clostridium difficile infection (cdi): prevention ... · pdf fileic/217/10 c.diff infection...
TRANSCRIPT
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
1
BASINGSTOKE AND NORTH HAMPSHIRE NHS FOUNDATION TRUST
Clostridium difficile Infection (CDI): Prevention, Treatment and Control
IC/217/10
Supersedes: IC/217/07 Owner / Author Name Hazel Gray / Dr Jacqui Prieto Job Title Senior Infection Control Nurse
/ Nurse Specialist in Infection Prevention
Final approval committee
Name Infection Control Committee
Date of meeting 23 July 2010 Authoriser Name Dr Nicki Hutchinson Job title Director Infection Prevention
and Control Signature
Date of authorisation 24.08.10 Review date (maximum 3 years from
date of authorisation) July 2013
Audience (tick all that apply) Trust staff NHS General public
Standards Standards for Better Health C4A NHSLA Hygiene Code Dec 2009 Executive summary This policy outlines the management and infection prevention and control procedures for Clostridium difficile infection (CDI). It emphasises the importance of early diagnosis and prompt isolation and treatment of patients with CDI to reduce the risk of spread to other patients and minimise morbidity for the affected patients. Maintaining high standards of infection prevention practice (hand hygiene, use of Personal Protective Equipment (PPE)), environmental cleanliness and compliance with guidelines for antibiotic prescribing are essential. The importance of providing patients and their relatives with the information they need about CDI is identified. CDIs are reported to the Department of Health through an enhanced surveillance system and outbreaks of infection are reportable as a serious untoward incident. Root cause analysis is performed on all cases of hospital-acquired CDI in order to monitor and improve practice. The PCT annually set targets for reduction of CDIs and for BNHFT. Non compliance with these targets can lead to large financial penalties for the Trust. In the event of death of a patient with CDI, the requirements regarding death certification are outlined.
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
2
Summary of changes The entire policy has been reviewed and updated in line with new national guidance. Action needed and owner of action
• All clinical staff working within the Trust should observe this policy at all times. Any deviation from it should be discussed with the infection control team or a consultant Microbiologist.
• The infection control team is responsible for monitoring compliance and for keeping this policy updated regularly.
• The Infection control team is responsible for ensuring that clinical staff are aware of procedures outlined in this policy and for monitoring compliance.
• Microbiologists and pharmacists are responsible for ensuring prudent use of antibiotics based on a regularly updated over arching antibiotic policy.
Audit and Monitoring: Standards:
• All infection episodes are monitored and reported and rates fed back to clinical staff, the Health Protection Agency (HPA) and the local authority (SHA).
• Patients infected with C. difficile infection (CDI) are appropriately and promptly isolated with infection control precautions essential for prevention of cross-infection and re-infection.
• Staff are aware of isolation procedures. • High risk antibiotics are not used to treat patients over the age of 65 years unless
absolutely necessary. Audit methods:
• Enhanced surveillance of cases of C. difficile with reporting within the Trust and to the SHA and HPA by surveillance nurse and infection control doctor (ICD).
• Root Cause analysis performed on all hospital acquired cases (stool sample positive more than 72hours after admission). This is led by the infection prevention and control team with the clinical and nursing staff looking after the patient.
• Audit of compliance with antibiotic prescribing undertaken by Microbiologists and clinical pharmacists e.g. point prevalence survey.

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
3
Contents Page 1.0 Introduction 4 2.0 What is Clostridium difficile? 4 3.0 Responsibilities for the management of CDI 5 4.0 Performance targets 5 5.0 What are the risk factors for CDI? 5 6.0 Antibiotic prescribing 6 7.0 Signs and Symptoms of CDI 6 8.0 Diagnosis of CDI 7 9.0 Treatment of CDI 7 10.0 Infection Prevention Measures 8 10.1 Prudent use of antibiotics 9 10.2 Isolation Precautions 9 10.3 Environmental Cleaning 10 10.4 Surveillance 11 11.0 Patient Information 11 12.0 Outbreak Control 11 13.0 Death Certification 13 14.0 Infection Prevention and Control Contacts 14 15.0 References 14 Appendix 1: Clostridium difficile Care Pathway 16 Appendix 2: Bristol Stool Chart 20

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
4
1.0 Introduction This policy outlines the management and infection prevention and control procedures for Clostridium difficile infection (CDI). It has been reviewed and updated in accordance with new national guidance issued in January 2009. Effective application of this policy, along with other relevant guidance on antimicrobial prescribing and infection prevention and control practice, by all staff will enable the Trust to maintain high standards of patient safety with respect to the prevention and control of CDI. 2.0 What is Clostridium difficile? Clostridium difficile is a Gram-positive anaerobic bacillus capable of forming spores. The organism can produce two principal toxins (Toxin A and Toxin B), although not all strains are toxin-producing. Both Toxin A and B can cause diarrhoea and colitis. C. difficile spores are capable of survival in the environment for long periods, as they are resistant to heat, drying and to the bactericidal effects of alcohol and most chemical disinfectants. This has implications for methods of hand hygiene and environmental disinfection. Antibiotics disturb the normal gut flora, some more than others. Ingested C. difficile spores germinate in this altered microbial environment and can multiply rapidly. Strains that produce toxin then cause symptoms of C. difficile infection (CDI). The clinical presentation ranges from mild diarrhoea to, more unusually, severe colitis with dehydration, pseudomembranous colitis, megacolon and perforation.
