cme monograph case studies - mededicus
TRANSCRIPT

CME MONOGRAPH
This activity is jointly provided by Postgraduate Institute for Medicine and MedEdicus LLC.
This activity is supported by an independent educational grant from Merck & Co., Inc.
Distributed with
FACULTY PARTICIPANTS:
Gary D. Steinberg, MD (Chair)Chicago, Illinois
Cheryl Lee, MDAnn Arbor, Michigan
Michael Kraft, PharmD, BCNSPAnn Arbor, Michigan
Visit www.cmeuniversity.com and search for 11146
for online testing and instant CME certificate.
IN ENHANCED RECOVERY AND
IMPROVED PATIENT OUTCOMES:
PREVENTING POSTOPERATIVE ILEUS
FOLLOWING CYSTECTOMY
CASE STUDIES
ORIGINAL RELEASE: December 2, 2015 LAST REVIEW: November 11, 2015 EXPIRATION: December 2, 2016
2
FACULTY PARTICIPANTS:
Gary D. Steinberg, MD (Chair)The Bruce and Beth White Family Professor and Director of Urologic OncologyVice Chairman Section of UrologyUniversity of Chicago Medical CenterChicago, Illinois
Cheryl Lee, MDProfessor of UrologyUniversity of Michigan Medical SchoolAnn Arbor, Michigan
Michael Kraft, PharmD, BCNSPDepartment of Pharmacy ServicesUniversity of Michigan College of PharmacyAnn Arbor, Michigan
Estimated time to complete activity: 1.25 hours
Target AudienceThis activity is intended for urologists and other healthcare providers with an interest in urologic surgery.
Learning ObjectivesUpon completion of this activity, urologists will be better able to: 1. Evaluate the efficacy and safety of current strategies to reduce perioperative complications in procedures involving gastrointestinal (GI)/genitourinary (GU) tract surgeries2. Manage patients who are candidates for procedures involving GI/GU tract surgeries with evidence-based perioperative strategies to prevent postoperative ileus3. Articulate features of perioperative enhanced recovery after surgery protocols that might improve patient outcomes
System Requirements for Digital EditionsIf you are viewing this activity online please ensure the computer you plan to use meets the following requirements:• Operating System: Windows or Macintosh• Media Viewing Requirements: Flash Player or Adobe Reader• Supported Browsers: Microsoft Internet Explorer, Firefox, Google Chrome, Safari, and Opera• A good Internet connection
Accreditation StatementThis activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Postgraduate Institute for Medicine and MedEdicus LLC. The Postgraduate Institute for Medicine is accredited by the ACCME to provide continuing medical education for physicians.
Credit Designation The Postgraduate Institute for Medicine designates this enduring material for a maximum of 1.25 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Disclosure of Conflicts of InterestPostgraduate Institute for Medicine (PIM) requires instructors, planners, managers and other individuals who are in a position to control the content of this activity to disclose any real or apparent conflict of interest (COI) they may have as related to the content of this activity. All identified COI are thoroughly vetted and resolved according to PIM policy. PIM is committed to providing its learners with high quality CME activities and related materials that promote improvements or quality in healthcare and not a specific proprietary business interest of a commercial interest.
The faculty reported the following financial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME activity:
Michael Kraft, PharmD, BCNSP, has had a financial agreement or affiliation during the past year with the following commercial interests in the form of Consulting Fees (e.g., advisory boards): Fresenius Kabi; and B. Braun.Cheryl Lee, MD, has had a financial agreement or affiliation during the past year with the following commercial interest in the form of Contracted Research: Endo Pharmaceuticals Inc.Gary D. Steinberg, MD, has no real or apparent conflicts of interest to report.
The planners and managers reported the following financial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME activity:
The following PIM planners and managers, Trace Hutchison, PharmD, Samantha Mattiucci, PharmD, CHCP, Judi Smelker-Mitchek, RN, BSN and Jan Schultz, RN, MSN, CHCP, hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.
Medical Writer: Robert M. Geist IV, MD, has no real or apparent conflicts of interest to report.
MedEdicus Planners: Diane McArdle, PhD, and Cynthia Tornallyay, RD, MBA, CCMEP, have no real or apparent conflicts of interest to report.
Method of Participation and Request for CreditThere are no fees for participating in and receiving CME credit for this activity. During the period December 2, 2015, through December 2, 2016, participants must read the learning objectives and faculty disclosures and study the educational activity.
PIM supports Green CME by offering your Request for Credit online. If you wish to receive acknowledgment for completing this activity, please complete the post-test and evaluation on www.cmeuniversity.com. On the navigation menu, click on “Find Post-Test/Evaluation by Course” and search by course ID 11146. Upon registering and successfully completing the post-test with a score of 75% or better and the activity evaluation, your certificate will be made available immediately. Or you can mail or fax the completed post-test and evaluation to Postgraduate Institute for Medicine, 304 Inverness Way South, Suite 100, Englewood, CO 80112; Fax: (303) 858-8848.
MediaPrint and Internet
Disclosure of Unlabeled UseThis educational activity might contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. The planners of this activity do not recommend the use of any agent outside of the labeled indications.
The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
DisclaimerParticipants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patients’ conditions and possible contraindications and/or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.This CME activity is copyrighted to MedEdicus LLC ©2015.All rights reserved.
3
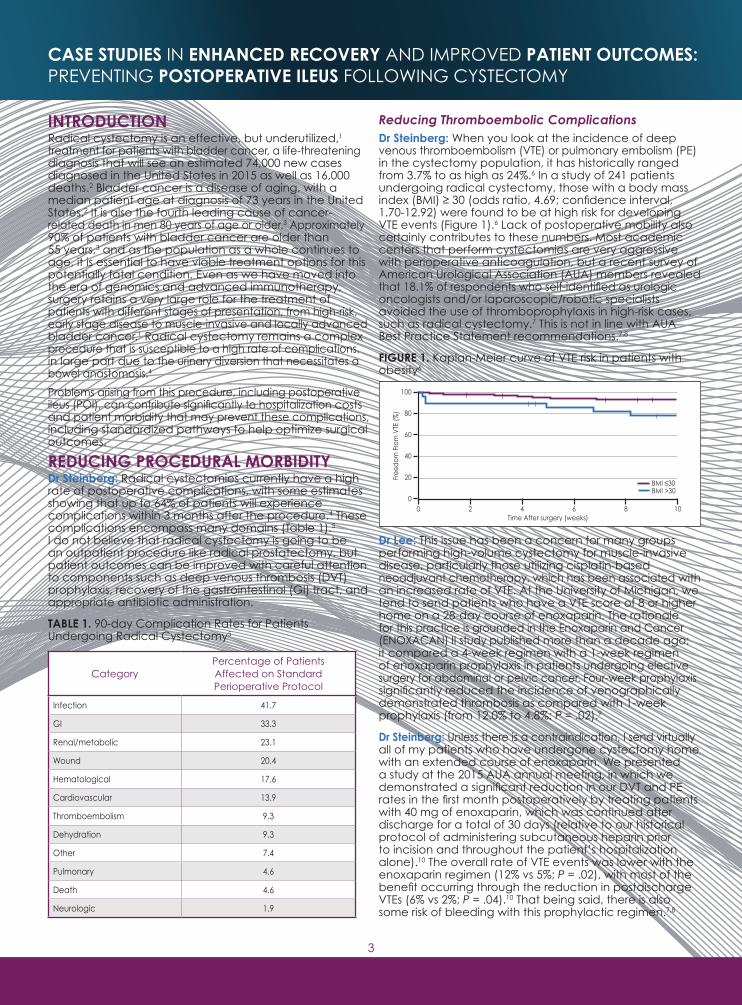
Reducing Thromboembolic ComplicationsDr Steinberg: When you look at the incidence of deep venous thromboembolism (VTE) or pulmonary embolism (PE) in the cystectomy population, it has historically ranged from 3.7% to as high as 24%.6 In a study of 241 patients undergoing radical cystectomy, those with a body mass index (BMI) ≥ 30 (odds ratio, 4.69; confidence interval, 1.70-12.92) were found to be at high risk for developing VTE events (Figure 1).6 Lack of postoperative mobility also certainly contributes to these numbers. Most academic centers that perform cystectomies are very aggressive with perioperative anticoagulation, but a recent survey of American Urological Association (AUA) members revealed that 18.1% of respondents who self-identified as urologic oncologists and/or laparoscopic/robotic specialists avoided the use of thromboprophylaxis in high-risk cases, such as radical cystectomy.7 This is not in line with AUA Best Practice Statement recommendations.7,8
FIGURE 1. Kaplan-Meier curve of VTE risk in patients with obesity6
Dr Lee: This issue has been a concern for many groups performing high-volume cystectomy for muscle-invasive disease, particularly those utilizing cisplatin-based neoadjuvant chemotherapy, which has been associated with an increased rate of VTE. At the University of Michigan, we tend to send patients who have a VTE score of 8 or higher home on a 28-day course of enoxaparin. The rationale for this practice is grounded in the Enoxaparin and Cancer (ENOXACAN) II study published more than a decade ago; it compared a 4-week regimen with a 1-week regimen of enoxaparin prophylaxis in patients undergoing elective surgery for abdominal or pelvic cancer. Four-week prophylaxis significantly reduced the incidence of venographically demonstrated thrombosis as compared with 1-week prophylaxis (from 12.0% to 4.8%; P = .02).9
Dr Steinberg: Unless there is a contraindication, I send virtually all of my patients who have undergone cystectomy home with an extended course of enoxaparin. We presented a study at the 2015 AUA annual meeting, in which we demonstrated a significant reduction in our DVT and PE rates in the first month postoperatively by treating patients with 40 mg of enoxaparin, which was continued after discharge for a total of 30 days (relative to our historical protocol of administering subcutaneous heparin prior to incision and throughout the patient’s hospitalization alone).10 The overall rate of VTE events was lower with the enoxaparin regimen (12% vs 5%; P = .02), with most of the benefit occurring through the reduction in postdischarge VTEs (6% vs 2%; P = .04).10 That being said, there is also some risk of bleeding with this prophylactic regimen.7,8
INTRODUCTIONRadical cystectomy is an effective, but underutilized,1 treatment for patients with bladder cancer, a life-threatening diagnosis that will see an estimated 74,000 new cases diagnosed in the United States in 2015 as well as 16,000 deaths.2 Bladder cancer is a disease of aging, with a median patient age at diagnosis of 73 years in the United States.2 It is also the fourth leading cause of cancer-related death in men 80 years of age or older.3 Approximately 90% of patients with bladder cancer are older than 55 years,3 and as the population as a whole continues to age, it is essential to have viable treatment options for this potentially fatal condition. Even as we have moved into the era of genomics and advanced immunotherapy, surgery retains a very large role for the treatment of patients with different stages of presentation, from high-risk, early stage disease to muscle-invasive and locally advanced bladder cancer.1 Radical cystectomy remains a complex procedure that is susceptible to a high rate of complications, in large part due to the urinary diversion that necessitates a bowel anastomosis.4
Problems arising from this procedure, including postoperative ileus (POI), can contribute significantly to hospitalization costs and patient morbidity that may prevent these complications, including standardized pathways to help optimize surgical outcomes.
