and mood problemsnd improves overall quality of life. However, leavingeizure control aside, brain surgery can have negativeffects on cognition and behaviour, resulting in impair-ents which quantitatively and qualitatively exceed
hose observed before surgery (Helmstaedter, 2004).able 1 provides a comprehensive overview of therequency of cognitive deficits and changes in postop-rative performance in a large cohort of 732 patientsith TLE, who received surgery in Bonn between
989 and 2007 (Helmstaedter et al., 2007). Accord-ng to categorical test results (using a point systemccording to standard deviations, whereby 0 to 4epresents severely impaired to above average perfor-
ance, and 3 represents average performance), 78%f patients with chronic pharmacoresistant TLE alreadyad cognitive impairment (values <2) of either verbalemory, figural memory, or attention/executive func-
ions before surgery. Regarding the localisation of thepileptogenic focus in brain regions relevant to memo-y processing, the most commonly affected cognitiveomains in TLE are verbal and figural memory, fol-
owed by complications in language, attention, andotor and visuo-constructive functions. Consistentith the literature, lateralisation-dependent results are
een regarding verbal memory impairment and a morerequent atypical language dominance in left sidedLE, and with more frequent impairments in figuralemory and attention in right-sided TLE. In addition to
ateralisation, factors such as the time of epilepsy onsetduring brain maturation or after), presence versusbsence and type of underlying lesion (e.g. neoplasticersus developmental), patient variables (such as age,ender, and education), and last, but not least, medi-ation and seizure situation differentially contributeo the cognitive capabilities observed in individualatients. One year after surgery, 65% of 732 patientsere completely seizure-free, i.e. they did not have
ny seizures or aura. By applying 90% reliability ofhange indices (RCI), individually significant gains andosses in the assessed domains were evident for 10-0% of the patients. According to table 1, major gains
22
oncern extratemporal non-memory functions. Lossesre prominent in memory, and here patients with left-ided temporal epilepsy are more frequently affectedhan those with right-sided temporal epilepsy. Patientsith left-sided temporal epilepsy also worsen with
egards to language functions which tend to improvefter right-sided surgery.
cFsmooH
he findings in this large cohort of patients fit wellith base-rate estimates of expected gains and losses
fter TL surgery which were published in a recenteta-study on cognitive outcomes after TL surgery
Sherman et al., 2011). Regarding 22 of 193 evaluatedtudies investigating temporal lobe surgery and takingCI or standardised regression-based (SRB) changecores into consideration, the pooled estimates ofains and losses for the assessed cognitive domains
ndicated a rate of 44% patients with verbal memoryecline after left-sided surgery, compared to 20% afteright-sided surgery. The gains for verbal memory werecarce; 7% (left side) versus 14% (right side). Losses ingural memory were not different between left-sided
15%) and right-sided (10%) surgery. The total averageate of decline in language (naming) was 34%. As inhe Bonn sample, benefits were identified for execu-ive functions after left-sided surgery (10% losses and7% gains); for right-sided surgery, the losses and gainsere 21% and 16%, respectively.ummarising the findings so far, TLE patients andhose with left TLE in particular, bear an increasedisk of cognitive decline in memory after temporalobe surgery. In some patients, improvement of cog-itive functions is possible. The role of seizure control
or the postoperative course of cognition is still aatter of debate. While Rebecca Rausch reported a
rogressive decline, independent of seizure outcome,n a long-term follow-up study, our own long termollow-up study indicated that further decline versusecovery depended on seizure control (Helmstaedtert al., 2003; Rausch et al., 2003). Recent evidence fromwo other long term follow-up studies indicates a sta-le course of memory from two years after surgery
Alpherts et al., 2006; Andersson-Roswall et al., 2010).
eterminants of cognitive outcomefter surgery
wo major factors determine the cognitive outcomef epilepsy and its treatment. The first and probablyost predictive factor is the “functionality” of brain
reas affected by epilepsy which are to be resectedChelune, 1995; Stroup et al., 2003). The second factor,losely connected to the question of “functionality”,oncerns the brain areas and functions not affected bypilepsy or surgery, referred to as the patient’s “mentaleserve capacity” (Helmstaedter, 1999). Mental reserve
Epileptic Disord, Vol. 15, No. 3, September 2013
apacities can help to compensate surgical defects.unctionality of the brain also appears to predict latereizure control (Helmstaedter, 2009). Seizure controlay be discussed as a third determinant of cognitive
utcome. Here, the principal idea is that of a releasef functions due to control of epileptic dysfunction.owever, up to now, there is only sparse evidence
E
Cognitive outcome and surgery in TLE
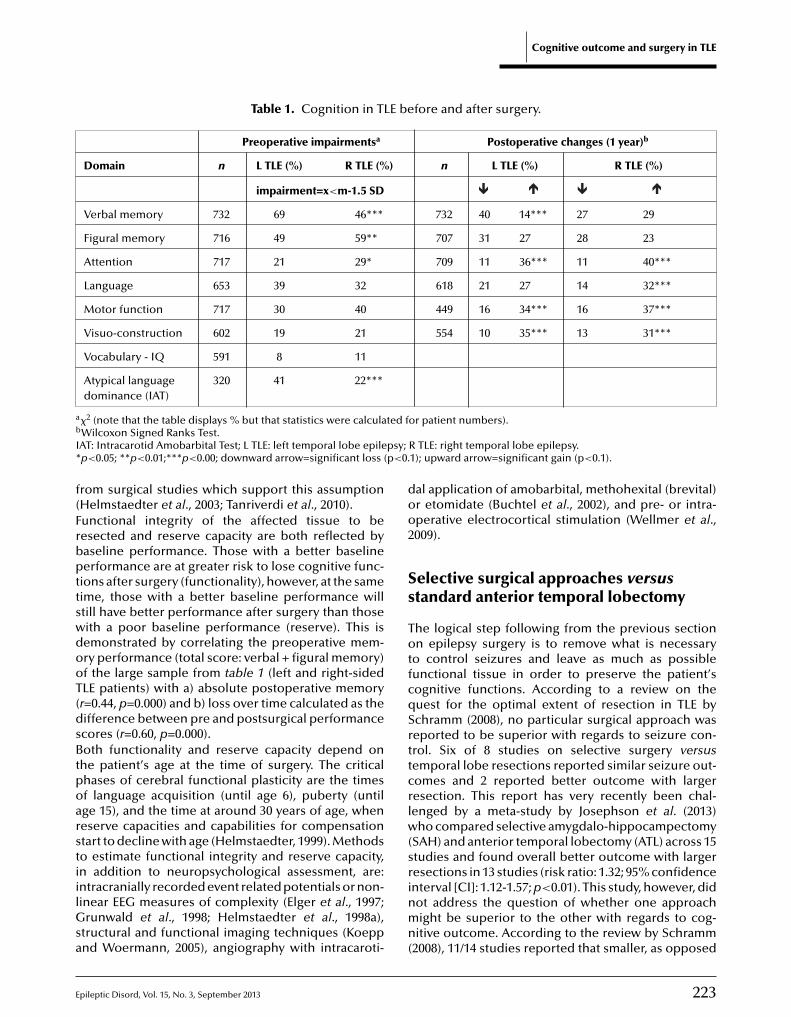
Table 1. Cognition in TLE before and after surgery.
Preoperative impairmentsa Postoperative changes (1 year)b
Domain n L TLE (%) R TLE (%) n L TLE (%) R TLE (%)
impairment=x<m-1.5 SD
Verbal memory 732 69 46*** 732 40 14*** 27 29
Figural memory 716 49 59** 707 31 27 28 23
Attention 717 21 29* 709 11 36*** 11 40***
Language 653 39 32 618 21 27 14 32***
Motor function 717 30 40 449 16 34*** 16 37***
Visuo-construction 602 19 21 554 10 35*** 13 31***
Vocabulary - IQ 591 8 11
Atypical language 320 41 22***
a ted fb
I psy;* p<0.
f(FrbpttswdooT(dsBtpoarstiilGsa
doo2
Ss
TotfcqSrttcrlw(
dominance (IAT)
�2 (note that the table displays % but that statistics were calculaWilcoxon Signed Ranks Test.AT: Intracarotid Amobarbital Test; L TLE: left temporal lobe epilep<0.05; **p<0.01;***p<0.00; downward arrow=significant loss (
rom surgical studies which support this assumptionHelmstaedter et al., 2003; Tanriverdi et al., 2010).unctional integrity of the affected tissue to beesected and reserve capacity are both reflected byaseline performance. Those with a better baselineerformance are at greater risk to lose cognitive func-
ions after surgery (functionality), however, at the sameime, those with a better baseline performance willtill have better performance after surgery than thoseith a poor baseline performance (reserve). This isemonstrated by correlating the preoperative mem-ry performance (total score: verbal + figural memory)f the large sample from table 1 (left and right-sidedLE patients) with a) absolute postoperative memoryr=0.44, p=0.000) and b) loss over time calculated as theifference between pre and postsurgical performancecores (r=0.60, p=0.000).oth functionality and reserve capacity depend on
he patient’s age at the time of surgery. The criticalhases of cerebral functional plasticity are the timesf language acquisition (until age 6), puberty (untilge 15), and the time at around 30 years of age, wheneserve capacities and capabilities for compensationtart to decline with age (Helmstaedter, 1999). Methods
pileptic Disord, Vol. 15, No. 3, September 2013
o estimate functional integrity and reserve capacity,n addition to neuropsychological assessment, are:ntracranially recorded event related potentials or non-inear EEG measures of complexity (Elger et al., 1997;
runwald et al., 1998; Helmstaedter et al., 1998a),tructural and functional imaging techniques (Koeppnd Woermann, 2005), angiography with intracaroti-
srinmn(
or patient numbers).
