cns 2 physiology lab - judoctors « medicine lectures ... · cns 2 physiology lab 3 | p a g e when...
TRANSCRIPT

CNS 2 Physiology lab
1 | P a g e
Presbiopia: is decrease in accommodation of the lens, and it happens
in old ladies
Astigmatism: a problem in one of the focal planes; due to irregularity
(in cornea or lens), one of the focal planes is out of focus compared
to the others. It is tested by the chart shown below:
You ask the patient, which line you see shorter, longer, or thicker than
the others; since only one plane is out of focus and all the other planes
are in focus, one line will be different from the others.
It should be noted that the doctor emphasized that this material is also
considered as continuation of the theory material and is INCLUDED IN THE
THEORY EXAM.

CNS 2 Physiology lab
2 | P a g e
Confrontational visual field exam is used to test the visual field of a
patient and know if he has quadrant-anopia or bilateral hemi-anopia
Now if you stand in front of the patient and point your finger and
ask him/her if he can see your finger, the patient might move his
head.
To make sure that the test is done properly, you should stand
straight opposite to the patient, leaving some distance, and ask
the patient to cover one eye and you (the examiner) cover the
eye opposite to the patient's covered eye (i.e. if the patient
covers his right eye, you cover your left eye) and make the
patient focus on you, by this you make sure that the patient does
not move his eyes. Now, you start moving your finger around
midway between you and the patient, and ask the patient if he
can see your finger without him moving his eyes away from you.
In this situation, you are the control because when you place your
finger outside the patient's visual field, you know it's outside the
visual field and not a defect because you can't see your finger
either.
After you are done, you examine the other eye by the same way.
The pictures below show you how the test is done:

CNS 2 Physiology lab
3 | P a g e
When we talked about light refraction, accommodation must occur.
In order to look at a near object, the following occur:
1. Pupil constriction
2. Accommodation of the lens, in which it becomes more dense and
rounded
Even in dim light, if you want to look at a near object, the pupil will
constrict, even though the pupil should be dilated. This is called pupil
near reflex.
Now light coming from the outside can fall anywhere on the retina
depending on its source.
If the light is refracted at the periphery of the lens, it will not give a
good well-formed refraction; it will make a point concentration of
light, but it will be really small; thus, the region that you see is a
really small point.
When light passes through the center of the lens, there will be
more uniform refraction; the light will be focused on a larger point.
In lenses, not only eyes, the distance in which the light is
concentrated on one point is called focal depth.
If a lens's focal depth is small, like 1mm, any point that is 1mm
will be in focus, but anything more than 1mm will be out of focus
If the focal depth is large, like 5mm, any point less than 5mm will
still be in focus.
Q) Why is it important for the pupil to be constricted when looking at
a near object even in dim light?
Ans.) When the pupil is constricted, the light will fall on the center of
the lens and not the retina. Whether the pupil is constricted or dilated
the light will fall on the same point on the retina however, the focal
depth differs when the pupil is constricted or dilated.

CNS 2 Physiology lab
4 | P a g e
This is important in near vision because 1mm doesn't make a difference
in far vision. When you focus on your finger, you want to see your whole
finger not just the surface or one part of it; in this case, 1mm makes a
difference, in order to do that you must have a bigger focal depth. When
you are reading from a book and not a board in which it has a flat
surface, if you want to focus on a word; if the focal depth is small, the
upper part will be out of focus and all other words will be out of focus
too, so you need to focus on each word by itself.
For this reason, in near vision, even in the dark, there will be pupil
constriction and accommodation of the lens; this results in the passage
of light through the center of the lens and the focal depth is large, and
this allows you to see more than one level in focus together (more than
one dimension).
An example is when you enter a hall; you stand at the front row and
start looking at chairs in the 7th, 8th or 9th row, you can see the numbers
of 3 chairs at the same time; then you look at the 2nd or 3rd row (without
accommodation), you can see the number of one chair only.
This example might be useful:
Figure A shows the situation of an eye looking at a man through a narrow pupil. Everything from close to far away is in focus, because the dispersion of light from each point of the image in front or behind the focal point on the retina is minimal.
Figure B shows the same situation, but with a wide pupil. The image at the focal point on the retina is sharp, but because the dispersion of light from each point of the image is quite large, the sharpness of the image rapidly diminishes at points behind, or in front of the focal point.
Dispersion of light

