cognitive bias and clinical decision making · 2019-10-07 · dual process theory pathways •type...
TRANSCRIPT

Cognitive Bias and
Clinical Decision Making Educational Strategies
JERRY ERICKSON, DMSC, PA-C, DFAAPADAVID KLOCKO, MPAS, PA-C
2019 PAEA EDUCATIONAL FORUM

Learning Objectives:
• By the end of the session, the participant should be able to:
• Describe the common types and prevalence of cognitive biases found in medicine.
• Discuss different consequences of utilizing cognitive biases.
• Describe how to recognize and detect cognitive self-biases.
• Explain effective approaches and specific strategies to deal with cognitive bias and instruction.
• Discuss educational intervention on cognitive biases and debiasing strategies to improve the ability of physician assistant students to make clinical decisions.
• Recognize the importance of willingness to be innovative and collaborative to create new methodologies to incorporate into curriculum.

This presentation will use audience response system (ARS) by
•When Poll is active, please go to PollEv.com/
- Or
•Text to 37607 once to join

Cognitive Bias•Defined as an error in judgment, memory, decision-making, evaluation, or other cognitive process, usually happening by retaining personal beliefs and preferences in the presence of differing evidence
Cherry K. How Cognitive Biases Influence How You Think and Act. https://www.verywellmind.com/what-is-a-cognitive-bias-2794963 Updated November 6, 2018. Accessed November 23, 2018.

What cognitive biases exist in medicine?
•There are over 100 types of cognitive bias identified in the general literature, and at least 38 in the medical literature
•19 identified in one systematic review
Saposnik G, Relemeier D, Ruff C, Tobler P. Cognitive biases associated with medical decisions: a systematic review BMC Medical Informatics and Decision Making (2016) 16:138.

Benson B, Manoogian J. Cognitive Bias Codex. https://ritholtz.com/wp-content/uploads/2016/09/1-71TzKnr7bzXU_l_pU6DCNA.jpeg. Accessed August 1, 2019.

Cognitive Bias Infographic. Raconteur.net. http://rcnt.eu/7wk5c. Accessed August 1, 2019.

Most common cognitive biases in medicine•Anchoring• Anchoring bias is compounded by
confirmation bias
•Availability
•Overconfidence
• Low Tolerance to RiskSaposnik G, Relemeier D, Ruff C, Tobler P. Cognitive biases associated with medical decisions: a systematic review BMC Medical Informatics and Decision Making (2016) 16:138.
What is the problem?•Cognitive bias in clinical decision making contributes up to 28 percent of diagnostic errors in medicine.• Post-mortem study found:• 8% Class 1 errors
• 28% of all cases had ≥ 1 diagnostic error
Cognitive biases in health care. 28 1-3. https://www.jointcommission.org/assets/1/23/Quick_Safety_Issue_28_Oct_2016.pdf. Published October 2016, accessed July 22, 2018.
Winters B, Custer J, Galvagno SM, Colantuoni E, Kapoor SG, Lee H, Goode V, Robinson K, Nakhasi A, Pronovost P. Diagnostic errors in the intensive care unit: A systematic review of autopsy studies. BMJ Quality and Safety. 2012;21(11):894–902.

What is the other problem?•A literature search describing strategies and methods to educate students and clinicians about biases in medical education reveals very little results.
•Diagnostic safety is not sufficiently promoted and taught in graduate medical programs.
Reilly JB, Ogdie AR, Feldt JMV, Myers JS. Teaching about how doctors think: a longitudinal curriculum in cognitive bias and diagnostic error forresidents. BMJ Quality & Safety. 2013;22(12):1044-1050. doi:10.1136/bmjqs-2013-001987.
Graber ML, Rencic J, Rusz, D et al. Improving diagnosis by improving education: a policy brief on education in healthcare professions. Diagnosis, 2018;5(3):107-118. doi:10.1515/dx-2018-0033

What is the solution?•There is a need to start a deliberation of evidence-based methods and strategies to be incorporated into medical education to recognize and respond to specific cognitive biases
Critical Thinking and Clinical Decision Making