R TLE: right temporal lobe epilepsy.1); upward arrow=significant gain (p<0.1).
al application of amobarbital, methohexital (brevital)r etomidate (Buchtel et al., 2002), and pre- or intra-perative electrocortical stimulation (Wellmer et al.,009).
elective surgical approaches versustandard anterior temporal lobectomy
he logical step following from the previous sectionn epilepsy surgery is to remove what is necessary
o control seizures and leave as much as possibleunctional tissue in order to preserve the patient’sognitive functions. According to a review on theuest for the optimal extent of resection in TLE bychramm (2008), no particular surgical approach waseported to be superior with regards to seizure con-rol. Six of 8 studies on selective surgery versusemporal lobe resections reported similar seizure out-omes and 2 reported better outcome with largeresection. This report has very recently been chal-enged by a meta-study by Josephson et al. (2013)
ho compared selective amygdalo-hippocampectomySAH) and anterior temporal lobectomy (ATL) across 15
223
tudies and found overall better outcome with largeresections in 13 studies (risk ratio: 1.32; 95% confidencenterval [CI]: 1.12-1.57; p<0.01). This study, however, didot address the question of whether one approachight be superior to the other with regards to cog-
itive outcome. According to the review by Schramm2008), 11/14 studies reported that smaller, as opposed

2
C
tnmbtbop1asWihiattgElafslawarltivypoocd(Ferrsmppdrnreoc
TssermltouOobsaTlli2DmasuaA1tnsgiloanlsclovaW(lmA
. Helmstaedter
o larger, resections are associated with better cog-itive outcome. In addition, taking the extent of theesial resection into consideration, an association
etween better seizure control and larger resec-ions was reported in 5/12 studies and an associationetween extent of resection and neuropsychologicalutcome was not identified in 8/9 studies. A reviewrovided in a study by Tanriverdi et al. reported that6/21 studies demonstrated better cognitive outcomefter selective surgery, compared to 5/21 studies whichhowed no difference (Tanriverdi et al., 2010).
ithin the last 20 years, surgery for TLE has becomencreasingly selective due to major improvements inigh-resolution structural and functional imaging, with
ncreased reliability for detecting subtle lesions suchs dysplasia or hippocampal sclerosis in patients withemporal lobe epilepsies. In its beginnings, selec-ive surgery was only performed for patients withross lesions and/or with evidence from intracranialEG recordings. In 1982, Wieser and Yasargil pub-ished a series of 27 patients (12 with mesial tumoursnd epileptogenic area identified by stereo or sur-ace EEG in 13 and 2 patients, respectively) whichhowed good seizure control, improved general intel-igence, and minor-to-no decline in verbal memoryfter SAH, compared to large temporal lobe resectionshich caused significant functional losses (Wieser
nd Yasargil, 1982). In 1993, Goldstein and Polkeyeported that both surgical approaches cause simi-ar decrease in delayed recall in logical memory, buthat ATL, in contrast to SAH, causes more impairmentn paired associate learning and immediate recall ofisuo-spatial material (Goldstein and Polkey, 1993). Aear before, the same authors reported that whereasatients who had undergone either selective surgeryr en-bloc resections could be distinguished basedn a traditional memory test score, this was not thease for memory measures more related to every-ay behaviour (Rivermead Behavioural Memory Test)
Goldstein and Polkey, 1992).or a long time, selective surgery was performedxclusively at a few centres. However even for ATLesections it was demonstrated that lateral extent ofesection (<3 cm) (Helmstaedter and Elger, 1996), con-ideration of cortical eloquent sites for language oremory (Ojemann and Dodrill, 1985), and the patients
athological status (presence/absence of hippocam-al pathology) (Hermann et al., 1992) were decisiveeterminants for memory decline after surgery. In a
24
etrospective study by Wolf et al., performed in 1993,o difference in memory outcome (RAVLT, WMS) waseported, taking the extent of mesial (>/<2 cm) or lat-ral (>/<4 cm) resection into consideration. Instead,lder age at seizure onset was decisive for worse out-ome (Wolf et al., 1993).
rslSwt
he earlier studies performed in patients undergoingtandard ATL already implicitly hinted that differenturgical procedures within the language-dominant lat-ral temporal neo-cortex affect learning capability,ather than delayed recall, and that, based on memoryeasures (mainly RAVLT, CVLT and WMS), the patient
anguage capabilities should be taken into considera-ion in order to understand the memory impairmentsbserved in TLE (Hermann et al., 1988) (see belownder Living in a different test universe). In thejemann and Dodrill study from 1985, 80% of the mem-
ry outcomes assessed by WMS could be predictedased on the association between the resection andites essential for naming, encoding, or memory stor-ge, as identified by electrical stimulation mapping.his close relationship between verbal memory and
anguage indicates that preoperative determination ofanguage sites can be used to protect against lossesn either function (Hamberger, 2007; Hamberger et al.,010).ifferential cognitive sequelae of surgery of temporo-esial and temporo-lateral structures for different
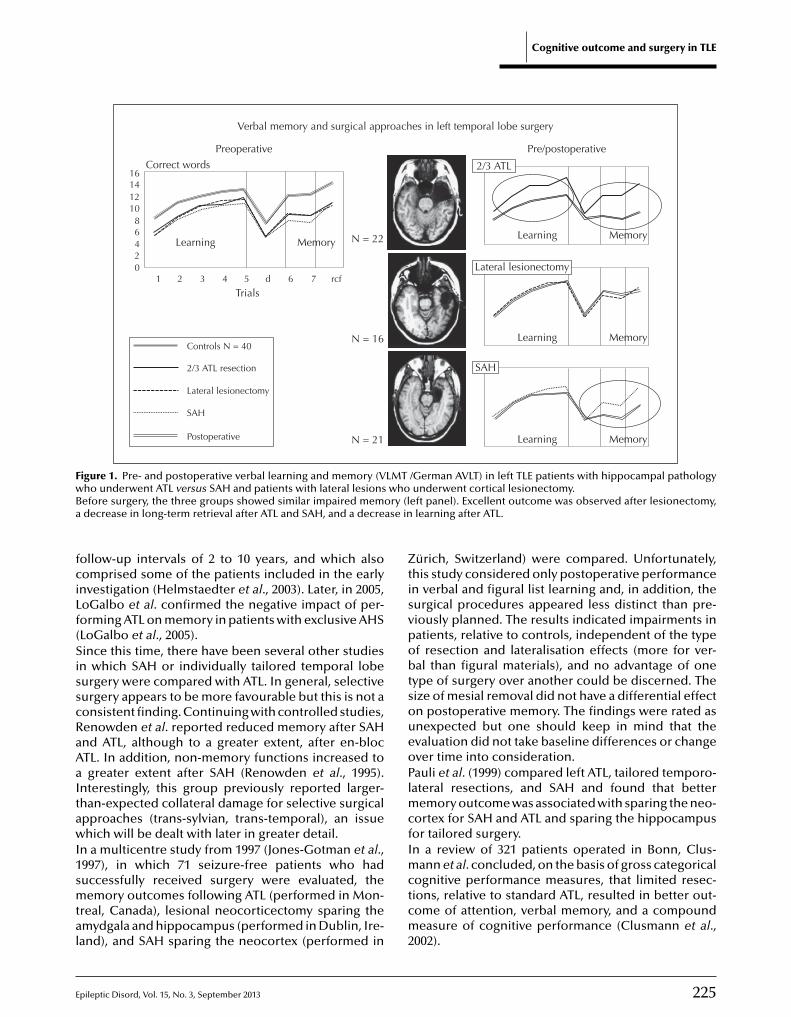
spects of verbal learning and memory were demon-trated in a study which compared patients whonderwent cortical lesionectomy to patients withmmonshorn sclerosis who either underwent SAH orTL (Helmstaedter et al., 1996; Helmstaedter et al.,997) (figure 1). This study had been performed at aime in Bonn when selective surgery had become aew treatment option for mesial TLE. Thus, a retro-pective comparison was possible between tworoups of M-TLE patients; one group who, accord-
ng to the new treatment guidelines, underwenteft-sided SAH and another who, according to theld guidelines, received left-sided ATL, includingmygdalo-hippocampectomy. The third group witheocortical temporal lobe lesions and circumscribed
esionectomy, not affecting the mesial structures,erved as another control in order to compare betweenortical lesionectomy and cortical resection of non-esional tissue in ATL. Consistent with the presencef left TLE, patients from all groups showed impairederbal memory before surgery, but differed consider-bly with regards to postoperative memory outcome.
ith regards to average group data, least lossesi.e. unchanged performance) were observed afteresionectomy, SAH mainly caused a loss in long-term
emory aspects of verbal learning and memory, andTL, in which unaffected neocortical tissues had been
Epileptic Disord, Vol. 15, No. 3, September 2013
emoved, additionally caused a significant loss in thehort-term and working memory aspects of verbalearning and memory. The differential effects of leftAH and ATL on verbal learning and memory, whiche described in 1996 and 1997, were also observed in
he longitudinal study published in 2003 which had
E
Cognitive outcome and surgery in TLE
Verbal memory and surgical approaches in left temporal lobe surgery
Preoperative
Correct words 2/3 ATL
Lateral lesionectomy
SAH
Learning
1614121086420
1 2 3 4 5 6d rcf
Trials
Controls N = 40
2/3 ATL resection
Lateral lesionectomy
SAH
Postoperative
7
MemoryLearning Memory
Learning Memory
Learning Memory
N = 22
N = 16
N = 21
Pre/postoperative
F LMTw whoB ry (la ase in
fciLf(SisscRaAaItawI1smtal
ZtisvpobtsoueoPlmcfI
igure 1. Pre- and postoperative verbal learning and memory (Vho underwent ATL versus SAH and patients with lateral lesionsefore surgery, the three groups showed similar impaired memodecrease in long-term retrieval after ATL and SAH, and a decre
ollow-up intervals of 2 to 10 years, and which alsoomprised some of the patients included in the earlynvestigation (Helmstaedter et al., 2003). Later, in 2005,oGalbo et al. confirmed the negative impact of per-orming ATL on memory in patients with exclusive AHSLoGalbo et al., 2005).ince this time, there have been several other studies
n which SAH or individually tailored temporal lobeurgery were compared with ATL. In general, selectiveurgery appears to be more favourable but this is not aonsistent finding. Continuing with controlled studies,enowden et al. reported reduced memory after SAHnd ATL, although to a greater extent, after en-blocTL. In addition, non-memory functions increased togreater extent after SAH (Renowden et al., 1995).
nterestingly, this group previously reported larger-han-expected collateral damage for selective surgicalpproaches (trans-sylvian, trans-temporal), an issuehich will be dealt with later in greater detail.
n a multicentre study from 1997 (Jones-Gotman et al.,
pileptic Disord, Vol. 15, No. 3, September 2013
997), in which 71 seizure-free patients who haduccessfully received surgery were evaluated, theemory outcomes following ATL (performed in Mon-
real, Canada), lesional neocorticectomy sparing themydgala and hippocampus (performed in Dublin, Ire-and), and SAH sparing the neocortex (performed in
mctcm2
/German AVLT) in left TLE patients with hippocampal pathologyunderwent cortical lesionectomy.
eft panel). Excellent outcome was observed after lesionectomy,learning after ATL.
ürich, Switzerland) were compared. Unfortunately,his study considered only postoperative performancen verbal and figural list learning and, in addition, theurgical procedures appeared less distinct than pre-iously planned. The results indicated impairments inatients, relative to controls, independent of the typef resection and lateralisation effects (more for ver-al than figural materials), and no advantage of one
ype of surgery over another could be discerned. Theize of mesial removal did not have a differential effectn postoperative memory. The findings were rated asnexpected but one should keep in mind that thevaluation did not take baseline differences or changever time into consideration.auli et al. (1999) compared left ATL, tailored temporo-ateral resections, and SAH and found that better
emory outcome was associated with sparing the neo-ortex for SAH and ATL and sparing the hippocampusor tailored surgery.n a review of 321 patients operated in Bonn, Clus-
225
ann et al. concluded, on the basis of gross categoricalognitive performance measures, that limited resec-ions, relative to standard ATL, resulted in better out-ome of attention, verbal memory, and a compoundeasure of cognitive performance (Clusmann et al.,
002).