REDUCING PROCEDURAL MORBIDITYDr Steinberg: Radical cystectomies currently have a high rate of postoperative complications, with some estimates showing that up to 64% of patients will experience complications within 3 months after the procedure.4 These complications encompass many domains (Table 1).5 I do not believe that radical cystectomy is going to be an outpatient procedure like radical prostatectomy, but patient outcomes can be improved with careful attention to components such as deep venous thrombosis (DVT) prophylaxis, recovery of the gastrointestinal (GI) tract, and appropriate antibiotic administration.
TABLE 1. 90-day Complication Rates for Patients Undergoing Radical Cystectomy5
CategoryPercentage of Patients Affected on Standard Perioperative Protocol
Infection 41.7
GI 33.3
Renal/metabolic 23.1
Wound 20.4
Hematological 17.6
Cardiovascular 13.9
Thromboembolism 9.3
Dehydration 9.3
Other 7.4
Pulmonary 4.6
Death 4.6
Neurologic 1.9
Time After surgery (weeks)
Free
dom
Fro
m V
TE (%
)
0 2 4 6 8 100
20
40
60
80
100
BMI ≤30BMI >30
CASE STUDIES IN ENHANCED RECOVERY AND IMPROVED PATIENT OUTCOMES: PREVENTING POSTOPERATIVE ILEUS FOLLOWING CYSTECTOMY
4
In the intraoperative period, we have also gone to a more tailored intraoperative fluid program that we hope will reduce bowel edema and may improve outcomes. Currently, we base our fluid input on the patient’s weight, typically administering 2000 to 3000 mL of fluid throughout a typical cystectomy procedure. This figure is considerably less than it used to be. We have not been using a great deal of norepinephrine or other vasoactive drugs, but we have been considering doing so. We have also considered the use of a transesophageal echocardiogram to more precisely deliver intraoperative fluids to optimize cardiac output and ejection fraction.
Dr Steinberg: Intraoperative fluid management remains a great challenge, especially with a rotating staff of anesthesiologists. Some have tried to minimize fluid intake, and we have seen some significant elevations in postoperative serum creatinine, including a couple of cases of acute tubular necrosis. I understand the support in the literature for conservative fluid management, but I believe that utilization of a transesophageal echocardiogram to assess patient fluid volume is an important component of the conservative approach.19 Optimization of fluids with this technology may improve a variety of patient outcomes, including incidence of ileus, PONV, and wound infection rates.19 Fluid estimations can be challenging, and I would prefer to avoid the possibility of putting a patient into renal failure. It is important to get a good fluid and electrolyte balance because you also want to avoid any morbidity associated with interstitial edema, which happens commonly.20
Dr Lee: Other perioperative approaches can help to optimize GI recovery. Nasogastric (NG) or orogastric tubes are frequently employed during the cystectomy procedure, but the tube is generally removed at the end of the case. Studies have shown that early NG tube removal reduces GI recovery time, reduces patient morbidity, and also shortens the duration of hospitalization.21
With respect to early oral nutrition and mobilization, our approach to dietary advancement is not as aggressive as some centers, in which people may be started on a regular diet on postoperative day 0. We start with sips of water and ice chips on postoperative day 0. On postoperative day 1, the patient receives 8 oz of clear liquids, tea, and/or black coffee per shift. The patient receives an unrestricted clear liquid diet on day 2 and then a “regular” diet by postoperativeday 3. Our center encourages ambulation in the early postoperative period, including postoperative night 0 if the patient is able.
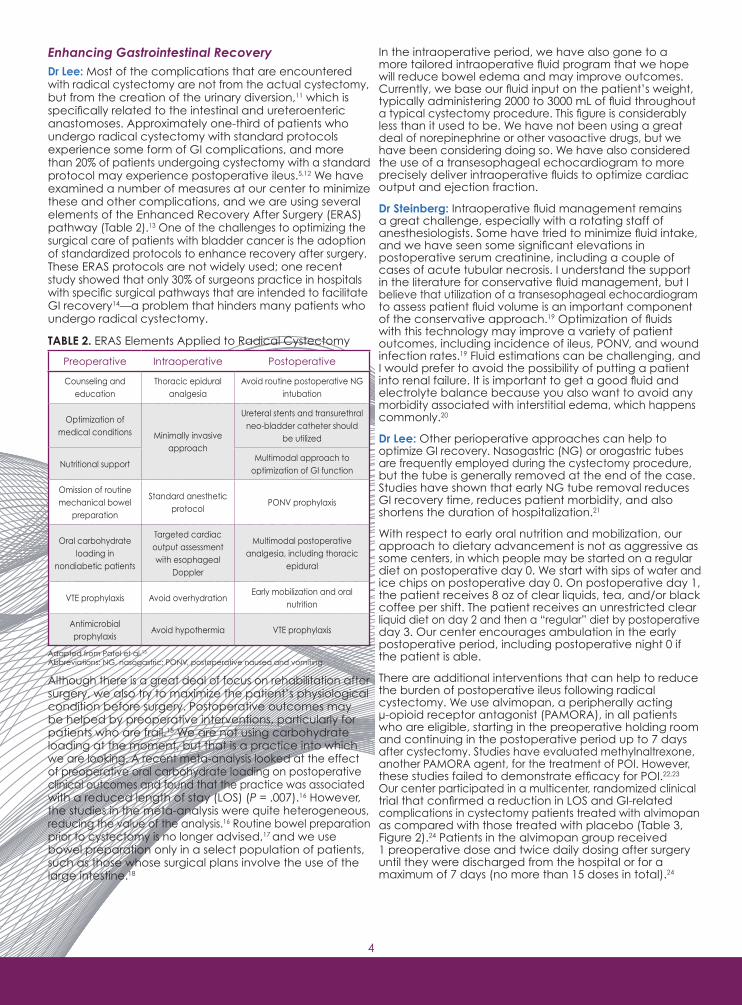
There are additional interventions that can help to reduce the burden of postoperative ileus following radical cystectomy. We use alvimopan, a peripherally acting μ-opioid receptor antagonist (PAMORA), in all patients who are eligible, starting in the preoperative holding room and continuing in the postoperative period up to 7 daysafter cystectomy. Studies have evaluated methylnaltrexone,another PAMORA agent, for the treatment of POI. However, these studies failed to demonstrate efficacy for POI.22,23 Our center participated in a multicenter, randomized clinical trial that confirmed a reduction in LOS and GI-related complications in cystectomy patients treated with alvimopan as compared with those treated with placebo (Table 3, Figure 2).24 Patients in the alvimopan group received 1 preoperative dose and twice daily dosing after surgery until they were discharged from the hospital or for a maximum of 7 days (no more than 15 doses in total).24
Enhancing Gastrointestinal RecoveryDr Lee: Most of the complications that are encountered with radical cystectomy are not from the actual cystectomy, but from the creation of the urinary diversion,11 which is specifically related to the intestinal and ureteroenteric anastomoses. Approximately one-third of patients who undergo radical cystectomy with standard protocols experience some form of GI complications, and more than 20% of patients undergoing cystectomy with a standard protocol may experience postoperative ileus.5,12 We have examined a number of measures at our center to minimize these and other complications, and we are using several elements of the Enhanced Recovery After Surgery (ERAS) pathway (Table 2).13 One of the challenges to optimizing the surgical care of patients with bladder cancer is the adoption of standardized protocols to enhance recovery after surgery. These ERAS protocols are not widely used; one recent study showed that only 30% of surgeons practice in hospitals with specific surgical pathways that are intended to facilitate GI recovery14—a problem that hinders many patients who undergo radical cystectomy.
