cme/moc composing personalized hcc treatment …
TRANSCRIPT

Ghassan Abou-Alfa, MD, MBAMemorial Sloan Kettering Cancer Center Weill Medical College at Cornell University New York, New York
Robin K. (“Katie”) Kelley, MDHelen Diller Family Comprehensive Cancer Center University of California, San Francisco San Francisco, California
Professor Riccardo Lencioni, MD, FSIR, EBIRUniversity of Pisa Pisa, Italy Miami Cancer Institute Miami, Florida
Amit Singal, MD, MSUT Southwestern Medical Center Dallas, Texas
Chair Faculty
Faculty Faculty
Participate in interactive questions, download activity slides, and obtain your instant CME/MOC credit online.This CME/MOC activity is jointly
provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
CME/MOC
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
What’s Inside
3
5
Welcome and Introduction: The Evolving Therapeutic Management of HCCChoosing and Sequencing TKIs Across the Continuum of Care in Advanced HCC
Newer Targeted and Immunotherapy Options as Second-Line Treatment and Beyond
The Next Wave: Expanding the Therapeutic Arsenal in Earlier-Stage Disease
Audience Q&A
11
19
26
PeerView.com/XKX900

2 Go online to complete the post-test and evaluation for CME/MOC credit
Activity Information
Media: Enduring MaterialAccredited Activity Release Date: November 4, 2019Accredited Activity Expiration Date: November 3, 2020Time to Complete Activity: 90 minutes
Activity DescriptionHepatocellular carcinoma (HCC) is an aggressive, complex disease and is a leading cause of cancer-related deaths worldwide. Research endeavors to mitigate HCC mortality have led to rapid advances, especially in the past two years. Today, clinicians specializing in HCC have various treatment options to select for their patients across the spectrum of the disease, and the therapeutic landscape continues to evolve with promising results from ongoing clinical trials investigating novel approaches.
This PeerView MasterClass and Tumor Board on-demand educational activity, based on a symposium held adjunct to the 13th Annual Conference of the International Liver Cancer Association (ILCA 2019), features a panel of multidisciplinary HCC experts who review pivotal evidence on available TKI, antiangiogenic, and checkpoint inhibitor therapies and their optimal treatment sequencing strategies, as well as emerging data on novel combinations and innovative modalities for early- to advanced-stage disease. The experts weave the science into real-world case scenarios, helping to translate the data into practical experiences in the HCC clinic.
Target AudienceThis activity has been designed to meet the educational needs of oncologists, hepatologists, gastroenterologists, radiologists, and other clinicians involved in the management of HCC.
Educational ObjectivesUpon completion of this activity, participants should be better able to:• Summarize recent safety and efficacy evidence of available targeted therapies, such as multikinase
inhibitors and monoclonal antibodies, for HCC• Evaluate the significance of new data and ongoing clinical trials with checkpoint inhibitors as
treatment options for HCC• Review the potential use of systemic treatments in novel multimodal strategies for intermediate
HCC• Construct safe and effective treatment plans across multiple lines of therapy for patients with HCC
based on multidisciplinary team–based strategies
Providership, Credit, and SupportThis CME/MOC activity is jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
This activity is supported by medical educational grants from Bayer Healthcare Pharmaceuticals Inc., Celsion Corporation, and Exelixis, Inc.
Physician Continuing Medical EducationThis activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education. The Medical Learning Institute, Inc. is accredited by the ACCME to provide continuing medical education for physicians.
The Medical Learning Institute, Inc. designates this enduring material for a maximum of 1.5 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
The European Union of Medical Specialists (UEMS)-European Accreditation Council for Continuing Medical Education (EACCME) has an agreement of mutual recognition of continuing medical education (CME) credit with the American Medical Association (AMA). European physicians interested in converting AMA PRA Category 1 Credit™ into European CME credit (ECMEC) should contact the UEMS (www.uems.eu).
MOC Statement
Successful completion of this CME activity, which includes participation in the evaluation component, enables the participant to earn up to 1.5 MOC points and patient safety MOC credit in the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) program. Participants will earn MOC points equivalent to the amount of CME credits claimed for the activity. It is the CME activity provider’s responsibility to submit participant completion information to ACCME for the purpose of granting ABIM MOC credit.
Participation information will be shared with ABIM through the ACCME’s Program and Activity Reporting System (PARS). Blinded individual or aggregated participant data may be shared with the funder of the activity.
Faculty DisclosuresChairGhassan Abou-Alfa, MD, MBAAttending Memorial Sloan Kettering Cancer Center Professor Weill Medical College at Cornell University New York, New York
Ghassan Abou-Alfa, MD, MBA, has a financial interest/relationship or affiliation in the form of: Consultant and/or Advisor for 3D Medicines Corporation; Agios, Inc.; Alignmed; Amgen Inc.; AstraZeneca; Bayer; BeiGene; Boston Scientific Corporation; BridgeBio Inc.; Bristol-Myers Squibb; CARsgen Therapeutics; CASI Pharmaceuticals Inc.; Celgene Corporation; Cipla Inc.; Daiichi Sankyo Company, limited; Debiopharm Group; Delcath Systems Inc.; Eisai Inc.; Eli Lilly and Company; Exelixis, Inc.; Flatiron; Genoscience Pharma; Halozyme, Inc.; Hengrui Therapeutics, Inc.; Incyte Corporation; Inovio Pharmaceuticals, Inc.; Ipsen Biopharmaceuticals, Inc.; Jazz Pharmaceuticals, Inc.; Klus Pharma Inc; Kyowa Kirin, Inc.; LAM Inc.; Merck & Co., Inc.; MINAPHARM Pharmaceuticals; Novella; Onxeo; PCI Biotech; QED Therapeutics; Redhill; sanofi-aventis U.S. LLC; Servier; SillaJen, Inc.; Tekmira; twoXAR; VIVUS Inc.; Yakult Pharmaceutical Industry Co., Ltd.; and Yiviva. Grant/Research Support from ActaBiologica; Agios, Inc.; Array BioPharma; AstraZeneca; Bayer; BeiGene; Bristol-Myers Squibb; CASI Pharmaceuticals Inc.; Celgene Corporation; Eli Lilly and Company; Exelixis, Inc.; F. Hoffmann-La Roche Ltd; Genentech, Inc.; Halozyme, Inc.; Incyte Corporation; MabVax
Therapeutics, Inc.; Novartis Pharmaceuticals Corporation; OncoQuest Inc.; Polaris Puma; and QED Therapeutics. Other Financial or Material Support from Spouse consulting for Bioline; Celgene Corporation; CytomX Therapeutics, Inc.; Janssen Pharmaceuticals, Inc.; Loxo Oncology; Merck & Co., Inc.; Pfizer Inc.; Silenseed LTD; Sobi, Inc; Targovax; and twoXAR.
FacultyRobin K. (“Katie”) Kelley, MDAssociate Professor of Clinical Medicine Helen Diller Family Comprehensive Cancer Center Division of Hematology/Oncology University of California, San Francisco San Francisco, California
Robin K. (“Katie”) Kelley, MD, has a financial interest/relationship or affiliation in the form of: Other Financial or Material Support from Investigator on Clinical Trials for Adaptimmune; Agios, Inc.; AstraZeneca; Bayer; Bristol-Myers Squibb; Eli Lilly and Company; Exelixis, Inc.; MedImmune; Merck & Co., Inc.; Novartis Pharmaceuticals Corporation; QED Therapeutics; and Taiho oncology, Inc. lOMC member of Genentech, Inc./ F. Hoffmann-La Roche Ltd.
Professor Riccardo Lencioni, MD, FSIR, EBIRDepartment of Radiology, University of Pisa Pisa, Italy Hon. Res. Prof. Interventional Oncology Miami Cancer Institute Miami, Florida
Professor Riccardo Lencioni, MD, FSIR, EBIR, has a financial interest/relationship or affiliation in the form of: Consultant and/or Advisor for AstraZeneca and Celsion, Inc.
Amit Singal, MD, MSMedical Director of Liver Tumor Program Associate Professor of Medicine UT Southwestern Medical Center Dallas, Texas
Amit Singal, MD, MS, has a financial interest/relationship or affiliation in the form of:Consultant and/or Advisor for Bayer Corporation; Bristol-Myers Squibb; Eisai Inc.; and Exelixis, Inc.Other Financial or Material Support from Target MCC for Steering Committee.
Planning Committee DisclosuresThe planners from Medical Learning Institute, Inc., the accredited provider, and PeerView Institute for Medical Education, the joint provider, do not have any financial relationships with an ACCME-defined commercial interest related to the content of this accredited activity during the past 12 months unless listed below.
Content/Peer Reviewer DisclosuresThe following Content/Peer Reviewers have nothing to disclose:
Steve S. Choi, MDTeresa Haile, RPh, MBA
Disclosure of Unlabeled UseThis educational activity may contain discussions of published and/or investigational uses of agents that are not indicated by the FDA. The planners of this activity do not recommend the use of any agent outside of the labeled indications. The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
DisclaimerParticipants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient's conditions and possible contraindications and/or dangers in use, review of any applicable manufacturer's product information, and comparison with recommendations of other authorities.
Method of ParticipationThere are no fees for participating in or receiving credit for this accredited activity. For information on applicability and acceptance of continuing education credit for this activity, please consult your professional licensing board.
A statement of credit will be issued only upon receipt of a completed activity evaluation form and will be emailed to you upon completion. You will receive your certificate from [email protected]. If you have questions regarding the receipt of your emailed certificate, please contact via email at [email protected].
In order to receive credit, participants must view the activity and complete the post-test and evaluation form. A score of 70% or higher is needed to obtain MOC credit. There are no pre-requisites and there is no fee to participate in this activity or to receive MOC credit. Statements of Credit are awarded upon successful completion of the post-test and evaluation form.
About This CME/MOC ActivityPVI, PeerView Institute for Medical Education, and Medical Learning Institute, Inc. are responsible for the selection of this activity’s topics, the preparation of editorial content, and the distribution of this activity. Our activities may contain references to unapproved products or uses of these products in certain jurisdictions. The preparation of PeerView activities is supported by educational grants subject to written agreements that clearly stipulate and enforce the editorial independence of PVI and Medical Learning Institute, Inc.
PeerView.com/XKX900

Ghassan Abou-Alfa, MD, MBA
3
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
Dr. Abou-Alfa: Welcome to, “Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble.” We are greatly honored to have today, a great group of panelists. My name is Ghassan Abou-Alfa, and next to me is Dr. Katie Kelley, Dr. Singal, and Professor Lencioni. I’ll go ahead and start with an introduction with regard to the evolving therapeutic management of HCC.
1. Petrick JL et al. J Clin Oncol. 2016;34:1787-1794.
Male HCC Incidence Rates
Projected Overserved
Rat
e pe
r 10,
000
Pers
on-Y
ears
Year of Diagnosis 2000 2005 2010 2015 2025 2030 2020
Hispanic Black All males White Asian
60
50
40
30
20
10
0
Projections of HCC Incidence Into 20301
Dr. Abou-Alfa: I think we all agree that HCC incidence into 2030 does not look good for the United States, and it does not look good worldwide. This is an important paper, which I’m sure you’re all familiar with, from July 2016 in the Journal of Clinical Oncology that looked at the incidence rate that’s been observed so far, until about 2013, and the projected incidence rate up to 2030.
No question, we’re proud to see a decline projected for the Asian population in regard to HCC in the United States. And this, of course, speaks to the [increased use of] vaccination against hepatitis B in this population. In addition to that, sadly, we’re seeing among all men and Caucasians, a continued projection for increased incidence of HCC, which is mainly driven by NASH, or nonalcoholic steatohepatitis.
And in regard to hepatitis C, we don’t yet see any change per se, despite the advent of curative therapy. But as you can see, it is almost slowing down, but not quite vigorously so, for Hispanic
Welcome and Introduction: The Evolving Therapeutic Management of HCC
and African American projections. This is because the willingness to use hepatitis C treatment is not necessarily 100% yet. As we all know, having one person with hepatitis C is enough in the community to really continue to spread the virus.
Mortality From Cancer According to Body Mass Index (BMI) for US Men1,2
1. https://www.cancer.org/research/we-conduct-cancer-research/epidemiology/cancer-prevention-study-2.html. Accessed September 12, 2019. 2. Calle EE et al. N Engl J Med. 2003;348:1625-1638.
0 1 2 3 4 5 6 7
Relative Risk of Death (95% CI)
Prostate (≥35)
Type
of C
ance
r (H
ighe
st B
MI C
ateg
ory)
Non-Hodgkin lymphoma (≥35) All cancers (≥40)
All other cancers (≥30) Kidney (≥35)
Multiple myeloma (≥35) Gallbladder (≥30)
Colon and rectum (≥35) Esophagus (≥30)
Stomach (≥35) Pancreas (≥35)
Liver (≥35)
1.34 Men
1.49 1.52
1.68 1.70
1.71 1.76
1.84 1.91
1.94 2.61
4.52
With this said, let’s go to the NASH story, where we said that most projections are going to go forward. This is a very important paper from 2003 published in The New England Journal of Medicine by Dr. Calle and colleagues from Emory University at that time. And as we can see here, body mass index is clearly correlated as an independent factor in regard to mortality from cancer across the board. We can see the numbers ranging for all cancers, but really, it was a whopping 4.52% chance, independent of anything else, to die from cancer.
Child–Pugh Score of Liver Cirrhosis1
1. Pugh RN et al. Br J Surg. 1973;60:646-649.
Parameter Points
1 2 3 Albumin, g/dL >3.5 2.8-3.5 <2.8
Bilirubin, mg/dL <2 2-3 >3
Ascites Absent Slight Moderate
Encephalopathy None I-II III-IV
PT, INR <1.7 1.8-2.3 >2.3
Score A B C
Points 5-6 7-9 10-15
One of the struggles we have—and many of you from the hepatology world are very familiar with this—continues to be bringing the awareness to the oncology world that, at the end of the day, liver cancer is two problems in one. There is the cancer itself, and there is the related liver cirrhosis, which might occur in most cases.

4 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
And, if anything, I’ll take you back in time. This is really almost 20 years ago. There was a settlement, and this is the best we can come up with for how to assess the cirrhosis, because there are different ways of doing so. And, at that time, this was part of the East–West meeting, which happened in Houston, TX, almost 20 years ago. We settled on the Child–Pugh score because everybody knows what it is. We can use it, and we’ll settle with it. And that’s why you’re seeing that all clinical trials are initially based on the Child–Pugh score. There are five parameters; three of them are measurable and can be assessed objectively. And encephalopathy and ascites, as we all know, are evaluated through subjective assessments. It’s not an evaluation of ascites by CT scan, it’s a physical exam. Encephalopathy is actually a neurologic exam; it’s not an ammonia level.
With this said, we end up with three scores: A, B, and C. This is an important reminder to all of us that the Child–Pugh scoring is not a linear curve. It’s not A to B to C at the same rate. Actually, people can live for a long time at Child–Pugh A, and then there is a turn to B, and then a chute into C. And as such, you might say to a patient, “Oh, by the way, your liver function is now level B,” and they’ll look at you and say, “Well, I never heard of this.” Because interestingly, the discussion about Child–Pugh A was so many years ago that they totally forgot about it, because life goes on. That’s why it’s important to really put this in the perspective in which we are dealing with it.
Barcelona Clinic Liver Cancer Staging1
1. Adapted from Forner A et al. Semin Liver Dis. 2010;30:61-74.
ECOG 0, Child A ECOG 0-2, Child A-B ECOG >2, Child C
Very early stage, single <2 cm
Early stage, ≤3 nodules, <3 cm, ECOG 0
Intermediate stage, multinodular, ECOG 0
Advanced stage, portal invasion, N1, M1, ECOG 1-2 Terminal stage
Single 3 nodules, ≤3 cm
Portal pressure/bilirubin
Increased
Associated diseases
No Normal
Resection
HCC
Yes
Sorafenib Transplant PEI/RFA
Curative Treatments
Chemoembolization
Palliative Options BSC
And with this said, we’ll move on to the Barcelona Clinic Liver Cancer (BCLC) staging system. It is a heavily used staging system by many of us because it really delineates very well what to do. It addresses not only who is the patient, but what to recommend for therapy. And, just to illustrate the point, small liver, small incursion, small lesion, and good liver function: surgery. Small lesion and a bad liver: transplant, et cetera.
One important component here—and these are probably things that we are learning as we move on in regard to the evaluation—is that the BCLC system does well in the early stages of the disease. It doesn’t do as well in regard to more advanced disease because it simply does not fine-tune this collection of patients with metastatic disease. Vascular invasion, N1, ECOG 1/2, and Child–
Pugh A/B are all put in one basket, while fine-tuning might be necessary.
Another important limitation of the Barcelona Clinic Liver Cancer staging system is there’s no horizontal translation in regard to where patients stand. If a patient is living with BCLC B, that’s it; you only can see them as BCLC B. How do they move from B to C? There were no intricate details that were written into this system, which at this point in time, I would definitely love to see it in a more three-dimensional perspective.
Tumor Board and MasterClass: Each speaker will present patient cases to illustrate the complexities of treatment decision-making and to effectively integrate multidisciplinary care strategies based on clinical evidence • Amit Singal, MD, MS, on selecting and sequencing TKIs across the continuum
of care in advanced HCC
• Katie Kelley, MD, on newer targeted and immunotherapy options as second-line treatment and beyond
• Prof. Riccardo Lencioni, MD, FSIR, EBIR, on expanding the therapeutic arsenal in earlier-stage disease
Today’s Agenda
With that said, there will be time for questions. And Dr. Singal will talk on selecting and sequencing TKIs across the continuum of care in advanced HCC. Dr. Kelley will talk on newer targeted and immunotherapy choices in second-line treatment and beyond, and Professor Lencioni will talk on expanding the therapeutic arsenal in the earlier-stage disease.
It’s my great honor to welcome Dr. Singal from UT Southwestern Medical Center, a very fine hepatologist about whom many of you know, and he’s going to talk to us about choosing and sequencing TKIs across the continuum of care in advanced HCC.
PeerView.com/XKX900