2
C
MmtolraeclA(pisgbSrmssIrwaTlbtab
Ro
Isptaft(Ttfeclnrepw
eslcVtroAsochmptammrtphoorotuaa
H
Sonivcgdsnatms
. Helmstaedter
orino et al. (2006) demonstrated better preservedemory function after trans-sylvian SAH, compared
o ATL, and Paglioli et al. (2006) reported greater post-perative improvements after left SAH, as opposed to
eft ATL. Alpherts et al. (2008) showed that tailoredesections caused additional problems in attentionnd working memory whereas ATL, dependent on thextent of the resection of the superior temporal gyrus,aused greater problems with regards to verbal intel-igence and verbal comprehension.
more recent study from the Montreal groupTanriverdi et al., 2010) compared large samples ofatients who underwent left/right cortectomy, includ-
ng a comparison between AH (ATL; n=123) andelective AH (n=133). The findings indicated thateneral intelligence increased after epilepsy surgery,ut that verbal IQ was negatively affected by leftAH. Verbal memory declined and non-verbal memo-y improved after left-sided surgery, and non-verbalemory decreased after right ATL. In addition, later
urgery was associated with worse memory, andeizure freedom was associated with better memory.nterestingly, in this study, immediate logical memo-y recall significantly decreased after left-sided ATL,hereas delayed logical memory recall was similarly
ffected by both approaches after left-sided surgery.his is in line with what was previously discussed;
earning parameters are more significantly affectedy left neocortical resections than left mesial resec-
ions, and delayed memory parameters are similarlyffected following left neocortical resections usingoth approaches.
esection versus preservationf non-affected tissue
n concluding the neuropsychological findings onelective surgery versus ATL, selective surgery is clearlyreferred. From a neuropsychological point of view,
he functional integrity of brain tissue to be resected,nd thus the question of sacrificing versus preservingunctional tissue, appears to be of major impor-ance regarding cognitive loss observed after surgeryChelune, 1995; Helmstaedter, 1999; Stern, 2003).he evaluation of impact of resection of non-lesionalissue, however, is not that straightforward sinceor two-third standard temporal lobe surgery, andven more so for selective surgery, it is very diffi-
26
ult to determine the proportion of functional andesional/epileptogenic tissues with regards to cog-itive outcome. Resection of non-lesional tissueequires clinical and ethical justification. The negativeffects of resection of unaffected lateral cortex in ATLerformed in patients, with AHS as the sole pathology,ere reported in the previous section (Helmstaedter
adbnhoe
t al., 1996; LoGalbo et al., 2005). In contrast to this,urgery, which is confined to neocortical temporalobe lesions, appeared to be associated with very goodognitive outcome.ery recently, Hamberger et al. (2010) demonstrated
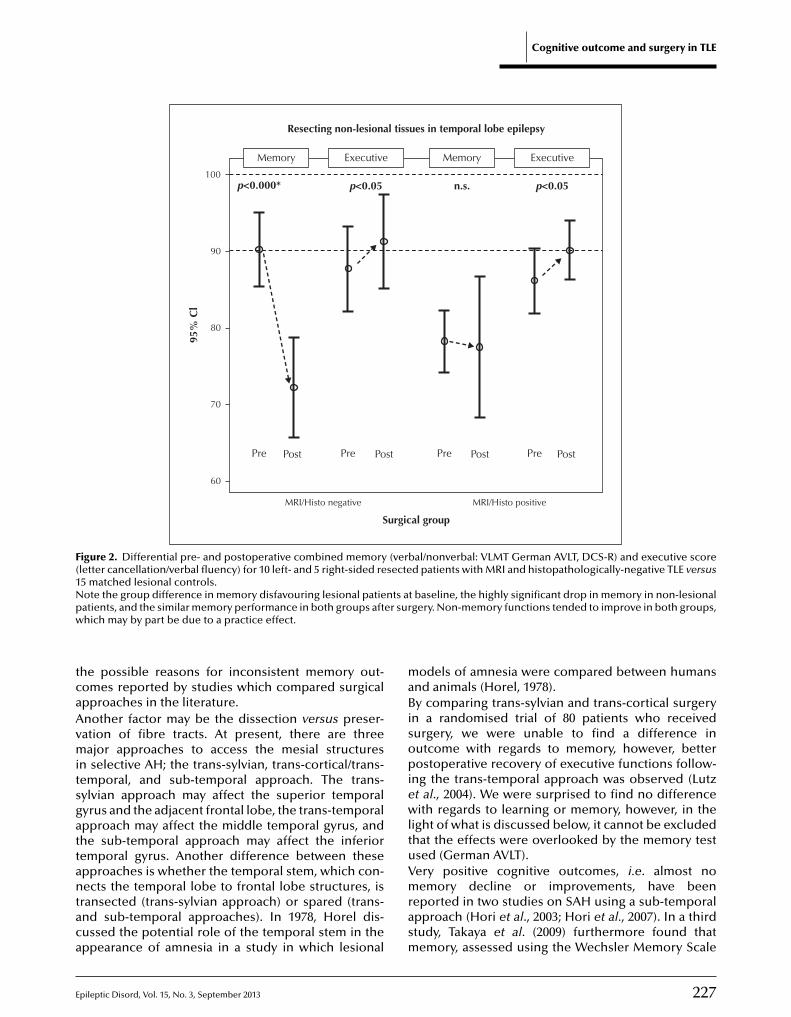
hat resection of a structurally intact hippocampusesulted in loss of visual naming ability, despite pre-perative mapping of the cortical naming sites.s a proof of principle that resection of pre-umably unaffected brain tissue worsens cognitiveutcome in TLE, we recently compared memory out-ome after temporal lobe surgery in 15 MRI- andistopathologically-negative patients and 15 pairwise-atched patients with MRI and histopathologically-
roven lesions. Clinical (e.g. side and site of surgery,ype of surgery, and onset and duration of epilepsy)nd neuropsychological performance, other thanemory (e.g. IQ, attention), were considered as theatching criteria. As for the question of whether
esected tissues were involved in epilepsy, it is impor-ant to note that 12/15 non-lesional patients showed noostoperative response with regards to seizures. It wasypothesized that preoperative differences in mem-ry outcome should reveal the impact of the lesionn memory, whereas postoperative differences shouldeveal the impact of resection of non-lesional tissuesn memory. The results impressively showed that for
he truly non-lesional TLE patients, memory is mostlynimpaired before surgery and drops to a postoper-tive level which is also observed in lesional patientsfter surgery (Helmstaedter et al., 2011a) (figure 2).
ow selective is selective surgery?
AH is a procedure aimed at the specific resectionf pathological mesial brain tissue whilst preservingon-affected lateral cortex which, to a varying degree,
s included in standard ATL. However, the selecti-ity of TLE surgery is limited by the fact that it mayause collateral neocortical damage due to the sur-ical approach. In this regard, we demonstrated thatamage of neocortical tissues adjacent to trans-sylvianurgery should be considered as a decisive determi-ant for postoperative decline of the more neocorticalspects of verbal learning and memory (learning, shorterm, and working memory). This observation was
ade independent of side of surgery. An effect of theide of surgery became evident only with regards to
Epileptic Disord, Vol. 15, No. 3, September 2013
measure of verbal, long-term consolidation (verbalelayed recall) which was affected, to a greater extent,y left-sided surgery. The size of mesial resection,egatively assessed by measurement of the residualippocampus after surgery, was of no relevance forutcome in verbal learning or memory (Helmstaedtert al., 2004). With this study, we identified one of
E
Cognitive outcome and surgery in TLE
Memory Executive ExecutiveMemory
Resecting non-lesional tissues in temporal lobe epilepsy
Surgical group
MRI/Histo negative MRI/Histo positive
60
70
80
90
100
95%
Cl
Pre Post Pre Post Pre Post Pre Post
p<0.000* p<0.05 p<0.05n.s.
Figure 2. Differential pre- and postoperative combined memory (verbal/nonverbal: VLMT German AVLT, DCS-R) and executive score( secte1N nts ap er surw
tcaAvmitsgattantaca
maBisopiewlt
letter cancellation/verbal fluency) for 10 left- and 5 right-sided re5 matched lesional controls.ote the group difference in memory disfavouring lesional patieatients, and the similar memory performance in both groups afthich may by part be due to a practice effect.
he possible reasons for inconsistent memory out-omes reported by studies which compared surgicalpproaches in the literature.nother factor may be the dissection versus preser-ation of fibre tracts. At present, there are threeajor approaches to access the mesial structures
n selective AH; the trans-sylvian, trans-cortical/trans-emporal, and sub-temporal approach. The trans-ylvian approach may affect the superior temporalyrus and the adjacent frontal lobe, the trans-temporalpproach may affect the middle temporal gyrus, andhe sub-temporal approach may affect the inferior
pileptic Disord, Vol. 15, No. 3, September 2013
emporal gyrus. Another difference between thesepproaches is whether the temporal stem, which con-ects the temporal lobe to frontal lobe structures, is
ransected (trans-sylvian approach) or spared (trans-nd sub-temporal approaches). In 1978, Horel dis-ussed the potential role of the temporal stem in theppearance of amnesia in a study in which lesional
uVmrasm
d patients with MRI and histopathologically-negative TLE versus
t baseline, the highly significant drop in memory in non-lesionalgery. Non-memory functions tended to improve in both groups,
odels of amnesia were compared between humansnd animals (Horel, 1978).y comparing trans-sylvian and trans-cortical surgery
n a randomised trial of 80 patients who receivedurgery, we were unable to find a difference inutcome with regards to memory, however, betterostoperative recovery of executive functions follow-
ng the trans-temporal approach was observed (Lutzt al., 2004). We were surprised to find no differenceith regards to learning or memory, however, in the
ight of what is discussed below, it cannot be excludedhat the effects were overlooked by the memory test
227
sed (German AVLT).ery positive cognitive outcomes, i.e. almost noemory decline or improvements, have been
eported in two studies on SAH using a sub-temporalpproach (Hori et al., 2003; Hori et al., 2007). In a thirdtudy, Takaya et al. (2009) furthermore found thatemory, assessed using the Wechsler Memory Scale

2
C
(dgoi(tttMrflbsattbfnfnfapwcwssvevtfltodopgieTtsftpSAcs2w
pfisAifImcttcc
Vh
Ioptowsclnwiecbpormltfmr(eowgot
. Helmstaedter
WMS), improved to a larger extent than attention afterominant side resections. At the same time, increasedlucose metabolism in extratemporal regions wasbserved. However, the latter observation was made
n only 7 patients. Unfortunately, a control conditionanother type of surgery) was not used in any ofhese studies, nor was the eventual effect of basalemporal lesions on language taken into considera-ion (Trebuchon-Da Fonseca et al., 2009). A study by
ikuni et al. (2006), in which the potential functionalelevance of the basal language area was considered,ocused only on memory. In this study, the basalanguage area, defined by strip electrodes, was sparedy entering the temporal horn via the collateralulcus, and verbal memory was found to be improvedfter surgery. However, it should be kept in mindhat all these studies were uncontrolled and thathe WMS was chosen for memory assessment ataseline and follow-up without explicitly controlling
or practice effects. The WMS is highly confounded byon-memory functions (IQ, language, and executive
unctions) (Helmstaedter et al., 2009a). Thus, it can-ot be excluded that postoperative improvement of
rontal lobe functioning, which is commonly observedfter temporal lobe surgery, had a beneficial effect onerformance in the WMS. Taking this into account,e very recently compared cognitive outcomes in
linically- and demographically-matched patientsho underwent subtemporal versus trans-sylvian
urgery (von Rhein et al., 2012). In this evaluation, bothurgical approaches caused a comparable decline inerbal learning and memory performance. Differentialffects became evident with regards to decline inerbal recognition memory (more affected by leftrans-sylvian SAH), as well as in verbal semanticuency and figural memory (more affected by sub-
emporal SAH) (for memory outcomes independentf side of surgery; see figure 3). The findings wereiscussed and thought to be probably due to the effectn the basal language area which is involved in lexicalrocessing and the effect on the inferior temporalyrus and ventral stream which have significant roles
n visual perception, imagery, and memory (Hamamet al., 2012; Hitomi et al., 2013).he temporal stem is not only preserved using therans-cortical or sub-temporal approach, but also pre-erved after surgery towards the mesial structuresollowing removal of the tip of the temporal pole untilhe mesial structures are visually accessible. By com-
28
aring memory outcomes after left/right trans-sylvianAH with those after temporal pole resections andH in 97 postsurgically seizure-free patients, an asso-iation between material (verbal/figural) and side ofurgery (left/right) was revealed (Helmstaedter et al.,008). For left-sided surgery, verbal memory outcomeas better after temporal pole resection and AH, com-
wn(Tttw
ared to trans-sylvian SAH; for right-sided surgery,gural memory outcome was better after the trans-ylvian approach, compared to the pole resection andH. The results were discussed in terms of different
mportance of the temporal stem and temporal poleor verbal and figural memory processing, respectively.n concluding this section, no single surgical approach
ay be discerned to be the safest with regards toognition, irrespective of seizure control. According tohe surgical approach, different tissues and fibre tractshat hinder the surgical procedure or locate to adja-ent areas may be affected and, either way, this hasonsequences for cognition.