TABLE 2. ERAS Elements Applied to Radical Cystectomy
Although there is a great deal of focus on rehabilitation after surgery, we also try to maximize the patient’s physiological condition before surgery. Postoperative outcomes may be helped by preoperative interventions, particularly for patients who are frail.15 We are not using carbohydrate loading at the moment, but that is a practice into which we are looking. A recent meta-analysis looked at the effect of preoperative oral carbohydrate loading on postoperativeclinical outcomes and found that the practice was associated with a reduced length of stay (LOS) (P = .007).16 However, the studies in the meta-analysis were quite heterogeneous, reducing the value of the analysis.16 Routine bowel preparation prior to cystectomy is no longer advised,17 and we use bowel preparation only in a select population of patients, such as those whose surgical plans involve the use of the large intestine.18
Preoperative Intraoperative Postoperative
Counseling and education
Thoracic epidural analgesia
Avoid routine postoperative NG intubation
Optimization of medical conditions Minimally invasive
approach
Ureteral stents and transurethral neo-bladder catheter should
be utilized
Nutritional supportMultimodal approach to
optimization of GI function
Omission of routine mechanical bowel
preparation
Standard anesthetic protocol
PONV prophylaxis
Oral carbohydrate loading in
nondiabetic patients
Targeted cardiac output assessment with esophageal
Doppler
Multimodal postoperative analgesia, including thoracic
epidural
VTE prophylaxis Avoid overhydrationEarly mobilization and oral
nutrition
Antimicrobial prophylaxis
Avoid hypothermia VTE prophylaxis
Adapted from Patel et al.13
Abbreviations: NG, nasogastric; PONV, postoperative nausea and vomiting.
5
TABLE 3. Safety and Efficacy Data: Alvimopan vs Placebo in a Study of Patients Undergoing Radical Cystectomy and Receiving Postoperative Intravenous Patient-Controlled Analgesia24
FIGURE 2. Postoperative LOS by day in modified intent-to-treat population.* Both mean and median postoperative LOS are shorter in the alvimopan group.24
Dr Lee: Although this particular study excluded the use of epidural analgesia, this practice is generally encouraged as part of ERAS guidelines following cystectomy.21 We believe that patients receiving opioid-based epidurals or multimodal analgesia involving opioids may see improvements in GI recovery with alvimopan use, but this effect has not been assessed in controlled studies.24
Dr Steinberg: I certainly feel that alvimopan has a good safety profile when used appropriately. There were more incidents of cardiac AEs, such as myocardial infarction and neoplasms, seen in a clinical trials in which patients with chronic opioid pain management were taking alvimopan twice daily for 12 months; these incidents were not statistically significant.25 This trend was less evident when data from this study were pooled with similar studies.25 It is only approved for short-term use through a risk evaluation and management strategy (REMS) program-enrolled pharmacy in facilities in which bowel resections are performed (see REMS Programs).26
Dr Kraft: As part of this program, hospital staff who prescribe, dispense, or administer alvimopan need to be provided with the educational materials on the need to limit use of alvimopan to short-term, inpatient use.26 Pharmacists can help with the development of these educational plans, including education modules and competency assessments.
Alvimopan Group (n=143)
Placebo Group (n=134)
Mean time to upper* and lower† GI recovery (HR 1.8 [P < .0001]), d
5.5 6.8
Mean LOS (P = .0051), d 7.4 10.1
Episodes of morbidity‡ related to postoperative ileus (P < .001), %
8.4 29.1
Cardiovascular AEs (P = .09), % 8.4 15.3
Serious AEs, % 25.7 48.9
Abbreviations: AEs, adverse events; HR, hazard ratio.* First tolerance of solid food. † First bowel movement. ‡ Need for postoperative NG tube placement, prolonged hospitalization due to POI, or readmission for POI within 1 week of discharge.
Hospitals must be enrolled in the specific alvimopan REMS program, and the pharmacy/hospital system should have measures in place to restrict administration to the inpatient setting (no more than 15 total doses), with no transfer of alvimopan to programs that are not enrolled in the specific REMS program.26 Pharmacists and surgeons can work together to develop care pathways and corresponding order sets that incorporate REMS-governed medications with appropriate criteria for use. Pharmacists can also develop plans to complete a medication use evaluation to assess appropriate use and impact on outcomes.
Dr Steinberg: Collaboration can definitely help to improve the range and appropriate use of pharmacologic treatment options available for our patients. Cost considerations are also a topic of importance. We performed an economic analysis of alvimopan usage vs placebo in patients undergoing radical cystectomy in a phase 4 clinical trial. Reduction in health care services related to POI and shorter hospital stays decreased hospitalization cost. Costs related to POI were $2340 less for patients receiving alvimopan, and mean total combined costs were $2640 less per patient for those receiving alvimopan.29 The mean difference in POI costs was significant (P = .04), but the total combined costs finding (P = .068) was not.
Chewing gum may also be used to facilitate bowel recovery for those patients who are willing to do it.30 Narcotic use is minimized, particularly after the first 24 to 36 hours following the procedure. Patients on an ERAS protocol after radical cystectomy have been shown to have less opioid use than those on a traditional protocol (4.9 mg vs 20.67 mg morphine equivalents; P < .001), but also report more discomfort (visual analog scale 3.1 vs 1.14; P < .001).12 To avoid opiates, in some cases, we are using regional anesthesia in the postoperative setting as well as lidocaine patches and ketorolac. With the use of nonsteroidal anti-inflammatory therapies to control pain, there is a risk for GI bleeding. I think that in the radical cystectomy patient population—which often has multiple medical comorbidities, including renal impairment—pharmacologic interventions certainly need to be used judiciously.
* All patients who received ≥1 dose of study medication, who had protocol-specified surgery and ≥1 postdose GI assessment after surgery for bowel movement or tolerability of solids.
Patie
nts
(%)
4 8765 1211109 16151413 20191817 772925 3922 31210
Alvimopan 12 mg (n=143)Placebo (n=134)
30
25
15
20
10
5
Postoperative LOS
REMS Programs REMS are mandated by the US Food and Drug Administration to address potentially serious risks that may be associated with particular medications.
Patients and providers should be well informed regarding specific benefits and risks associated with drugs that may be utilized in their care.27
This is frequently a cumbersome process for pharmacists because there is no standardization of REMS programs. There are currently active efforts to investigate and streamline this process.28
Pharmacists and surgeons should collaborate to ensure compliance with REMS programs and facilitate the appropriate use of medications that fall under them. Pharmacists should take a proactive role by identifying an appropriate person to enroll their institutions in the REMS program, such as the Director of Pharmacy.

6
patients who have multiple medical problems at baseline, C difficile infection can lead to diarrhea, sepsis, and even death. We are in need of further research to understand why some patients develop C difficile infections even with judicious use of antibiotics, early patient ambulation, early dietary advancement, and omission of bowel preparations.