5
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
Tumor Board 1: 57-Year-Old Male With NASH Cirrhosis
Metabolic syndrome with diabetes complicated by stage 2 nephropathy and hypertension
Child–Pugh A: bilirubin 0.6, albumin 3.4, INR 1.1; no ascites or encephalopathy AFP 247 ng/mL ECOG PS 0 MRI shows multifocal HCC (LR-5) with four lesions
– The largest is 6 cm, and all four are in the right lobe No evidence of vascular invasion or distant metastases
Dr. Singal: So, I’m going to start my talk by introducing a case that will walk us through the sequencing of the TKIs. The patient is a 57-year-old male with NASH cirrhosis. As you would expect with NASH cirrhosis, he has an underlying metabolic syndrome, so he has diabetes, which is complicated by stage 2 nephropathy. He also has hypertension. He has Child–Pugh A liver disease, so he has a bilirubin of 0.6 mg/dL, albumin of 3.4 g/dL, and an INR of 1.1. He’s compensated, and you can see that his AFP is elevated at 247 ng/mL. He undergoes an MRI and is found to have multifocal HCC—all of them being LI-RADS 5—and he has four lesions. The largest lesion is 6 cm, and all of them are in the right lobe. So, the first thing that we can say is that he’s not eligible for any curative therapies at this time, and he would squarely fall into this BCLC stage B category.
Tumor Board 1: 57-Year-Old Male With NASH Cirrhosis (Cont’d)
Treated with TARE; stable disease on follow-up imaging
Treated with TACE with disease progression, including new tumor thrombus in the main portal vein
So, appropriately, he’s treated with locoregional therapy, and this patient underwent radioembolization. After undergoing the radioembolization, he has follow-up imaging, which shows he has stable disease. Given that he continues to have viable disease, he is actually treated with repeat locoregional therapy, also given
Choosing and Sequencing TKIs Across the Continuum of Care in Advanced HCC
that he continues to have good liver function. And at this point, unfortunately, he has disease progression, including a new tumor thrombus in the main portal vein.
Tumor Board 1 Discussion: Modified BCLC Staging System 20181
1. Galle PR et al. J Hepatol. 2018;69:182-236.
HCC in cirrhotic liver
Solitary 2-3 nodules ≤3 cm
Transplant candidate
Resection
No Yes No
Transplant Ablation Chemoembolization Systemic therapy
>5 y 3 mo >2.5 y
Ablation BSC
Optimal surgical candidate
≥10 mo
Yes
Very early stage (0) Single <2 cm
Preserved liver function PS 0
Early stage (A) Single or 2-3
nodules <3 cm Preserved liver function
PS 0
Intermediate stage (B) Multinodular, unresectable
Preserved liver function PS 0
Advanced stage (C) Portal invasion/
extrahepatic spread, Preserved liver function
PS 1-2
Terminal stage (D) Not transplantable
End-stage liver function
PS 3-4
So, once again, you just saw this in Ghassan’s introduction, and I think that he pointed out the strengths and limitations of the BCLC system. I think that right now, we’re becoming more and more cognizant about the possibility and the increasing use of stage migration. So, this patient started in the intermediate-stage category; therefore, he was treated with locoregional therapy, but now he has progressed, and so, with this progression, he clearly would no longer be eligible for locoregional therapy, and so, he would move squarely into the bucket where he would benefit from systemic therapy.
I think the other point that I will make, which is somewhat tangential to this specific case but also increasingly important, is that we also find that these are initial recommendations, but there’s significant heterogeneity in terms of these patient groups. And so, there are many patients who fall in this intermediate-stage category who are actually not 2B, but what I call B-minuses. These are patients who have a more advanced intrahepatic tumor burden and also would benefit from systemic therapy. And so, we are realizing that this is more of a continuum rather than clean buckets with clean breaks.
Tumor Board 1 Discussion: Frontline Options1
Treatment Evidence Recommendation
Sorafenib is the standard first-line systemic therapy for HCC, indicated for patients with • Well-preserved liver function (Child–Pugh A), and advanced
tumors (BCLC stage C) • Earlier-stage tumors progressing on, or unsuitable for, LRTs
High Strong
Lenvatinib is noninferior to sorafenib and is also recommended as first-line therapy for patients with • Well-preserved liver function, good PS, and advanced tumors
(BCLC stage C) without main portal vein invasion • Tumors progressing on, or unsuitable for, LRTs
High Strong
There are no clinical or molecular biomarkers established to predict response to first- or second-line systemic treatments Moderate –
1. Galle PR et al. J Hepatol. 2018;69:182-236.
So, when we take a look at guidelines in terms of what would be frontline options for systemic therapy, the nice thing is that we now have choices. In the frontline setting, we have two choices
Amit Singal, MD, MS
6 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
that have a high level of evidence and a strong recommendation for frontline options: sorafenib and lenvatinib.
The unfortunate thing is that we actually have no clinical or molecular biomarkers that are established to predict response to either of these therapies, and so we’re forced instead to depend on clinical factors when trying to decide between these two options.
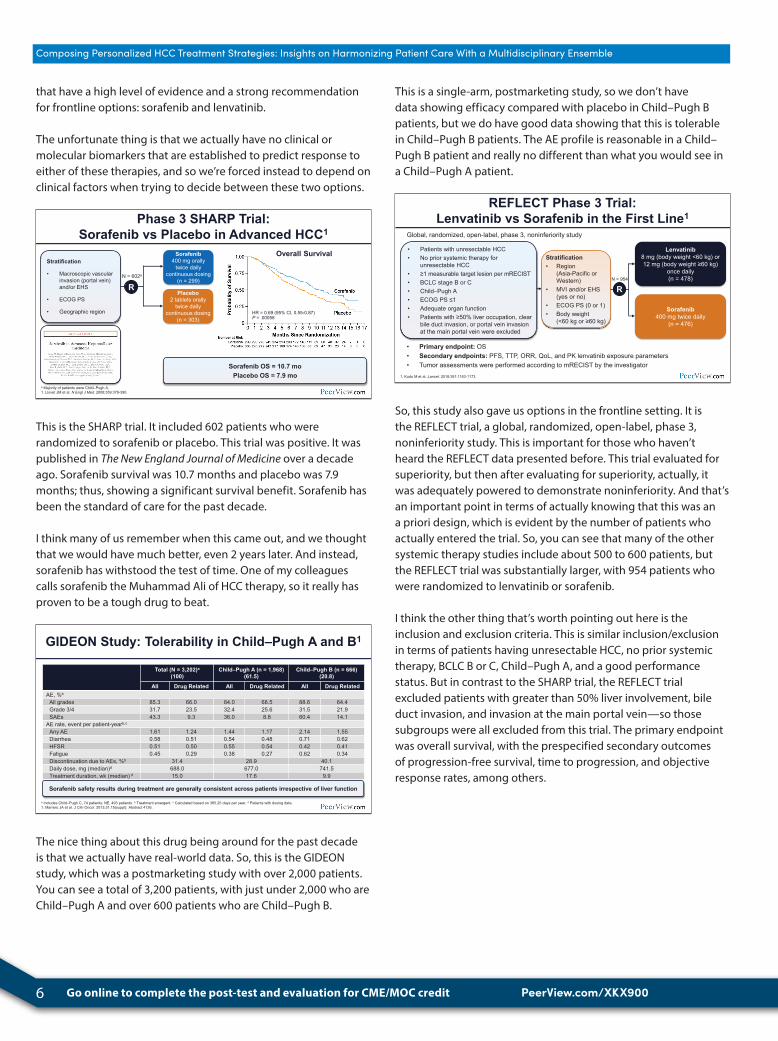
Phase 3 SHARP Trial: Sorafenib vs Placebo in Advanced HCC1
HR = 0.69 (95% CI, 0.55-0.87) P = .00058
Sorafenib OS = 10.7 mo Placebo OS = 7.9 mo
Stratification
• Macroscopic vascular invasion (portal vein) and/or EHS
• ECOG PS
• Geographic region
Sorafenib 400 mg orally
twice daily continuous dosing
(n = 299) R
N = 602a
Placebo 2 tablets orally
twice daily continuous dosing
(n = 303)
Overall Survival
a Majority of patients were Child–Pugh A. 1. Llovet JM et al. N Engl J Med. 2008;359:378-390.
This is the SHARP trial. It included 602 patients who were randomized to sorafenib or placebo. This trial was positive. It was published in The New England Journal of Medicine over a decade ago. Sorafenib survival was 10.7 months and placebo was 7.9 months; thus, showing a significant survival benefit. Sorafenib has been the standard of care for the past decade.
I think many of us remember when this came out, and we thought that we would have much better, even 2 years later. And instead, sorafenib has withstood the test of time. One of my colleagues calls sorafenib the Muhammad Ali of HCC therapy, so it really has proven to be a tough drug to beat.
GIDEON Study: Tolerability in Child–Pugh A and B1
a Includes Child–Pugh C, 74 patients; NE, 493 patients. b Treatment emergent. c Calculated based on 365.25 days per year. d Patients with dosing data. 1. Marrero JA et al. J Clin Oncol. 2013;31:15(suppl): Abstract 4126.
Total (N = 3,202)a (100)
Child–Pugh A (n = 1,968) (61.5)
Child–Pugh B (n = 666) (20.8)
All Drug Related All Drug Related All Drug Related AE, %b
All grades 85.3 66.0 84.0 68.5 88.6 64.4 Grade 3/4 31.7 23.5 32.4 25.6 31.5 21.9 SAEs 43.3 9.3 36.0 8.8 60.4 14.1
AE rate, event per patient-yearb,c
Any AE 1.61 1.24 1.44 1.17 2.14 1.55 Diarrhea 0.58 0.51 0.54 0.48 0.71 0.62 HFSR 0.51 0.50 0.55 0.54 0.42 0.41 Fatigue 0.45 0.29 0.38 0.27 0.62 0.34 Discontinuation due to AEs, %b 31.4 28.9 40.1 Daily dose, mg (median)d 688.0 677.0 741.5 Treatment duration, wk (median) d 15.0 17.6 9.9
Sorafenib safety results during treatment are generally consistent across patients irrespective of liver function
The nice thing about this drug being around for the past decade is that we actually have real-world data. So, this is the GIDEON study, which was a postmarketing study with over 2,000 patients. You can see a total of 3,200 patients, with just under 2,000 who are Child–Pugh A and over 600 patients who are Child–Pugh B.
This is a single-arm, postmarketing study, so we don’t have data showing efficacy compared with placebo in Child–Pugh B patients, but we do have good data showing that this is tolerable in Child–Pugh B patients. The AE profile is reasonable in a Child–Pugh B patient and really no different than what you would see in a Child–Pugh A patient.
REFLECT Phase 3 Trial: Lenvatinib vs Sorafenib in the First Line1
Global, randomized, open-label, phase 3, noninferiority study
• Primary endpoint: OS • Secondary endpoints: PFS, TTP, ORR, QoL, and PK lenvatinib exposure parameters • Tumor assessments were performed according to mRECIST by the investigator
• Patients with unresectable HCC • No prior systemic therapy for
unresectable HCC • ≥1 measurable target lesion per mRECIST • BCLC stage B or C • Child–Pugh A • ECOG PS ≤1 • Adequate organ function • Patients with ≥50% liver occupation, clear
bile duct invasion, or portal vein invasion at the main portal vein were excluded
Sorafenib 400 mg twice daily
(n = 476)
Lenvatinib 8 mg (body weight <60 kg) or 12 mg (body weight ≥60 kg)
once daily (n = 478)
R
1. Kudo M et al. Lancet. 2018;391:1163-1173.
Stratification • Region
(Asia-Pacific or Western)
• MVI and/or EHS (yes or no)
• ECOG PS (0 or 1) • Body weight
(<60 kg or ≥60 kg)
N = 954
So, this study also gave us options in the frontline setting. It is the REFLECT trial, a global, randomized, open-label, phase 3, noninferiority study. This is important for those who haven’t heard the REFLECT data presented before. This trial evaluated for superiority, but then after evaluating for superiority, actually, it was adequately powered to demonstrate noninferiority. And that’s an important point in terms of actually knowing that this was an a priori design, which is evident by the number of patients who actually entered the trial. So, you can see that many of the other systemic therapy studies include about 500 to 600 patients, but the REFLECT trial was substantially larger, with 954 patients who were randomized to lenvatinib or sorafenib.
I think the other thing that’s worth pointing out here is the inclusion and exclusion criteria. This is similar inclusion/exclusion in terms of patients having unresectable HCC, no prior systemic therapy, BCLC B or C, Child–Pugh A, and a good performance status. But in contrast to the SHARP trial, the REFLECT trial excluded patients with greater than 50% liver involvement, bile duct invasion, and invasion at the main portal vein—so those subgroups were all excluded from this trial. The primary endpoint was overall survival, with the prespecified secondary outcomes of progression-free survival, time to progression, and objective response rates, among others.
PeerView.com/XKX900
7
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
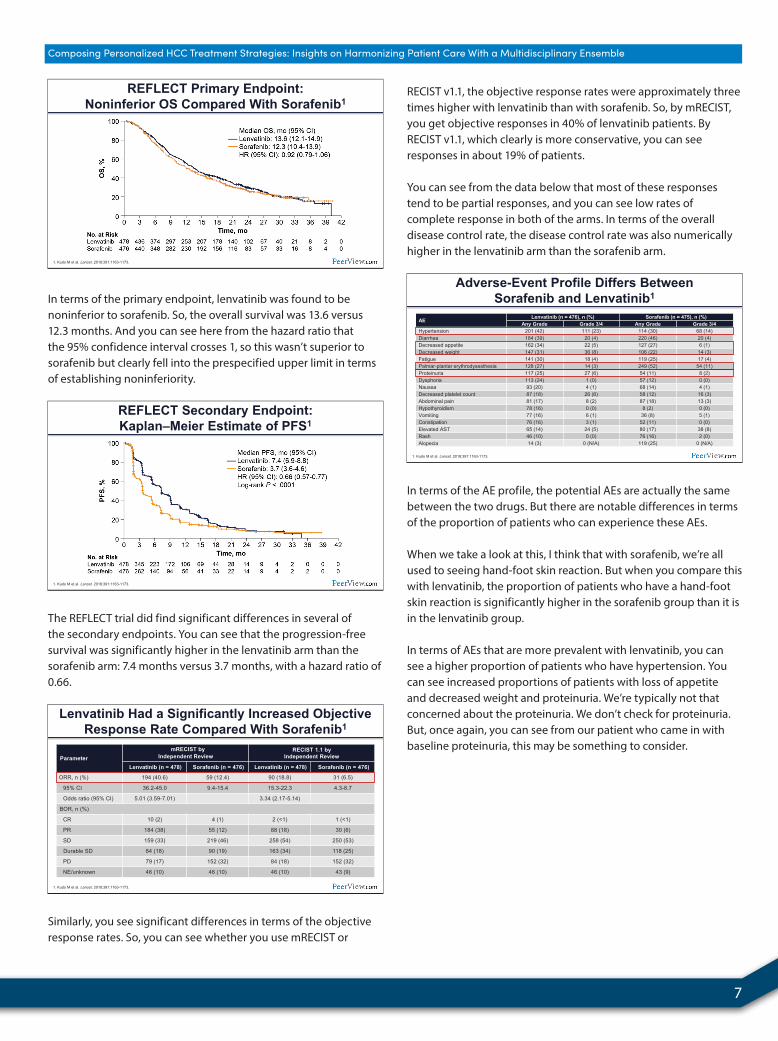
REFLECT Primary Endpoint: Noninferior OS Compared With Sorafenib1
1. Kudo M et al. Lancet. 2018;391:1163-1173.
In terms of the primary endpoint, lenvatinib was found to be noninferior to sorafenib. So, the overall survival was 13.6 versus 12.3 months. And you can see here from the hazard ratio that the 95% confidence interval crosses 1, so this wasn’t superior to sorafenib but clearly fell into the prespecified upper limit in terms of establishing noninferiority.
REFLECT Secondary Endpoint: Kaplan–Meier Estimate of PFS1
1. Kudo M et al. Lancet. 2018;391:1163-1173.
The REFLECT trial did find significant differences in several of the secondary endpoints. You can see that the progression-free survival was significantly higher in the lenvatinib arm than the sorafenib arm: 7.4 months versus 3.7 months, with a hazard ratio of 0.66.
Lenvatinib Had a Significantly Increased Objective Response Rate Compared With Sorafenib1
Parameter mRECIST by
Independent Review RECIST 1.1 by
Independent Review
Lenvatinib (n = 478) Sorafenib (n = 476) Lenvatinib (n = 478) Sorafenib (n = 476)
ORR, n (%) 194 (40.6) 59 (12.4) 90 (18.8) 31 (6.5)
95% CI 36.2-45.0 9.4-15.4 15.3-22.3 4.3-8.7
Odds ratio (95% CI) 5.01 (3.59-7.01) 3.34 (2.17-5.14)
BOR, n (%)
CR 10 (2) 4 (1) 2 (<1) 1 (<1)
PR 184 (38) 55 (12) 88 (18) 30 (6)
SD 159 (33) 219 (46) 258 (54) 250 (53)
Durable SD 84 (18) 90 (19) 163 (34) 118 (25)
PD 79 (17) 152 (32) 84 (18) 152 (32)
NE/unknown 46 (10) 46 (10) 46 (10) 43 (9)
1. Kudo M et al. Lancet. 2018;391:1163-1173.
Similarly, you see significant differences in terms of the objective response rates. So, you can see whether you use mRECIST or
RECIST v1.1, the objective response rates were approximately three times higher with lenvatinib than with sorafenib. So, by mRECIST, you get objective responses in 40% of lenvatinib patients. By RECIST v1.1, which clearly is more conservative, you can see responses in about 19% of patients.
You can see from the data below that most of these responses tend to be partial responses, and you can see low rates of complete response in both of the arms. In terms of the overall disease control rate, the disease control rate was also numerically higher in the lenvatinib arm than the sorafenib arm.
Adverse-Event Profile Differs Between Sorafenib and Lenvatinib1
1. Kudo M et al. Lancet. 2018;391:1163-1173.
AE Lenvatinib (n = 476), n (%) Sorafenib (n = 475), n (%) Any Grade Grade 3/4 Any Grade Grade 3/4
Hypertension 201 (42) 111 (23) 114 (30) 68 (14) Diarrhea 184 (39) 20 (4) 220 (46) 20 (4) Decreased appetite 162 (34) 22 (5) 127 (27) 6 (1) Decreased weight 147 (31) 36 (8) 106 (22) 14 (3) Fatigue 141 (30) 18 (4) 119 (25) 17 (4) Palmar-plantar erythrodysesthesia 128 (27) 14 (3) 249 (52) 54 (11) Proteinuria 117 (25) 27 (6) 54 (11) 8 (2) Dysphoria 113 (24) 1 (0) 57 (12) 0 (0) Nausea 93 (20) 4 (1) 68 (14) 4 (1) Decreased platelet count 87 (18) 26 (6) 58 (12) 16 (3) Abdominal pain 81 (17) 8 (2) 87 (18) 13 (3) Hypothyroidism 78 (16) 0 (0) 8 (2) 0 (0) Vomiting 77 (16) 6 (1) 36 (8) 5 (1) Constipation 76 (16) 3 (1) 52 (11) 0 (0) Elevated AST 65 (14) 24 (5) 80 (17) 38 (8) Rash 46 (10) 0 (0) 76 (16) 2 (0) Alopecia 14 (3) 0 (N/A) 119 (25) 0 (N/A)
In terms of the AE profile, the potential AEs are actually the same between the two drugs. But there are notable differences in terms of the proportion of patients who can experience these AEs.
When we take a look at this, I think that with sorafenib, we’re all used to seeing hand-foot skin reaction. But when you compare this with lenvatinib, the proportion of patients who have a hand-foot skin reaction is significantly higher in the sorafenib group than it is in the lenvatinib group.
In terms of AEs that are more prevalent with lenvatinib, you can see a higher proportion of patients who have hypertension. You can see increased proportions of patients with loss of appetite and decreased weight and proteinuria. We’re typically not that concerned about the proteinuria. We don’t check for proteinuria. But, once again, you can see from our patient who came in with baseline proteinuria, this may be something to consider.
8 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
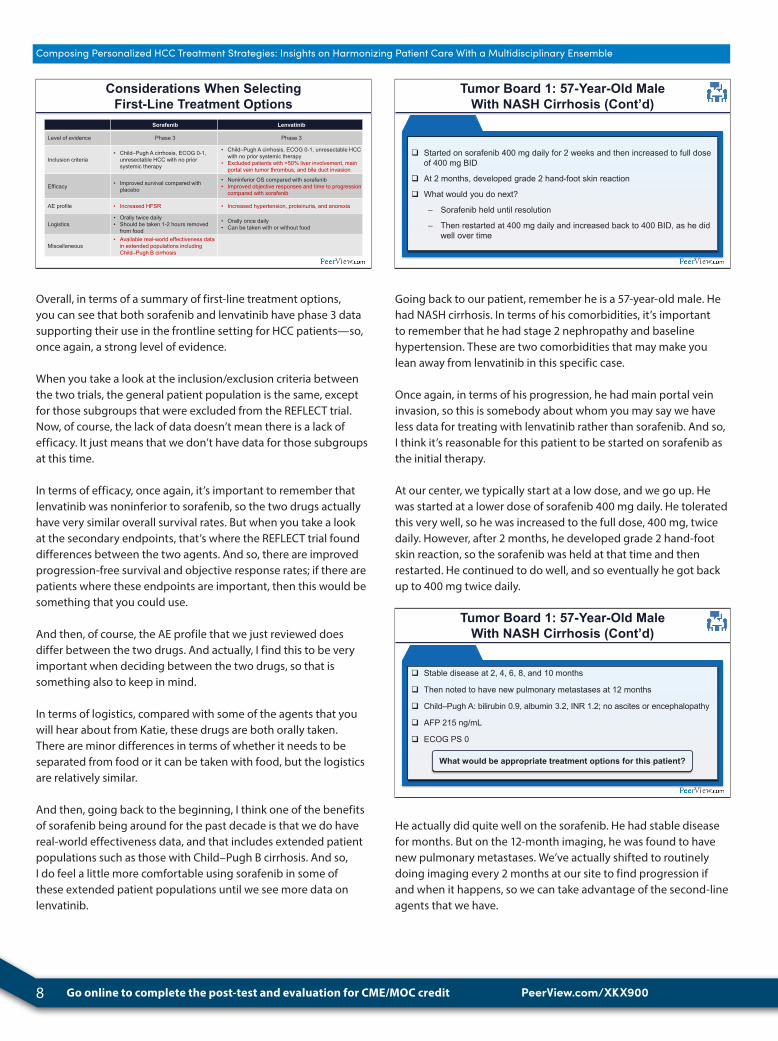
Sorafenib Lenvatinib
Level of evidence Phase 3 Phase 3
Inclusion criteria • Child–Pugh A cirrhosis, ECOG 0-1,
unresectable HCC with no prior systemic therapy
• Child–Pugh A cirrhosis, ECOG 0-1, unresectable HCC with no prior systemic therapy
• Excluded patients with >50% liver involvement, main portal vein tumor thrombus, and bile duct invasion
Efficacy • Improved survival compared with placebo
• Noninferior OS compared with sorafenib • Improved objective responses and time to progression
compared with sorafenib
AE profile • Increased HFSR • Increased hypertension, proteinuria, and anorexia
Logistics • Orally twice daily • Should be taken 1-2 hours removed
from food
• Orally once daily • Can be taken with or without food
Miscellaneous • Available real-world effectiveness data
in extended populations including Child–Pugh B cirrhosis
Considerations When Selecting First-Line Treatment Options
Overall, in terms of a summary of first-line treatment options, you can see that both sorafenib and lenvatinib have phase 3 data supporting their use in the frontline setting for HCC patients—so, once again, a strong level of evidence.
When you take a look at the inclusion/exclusion criteria between the two trials, the general patient population is the same, except for those subgroups that were excluded from the REFLECT trial. Now, of course, the lack of data doesn’t mean there is a lack of efficacy. It just means that we don’t have data for those subgroups at this time.
In terms of efficacy, once again, it’s important to remember that lenvatinib was noninferior to sorafenib, so the two drugs actually have very similar overall survival rates. But when you take a look at the secondary endpoints, that’s where the REFLECT trial found differences between the two agents. And so, there are improved progression-free survival and objective response rates; if there are patients where these endpoints are important, then this would be something that you could use.
And then, of course, the AE profile that we just reviewed does differ between the two drugs. And actually, I find this to be very important when deciding between the two drugs, so that is something also to keep in mind.
In terms of logistics, compared with some of the agents that you will hear about from Katie, these drugs are both orally taken. There are minor differences in terms of whether it needs to be separated from food or it can be taken with food, but the logistics are relatively similar.
And then, going back to the beginning, I think one of the benefits of sorafenib being around for the past decade is that we do have real-world effectiveness data, and that includes extended patient populations such as those with Child–Pugh B cirrhosis. And so, I do feel a little more comfortable using sorafenib in some of these extended patient populations until we see more data on lenvatinib.
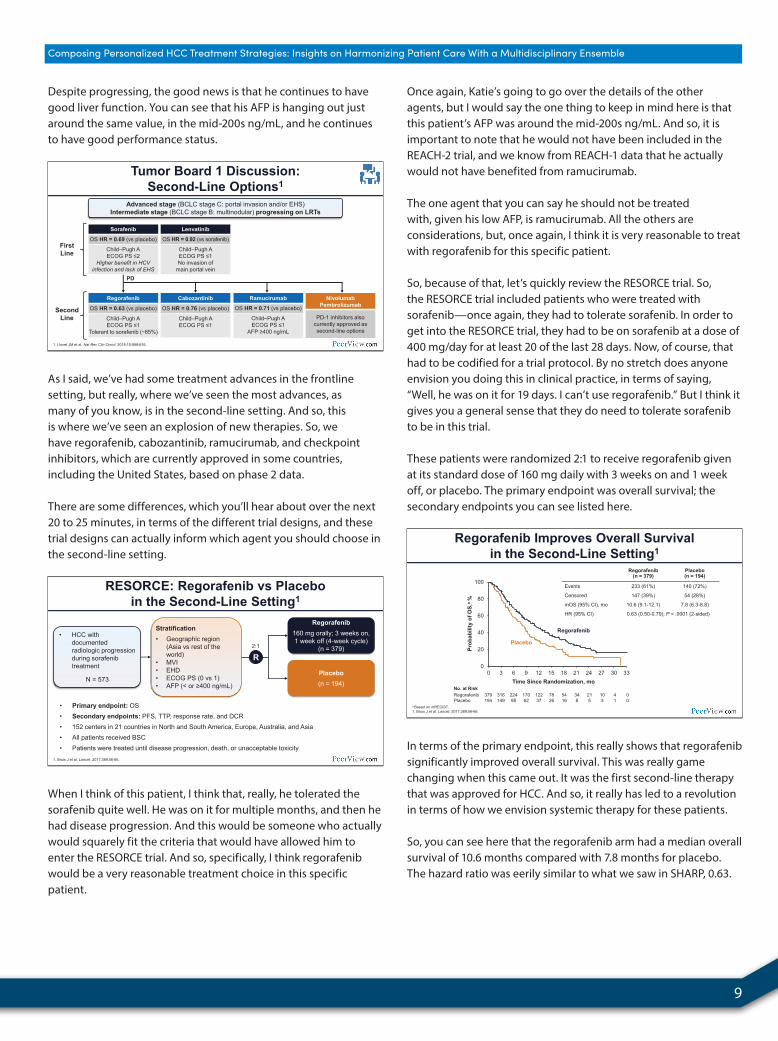
Tumor Board 1: 57-Year-Old Male With NASH Cirrhosis (Cont’d)
Started on sorafenib 400 mg daily for 2 weeks and then increased to full dose of 400 mg BID
At 2 months, developed grade 2 hand-foot skin reaction
What would you do next?
– Sorafenib held until resolution
– Then restarted at 400 mg daily and increased back to 400 BID, as he did well over time
Going back to our patient, remember he is a 57-year-old male. He had NASH cirrhosis. In terms of his comorbidities, it’s important to remember that he had stage 2 nephropathy and baseline hypertension. These are two comorbidities that may make you lean away from lenvatinib in this specific case.
Once again, in terms of his progression, he had main portal vein invasion, so this is somebody about whom you may say we have less data for treating with lenvatinib rather than sorafenib. And so, I think it’s reasonable for this patient to be started on sorafenib as the initial therapy.
At our center, we typically start at a low dose, and we go up. He was started at a lower dose of sorafenib 400 mg daily. He tolerated this very well, so he was increased to the full dose, 400 mg, twice daily. However, after 2 months, he developed grade 2 hand-foot skin reaction, so the sorafenib was held at that time and then restarted. He continued to do well, and so eventually he got back up to 400 mg twice daily.
Tumor Board 1: 57-Year-Old Male With NASH Cirrhosis (Cont’d)
Stable disease at 2, 4, 6, 8, and 10 months
Then noted to have new pulmonary metastases at 12 months
Child–Pugh A: bilirubin 0.9, albumin 3.2, INR 1.2; no ascites or encephalopathy
AFP 215 ng/mL
ECOG PS 0
What would be appropriate treatment options for this patient?
He actually did quite well on the sorafenib. He had stable disease for months. But on the 12-month imaging, he was found to have new pulmonary metastases. We’ve actually shifted to routinely doing imaging every 2 months at our site to find progression if and when it happens, so we can take advantage of the second-line agents that we have.
PeerView.com/XKX900
9
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
Despite progressing, the good news is that he continues to have good liver function. You can see that his AFP is hanging out just around the same value, in the mid-200s ng/mL, and he continues to have good performance status.
Tumor Board 1 Discussion: Second-Line Options1
1. Llovet JM et al. Nat Rev Clin Oncol. 2018;15:599-616.
First Line
SecondLine
PD
Nivolumab Pembrolizumab
PD-1 inhibitors also currently approved as second-line options
Ramucirumab
OS HR = 0.71 (vs placebo)
Child–Pugh A ECOG PS ≤1
AFP ≥400 ng/mL
Cabozantinib
OS HR = 0.76 (vs placebo)
Child–Pugh A ECOG PS ≤1
Regorafenib
OS HR = 0.63 (vs placebo)
Child–Pugh A ECOG PS ≤1
Tolerant to sorafenib (~85%)
Lenvatinib
OS HR = 0.92 (vs sorafenib)
Child–Pugh A ECOG PS ≤1 No invasion of
main portal vein
Sorafenib
OS HR = 0.69 (vs placebo)
Child–Pugh A ECOG PS ≤2
Higher benefit in HCV infection and lack of EHS
Advanced stage (BCLC stage C: portal invasion and/or EHS) Intermediate stage (BCLC stage B: multinodular) progressing on LRTs
As I said, we’ve had some treatment advances in the frontline setting, but really, where we’ve seen the most advances, as many of you know, is in the second-line setting. And so, this is where we’ve seen an explosion of new therapies. So, we have regorafenib, cabozantinib, ramucirumab, and checkpoint inhibitors, which are currently approved in some countries, including the United States, based on phase 2 data.
There are some differences, which you’ll hear about over the next 20 to 25 minutes, in terms of the different trial designs, and these trial designs can actually inform which agent you should choose in the second-line setting.
RESORCE: Regorafenib vs Placebo in the Second-Line Setting1
• Primary endpoint: OS • Secondary endpoints: PFS, TTP, response rate, and DCR • 152 centers in 21 countries in North and South America, Europe, Australia, and Asia • All patients received BSC • Patients were treated until disease progression, death, or unacceptable toxicity
• HCC with documented radiologic progression during sorafenib treatment
N = 573 Placebo (n = 194)
Regorafenib 160 mg orally; 3 weeks on, 1 week off (4-week cycle)
(n = 379) R
1. Bruix J et al. Lancet. 2017;389:56-66.
Stratification • Geographic region
(Asia vs rest of the world)
• MVI • EHD • ECOG PS (0 vs 1) • AFP (< or ≥400 ng/mL)
2:1
When I think of this patient, I think that, really, he tolerated the sorafenib quite well. He was on it for multiple months, and then he had disease progression. And this would be someone who actually would squarely fit the criteria that would have allowed him to enter the RESORCE trial. And so, specifically, I think regorafenib would be a very reasonable treatment choice in this specific patient.
Once again, Katie’s going to go over the details of the other agents, but I would say the one thing to keep in mind here is that this patient’s AFP was around the mid-200s ng/mL. And so, it is important to note that he would not have been included in the REACH-2 trial, and we know from REACH-1 data that he actually would not have benefited from ramucirumab.
The one agent that you can say he should not be treated with, given his low AFP, is ramucirumab. All the others are considerations, but, once again, I think it is very reasonable to treat with regorafenib for this specific patient.
So, because of that, let’s quickly review the RESORCE trial. So, the RESORCE trial included patients who were treated with sorafenib—once again, they had to tolerate sorafenib. In order to get into the RESORCE trial, they had to be on sorafenib at a dose of 400 mg/day for at least 20 of the last 28 days. Now, of course, that had to be codified for a trial protocol. By no stretch does anyone envision you doing this in clinical practice, in terms of saying, “Well, he was on it for 19 days. I can’t use regorafenib.” But I think it gives you a general sense that they do need to tolerate sorafenib to be in this trial.
These patients were randomized 2:1 to receive regorafenib given at its standard dose of 160 mg daily with 3 weeks on and 1 week off, or placebo. The primary endpoint was overall survival; the secondary endpoints you can see listed here.
Regorafenib Improves Overall Survival in the Second-Line Setting1
a Based on mRECIST. 1. Bruix J et al. Lancet. 2017;389:56-66.
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27 30 33
Prob
abili
ty o
f OS,
a %
Time Since Randomization, mo No. at Risk Regorafenib 379 316 224 170 122 78 54 34 21 10 4 0 Placebo 194 149 95 62 37 26 16 8 5 3 1 0
Placebo
Regorafenib
Regorafenib (n = 379)
Placebo (n = 194)
Events 233 (61%) 140 (72%)
Censored 147 (39%) 54 (28%)
mOS (95% CI), mo 10.6 (9.1-12.1) 7.8 (6.3-8.8)
HR (95% CI) 0.63 (0.50-0.79); P < .0001 (2-sided)
In terms of the primary endpoint, this really shows that regorafenib significantly improved overall survival. This was really game changing when this came out. It was the first second-line therapy that was approved for HCC. And so, it really has led to a revolution in terms of how we envision systemic therapy for these patients.
So, you can see here that the regorafenib arm had a median overall survival of 10.6 months compared with 7.8 months for placebo. The hazard ratio was eerily similar to what we saw in SHARP, 0.63.