ariation of the extent of mesialippocampal resection
n 1995, Wyler and colleagues published the first reportf a randomised study of mesial resection length inatients who underwent ATL (Wyler et al., 1995). In
his study, a maximal mesial resection to the levelf the superior colliculus led to a better outcomeith regards to seizure freedom (69%), in compari-
on to a smaller resection to the anterior edge of theerebral peduncle (38%). No effect of the resectionength on memory outcome (assessed by the Califor-ia Verbal Learning Test, CVLT) was obtained. However,hen hippocampal sclerosis was additionally taken
nto account, adverse memory outcome was associat-d with resection of non-sclerotic left hippocampus. Inontrast to the findings of Wyler et al., an early studyy Katz et al. in 1989 reported greater losses in WMSerformance (percent retained), related to the extentf the medial resection (Katz et al., 1989). Similarly,etention (%) of visual material was correlated to the
edial extent of the resection of the right temporalobe. Both studies did not account for the covaria-ion of lateral resections. A study by Joo et al. in 2005,or example, reported an association between verbal
emory decline and only larger resection of the infe-ior and basal temporal gyrus in regression analysisJoo et al., 2005). In the above-mentioned study of Wolft al. (1993), an association between either the lateralr mesial extent of resection and memory outcomeas not identified when patients were categorised intoroups with larger versus smaller resections. In ourwn study on memory outcome after SAH, as a func-
ion of collateral surgical damage, memory change
Epileptic Disord, Vol. 15, No. 3, September 2013
as not correlated with hippocampal remnants, as aegative indicator for the mesial extent of resection
Helmstaedter et al., 2004).hus, based on studies that address mesial resec-ion length, there is no consistent result regardinghe question of whether sparing hippocampal tissueill cause better memory outcome or not. With this
E
Cognitive outcome and surgery in TLE
Surgical approach
-10
Transsylvian Subtemporal
-5
0
5
10
95%
Cl
Verbal learning
Figural learning
Verbal loss over time
Verbal recognition
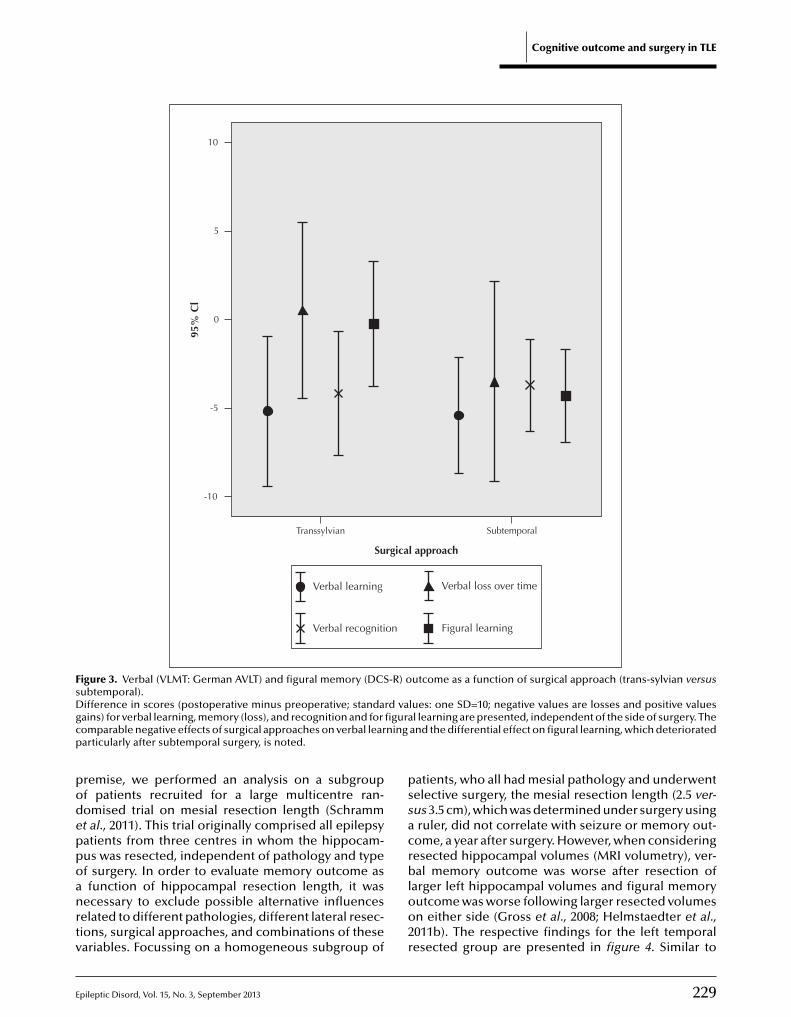
F -R) osD rd vag figurac ningp
podeppoanrtv
pssac
igure 3. Verbal (VLMT: German AVLT) and figural memory (DCSubtemporal).ifference in scores (postoperative minus preoperative; standaains) for verbal learning, memory (loss), and recognition and foromparable negative effects of surgical approaches on verbal leararticularly after subtemporal surgery, is noted.
remise, we performed an analysis on a subgroupf patients recruited for a large multicentre ran-omised trial on mesial resection length (Schrammt al., 2011). This trial originally comprised all epilepsyatients from three centres in whom the hippocam-
pileptic Disord, Vol. 15, No. 3, September 2013
us was resected, independent of pathology and typef surgery. In order to evaluate memory outcome asfunction of hippocampal resection length, it was
ecessary to exclude possible alternative influenceselated to different pathologies, different lateral resec-ions, surgical approaches, and combinations of theseariables. Focussing on a homogeneous subgroup of
rbloo2r
utcome as a function of surgical approach (trans-sylvian versus
lues: one SD=10; negative values are losses and positive valuesl learning are presented, independent of the side of surgery. The
and the differential effect on figural learning, which deteriorated
atients, who all had mesial pathology and underwentelective surgery, the mesial resection length (2.5 ver-us 3.5 cm), which was determined under surgery usingruler, did not correlate with seizure or memory out-
ome, a year after surgery. However, when considering
229
esected hippocampal volumes (MRI volumetry), ver-al memory outcome was worse after resection of
arger left hippocampal volumes and figural memoryutcome was worse following larger resected volumesn either side (Gross et al., 2008; Helmstaedter et al.,011b). The respective findings for the left temporalesected group are presented in figure 4. Similar to

2
C. Helmstaedter
Effects of lenght and volume of mesial resection on memory
Verbalmemory
Figurallearning
Figurallearning
Verbalmemory70
80
90
75
85
95
100
Stan
dart
val
ues
100+
/- 1
0 [9
5% C
l]
Pre Post Pre Post Pre Post Pre Post
Small Large
Intent-to-treat resection length
Verbalmemory
Figurallearning
Figurallearning
Verbalmemory70
80
90
75
85
95
Stan
dart
val
ues
100+
/- 1
0 [9
5% C
l]
Pre Post Pre Post Pre Post Pre Post
Small Large
Hippocampal volume difference
F -R) oi e reS sectet mory
t1tichsTtotaor(ItpooItbvts
a2bHit2toaevmi2afpd
igure 4. Verbal (VLMT: German AVLT) and figural memory (DCSntended hippocampal resection length (2.5 versus 3.5 cm) and thcores represent standard scores with mean=100, SD=10. The rehe intended resection length, is related to verbal and figural me
hat of Wyler’s randomised study of ATL (Wyler et al.,995), the major message from this study, with regardso SAH, was that consideration of resection length isrrelevant if the pathology at baseline is not taken intoonsideration. Thus, a large resection of an atrophiedippocampus will have fewer consequences than ahort resection of a non-atrophied hippocampus.he importance of removal of functional hippocampalissue is in line with Baxendaleı̌s finding that shrinkagef the hippocampal remnant after surgery is relevant
o memory outcome (Baxendale et al., 2000) and islso in line with recent findings on the dependencyf memory outcomes on functionality of the poste-ior hippocampus, as determined by functional MRIBaxendale et al., 2000; Bonelli et al., 2010).n conclusion, we face the same situation with regardso hippocampal resections as we have done for tem-oral neocortical resections, i.e. postoperative declinef learning and memory mostly results from resection
30
r dissection of non-affected functional brain tissues.n this regard, the degree of preservation of functionalissue, which can be achieved with radiosurgery, maye of future interest. Radiosurgery is claimed to pro-ide high spatial resolution with the aim of changinghe intrinsic epileptic characteristics of radiated tis-ue. First reports on the neuropsychological outcome
ttdpsrm
utcome in patients with left M-TLE after SAH as a function of thesected hippocampal volume (median split).d volume, taking preoperative pathology into account but notoutcome.
