cochlear implants & multiple disabilities: what we’ve learned so far
DESCRIPTION
Cochlear Implants & Multiple Disabilities: What We’ve Learned So Far. Ella L. Taylor Western Oregon University Susan M. Bashinski University of Kansas 2008 Council for Exception Children Conference Boston, MA. Session Goals. - PowerPoint PPT PresentationTRANSCRIPT
Cochlear Implants & Multiple Disabilities: What We’ve Learned So Far
Ella L. TaylorWestern Oregon University
Susan M. BashinskiUniversity of Kansas
2008 Council for Exception Children ConferenceBoston, MA
Session GoalsStatus of research on children
with multiple disabilities and cochlear implants
Challenges of working with multiple partners
Characteristics of children with deaf-blindness who have cochlear implants
Impact of CI on communication
Trends in Cochlear Implantation
FDA continues to lower the age of eligibility for receiving a cochlear implant
Cochlear implant centers are reporting a dramatic increase in the number of bilateral implants
CI technology continues to advance (i.e., the number of implant channels, amount of damage done to ear physiology by implant, etc.)
Research on CI & Multiple ImpairmentsEdwards (2007) reviews the small
amount of research focusing on CI and children with multiple disabilities
General findings from her examination:◦Cognitive functioning is one of the strongest
predictors of progress in developing speech perception and speech production
◦Parents report satisfaction with CI due to increased eye contact, awareness of the environment and response to requests.
Trends in Results of Cochlear Implantation (HI only)
Earlier ages for implantation are associated with more significant, and rapid, progress
Variability in outcomes continues to exist, especially for children who receive implants at older ages
Orally-focused post-implant habilitation is, generally, associated with more positive outcomes than is total communication
Importance of This Research ProjectStates across the country are
reporting:
A significant increase in the number of children with DB receiving implants
Increasing numbers of children with multiple disabilities receiving implants
Importance of This Research ProjectCurrent extant literature base
nearly entirely reports data re: cochlear implants with children who are deaf
Very limited data exist regarding post-implant outcomes for children with deaf-blindness
Outcomes with children who are deaf are NOT transferable to children with deaf-blindness
PurposeThe overall purpose of this
project is NEITHER to: encourage families of children who have DB to seek out an implant
NOR to discourage families from doing so.
The purpose of the study is to establish a database that
families, in the future, might consult to make more informed decisions.

Research Partners
Deaf-Blind Services Projects in 22 states (AZ, CA, CT, DE, FL, GA, IL, KS, KY, MA, MD, MN, MO, NC, NE, NJ, NY, OH, OK, OR, PA, TX)
Cochlear Implant Centers: Midwest Ear Institute (Kansas City, MO) Cincinnati Children’s Hospital (Ohio) Boys’ Town National Research Hospital
(Omaha, NE)
ChallengesNumerous collaborative partners
exacerbate the challenge of compliance with IRB requirements
Completion of subcontracts and / or collaborative agreements has had a negative impact on ID & consent with participants
Identification and assessment of pre-implant participants has been difficult because of health and scheduling variables
Assessment PackageCIDB Project Demographic Survey
MacArthur-Bates Communicative Development Inventories Words & Gestures Words & Sentences
Communication & Symbolic Behavior Scales Developmental Profile (CSBS-DP)
Reynell-Zinkin Developmental Scales for Young Children with Visual Impairments
Speech Intelligibility Rubric
C-SIM
Assessment Schedule
Participants are divided into three groups, for purposes of assessment:
Pre-implant Post-implant
Implant less than seven years Implant for seven years or longer
Assessment schedule varies according to the amount of time the child has had a cochlear implant
ParticipantsDemographics reported here are in regard to 63 participants:
Chronological age: 13 mos. to 12 yrs. 7 mos.