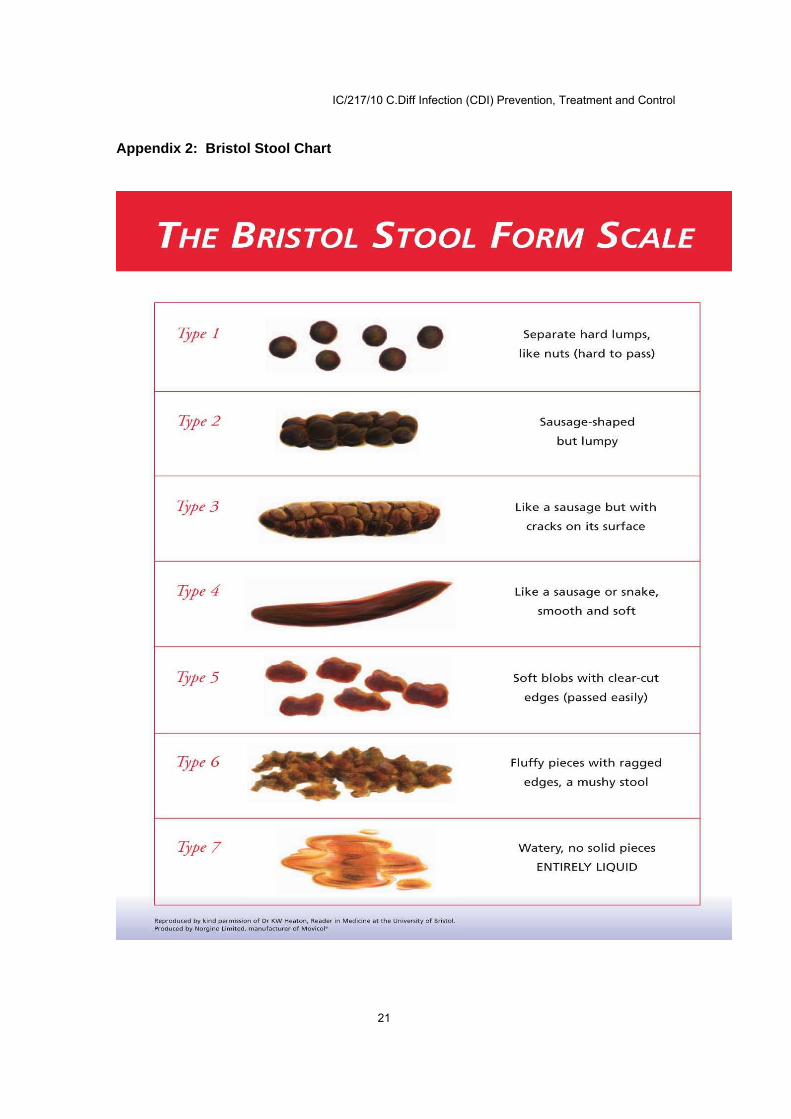
The attack rate is variable, complicating our understanding of the epidemiology of outbreaks. People with serious underlying illnesses and the elderly are at greatest risk – over 80% of CDIs reported are in people aged over 65 years. Community-associated CDI has been increasingly recognized, although the extent of, and risk factors for community acquisition are not well understood. A new type of C. difficile (type 027), which was first isolated in 1999, has caused major outbreaks, including those in Stoke Mandeville Hospital in 2004-2005 and in Maidstone and Tunbridge Wells NHS Trust in 2006, that were the subject of investigation by the Healthcare Commission. This type lacks the gene that restricts toxin production resulting in excessive production of toxins and a higher proportion of severe disease in patients affected. As a result it has a higher mortality rate and is more able to spread between patients. Definitions: C. difficile infection: one episode of diarrhoea, defined either as stool loose enough to take the shape of a container used to sample it or as Bristol Stool Chart types 5–7 (Appendix 1), that is not attributable to any other cause, including medicines (Appendix 2), and that occurs at the same time as a positive toxin assay (with or without a positive C. difficile culture) and/or endoscopic evidence of pseudomembranous colitis (PMC). (Code: Duty 10l; Annex 2) B A period of increased incidence (PII) of CDI: two or more new cases (occurring >48 hours post admission, not relapses) in a 28-day period on a ward. An outbreak of C. difficile infection: two or more cases caused by the same strain related in time and place over a defined period that is based on the date of onset of the first case.

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
5
3.0 Responsibilities for the management of CDI The latest DH guidance on CDI emphasises three key principles in the management of CDI:
• CDI should be managed as a diagnosis in its own right (Healthcare Commission, 2007b in DH/HPA 2009).
• The safety of patients cannot be compromised by other strategic or financial objectives but is at the centre of everything we do (Commission for Healthcare Audit and Inspection, 2006 and Healthcare Commission, 2007a in DH/HPA 2009).