ppear optimistic (Bartolomei et al., 2008; Barbaro et al.,009). Comparably, the cognitive outcomes of deeprain stimulation will be of interest in the future.owever, it should be established whether stimulation
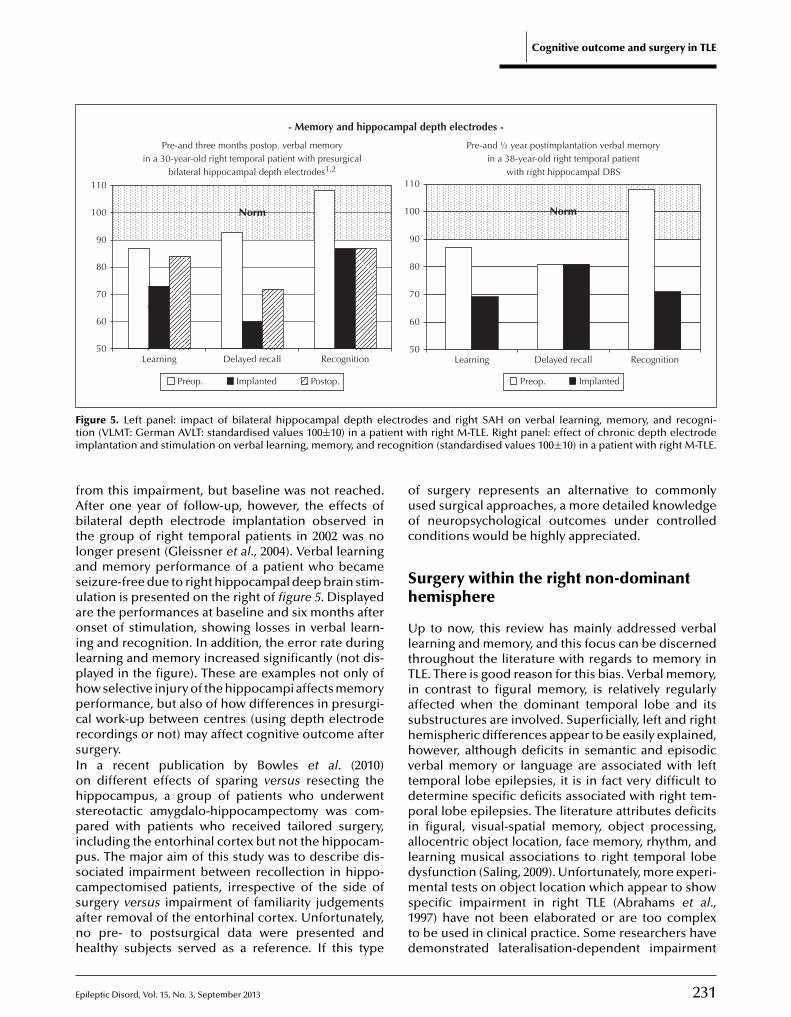
ndeed preserves function or whether it interferes withhe functionality of the stimulated area (Benabid et al.,002; Boon et al., 2007; Velasco et al., 2007). In addition,he possible effects of acute or chronic implantationf depth electrodes need to be systematically evalu-ted. For example, we previously described negativeffects of bilateral depth electrode implantation onerbal memory, which were still evident after threeonths of postoperative follow-up, in patients follow-
ng right-sided selective TLE surgery (Gleissner et al.,002). As an example, verbal learning and memory of30-year-old female patient of this series, who suf-
ered from right TLE with hippocampal sclerosis, isresented on the left of figure 5. Displayed are the stan-ardised values of learning (sum across five learning
Epileptic Disord, Vol. 15, No. 3, September 2013
rials), free recall after a 30-minute delay, and recogni-ion memory, at baseline, after implantation of bilateralepth electrodes (implanted posteriorly along the hip-ocampal axis), postoperatively. The patient becameeizure-free. Following implantation, verbal memo-y significantly dropped with regards to long-termemory. After surgery, the patient partly recovered
E
Cognitive outcome and surgery in TLE
- Memory and hippocampal depth electrodes -
50
60
70
80
90
100
110
Learning Delayed recall Recognition50
60
70
80
90
100
110
Learning Delayed recall Recognition
NormNorm
Pre-and three months postop. verbal memoryin a 30-year-old right temporal patient with presurgical
bilateral hippocampal depth electrodes1,2
Pre-and ½ year postimplantation verbal memoryin a 38-year-old right temporal patient
with right hippocampal DBS
Preop. Implanted Postop. Preop. Implanted
F ectrot ient wi cogn
fAbtlasuaoilphpcrsIohspipscsanh
ouoc
Sh
UltTiashhvtdpia
igure 5. Left panel: impact of bilateral hippocampal depth elion (VLMT: German AVLT: standardised values 100±10) in a patmplantation and stimulation on verbal learning, memory, and re
rom this impairment, but baseline was not reached.fter one year of follow-up, however, the effects ofilateral depth electrode implantation observed in
he group of right temporal patients in 2002 was noonger present (Gleissner et al., 2004). Verbal learningnd memory performance of a patient who becameeizure-free due to right hippocampal deep brain stim-lation is presented on the right of figure 5. Displayedre the performances at baseline and six months afternset of stimulation, showing losses in verbal learn-
ng and recognition. In addition, the error rate duringearning and memory increased significantly (not dis-layed in the figure). These are examples not only ofow selective injury of the hippocampi affects memoryerformance, but also of how differences in presurgi-al work-up between centres (using depth electrodeecordings or not) may affect cognitive outcome afterurgery.n a recent publication by Bowles et al. (2010)n different effects of sparing versus resecting theippocampus, a group of patients who underwenttereotactic amygdalo-hippocampectomy was com-ared with patients who received tailored surgery,
ncluding the entorhinal cortex but not the hippocam-
pileptic Disord, Vol. 15, No. 3, September 2013
us. The major aim of this study was to describe dis-ociated impairment between recollection in hippo-ampectomised patients, irrespective of the side ofurgery versus impairment of familiarity judgementsfter removal of the entorhinal cortex. Unfortunately,o pre- to postsurgical data were presented andealthy subjects served as a reference. If this type
ldms1td
des and right SAH on verbal learning, memory, and recogni-ith right M-TLE. Right panel: effect of chronic depth electrode
ition (standardised values 100±10) in a patient with right M-TLE.
f surgery represents an alternative to commonlysed surgical approaches, a more detailed knowledgef neuropsychological outcomes under controlledonditions would be highly appreciated.
urgery within the right non-dominantemisphere
p to now, this review has mainly addressed verbalearning and memory, and this focus can be discernedhroughout the literature with regards to memory inLE. There is good reason for this bias. Verbal memory,
n contrast to figural memory, is relatively regularlyffected when the dominant temporal lobe and itsubstructures are involved. Superficially, left and rightemispheric differences appear to be easily explained,owever, although deficits in semantic and episodicerbal memory or language are associated with leftemporal lobe epilepsies, it is in fact very difficult toetermine specific deficits associated with right tem-oral lobe epilepsies. The literature attributes deficits
n figural, visual-spatial memory, object processing,llocentric object location, face memory, rhythm, and
231
earning musical associations to right temporal lobeysfunction (Saling, 2009). Unfortunately, more experi-ental tests on object location which appear to show
pecific impairment in right TLE (Abrahams et al.,997) have not been elaborated or are too complexo be used in clinical practice. Some researchers haveemonstrated lateralisation-dependent impairment

2
C
irodssiclSole1eostben(dvHdavtpllowotgtioenTrlmrolbcFtomn
s(SbispsecMhsTtntodd“sem(maiv(Awrtdtt
L
Ttgtepu1
. Helmstaedter
n visual spatial memory in patients with TLE whoeceived surgery (Smith and Milner, 1989). The valuef these results for monitoring surgery is difficult toetermine since the pathological condition beforeurgery is not taken into consideration. Similarly,tudies are difficult to rate which show differencesn performances in right temporal lobe patients whenompared to healthy subjects, rather than left temporalobe patients (Saling, 2009).tandard tests of figural and visual spatial memorynly partially show the expected differences between
eft and right temporal lobe epilepsies (Hampsteadt al., 2010; Helmstaedter et al., 1991; Piguet et al.,994). More often, they fail to show differences (Barrt al., 2004; Barr et al., 1997; McConley et al., 2008)r require different evaluations in order to gainpecificity (Helmstaedter et al., 1995). Moreover, evenhough establishing right temporal lobe dysfunctionefore surgery is possible, monitoring the effects ofpilepsy surgery within the right temporal lobe mayot necessarily be possible with such tests (see table 1)
Gleissner et al., 1998a). Two of the few studies thatemonstrated dissociated surgical outcome (left/righterbal/figural) have already been cited (Katz et al., 1989;elmstaedter et al., 2008). Right temporal lobe surgeryoes cause decline in verbal and also figural memory,nd this is often overseen. To sum up losses in eithererbal or figural memory, 45% of 365 patients with rightemporal lobe resections in our series (see table 1)resented with memory loss and 8% presented with
oss in both performances. For the 351 patients witheft temporal lobe resections, 54% presented with lossf either verbal or figural memory and 16% presentedith loss of both. These figures, although evaluatedn the basis of gross test-wise categorisations, parallel
he outcome reported on a test score level in our lon-itudinal study (Helmstaedter et al., 2003). The facthat, unlike left temporal lobe surgery, losses follow-ng right temporal lobe surgery are often balanced orutweighed by gains (see table 1) easily leads to therroneous conclusion that losses in this group can beeglected.aken together, it is difficult to reliably relate figu-al/spatial memory performance to the right temporalobe or right mesial structures, and it appears even
ore difficult to specifically relate impairments toight-sided surgery. We recently concluded, basedn a long-term study of patients aged 6-68, that
eft/right temporal lobe differences in verbal memory
32
ecome evident only in the mature brain and not inhildren or the elderly (Helmstaedter and Elger, 2009).igural memory appears to be organised differentlyo verbal memory. This is indicated by observationsf “crowding” or the “suppression” of figural-visualemory in the presence of atypical language domi-
ance and the differential impact of lateralised epilep-
trbseas
ies on material-specific memory in men and womenHelmstaedter et al., 1994; Helmstaedter et al., 1999).imilar effects on language functions have not yeteen described. On discussing the “crowding” effect
n 1994, we suggested that it would be better to con-ider two hemisphere-specific styles of informationrocessing rather than material specificity. Material-pecific tasks represent an expression and not anquivalent of the respective type of information pro-essing (Helmstaedter et al., 1994). In this respect,ichael Saling in 2009 made the statement that
emispheric lateralisation is task- rather than material-pecific (Saling, 2009).aking into account the large number of left and rightemporal lobe patients who are not left-side domi-ant for language (see table 1), it comes as no surprise
hat lateralisation via material-specific memory testingften fails. This is particularly true for atypical languageominance in left temporal lobe epilepsies which,ue to “plasticity”, often show unimpaired verbal andunexpected” figural memory impairment. One rea-on why right temporal patients often do not show thexpected impairment is verbalisation of the non-verbalaterial. Verbalisation almost always interferes with
or supports?) figural/visual spatial memory assess-ent and this should be controlled either by choosing
bstract and hard-to-verbalise material or by increas-ng the complexity of the material in such a way thaterbal memory fails to compensate for the impairmentHelmstaedter et al., 1995).s a more general consideration, one may discusshether the common concepts of testing which are
elevant in the investigation of left hemisphere func-ion (i.e. mental reasoning) are appropriate to furtherelineate right hemisphere functions. The identifica-
ion and assessment of right hemisphere functionsherefore remains a challenge.