Gender: 64% male, 36% female
Ethnicity: 70% Caucasian 13% Latino 13% African-American 2% Native American 3% Other
Prematurity : 1 out of every 2 born prematurely
CI Status: Pre-implant (19%), Post-implant (81%)
47% were premature
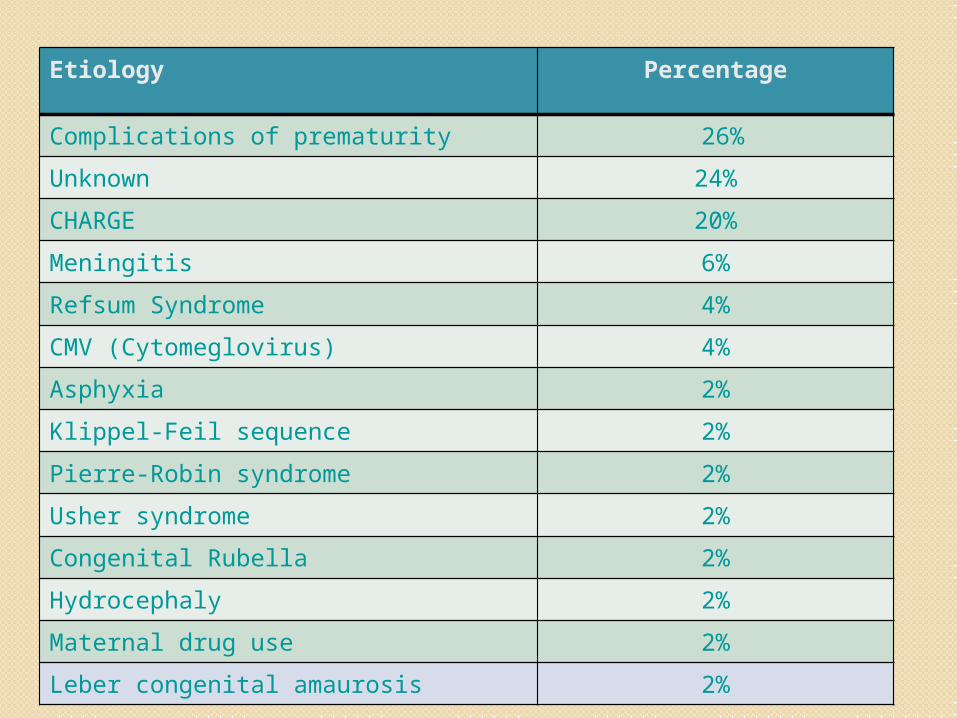
Etiology Percentage
Complications of prematurity 26%
Unknown 24%
CHARGE 20%
Meningitis 6%
Refsum Syndrome 4%
CMV (Cytomeglovirus) 4%
Asphyxia 2%
Klippel-Feil sequence 2%
Pierre-Robin syndrome 2%
Usher syndrome 2%
Congenital Rubella 2%
Hydrocephaly 2%
Maternal drug use 2%
Leber congenital amaurosis 2%
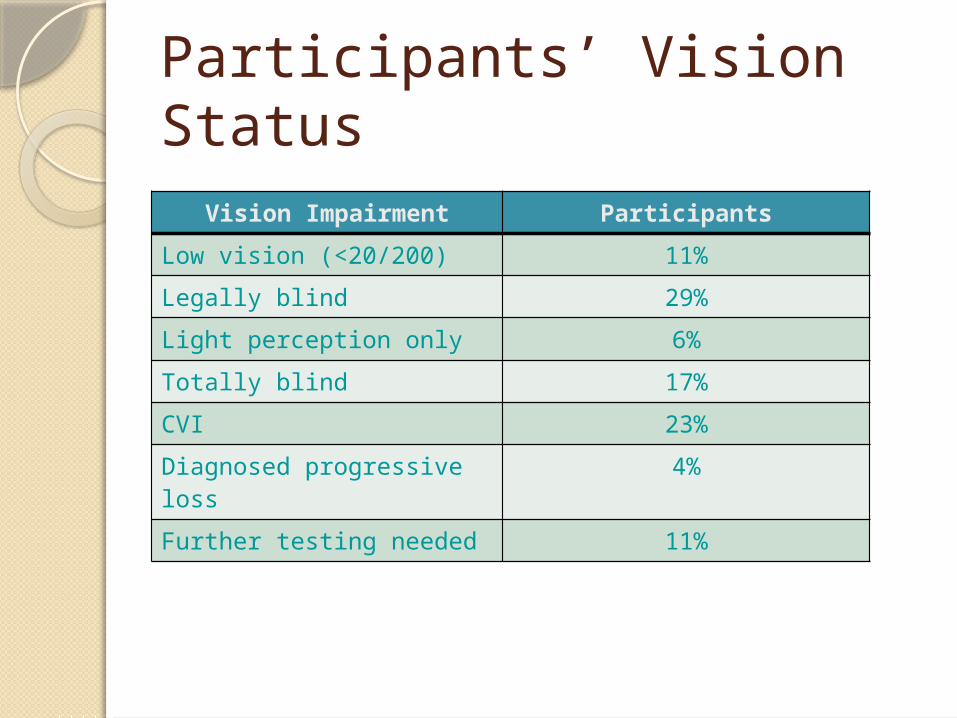
Participants’ Vision Status
Vision Impairment Participants
Low vision (<20/200) 11%
Legally blind 29%
Light perception only 6%
Totally blind 17%