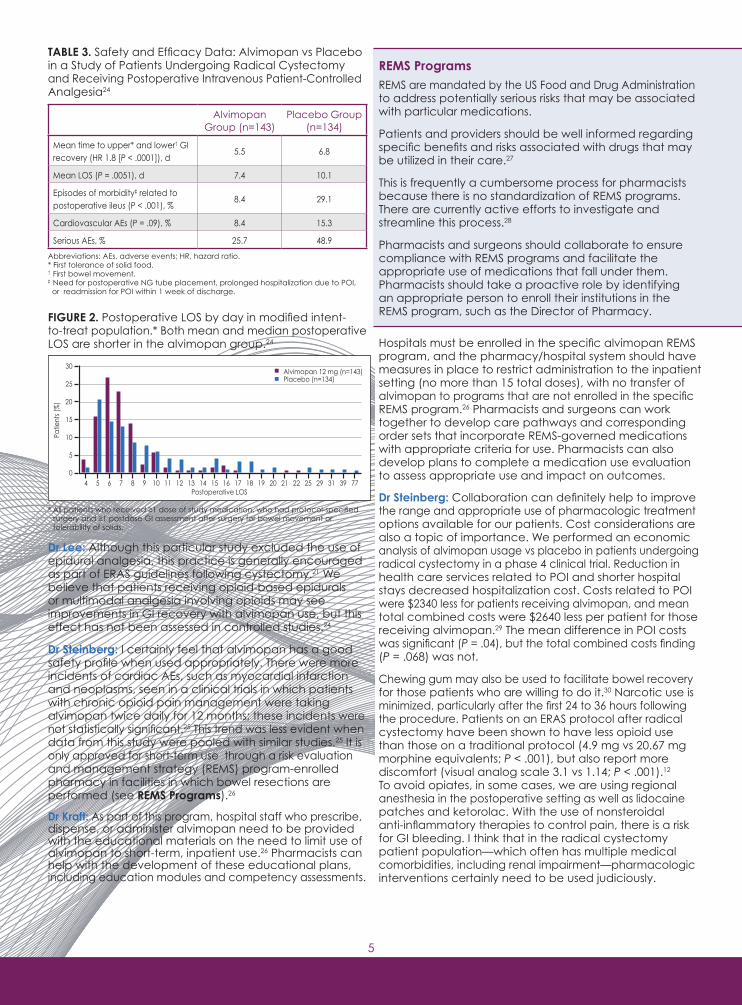
FIGURE 3. Rates of C difficile infection among hospitalized patients aged ≥65 years* by age group: National Hospital Discharge Survey, United States, 1996-200943
SUMMARYDr Lee: Although the majority of radical cystectomies take place at community hospitals, most of these individual centers perform very few procedures.44,45 It can be difficult to develop protocols and pathways for low-volume procedures because there is unlikely to be a dedicated health care team to sustain the practices. Moreover, creating and maintaining these pathways requires an investment in time from pharmacists, nurses, and physicians.
Dr Steinberg: Each center may only perform a couple of cystectomies during an entire year. Even in community hospitals in which the integration of an ERAS pathway can exceed the resources available, the development of pathways that can improve patient outcomes is essential, particularly regarding pharmaceutical measures that may be employed.
Dr Kraft: The implementation of electronic health records has also helped with the development of standardized perioperative plans. They have helped to improve the efficiency of requests for particular pharmaceutical options that may enhance patient outcomes but require a REMS. Preoperative electronic order sets can help prompt clinicians to address the risks and benefits of pharmaceutical interventions on a case-by-case basis.
CASE 1Initial PresentationA 70-year-old man with multifocal high-grade Ta urothelial cell carcinoma (UCC) presents for assessment after recurrence of his cancer.
History of Present IllnessHe originally presented to the urology clinic in the Fall of 2014 with painless gross hematuria. He underwent a transurethral resection of a bladder tumor (TURBT), which revealed high-grade T1 UCC with associated carcinoma in situ. He received 5 weeks of induction bacille Calmette-Guérin (BCG), not getting the full 6 weeks due to a BCG shortage. He did receive 3 weeks of maintenance BCG. Unfortunately, he experienced a fairly rapid recurrence
I have tried the use of prokinetic agents to help accelerate bowel recovery in patients undergoing cystectomy, but I have not had a great deal of success. A Cochrane review has shown inconsistent evidence of efficacy for several agents in the treatment of postoperative ileus, including cisapride, propranolol, cholecystokinin-like drugs, vasopressin, and dopamine antagonists.31 There was no evidence of efficacy for erythromycin.31 For bowel recovery, I am leery of using neostigmine on the floor in situations in which there is no cardiac monitoring, especially because many of the elderly patients who undergo cystectomy also have some degree of a cardiac history. Although the dose of neostigmine used in ERAS pathways is very low (0.5 mg subcutaneously twice daily starting on postoperative day 1 until bowel activity for a maximum of 72 hours),18 it still concerns me.
Dr Lee: Those are definitely some important points. Despite the use of perioperative pathways, it is still important to be aware of the individual patient’s needs and comorbidities. I will refrain from using ketorolac on postoperative day1 in patients who have worrisome serum creatinine and glomerular filtration rate values or a hematocrit level that is trending downward from the postoperative value.
Infection PreventionDr Steinberg: Radical cystectomy has been associated with a high incidence of health care–associated infections.32 Infection prevention is also another key component in improving outcomes for patients who undergo cystectomy. We used to create a perfect storm for complications by administering bowel preparations, keeping patients on nothing-by-mouth for 5 to 7 days and giving them antibiotics at length. Then, we could not figure out why they had trouble with resistant pathogens and Clostridium difficile infections. Some institutions have reported rates of postoperative C difficile infection as high as 8.8% for patients undergoing radical cystectomy, with extended antibiotic exposure and chronic antacid therapy as associated factors.33,34 Our rates of C difficile have plummeted recently, with more judicious utilization of antibiotic therapy. The overall compliance rate of appropriate antimicrobial use for radical cystectomy in community practice urology (according to the 2008 AUA Best Practice Policy Statement) was only 0.6%.35 We do not use routine bowel preparations and try to preserve a healthy microbiome as much as possible. With normal motility and normal bacterial colonization, GI outcomes have improved. Based on our own experience and other data, I believe that prompt recovery of bowel function can reduce the risk of severe C difficile infection,36-38 which can be a tremendously difficult problem to overcome in the perioperative and postoperative period.
Dr Kraft: Some of the classes of agents that have been particularly problematic with respect to C difficile infections include proton pump inhibitors,39 fluoroquinolones,40 second- and third-generation cephalosporins,41 and clindamycin.42 Studies have identified use of these agents as a risk factor for the development of C difficile infections, and I believe that it is imperative to reduce/avoid risk factors whenever possible and appropriate.
Dr Lee: We have struggled with C difficile infections in the past, and although we have employed several of the measures that you just mentioned, we still have occasional spikes in infection rates. Our institutional infection control group has done handwashing and gown/glove studies to observe behavior and practices of the care team as well as a number of the other ancillary workers who interact with patients. We still do not have a great answer. The rates of C difficile among hospitalized patients who are older than 65 are significant (Figure 3).43 We have seen some severe cases of C difficile infection, including resistant strains. Some patients have required operative interventions. For
Year
Rate
per
100
,000
pop
ula
tion†
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 20090
≥65 y65-74 y75-84 y≥85 y
1,250
1,000
750
500
250
* Includes patients aged ≥65 years who were either hospitalized with Clostridium difficile infections or who acquired C difficile during the hospital stay. All of these patients had a discharge diagnosis coded 008.45 based on the International Classification of Diseases, Ninth Revision, Clinical Modification, either as a first-listed diagnosis or as 1 of up to 6 secondary diagnosis codes collected in the survey.† Rates for 1996-1999 were based on U.S. Census Bureau civilian population estimates adjusted for the net underenumeration in the 1990 census. Rates for 2000-2009 were calculated using U.S. Census Bureau 2000–based postcensal civilian population estimates.

7
of multifocal high-grade Ta UCC, which was revealed during a second TURBT in April 2015.
Medical History and Social HistoryThe patient is noted to have several chronic medical problems, including atrial fibrillation, hypertension, hyperlipidemia, diabetes, congestive heart failure, and coronary artery disease (with coronary artery bypass graft procedures in 2000 and 2009). He currently takes several medications to manage these conditions. He is a former smoker, quitting 6 years ago after a 50-pack/y history. He remains fairly active, with a BMI of 24.8 kg/m2.
Operative PlanThe patient decides to undergo radical cystectomy, with accompanying bilateral pelvic lymph node dissection and ileal conduit diversion. He is placed on a perioperative pathway that is standard for the surgical center. He does not have an NG tube placed but has an orogastric tube that is removed when he is extubated. He receives DVT and PE prophylaxis as well as intravenous (IV) fluids. Early patient ambulation efforts are encouraged, with the involvement of physical therapy and occupational therapy. Chest physiotherapy is also involved, with the use of incentive spirometry. Patient-controlled analgesia is provided. He receives his first dose of antibiotic therapy before surgery and receives a total course of 24 hours. The patient receives alvimopan in the preoperative holding area before his procedure and continues this therapy on a twice-daily basis.
Postoperative CourseOn postoperative day 1, the patient experiences paroxysmal atrial fibrillation. He receives a cardiology consultation, and his atrial fibrillation is managed with adjustment of his metoprolol and fluids. He begins ambulation with physical therapy and experiences an elevation in his serum creatinineon postoperative day 2, which rises from 1.6 to 2.8. He receives a nephrology consultation and undergoes a renal ultrasound, which shows no signs of hydronephrosis (Figure 4).
FIGURE 4. Renal ultrasound, postoperative day 2
On postoperative day 4, he has flatus and is tolerating sips of liquids. His diet is advanced over the next 48 hours, with commencement of bowel movements and normalization of his creatinine to 1.2. He is discharged on postoperative day 7. The final pathology assessment reveals high-grade papillary carcinoma and carcinoma in situ, with negative margins, pT1N0MX.