Critical Thinking• Dictionary definition:• The objective analysis and evaluation of an issue in order to
form a judgment.
• The Foundation for Critical Thinking:• Critical thinking is the intellectually disciplined process of
actively and skillfully conceptualizing, applying, analyzing, synthesizing, and/or evaluating information gathered from, or generated by, observation, experience, reflection, reasoning, or communication, as a guide to belief and action.
Dictionary.com definition https://www.dictionary.com/browse/critical-thinking?s=t
https://www.criticalthinking.org/pages/defining-critical-thinking/766

Clinical Decision Making
• Skill that health care providers use every day• Mastery of this ability is honed over time
• Developing in students • Not routinely and commonly formalized in the
medical education literature• Hidden curriculum
Hafferty FW, Beyond curriculum reform: confronting medicine’s hidden curriculum. Academic Medicine: 1998 Apr;73(4):403-7.
Dual Process Theory
Dual Process Theory
• Cognitive psychology• Decision-making process
• Two types of pathways
• Well-known and frequently used model for diagnostic reasoning and clinical decision making
Graber ML, Rencic J, Rusz, D et al. Improving diagnosis by improving education: a policy brief on education in healthcare professions. Diagnosis, 2018;5(3):107-118. doi:10.1515/dx-2018-0033.

Dual Process Theory Pathways• Type 1
• Intuitive, fast, effortless with automaticity and are based on associations of similar actions in memory
• Implicit or intuitive processes
• Type 2
• Deliberate, slow, non-programmed, conscious and occur with analysis, effort and logic
• Explicit processesLakoff G, Johnson M. Philosophy in the Flesh: The Embodied Mind and Its Challenge to Western Thought. New York, NY: Basic Books; 1999.
Saposnik G, Relemeier D, Ruff C, Tobler P. Cognitive biases associated with medical decisions: a systematic review BMC Medical Informatics and Decision Making (2016) 16:138.

Pathway examples
•Type 1
Kahneman D. Thinking, Fast and Slow. New York, NY; Farrar, Straus and Giroux; 2011.

Pathway examples
• Type 2
412 x 8 = ___________
Kahneman D. Thinking, Fast and Slow. New York, NY; Farrar, Straus and Giroux; 2011.

Pathway example questions
• What is your diagnosis?

Pathway example questions
• How quickly did you come up with an answer?
• Type I mode?
• Type 2 mode?
https://commons.wikimedia.org/wiki/File:Herpes_zoster_3days_passed.jpg

Pathway example questions
• What is your diagnosis?

Pathway example questions
• How quickly did you come up with an answer?
• Type I mode?
• Type 2 mode?
https://commons.wikimedia.org/wiki/File:Chest_radiograph_in_influensa_and_H_influenzae,_posteroanterior.jpg
Poll Everywhere Question
•Type 1 or Type 2

Multi-Level Processing• Alternating between Type 1 and Type 2• Override of faster Type 1 with uncertainty
• Gained Knowledge, experience & time • Type 1 more dominant
• Collection of pattern recognitions• Trigger switch from Type 1 to Type 2
Lakoff G, Johnson M. Philosophy in the Flesh: The Embodied Mind and Its Challenge to Western Thought. New York, NY: Basic Books; 1999.
Norman G, Young M, Brooks L. Non-analytical models of clinical reasoning: the role of experience. Medical Education. 2007. doi:10.1111/j.1365-2923.2007.02914.x.
Types of Cognitive Biases
Saposnik G, Relemeier D, Ruff C, Tobler P. Cognitive biases associated with medical decisions: a systematic review BMC Medical Informatics and Decision Making (2016) 16:138.

Most common cognitive biases
•Anchoring• Anchoring bias is compounded by confirmation bias
•Availability
•Overconfidence
• Low Tolerance to Risk

Anchoring Bias
• The tendency of locking on to a diagnosis early on and failure to adjust with new information
• Example:• Diagnosing and treating for GABHS with sore
throat, fever and tonsillar exudate. Patient had cough, no LAD, and was 20 y/o

Confirmation Bias (as commonly tied to Anchoring)
• The tendency to search for evidence to
support a diagnosis rather than to disprove it
• Example:• Same patient that was diagnosed and treated
for GABHS. RAST negative, Culture negative

Availability Bias
•The tendency to choose a diagnosis if
easily comes to mind with frequently
occurring
•Example:• 3 previous patients with similar symptoms