CVI 23%
Diagnosed progressive loss
4%
Further testing needed 11%
Participants’ Hearing StatusALL participants have severe or
profound hearing loss-MUST have to qualify for cochlear implant
76% born with hearing impairment
6% of those tested diagnosed with central auditory processing disorder (CAPD)
27% of those tested diagnosed with auditory neuropathy (AN)
Six children have bilateral CI
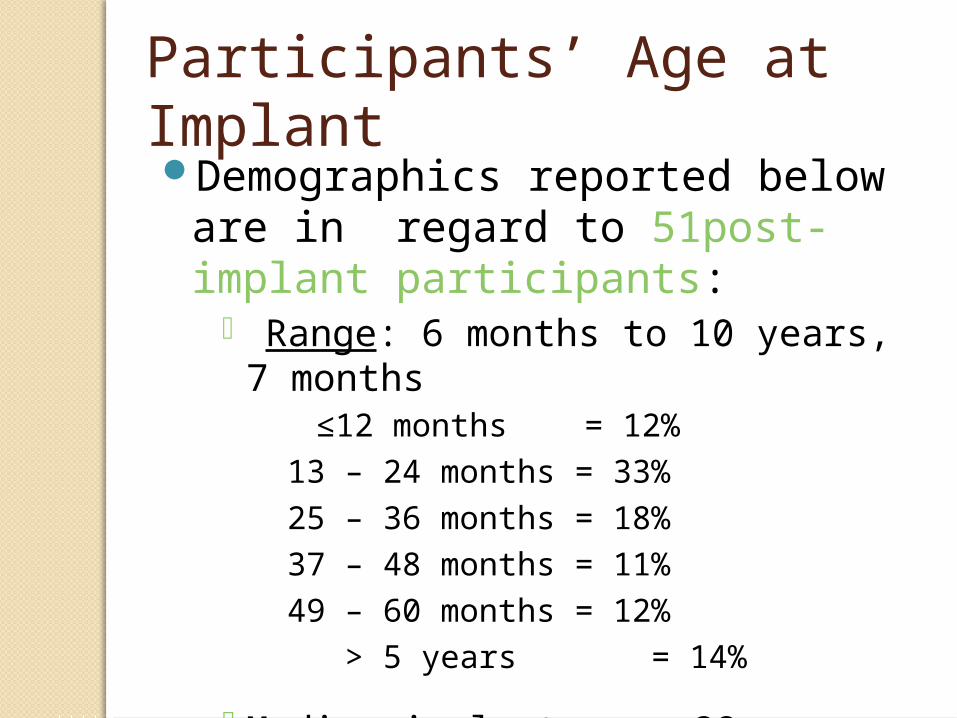
Participants’ Age at ImplantDemographics reported below
are in regard to 51post-implant participants:
Range: 6 months to 10 years, 7 months
≤12 months = 12% 13 – 24 months = 33%25 – 36 months = 18%37 – 48 months = 11%49 – 60 months = 12% > 5 years = 14%
Median implant age: 28 months
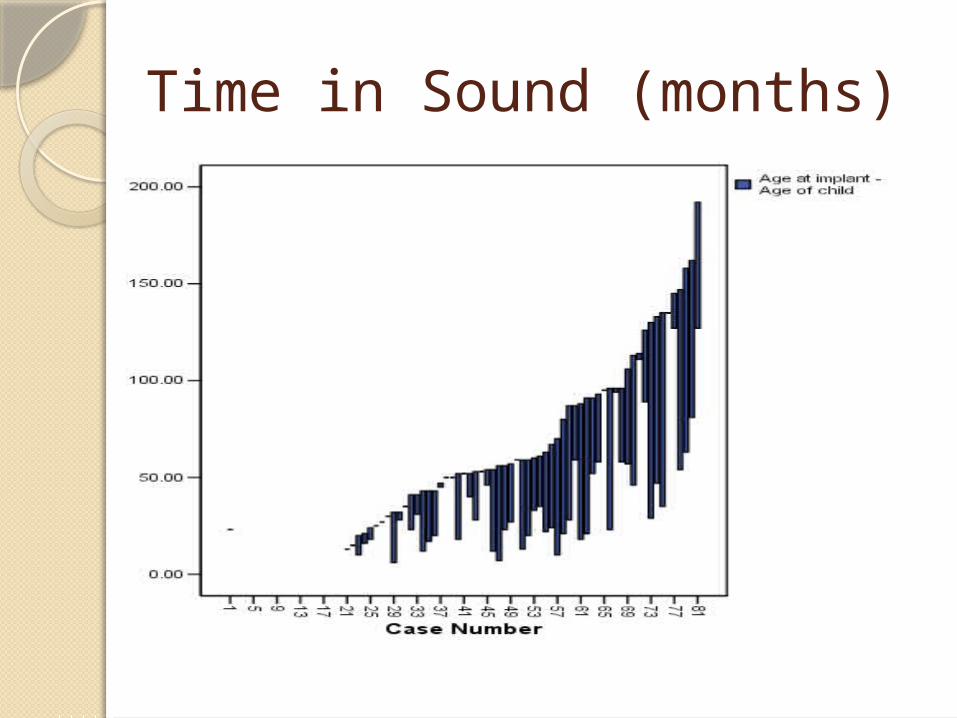