10 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
Regorafenib Survival Benefit Consistent Across Subgroup Analyses1
1. Bruix J et al. Lancet. 2017;389:56-66.
When you take a look at the subgroup analyses, you can see that regorafenib had a consistent survival benefit across all different subgroups. I’m not going to go through these one by one. But I do want to point out, once again, because AFP is now being used as a selection biomarker for ramucirumab, I think it is worth noting that in the subgroup analyses from the RESORCE trial that regorafenib had a consistent benefit in both low-AFP and high-AFP patients.
Treatment-Emergent AE Profile1
1. Bruix J et al. Lancet. 2017;389:56-66.
Regorafenib (n = 374), n (%) Placebo (n =193), n (%)
Any Grade Grade 3 Grade 4 Any Grade Grade 3 Grade 4
Any AE 346 (93) 173 (46) 14 (4) 100 (52) 31 (16) 1 (1)
HFSR 196 (52) 47 (13) N/A 13 (7) 1 (1) N/A
Diarrhea 125 (33) 9 (2) 0 18 (9) 0 0
Fatigue 110 (29) 24 (6) N/A 37 (19) 3 (2) N/A
Hypertension 87 (23) 48 (13) 1 (<1) 9 (5) 6 (3) 0
Anorexia 88 (24) 10 (3) 0 12 (6) 0 0
Increased blood bilirubin 70 (19) 24 (6) 1 (<1) 7 (4) 4 (2) 0
Abdominal pain 34 (9) 5 (1) N/A 5 (3) 0 N/A
Increased AST 48 (13) 16 (4) 3 (1) 15 (8) 9 (5) 1 (1)
When you take a look at the AE profile, once again, given the similarity in terms of structure to sorafenib, it’s not surprising that the AE profile is similar to that of other TKIs. And so, there’s nothing surprising in terms of the AEs, including hand-foot skin reaction, diarrhea, fatigue, hypertension, and anorexia.
I think all of us are very comfortable managing these AEs. I think the one thing to take away from this is that, compared with some of the horror stories you hear with regorafenib in colon cancer, regorafenib actually appears to be much better tolerated in HCC patients. The AEs are not as difficult to manage, at least in our experience. And I think part of this, once again, is related to that patient selection because of the requirement of sorafenib tolerance to get into the trial.
Sequencing Systemic Therapies Can Provide Meaningful Survival Exceeding 2 Years1,2
1. Finn RS et al. 2017 American Society of Clinical Oncology Gastrointestinal Cancers Symposium (ASCO GI 2017). Abstract 344. 2. Finn RS et al. J Hepatol. 2018;69:353-358.
n = 374 n = 193
n = 143 n = 73
n = 231 n = 120
0 10 20 30
Rest of the World
Asia
All Patients
Time From Start of Sorafenib Treatment to Death, mo
26 (22.6-28.1) 19.2 (16.3-22.8)
21.5 (19.6-27.8) 15.6 (12.2-24.9)
26.8 (23.3-29.1) 20.1 (17.5-25.9)
n = 374 n = 193
n = 143 n = 73
n = 231 n = 120
Regorafenib Placebo
This was a nice post hoc analysis, which was done by Richard Finn and colleagues, in terms of showing the benefit of sequential therapy. And so, what this did was actually take a look at the median survival from the start of sorafenib all the way through regorafenib. You can see that by using the two drugs in sequence, you can actually get a median survival of 26 months.
I actually find these data very helpful personally when I’m talking to patients because I think it takes away some of the historic skepticism, which we used to sometimes hear of, “Oh, it improves survival, but it’s still only a year.” This is why I think that this was really revolutionary, because now, by sequencing these drugs and doing this appropriately, you can actually achieve a meaningful survival that actually exceeds 2 years.
And this also informed our clinical practice, where once again, we monitor these patients on first-line therapy very closely, so we know when to switch to second-line therapy. And, equally important, when they’re on locoregional therapy, we look for TACE failure or TARE failure or locoregional therapy failure, so we can actually transition to first-line therapy at a good time. So, it’s really important that patients come in with a good performance status and good reserve, so we can get them through the entire sequence of systemic therapy.
• Sorafenib and lenvatinib are both approved options for first-line treatment of patients with unresectable HCC
– There are subtle differences in inclusion criteria, efficacy, and adverse event profiles that can help us decide between two agents
• There are multiple options for second-line treatment of patients who are intolerant or have disease progression on first-line therapy
– Regorafenib: RESORCE trial showed superiority over placebo
– Using agents in sequence can result in a meaningful survival benefit
• Studies are needed to identify treatment-response biomarkers to select the ideal sequence of treatments for individual patients
Conclusions
In conclusion, sorafenib and lenvatinib are both approved options for first-line treatment of patients with unresectable HCC. Once again, we’ve extensively talked about the differences between these agents in terms of inclusion/exclusion criteria, efficacy, and
PeerView.com/XKX900