• Infection control, including CDI, is “everybody’s business” (Committee on Public Accounts, 2000 and Healthcare Commission, 2007a in DH/HPA 2009), requiring not only a ‘board to ward’ approach in the hospital but active engagement of primary care trusts (PCTs), health protection units (HPUs) and strategic health authorities (SHAs), using the rubric of clinical and corporate governance.
Individual doctors and nurses are responsible for initiating early diagnosis and prompt isolation, and for compliance with guidelines for antibiotic prescribing, hand hygiene and wearing disposable gloves and aprons. Trust management and PCTs are responsible for ensuring that isolation facilities match demand; that resources are made available for antimicrobial management teams (AMTs), surveillance, audit, rapid diagnosis, environmental cleaning and education; that there are collaborative links with HPUs and SHAs; and that patients and the public are kept informed proactively of policies and practice, as appropriate. 4.0 Performance targets Currently there is public, media and political interest in CDI and the Hygiene Code updated in 2009 recognises the growing problem with CDI as a cause of healthcare associated infections. Targets for reducing these infections have been set up locally by the health authority. For 2010/11 BNHFT has a ceiling of 60 cases with an internal stretch to 48. ll clinical staff have a role to play to help achieve this. CDI causes significant morbidity and mortality and directly impacts on overall patient flow and care. With an average increased length of stay of 21 days, the total cost of CDI has been estimated at over £4000 per case. A reduction in these infections will have significant clinical, operational and financial implications. 5.0 What are the risk factors for CDI? The pathogenesis of CDI involves 3 key elements: (1) disruption of normal intestinal flora (usually by broad spectrum antibiotics), (2) exposure to C. difficile (usually during hospitalisation) and (3) host factors (co-morbidity and advanced age or impaired immune status) (McFarland et al, 2007). Factors known to increase the risk of CDI have been identified as follows:
• Antibiotic use (see below under 6.0) • Age over 65 years* • Hospitalisation** • Debility or impaired immune function • Nasogastric tube feeding • Recent endoscopic procedure
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
6
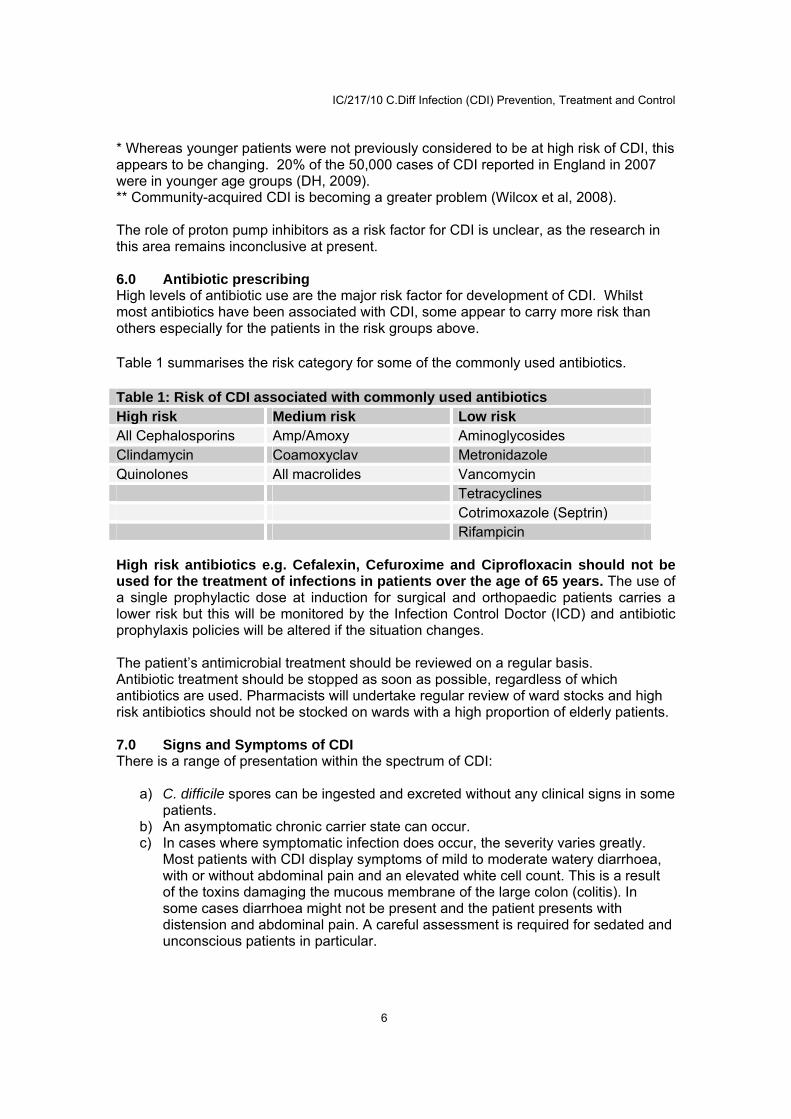
* Whereas younger patients were not previously considered to be at high risk of CDI, this appears to be changing. 20% of the 50,000 cases of CDI reported in England in 2007 were in younger age groups (DH, 2009). ** Community-acquired CDI is becoming a greater problem (Wilcox et al, 2008). The role of proton pump inhibitors as a risk factor for CDI is unclear, as the research in this area remains inconclusive at present. 6.0 Antibiotic prescribing High levels of antibiotic use are the major risk factor for development of CDI. Whilst most antibiotics have been associated with CDI, some appear to carry more risk than others especially for the patients in the risk groups above.