iving in a different test universe
he discussion in the previous section demonstrateshat neuropsychological assessment, like other dia-nostic tools, opens a window with a view intohe nature of cognitive impairment associated withpilepsy and after epilepsy surgery. However, neuro-sychological outcomes much depend on the testssed. As already demonstrated by Jones-Gotman in993, different epilepsy centres use different tests or
Epileptic Disord, Vol. 15, No. 3, September 2013
est batteries (Jones-Gotman et al., 1993) and recenteviews suggest that this has not changed since then. Atest, one can make recommendations as to which testshould be used for neuropsychological assessment inpilepsy patients. A recent evaluation of tests whichre currently used in epilepsy centres in German-peaking countries showed that over 200 different

E
tmsHadftwt2fatiiaatnfatdiSmushocctdCcbtBefsidfdoAciapnr
mbobeecp
D
AgfagfaTlcwrfIaiHwpfdTtp(lgaDnsmrweOl
ools were in use and that there was, at best, some com-on sense with regards to which functional domains
hould be addressed (Witt and Helmstaedter, 2009a).ence, discussing the outcomes of epilepsy surgery
nd different surgical approaches also requires aiscussion of the tests in use and their psychometric
eatures. Focusing on memory tests in TLE, differentests appear to have different sensitivity and specificityith regards to differentially lateralised and localised
emporal lobe lesions and epilepsies (Loring et al.,008). A comparison of the Logical Memory subtestrom the WMS-R, the California Verbal Learning Test,nd the Verbal Learning and Memory Test showedhat although the three tests provided overlappingndicators for TLE or mesial pathology, they are barelynterchangeable (Helmstaedter et al., 2009b). The testsddressed different aspects of semantic processingnd memory organisation, and thus were differen-ially sensitive to performance and impairments inon-memory domains. This is indicated by the dif-
erent correlations between the three memory testsnd non-memory functions which are reported inable 2. Accordingly, confounding memory testing byemands on language, attention, intelligence, order-
ng, or semantic memory can easily bias the findings.pecific temporal or temporo-mesial memory impair-ent may be overlooked or the memory test may pick
p impairments in extratemporal executive functions,emantic memory, and language functions (compre-ension, fluency). Postoperatively, for example, theften observed improvements in executive functionsan support short-term and working memory whichan compensate for additional problems with long-erm retention. Thus, study results obtained withifferent tests must be compared with great caution.entres differ not only with regards to neuropsy-hological tests in use. For example, we comparedaseline and outcome data obtained using the same
ests at different surgical centres (Zürich, Freiburg,erlin) and in each case, a highly significant centreffect was obtained (Helmstaedter, 2004). Differentactors may contribute to centre effects and thesehould be controlled for when comparing or merg-ng data from different centres. Recruited patients mayiffer (collection bias), presurgical diagnoses may dif-
er (drug withdrawal, provoked seizures, subdural orept electrodes), and only some patients are placedn a postoperative drug schedule, preoperatively.dditional scientifically-motivated neuropsychologi-
pileptic Disord, Vol. 15, No. 3, September 2013
al evaluations (e.g. in fMRI or EEG/ERP studies) mightnterfere with routine neuropsychological testing. Inddition, there is not yet a full consensus on inter-retation of imaging and neuropathological data andeurologists/patients may be willing to take differentisks with regards to referral for surgery, also surgeons
anddij
Cognitive outcome and surgery in TLE
ay follow an individual approach. Further factors maye added, but the major message is that neuropsychol-gists (although not exclusively) are very likely biasedy their own view and procedures, and that a greaterxchange of knowledge and a common language aressential to achieve further progress in order to dis-ern the best treatment for the individual patient withharmacoresistant epilepsy.
oes memory impairment matter?
s discussed in the previous sections, patients under-oing epilepsy surgery have an increased risk ofurther memory impairment after surgery. The explicitim of this article was to discuss whether there is areater preservation of patients’ cognitive capabilitiesollowing different individual and selective surgicalpproaches, relative to extended standard resections.he answer to this is yes, however, for neuropsycho-
ogists, this is a legitimate question since it may not belear whether subtle differences in memory outcome,hich are assessed using sophisticated tests in a labo-
atory, have any relevance for the patient who wantsoremost to become seizure-free.n this regard, it has been demonstrated that patientsre, in part, willing to risk some cognitive declinen order to become seizure-free (Langfitt et al., 2007;
elmstaedter, 2008). In our long term follow-up study,e discussed so called “double losers”, referring toatients who, in the long run, do not become seizure-
ree and, in addition, experience significant memoryecline (Helmstaedter et al., 2003). Of the group of 732LE patients presented in table 1, about 15% belong tohis group (verbal memory decline >2 SD). Includingatients who are not seizure-free with milder losses
decline >1 SD), the group increases to 37%. In theong-term, follow-up study of Langfitt et al. (2007), aroup of double losers (only 8%) were identified to bet a particular risk of losing quality of life over time.ependent on aetiology, chronic epilepsy does notecessarily cause mental decline. Temporal lobeurgery, in contrast, often does, and there is the legiti-ate fear that every additional loss poses an increased
isk of later acceleration of mental/memory declineith normal or even pathological aging (Helmstaedtert al., 2002).ne should bear in mind that patients with long-
asting epilepsies, particularly with early onset, have
233
lready adapted to their impairments in a way that cog-itive losses due to surgery will probably not affectomains which are of major importance for their everyay life. However, patients postoperative performance
s still often considerably below that of healthy sub-ects, and patients often are still aware of, and suffer

234 Epileptic Disord, Vol. 15, No. 3, September 2013
C. Helmstaedter
Tab
le2.
Co
rrel
atio
ns
bet
wee
nve
rbal
mem
ory
test
san
dte
sts
on
IQ,e
xecu
tive
,an
dla
ngu
age
fun
ctio
ns
(on
lyst
atis
tica
llysi
gnifi
can
tres
ult
sar
ed
isp
laye
d).
Voca
bu
lary
WA
IS-R
IQD
igit
sSp
eed
Flex
ibili
tySi
mila
riti
esC
om
pre
-h
ensi
on
Flu
ency
Nam
ing
VLM
Tto
tall
earn
ing
rN
A0.
444**
0.41
7**0.
268*
NA
0.31
6*0.
419**
0.49
3**N
Asi
g.0.
002
0.00
10.
040
0.04
10.
002
0.00
0
VLM
Td
elay
edfr
eere
call
rN
A0.
348*
NA
NA
NA
NA
0.40
2**N
A0.
299*
sig.
0.01
50.
003
0.03
5V
LMT
loss
ove
rti
me
rN
AN
AN
AN
AN
AN
AN
AN
AN
Asi
g.
VLM
Tre
cogn
itio
nr
NA
0.53
4**N
AN
AN
A0.
347*
0.53
4**0.
306*
0.35
2*
sig.
0.00
00.
024
0.00
00.
018
0.01
2
CV
LTto
tall
earn
ing
r0.
295*
0.42
4**0.
391**
0.34
2**0.
388**
0.43
1**0.
407**
0.51
6**0.
410**
sig.
0.04
40.
003
0.00
20.
008
0.00
30.
004
0.00
30
0.00
3
CV
LTd
elay
free
reca
llr
0.31
7*0.
474**
0.32
4*0.
470**
0.42
3**0.
393**
0.56
2**0.
554**
0.46
3**
sig.
0.03
00.
001
0.01
10.
000
0.00
10.
010
0.00
00.
000
0.00
1
CV
LTlo
sso
ver
tim
er
NA
NA
NA
0.37
2**N
AN
A0.
400**
0.34
0**0.
292*
sig.
0.00
40.
004
0.00
90.
04
CV
LTre
cogn
itio
nr
NA
NA
NA
NA
0.29
6*N
AN
AN
AN
Asi
g.0.
026
Logi
calM
emo
ryI
P0.
329*
0.33
1*N
AN
A0.
376**
0.40
4**N
A0.
268*
0.36
9**
sig.
0.02
40.
022
0.00
40.
008
0.04
00.
008
Logi
calM
emo
ryII
P0.
298*
0.35
6*0.
371**
NA
0.30
7*0.
387*
0.29
9*0.
258*
0.50
3**
sig.
0.04
20.
013
0.00
30.
020
0.01
10.
033
0.04
90.
000
VLM
T:G
erm
anA
VLT
;CV
LT:C
alif
orn
iaV
erb
alLe
arn
ing
Test
;WM
S:W
ech
sler
Mem
ory
Scal
e;W
AIS
:Wec
hsl
erA
du
ltIn
telli
gen
ceSc
ale
revi
sed
;NA
:no
tap
plic
able
;r:c
orr
elat
ion
coef
fici
ent;
sig:
sign
ifica
nce
leve
l.**
Co
rrel
atio
nis
sign
ifica
nta
tth
e0.
01le
vel(
2-ta
iled
);*C
orr
elat
ion
issi
gnifi
can
tatt
he
0.05
leve
l(2-
taile
d).

E
feptt1ammeBasrotqWpc1saei
S
SmpibfaTtheHgebdAeroTlfOtaw
aminHaon(sdist2
DCw
R
Aoh
AVsN
AVt2
AKe2
Bpme
Bri1
BBr
rom, their impairments. Contrary to what one mayxpect, a study addressing the relationship betweenerformance and complaint showed that lower cogni-
ive demands were associated with stronger, ratherhan weaker, subjective complaints (Gleissner et al.,998b). Other studies indicate that there is no reli-ble correlation between subjective complaints andemory performance, and that complaints aboutemory problems after surgery are better consid-
red as a marker of depression (Sawrie et al., 1999;axendale and Thompson, 2005). Different findingsnd positions on the ecological validity issue demon-trate that more research, as well as presumably moreeliable ways for the assessment of the consequencesf memory impairment and loss on everyday func-
ioning in TLE, are needed. In any case, quality of lifeuestionnaires do not appear to be sufficient.ith regards to the memory tests in use, we have
reviously demonstrated that they not only providelinical but also ecological validity (Helmstaedter et al.,998b). In addition, we were repeatedly able to demon-trate a correlation between surgical memory outcomend psychosocial socioeconomic outcome (Lendtt al., 1997; Helmstaedter et al., 2003). Thus, memory
mpairment and change in memory are important.
ummary
urgery is a very successful treatment option for phar-acoresistant TLE, however, 30% to 50% of surgery
atients face a risk of additional postoperative memorympairment. The patients’ mental reserve capacities ataseline, seizure outcome, and, most importantly, the
unctional integrity of the brain tissues to be resectedre major determinants of surgical cognitive outcome.here is now converging evidence that individuallyailored and standard selective surgical approachesave a superior functional outcome, compared toxtended standard ATL (including mesial structures).owever, even with selective approaches, collateralrey and white matter damage should be consid-red. Whether cognitive losses can be further reducedy superselective treatments such as radiosurgery oreep brain stimulation is yet to be determined.s already mentioned, this article focuses on thexperiences, development, and observations prima-ily from one centre in Bonn/Germany over a periodf more than 20 years, and is referenced accordingly.
pileptic Disord, Vol. 15, No. 3, September 2013
he different views and opinions of others are acknow-edged and the ongoing discourse and initiation ofurther studies is highly appreciated.
f major concern is how neuropsychology may con-ribute to improvements in surgical outcome. Qualitynd outcome control, however, require instrumentshich reliably reflect patients’ functionality at baseline
E
Bce
Bau
Cognitive outcome and surgery in TLE
s well as changes in intervention-related perfor-ance. A consensus regarding assessments is required
n order to enable better comparison and commu-ication across centres (Witt et al., 2009; Witt andelmstaedter, 2009b; Helmstaedter and Witt, 2012). In
ddition, measures that are more valid than qualityf life questionnaires or depression inventories areeeded to assess the everyday functioning of patients
Helmstaedter et al., 2011c). Finally, the long-term con-equences of (additional) cognitive impairments in theeveloping and aging brain remain to be determined
n more detail as well as the role of uncontrolledeizures, interictal epileptic activity, and antiepilepticreatment for cognitive outcomes (Helmstaedter et al.,011d). �
isclosures.. Helmstaedter declares that there are no conflicts of interestith regard to the contents of this article.
eferences
brahams S, Pickering A, Polkey CE, Morris RG. Spatial mem-ry deficits in patients with unilateral damage to the rightippocampal formation. Neuropsychologia 1997; 35: 11-24.
lpherts WC, Vermeulen J, van Rijen PC, da Silva FH, vaneelen CW. Verbal memory decline after temporal epilepsyurgery? A 6-year multiple assessments follow-up study.eurology 2006; 67: 626-31.
lpherts WC, Vermeulen J, van Rijen PC, da Silva FH, vaneelen CW. Standard versus tailored left temporal lobe resec-
ions: differences in cognitive outcome? Neuropsychologia008; 46: 455-60.
ndersson-Roswall L, Engman E, Samuelsson H, Malmgren. Cognitive outcome 10 years after temporal lobepilepsy surgery: a prospective controlled study. Neurology010; 74: 1977-85.
arbaro NM, Quigg M, Broshek DK, et al. A multicenter,rospective pilot study of gamma knife radiosurgery foresial temporal lobe epilepsy: seizure response, adverse
vents, and verbal memory. Ann Neurol 2009; 65: 167-75.
arr WB, Chelune GJ, Hermann BP, et al. The use of figu-al reproduction tests as measures of nonverbal memoryn epilepsy surgery candidates. J Int Neuropsychol Soc997; 3: 435-43.
arr W, Morrison C, Zaroff C, Devinsky O. Use of therief Visuospatial Memory Test-Revised (BVMT-R) in neu-opsychological evaluation of epilepsy surgery candidates.pilepsy Behav 2004; 5: 175-9.