CNS 2 Physiology lab
5 | P a g e
Its pathway:
Optic nerve to geniculate nucleus, visual cortex (area 17), secondary
visual cortex (areas 18 and 19) and then signals telling that the image is
out of focus travel down parasympathetic oculomotor to cause
constriction. It differs from the light reflex in its sensory component
only.
This lesion results in what is known as light-near dissociation, where
there is no light reflex but near reflex is present.
A lesion in the posterior part of the midbrain affecting the olivary
pretectal area is called dorsal midbrain syndrome; an example is
Parinaud's syndrome.
Visual acuity is the accuracy of vision, seeing things clearly; it is
determined mainly by refraction errors.
In normal people two points 1.75 mm apart are recognized as 2
separate points from a distance of 6m.
Any person who needs the distance to be less than 6m, like 4 or
5m, in order to recognize them as 2 separate points, then he has
decreased visual acuity
A person who can still see them as two separate points from a
larger distance, like 7m, then he has increased acuity or super
acuity.
If there was a lesion in the posterior part of the midbrain (lesion in
the olivary pretectal nucleus; EW nucleus is intact), will the
pupillary light reflex be lost? The light reflex will be lost since it
interferes with its pathway (olivary pretectal nucleus is damaged);
but the pupil near reflex will not be lost because it will not interfere
with its pathway (EW nucleus is intact), the impulses will travel
directly from higher centers to parasympathetic oculomotor.
CNS 2 Physiology lab
6 | P a g e
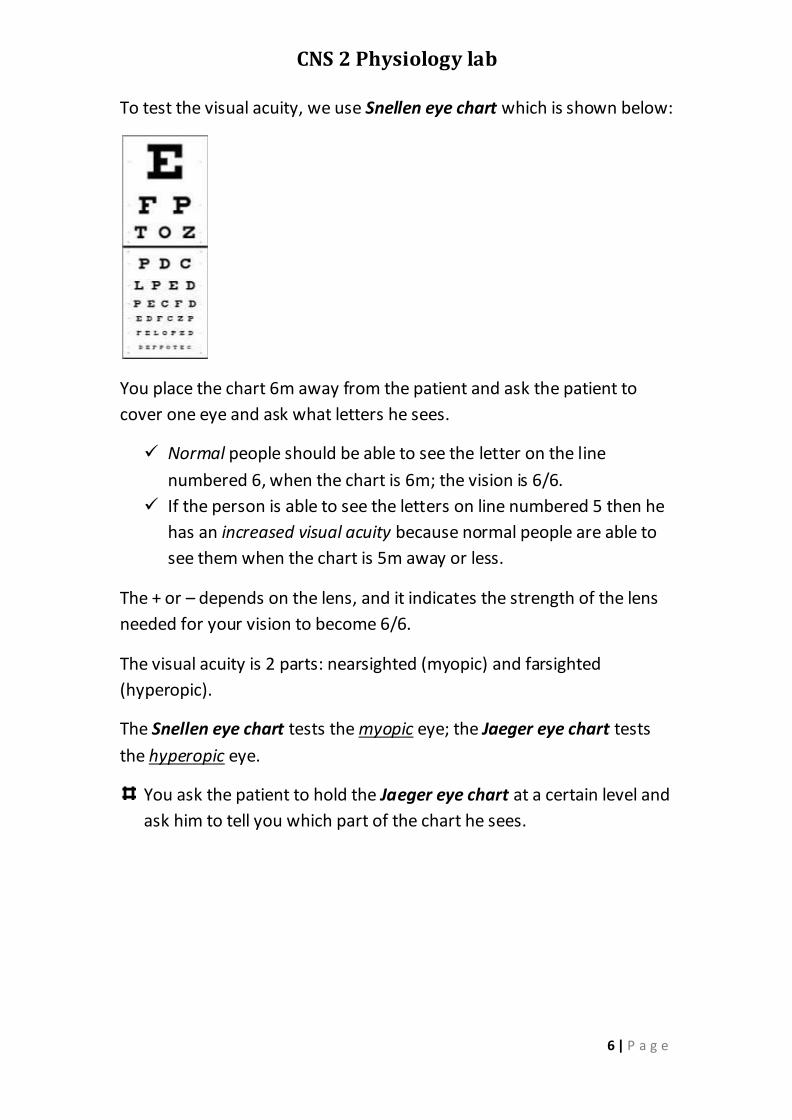
To test the visual acuity, we use Snellen eye chart which is shown below:
You place the chart 6m away from the patient and ask the patient to
cover one eye and ask what letters he sees.
Normal people should be able to see the letter on the line
numbered 6, when the chart is 6m; the vision is 6/6.
If the person is able to see the letters on line numbered 5 then he
has an increased visual acuity because normal people are able to
see them when the chart is 5m away or less.
The + or – depends on the lens, and it indicates the strength of the lens
needed for your vision to become 6/6.
The visual acuity is 2 parts: nearsighted (myopic) and farsighted
(hyperopic).
The Snellen eye chart tests the myopic eye; the Jaeger eye chart tests
the hyperopic eye.
You ask the patient to hold the Jaeger eye chart at a certain level and
ask him to tell you which part of the chart he sees.