Table 1 summarises the risk category for some of the commonly used antibiotics.
Table 1: Risk of CDI associated with commonly used antibiotics High risk Medium risk Low risk All Cephalosporins Amp/Amoxy Aminoglycosides Clindamycin Coamoxyclav Metronidazole Quinolones All macrolides Vancomycin Tetracyclines Cotrimoxazole (Septrin) Rifampicin High risk antibiotics e.g. Cefalexin, Cefuroxime and Ciprofloxacin should not be used for the treatment of infections in patients over the age of 65 years. The use of a single prophylactic dose at induction for surgical and orthopaedic patients carries a lower risk but this will be monitored by the Infection Control Doctor (ICD) and antibiotic prophylaxis policies will be altered if the situation changes. The patient’s antimicrobial treatment should be reviewed on a regular basis. Antibiotic treatment should be stopped as soon as possible, regardless of which antibiotics are used. Pharmacists will undertake regular review of ward stocks and high risk antibiotics should not be stocked on wards with a high proportion of elderly patients. 7.0 Signs and Symptoms of CDI There is a range of presentation within the spectrum of CDI:
a) C. difficile spores can be ingested and excreted without any clinical signs in some patients.
b) An asymptomatic chronic carrier state can occur. c) In cases where symptomatic infection does occur, the severity varies greatly.
Most patients with CDI display symptoms of mild to moderate watery diarrhoea, with or without abdominal pain and an elevated white cell count. This is a result of the toxins damaging the mucous membrane of the large colon (colitis). In some cases diarrhoea might not be present and the patient presents with distension and abdominal pain. A careful assessment is required for sedated and unconscious patients in particular.

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
7
d) A small proportion of patients develop a condition known as pseudo membranous colitis (or PMC). These patients develop frequent, profuse, foul-smelling diarrhoea accompanied by abdominal pain, distension, fever and a raised white cell count. PMC can lead to toxic mega colon and death.
Older age, WBC >20, increased peak serum creatinine, low potassium and low albumin are associated with greater risk of severe CDI. Re-infection is a common cause of recurrence in C. difficile. Recurrent attacks and intractable diarrhoea can complicate cases. Diarrhoea usually starts a few days after commencing antibiotics but can be up to 2 months later. 8.0 Diagnosis of CDI When a patient presents with diarrhoea, the possibility that it may be infectious in origin must be considered where there is no clear alternative cause. A specimen of faeces should be sent to the microbiology laboratory unless a laboratory confirmed positive diagnosis has been made within the previous 4 weeks. Children under the age of 2 years should not have stool samples sent for a C. difficile toxin (CDT) test, as children under this age do not develop CDI due to lack of specific receptors for the toxins.
The diagnosis should be made on: clinical and/or laboratory and/or endoscopic findings. In cases where CDI is suspected and there is no diarrhoea, a specific request should be made for testing a semi-formed or formed stool sample for toxins by the treating doctor.
All patients over the age of 2 years with diarrhoea (a stool sample that takes the shape of the container) should be tested for C. difficile toxins.
In completing the specimen form, it must be clearly stated that testing for C. difficile toxins is required. Any history of antibiotics taken by the patient in the last 6-8 weeks, along with the patient’s present medical history, should be included on the specimen request form. Doctors should consider CDI as a diagnosis in its own right, grading each confirmed case for severity, treating accordingly and reviewing each patient daily, monitoring bowel function using the Bristol Stool Chart (See Appendix 2).
Repeat testing: Clostridium difficile toxins can be excreted in the faeces of patients for weeks so stool samples are not needed following a positive test and clearance of infection is indicated by disappearance of symptoms. If a patient has not had diarrhoea for 48 hours they should be regarded as non-infectious.