Time in Sound (months)
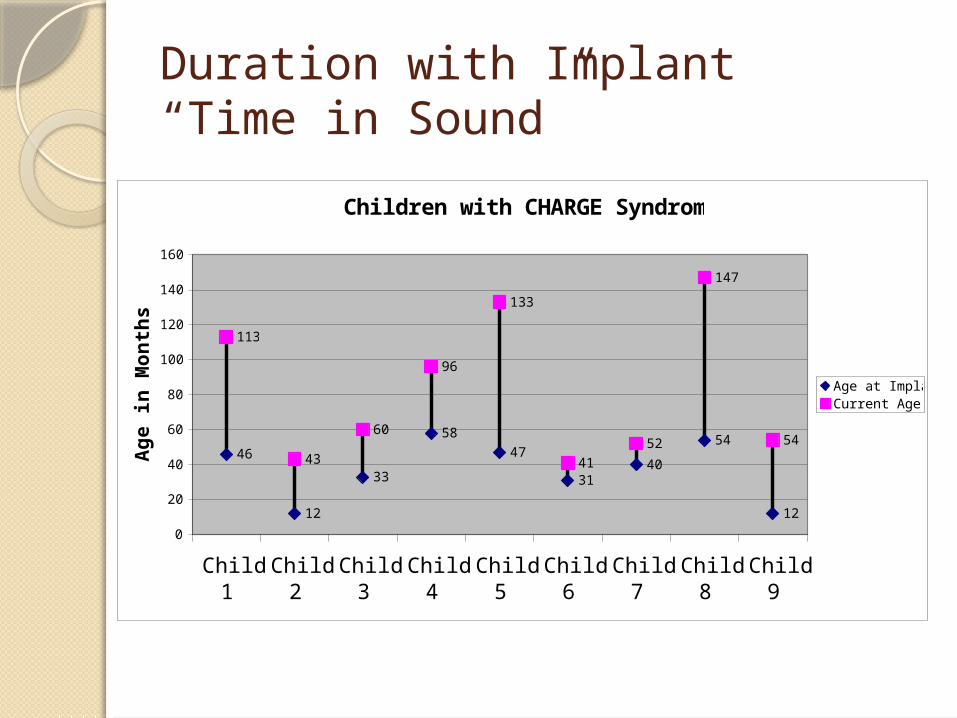
Duration with Implant“Time in Sound”
Children with CHARGE Syndrome
46
12
33
58
47
3140
54
12
113
43
60
96
133
41
52
147
54
0
20
40
60
80
100
120
140
160
Child1
Child2
Child3
Child4
Child5
Child6
Child7
Child8
Child9
Ag
e in
Mo
nth
s
Age at ImplantCurrent Age
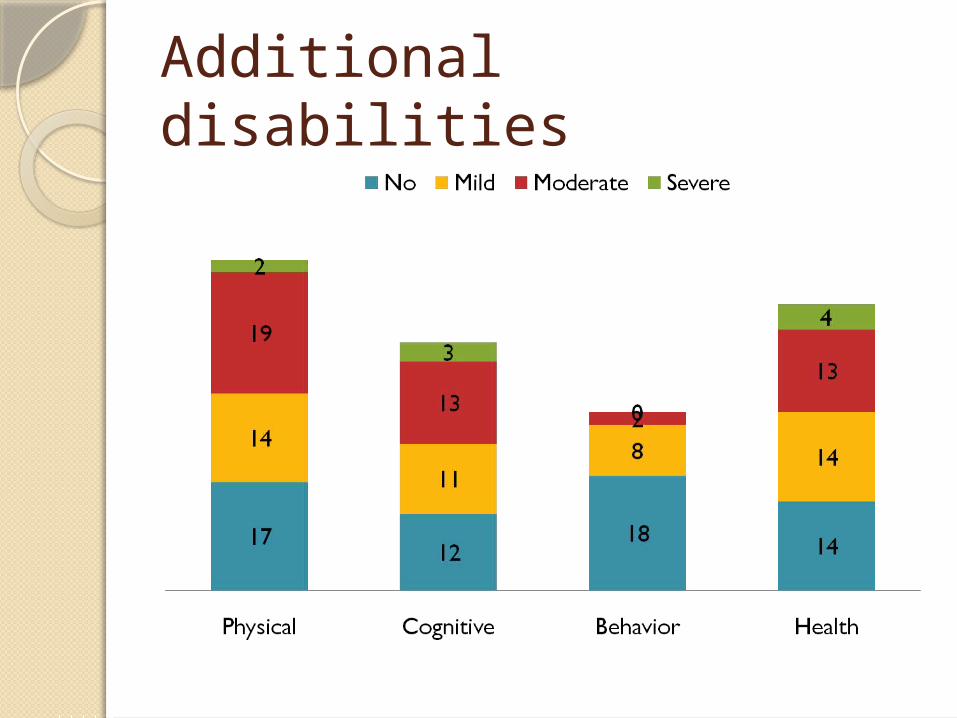
Additional disabilities
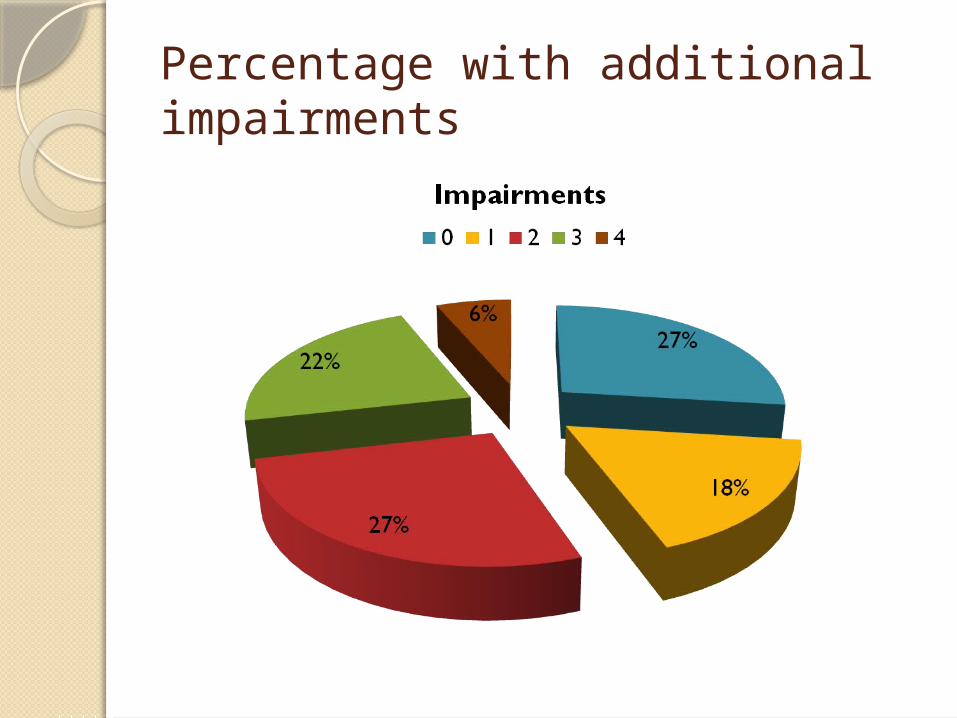
Percentage with additional impairments
Communication (initial assessment)Large percentage of participants
demonstrate little vocabulary comprehension (> 75%)◦92% pre have less than 5 words◦75% post have less than 5 words
Large percentage have little vocabulary production (>80%)◦92% pre have less than 10 words◦88% post have less than 10 words