Overconfidence Bias
•The tendency to over evaluate one’s
own knowledge, judgement, skills
•Example:• Medically treating a choledocholithiasis without surgeon referral
Low Tolerance to Risk or Ambiguity Bias
•The avoidance of decisions when probability
(knowledge or ability to obtain) is unknown
•Example:• Patient presents with fever and joint pains after a cruise in the Caribbean and you diagnose influenza without checking for Chikungunya

Current Strategies of Debiasing Techniques

Current Strategies of Debiasing Techniques
•Two major strategies•Cognitive 41.1%
•Technological 37.9%
Ludolph R, Schulz P. Debiasing Health-Related Judgments and Decision Making: A Systematic Review. Medical Decision Making. 2018;38(1), 3–13. https://doi.org/10.1177/0272989X17716672.
Cognitive Debiasing Techniques
•Two major principles•Awareness and recognition• Self-evaluation exist?
•Utilizing Type 2 processes• Override Type 1 processes
Ludolph R, Schulz P. Debiasing Health-Related Judgments and Decision Making: A Systematic Review. Medical Decision Making. 2018;38(1), 3–13. https://doi.org/10.1177/0272989X17716672.

Technological Debiasing Techniques•Current• Cognitive Tutoring Systems• Simulation Training• Decision Support Systems
•Other• Forcing functions• Check lists
Croskerry P, Singhal G, Mamede S. Cognitive debiasing 2: impediments to and strategies for change. BMJ Quality & Safety. 2013;22(Suppl 2):ii65-ii72. doi:10.1136/bmjqs-2012-001713.
Chew KS, Durning SJ, van Merriënboer JJ. Teaching metacognition in clinical decision-making using a novel mnemonic checklist: an exploratory study. Singapore Med J. 2016;57(12):694–700. doi:10.11622/smedj.2016015
Ely JW, Graber ML, Croskerry P. Checklists to Reduce Diagnostic Errors. Acad Med. 2011;86(3):307-313. doi:10.1097/acm.0b013e31820824cd.

Current Debiasing Techniques Effectiveness
•Overall 69%•Technological 89.7%
•Cognitive 50%
•Teaching students 71.4%
•Advantageous
Ludolph R, Schulz P. Debiasing Health-Related Judgments and Decision Making: A Systematic Review. Medical Decision Making. 2018;38(1), 3–13. https://doi.org/10.1177/0272989X17716672.

•Technological 89.7%
•Cognitive 50%
•Teaching students 71.4%•Advantageous
Ludolph R, Schulz P. Debiasing Health-Related Judgments and Decision Making: A Systematic Review. Medical Decision Making. 2018;38(1), 3–13. https://doi.org/10.1177/0272989X17716672.
Current Debiasing Techniques Effectiveness

Current Debiasing Technique Challenges•Cost $$
• Time to learn and master EMR!?
• Provider reluctance• Deemed unnecessary
• Hmmmm- what kind of BIAS is that?
Ludolph R, Schulz P. Debiasing Health-Related Judgments and Decision Making: A Systematic Review. Medical Decision Making. 2018;38(1), 3–13. https://doi.org/10.1177/0272989X17716672.

Recognizing and Detecting Cognitive Self-Biases

Recognizing and Detecting Cognitive Self-Biases
•How do we recognize bias in our self?
•Recognize in others much easier
•Self-reflection and awareness
•Metacognition
•Different techniques• Observing known biases (cases/clinical) and giving:• Self-reflections
• Evaluations of self, others
• Feedback
Recognizing and Detecting Cognitive Self-Biases

•Case Scenarios/Vignettes
• Two of them
•Will show a case and then have an ARS question to follow
Recognizing and Detecting Cognitive Self-Biases

Case #1 follow up question
•Given the information at hand, what are the major concerns about this case?
Case #2 follow up question
•Given the information at hand, what are the major concerns about this case?

Proposed Educational Methodology and Strategy
Putting into curriculum
•Cognitive debiasing • Critical thinking techniques and strategies found in literature
• Earlier introduction to components and methodologies • Using the didactic and clinical model
Graber ML, Rencic J, Rusz, D et al. Improving diagnosis by improving education: a policy brief on education in healthcare professions. Diagnosis, 2018;5(3):107-118. doi:10.1515/dx-2018-0033.