FACULTY DISCUSSIONDr Lee: Patients such as this who have multiple medical comorbidities may not be able to adhere to established pathways as strictly as those who have fewer health problems. Many of these patients may have complications that develop during their stay in the hospital. Often, frail patients may experience a cascade of complications simply related to changes in fluid status, including cardiac arrhythmias, acute kidney injury, and labile blood pressure. As the major physiologic shifts associated with major surgery cease and patients mobilize excessive fluids 3 to 4 days after surgery, there is greater resolution of hemodynamic instability.
Dr Steinberg: Some patients need additional time to recover from surgery, especially those who may lack physiologic reserve. Historically, small complications could readily turn into larger problems. I believe that mobilization efforts and facilitation of GI tract recovery have helped to mitigate many of the significant perioperative problems that bladder cancer surgeons face, even today.
Dr Kraft: Some patients may develop a transient increase in serum creatinine in the postoperative period. This patient recovered; however, any patient who goes on to develop acute kidney injury (although uncommon) may require medication dose adjustments.46 Assessment of renal function should be a part of the patient evaluation, especially for someone who continues to receive alvimopan. In this particular case, alvimopan should be accompanied by ongoing renal assessment to ensure its safety and the satisfaction of criteria for its usage.
CASE 2Initial PresentationA 72-year-old man with high-grade T1 UCC presents for assessment after recurrence of his cancer.
History of Present IllnessHe underwent a TURBT in August 2012, which revealed high-grade T1 UCC. He underwent 6 weeks of induction BCG. A second TURBT, in August 2014, again revealed high-grade T1 UCC. He underwent 6 weeks of induction BCG and 3 weeks of maintenance BCG. A third TURBT, in April 2015, revealed high-grade T1 UCC. A chest x-ray and computed tomography (CT) scan of the abdomen and pelvis in May 2015 showed no evidence of metastases.
Medical History and Social HistoryThe patient is noted to have several chronic medical problems, including hypertension, hyperlipidemia, diabetes mellitus, and a history of prostate cancer that was treated with radical retropubic prostatectomy in 2006. He takes several medications for his chronic medical conditions. He is a former 30-pack/y smoker and remains active, with a BMI of 26.0 kg/m2.
Operative PlanThe patient decides to undergo radical cystectomy, with bilateral pelvic lymph node dissection and ileal conduit creation, in June 2015. He is noted to have significant pelvic adhesions, with his bladder closely adhered to the symphysis pubis. He is placed on a postoperative pathway that is standard for the surgical center, involving early ambulation, initial nothing-by-mouth status, and treatment with alvimopan.
Postoperative CourseFrom postoperative day 2 through postoperative day 4, the patient experiences intermittent nausea and abdominal distension. On postoperative day 4, he has an obstructive abdominal series obtained, which is consistent with ileus (Figure 5).
FIGURE 5. Obstructive series, postoperative day 4 (dilated loops of large and small intestine with air throughout, consistent with ileus)
8
CASE 3Initial PresentationA 64-year-old man with a history of high-grade pT1 UCC of the bladder presents for assessment.
History of Present IllnessThe muscularis propria was present and uninvolved on the initial TURBT in March 2014. He had a CT urogram and chest x-ray that showed no evidence of metastases/other disease outside of the bladder. A restaging TURBT again revealed high-grade pT1 UCC. The patient underwent induction BCG, followed by 1 cycle of maintenance BCG. He experienced a recurrence of high-grade pT1 UCC following the first cycle of maintenance BCG in February 2015.
Medical History and Social HistoryHis medical history is remarkable for glaucoma, arthritis, and obesity. He has a 60-pack/y history of smoking but quit 15 years ago. He is a moderate social drinker and takes naproxen as needed for his arthritis. With a BMI of 35.25 kg/mg2, he was felt to be a good candidate for robotic-assisted cystoprostatectomy.
Operative PlanThe patient was counseled regarding his options, and, in April 2015, he elected to pursue more definitivetherapy with a robotic-assisted, laparoscopic radical cystoprostatectomy (nerve sparing), along with bilateral pelvic lymphadenectomy and extracorporeal ileal conduit urinary diversion. The duration of his procedure was 6.5 hours; he subsequently began a postoperative pathway that was standard for the operating center. He received an initial dose of alvimopan prior to surgery, and this medication was continued postoperatively for 7 days.
Postoperative CourseHe was started on a low-residue diet on postoperative day 1, with the ability to self-titrate. On the evening of postoperative day 1, he began passing flatus, and his pain was managed with IV ketorolac and acetaminophen/hydrocodone by mouth over the next 2 days. He continued passing flatus on postoperative day 3, augmenting his dietary intake, with high drain output. His IV fluid needs resolved by postoperative day 4, and his pain control was transitioned to oral medication. He was discharged home on postoperative day 5 with an abdominal drain and oral pain medications. He has had no concern for ileus, bowel obstruction, or failure to thrive. There was no need for readmission. His final pathology report revealed pTis urothelial carcinoma of the bladder only. All 25 lymph nodes were negative for metastasis. His incidental Gleason score: (3 + 3 = 6) prostate cancer, pT2a.
FACULTY DISCUSSIONDr Lee: This case exemplifies the potential benefits of utilizing a standardized postoperative protocol. This particular patient was able to self-regulate his diet in the perioperative setting and had a positive outcome. Given his timely GI recovery, he was able to be discharged after a short postoperative stay. The patient’s course also raises a discussion about the surgical technique that was employed in his case. A number of the urological surgeons at our center perform robotic-assisted cystectomies. There may not be a clear advantage in terms of perioperative out-comes other than reduction in blood loss.47,48 However, the use of robotic surgery for radical cystectomy, as has happened for radical nephrectomy and prostatectomy, has forced those surgeons who practice open radical cystectomy to focus on, and work to, improve perioperative outcomes. The use of standardized pathways has greatly facilitated this effort. I suspect that the technique will not
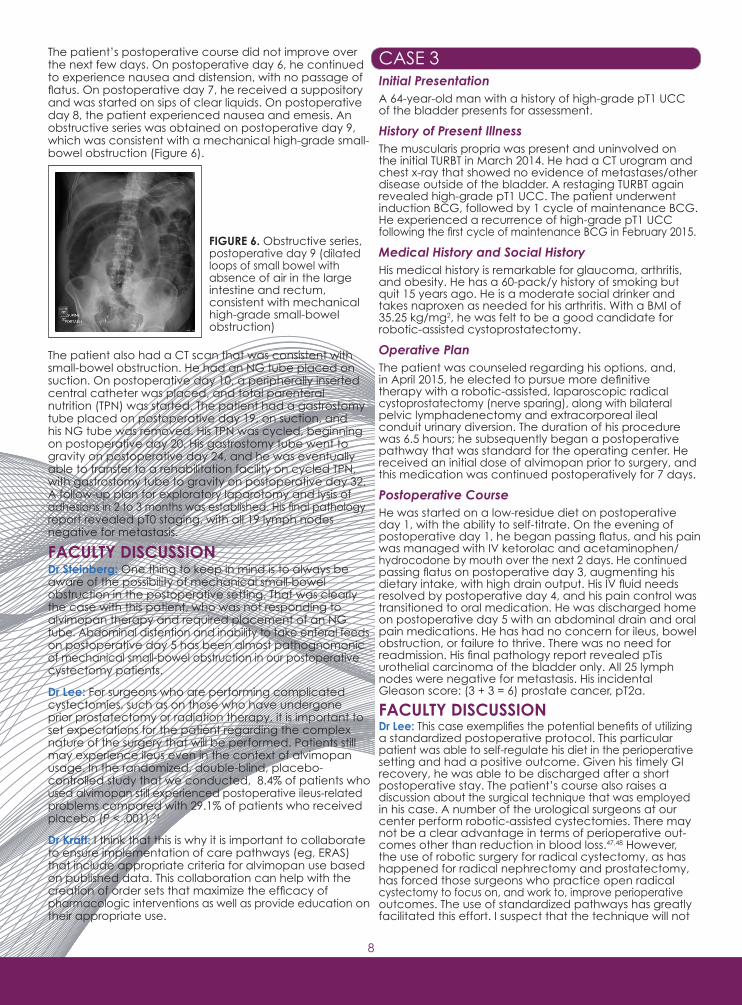
The patient’s postoperative course did not improve over the next few days. On postoperative day 6, he continued to experience nausea and distension, with no passage of flatus. On postoperative day 7, he received a suppository and was started on sips of clear liquids. On postoperative day 8, the patient experienced nausea and emesis. An obstructive series was obtained on postoperative day 9, which was consistent with a mechanical high-grade small-bowel obstruction (Figure 6).