11
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
AE profiles, which can help us decide. I think everyone hopes that we’ll have some kind of biomarker in the future, but in the meantime, I think these are helpful in clinical practice.
Multiple options for second-line therapies—you’ll hear about more of that from Katie in just a minute. But, once again, you did hear the RESORCE trial data that showed superiority over placebo and really established regorafenib as an option in the second-line setting. By using these therapies in sequence, we can really have a meaningful survival benefit.
And then, once again, to highlight this because I think it is really an important point, the hope is that we can really have treatment-response biomarkers so we can really start toward a personalized regimen and really select things individually. And, therefore, we can become much smarter than what we do right now. Thank you.
Newer Targeted and Immunotherapy Options as Second-Line Treatment and Beyond
Tumor Board 2: 62-Year-Old Male With Chronic HBV
Asian male with chronic HBV on entecavir with undetectable viral load
Child–Pugh A, platelets 259, ECOG 0
Screening AFP showed new elevation to 58 ng/mL; was normal 12 months earlier
MRI showed 14-cm right lobe tumor, HCC (LR-5), with two satellite lesions; diminutive left lobe
No evidence of vascular invasion or distant metastases
Treated with TARE with tumor necrosis but new tumor thrombus in main portal vein and multiple new bilateral pulmonary nodules
Started on sorafenib 400 mg twice daily (standard dose)
– Developed redness and discomfort of palms and soles after 2 weeks, blistering at 3 weeks despite optimal hand-foot skin care; required treatment delay then dose reduction after 3 weeks
– Patient did not tolerate sorafenib despite dose reduction and delays due to grade 3 hand-foot skin reaction and had to discontinue
AFP 283 ng/mL
ECOG PS 0
Dr. Abou-Alfa: We’ll move on to the next presentation by Dr. Katie Kelley, who is Associate Professor at the University of California, San Francisco. She is going to talk to us about newer targeted immunotherapy options in second-line treatment and beyond. Thank you.
Dr. Kelley: Thank you so much for having me today, Ghassan, and to all of you for your attention. I’ll start also with a case from my practice, which is a pretty common type of patient, a 62-year-old gentleman with chronic hepatitis B on antiviral therapy. He was well suppressed on entecavir, Child–Pugh A, and had no evidence of portal hypertension with normal platelets, and ECOG 0.
He was being closely followed in our hepatology practice and was found to have a new elevation in AFP, which had been normal about 12 months prior. This prompted imaging that eventually showed a rather large, out-of-the-blue tumor, which hadn’t been seen on prior scans, maybe 2 years earlier. It was a 14-cm right lobe tumor, with two satellite lesions and a pretty diminutive left lobe.
He had no evidence of vascular invasion or distant metastases, so he was treated with liver-directed therapy, with TARE, and had, initially, a good response with tumor necrosis. But eventually, he developed new tumor thrombus in the main portal vein and new bilateral pulmonary nodules, so he was referred to oncology for systemic therapy.
So, this patient actually presented a couple of years prior to the advent of lenvatinib, though his tumor was quite large, he wouldn’t have qualified for the REFLECT trial—as Amit has just described to us. He was started on sorafenib 400 mg twice a day, which is, of course, the standard dose. But, after just 2 weeks, he
Robin K. (“Katie”) Kelley, MD

12 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
developed redness and pain in his palms and soles, which was considered consistent with palmoplantar erythrodysesthesia, or hand-foot syndrome. He required treatment delay and then dose reduction. However, despite dose reduction, he actually required several other delays and finally discontinued [sorafenib] because of hand-foot syndrome.
So, at this point, we have a patient who had discontinued sorafenib for hand-foot syndrome. He had an AFP of 283 ng/mL at this point, so he had some evidence of progression as well, and an ECOG that remained 0.
Tumor Board 2 Discussion: Multiple Options Beyond First-Line Therapy1
1. Llovet JM et al. Nat Rev Clin Oncol. 2018;15:599-616.
First Line
SecondLine
PD
Nivolumab Pembrolizumab
PD-1 inhibitors also currently approved as second-line options
Ramucirumab
OS HR = 0.71 (vs placebo)
Child–Pugh A ECOG PS ≤1
AFP ≥400 ng/mL
Cabozantinib
OS HR = 0.76 (vs placebo)
Child–Pugh A ECOG PS ≤1
Regorafenib
OS HR = 0.63 (vs placebo)
Child–Pugh A ECOG PS ≤1
Tolerant to sorafenib (~85%)
Lenvatinib
OS HR = 0.92 (vs sorafenib)
Child–Pugh A ECOG PS ≤1 No invasion of
main portal vein
Sorafenib
OS HR = 0.69 (vs placebo)
Child–Pugh A ECOG PS ≤2
Higher benefit in HCV infection and lack of EHS
Advanced stage (BCLC stage C: portal invasion and/or EHS) Intermediate stage (BCLC stage B: multinodular) progressing on LRTs
So, turning back to Amit’s slides, here is sort of the lay of the land of our treatment options for this patient. We have sorafenib and lenvatinib in the first line. This patient has already received sorafenib and did not tolerate it. Therefore, he did not meet criteria for participation in the RESORCE trial because he was not sorafenib tolerant.
CELESTIAL: Cabozantinib vs Placebo After Prior Sorafenib1
• Primary endpoint: OS • Secondary endpoints: PFS and ORR
• Advanced HCC; Child–Pugh A
• ECOG PS 0-1 • Prior sorafenib • Progression on ≥1
prior therapy • ≤2 prior therapies
N = 760
Placebo
Cabozantinib 60 mg/d
R
1. Abou-Alfa G et al. N Engl J Med. 2018;379:54-63.
Stratification
• Disease etiology (HBV, HCV, other)
• Region (Asia, other)
• Presence of MVI and/or EHS of disease (yes or no)
2:1
All patients had previously received sorafenib, and 27% had received two previous systemic anticancer regimens for advanced HCC
And so, I’ll use this case to move on to the next agent in our armamentarium now, which is cabozantinib, to describe where it fits in this new and evolving complex second-line landscape.
So, the CELESTIAL trial was a randomized, phase 3, international trial of cabozantinib versus placebo in patients with advanced HCC. The trial required Child–Pugh A for eligibility, as well as a good performance status, and progression on one or two—no more than two—prior systemic therapies. They also had to have
had prior sorafenib, although no duration, dose, or tolerability of sorafenib was specified in the eligibility criteria.
About 760 patients were enrolled and stratified according to disease etiology—hepatitis B, hepatitis C, or other—geographical region, and the presence or absence of macrovessel invasion and/or extrahepatic spread. The randomization was 2:1 to cabozantinib 60 mg/day versus placebo. The primary endpoint was overall survival, and the key secondary endpoints were PFS and ORR.
January 2019: Cabozantinib was approved for use in patients with advanced HCC previously treated with sorafenib
Cabozantinib Improves Overall Survival in the Second- or Third-Line Setting1
a Critical P ≤ .021 for second interim analysis. 1. Abou-Alfa G et al. N Engl J Med. 2018;379:54-63.
a
This study showed that cabozantinib improves overall survival in either the second- or third-line setting. Here, you can see the Kaplan–Meier curve showing the median overall survival on cabozantinib was 10.2 months by comparison with 8.0 months for placebo. It had a hazard ratio of 0.76 and a P value of.005.
Cabozantinib Improves Progression-Free Survival in the Second- or Third-Line Setting1
1. Abou-Alfa G et al. N Engl J Med. 2018;379:54-63.
• ORR: cabozantinib 4% vs placebo 0.4% (P = .0086) • PR or SD: cabozantinib 64% vs placebo 33%
Progression-free survival was likewise improved, with a median PFS of 5.2 months for cabozantinib and 1.9 months for placebo. It had a hazard ratio of 0.44 and a P value of less than.0001. The objective response rate was rather low, which is consistent with TKIs using RECIST v1.1 for measurement. The objective response rate was 4.4% for cabozantinib versus almost zero for placebo.
PeerView.com/XKX900

13
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
No. of patients OS PFS
HR HR
Overall 707 0.76 0.44
Region Asia Other regions
175 532
1.01 0.71
0.46 0.45
Race Asian Non-Asian
241 423
0.86 0.75
0.43 0.47
EHS and/or MVI Yes No
598 109
0.73 0.99
0.45 0.46
Etiology HBV HCV Other
267 156 284
0.69 1.11 0.72
0.31 0.61 0.48
Prior lines of therapy 1 prior regimen 2 prior regimens
509 192
0.74 0.90
0.43 0.58
Cabozantinib Survival Benefit Consistent Across Subgroup Analyses1
1. Abou-Alfa G et al. N Engl J Med. 2018;379:1384-1385.
0.5 Favors cabozantinib
0.25 1 2 Favors placebo
0.5 Favors cabozantinib
0.25 0.1 0.2 Favors placebo
We can see a forest plot according to relevant subgroups showing a generally favorable OS across subgroups and a clear significant benefit of PFS for all subgroups analyzed.
All-Causality Grade 3 or 4 AEs1,a
a Grade 3/4 events reported in at least 5.0% of patients in either treatment group. 1. Abou-Alfa G et al. N Engl J Med. 2018;379:54-63.
AE, % Cabozantinib (n = 467)
Placebo (n = 237)
Any grade 3 or 4 AE 68 36
HFSR 17 0
Hypertension, 16 2
Increased AST 12 7
Fatigue 10 4
Diarrhea 10 2
Asthenia 7 2
Decreased appetite 6 <1
Anemia 4 5
Grade 5 TRAEs • Cabozantinib (n = 6):
hepatic failure, esophagobronchial fistula, portal vein thrombosis, upper GI hemorrhage, pulmonary embolism, and hepatorenal syndrome
• Placebo (n = 1): hepatic failure
The adverse event profile on cabozantinib, again, is consistent with its status as a multikinase inhibitor, including classic TKI toxicities of hand-foot skin reaction in about 17% of patients at the grade 3 or 4 level, hypertension, increased AST, fatigue, diarrhea, asthenia, and decreased appetite. Again, it is similar to what we expect with sorafenib, lenvatinib, and regorafenib, but with slightly different incidences according to each drug, and all were manageable.
There were class-effect grade 5 AEs, including antiangiogenic toxicity, such as fistula, portal vein thrombosis, and bleeding, in about six patients in the treatment arm compared with one in the placebo arm. Noting, again, the 2:1 randomization, we did expect more patients to develop AEs in the treatment arm.
Tumor Board 2 Discussion: 62-Year-Old Male With Chronic HBV (Cont’d)
Started cabozantinib with empiric starting dose reduction to 40 mg daily; AFP 283 ng/mL
Required dose reduction to 20 mg daily after 2 weeks due to abdominal cramping and diarrhea
Restaging CT after 2 and 4 months showed tumor regression; AFP declined to nadir of 137 ng/mL
Restaging CT after 6 months showed tumor progression with new ascites, elevated bilirubin, AFP elevation to 400 ng/mL; discontinued cabozantinib; required paracentesis and transitioned to palliative care
So, turning back to the case again, the patient had been sorafenib intolerant and would not have qualified for regorafenib, so I actually started him on cabozantinib with an empiric starting dose reduction—again, that’s not based on any prospective data but based on clinical experience so far. I started him on 40 mg/day.
He eventually required further dose reduction to 20 mg daily after about 2 weeks because of some abdominal symptoms, but actually, he tolerated that quite well. I restaged him 2 months and 4 months later. He actually had an initial AFP response and rather impressive tumor regression. And he had a period of time where he was able to go to Disneyland and had a pretty nice quality of life during that 4-month period. Unfortunately, by 6 months, though, he started to have progression again and eventually had to discontinue cabozantinib because of progression.
Tumor Board 3: 64-Year-Old Male With HCV Cirrhosis
Metabolic syndrome with diabetes complicated by stage 2 nephropathy and hypertension
Child–Pugh A: bilirubin 1.2, albumin 3.1, INR 1.1; no ascites or encephalopathy
AFP 247 ng/mL ECOG PS 0 MRI showed multifocal HCC (LR-5) with four
lesions (the largest was 6 cm), and hepatic vein tumor thrombus
Treated with multiple TACE over 2 years – Developed disease progression including rib,
nodal, and adrenal metastases – Received palliative RT to painful rib metastasis
Started on sorafenib 400 mg BID
– Required augmented antihypertensive regimen
– Grade 1-2 hand-foot syndrome and loose stools
Had stable disease and AFP declined to nadir 120 ng/mL over 6 months, then developed rising AFP and progression in adrenal, nodal, and rib metastases
AFP 1,054 ng/mL
ECOG PS 0
So, here’s another real-world case: A 64-year-old man with hepatitis C cirrhosis attributed to metabolic syndrome. He also had stage 2 nephropathy and some hypertension, but he was Child–Pugh A with an ECOG of 0 and an AFP of 247 ng/mL.
He eventually got scanned because of abdominal pain and was found to have multifocal HCC, which was radiographically diagnosed by LI-RADS 5 criteria with four lesions, as well as hepatic vein tumor thrombus consistent with BCLC C.
He actually did well with TACE, despite the small vascular invasion, and received TACE for about 2 years after diagnosis. But he developed multifocal progression, including rib, nodal, and

14 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
adrenal metastases, which we treated with palliative radiation to the bone metastases, and then we started him on first-line sorafenib. Again, sorafenib was the only FDA-approved agent at the time.
He did require blood pressure medications for hypertension and had grade 1/2 hand-foot syndrome, but it was well controlled with topical therapies. He was treated with sorafenib for about 6 months before he developed rising AFP and radiographic progression, as well as an AFP progression to over 1,000 ng/mL, but he still had a good performance status.
Tumor Board 3 Discussion: Multiple Options Beyond First-Line Therapy1
1. Llovet JM et al. Nat Rev Clin Oncol. 2018;15:599-616.
First Line
SecondLine
PD
Nivolumab Pembrolizumab
PD-1 inhibitors also currently approved as second-line options
Ramucirumab
OS HR = 0.71 (vs placebo)
Child–Pugh A ECOG PS ≤1
AFP ≥400 ng/mL
Cabozantinib
OS HR = 0.76 (vs placebo)
Child–Pugh A ECOG PS ≤1
Regorafenib
OS HR = 0.63 (vs placebo)
Child–Pugh A ECOG PS ≤1
Tolerant to sorafenib (~85%)
Lenvatinib
OS HR = 0.92 (vs sorafenib)
Child–Pugh A ECOG PS ≤1 No invasion of
main portal vein
Sorafenib
OS HR = 0.69 (vs placebo)
Child–Pugh A ECOG PS ≤2
Higher benefit in HCV infection and lack of EHS
Advanced stage (BCLC stage C: portal invasion and/or EHS) Intermediate stage (BCLC stage B: multinodular) progressing on LRTs
So, this brings us back to our treatment options, and I’ll take this opportunity to discuss the third box in our new second-line options section on the slide, which is ramucirumab.
197 172 121 87 56 37 26 14 4 0 0 0 0 0 95 76 50 36 19 12 4 1 0 0 0 0 0 0
119 93 65 46 35 22 12 8 4 2 1 1 1 0 131 90 44 28 18 14 8 4 3 1 0 0 0 0
Ramucirumab Improves Overall Survival in the Second-Line Setting in Patients With AFP ≥4001,2
1. Zhu AX et al. Lancet Oncol. 2015;16:859-870. 2. Zhu AX et al. J Clin Oncol. 2018;36:15(suppl): Abstract 4003.
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27 30 33 36 39
OS,
%
Time, mo
Censored observations Ramucirumab Placebo
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27 30 33 36 39
OS,
%
Time, mo No. at Risk Ramucirumab Placebo
Censored observations Ramucirumab Placebo
AFP ≥ 400 ng/mL REACH: RCT Subgroup Analysis REACH-2: RCT
Ramucirumab (n = 197)
Placebo (n = 95) Difference P
mOS, mo 8.5 7.3 1.2 – HR (95% CI) 0.710 (0.531-0.949) .0199
Ramucirumab (n = 119)
Placebo (n = 131) Difference P
mOS, mo 7.8 4.2 3.6 – HR (95% CI) 0.674 (0.508, 0.895) .0059
No. at Risk Ramucirumab Placebo
Ramucirumab was initially studied in the REACH trial, or REACH-1 trial, as we can now call it, retrospectively, which was an all-comer trial without selection by AFP criteria. It did not achieve significance for overall survival benefit in the overall study population. But subgroup analyses showed that patients with elevated alpha-fetoprotein greater than 400 ng/mL did have a significant benefit on ramucirumab, with a median overall survival of 7.8 months compared with 4.2 months. And, as we know from early-stage disease, this is a poor prognostic subgroup.
So, the strength of these findings prompted the development of REACH-2, a new and entirely separate phase 3 trial with biomarker selection for patients with elevated AFP greater than or equal
to 400 ng/mL for enrollment. And ramucirumab was found to have a significant prolonged overall survival of 8.5 months compared with 7.3 months for placebo, which did reach statistical significance with a hazard ratio of 0.7 and a P value of .0199.
And, while the difference was rather modest—we all would agree, I think, 1.2 months is a small delta—I think what’s important to note is there is a tail on these curves, which has been followed out and holds true for much longer than the study follow-up shown here. It potentially represents a meaningful benefit in these patients for the long term—or longer term, I should say.
Ramucirumab Improves Overall Survival in the Second-Line Setting in Patients With AFP ≥4001
1. Galle P et al. 12th Annual Conference of the International Liver Cancer Association (ILCA 2018). Abstract O-001.
Ramucirumab (n = 316)
Placebo (n = 226) Difference P
Death, n (%) 246 (77.8) 190 (84.1) – – mOS, mo 8.1 5.0 3.1 – HR (95% CI) 0.694 (0.571-0.842) .0002
And so, this again shows the pooled analysis of patients from REACH-2 and the original REACH-1, which had a larger number of patients.
It showed that if you combine the patients from the first study and from the REACH-2 study, the median overall survival is 8.1 months versus 5.0 months with placebo, again, supporting the approval of ramucirumab earlier this year [2019] for patients with a high AFP after progression on sorafenib—again, a high AFP being defined as greater than or equal to 400 ng/mL.
Ramucirumab Improves Overall Survival in the Second-Line Setting in Patients With AFP ≥4001
a Analysis used RECIST 1.1. 1. Llovet JM et al. ASCO 2019. Abstract 4073.
Analysis Populationa (Ramucirumab vs Placebo)
SOR Intolerant, n = 70 (Ramucirumab 42,
Placebo 28)
SOR Progressors, n = 472 (Ramucirumab 274,
Placebo 198)
OS median, mo 10.2 vs 6.7 8.0 vs 4.7
HR (95% CI) 0.59 (0.34-1.02) 0.71 (0.58-0.88)
PFS median, mo 4.4 vs 1.4 2.7 vs 1.6
HR (95% CI) 0.32 (0.19-0.55) 0.64 (0.52-0.79)
ORR, % 12 vs 0 4 vs 1
DCR, % 79 vs 21 53 vs 39
Discontinued due to related AEs any grade, % 12 vs 0 9 vs 4
At the 2019 ASCO Annual Meeting (ASCO 2019) this year, Dr. Llovet and colleagues presented an abstract looking at outcomes in patients receiving ramucirumab in the second-line setting. The patients were divided according to whether they had prior progression on sorafenib—the sorafenib progressors—and had prior exposure to antiangiogenic TKIs prior to ramucirumab,
PeerView.com/XKX900