Curriculum content and approaches• ↑ knowledge base
• Optimize clinical reasoning
• Understand system-related aspects of care
• Engaging patients & members of the diagnostic team
• ↑perspectives and attitudes Graber ML, Rencic J, Rusz, D et al. Improving diagnosis by improving education: a policy brief on education in healthcare professions. Diagnosis, 2018;5(3):107-118. doi:10.1515/dx-2018-0033.

Evaluation and data
•All topics will be assessed for an outcome
•Evaluation tools designed to:• Align with the program competency domains
• Course outcomes
• Accreditation standards

Curriculum Example of Proposed Educational Methodology and Strategy
•Didactic Year• First Semester Didactic• Evidence-based medicine course to be delivered early in
curriculum. It is imperative for students to be able to acquire and effectively use a relevant knowledge base
• Introduce concepts of critical thinking and metacognition early in didactic curriculum
Curriculum Example of Proposed Educational Methodology and Strategy
•Didactic Year• Second and Third Semester Didactic• Introduce the clinical decision making processes in a
clinical medicine or problem based learning course with evidence-based medicine clinical reasoning
• Introduce concept of diagnostic safety
• Emphasize system-related aspects of care and how they can contribute to errors

Curriculum Example of Proposed Educational Methodology and Strategy
•Didactic Year• Fourth Semester Didactic• Introduce cognitive biases, how they are tied into
diagnostic errors and techniques/strategies to minimize in a clinical medicine or problem based learning course
• Case vignettes to review and give reflections/evaluations/ and feedbacks
• Develop objective structured clinical examination(OSCE) cases to assess student’s ability of identification and displaying techniques to avoid

Curriculum Example of Proposed Educational Methodology and Strategy
•Clinical Year• End of Rotation callbacks• As a part of supervised clinical practice
experiences(SCPE) assignments, having to write a reflection essay of biases they have seen, been a part of, and techniques used

Curriculum Example of Proposed Educational Methodology and Strategy
•Clinical Year• Summative evaluation• As a part of summative evaluation with a two part
assessment of competency, the student will have a written examination and an OSCE with common biases to identify and address with de-biasing technique

Accreditation Standard Mapping from version 5
ARC-PA Relevant StandardsB1.07 The curriculum must include instruction related
to the development of problem solving and
medical decision-making skills
Accreditation Standards for Physician Assistant Education, Fifth Edition. Accreditation Review Commission on Education for the Physician Assistant, Inc. http://www.arc-pa.org/wp-content/uploads/2018/10/ARC-PA.DRAFT5th-edit-Revised-Stds-CLEAN-version.10.2018-2.pdf. Effective January 1, 2020. Accessed November 1, 2018.

Accreditation Standard Mapping from version 5
ARC-PA Relevant StandardsB2.13 The program curriculum must include instruction
in risk reduction including:
a) patient safety,
b) prevention of medical errors,
c) quality improvement, and
d) risk management.
Accreditation Standards for Physician Assistant Education, Fifth Edition. Accreditation Review Commission on Education for the Physician Assistant, Inc. http://www.arc-pa.org/wp-content/uploads/2018/10/ARC-PA.DRAFT5th-edit-Revised-Stds-CLEAN-version.10.2018-2.pdf. Effective January 1, 2020. Accessed November 1, 2018.