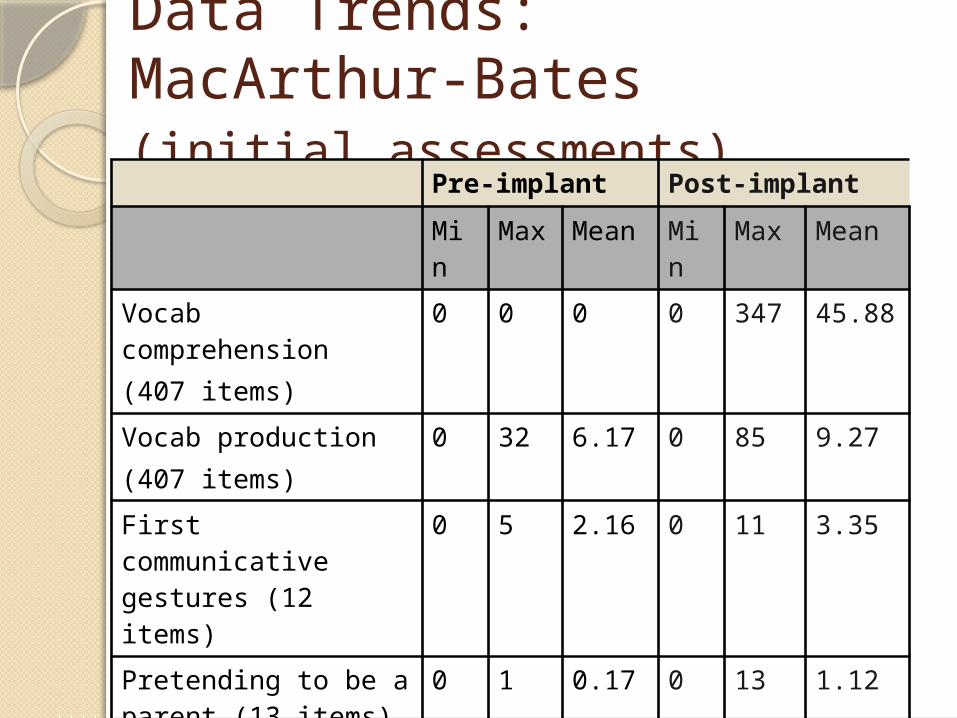
Data Trends: MacArthur-Bates(initial assessments)
Pre-implant Post-implant
Min
Max Mean Min
Max Mean
Vocab comprehension(407 items)
0 0 0 0 347 45.88
Vocab production(407 items)
0 32 6.17 0 85 9.27
First communicative gestures (12 items)
0 5 2.16 0 11 3.35
Pretending to be a parent (13 items)
0 1 0.17 0 13 1.12
Imitating adult actions(15 items)
0 9 1.50 0 15 2.73
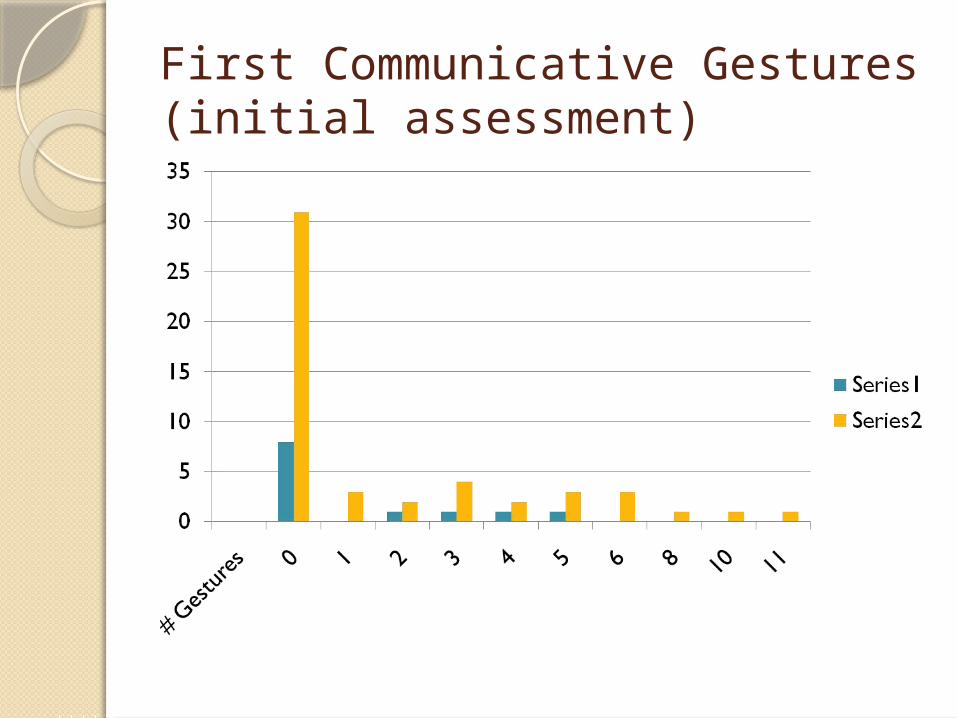
First Communicative Gestures(initial assessment)
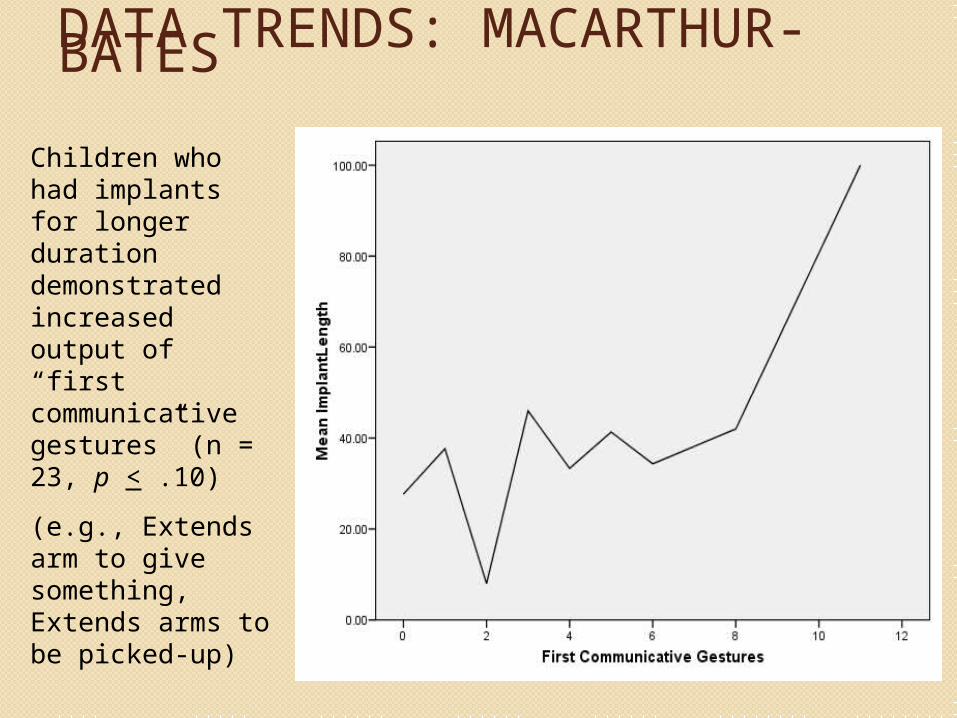
DATA TRENDS: MACARTHUR-BATES
Children who had implants for longer duration demonstrated increased output of “first communicative gestures” (n = 23, p < .10)
(e.g., Extends arm to give something, Extends arms to be picked-up)