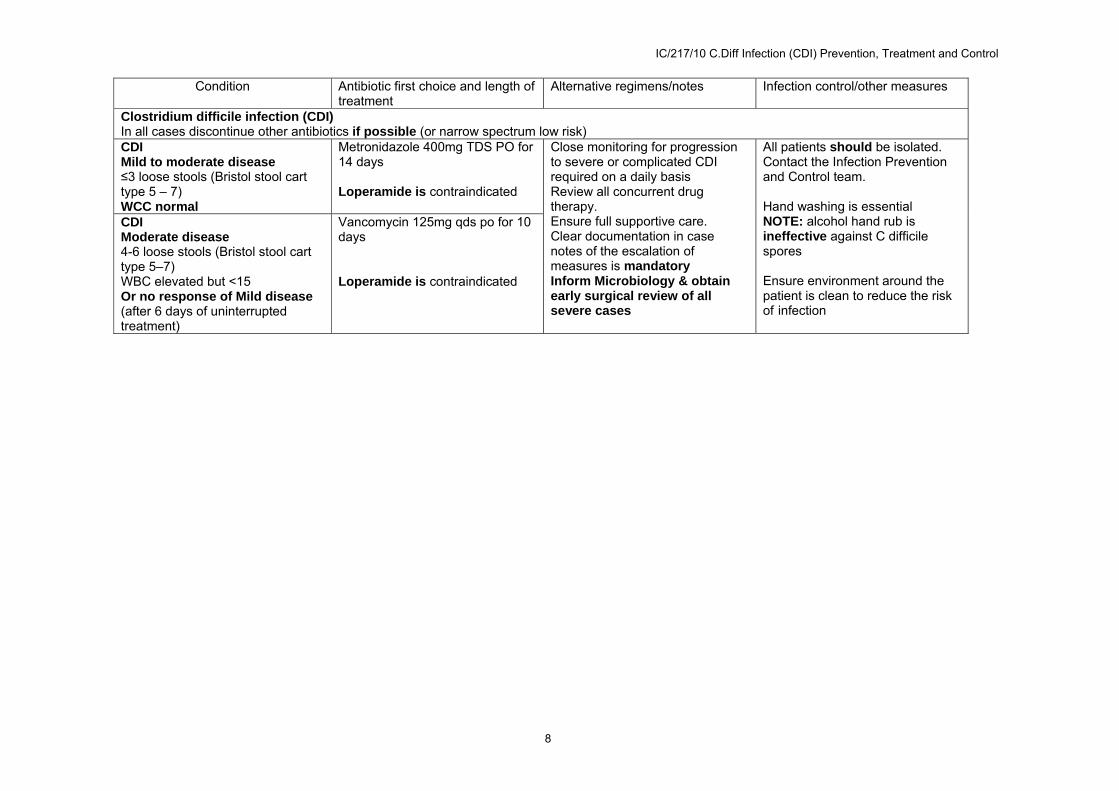
If relapse/re-infection occurs, isolation precautions should recommence. 9.0 Treatment of CDI The first line treatment for Clostridium difficile is to discontinue the offending antibiotic/s that has been prescribed for the patient, if possible. In some cases this may be enough for the normal bowel flora to re-grow and no further intervention is required. The trust antibiotic treatment policy for CDI is as below
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
8
Condition Antibiotic first choice and length of treatment
Alternative regimens/notes Infection control/other measures
Clostridium difficile infection (CDI) In all cases discontinue other antibiotics if possible (or narrow spectrum low risk) CDI Mild to moderate disease ≤3 loose stools (Bristol stool cart type 5 – 7) WCC normal
Metronidazole 400mg TDS PO for 14 days Loperamide is contraindicated
Close monitoring for progression to severe or complicated CDI required on a daily basis Review all concurrent drug therapy. Ensure full supportive care. Clear documentation in case notes of the escalation of measures is mandatory Inform Microbiology & obtain early surgical review of all severe cases
All patients should be isolated. Contact the Infection Prevention and Control team. Hand washing is essential NOTE: alcohol hand rub is ineffective against C difficile spores Ensure environment around the patient is clean to reduce the risk of infection
CDI Moderate disease 4-6 loose stools (Bristol stool cart type 5–7) WBC elevated but <15 Or no response of Mild disease (after 6 days of uninterrupted treatment)
Vancomycin 125mg qds po for 10 days Loperamide is contraindicated
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
9
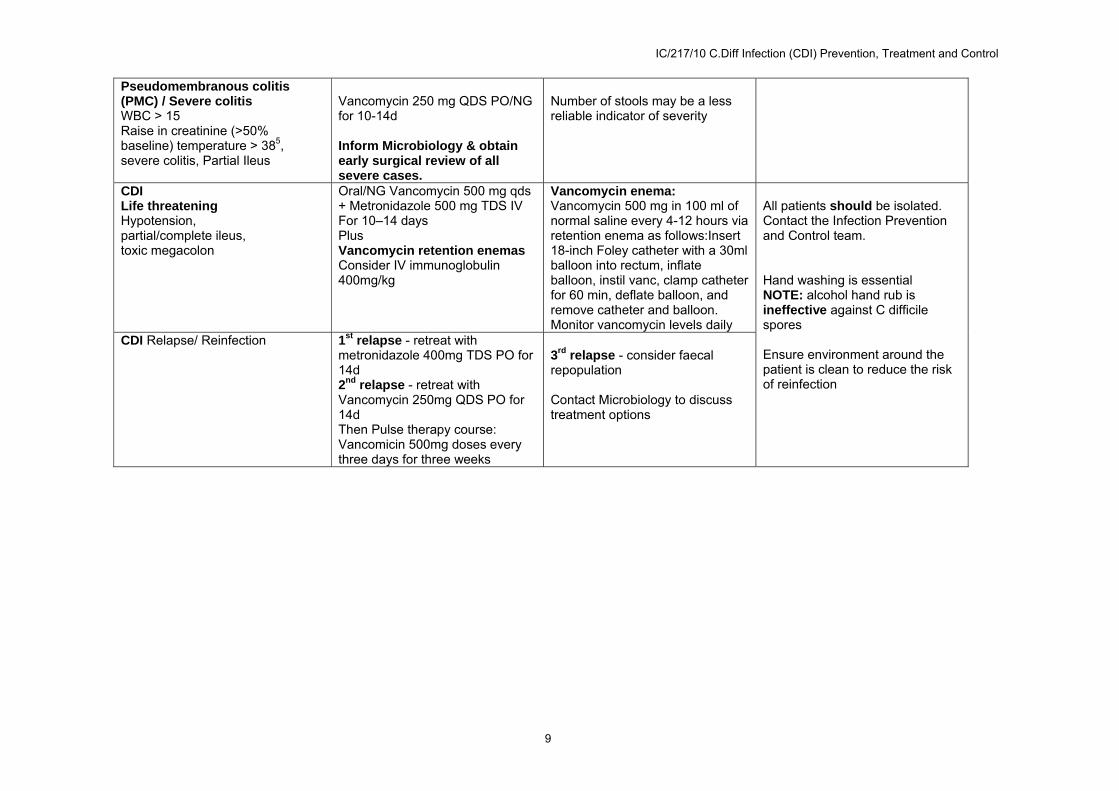
Pseudomembranous colitis (PMC) / Severe colitis WBC > 15 Raise in creatinine (>50% baseline) temperature > 385, severe colitis, Partial Ileus
Vancomycin 250 mg QDS PO/NG for 10-14d Inform Microbiology & obtain early surgical review of all severe cases.