The patient also had a CT scan that was consistent with small-bowel obstruction. He had an NG tube placed on suction. On postoperative day 10, a peripherally inserted central catheter was placed, and total parenteral nutrition (TPN) was started. The patient had a gastrostomy tube placed on postoperative day 19, on suction, and his NG tube was removed. His TPN was cycled, beginning on postoperative day 20. His gastrostomy tube went to gravity on postoperative day 24, and he was eventually able to transfer to a rehabilitation facility on cycled TPN, with gastrostomy tube to gravity on postoperative day 32. A follow-up plan for exploratory laparotomy and lysis of adhesions in 2 to 3 months was established. His final pathology report revealed pT0 staging, with all 19 lymph nodes negative for metastasis.
FACULTY DISCUSSIONDr Steinberg: One thing to keep in mind is to always be aware of the possibility of mechanical small-bowel obstruction in the postoperative setting. That was clearly the case with this patient, who was not responding to alvimopan therapy and required placement of an NG tube. Abdominal distention and inability to take enteral feeds on postoperative day 5 has been almost pathognomonic of mechanical small-bowel obstruction in our postoperative cystectomy patients.
Dr Lee: For surgeons who are performing complicated cystectomies, such as on those who have undergone prior prostatectomy or radiation therapy, it is important to set expectations for the patient regarding the complex nature of the surgery that will be performed. Patients still may experience ileus even in the context of alvimopan usage. In the randomized, double-blind, placebo-controlled study that we conducted, 8.4% of patients who used alvimopan still experienced postoperative ileus-related problems compared with 29.1% of patients who received placebo (P < .001).24
Dr Kraft: I think that this is why it is important to collaborate to ensure implementation of care pathways (eg, ERAS) that include appropriate criteria for alvimopan use based on published data. This collaboration can help with the creation of order sets that maximize the efficacy of pharmacologic interventions as well as provide education on their appropriate use. ASE 3
FIGURE 6. Obstructive series, postoperative day 9 (dilated loops of small bowel with absence of air in the large intestine and rectum, consistent with mechanical high-grade small-bowel obstruction)

9
with all of the ERAS elements, it is a good place to start. Having a standardized pathway can promote efficiency and serve as a base upon which care can be improved. Multidisciplinary conversations between urologists and anesthesiologists are important to help build effective perioperative management plans. Such plans can help to optimize anesthesia administration, fluid management, and other factors that can influence operative outcomes. A collaborative relationship between urologists and pharmacists can also help to promote surgical efficiency and optimize outcomes through the establishment of REMS and standardized order sets for pharmacologic options commonly used in urologic surgery.
Dr Steinberg: It is essential to consider the total picture and all of the different systems that must be preserved when urologic surgery is performed. A consistent, comprehensive plan that addresses perioperative antibiotic management, anticoagulation management, and recovery of the GI tract can improve surgical outcomes.
Dr Kraft: The development of a standardized approach can definitely help to improve outcomes, helping patients realize the full benefits of medical interventions. Medicines need to be utilized appropriately. A collaboration between pharmacists and surgeons can help to develop optimal order sets in the electronic health record. Reduction of hospital costs can be enhanced through efficiencies like this, allowing for shorter hospital stays while preserving other surgical outcomes. Any intervention that can help to minimize or avoid the use of parenteral nutrition altogether can help to reduce complications.
It is also important for all providers involved in the care of patients who undergo cystectomy to review analgesia techniques that can provide the greatest deal of efficacy while reducing the likelihood of postoperative complications. Although there are no data from studies specifically looking at the merits of perioperative epidural analgesia for patients undergoing cystectomy, epidurals have been established as a key component of urology fast-track protocols.21 The ERAS society has stated that “it seems justified to strongly recommend the use of thoracic epidural analgesia for 72 hours after cystectomy.”21
Multimodal analgesia techniques that limit the use of opioids have also been suggested as a strategy for postoperative pain control.51 Again, there are no prospective data specifically pertaining to cystectomy procedures.21 Techniques such as local anesthesia52,53 and the use of acetaminophen and NSAIDs have also been suggested for colorectal procedures, although there is some concern about the possibility of increased anastomotic leakage with NSAID use.21 The multimodal approach can “probably safely be adopted in major urology surgery,” again according to the ERAS society.21,54,55
KEY TAKE-HOME MESSAGES• Standardized protocols, such as those in the ERAS pathways, can be helpful in improving patient outcomes and clinical efficiency• Routinemechanicalbowelpreparationhasnotbeen shown to improve outcomes for patients undergoing radical cystectomy• Minimization of delays in recovery of GI function is important in improving patient outcomes and can be accomplished through interventions such as early mobilization and enteral feeding, early removal of NG tubes, use of alvimopan, use of chewing gum, and minimization of opiate use• Otherkeyperioperativeinventionsthatcanhelpinclude DVT prophylaxis, appropriate use of perioperative antibiotics, andcarefulmanagementoffluidadministrationAcknowledgement: The authors would like to thank Dr Robert MacLaren, PharmD, FCCM, FCCP, for thoughtful review of this manuscript.
make that much of a difference, but the utilization of, and adherence to, a specific pathway will contribute to real decreases in LOS. The results of the multicenter, prospective, randomized trial comparing open versus robotic cystectomy should be available soon.49
Dr Steinberg: I think that it is important to be able to provide both techniques. Clinical decision making and the overall health of the patient are also factors to consider. Urologic surgeons should be aware of the disease process of bladder cancer and nuances of patient management, regardless of surgical technique. Some complications associated with robotic surgery are potentially even more problematic than those encountered with open surgery because our knowledge base regarding the management of open surgery is greater. Cystectomies and prostatectomies are not equivalent procedures.
Dr Lee: One other item to consider is the decision-making process regarding urinary diversion. In our experiences, the nature of the diversion does not change the perioperative pathway for the patient. In the postoperative setting, however, those patients with continent diversions receive education regarding their indwelling catheters and the potential need for cystograms or other studies that may be needed prior to catheter removal. Our patients who have continent diversions or orthotopic diversions participate in pelvic rehabilitation in the perioperative period after the catheters are removed. These patients focus on voiding schedules with maintenance of voiding diaries. Patients are also trained in intermittent catheterization, should it be necessary. Other than that, we have not tailored our perioperative pathway with respect to diversion type.
Dr Steinberg: Specific procedure selection should be a joint decision between the patient and the surgeon. Most surgeons who operate on urologic cancers have no concept of how our lives would be affected by an ileal conduit or a cutaneous continent catheterizeable urinary diversion or neobladder. I think that it is the duty of the surgeon to provide as much information as possible before the procedure takes place.