CNS 2 Physiology lab
7 | P a g e
Pupillary light reflex:
As we all know, shining light on one eye will cause light reflex to occur in
both eyes.
Actually 53-67% of fibers cross in the optic chiasma, but for simplicity
we're going to take the average in which 60% of the fibers cross. Due to
this, relative afferent pupillary reflex will occur.
To test the light reflex: make the patient look at you and shine light on
one eye, both eyes will constrict. Do the same for the other eye.
There is swinging light test: you shine the light on one eye, wait for 3
seconds then move the light to the other eye, then move the light back
to the other eye; in normal people, both eyes will be constricted in the
same manner no matter how many times you swing the light.
Sometimes there is a difference in the constriction of each eye that can't
be detected except with swinging light test. When swinging the light the
affected eye will dilate a little, this means that constriction actually
occurred in one eye only; if the affected eye is the right eye, then we say
the patient has positive right relative afferent pupillary defect or positive
true swinging test.
Relative afferent pupillary defect is usually due to before the chiasm
problem:
Retinal detachment: for example, the right eye has 10% retinal
detachment which means that only 90% of the eye is active for
light reflex; this will result in a smaller constriction than the left eye
Ischemic retina
Problem in optic nerve: not a complete cut like ischemia,
compression, neuritis… mainly recovered neuritis because in all the
previously mentioned causes, the vision will be affected, however,
in recovered neuritis, the vision is normal but the nerve is not
completely recovered so there will be a difference in the pupillary
reflex between the two eyes.
Diabetic retinopathy

CNS 2 Physiology lab
8 | P a g e
Optic track lesion with no visual defects
Cut at B (consider it to be on the right side), left homonymous
hemianopia occurs; light reflex is positive in both eyes, but the
constriction in the right will be more than in the left. In swinging
light test, it will be positive in the left eye because 60% of the
fibers cross to the right side; the positive RAPD test is due to
unequal decussation in the chiasma.
This test was used in the past to differentiate between optic tract
lesion and optic radiation lesion; but now is of less significance
because of MRI.
Unilateral midbrain lesion: no visual defects occur; like we said in
dorsal midbrain syndrome, but here the defect is only on one side
so RAPD will occur.