Number of stools may be a less reliable indicator of severity
CDI Life threatening Hypotension, partial/complete ileus, toxic megacolon
Oral/NG Vancomycin 500 mg qds + Metronidazole 500 mg TDS IV For 10–14 days Plus Vancomycin retention enemas Consider IV immunoglobulin 400mg/kg
Vancomycin enema: Vancomycin 500 mg in 100 ml of normal saline every 4-12 hours via retention enema as follows:Insert 18-inch Foley catheter with a 30ml balloon into rectum, inflate balloon, instil vanc, clamp catheter for 60 min, deflate balloon, and remove catheter and balloon. Monitor vancomycin levels daily
All patients should be isolated. Contact the Infection Prevention and Control team. Hand washing is essential NOTE: alcohol hand rub is ineffective against C difficile spores Ensure environment around the patient is clean to reduce the risk of reinfection
CDI Relapse/ Reinfection 1st relapse - retreat with metronidazole 400mg TDS PO for 14d 2nd relapse - retreat with Vancomycin 250mg QDS PO for 14d Then Pulse therapy course: Vancomicin 500mg doses every three days for three weeks
3rd relapse - consider faecal repopulation Contact Microbiology to discuss treatment options

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
10
To prevent CDI consider giving probiotics when starting antibiotics, if not contraindicated. Surgical intervention: In a series of patients who were assessed for the effectiveness of surgical intervention, a serum lactate >5mmol/L was associated with almost 100% mortality. Total or subtotal colectomy is likely to be more effective than hemicolectomy.
10.0 Infection Prevention Measures
It is important that when a patient presents with diarrhoea, the possibility that it may have an infectious cause is considered. Patients with suspected potentially infectious diarrhoea should be isolated in a single room.
Prevention of CDI is mainly through prudent use of antibiotics in patients >65 years of age and infection prevention measures, including patient isolation, hand hygiene, personal protective equipment and environmental cleanliness. Surveillance and feed back of data play a key role in infection prevention and control.
10.1 Prudent use of antibiotics
There is a trust wide antibiotic policy, which promotes prudent use of antibiotics and it is crucial that compliance is ensured. For further information, see under section 6.
10.2 Isolation precautions
• Patients with CDI should be moved to the isolation ward as soon as a side room is available. IF this is not possible the patient should be isolated in a side room with an en suite toilet and hand wash basin. If an en suite is not available then the patient will need a dedicated commode. The room should have Lino flooring not carpet. If isolation is not possible the Site Coordinator must be informed of the situation immediately.
• All patients need to be placed on the C difficile care pathway • All staff anticipating physical contact with the patient or their
equipment/environment must wear a plastic apron and gloves when entering the room. Gloves must be changed and hands washed between ‘dirty’ and ‘clean’ procedures on the patient. Gloves do not obviate the need to wash hands. Following use, PPE must be disposed of in a clinical waste bag before leaving the room and hands must then be washed. Hands must be washed with soap and water following contact with the patient and removal of gloves.
• Alcohol hand rub must not be used as an alternative to soap. It can be applied after washing to rid hands of remaining non-clostridial organisms.
• All patients must be offered the opportunity to wash their hands or use a hand wipe after using the toilet/commode and before meals. They should be informed about the importance of hand hygiene while in hospital, particularly before hand to mouth contact. Patients unable to perform hand hygiene themselves should be assisted by a healthcare worker.
• Visitors should be asked to wash their hands using soap and water on entering and leaving the patient’s room. They do not need to wear protective clothing unless assisting with the patient’s physical care, but should refrain from sitting on the bed.

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
11
• Open food e.g. fruits should be removed from affected areas immediately and visitors stopped from bringing in any foods.
• Crockery and cutlery can be used as long as it goes through a hot dishwasher cycle.