MANAGING PATIENT EXPECTATIONSDr Lee: Patients who undergo cystectomy require a great deal of support, not only during the surgical procedure but also during the ensuing months and years. Only about 33% of centers that perform radical cystectomies offer bladder cancer support groups to patients.50 We also engage in a great deal of patient reinforcement and education in the preoperative setting to set and manage patient expectations about surgery, particularly about the expected time of discharge. This is helpful for the patient and his/her family. If patients are told that they will go home in 5 days, that is their expectation and they plan to go home at that time. As we have reduced our median LOS, we have also established support for patients who are going home earlier. Patients receive a nurse call within the first 24 to 48 hours after discharge. We have also established a clinic (run by advanced practice nurses or physician assistants) for cystectomy patients to be seen within 1 week of discharge to address evolving questions or worrisome signs and symptoms. Simply having a visiting nurse is not a complete answer, although that can be helpful for patient assessment and obtaining blood draws when necessary. The family needs more than the 1 visit every 2 or so days that is often allowable through insurance. Survivorship programming may also provide support to patients during this period, but, unfortunately, few institutions have these types of resources to assist patients.50
BUILDING EFFECTIVE MULTIDISCIPLINARYCOMMUNICATIONDr Lee: The ERAS protocol is a great model, and although it may be difficult for centers to establish new protocols

10
31. Traut U, Brügger L, Kunz R, et al. Systemic prokinetic pharmacologic treatment for postoperative adynamic ileus following abdominal surgery in adults. Cochrane Database Syst Rev. 2008;23;(1):CD004930.32. Medina-Polo J, Jiménez-Alcaide E, García-Gonzáles L, et al. Health care-associated infections in a department of urology: incidence and patterns of antibiotic resistance. Scand J Urol. 2014;48(2):203-209.33. Liu NW, Shatagopam K, Monn MF, et al. Risk for Clostridium difficile infection after radical cystectomy for bladder cancer: analysis of a contemporary series [published online ahead of print August 13, 2015]. Urol Oncol. doi:10.1016/j.urolonc.2015.07.007. 34. Calvert JK, Holt SK, Mossanen M, et al. Use and outcomes of extended antibiotic prophylaxis in urological cancer surgery. J Urol. 2014;192(2): 425-429.35. Mossanen M, Calvert JK, Holt SK, et al. Overuse of antimicrobial prophylaxis in community practice urology. J Urol. 2015;193(2):543-547.36. Seril DN, Ashburn JH, Lian L, Shen B. Risk factors and management of refractory of recurrent clostridium difficile infection in ileal pouch patients. Inflamm Bowel Dis. 2014;20(12):2226-2233.37. Kim MJ, Kim BS, Kwon JW, et al. Risk facrots for the development of Clostridium difficile colitis in a surgical ward. J Korean Surg Soc. 2012;83(1):14-20.38. Hritani AW, Alkaddour A, House J. Does gastrointestinal dysmotility predispose to recurrent or severe forms of Clostridium difficile infections? Case Rep Gastrointest Med. 2014;2014:575216.39. Barletta JF, El-Ibiary SY, Davis LE, Nguyen B, Raney CR. Proton pump inhibitors and the risk for hospital-acquired Clostridium difficile infection. Mayo Clin Proc. 2013;88(10):1085-1090.40. Sarma JB, Marshall B, Cleeve V,Tate D, Oswald T, Woolfrey S. Effects of fluoroquinolone restriction (from 2007 to 2012) on Clostridium difficile infections: interrupted time-series analysis. J Hosp Infect. 2015;91(1):74-80.41. Pereira JB, Farragher TM, Tully MP, Jonathan Cooke J. Association between Clostridium difficile infection and antimicrobial usage in a large group of English hospitals. Br J Clin Pharmacol. 2014;77(5):896-903.42. Cruz-Rodríguez NC, Hernández-García R, Salinas-Caballero AG, Pérez- Rodríguez E, Garza-González E, Camacho-Ortiz A. The effect of pharmacy restriction of clindamycin on Clostridium difficile infection rates in an orthopedics ward. Am J Infect Control. 2014;42(6):e71-e73.43. QuickStats: rates of Clostridium difficile infection among hospitalized patients aged ≥65 years by age group – National Hospital Discharge Survey, United States, 1996-2009. September 2,2011;60(34):1171. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6034a7.htm. Accessed October 26, 2015.44. Hollenbeck BK, Taub DA, Miller DC, Dunn RL, Montie JE, Wei JT. The regionalization of radical cystectomy to specific medical centers. J Urol. 2005;174(4 Pt 1):1385-1389.45. Barbieri CE, Lee B, Cookson MS, et al. Association of procedure volume with radical cystectomy outcomes in a nationwide database. J Urol. 2007;178(4 Pt 1):1418-1421, discussion 1421-1422.46. Matzke GR, Aronoff GR, Atkinson AJ Jr, et al. Drug dosing consideration in patients with acute and chronic kidney disease—a clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2011;80(11):1122-1137.47. Bochner BH, Dalbagni G, Sjoberg DD, et al. Comparing open radical cystectomy and robot-assisted laparoscopic radical cystectomy: a randomized clinical trial. Eur Urol. 2015;67(6):1042-1050.48. Wilson TG, Guru K, Rosen RC, et al. Best practices in robot-assisted radical cystectomy and urinary reconstruction: recommendations of the Pasadena Consensus Panel. Eur Urol. 2015;67(3):363-375.49. Parekh DJ, Messer J, Fitzgerald J, Ercole B, Svatek R. Perioperative outcomes and oncologic efficacy from a pilot prospective randomized clinical trial of open versus robotic assisted radical cystectomy. J Urol. 2013;189(2):474-479.50. Lee CT, Mei M, Ashley J, et al. Patient resources available to bladder cancer patients: a pilot study of healthcare providers. Urology. 2012;79(1):172-177.51. Gustafsson UO, Scott MJ, Schwenk W, et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations. World J Surg. 2013;37(2):259-284.52. Bertoglio S, Fabiani F, Negri PD, et al. The postoperative analgesic efficacy of preperitoneal continuous wound infusion compared to epidural continuous infusion with local anesthetics after colorectal cancer surgery: a randomized controlled multicenter study. Anesth Analg. 2012;115(6): 1442-1450.53. Jouve P, Bazin JE, Petit A, et al. Epidural versus continuous preperitoneal analgesia during fast-track open colorectal surgery: a randomized controlled trial. Anesthesiology. 2013;118(3):622-630.54. Maffezzini M, Campodonico F, Capponi G, et al. Fast-track surgery and technical nuances to reduce complications after radical cystectomy and intestinal urinary diversion with the modified Indiana pouch. Surg Oncol. 2012;21(3):191-195.55. Toren P, Ladak S, Ma C, et al. Comparison of epidural and intravenous patient controlled analgesia in patients undergoing radical cystectomy. Canadian J Urol. 2009;16(4):4716-4720.
REFERENCES 1. Spencer ES, Smith AB. Exploring the 3 A’s of cystectomy access to care for muscle-invasive bladder cancer. Urol Oncol. 2015;33(3):105-107.2. National Cancer Institute. SEER stats fact sheets: bladder cancer. http://www.seer.cancer.gov/statfacts/html/urinb.html. Accessed September 15, 2015. 3. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65(1):5-29. 4. Richards KA, Steinberg GD. Perioperative outcomes in radical cystectomy: how to reduce morbidity? Curr Opin Urol. 2013;23(5):456-465.5. Katebian B, Bazarghani S. MP5-06 90-day complications in patients undergoing radical cystectomy on enhanced recovery protocol. J Urol. 2015;193(4S):e47.6. Potretzke AM, Wong KS, Shi F, Christensen W, Downs TM, Abel EJ. Highest risk of symptomatic venous thromboembolic events after radical cystectomy occurs in patients with obesity or nonurothelial cancers. Urol Ann. 2015;7(3):355-360.7. Sterious S, Simhan J, Uzzo RG, et al. Familiarity and self-reported compliance with American Urological Association best practice recommendations for use of thromboembolic prophylaxis among American Urological Association members. J Urol. 2013;190(3):992-998.8. Forrest JB, Clemens JQ, Finamore P, et al. AUA Best Practice Statement for the prevention of deep vein thrombosis in patients undergoing urologic surgery. J Urol. 2009;181(3):1170-1177.9. Bergqvist D, Agnelli G, Cohen AT, et al. Duration of prophylaxis against venous thromboembolism with enoxaparin after surgery for cancer. N Engl J Med. 2002;346(13):975-980.10. Pariser JJ, Pearce SM, Anderson BB, et al. Extended-duration enoxaparin lowers thromboembolic events after radical cystectomy compared to inpatient-only subcutaneous heparin [Abstract MP65-15]. J Urol. 2015;193 (4 suppl):e813. 11. Liedberg F. Early complications and morbidity of radical cystectomy. Eur Urol Suppl. 2010;9:25-30.12. Xu W, Daneshmand S, Bazargani ST, et al. Postoperative pain management after radical cystectomy: comparing traditional versus enhanced recovery protocol pathway. J Urol. 2015;194(5):1209-1213. 13. Patel HRH, Cerantola Y, Valerio M, et al. Enhanced recovery after surgery: are we ready, and can we afford not to implement these pathways for patients undergoing radical cystectomy? Eur Urol. 2014;65(2):263-266. 14. Delaney CP, Senagore AJ, Gerkin TM, et al. Association of surgical care practices with length of stay and use of clinical protocols after elective bowel resection: results of a national survey. Am J Surg. 2010;199(3):299-304.15. Carli F, Awasthi R, Gillis C, Kassouf W. Optimizing a frail elderly patient for radical cystectomy with a prehabilitation program. Can Urol Assoc J. 2014;8(11-12):E884-E887.16. Awad S, Varadhan KK, Ljungqvist O, Lobo DN. A meta-analysis of randomised controlled trials on preoperative oral carbohydrate treatment in elective surgery. Clin Nutr. 2013;32(1):34-44.17. Duncan JE, Quietmeyer CM. Bowel preparation: current status. Clin Colon Rectal Surg. 2009;22(1):14-20.18. Daneshmand S, Ahmadi H, Schuckman AK, et al. Enhanced recovery protocol after radical cystectomy for bladder cancer. J Urol. 2014;192(1):50-55.19. Pillai P, McEleavy I, Guaghan M, et al. A double-blind randomized controlled clinical trial to assess the effect of Doppler optimized intraoperative fluid management on outcome following radical cystectomy. J Urol. 2011;186(6):2201-2206. 20. Chowdhury AH, Lobo DN. Fluids and gastrointestinal function. Curr Opin Clin Nutr Metab Care. 2011;14(5):469-476.21. Cerantola Y, Valerio M, Persson B, et al. Guidelines for perioperative care after radical cystectomy for bladder cancer: Enhanced Recovery After Surgery (ERAS®) society recommendations. Clin Nutr. 2013;32(6):879-887.22. Rodriguez RW. Off-label uses of alvimopan and methylnaltrexone. Am J Health Syst Pharm. 2014;71(17):1450-1455.23. Yu CS, Chun HK, Stambler N, et al. Safety and efficacy of methylnaltrexone in shortening the duration of postoperative ileus following segmental colectomy: results of two randomized, placebo-controlled phase 3 trials. Dis Colon Rectum. 2011;54(5):570-578.24. Lee CT, Chang SS, Kamat AM, et al. Alvimopan accelerates gastrointestinal recovery after radical cystectomy: a multicenter randomized placebo- controlled trial. Eur Urol. 2014;66(2):265-272.25. Marderstein EL, Delaney CP. Management of postoperative ileus: focus on alvimopan. Ther Clin Risk Manag. 2008;4(5):965-973.26. ENTEREG (alvimopan) [package insert]. Whitehouse Station, NJ: Merck & Co, Inc; 2015.27. Hollingsworth K, Toscani M. Risk evaluation mitigation strategies: the evolution of risk management policy. Popul Health Manag. 2013;16(2): 132-137.28. Barlas S. Pharmacists, deluged with requirements, pressure FDA to standardize REMS programs. P T. 2014;39(1):12-13.29. Kauf TL, Svatek RS, Amiel G, et al. Alvimopan, a peripherally acting μ-opioid receptor antagonis, is associated with reduced costs after radical cystectomy: economic analysis of a phase 4 randomized, controlled trial. J Urol. 2014;191(6):1721-1727.30. Li S, Liu Y, Peng Q, Xie L, Wang J, Qin X. Chewing gum reduces postoperative ileus following abdominal surgery: a meta-analysis of 17 randomized controlled trials. J Gastroenterol Hepatol. 2013;28(7): 1122-1132.