15
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
or if they had been sorafenib intolerant, which was a smaller population but included patients who had not had prior exposure to antiangiogenic therapy due to discontinuation for toxicity.
And this interesting subanalysis showed that patients with sorafenib intolerance had a distinctly longer overall survival on ramucirumab, as one might expect, since ramucirumab is a VEGFR2 monoclonal antibody—and reinforces the value of hitting this target in the second line.
AE,a n (%) Ramucirumab (n = 197) Placebo (n = 95)
Any Grade Grade ≥3 Any Grade Grade ≥3 Hypertension 49 (24.9) 25 (12.7) 12 (12.6) 5 (5.3) Bleeding/hemorrhage events 48 (24.4) 10 (5.1) 12 (12.6) 3 (3.2)
GI hemorrhage events 12 (6.1) 7 (3.6) 5 (5.3) 2 (2.1) Epistaxis 27 (13.7) 1 (0.5) 3 (3.2) 0
Proteinuria 40 (20.3) 4 (2.0) 4 (4.2) 0 Arterial thromboembolic events 5 (2.5) 3 (1.5) 1 (1.1) 1 (1.1) Venous thromboembolic events 2 (1.0) 0 2 (2.1) 1 (1.1) GI perforation 2 (1.0) 2 (1.0) 2 (2.1) 2 (2.1) Fistula 1 (0.5) 0 0 0
Ascites 35 (17.8) 8 (4.1) 7 (7.4) 2 (2.1) Hepatic encephalopathy 8 (4.1) 6 (3.0) 0 0
Infusion-related reactionsb 17 (8.6) 0 3 (3.2) 0
Adverse Events of Special Interest1
a AEs of special interest according to MedRA preferred terms or consolidated categories. b Infusion-related reactions occuring within 24 hours of infusion. 1. Zhu AX et al. Lancet Oncol. 2019;20:282-296.
So, adverse events of special interest on ramucirumab, again, follow its class effect as an antiangiogenic VEGFR2 monoclonal antibody. And we see highlighted, grade 3 and greater hypertension, with 25% for ramucirumab by comparison with 5% for the placebo.
Also highlighted, is an important finding. Though not too common, there were 25 events or 12% of patients with grade 3 hypertension and six events or 3% of patients with grade 3 or higher encephalopathy, which, again, is a rare event but important in our population with underlying liver dysfunction. And also, it’s a reminder to watch for hepatic decompensation, in particular, in patients on all therapies.
Tumor Board 3: Decision-Making
• Regorafenib, cabozantinib, and ramucirumab are all appropriate choices for second-line therapy based on the case features (AFP >400, tolerance of first-line treatment, and Child–Pugh A)
– Benefit with ramucirumab in patients with AFP ≥400 ng/mL
– Benefit with cabozantinib and regorafenib is independent of baseline AFP and includes high AFP subgroups
• Could also consider IO therapies in the second-line setting based on phase 2 data
So, returning to the case, just to refresh, he had tolerated sorafenib and had initially done well, but then he progressed with metastatic progression in adrenal gland and bone. He also had an AFP rise to greater than 1,000 ng/mL.
So, in this case, as he had tolerated sorafenib, he would have been a good candidate for regorafenib. Cabozantinib doesn’t require prior sorafenib tolerance, so cabozantinib would also have been a reasonable choice. And based on his high AFP value, ramucirumab may also have been an option.
This highlights the challenges we now have in the clinic when choosing between these agents, which all have positive data showing the prolongation of survival in the second or higher setting. But, just a reminder that to distinguish among these agents, ramucirumab really only has a benefit that we’ve seen in patients with greater than or equal to AFP of 400 ng/mL, while cabozantinib and regorafenib have a benefit independent of baseline AFP and show survival and PFS improvements across a range of AFP levels, including greater than 400 ng/mL.
Have We Made Progress With Immunotherapy?
And as a segue into the next part of the talk, the plot is even more complex now with IO therapies, or immuno-oncology therapies, which are now approved in the second-line setting based on phase 2 data. So, that brings me to the next section. Have we made progress with immunotherapy?
Checkpoint Inhibitor Landscape for HCC in the United States
1. NCCN Clinical Practice Guidelines in Oncology. Hepatobiliary Cancers. V2.2019. Accessed September 15, 2019. 2. http://www.clinicaltrials.gov. Accessed September 15, 2019.
FDA Approved for Subsequent-Line Therapy if There Is Disease Progression1
Pembrolizumab Child–Pugh A
Nivolumab Child–Pugh A or B7
Emerging Checkpoint Inhibitors Under Investigation for HCC2 Tislelizumab Targets PD-1
Phase 3: Monotherapy in first line
Atezolizumab Targets PD-L1
Phase 3: With cabozantinib in first line Phase 3: With bevacizumab in first line
Durvalumab
Targets PD-L1 Phase 3: With tremelimumab in first line
Pembrolizumab Targets PD-1
Phase 3: With lenvatinib in first line
So, this shows the dramatic differences now compared with just a few years ago in HCC. These are all the checkpoint inhibitor immunotherapy agents under investigation or approved for HCC, with nivolumab and pembrolizumab now approved after sorafenib for use in HCC. There are also ongoing pivotal trials of pembrolizumab, tislelizumab, durvalumab, and atezolizumab in various combinations for advanced HCC in the first line.

16 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
CheckMate -040: Nivolumab in HCC1,2
• Primary endpoints: safety/tolerability and ORR • Other endpoints: CR, DCR, DOR, TTR, TTP, TTP rate, PFS, OS, OS rate, biomarkers, and PK
• HCC not amenable to curative resection
• Child–Pugh ≤6, ≤7 for dose escalation, Child–Pugh B cohort
• Progressed on ≥1 prior line of systemic therapy, intolerant to sorafenib, or refused sorafenib
Nivolumab noninfected/HBV/HCV Dose escalation (n = 48)
Dose expansion (n = 214)
1. https://clinicaltrials.gov/ct2/show/NCT01658878. Accessed September 15, 2019. 2. El-Khoueiry AB et al. Lancet. 2017;389:2492-2502.
N = 620
Nivolumab
Sorafenib
Nivolumab Child–Pugh B
Nivolumab + ipilimumab
Nivolumab ± ipilimumab + cabozantinib
R
R
So, taking first, the checkpoint inhibitor, nivolumab, I think the most important data on this agent came from CheckMate -040. Nivolumab is a PD-1 checkpoint inhibitor that blocks a negative inhibition of the immune checkpoint and immune microenvironment, and it allows for T-cell activation upon recognition of tumor-associated antigens.
Initially, nivolumab was studied as a monotherapy in this arm of this complex trial design with three carefully selected cohorts of noninfected patients, hepatitis B patients, and hepatitis C patients. The study’s intent was to really ascertain the toxicity according to viral status, given the concern for possible immune-related adverse events. So, that was a phase 1 dose escalation and led subsequently to a large dose expansion, which was the study that resulted in approval by the FDA of nivolumab in the second-line setting.
Since then, the promising results from this part of the study, which I’ll show you momentarily, have led to a set of different cohorts, including a randomized comparison of nivolumab versus sorafenib, nivolumab in patients with Child–Pugh B status, the combination of nivolumab plus ipilimumab, and then a three-drug combination, nivolumab, ipilimumab, and cabozantinib.
Uninfected, Sorafenib
Naïve (n = 56)
Uninfected, Sorafenib
Progressor (n = 57)
HCV (n = 50)
HBV (n = 51)
Total (N = 214)
ORb 13 (23%; 13-26) 12 (21%; 11-34) 10 (20%; 10-34) 7 (14%; 6-26) 42 (20%; 15-26)
CR 0 2 (4%) 0 1 (2%) 3 (1%) PR 13 (23%) 10 (18%) 10 (20%) 6 (12%) 39 (18%) SD 29 (52%) 23 (40%) 23 (46%) 21 (41%) 96 (45%) PD 13 (23%) 18 (32%) 14 (28%) 23 (45%) 68 (32%) NE 1 (2%) 4 (7%) 3 (6%) 0 8 (4%)
DORb KM median 8.4 (8.3-NE) NR 9.9 (4.5-9.9) NR 9.9 (8.3-NE) Ongoing, n/N (%) 8/13 (62%) 7/12 (58%) 8/10 (80%) 5/7 (71%) 28/42 (67%)
Disease controlb 42 (75%; 62-86) 35 (61%; 48-74) 42 (75%; 62-86) 42 (75%; 62-86) 42 (75%; 62-86) Disease control with SD for ≥6 mo 22 (39%; 27-53) 22 (39%; 26-52) 17 (34; 21-49) 18 (35%; 22-50) 79 (37%; 30-44)
Outcomes With Nivolumab in HCC1,a
a Unless otherwise indicated, data are n (%; 95% CI); n (%); months (95% CI); or % (95% CI). b Determined by investigator assessment using RECIST 1.1. 1. El-Khoueiry AB et al. Lancet. 2017;389:2492-2502.
ORR by RECIST 1.1 in the post-sorafenib population was 14.3% (n = 154)
So, looking at that first monotherapy expansion cohort of nivolumab according to the important categories of hepatitis C, hepatitis B, and the uninfected patients, or the nonviral, who were divided into sorafenib-naïve and sorafenib-progressors groups, this slide shows us several very important efficacy outcomes. One,
while we’re used to seeing relatively low response rates to tyrosine kinase inhibitors, with lenvatinib being a recent exception with a much higher response rate than we’ve seen historically, nivolumab achieved objective responses in 23% of the uninfected sorafenib-naïve group, 21% in the uninfected sorafenib-progressor group, 20% in the hepatitis C group, and 14% in the hepatitis B group, with an overall response in 20% of the total study population.
And impressively, the duration of responses has been quite long. Some of the cohorts have not yet reached progression but are ranging in the 8-plus month range; so, dramatically longer than we usually see for responses. And so, in addition, there are even cases here, you’ll note, with complete response, meaning no residual visible tumor on imaging, which was achieved with nivolumab.
Arm A: Nivolumab 1 mg/kg
+ Ipilimumab 3 mg/kg Every 3 Weeks
(n = 49)
Arm B: Nivolumab 3 mg/kg
+ Ipilimumab 1 mg/kg Every 3 Weeks
(n = 49)
Arm C: Nivolumab 3 mg/kg
Every 2 Weeks + Ipilimumab 1 mg/kg
Every 6 Weeks (n = 48)
ORR, n (%) 16 (32) 15 (31) 15 (31) Median DOR (range) 17.5 (4.6-30.5+) 22.2 (4.2-29.9+) 16.6 (4.1-32.0+) mOS (95% CI), mo 23 (9-NA) 12 (8-15) 13 (7-33)
CheckMate -040: Nivolumab + Ipilimumab1
1. Yau T et al. American Society of Clinical Oncology Annual Meeting 2019 (ASCO 2019). Abstract 4012.
AE Arm A Arm B Arm C
Any Grade Grade 3-4 Any Grade Grade 3-4 Any Grade Grade 3-4 Rash 17 (35) 3(6) 14 (29) 2 (4) 8 (17) 0 Hepatitis 10 (20) 10 (20) 6 (12) 5 (10) 3 (6) 3 (6) Adrenal insufficiency 9 (18) 2 (4) 3 (6) 0 3 (6) 0 Diarrhea/colitis 5 (10) 3 (6) 1 (2) 1 (2) 1 (2) 1 (2) Pneumonitis 5 (10) 3 (6) 0 0 0 0
The CheckMate -040 efficacy data on nivolumab as monotherapy has also prompted a combination of IO therapies, such as nivolumab plus another checkpoint inhibitor, ipilimumab, a CTLA-4 inhibitor.
To highlight—with adding another checkpoint inhibitor, the objective response rates are potentially even higher, up to 32%, with the duration of response now approaching the 17- to 22-month range in relatively large cohorts, with 49, almost 50, patients each. So, it’s quite an encouraging signal of efficacy.
Now, these are single-arm studies, and they require confirmation in randomized settings, and that’s what is ongoing as we speak. I’ll show you a couple of those ongoing studies in a moment.
Now, while the outcomes of nivolumab as monotherapy have not resulted in substantial rates of immune-related hepatitis, with rates of approximately 3% or 4%, the combination numbers are looking higher. We’re seeing up to 20% for the combination of nivolumab plus ipilimumab, and that raised, certainly, the requirement for very close monitoring, which will guide the decision about dosing in future trials.
PeerView.com/XKX900

17
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
CheckMate -459: Nivolumab vs Sorafenib in Advanced HCC (Phase 3)1
• Primary endpoint: OS • Secondary endpoints: ORR, PFS, and biomarkers
• Advanced HCC not eligible for or progressive after surgical and/or LRTs
• Child–Pugh A
• N = 726 Sorafenib
Nivolumab
R
1. https://clinicaltrials.gov/ct2/show/NCT02576509. Accessed September 12, 2019.
So, the nivolumab efficacy in the CheckMate -040 study as monotherapy prompted this pivotal, randomized, phase 3 trial, CheckMate -459 with nivolumab versus sorafenib, which was a first-line trial looking at patients with advanced HCC who are not eligible for locoregional or surgical therapies and are Child–Pugh A. The sample size was 726 patients. The primary endpoint was overall survival, and the secondary endpoints were objective response rate, PFS, and biomarker analyses. Patients were randomized to nivolumab versus sorafenib as first-line therapy, and the study’s been eagerly awaited now for almost 2 years.
• The trial did not achieve statistical significance for its primary endpoint of OS per the prespecified analysis (HR = 0.85 [95% CI, 0.72-1.02]; P = .0752)
CheckMate -459: Efficacy Results1
1. Yau T et al. ESMO 2019. Abstract LBA38_PR.
Nivolumab (n = 371) Sorafenib (n = 372) Median OS (95% CI), mo 16.4 (13.9-18.4) 14.7 (11.9-17.2) 12-mo OS rate (95% CI), % 59.7 (54.4-64.6) 55.1 (49.8-60.1) 24-mo OS rate (95% CI), % 36.8 (31.8-41.8) 33.1 (28.3-38.0) Median PFS (95% CI), mo 3.7 (3.1-3.9) 3.8 (3.7-4.5) ORR, n (%) 57 (15) 26 (7) BOR, n (%) CR 14 (4) 5 (1) PR 43 (12) 21 (6) ORR by baseline tumor PD-L1 expression, n/n (%) PD-L1 ≥1% 20/71 (28) 6/64 (9) PD-L1 <1% 36/295 (12) 20/300 (7)
And, unfortunately, just recently, we received the results at ESMO 2019. The study, despite the promise of nivolumab in a single-arm study, did not achieve statistical significance for its primary endpoint, although there was a trend toward benefit.
• Nonrandomized, multicenter, open-label, phase 2 trial assessing the PD-1 inhibitor pembrolizumab 200 mg every 3 weeks
• The study enrolled patients (N = 104) with HCC previously treated with sorafenib who were either intolerant to this treatment or showed radiographic progression after treatmenta
• The primary endpoint was objective response
KEYNOTE-224: Phase 2 Study of Pembrolizumab in Previously Treated HCC1
a ECOG PS of 0-1; adequate organ function, Child–Pugh class A. 1. Zhu AX et al. Lancet Oncol. 2018;19:940-952.
Another study was KEYNOTE-224, which was looking at pembrolizumab in patients with previously treated HCC. Pembrolizumab is also a PD-1 inhibitor.
KEYNOTE-224: Phase 2 Study of Pembrolizumab in Previously Treated HCC1
1. Zhu AX et al. Lancet Oncol. 2018;19:940-952.
Median DOR not reached Objective response: 17%
And I’ll show that, like nivolumab as a monotherapy, pembrolizumab achieved meaningful durable responses in about 17% of patients as monotherapy, but with an extremely long duration of response, and the median was not reached.
KEYNOTE-240: Phase 3 Pembrolizumab vs BSC as Second-Line Therapy1
1. Finn RS et al. ASCO 2019. Abstract 4004.
OS,
%
Pembrolizumab reduced the risk of death by 22% and improved PFS over placebo “These differences did not meet significance per the prespecified statistical plan”
N = 413
Pembrolizumab (n = 278)
R Placebo (n = 135)
Time, mo
100 90 80 70 60 50 40 30 20 10
0 0 4 8 12 16 20 24 28 32
Median (95% CI), mo 13.9 (11.6-16.0) 10.6 (8.3-13.5) Dual primary endpoints: OS and PFS
Prespecified P = .0174 required for statistical significance
Events HR (95% CI) P
Pembrolizumab 183 0.781 (0.611-0.998) .0238 Placebo 101
No. at Risk Pembrolizumab
Placebo 278 135
237 113
190 84
152 65
110 42
57 23
16 8
1 1
0 0
Pembrolizumab Placebo
The KEYNOTE-224 trial prompted a phase 3 trial looking at pembrolizumab versus placebo called KEYNOTE-240, which was presented by Dr. Finn and colleagues at ASCO 2019, with best supportive care as a comparator. And if one looks at this study in the abstract, we see a median overall survival of 13.9 months for pembrolizumab versus 10.6 months for placebo, and a P value of .238.