• Used disposable bedpans must be removed from the room and placed in the macerator.
• Bed linen should be changed daily. All used linen should be regarded as infected and handled as per the Linen Policy.
• Whenever possible, a patient with suspected/confirmed CDI should have designated equipment and in particular, a designated toilet/commode.
• All waste leaving the room must be classed as clinical waste and disposed of in a yellow bag.
• The patient may undergo essential investigations and treatment including physiotherapy and occupational therapy. A risk assessment must be undertaken by the staff involved. Staff should ensure that all relevant members of the multidisciplinary team are kept informed concerning the patient’s condition.
10.3 Environmental cleaning: (to be read in conjunction with the Trust’s cleaning standards manual)
• It is the responsibility of all clinical staff to ensure adequate environmental hygiene in clinical areas, especially around infected patients. The patient care environment acts as a reservoir for C. difficile spores and thorough cleaning of all surfaces is essential.
• Cleaning frequency must be increased to three times a day using ‘Actichlor Plus’ (general purpose detergent combined with hypochlorite solution) at a strength of 1000ppm (one 1.7G tablet diluted in one litre of warm water). The nurse in charge is responsible for ensuring that increased cleaning using ‘Actichlor Plus’ is requested from domestic services.
• Toilets/commodes need special attention and must be decontaminated after use by a patient with diarrhoea. Ideally, the patient will have a designated toilet/commode and this should be cleaned after each use and disinfected when soiled. Before use by another patient, commodes must be decontaminated using ‘Actichlor Plus’ and indicator tape applied to confirm readiness for re-use. A protective visor/goggles must be worn in addition to an apron and gloves when using ‘Actichlor Plus’ to clean toilets/commodes.
• When a room/area is about to reopen: a deep clean should be undertaken. Curtains and linen should be removed before cleaning and sent to be laundered as clinical laundry in a hot wash cycle. All surfaces and equipment must be decontaminated thoroughly using ‘Actichlor Plus’ at 1000ppm strength (one 1.7G tablet diluted in one litre of warm water) or as per manufacturer’s recommendations.
• Steam cleaners are also effective and can be used (see Trust Cleaning Standards Manual).
• Ward areas/side rooms should not reopen without the cleaning standard being checked by the senior nurse responsible for that area.
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
12
10.4 Surveillance
• Surveillance of CDI is carried out routinely by the Infection Prevention and Control Team as part of the surveillance programme
• CDIs are reported to the Department of Health through an enhanced surveillance system
• All outbreaks of infection are reportable as a serious untoward incident using a specially designed form
• Clinical staff should review their practice supported by the IPCT and through use of the DH (2006) High Impact Intervention No. 6: Reducing the risk from and presence of Clostridium difficile.
• Surveillance data is fed back to all senior and general managers and clinical teams within the Trust.
• Root cause analysis is performed on all hospital-acquired CDI cases, action plans created and key findings fed back to senior and general managers and clinical teams within the Trust.
• The local health authority is responsible for setting up annual targets for reduction of infections and monitoring progress.
11.0 Patient information Patients and relatives must be provided with appropriate information. The Trust has a question and answer fact sheet or www.hpa.org.uk has information that can be used. ‘A Simple Guide to Clostridium difficile’ DH 2006 is available from www.dh.gov.uk/hcai 12.0 Outbreak Control
The definition of periods of increased incidence or an outbreak is as follows:
A period of increased incidence (PII) of CDI: two or more new cases (occurring >48 hours post admission, not relapses) in a 28-day period on a ward. An outbreak of C. difficile diarrhoea: two or more cases caused by the same strain related in time and place over a defined period that is based on the date of onset of the first case. The following actions are to be taken if a PII is identified on a ward (see Figure 1):
i. Urgently inform the clinical director, matron, ward manager and directorate manager.
ii. Conduct a weekly C. difficile ward audit using the Department of Health’s C. difficile High Impact Intervention (HII) tool by infection control nurse or infection control doctor to continue until the weekly score is >90% in three consecutive weeks and there have been no further >48 hours cases of CDI on the ward during that period. Feed back the audit results to the matron or ward manager.
iii. Carry out a weekly antibiotic review in each ward, (using local tools); this is the responsibility of the antibiotic pharmacist.
iv. Clean the whole ward with chlorine-containing agent until no further symptomatic patients are present on the ward. Emphasise that each bed space needs to be cleaned separately with separate cloths.

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
13
v. Use HPA CDRNE or CfI to undertake PCR ribotyping of all isolates from patients in the ward.
vi. The ICT should carry out an automatic review of ward PIIs each week. vii. An incident meeting should be held as determined by the size and rate of growth
of the PII by assessment of the situation by the DIPC and/or the duty microbiologist with the clinical director and consultants.
Figure 1:

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
14
OUTBREAKS
An outbreak will be managed as per the trust outbreak policy
In these cases it may be necessary to cohort the patients into the same bay/ward and initiate isolation precautions. If this occurs staff must:
• Inform the Infection Prevention and Control team about the outbreak • Draw up a list of all affected patients and update each shift • Stool samples must be sent from all patients with symptoms of diarrhoea • If single rooms are not available then the patients may be cohort nursed in a bay.