235
artolomei F, Hayashi M, Tamura M, et al. Long-term effi-acy of gamma knife radiosurgery in mesial temporal lobepilepsy. Neurology 2008; 70: 1658-63.
axendale S, Thompson P. Defining meaningful postoper-tive change in epilepsy surgery patients: measuring thenmeasurable? Epilepsy Behav 2005; 6: 207-11.

2
C
Bhd
BEsif9
Bil
Bi2
BstN
BDW
Crl
Coe
Epr
GccN
Gpe4
Gos2
GopE
Gl1
GahN
GHmd
GpN
Hev2
Hi
HDh
HKvw2
HA
Hs
HoP
Hr
Hti1
HaB
He2
Hie
Hshl
. Helmstaedter
axendale SA, Thompson PJ, Kitchen ND. Postoperativeippocampal remnant shrinkage and memory decline: aynamic process. Neurology 2000; 55: 243-9.
enabid AL, Minotti L, Koudsie A, de Saint Martin A, Hirsch. Antiepileptic effect of high-frequency stimulation of theubthalamic nucleus (corpus luysi) in a case of medicallyntractable epilepsy caused by focal dysplasia: a 30-monthollow-up: technical case report. Neurosurgery 2002; 50: 1385-1; discussion: 91-2.
onelli SB, Powell RH, Yogarajah M, et al. Imaging memoryn temporal lobe epilepsy: predicting the effects of temporalobe resection. Brain 2010; 133: 1186-99.
oon P, Vonck K, De Herdt V, et al. Deep brain stimulationn patients with refractory temporal lobe epilepsy. Epilepsia007; 48: 1551-60.
owles B, Crupi C, Pigott S, et al. Double dissociation ofelective recollection and familiarity impairments followingwo different surgical treatments for temporal-lobe epilepsy.europsychologia 2010; 48: 2640-7.
uchtel HA, Passaro EA, Selwa LM, Deveikis J, Gomez-Hassan. Sodium methohexital (brevital) as an anesthetic in theada test. Epilepsia 2002; 43: 1056-61.
helune GJ. Hippocampal adequacy versus functionaleserve: predicting memory functions following temporalobectomy. Arch Clin Neuropsychol 1995; 10: 413-32.
lusmann H, Schramm J, Kral T, et al. Prognostic factors andutcome after different types of resection for temporal lobepilepsy. J Neurosurgery 2002; 97: 1131-41.
lger CE, Grunwald T, Lehnertz K, et al. Human temporal lobeotentials in verbal learning and memory processes. Neu-
opsychologia 1997; 35: 657-67.
leissner U, Helmstaedter C, Elger CE. Right hippocampalontribution to visual memory: a presurgical and postsurgi-al study in patients with temporal lobe epilepsy. J Neuroleurosurg Psychiatry 1998a; 65: 665-9.
leissner U, Helmstaedter C, Quiske A, Elger CE. Theerformance-complaint relationship in patients withpilepsy: a matter of daily demands? Epilepsy Res 1998b; 32:01-9.
leissner U, Helmstaedter C, Schramm J, Elger CE. Mem-ry outcome after selective amygdalohippocampectomy: atudy in 140 patients with temporal lobe epilepsy. Epilepsia002; 43: 87-95.
leissner U, Helmstaedter C, Schramm T, Elger CE. Mem-ry outcome after selective amygdalohippocampectomy inatients with temporal lobe epilepsy: One-year follow-up.pilepsia 2004; 45: 960-2.
oldstein LH, Polkey CE. Behavioural memory after temporal
36
obectomy or amygdalo-hippocampectomy. Br J Clin Psychol992; 31: 75-81.
oldstein LH, Polkey CE. Short-term cognitive changesfter unilateral temporal lobectomy or unilateral amygdalo-ippocampectomy for the relief of temporal lobe epilepsy. Jeurol Neurosurg Psychiatry 1993; 56: 135-40.
Haie
HJ
ross RE, Loring DW, Langfitt JT, Ojemann GA, Olivier A,elmstaedter C. Surgical controversies in the treatment ofesial temporal lobe epilepsy: how to get there and what to
o when you get there. Epilepsia 2008; 49: 497.
runwald T, Lehnertz K, Helmstaedter C, et al. Limbic ERPsredict verbal memory after left-sided hippocampectomy.euroreport 1998; 9: 3375-8.
amame CM, Vidal JR, Ossandon T, et al. Reading the mind’sye: online detection of visuo-spatial working memory andisual imagery in the inferior temporal lobe. Neuroimage012; 59: 872-9.
amberger MJ. Cortical language mapping in epilepsy: a crit-cal review. Neuropsychol Rev 2007; 17: 477-89.
amberger MJ, Seidel WT, Goodman RR, McKhann GM 2nd.oes cortical mapping protect naming if surgery includesippocampal resection? Ann Neurol 2010; 67: 345-52.
ampstead BM, Lacey S, Ali S, Phillips PA, Stringer AY, Sathian. Use of complex three-dimensional objects to assessisuospatial memory in healthy individuals and patientsith unilateral amygdalohippocampectomy. Epilepsy Behav
010; 18: 54-60.
elmstaedter CA. Prediction of memory reserve capacity.dv Neurol 1999; 81: 271-9.
elmstaedter C. Neuropsychological aspects of epilepsyurgery. Epilepsy Behav 2004; 5: S45-55.
elmstaedter C. Temporal lobe resection-does the prospectf seizure freedom outweigh the cognitive risks? Nat Clinract Neurol 2008; 4: 66-7.
elmstaedter C. Assessment of cognitive function-does iteveal the patients at risk? Epilepsia 2009; 50: 34.
elmstaedter C, Elger CE. Cognitive consequences of two-hirds anterior temporal lobectomy on verbal memoryn 144 patients: a three-month follow-up study. Epilepsia996; 37: 171-80.
elmstaedter C, Elger CE. Chronic temporal lobe epilepsy:neurodevelopmental or progressively dementing disease?rain 2009; 132: 2822-30.
elmstaedter C, Witt JA. Clinical neuropsychology inpilepsy: theoretical and practical issues. Handb Clin Neurol012; 107: 437-59.
elmstaedter C, Pohl C, Hufnagel A, Elger CE. Visual learn-ng deficits in nonresected patients with right temporal lobepilepsy. Cortex 1991; 27: 547-55.
elmstaedter C, Kurthen M, Linke DB, Elger CE. Right hemi-phere restitution of language and memory functions in rightemisphere language-dominant patients with left temporal
obe epilepsy. Brain 1994; 117: 729-37.
Epileptic Disord, Vol. 15, No. 3, September 2013
elmstaedter C, Pohl C, Elger CE. Relations between verbalnd nonverbal memory performance: evidence of confound-ng effects particularly in patients with right temporal lobepilepsy. Cortex 1995; 31: 345-55.
elmstaedter C, Elger CE, Hufnagel A, Zentner J, Schramm. Different effects of left anterior temporal lobectomy,

E
slE
HCpm1
HNpI
HlvN
Hmdr
HaN
HCp
HCom2
HsoSM
HLwhw8
Hivo2
Hivo2
Hqrt
HJs2
HiN
Hme(
Hilt
HJmN
HHi2
Hh
Hpit
HaeN
JcrY
Jrmg
Jel
Jae
Kl
elective amygdalohippocampectomy, and temporal corticalesionectomy on verbal learning, memory, and recognition. Jpilepsy 1996; 9: 39-45.
elmstaedter C, Grunwald T, Lehnertz K, Gleissner U, ElgerE. Differential involvement of left temporolateral and tem-oromesial structures in verbal declarative learning andemory: evidence from temporal lobe epilepsy. Brain Cogn
997; 35: 110-31.
elmstaedter C, Lehnertz K, Widman G, Weber B, Elger CE.euronal complexity loss in temporomesially recorded EEGredicts recall performance of incidentally learned material.
nter J Psychophysiol 1998a; 30: 30.
elmstaedter C, Hauff M, Elger CE. Ecological validity ofist-learning tests and self-reported memory in healthy indi-iduals and those with temporal lobe epilepsy. J Clin Expeuropsychol 1998b; 20: 365-75.
elmstaedter C, Kurthen M, Elger CE. Sex differences inaterial-specific cognitive functions related to language
ominance: an intracarotid amobarbital study in left tempo-al lobe epilepsy. Laterality 1999; 4: 51-63.
elmstaedter C, Reuber M, Elger CC. Interaction of cognitiveging and memory deficits related to epilepsy surgery. Anneurol 2002; 52: 89-94.
elmstaedter C, Kurthen M, Lux S, Reuber M, Elger CE.hronic epilepsy and cognition: a longitudinal study in tem-oral lobe epilepsy. Ann Neurol 2003; 54: 425-32.
elmstaedter C, Van Roost D, Clusmann H, Urbach H, ElgerE, Schramm J. Collateral brain damage, a potential sourcef cognitive impairment after selective surgery for control ofesial temporal lobe epilepsy. J Neurol Neurosurg Psychiatry
004; 75: 323-6.
elmstaedter C, Schramm J, Elger CE. 15 years epilepsyurgery in Bonn: cognitive and seizure outcome. Abstractsf the 5th joint meeting of the German, Austrian, and Swissections of the International League Against Epilepsy, Basle,ay 16-19, 2007. Epilepsia 2007; 48(S3): 14.
elmstaedter C, Richter S, Roske S, Oltmanns F, Schramm J,ehmann TN. Differential effects of temporal pole resectionith amygdalohippocampectomy versus selective amygdalo-ippocampectomy on material-specific memory in patientsith mesial temporal lobe epilepsy. Epilepsia 2008; 49:
8-97.
elmstaedter C, Wietzke J, Lutz MT. Unique and shared valid-ty of the “Wechsler logical memory test”, the “Californiaerbal learning test”, and the “verbal learning and mem-ry test” in patients with epilepsy. Epilepsy Res 2009a; 87:03-12.
elmstaedter C, Wietzke J, Lutz MT. Unique and shared valid-ty of the “Wechsler logical memory test”, the “California
pileptic Disord, Vol. 15, No. 3, September 2013
erbal learning test”, and the “verbal learning and mem-ry test” in patients with epilepsy. Epilepsy Res 2009b; 87:03-12.