Accreditation Standard Mapping from version 5ARC-PA Relevant Standards
B4.05 The program must conduct and document a summative
evaluation of each student within the final four months
of the program to verify that each student meets the
program competencies required to enter clinical practice,
including:
a) clinical and technical skills,
b) clinical reasoning and problem-solving skills,
c) knowledge,
d) interpersonal skills, and
e) professionalism. Accreditation Standards for Physician Assistant Education, Fifth Edition. Accreditation Review Commission on Education for the Physician Assistant, Inc. http://www.arc-pa.org/wp-content/uploads/2018/10/ARC-PA.DRAFT5th-edit-Revised-Stds-CLEAN-version.10.2018-2.pdf. Effective January 1, 2020. Accessed November 1, 2018.
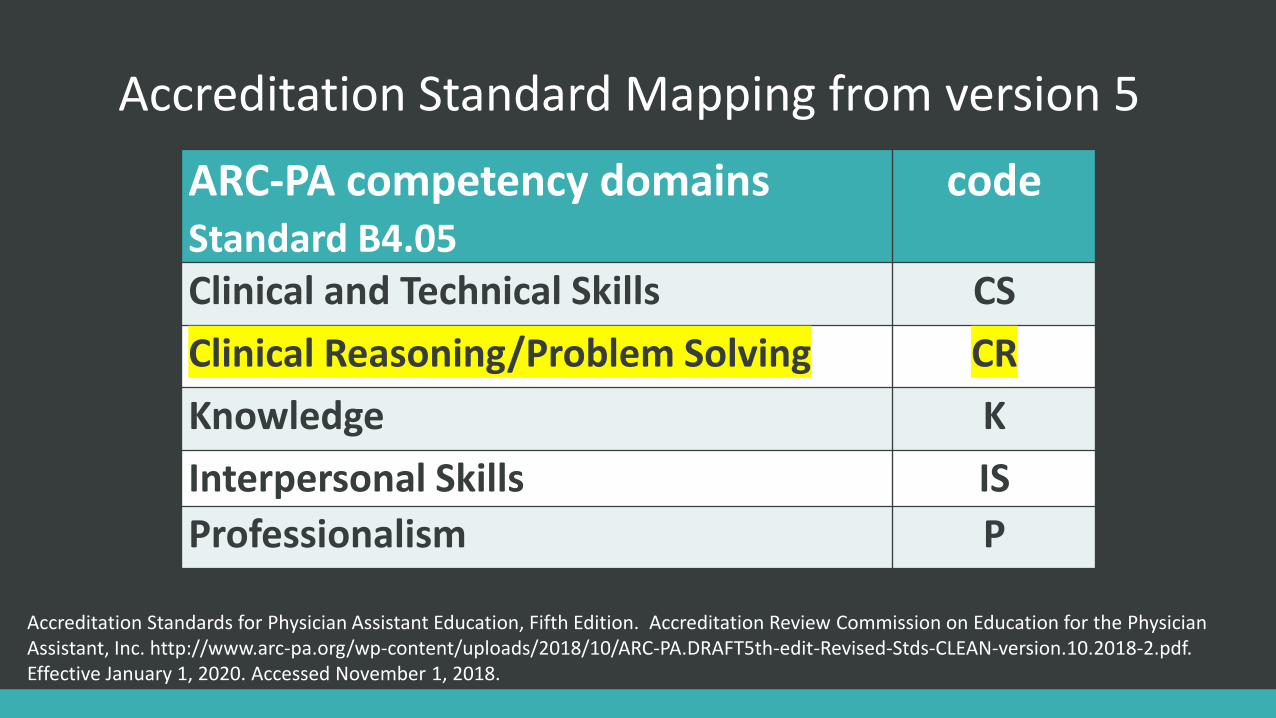
Accreditation Standard Mapping from version 5
ARC-PA competency domains Standard B4.05
code
Clinical and Technical Skills CS
Clinical Reasoning/Problem Solving CR
Knowledge K
Interpersonal Skills IS
Professionalism P
Accreditation Standards for Physician Assistant Education, Fifth Edition. Accreditation Review Commission on Education for the Physician Assistant, Inc. http://www.arc-pa.org/wp-content/uploads/2018/10/ARC-PA.DRAFT5th-edit-Revised-Stds-CLEAN-version.10.2018-2.pdf. Effective January 1, 2020. Accessed November 1, 2018.

Accreditation Standard Mapping from version 5
4 PA Organizations Competencies and coding to DomainsPatient Care CR, K, CS, IS, PMedical Knowledge and Skills K, CSInterpersonal Communication ISSystem-Based Practice CR, K, CS, IS, PPractice Based & Lifelong Learning CR, K, CS, IS, PProfessionalism P
Accreditation Standards for Physician Assistant Education, Fifth Edition. Accreditation Review Commission on Education for the Physician Assistant, Inc. http://www.arc-pa.org/wp-content/uploads/2018/10/ARC-PA.DRAFT5th-edit-Revised-Stds-CLEAN-version.10.2018-2.pdf. Effective January 1, 2020. Accessed November 1, 2018.
Conclusion
• Cognitive bias
•Need to be:• Cognizant
• Vigilant
•Educating Students • Existence and impact on patient care
• How to avoid them

Thank youQUESTIONS?