18 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
And so, it certainly looks like a potentially positive study as a new second-line treatment option, but unfortunately, because of a dual primary endpoint of OS and PFS, the prespecified P value for significance was .0174. Thus, this is a negative study despite these trends toward benefit.
DOR, median (range)b,c
• Pembrolizumab: 13.8 mo (1.5+ mo-23.6+ mo) • Placebo: not reached (2.8 mo-20.4+ mo)
a Nominal one-sided P based on the Miettinen and Nurminen method, stratified by randomization factors. b From product-limit (Kaplan–Meier) method for censored data. C + indicates no PD by the time of last disease assessment.
1. Finn RS et al. ASCO 2019. Abstract 4004.
KEYNOTE-240: Phase 3 Pembrolizumab vs BSC as Second-Line Therapy1 (Cont’d)
ORR at Final Analysis (RECIST 1.1, BICR)
Response, n (%) Pembrolizumab (n = 278)
Placebo (n = 135)
Best OR CR PR SD SD ≥23 wk
6 (2.2)
45 (16.2) 122 (43.9) 37 (18.3)
0 (0.0) 6 (4.4)
66 (48.9) 20 (14.8)
PD 90 (32.4) 57 (42.2)
DCR (CR + PR + SD) 173 (62.2) 72 (53.3)
OR
R, %
(95%
CI)
Pembrolizumab Placebo
13.8 (7.7-19.5) P = .00007a
18.3 (14.0-23.4)
4.4 (1.6-9.4)
30
20
10
0
Looking at the response rate outcomes, again, we see that 18% of patients in the pembrolizumab arm compared with 4.4% of patients in placebo arm had a response, which was a highly significant difference. But the alpha was spent because of the statistical design on the dual primary endpoint; thus, there was no plan for analysis for this objective response rate.
So, owing to the nuances of this very complex statistical design, the overall study was negative, and we were left with a very promising overall response rate, but no statistically significant association with survival endpoints to date.
So, this puts us in a very difficult predicament: How do we understand the data in the context of immunotherapy monotherapy? One of the potential explanations is that the sample sizes have been too small to identify a benefit in median overall survival or progression-free survival by area under the curve in an overall unselected study population. And thus, despite the improvements in prolonged responses in subsets of patients, the overall survival and PFS in these two unselected studies, CHECKMATE -459 and KEYNOTE-240, with pembrolizumab and nivolumab, respectively, have been negative.
• Patients with Child–Pugh B status (CheckMate -040 cohort, other retrospective series)1,2
– NCCN includes nivolumab as second-line therapy for Child–Pugh Class A or B73
• Selected ongoing combination strategies in pivotal trials4
– HIMALAYA: durvalumab plus tremelimumab – CheckMate -9DW: nivolumab plus ipilimumab5
– IMbrave150: atezolizumab plus bevacizumab – LEAP-002: lenvatinib plus pembrolizumab – COSMIC-312: cabozantinib plus atezolizumab – Camrelizumab plus apatinib
New Directions With Immunotherapy
1. Kudo M et al. ASCO GI 2019. Abstract 327. 2. Kambhampati S et al. Cancer. 2019;125:3234-3241. 3. NCCN Clinical Practice Guidelines in Oncology. Hepatobiliary Cancers. Version 2.2019. Accessed September 15, 2019. 4. https://clinicaltrials.gov. Accessed September 15, 2019. 5. Yau T et al. ASCO 2019. Abstract 4012.
But now, at present, we have multiple combination strategies in pivotal trials asking the question, like nivolumab plus a CTLA-4 inhibitor such as ipilimumab, can we improve upon this response rate and achieve improvements in survival endpoints, including OS and PFS, by combining immunotherapies with other agents to increase their potency or augment the number of patients likely to respond?
And so, listed here is the next wave of trials underway, including HIMALAYA, studying durvalumab and tremelimumab. It’s a phase 3 trial expected to report in the next year or so. CheckMate -9DW is another phase 3 trial moving from the data of nivolumab plus ipilimumab, which will compare that combination with sorafenib to determine first-line therapy superiority. Also completed and scheduled to report in the next year or so is the IMbrave150 trial of atezolizumab plus bevacizumab based on the biologic rationale that antiangiogenic agents may improve upon the efficacy of immunotherapy. And then, the last three trials are combinations of immunotherapy plus tyrosine kinase inhibitors, again, based on preclinical data and data in other tumor types, including renal cell carcinoma and uterine cancer now, that combining a TKI with immunotherapy may improve upon the immune microenvironment’s likelihood of response to immunotherapy.
So, it’s a very complex area right now with a lot of studies going on, so I apologize for covering a lot in a very short time, but I think there will be much more next year and the years ahead.
PeerView.com/XKX900

19
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
Conclusions
• Multiple new treatment options are available after progression on sorafenib for advanced HCC – Anti-angiogenic therapies with level 1 evidence
Regorafenib (after prior tolerance of sorafenib)
Cabozantinib Ramucirumab (AFP ≥400 ng/mL)
– Immune checkpoint inhibitors based on phase 2 data Nivolumab and pembrolizumab Randomized trials have been negative to date
• Studies of combination strategies are ongoing • The expanding treatment landscape will enable and require intensified efforts to identify
biomarkers of prognosis and response to guide choice and sequence of therapy
So, in conclusion, there are multiple new treatment options after progression occurs in patients on sorafenib for advanced HCC. There are antiangiogenic therapies with level 1 evidence, including regorafenib, as Amit presented earlier from the RESORCE trial in patients with prior tolerance of sorafenib; cabozantinib from the CELESTIAL trial in second- or third-line; and ramucirumab, which is restricted to patients with an AFP greater than or equal to 400 ng/mL.
Right now we have the option of using immune checkpoint inhibitors based on phase 2 data but without confirmation in phase 3 trials to date for any survival benefit, which includes nivolumab and pembrolizumab based on CheckMate -040, nivolumab also based on KEYNOTE-224, and KEYNOTE-240 for pembrolizumab. Though the randomized trials have been negative to date, there are many follow-up studies pending, including an enormous potential for combination strategies.
The expanding treatment landscape will enable and really require us to start to study, again, biomarkers of prognosis and response to guide our choice in sequence of therapy in the future. Thank you.
Dr. Abou-Alfa: Thank you very much. Thank you, Katie.
The Next Wave: Expanding the Therapeutic Arsenal in Earlier-Stage DiseaseProfessor Riccardo Lencioni, MD, FSIR, EBIR
Modified BCLC Staging System: 20181
1. Galle PR et al. J Hepatol. 2018;69:182-236.
HCC in cirrhotic liver
Solitary 2-3 nodules ≤3 cm
Transplant candidate
Resection
No Yes No
Transplant Ablation Chemoembolization Systemic therapy
>5 y 3 mo >2.5 y
Ablation BSC
Optimal surgical candidate
≥10 mo
Yes
Very early stage (0) Single <2 cm
Preserved liver function PS 0
Early stage (A) Single or 2-3
nodules <3 cm Preserved liver function
PS 0
Intermediate stage (B) Multinodular, unresectable
Preserved liver function PS 0
Advanced stage (C) Portal invasion/
extrahepatic spread, Preserved liver function
PS 1-2
Terminal stage (D) Not transplantable
End-stage liver function
PS 3-4
Dr. Abou-Alfa: Without any further ado, we’ll move on to the next lecture from Professor Lencioni from Pisa, Italy, and also an honorary research interventional radiology professor at the University of Miami. He’s going to talk to us about, “The Next Wave: Expanding the Therapeutic Arsenal in Earlier-Stage Disease.” Riccardo, please.
Dr. Lencioni: Thank you, Ghassan. You heard a lot about what is available and the research that is ongoing for patients with advanced-stage disease. However, there is clearly another top priority in the management of hepatocellular carcinoma, and this is to improve the ability to offer a cure to these patients. Clearly, this has to do with the improvement of surveillance programs, but it has also to do with the therapeutic armamentarium that we can offer to patients with early-stage disease and recognizing that these patients deserve—and it is the target of therapy—a median survival in excess of 5 years.
Radiofrequency Ablation of Early-Stage HCC: Long-Term Survival1
a Only 4 of 98 patients had Child–Pugh C cirrhosis. b Based on BCLC criteria for resection: single tumor, normal bilirubin level (<1.5 mg/dL), and absence of significant portal hypertension.
1. Breen DJ, Lencioni R. Nat Rev Clin Oncol. 2015;12:175-186.
Study n OS Rate, %
1 y 3 y 5 y
Lencioni et al. 2005
Child–Pugh A: 144 Child–Pugh B: 43
Child–Pugh A: 100 Child–Pugh B: 89
Child–Pugh A: 76 Child–Pugh B: 46
Child–Pugh A: 51 Child–Pugh B: 31
Tateishi et al. 2005
Child–Pugh A: 221 Child–Pugh B-C:a 98
Child–Pugh A: 96 Child–Pugh B-C: 90
Child–Pugh A: 83 Child–Pugh B-C: 65
Child–Pugh A: 63 Child–Pugh B-C: 31
Choi et al. 2007
Child–Pugh A: 359 Child–Pugh B: 160
Child–Pugh A: NR Child–Pugh B: NR
Child–Pugh A: 78 Child–Pugh B: 49
Child–Pugh A: 64 Child–Pugh B: 38
N’Kontchou et al. 2009
Resectable:b 67 Unresectable:b 168
Resectable: NR Unresectable: NR
Resectable: 82 Unresectable: 49
Resectable: 76 Unresectable: 27
Mean HCC size: 2.8 cm
Mean HCC size: 2.6 cm
Mean HCC size: 2.2 cm
Mean HCC size: 2.9 cm
At this point in time, the only approach that we can offer to nonsurgical patients with early-stage HCC is ablation. Historical data, particularly for radiofrequency ablation, have shown that in

20 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
PeerView.com/XKX900
05
101520253035404550
0 10 20 30 40 50 60
Image-Guided Ablation of Early-Stage HCC: Imaging vs Pathology1
1. Sasaki A et al. Cancer. 2005;103:299-306.
Nearly 50% of patients with
a solitary HCC <5 cm on imaging have microsatellites on histology1
3 cm 5 cm Tumor
Size of Main Tumor, mm
x x x x x x x x x x x x
N = 100 y = -3.44 + 0.24 x r2 = .084 P < .001
Dist
ance
of M
icro
sate
llite
, mm
40
30
20
10
0
Now, why is that? Clearly, one important reason is the decorrelation between what we see on imaging and what pathology shows. This looks like the perfect target for ablation, right? It’s a single tumor. It looks perfectly marginated, so it’s a kind of tumor that we will definitely feel confident in being able to eradicate with ablation technologies.
However, based on pathology, we know that at least 50% of these patients, even when the main tumor is smaller than 5 cm, do have microsatellites. Most of these microsatellites, clearly, are undetectable on imaging. So, is that the reason for most of the recurrences?
Another important concept is the distance between the microsatellite and the main tumor. And you can see here that, clearly, for tumors above 2.5 or 3 cm, the distance between the main mass and the microsatellites increases, so when we are trying to ablate in excess, trying to encompass the target tumor into a larger ablation volume, it’s very likely that some of these satellites will not be included in the ablation volume.
Tumor Board 4: 60-Year-Old Male With HCV-Related Cirrhosis
1. Fang KC et al. Liver Cancer. 2018;7:335-358.
Child–Pugh A5, ECOG 0, AFP 130 ng/mL Solitary HCC 6 cm, no MVI/EHS, BCLC A Unsuitable for surgery due to comorbidities
Baseline CT Scan
Therapeutic management • Ablation • TACE • Y90 • SBRT • Systemic tx
Single Large HCC: Curative vs Noncurative Treatment1
0
0.2
0.4
0.6
0.8
1
0 12 24 36 48 60 72 84 96Follow-Up, mo
Curative treatment (n = 251)
Noncurative treatment (n = 215) P < .001
OS,
Pro
port
ion
1.0
Now, let’s see an example that fits perfectly with this scenario. This is a patient with extremely well compensated cirrhosis, Child–Pugh A5 status, excellent general conditions, ECOG 0, and an alpha-fetoprotein of 130 ng/mL.
And as you can see, he has a solitary 6-cm HCC without evidence of vascular invasion or extrahepatic spread. This patient would be classified according to the Barcelona Clinic Liver Cancer staging
properly selected candidates, long-term survival can definitely match and be very competitive with the best reported results for surgery and exceed a 5-year survival rate as a median in this patient population. However, this is only applicable to patients with small tumors, and, as you can see, the average size, typically, as you are familiar with in your clinical practice, is below 3 cm.
Novel Technologies for Image-Guided Liver Tumor Ablation1
1. Lencioni R et al. Liver Cancer. 2015;4:208-214.
Technology Potential Advantages Potential Disadvantages
RFA
• High rates of local control in tumors ≤3 cm
• Established safety profile • Known limitations • Experience in combination
treatments (HCC) • Widely available
• High rates of incomplete ablation in tumors >3 cm
• Heat sink effect in perivascular tumors
• Potential risk of thermal injury to critical structures
• Variability in RFA devices
MWA
• Potential to treat tumors >3 cm more effectively
• Less impacted by heat sink effect • Ability to activate multiple probes
at the same time • No grounding pads required
• Limited efficacy data (predictability and reproducibility)
• Limited safety data • Potential risk of thermal injury
to critical structures (and vessels?) • Variability in MWA devices
Cryoablation • Ability to activate multiple probes
at the same time • Ability to image the ice-ball formation
• Insufficient clinical data • Risk of bleeding • Risk of cryoshock
IRE • Potential to treat tumors located in
the vicinity of critical structures • Heat sink effect not relevant
• Insufficient clinical data • Neuromuscular blockage
and cardiac gating required
Main Potential Advantages and Disadvantages of Energy-Based Ablative Technologies Image-Guided Ablation of Malignant Liver Tumors: Recommendations for Clinical
Validation of Novel Thermal and Nonthermal Technologies—A Western Perspective
Riccardo Lencioni, Thierry de Baere, Robert C. Martin, Charles W. Nutting,
Govindarajan Narayanan
Because of this limitation, there was a lot of focus in interventional radiology on developing novel technologies that could overcome this limitation and particularly ensure more consistent, predictable, and reproducible ablations of larger tumors. And particularly, microwave ablation looks like a very attractive option. I think in the United States, many centers have adopted this technology with success in a variety of cancers.
No. at Risk (Censored)
0
20
40
60
80
100
0 0.5 1 1.5 2 2.5 3
OS,
%
Time, y
Log-rank P = .8012
RFA MWA
0
20
40
60
80
100
0 0.5 1 1.5 2
Log-rank P = .1854
RFA MWA
Loca
l Tum
or P
FS, %
Time, y
Early-Stage HCC: RFA vs MWA A Randomized Phase 2 Clinical Trial1
1. Vietti Violi N et al. Lancet Gastroenterol Hepatol. 2018;3:317-325.
Baseline Patient Characteristicsa Treatment Complications
MWA (n = 71)
RFA (n = 73)
No. lesions treated per patient, n (%)
1 2 3
44 (62) 18 (25) 6 (8)
46 (63) 20 (27)
6 (8)
Stage at inclusion, n (%)
BCLC stage 0 A Child–Pugh score A B
8 (11)
63 (89)
57 (80) 14 (20)
11 (15) 62 (85)
53 (73) 20 (27)
Blood liver function values at inclusion, median (IQR) Bilirubin, μmol/L Albumin, g/L
14 (10-20 39 (36-43)
16 (10-23) 38 (34-42)
AFP, ng/mL
<10, n ≥10, n Unknown, n
22 41 8
25 36 12
MWA (n = 98)
RFA (n = 104)
Grade 1, n (%) Subcapsular hepatic hematoma Peritoneal fluid effusion Minor hepatic blood test perturbation
3 (3) 2
1 0
9 (9) 7
1 1
Grade 2, n (%) Pain requiring medication Infection of the puncture site
2 (2) 1 1
3 (3) 3 0
Grade 3, n (%) Pneumothorax requiring drainage Umbilical vein lesion requiring surveillance Intrahepatic segmental necrosis
0 0
0
0
3 (3) 1
1
1
Grade 4, n (%) Arterial bleeding requiring embolization
2 (2) 2
0 (0) 0
Grade 5, n (%) 0 0
RFA 104 (0) 94 (9) 89 (12) 69 (27) 44 (48) MWA 98 (0) 95 (3) 77 (15) 67 (26) 52 (41)
RFA 73 (0) 66 (4) 63 (4) 52 (14) 34 (27) 17 (43) 13 (46) MWA 71 (0) 68 (3) 57 (8) 49 (15) 36 (25) 17 (42) 12 (47)
No. at Risk (Censored)
But, unfortunately for HCC, the data are not really supportive of this approach. When compared with radiofrequency ablation in the setting of patients with BCLC stage A with single tumors above the 2-cm threshold, you can see that in reality, when looking at local tumor control or overall survival, microwave ablation failed to show any edge over radiofrequency ablation.