CNS 2 Physiology lab
9 | P a g e
Anisocoria is when the pupil of one eye is larger than the other.
In Horner's syndrome, the pupil of one eye is smaller than the
other on the ipsilateral side.
In 20% of people, it is normal physiological thing, which means
that there is no deficit or anything. Anisocoria is abnormal, but
some people have it physiologically with no underlying cause.
Anisocoria is tested in light and dark; and the pupil diameter is
observed in both situations.
Anisocoria is due to a defect in the efferent pathway, either
sympathetic or parasympathetic. If the defect is in sympathetic,
anisocoria is observed in dark; if in parasympathetic in light.
In Horner's syndrome, there is a defect in the sympathetic
neurons; anisocoria is apparent in dark.
Adie's tonic pupil, defect in the parasympathetic postganglionic
neuron degenerates; there is a defect in pupillary reflex, and
light-near dissociation is present because the neurons for
accommodation are more than those for pupillary reflex
Dorsal midbrain syndrome results in light-near dissociation; if it
was on one side, anisocoria results.
Photoreceptors are of 2 kinds:
Rods
Cones: for color vision and has three types of photosensitive
proteins: blue, green and red (in the past, they used to call them
low, medium and high frequency; but it is less accurate). They
allow me to see all colors by combination of their activities.
In Horner's syndrome, the affected eye's pupil will be already constricted, in order to
detect is anisocoria, it must be dark. In Adie's tonic pupil, the pupil will be dilated; in
order to detect anisocoria, there must be light.

CNS 2 Physiology lab
10 | P a g e
Color blindness is mainly in red and green; there is blue color
blindness but is rare.
Color blindness is X-linked, that's why it is more common in males
than in females.
There may be loss of the green or red color. If the green is lost,
then it called Deuteranope; if red is Protanope.
Blue color: wave
at 450 nm.
There is activation
of 97% of low
frequency (blue
wave) while the
others are zero.
Green color: activation
of 31% red, 36% blue
and 67% green.

CNS 2 Physiology lab
11 | P a g e
Deuternope
Now if you show a patient with Deuternope a green card, what color will
he see?
He will see the color green, why? The green wavelength is 500nm.
In normal people, the
brain will recognize it by
the activities of 36% for
low frequency (blue),
67% for medium
frequency (green), and
31% for high frequency
(red); so it understands
the color as green
In a person with
deuteranope, the brain
receives the signals as 36
for low frequency and 31
for high frequency but
perceives the color as
green because colors are
already coded by 2 codes only.