References1. Cherry K. How Cognitive Biases Influence How You Think and Act. https://www.verywellmind.com/what-is-a-cognitive-
bias-2794963 Updated November 6, 2018. Accessed November 23, 2018.
2. Saposnik G, Relemeier D, Ruff C, Tobler P. Cognitive biases associated with medical decisions: a systematic review BMC Medical Informatics and Decision Making (2016) 16:138.
3. The Joint Commission: Quick safety: Cognitive biases in health care. 28 1-3. https://www.jointcommission.org/assets/1/23/Quick_Safety_Issue_28_Oct_2016.pdf. Published October 2016, accessed July 22, 2018.
4. Winters B, Custer J, Galvagno SM, Colantuoni E, Kapoor SG, Lee H, Goode V, Robinson K, Nakhasi A, Pronovost P. Diagnostic errors in the intensive care unit: A systematic review of autopsy studies. BMJ Quality and Safety. 2012;21(11):894–902.
5. Reilly JB, Ogdie AR, Von Feldt JM, et al Teaching about how doctors think: a longitudinal curriculum in cognitive bias and diagnostic error for residents BMJ Qual Saf 2013;22:1044-1050.
6. Dictionary.com. Critical Thinking Definition. https://www.dictionary.com/browse/critical-thinking?s=t Accessed 8/12/2019
7. The Foundation for Critical Thinking. Critical Thinking Definition. https://www.criticalthinking.org/pages/defining-critical-thinking/766 Accessed 8/12/2019.
8. Hafferty FW, Beyond curriculum reform: confronting medicine’s hidden curriculum. Academic Medicine: 1998 Apr;73(4):403-7.
9. Graber ML, Rencic J, Rusz, D et al. Improving diagnosis by improving education: a policy brief on education in healthcare professions. Diagnosis, 2018;5(3):107-118. doi:10.1515/dx-2018-0033.
10. Lakoff G, Johnson M. Philosophy in the Flesh: The Embodied Mind and Its Challenge to Western Thought. New York, NY: Basic Books; 1999.

References11. Kahneman D. Thinking, Fast and Slow. New York, NY; Farrar, Straus and Giroux; 2011.
12. Norman G, Young M, Brooks L. Non-analytical models of clinical reasoning: the role of experience. Medical Education. 2007. doi:10.1111/j.1365-2923.2007.02914.x.
13. Ludolph R, Schulz P. Debiasing Health-Related Judgments and Decision Making: A Systematic Review. Medical Decision Making. 2018;38(1), 3–13. https://doi.org/10.1177/0272989X17716672.
14. Croskerry P, Singhal G, Mamede S. Cognitive debiasing 2: impediments to and strategies for change. BMJ Quality & Safety. 2013;22(Suppl 2):ii65-ii72. doi:10.1136/bmjqs-2012-001713.
15. Chew KS, Durning SJ, van Merriënboer JJ. Teaching metacognition in clinical decision-making using a novel mnemonic checklist: an exploratory study. Singapore Med J. 2016;57(12):694–700. doi:10.11622/smedj.2016015
16. Ely JW, Graber ML, Croskerry P. Checklists to Reduce Diagnostic Errors. Acad Med. 2011;86(3):307-313. doi:10.1097/acm.0b013e31820824cd.
17. Accreditation Standards for Physician Assistant Education, Fifth Edition. Accreditation Review Commission on Education for the Physician Assistant, Inc. http://www.arc-pa.org/wp-content/uploads/2018/10/ARC-PA.DRAFT5th-edit-Revised-Stds-CLEAN-version.10.2018-2.pdf. Effective January 1, 2020. Accessed November 1, 2018.
18. Benson B, Manoogian J. Cognitive Bias Codex. https://ritholtz.com/wp-content/uploads/2016/09/1-71TzKnr7bzXU_l_pU6DCNA.jpeg. Accessed August 1, 2019.
19. Cognitive Bias Infographic. Raconteur.net. http://rcnt.eu/7wk5c. Accessed August 1, 2019.