21
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
as stage A. Any patient with a single tumor of any size is Barcelona Clinic Liver Cancer stage A. But, unfortunately, this patient was unsuitable for surgery because of a number of comorbidities.
And clearly, the management of these patients, as well as the discussion, is open to how to approach a patient like this and recognizing that there is a huge difference in survival in this particular patient subset depending on whether we can offer curative versus noncurative treatment. This was a recent paper in Liver Cancer clearly showing a highly significant difference in overall survival.
Tumor Board 4: 60-Year-Old Male With HCV-Related Cirrhosis
Child–Pugh A5, ECOG 0, AFP 130 ng/mL Solitary HCC 6 cm, no MVI/EHS, BCLC A Unsuitable for surgery due to comorbidities
Baseline CT Scan
Therapeutic management • Ablation • TACE • Y90 • SBRT • Systemic tx
4-Month CT Scan
1-Month CT Scan
So, this patient was treated with a combination of ablation and TACE in the effort to offer the best possible interventional management, and, as you can see, the 1-month CT looks fine and is consistent with a complete response.
Tumor Board 4: What Are His Options?
Child–Pugh A5, ECOG 0, AFP 130 ng/mL Solitary HCC 6 cm, no MVI/EHS, BCLC A Unsuitable for surgery due to comorbidities
Baseline CT Scan
Therapeutic management • Ablation • TACE • Y90 • SBRT • Systemic tx
4-Month CT Scan
1-Month CT Scan
But 4 months later, you can see multiple instances of nodular regrowth at the periphery. This is in the arterial phase, and this is in the venous phase. You can see, unequivocally, new nodules with announcement and washout, so clearly, this is a treatment failure and a failure to offer this patient a radical cure.
50 °C Tissue coagulation
Sublethal heating 40 °C
1. Lencioni R, Cioni D. Hepatic Oncol. 2016;3:193-200. 2. Ahmed M et al. Radiology. 2005;235:469-77.
RF alone RF + Doxorubicin
The Next Wave: Ablation Plus IV Thermosensitive Drug Carriers1,2
40 °C
This is the area where we are expecting major progress from thermally sensitive drug carriers, such as lyso-thermosensitive liposomal doxorubicin. This is a carrier that is injected intravenously, and then it releases a highly concentrated amount of doxorubicin into the tumoral area using the heat produced by concurrent radiofrequency ablation.
On top of that, around the volume of coagulation achieved by radiofrequency ablation, there is a wide area of sublethal heating. Several studies have consistently shown damage to the tumor and parenchymal cells in the area of sublethal heating, so when the highly concentrated amount of doxorubicin is delivered in this area, the cells are already damaged.
15 min 45 min
1. Lencioni R, Cioni D. Hepatic Oncol. 2016;3:193-200. 2. Swenson CE et al. PLoS One. 2015;10:e0139752.
The Next Wave: Ablation Plus IV Thermosensitive Drug Carriers1,2 (Cont’d)
40 °C
020406080
100120140160180
5 15 30 60
Dox in center Dox in margin
Tota
l Tis
sue
Dox
, mcg
Ablation Time, min
You can see evidence of how this increases the treatment zone in experimental studies, and how the amount of additional ablation achieved by the administration of thermosensitive drug carriers is dependent on the burn time. It takes, ideally, 45 minutes or more for the circulating carrier to release, in situ, a clinically meaningful amount of drug.

22 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
PeerView.com/XKX900
1. Tak WY et al. Clin Cancer Res. 2018;24:73-83.
PFS ITT Population (n = 701)
RFA Plus LTLD vs RFA Alone: A Randomized Phase 3 Trial1
00.10.20.30.40.50.60.70.80.9
1
0 6 12 18 24 30 36 42 48 54Time Since Randomization, mo
LTLD + RFA 354 303 244 200 160 102 59 18 2 RFA 347 292 250 195 153 106 47 10 0
LTLD + RFA RFA Alone Events/n 187/354 187/347 Median, mo 13.9 13.9 HR (95% CI) 0.96 (0.79-1.18) P (stratified log-rank) .71
LTLD + RFA 354 207 133 95 61 40 18 7 2 1 RFA 347 218 130 85 53 30 13 4 1 0
No. at Risk
No. at Risk
Prob
abili
ty o
f PFS
LTLD + RFA RFA alone
Phase 3 HEAT Study Adding Lyso-Thermosensitive Liposomal Doxorubicin to Radiofrequency Ablation in Patients With Unresectable Hepatocellular Carcinoma Lesions Won Young Tak, Shi-Ming Lin, Yijun Wang, Jiasheng Zheng, Aldo Vecchione, Soo Young Park, Min Hua Chen, Stephen Wong, Ruocai Xu, Cheng-Yuan Peng, Yi-You Chiou, Guan-Tarn Huang, Jianqiang Cai, Basri Johan Jeet Abdullah, June Sung Lee, Jae Young Lee, Jong-Young Choi, Julieta Gopez-Cervantes, Morris Sherman, Richard S. Finn, Masao Omata, Michael O’Neal, Lukas Makris, Nicholas Borys, Ronnie Poon, and Riccardo Lencioni
1.0
OS ITT Population (n = 701)
LTLD + RFA RFA Alone Events/n 189/354 188/347 Median, mo 53.7 53.4 HR (95% CI) 0.98 (0.80-1.20) P (Cox PH regression) .82
Prob
abili
ty o
f OS
LTLD + RFA RFA alone
00.10.20.30.40.50.60.70.80.9
1
0 12 24 36 48 60 72 84 96Time Since Randomization, mo
1.0
This has been shown clinically. This is an article, which was published last year [2018] in Clinical Cancer Research on the HEAT study. This was a large, 700-patient, randomized, controlled trial of radiofrequency plus LTLD, or lyso-thermosensitive liposomal doxorubicin, versus RFA alone. As you can see, the trial did not show differences in OS or PFS.
1. Tak WY et al. Clin Cancer Res. 2018;24:73-83.
RFA Plus LTLD vs RFA Alone: A Randomized Phase 3 Trial1 (Cont’d)
PFS ITT Population (n = 701)
00.10.20.30.40.50.60.70.80.9
1
0 6 12 18 24 30 36 42 48 54Time Since Randomization, mo
LTLD + RFA RFA Alone Events/n 189/354 188/347 Median, mo 53.7 53.4 HR (95% CI) 0.98 (0.80-1.20) P (Cox PH regression) .82
LTLD + RFA 354 303 244 200 160 102 59 18 2 RFA 347 292 250 195 153 106 47 10 0
LTLD + RFA RFA Alone Events/n 187/354 187/347 Median, mo 13.9 13.9 HR (95% CI) 0.96 (0.79-1.18) P (stratified log-rank) .71
LTLD + RFA 354 207 133 95 61 40 18 7 2 1 RFA 347 218 130 85 53 30 13 4 1 0
No. at Risk
No. at Risk
Prob
abili
ty o
f OS
Prob
abili
ty o
f PFS
LTLD + RFA RFA alone
LTLD + RFA RFA alone
Patients With Single HCC (3-7 cm) and Ablation Time ≥45 min: OS (n = 285)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 12 24 36 48 60 72 84 96
Prob
abili
ty o
f OS
Time Since Randomization, mo
LTLD + RFA RFA Alone Events/n 54/138 73/147 Median, mo NR 60.2 HR (95% CI) 0.65 (0.45-0.94) P (Cox PH regression) < .05
LTLD + RFA 138 124 108 96 84 55 33 13 2 RFA 147 127 113 90 76 48 19 3 0
No. at Risk
LTLD + RFA RFA alone
1.0
00.10.20.30.40.50.60.70.80.9
1
0 12 24 36 48 60 72 84 96Time Since Randomization, mo
OS ITT Population (n = 701)
1.0
1.0
However, a subgroup analysis performed in patients with single HCC ranging 3 to 7 cm and an ablation time in excess of 45 minutes did show a meaningful improvement in survival for the combination of lyso-thermosensitive liposomal doxorubicin and radiofrequency ablation.
Of course, this is something that was found in a post hoc analysis because the trial was designed years ago. You can see the median survival, particularly for the control group, the RFA alone, is in excess of 60 months, so an excellent outcome for the control arm.
At that time, ablation time was not standardized, so patients were treated with radiofrequency ablation according to the best local practice. But the subgroup where treatment was 45 minutes or less had an OS benefit, as you can see. There was a hazard ratio of 0.65, which is not only significant in this patient population, but also means, in terms of median survival that was not even reached in the combination group, an improvement of around 2 years. So, the magnitude of improvement in survival is clearly something very big in this case.
Radiofrequency Ablation Duration per Tumor Volume May Correlate With Overall Survival in Solitary
Hepatocellular Carcinoma Patients Treated With RF Ablation Plus Lyso-Thermosensitive
Liposomal Doxorubicin
1. Celik H et al. J Vasc Interv Radiol. 2019. pii: S1051-0443(19)30416-6.
RFA Plus LTLD: Burn Time per Tumor Volume is Key1
Covariates Output P HR CI
TG TG .445 0.895 0.674-1.189
TG + BPV TG BPV
.416
.149 0.888 0.942
0.669-1.181 0.868-1.022
TG x BPV TG
BPV TG x BPV
.290
.591
.038
1.249 0.987 0.85
0.827-1.887 0.939-1.036 0.728-0.991
TG + BPD TG BPD
.468
.328 0.900 0.891
0.678-1.196 0.707-1.122
TG x BPD TG
BPD TG x BPD
.339
.678
.147
1.352 1.072 0.711
0.728-2.513 0.771-1.492 0.448-1.127
BPD: burn time per longest diameter BPV: burn time per tumor volume
TG: treatment group
Cox Survival Analysis of the Covariates
Haydar Celik, PhD, Paul Wakim, PhD, William F. Pritchard, MD, PhD, Meryll Castro, BS, Shelby Leonard, BS, John W. Karanian, PhD, Mark W. Dewhirst, PhD, Riccardo Lencioni,
MD, PhD, and Bradford J. Wood, MD
Bur
n Ti
me,
min
Bur
n Ti
me,
min
Tumor Volume, mL Largest Tumor Diameter, mm
RFA only LTLD + RFA
RFA only LTLD + RFA
And this was confirmed by a subsequent investigation. This was done in collaboration with the National Institutes of Health (NIH), showing that burn time per tumor volume is key.
1. Celik H et al. J Vasc Interv Radiol. 2019. pii: S1051-0443(19)30416-6.
RFA Plus LTLD: Burn Time per Tumor Volume is Key1 (Cont’d)
Radiofrequency Ablation Duration per Tumor Volume May Correlate With Overall Survival in Solitary
Hepatocellular Carcinoma Patients Treated With RF Ablation Plus Lyso-Thermosensitive
Liposomal Doxorubicin Haydar Celik, PhD, Paul Wakim, PhD, William F. Pritchard, MD, PhD, Meryll Castro, BS, Shelby Leonard, BS, John W. Karanian, PhD, Mark W. Dewhirst, PhD, Riccardo Lencioni,
MD, PhD, and Bradford J. Wood, MD
Bur
n Ti
me,
min
Bur
n Ti
me,
min
Tumor Volume, mL Largest Tumor Diameter, mm
RFA only LTLD + RFA
RFA only LTLD + RFA
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
1
0 1 2 3 4 5
Haz
ard
Rat
io
Lower Threshold of BPV, min/mL
And, essentially, the hazard ratio for the combination—in other words, the higher the burn time, the higher the effect.
LTLD + RFA vs RFA Only HR = 0.70
LTLD + RFA vs RFA Only HR = 0.50
Burn Time per Volume >2 min/mL Burn Time per Volume >3.4 min/mL
1. Celik H et al. J Vasc Interv Radiol. 2019. pii: S1051-0443(19)30416-6.
RFA Plus LTLD: Burn Time per Tumor Volume is Key1
0.9
0.8
0.7
0.6
0.5
0.4
1
0 20 40 60 80
Prob
abili
ty o
f Sur
viva
l
Lifetime, mo
0.9
0.8
0.7
0.6
0.5
0.4
1
0 20 40 60 80
Prob
abili
ty o
f Sur
viva
l
Lifetime, mo
LTLD + RFA RFA alone
LTLD + RFA RFA alone
You can see the comparison of survival between the combination versus RFA alone at different burn time intervals.

23
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
RFA Plus LTLD vs RFA Alone: The OPTIMA Phase 3 Trial1
• Primary endpoint: OS • Secondary endpoints: PFS, safety, others
• Single HCC 3-7 cm • Child–Pugh A • ECOG PS 0 • Candidate for RFA • No PVT/EHS • No prior treatment
N = 550 RFA (≥45 min)
+ dummy infusion
RFA (≥45 min) + LTLD (50 mg/m2)
R
1. https://clinicaltrials.gov/ct2/show/NCT02112656. Accessed September 15, 2019.
This was the basis to design a new phase 3 trial. I mean, of course, the post hoc analysis is only hypothesis generating. The new trial, OPTIMA, is a phase 3 trial. The recruitment has been completed, with 550 patients randomized, again, to an RFA standardized at 45 minutes or more combined with LTLD versus RFA combined with a dummy infusion.
The primary endpoint is overall survival, and we’re really looking forward to the results of this study, which potentially can change the standard of care for early-stage disease and offer a clinically meaningful improvement to many more patients with early-stage disease and tumors above the 2- to 3-cm threshold.
Modified BCLC Staging System: 20181
1. Galle PR et al. J Hepatol. 2018;69:182-236.
HCC in cirrhotic liver
Solitary 2-3 nodules ≤3 cm
Transplant candidate
Resection
No Yes No
Transplant Ablation Chemoembolization Systemic therapy
>5 y 3 mo >2.5 y
Ablation BSC
Optimal surgical candidate
≥10 mo
Yes
Very early stage (0) Single <2 cm
Preserved liver function PS 0
Early stage (A) Single or 2-3
nodules <3 cm Preserved liver function
PS 0
Intermediate stage (B) Multinodular, unresectable
Preserved liver function PS 0
Advanced stage (C) Portal invasion/
extrahepatic spread, Preserved liver function
PS 1-2
Terminal stage (D) Not transplantable
End-stage liver function
PS 3-4
Let’s talk for a few minutes about the intermediate stage. This is the area where patients are treated with chemoembolization, as you know.
Nonselective treatment of the
whole liver parenchyma
Selective treatment (segmental
approaches with microcatheters)
Conventional 2D angiography guidance and
monitoring
3D navigation C-arm rotational
angiography (cone-beam CT)
1. Images provided courtesy of Dr. Lencioni.
TACE: Evolving Techniques, Approaches, and Imaging Guidance1
TACE is another technology that has improved significantly in terms of catheters, imaging guidance, and the ability to precisely catheterize, as well as see and reach the target.
Lipiodol Transarterial Chemoembolization for Hepatocellular Carcinoma: A Systematic Review of Efficacy and Safety Data
Mortality:
214/34,137
0.6%
Cause of death
Hepatic failure Hepatic encephalopathy Infectious complications Gastrointestinal bleeding Tumor rupture Liver abscess Pulmonary embolization Other/not specified Any cause
No.
59 9
20 17
8 4 4
93 214
Safety Analysis (n = 34,137) Efficacy Analysis (n = 10,108)
1. Lencioni R et al. Hepatology. 2016;64:106-116.
TACE: A Systematic Review of Efficacy and Safety Data1
OS No. of Studies Estimate Lower
95% CI Upper 95% CI
Median, mo ≤2002 >2002
19 44
18.5 19.8
14.6 15.5
22.4 24.1
1-year, % ≤2002 >2002
19 71
70.7 70.4
63.2 65.2
78.3 75.5
2-year, % ≤2002 >2002
21 50
51.1 52.0
37.1 43.9
65.1 60.2
3-year, % ≤2002 >2002
13 53
27.8 43.4
18.3 34.9
37.4 51.8
Analysis of OS After Lipiodol TACE for HCC by Year of Publication
0
20
40
60
80
100
6 mo 1 y 2 y 3 y 5 y
81%
70%
52%
40%
32%
Time O
S, %
However, in terms of overall survival and outcomes, despite the improvement in safety and the trend for higher and longer survival rates, a recent publication compared [TACE] with historic data. It found that these approaches really failed to bring TACE therapy to a brand-new level.
05
101520253035
DEB-TACE TACE
Objective Response
Drug-Related AEs
1. Lammer J et al. Cardiovasc Intervent Radiol. 2010;33:41-52.
DEB-TACE vs Conventional TACE: A Randomized Phase 2 Trial1
Prospective Randomized Study of Doxorubicin-Eluting Bead Embolization in the Treatment of Hepatocellular Carcinoma: Results of the PRECISION V Study
Johannes Lammer, Katarina Malagari, Thomas Vogl, Frank Pilleul, Alban Denys, Anthony Watkinson, Michael Pitton, Geraldine Sergent, Thomas Pfammatter, Sylvain Terraz, Yves Benhamou, Tves Avajon, Thomas Gruenberger, Maria Pomoni, Herbert Langenberger, Marcus Schuchmann, Jerome Dumortier, Christian Mueller, Patrick Chevallier, Riccardo Lencioni
0
10
20
30
40
50
60
70
DEB-TACE TACE
63%
52%
27%
52% 44%
22%
CR OR DCR CR OR DCR
Even
ts/1
00 P
atie
nts
Patie
nts,
%
An example of this is the use of drug-eluting beads. This is an approach that was supposed to revolutionize chemoembolization. Phase 2 data suggested that there was a trend for improved response, which was interesting.