Bilateral Cochlear ImplantsSix participants have bilateral
cochlear implantsTend to be youngerIntroducing Grace
Preliminary FindingsPopulation of children with DB is
extremely diverse; receiving a cochlear implant is not associated with any particular etiology
Majority of participants have two or more additional disabilities (beyond DB)
Younger participants in study, as a group, received their implants at earlier ages
Participants in study, who had more additional disabilities, as a group received their implants at older ages
Participants appear to be demonstrating tremendous variability in their outcomes
Preliminary FindingsImplantation at an earlier age appears
to be associated with more rapid, significant progress
Participants with longer “time in sound” appear to demonstrate increased output
Participants appear to be showing increased vocalizations during play, after CI
Participants appear to begin to show small increases in response to gestures and words
Concerns and LimitationsIncredible variety in participants’
cochlear implant wearing patterns
Reportedly: some children wear their implants during
all waking hours many children wear their implants only
at school a number of children wear their implants
inconsistently-home and school some participants’ families have
discontinued use of their child’s implant (as much as 10% reported in some states)
Concerns and Limitations
Intensity, frequency, and types of available intervention / habilitation vary widely across children and families
Tremendous need exists for appropriate intervention / habilitation techniques for implementation with children who have concurrent vision and hearing losses AND additional disabilities
Concerns and Limitations
Severe shortage of personnel trained in auditory-verbal (A-V) therapy techniques
Even therapists trained in AV techniques are unsure of how to adapt these for implementation with children with DB
Acknowledgements
USDE grant award H327A050079Co-Investigators:
Kat Stremel, NCDBLisa Cowdrey, Midwest Ear InstituteState Deaf-Blind Project directors
Teachers and families who allowed us to complete research in their classrooms and homes
Contact InfoSusan M. Bashinski (
Ella Taylor ([email protected])
Project Websitehttp://www.wou.edu/cidb