11
6. A 70-year-old male patient with muscle-invasive bladder cancer is preparing for radical cystectomy. The surgeon plans to utilize the large bowel as part of the diversion. Which of the following statements regarding mechanical bowel preparation in this patient’s case is true? a. He should never undergo mechanical bowel preparation b. Mechanical bowel preparation may be used in this patient’s case c. The patient may undergo mechanical bowel preparation if he receives extended postoperative antibiotic prophylaxis d. The patient may undergo mechanical bowel preparation if he has NG tube placement
7. Which of the following outcomes has been shown to be superior with robotic-assisted radical cystectomy relative to open radical cystectomy? a. Complication rates b. Blood loss c. Intermediate-term cancer-specific survival d. Individual procedure costs
8. The use of nonsteroidal anti-inflammatory drugs for pain control in patients who undergo radical cystectomy: a. Is contraindicated b. Should be considered on postoperative day 3 or later c. Contributes to delays in GI recovery d. None of the above
9. Optimization of intraoperative fluid management using transesophageal Doppler may improve all of the following outcomes for patients undergoing radical cystectomy except: a. Nausea and vomiting b. Wound infection rates c. Incidence of ileus d. All of the above
10. What percentage of patients who receive alvimopan after undergoing radical cystectomy experience postoperative ileus-related morbidity? a. 8% b. 18% c. 28% d. 38%
1. Which of the following statements regarding the use of DVT prophylaxis for patients undergoing radical cystectomy is true? a. It is a practice that differs from AUA Best Practice Guidelines b. It reduces bleeding risk for patients with bladder cancer c. It is not a part of ERAS protocols d. It is avoided by many robotic/laparoscopic specialists and urologic oncologists
2. All of the following measures may improve GI recovery time in patients undergoing radical cystectomy except: a. Chewing gum b. Usage of alvimopan c. Postoperative continuation of NG tube placement d. Limitation of postoperative narcotics
3. Which of the following statements regarding C difficile infections in patients undergoing radical cystectomy is false? a. They are a potentially fatal complication of the cystectomy procedure b. They have been associated with the use of prolonged antibiotic coverage c. Current infection rates are less than 2% d. They have been associated with chronic antacid therapy
4. Which of the following practices has been associated with reduction in hospitalization time after radical cystectomy? a. Routine preoperative bowel preparation b. Preoperative carbohydrate loading c. Avoidance of DVT prophylaxis d. Liberal use of opioids for pain management
5. All of the following are true with the use of alvimopan for surgeries involving bowel resection and primary anastomosis except: a. It requires the use of a REMS b. It cannot be administered for more than 15 doses c. It has been shown to help improve GI recovery time following radical cystectomy d. Its use can be continued after hospital discharge
Post-Test QuestionsTo obtain AMA PRA Category 1 Credit™ for this activity, complete the CME Post-Test by writing the best answer to eachquestion in the Answer Box located on the Activity Evaluation/Credit Request form on the following page. Alternatively, you can complete the CME Post-Test at http://www.cmeuniversity.com.
See detailed instructions at Method of Participation and Request for Credit on page 2.

Evaluation FormCASE STUDIES IN ENHANCED RECOVERY AND IMPROVED PATIENT OUTCOMES: PREVENTING POSTOPERATIVE ILEUS FOLLOWING CYSTECTOMY
Activity ID: 11146-EJ-42
ORIGINAL RELEASE: December 2, 2015 LAST REVIEW: November 11, 2015 EXPIRATION: December 2, 2016
Please complete the following evaluation questions to receive your certificate.1. What degree best describes you?o MD/DO o PA/PA-C o NP o RN o PharmD/RPh o PhD o Other, please specify:
2. What is your area of specialization?o Surgery, surgical oncology o Urology o Oncology, medical o Other, please specify:
3. Which of the following best describes your primary practice setting?o Solo practice o Group practice o Government o University/teaching systemo Community hospital o HMO/managed care o Nonprofit/community o I do not actively practiceo Other, please specify:
4. How long have you been in practice?o More than 20 years o 11-20 years o 6-10 years o 1-5 years o Less than 1 year o I do not directly provide care
5. Approximately how many patients do you see each week?o Less than 50 o 50-99 o 100-149 o 150-199 o 200+ o I do not directly provide care
6. How many patients undergoing radical cystectomy do you currently see each week? o Less than 5 o 5-15 o 16-25 o 26-35 o 36-45 o 46-55 o 56 or more o I do not directly provide care
7. Please select the extent to which you agree/disagree that the activity supported the achievement of each learning objective?5 = Strongly Agree 4 = Agree 3 = Neutral 2 = Disagree 1 = Strongly Disagree
• Evaluate the efficacy and safety of current strategies to reduce perioperative complications in procedures involving gastrointestinal (GI)/genitourinary (GU) tract surgeries 5 4 3 2 1• Manage patients who are candidates for procedures involving GI/GU tract surgeries with evidence-based perioperative strategies to prevent postoperative ileus 5 4 3 2 1• Articulate features of perioperative enhanced recovery after surgery protocols that might improve patient outcomes 5 4 3 2 1
8. Please select the extent to which you agree/disagree that the activity achieved the following:5 = Strongly Agree 4 = Agree 3 = Neutral 2 = Disagree 1 = Strongly Disagree
• The faculty were effective in presenting the material 5 4 3 2 1• The content was evidence based 5 4 3 2 1• The educational material provided useful information for my practice 5 4 3 2 1• The activity enhanced my current knowledge base 5 4 3 2 1• The activity provided appropriate and effective opportunities for active learning (eg, case studies, discussion, and Q&A) 5 4 3 2 1• The opportunities provided to assess my own learning were appropriate (eg, questions before, during, or after the activity) 5 4 3 2 1
9. Based upon your participation in this activity, do you intend to change your practice behavior? (Choose only one of the following options)o I do plan to implement changes in my practice based on the information presentedo My current practice has been reinforced by the information presentedo I need more information before I will change my practice
10. Thinking about how your participation in this activity will influence your patient care, how many of your patients are likely to benefit? Please use a number (eg, 250):
11. If you plan to change your practice behavior, what type of changes do you plan to implement? (Check all that apply)o Apply latest guidelines o Choice of treatment/management approach o Change in pharmaceutical therapy o Change in current practice for referral o Change in nonpharmaceutical therapy o Change in differential diagnosis o Change in diagnostic testing o Other, please specify:
12. How confident are you that you will be able to make your intended changes?o Very confident o Somewhat confident o Unsure o Not very confident
13. Which of the following do you anticipate will be the primary barrier to implementing these changes?o Formulary restrictions o Insurance/financial issue o Time constraints o Lack of multidisciplinary supporto System constraints o Treatment-related adverse events o Patient adherence/compliance o Other, please specify:
14. Was the content of this activity fair, balanced, objective, and free of bias?o Yes o No, please explain:
15. Please list any clinical issues/problems within your scope of practice you would like to see addressed in future educational activities:
Request for Credit (*required fields)
Name* Degree* Organization
Specialty* Address*
City, State, ZIP* Telephone Fax
IMPORTANT: Your certificate will be E-MAILED to your listed e-mail address* below. (Please print legibly)
*Valid e-mail address required for receipt of your certificate. You will receive your certificate from [email protected].
For Physicians Onlyo I participated in the entire activity and claim 1.25 credits.o I participated in only part of the activity and claim _____ credits.
89 GU
Post-Test Answer Box1 2 3 4 5 6 7 8 9 10