24 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
PeerView.com/XKX900
1. Brown K et al. J Clin Oncol. 2016;34:2046-2053.
DEB-TACE vs Bland Embolization: A Randomized Phase 2 Trial1
0
0.2
0.4
0.6
0.8
1
0 10 20 30 40 50 60 70
PFS,
Pro
port
ion
0
0.2
0.4
0.6
0.8
1
0 10 20 30 40 50 60 70
OS,
Pro
port
ion
P = .64
DEB-TACE Bead block
P = .11
DEB-TACE Bead block
Celiac, SMA, hepatic angiogram
Select target vessel
Embolize with 100-300 µm Bead block ≤10 cc
Stasis?
Embolize with 300-500 µm Bead block ≤10 cc
Postembolization angiogram
Procedure complete
Additional target vessels? Stasis?
Stasis?
Stasis?
Embolize with 500-700 µm Bead block ≤10 cc
Embolize with 700-900 µm Bead block ≤10 cc
Complete embolization with 100 µm PVA
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
Embolization Procedure: Bead Block Embolization Procedure: DEB-TACE Celiac, SMA, hepatic angiogram
Identify target vessels
Divide DEB proportionally
Administer entire 100-300 µm DEB volume if possible
Stasis?
Additional target vessels?
Postembolization angiogram
Embolize target vessel with 100-300 µm DEB
Stasis?
Stasis?
Stasis?
Embolize with 100-300 µm Bead block to total ≤10 cc
Embolize with 300-500 µm Bead block ≤10 cc
Embolize with 500-700 µm Bead block ≤10 cc
Stasis?
Complete embolization with 100 µm PVA
Procedure complete
Yes
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
No
One target vessel More than one target vessel
Time Since Randomization, mo
Time Since Randomization, mo
OS
PFS
But unfortunately, when tested in randomized trials and looking at hard endpoints, such as OS—this was a study conducted at Memorial Sloan Kettering Cancer Center by Ghassan Abou-Alfa and the interventional radiology team—this study failed to show any meaningful difference between the use of drug-eluting beads versus bland embolization.
Moving TKIs to Earlier-Stage Disease: Rationale and Early Evidence1
Angiogenic switch • Proangiogenic >
antiangiogenic factors
• Exposure + shedding of tumor cells into circulation
• ↑ MMP during angiogenesis
• Central hypoxia • Vessel compression by edema • Starvation treatments (eg, TACE)
Leaky vessels • Abnormal flow • Interstitial hypertension • Peritumor edema • Ineffective delivery of O2
and nutrients
• ↑ Growth factors • ↑ Anti-apoptotic proteins • Resistance to chemo/radiotherapy • Impaired tumor immune response
– ↓ CD8+
– ↑ Treg/MDSC – ↑ PD-1/PD-L1
Angiogenesis
Hypoxia Tumor growth (and Metastasis)
1. Liu K et al. Clin Transl Gastroenterol. 2017;8:e98.
↑ HIF-1α, VEGF, IGF2
The problem with chemoembolization is really a kind of vicious cycle. In a way, hypoxia is needed because ischemia is what generates most of the antitumoral effect. However, hypoxia is also known to upregulate some mediators involved in angiogenesis, such as hypoxia-inducible factor 1-alpha and VEGF, so that, in a way, can stimulate and even facilitate tumor recurrence and progression.
TACE ± Sorafenib: SPACE Trial1
(Global Study, 307 Patients)
HR = 0.90 (0.61-1.33)
TACE ± Sorafenib: TACE 2 Trial2
(UK Study, 313 Patients)
HR = 0.91 (0.67-1.24)
TACE Plus Molecular Targeted Agents: Randomized Trials
1. Lencioni R et al. J Hepatol. 2016;64:1090-1098. 2. Meyer T et al. Lancet Gastroenterol Hepatol. 2017;2:565-575.
No. at Risk Time, d
Prob
abili
ty o
f Sur
viva
l
Sorafenib Median: NR 95%, 554-NR Placebo Median: NR 95% CI, 562-NR
1.00
0.75
0.50
0.25
0 0 100 200 300 400 500 600 700 800
No. at Risk Time, d
OS,
%
TACE + sorafenib TACE + placebo
100
75
50
25
0 0 250 500 750 1,000 1,250 1,500 1,750 2,000
And that was the rationale to combine [TACE with TKIs] to try
to prevent or mitigate this effect. As you know, this was done extensively with sorafenib in SPACE, which was a phase 2 trial that failed to show any meaningful effect, particularly on survival from the combination of the two.
TACE ± Brivanib: BRISK-TA Trial1
(Global Study, 502 Patients)
HR = 0.90 (0.66-1.23)
TACE ± Orantinib: ORIENTAL Trial2
(Japanese Study, 888 Patients)
HR = 1.09 (0.88-1.35)
1. Kudo M et al. Hepatology. 2014;60:697-707. 2. Kudo M et al. Lancet Gastroenterol Hepatol. 2018;3:37-46.
TACE Plus Molecular Targeted Agents: Randomized Trials (Cont’d)
0102030405060708090
100
0 6 12 18 24 30 36 420
0.2
0.4
0.6
0.8
1
0 3 6 9 12 15 18 21 24 27 30 33 36
Time, mo
Orantinib Placebo Events/n 168/444 163/444 Median, mo 31.1 32.3 P (stratified log-rank) .435
OS,
%
Time, mo
OS,
Pro
port
ion
Brivanib Placebo Events/n 79/249 85/253 Median, mo 26.4 26.1 P (stratified log-rank) .5280
And even the use of other drugs, such as brivanib, and recently, orantinib [combined with TACE], as you can see, did not really have a significant effect when compared with TACE alone. This probably was because of an issue in understanding how to manage patients undergoing a combination of local and systemic therapies. Particularly, the duration of the systemic treatment is a key factor, and some of the early studies were suboptimal in the way the drug was administered.
Lessons Learned With Locoregional Therapy Plus TKI Combinations
1. Kudo M et al. ASCO GI 2018. Abstract 206.
No. at Risk TACE + sorafenib 80 56 36 17 12 3 0 TACE alone 76 37 22 8 4 2 0
TACTICS Trial: Phase 21
• Significantly improved PFS with TACE + sorafenib vs TACE alone
• 25.2 vs 13.5 months, respectively; HR = 0.59 (95% CI, 0.41-0.87); P = .006
TACE + sorafenib TACE alone
0.0
0.5
1.0
0 12 24 36 48 60 72
PFS,
%
Time, mo
0
• Different populations, including earlier-stage HCC
• Timing of sorafenib • Dose of sorafenib • Duration of sorafenib • Early termination of study
based on other studies • Study design has
conservative stopping rules
This is a more recent presentation from Professor Kudo and colleagues on the TACTICS trial suggesting that there could be an improvement, particularly in PFS, from the combination of TACE and sorafenib. We are looking forward to seeing OS data from this study.

25
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
Immunotherapy
Ablation TACE Y90
SBRT
1. Duffy AG et al. J Hepatol. 2017;66:545-551.
The Next Wave: Locoregional Therapy Plus Immunotherapy1
Liver-Directed Locoregional Therapy + Immunotherapy
AFP
Afte
r B
efor
e
H&E CD3 CD8 IHC Staining in Response to Treatment
CD3 CD8
Pixe
l Cou
nt, %
8
0
CD3 CD8
Pixe
l Cou
nt, %
15
10
0
5
CD3 CD8 Responders Nonresponders
6
4
2
Before After
Baseline
6 mo
Time, mo Time, mo Time, d Su
m o
f Les
ions
R
el. t
o B
asel
ine
Clearly, the focus in this area with the new wave of immunotherapy is also trying to understand whether locoregional therapy is a good partner for checkpoint inhibitors. There is a lot of basic research suggesting that the increased antigen exposure associated with ablation using TACE or Y90 could be an important factor for a synergy between these approaches.
Study Arms Phase Patient Population NCT Identifier
Nivolumab + TACE (IMMUTACE) 2 Intermediate-stage HCC NCT03572582
Durvalumab + tremelimumab + DEB-TACE 2 Intermediate-stage HCC NCT03638141
Pembrolizumab + local ablation 2 Candidates for local ablation NCT03753659
Nivolumab after SIRT (Y90) 2 Candidates for locoregional therapy NCT03380130
Durvalumab + tremelimumab + radiation 2 Locally advanced/unresectable or metastatic HCC NCT03482102
Pembrolizumab + TACE 1,2 Intermediate-stage HCC NCT03397654
Durvalumab + tremelimumab with TACE, RFA, or cryoablation 1, 2 Locally advanced/advanced HCC NCT02821754
DEB-TACE + nivolumab 1 BCLC B NCT03143270
Pembrolizumab + Y90 1 Locally advanced, high-risk HCC NCT03099564
SBRT then nivolumab ± ipilimumab 1 Unresectable HCC NCT03203304
Ongoing Trials Combining Local and Immune-Based Therapy1
1. http://www.clinicaltrials.gov. Accessed May 13, 2019.
And, as you can see, there is clearly now a huge focus in research trying to combine different interventional locoregional approaches with different immune-based regimens.
Phase 3 Trial EMERALD-1: TACE Plus Immunotherapy1
Phase 3, Randomized, Double-Blind, Placebo-Controlled Study
• Primary endpoint: PFS for Arm A vs Arm C (BICR) • Secondary endpoints: PFS for Arm B vs Arm C (BICR), OS, and PROs • Other endpoints: safety and PK
• Confirmed HCC • Unsuitable for curative therapy,
e.g. surgical resection, ablation, transplantation
• Disease amenable to TACE • No extrahepatic disease • Child–Pugh A to B7 • ECOG 0 or 1 • Exclude Vp3 and Vp4
Arm C TACE + placebo
Arm A Durvalumab + TACE
R
1. https://clinicaltrials.gov/ct2/show/NCT03847428. Accessed September 15, 2019.
Arm B Durvalumab + TACE + bevacizumab
N = 600
One phase 3 trial, the EMERALD-1, has already started. It includes patients with intermediate-stage disease who are candidates for TACE. These patients would be randomized to receive TACE and placebo, TACE plus durvalumab, or TACE, durvalumab, and bevacizumab. The primary endpoint is progression-free survival.
Conclusions
• Image-guided ablation is the standard of care for very early/early-stage HCC in nonsurgical patients
– Alternative to resection for very early tumors 2 cm or less (location does matter!) – Research is currently focused on thermosensitive drug carriers to enable radical cure
for a greater number of patients with intermediate-size tumors
• TACE is the standard of care for intermediate-stage HCC and preserved liver function – Drug-eluting beads did not improve clinical benefit with respect to conventional TACE – Combination of TACE and TKIs failed to show meaningful synergistic effect, although
research is still ongoing after the lessons learned from previous trials
• Combination of locoregional and immune-based therapy is a very active area of research – Phase 3 trials combining TACE and checkpoint inhibitors ± VEGF inhibitors – Phase 3 trials in the adjuvant setting after resection/ablation
I think it’s time for me to come to the conclusions. And clearly, we have seen a lot of research in the advanced setting, but early- and intermediate-stage disease are also top priorities for research because these are the patients where survival rates can be pushed out and counted in years instead of months.
Image-guided ablation is the standard of care for small tumors. And we look forward to thermosensitive drug carriers to be able to ensure radical cures for a greater number of patients, particularly those with intermediate-size tumors.
TACE is the standard of care for intermediate-stage disease, but, unfortunately, research until now has not truly identified drug-eluding beads as the best partner for systemic therapy. This is why the focus is now on the combination of checkpoint inhibitors plus/minus VEGF inhibitors and TACE, as well as other combinations.
I didn’t have time to discuss the adjuvant setting of resection and ablation, but that is also a very active area for research. Thank you very much.
Dr. Abou-Alfa: Thank you very much. Thanks to Professor Lencioni. That was excellent.

Ghassan Abou-Alfa, MD, MBA
Robin K. (“Katie”) Kelley, MD
Professor Riccardo Lencioni, MD, FSIR, EBIR
Amit Singal, MD, MS
26 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
Audience Q&A: Question 1 What does noninferiority mean?
Dr. Abou-Alfa: We have plenty of questions. Amit, you brought up the data on lenvatinib, which understandably was positive. However, it was positive based on this noninferiority complex. I have literally three or four questions asking, “’What’s noninferiority?”
Dr. Singal: Yes. So, noninferiority is a statistical design where, instead of taking the 95% confidence interval, instead of basically not having to cross 1—so staying on one side of it—you actually adequately power this so you can show the two drugs have similar efficacy. And a priori, you define a confidence interval around that hazard ratio of 1.
For the REFLECT trial, it was allowed to go up to a hazard ratio, I think, of 1.12. And so, when you take a look at the confidence interval of the actual effect size, it falls squarely within that a priori designed new upper threshold, which allows you to establish similarity.
But, I think, compared with some of the other negative trials, which we’ve heard spun as saying, “Oh, it’s similar in terms of efficacy,” it really has to be decided ahead of time and adequately powered to prove that the two drugs actually have similar efficacy.
Dr. Abou-Alfa: That’s right. And again, to reiterate the fact that the two curves on the Kaplan–Meier are hugging each other, that’s a positive thing. That’s really what you want to see, rather than what you are used to seeing in a superiority study.
Dr. Singal: Yes, and I think that you can see that sometimes a study’s underpowered, but that clearly wasn’t the case here. And so, once again, I think the difference compared with an
underpowered study is that this is decided ahead of time, and you’re actually proving equivalence.
Audience Q&A: Question 2 In data from the retrospective analysis of sorafenib followed by
regorafenib showing improvement in survival, has there been any doubt, or could there be any, in regard to selectivity that made this happen?
Dr. Abou-Alfa: So, let’s switch to sorafenib. Another question is, “As you said, the retrospective analysis of sorafenib followed by regorafenib, altogether, shows an improvement in survival." The question is, "Has there been any doubt, or could there be any, in regard to selectivity that made this happen?” What are your thoughts on that?
Dr. Singal: Yes. So, this was a post hoc analysis, it wasn’t like there are patients who drop off between those two, so not everyone who is on sorafenib actually makes it to the second-line setting. We know that there is a substantial drop-off at that point.
And so, when you talk about a median survival of 26 months, this is really selecting for patients who tolerate sorafenib, are able to go on regorafenib, and continue to have good liver function and good performance status; unfortunately, that isn’t everyone. But it is important to note that, I think, if we appropriately manage patients—and there’s a nice recent study, which shows that expert management of sorafenib significantly improves outcomes with these. I think that in high-volume centers that actually are good at this, you can get a sizeable portion of your population on second-line therapies.
So, there is some selection, but, of course, those data don’t apply to everyone. For those people who can do it, I think those are useful data.
Audience Q&A
PeerView.com/XKX900

27
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
Audience Q&A: Question 3 Have you seen any reverse-stage migration with TKIs?
Dr. Abou-Alfa: Have you seen any reverse-stage migration with any TKIs, where people have metastatic disease and they move on to local disease or what have you?
Dr. Singal: Yes. So, I think that the name of the game for the last decade really was stable disease. And so, with sorafenib, we saw a lot of stability. I think we really weren’t used to talking about—I think you brought it up, moving to the left here in terms of the BCLC with systemic therapies—trying to downstage somebody from systemic to locoregional.
I think it is one of the nice things with lenvatinib, in terms of the higher response rates, and, of course, with some of the agents, such as checkpoint inhibitors. With these responses, you can see patients who start off in the BCLC C stage with systemic disease, and then they have responses. So you may actually be able to get them to the point where they can be treated with locoregional therapy. Have we seen it? Yes, but I don’t think it’s standard. I think it’s only in some patients.
Audience Q&A: Question 4 Can you discuss how you’re increasing
the frequency of follow-up imaging?
Dr. Eswaran: Sheila Eswaran, my specialty is hepatology here in Chicago at Rush University Medical Center. Thanks, Amit, for the great talk. Can you talk a little bit more about how you’re increasing the frequency of follow-up imaging?
Dr. Singal: Yes. So, I’d be interested to see what the rest of the panelists do, but we’ve done this because of this idea that we want to try to find progression if and when it happens. And so, we’ve tried to tighten our surveillance imaging interval.
We now do this routinely for everyone who’s on systemic therapy. We do it every 2 months. We use MRI as a standard imaging technique in our center. I don’t know if there are other details, but that’s our standard protocol on first line. And we do the same thing on second-line therapy if there’s any hope of getting people on third line or subsequent lines.
If somebody, for example, has Child–Pugh B disease, or they have poor performance status, I don’t think you necessarily watch those patients as closely, but, I mean, if you really think this patient’s eligible for second-line therapy, I think that’s where that tighter surveillance is helpful.
What do you guys do at your centers in terms of follow-up imaging at 2 or 3 months? What do you guys typically do?
Dr. Abou-Alfa: The standard has been 2 months for patients on therapy. And for follow-ups for ruling out recurrence, it’s 3 months. But again, there’s no science over here, so I can totally understand why perceptions might differ in that regard.
Audience Q&A: Question 5 Do you do next-generation sequencing?
If so, why? And if not, why?
Dr. Abou-Alfa: I would love for this one to have two answers, one from Dr. Singal as a hepatologist and one from Dr. Kelley as an oncologist—next-generation sequencing, do you do it? And if so, why? And if not, why?
Dr. Singal: Yes. So, we’ve just started to do this with select patients. I think it’s about 20% of patients with HCC who have actionable mutations. I think it’s something that we’re starting to do, but it’s early on in terms of our practice picking this up. I think that we’re probably going to see more and more of this in the future. If the insurance will cover it, we do it. If not, we don’t make the patient pay huge out-of-pocket costs to do it.
Dr. Abou-Alfa: Katie, how would you do it at University of California, San Francisco?
Dr. Kelley: We generally do not test HCC patients with next-generation sequencing, currently. I think the definitions of actionable are a little difficult in HCC. Since, while they may be actionable in some tumor types, we don’t have a lot of evidence

28 Go online to complete the post-test and evaluation for CME/MOC credit
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
of efficacy for these agents in HCC, even to the best of our ability when looking at molecular subgroups.
That said, obviously, the promise is enormous down the road, and we really do want to start moving toward molecular profiling to make progress and to really understand the biology, which is so heterogeneous. And so, I think, right now, the way I use molecular profiling outside of clinical trials is in patients in whom I potentially suspect mixed HCC/cholangiocarcinoma because we certainly know of actionable targets now in cholangiocarcinoma, from IDH1 to FGFR2. If there’s any doubt about whether there’s a cholangiocarcinoma component, I check, and for patients when I suspect that they may have it or I’m not confident in the primary or where it’s a very atypical presentation, particularly in a young patient or when there’s something atypical about the course.
Audience Q&A: Question 6 Do you think the new data, such as the negative findings from
CheckMate -459, will cause the FDA to revise the second-line indication for the use of nivolumab with pembrolizumab? Or do you think the FDA
will wait until the combination therapy data are available?
Dr. Abou-Alfa: One question for you, Katie. Do you think that with the advent of the new data, such as the negative findings from CHECKMATE -459 and the negative pembrolizumab findings, will cause the FDA to change anything in regard to the second-line indications for the use of nivolumab with pembrolizumab, or will they wait until the combination therapy comes on board?
Dr. Kelley: I don’t think they’ll change anything. I think the strength of the responses and the durability of responses are dramatically different than what we’ve seen in the past. So, my expectation is no they will not—and also considering the legacy of response in other tumor types.
Dr. Abou-Alfa: I totally agree. Well, thanks again.
Narrator: This activity has been jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
PeerView.com/XKX900

CME/MOC
Composing Personalized HCC Treatment Strategies: Insights on Harmonizing Patient Care With a Multidisciplinary Ensemble
Sign up for email alerts on new clinical advances and educational activities in your specialty: PeerView.com/signup
Copyright © 2000-2019, PeerView
This CME/MOC activity is jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
This activity is supported by medical educational grants from Bayer Healthcare Pharmaceuticals Inc., Celsion Corporation, and Exelixis, Inc.
Based on a panel discussion and on data from recent medical literature. The materials presented here are used with the permission of the authors and/or other sources. These materials do not necessarily reflect the views of PeerView or any of its partners, providers, and/or
PeerView.com/XKX900The Oncology Topics You Want
From the Experts You Trust