elmstaedter C, Petzold I, Bien CG. The cognitive conse-uence of resecting nonlesional tissues in epilepsy surgery-esults from MRI and histopathology-negative patients withemporal lobe epilepsy. Epilepsia 2011a; 52: 1402-8.
c
Kr
Lqm
Cognitive outcome and surgery in TLE
elmstaedter C, Roeske S, Kaaden S, Elger CE, Schramm. Hippocampal resection length and memory outcome inelective epilepsy surgery. J Neurol Neurosurg Psychiatry011b; 82: 1375-81.
elmstaedter C, Droge F, Witt JA. “Activities of daily living”n epilepsy-a worthwhile diagnostic supplement? European J
eurol 2011c; 18: 172.
elmstaedter C, Hermann B, Lassonde M, Kahane P, Arzi-anoglou A. Neuropsychology in the care of people with
pilepsy. Progress in Epileptic Disorders, Vol.11. MontrougeFrance): John Libbey Eurotext, 2011d.
ermann BP, Wyler AR, Steenman H, Richey ET. Thenterrelationship between language function and verbalearning/memory performance in patients with complex par-ial seizures. Cortex 1988; 24: 245-53.
ermann BP, Wyler AR, Somes G, Berry AD 3rd, Dohan FCr. Pathological status of the mesial temporal lobe predicts
emory outcome from left anterior temporal lobectomy.eurosurgery 1992; 31: 652-6; discussion: 6-7.
itomi T, Koubeissi MZ, Kaffashi F, Turnbull J, LüdersO. Visual processing in the inferior temporal cortex: an
ntracranial event related potential study. Clin Neurophysiol013; 124: 164-70.
orel JA. The neuroanatomy of amnesia. A critique of theippocampal memory hypothesis. Brain 1978; 101: 403-45.
ori T, Yamane F, Ochiai T, Hayashi M, Taira T. Subtem-oral amygdalohippocampectomy prevents verbal memory
mpairment in the language-dominant hemisphere. Stereo-act Funct Neurosurg 2003; 80: 18-21.
ori T, Yamane F, Ochiai T, et al. Selective subtemporalmygdalohippocampectomy for refractory temporal lobepilepsy: operative and neuropsychological outcomes. Jeurosurg 2007; 106: 134-41.
ones-Gotman M, Smith ML, Zatorre RJ. Neuropsychologi-al testing for localizing and lateralizing the epileptogenicegion. In: Engel J. Surgical treatment of the epilepsies. Nework: Raven Press, 1993: 245-62.
ones-Gotman M, Zatorre RJ, Olivier A, et al. Learning andetention of words and designs following excision from
edial or lateral temporal-lobe structures. Neuropsycholo-ia 1997; 35: 963-73.
oo EY, Han HJ, Lee EK, et al. Resection extent versus postop-rative outcomes of seizure and memory in mesial temporal
obe epilepsy. Seizure 2005; 14: 541-51.
osephson CB, Dykeman J, Fiest KM, et al. Systematic reviewnd meta-analysis of standard vs selective temporal lobepilepsy surgery. Neurology 2013; 80: 1669-76.
atz A, Awad IA, Kong AK, et al. Extent of resection in temporalobectomy for epilepsy. II. Memory changes and neurologic
237
omplications. Epilepsia 1989; 30: 763-71.
oepp MJ, Woermann FG. Imaging structure and function inefractory focal epilepsy. Lancet Neurol 2005; 4: 42-53.
angfitt JT, Westerveld M, Hamberger MJ, et al. Worsening ofuality of life after epilepsy surgery: effect of seizures andemory decline. Neurology 2007; 68: 1988-94.

2
C
Lte
Lca3
LrJ
LChaf
MRfipB
Mpfr
Mct2
Ota
Pocs
PNr3
PRbe
REs
Rtp1
Sb
Sss
Sq2
StiN
Srr
SrN
Sr
SPp
Tfa
Taht
TWe2
Tre
VRfs
vHav
Wue
WcE
Wt
. Helmstaedter
endt M, Helmstaedter C, Elger CE. Pre- and postopera-ive socioeconomic development of 151 patients with focalpilepsies. Epilepsia 1997; 38: 1330-7.
oGalbo A, Sawrie S, Roth DL, et al. Verbal memory out-ome in patients with normal preoperative verbal memorynd left mesial temporal sclerosis. Epilepsy Behav 2005; 6:37-41.
oring DW, Strauss E, Hermann BP, et al. Differential neu-opsychological test sensitivity to left temporal lobe epilepsy.Int Neuropsychol Soc 2008; 14: 394-400.
utz MT, Clusmann H, Elger CE, Schramm J, Helmstaedter. Neuropsychological outcome after selective amygdalo-ippocampectomy with transsylvian versus transcorticalpproach: a randomized prospective clinical trial of surgeryor temporal lobe epilepsy. Epilepsia 2004; 45: 809-16.
cConley R, Martin R, Palmer CA, Kuzniecky R, Knowlton, Faught E. Rey Osterrieth complex figure test spatial andgural scoring: relations to seizure focus and hippocampalathology in patients with temporal lobe epilepsy. Epilepsyehav 2008; 13: 174-7.
ikuni N, Miyamoto S, Ikeda A, et al. Subtemporal hip-ocampectomy preserving the basal temporal language area
or intractable mesial temporal lobe epilepsy: preliminaryesults. Epilepsia 2006; 47: 1347-53.
orino M, Uda T, Naito K, et al. Comparison of neuropsy-hological outcomes after selective amygdalohippocampec-omy versus anterior temporal lobectomy. Epilepsy Behav006; 9: 95-100.
jemann GA, Dodrill CB. Verbal memory deficits after leftemporal lobectomy for epilepsy. Mechanism and intraoper-tive prediction. J Neurosurg 1985; 62: 101-7.
aglioli E, Palmini A, Portuguez M, et al. Seizure and mem-ry outcome following temporal lobe surgery: selectiveompared with nonselective approaches for hippocampalclerosis. J Neurosurg 2006; 104: 70-8.
auli E, Pickel S, Schulemann H, Buchfelder M, Stefan H.europsychologic findings depending on the type of the
esection in temporal lobe epilepsy. Adv Neurol 1999; 81:71-7.
iguet O, Saling MM, O’Shea MF, Berkovic SF, Bladin PF.ey figure distortions reflect nonverbal recall differencesetween right and left foci in unilateral temporal lobepilepsy. Arch Clin Neuropsychol 1994; 9: 451-60.
ausch R, Kraemer S, Pietras CJ, Le M, Vickrey BG, PassaroA. Early and late cognitive changes following temporal lobeurgery for epilepsy. Neurology 2003; 60: 951-9.
enowden SA, Matkovic Z, Adams CB, et al. Selec-ive amygdalohippocampectomy for hippocampal sclerosis:ostoperative MR appearance. AJNR Am J Neuroradiol
38
995; 16: 1855-61.
aling MM. Verbal memory in mesial temporal lobe epilepsy:eyond material specificity. Brain 2009; 132: 570-82.
awrie SM, Martin RC, Kuzniecky R, et al. Subjective ver-us objective memory change after temporal lobe epilepsyurgery. Neurology 1999; 53: 1511-7.
S
WF
WtN
chramm J. Temporal lobe epilepsy surgery and theuest for optimal extent of resection: a review. Epilepsia008; 49(8): 1296-307.
chramm J, Lehmann TN, Zentner J, et al. Randomized con-rolled trial of 2.5-cm versus 3.5-cm mesial temporal resectionn temporal lobe epilepsy-Part 1: intent-to-treat analysis. Acta
eurochir (Wien) 2011; 153: 209-19.
herman EM, Wiebe S, Fay-McClymont TB, et al. Neu-opsychological outcomes after epilepsy surgery: systematiceview and pooled estimates. Epilepsia 2011; 52: 857-69.
mith ML, Milner B. Right hippocampal impairment in theecall of spatial location: encoding deficit or rapid forgetting?europsychologia 1989; 27: 71-81.
tern Y. The concept of cognitive reserve: a catalyst foresearch. J Clin Exp Neuropsychol 2003; 25: 589-93.
troup E, Langfitt J, Berg M, McDermott M, Pilcher W, Como. Predicting verbal memory decline following anterior tem-oral lobectomy (ATL). Neurology 2003; 60: 1266-73.
akaya S, Mikuni N, Mitsueda T, et al. Improved cerebralunction in mesial temporal lobe epilepsy after subtemporalmygdalohippocampectomy. Brain 2009; 132: 185-94.
anriverdi T, Dudley RW, Hasan A, et al. Memory outcomefter temporal lobe epilepsy surgery: corticoamygdalo-ippocampectomy versus selective amygdalohippocampec-
omy. J Neurosurg 2010; 113: 1164-75.
ellez-Zenteno JF, Hernandez Ronquillo L, Moien-Afshari F,iebe S. Surgical outcomes in lesional and non-lesional
pilepsy: a systematic review and meta-analysis. Epilepsy Res010; 89: 310-8.
rebuchon-Da Fonseca A, Guedj E, Alario FX, et al. Brainegions underlying word finding difficulties in temporal lobepilepsy. Brain 2009; 132: 2772-84.
elasco AL, Velasco F, Velasco M, Trejo D, Castro G, Carrillo-uiz JD. Electrical stimulation of the hippocampal epileptic
oci for seizure control: a double-blind, long-term follow-uptudy. Epilepsia 2007; 48: 1895-903.
on Rhein B, Nelles M, Urbach H, Von Lehe M, Schramm J,elmstaedter C. Neuropsychological outcome after selective
mygdalohippocampectomy: subtemporal versus transsyl-ian approach. J Neurol Neurosurg Psychiatry 2012; 83: 887-93.
ellmer J, Weber C, Mende M, et al. Multitask electrical stim-lation for cortical language mapping: hints for necessity andconomic mode of application. Epilepsia 2009; 50: 2267-75.
iebe S, Blume WT, Girvin JP, Eliasziw M. A randomized,ontrolled trial of surgery for temporal-lobe epilepsy. Newngl J Med 2001; 345: 311-8.
ieser HG, Yasargil MG. Selective amygdalohippocampec-omy as a surgical treatment of mesiobasal limbic epilepsy.
Epileptic Disord, Vol. 15, No. 3, September 2013
urg Neurol 1982; 17: 445-57.
itt JA, Helmstaedter C. Neuropsychology in epilepsy.ortschr Neurol Psychiatr 2009a; 77: 691-8.
itt JA, Helmstaedter C. Neuropsychology in epilepsy Part II:owards an establishment of diagnostic guidelines. Fortschreurol Psychiatr 2009b; 77: 691-8.

E
Wbcc
WM
pileptic Disord, Vol. 15, No. 3, September 2013
itt JA, Bodner T, Bruckner K, et al. Is there a commonasis for establishing guidelines for the neuropsychologi-al assessment in epilepsy? A survey across German epilepsyentres. Epilepsia 2009; 50: 45.
olf RL, Ivnik RJ, Hirschorn KA, Sharbrough FW, Cascino GD,arsh WR. Neurocognitive efficiency following left temporal
l1
Wrrd
Cognitive outcome and surgery in TLE
239
obectomy: standard versus limited resection. J Neurosurg993; 79: 76-83.
yler AR, Hermann BP, Somes G. Extent of medial temporalesection on outcome from anterior temporal lobectomy: aandomized prospective study. Neurosurgery 1995; 37: 982-90;iscussion: 90-1.