CNS 2 Physiology lab
12 | P a g e
Any region that has no overlap will be a problem; for example,
light of wave 550
Some of the shades of yellow and orange will have the same color
in people with deuteranope.
A normal person with 3
codings will activate high
frequency 85% and
medium frequency 83%
and low frequency 0%.
It is different from 610
wave which has 85% high
frequency and the others
are 0%.
A person with
deuteranope will see
both the same color
because both will
activate high
frequency 85% and
the others 0%.
CNS 2 Physiology lab
13 | P a g e
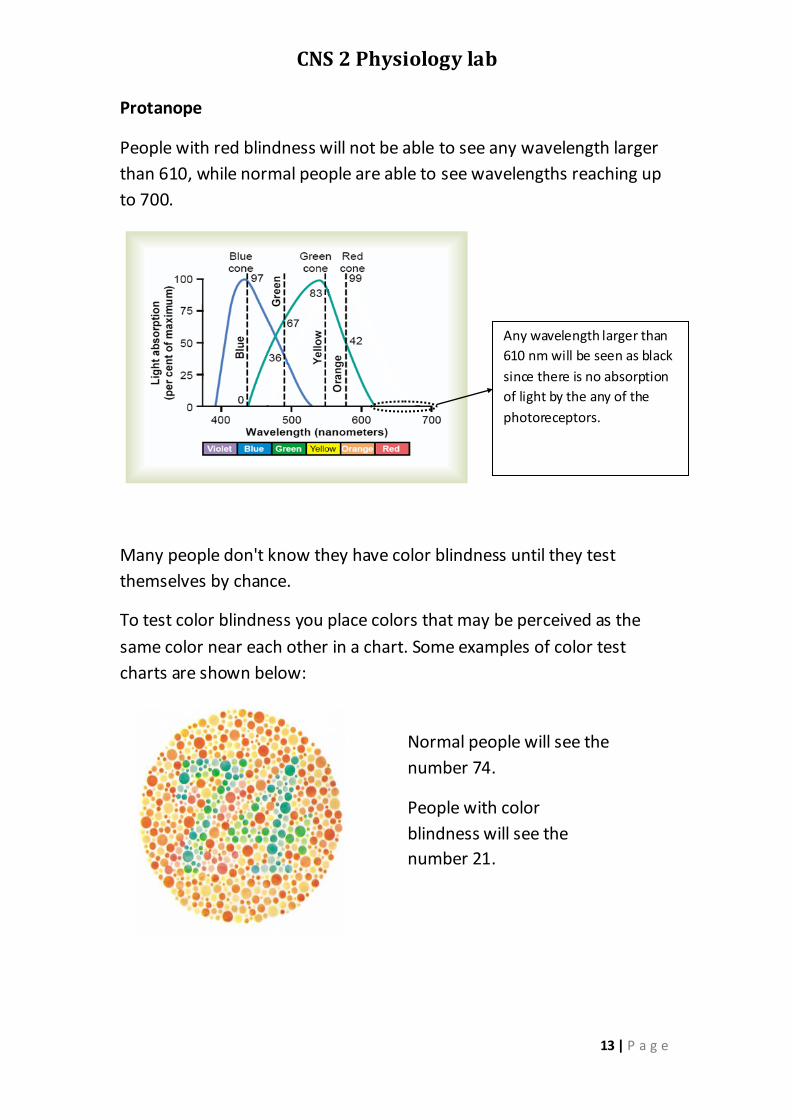
Protanope
People with red blindness will not be able to see any wavelength larger
than 610, while normal people are able to see wavelengths reaching up
to 700.
Many people don't know they have color blindness until they test
themselves by chance.
To test color blindness you place colors that may be perceived as the
same color near each other in a chart. Some examples of color test
charts are shown below:
Any wavelength larger than
610 nm will be seen as black
since there is no absorption
of light by the any of the
photoreceptors.
Normal people will see the
number 74.
People with color
blindness will see the
number 21.

CNS 2 Physiology lab
14 | P a g e
To distinguish between red color blindness and green color blindness,
you use the chart below:
Test for hearing
Sound from outside, reaches the brain and is heard. If the sound
doesn't reach the brain and is not heard then there may be deafness
which is of 2 types:
Conductive deafness: improper conduction of sound from outside
to sensory organ
Sensorineural deafness: Can't convert the sound from vibration
to a neuronal signal or to transmit the neuronal signal to the
brain.
To test for hearing, you use Rinne and Weber test, which depend on the
fact that air conduction is better than bone conduction because there is
amplification of the sound in the middle ear; in bone conduction, there
is no amplification of sound in the middle ear. In normal people, the air
conduction is better than the bone conduction.
To perform the test, you use the tuning fork
Rinne test, you place the base of the tuning fork on the mastoid
process until the patient no longer hears the sound and then place
the tuning fork beside the ear. Normal subjects will hear the vibration
after bone conduction is over. In conduction deafness, air conduction
is not heard after bone conduction is over.
Normal people will see 42
People with green will see 4
People with red will see 2.

CNS 2 Physiology lab
15 | P a g e
You can use yourself as a control when it comes to air
conduction; if the patient stops hearing the vibration before
you do, you suspect that he has some kind of conductive
deafness and you do further tests.
Now if the patient hears the air conduction better than the
bone conduction, it is not necessarily normal and the patient
may have sensorineural deafness. To make sure that the
patient is normal, we perform Weber's test.
In Weber's test, you place the base of the tuning fork on the vertex of
the skull (you may place it on the forehead, but the vertex of the skull
is better) and the test is performed in a noisy room. Normal subjects
will hear the vibration in both ears equally. Patients with conductive
loss will hear the vibration better in the affected ear because there is
no masking noise. Patients with sensorineural deafness will hear the
vibration better in the normal ear.
I'm sorry for any mistakes
Wish you the best of luck in the exam☺
Your colleague Jumanah Nayef
"Turn your face
towards the sun, and
the shadows fall
behind you"