The doors must be kept closed or screens used if doors are not available. • The area must be scrupulously decontaminated three times a day using
‘Actichlor Plus’ (general purpose detergent combined with hypochlorite solution at 1000ppm strength (one 1.7G tablet diluted in one litre of warm water)
• The affected bay/ward should be closed to all admissions and transfers to other areas within the hospital or other hospitals, unless approved by a consultant microbiologist.
• Isolation precautions apply and must be adhered to at all times. • All staff entering the area MUST wear an apron and gloves for physical contact
with the patient or their equipment/environment. PPE must be changed between patients and between different tasks on the same patient. PPE must be disposed of and hands washed before leaving the infected area
• Isolation precautions MUST continue until ALL infected patients have been free from diarrhoea for 48 hours
• Hospital staff and visitors are at little risk of catching the illness themselves • Patient movement between units increases the risk of the outbreak spreading to
other units/wards. This is because information about diarrhoea may not be highlighted on transfer therefore, delaying isolation precautions and/or diagnosis.
13.0 Death Certification
• If a patient with CDI dies, the death certificate should state whether CDI was part of the sequence of events leading directly to death or whether it was the underlying cause of death. If either case applies CDI should be mentioned in Part 1 of the certificate.
• If CDI was not part of the sequence of events leading directly to death but contributed in some way to it, this should be mentioned in Part 2.
• If a doctor is in doubt about the circumstances of death when writing the certificate, they should consult with the trust’s multidisciplinary clinical review team for CDI. Doctors have a legal duty to mention CDI on a death certificate if it was part of the sequence of events directly leading to death or contributed in some way. B
• Medical directors should ensure that training is provided on death certification and should audit certificates to check that they accurately record HCAI.
B#
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
15
14.0 Infection Prevention and Control Contacts Dr N Hutchinson, Consultant Microbiologist/Infection Control Doctor Ext 3310 Dr F El Bakri, Consultant Microbiologist Ext 3305 Dr Jorge Cepeda, Consultant Microbiologist Ext 3308
Hazel Gray, Senior Infection Control Sister Ext 6774 or bleep 2364
Linda Swanson, Infection Control Sister Ext 6774 or bleep 2364
Bruce Wake, Trust Surveillance Co-ordinator Ext 6774 or bleep 2433
Taryn Keyser, Antibiotic Pharmacist Ext 3340 or bleep 2435 15.0 References Boyce JM and Pittet D (2002). Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HIPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Healthcare Infection Control Practices Advisory Committee. HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. American Journal of Infection Control, 30(8):S1-46, 2002 Dec. Chief Medical Officer (2007). Healthcare Associated Infections and Death Certification. PL CMO (2007)8. www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/Professionalletters/Chiefmedicalofficerletters/DH_079104 Chief Medical Officer/Chief Nursing Officer (2008). Changes to the mandatory healthcare associated infection surveillance system for Clostridium difficile infection (CDI) from 1st January 2008. PL CMO (2008)1. www.dh.gov.uk/en/Publicationsandstatistics/Lettersandcirculars/Professionalletters/ Chiefmedicalofficerletters/DH_082107 Commission for Healthcare Audit and Inspection (2006). Investigation into outbreaks of Clostridium difficile at Stoke Mandeville Hospital, Buckinghamshire Hospitals NHS Trust. www.healthcarecommission.org.uk/_db/_documents/Stoke_Mandeville.pdf Department of Health and Health Protection Agency (January 2009). Clostridium difficile infection: How to deal with the problem. London. Department of Health (2007). Saving Lives: Reducing infection, delivering clean and safe care. High Impact Intervention No 7. Care bundle to reduce the risk from Clostridium difficile. London: Department of Health. www.clean-safe care.nhs.uk/toolfiles/79_SL_HII_7_v2.pdf Department of Health (2007). Saving Lives: Reducing infection, delivering clean and safe care – Antimicrobial prescribing. London: Department of Health. www.clean-safe-care.nhs.uk/toolfiles/104_281812ANT_antimicrobial_pres.pdf

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
16
Department of Health (2007). Saving Lives: Reducing infection, delivering clean and safe care – Isolating patients with healthcare-associated infection. London: Department of Health www.clean-safe-care.nhs.uk/toolfiles/116_283198IP_isolating_patients.pdf Department of Health (2008). The Health and Social Care Act 2008: Code of practice for the NHS on the prevention and control of healthcare associated infections and related guidance. London: Department of Health. www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_093762 Healthcare Commission (2006). Management, Prevention and Surveillance of Clostridium difficile: Interim findings from a national survey of NHS acute trusts. London: Healthcare Commission/Health Protection Agency. www.healthcarecommission.org.uk/_db/_documents/Management_prevention_ Clostridium_difficile_200608145413.pdf McFarland LV, Beneda HW, Clarridge JE et al (2007). Implications of the changing face of Clostridium difficile disease for health care practitioners. American Journal of Infection Control, 35: 237-253. Wilcox MH, Mooney L, Bendall R et al. (2008). A case-control study of community associated Clostridium difficile infection. J Antimicrobial Chemotherapy, 62(2): 388-396.
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
17
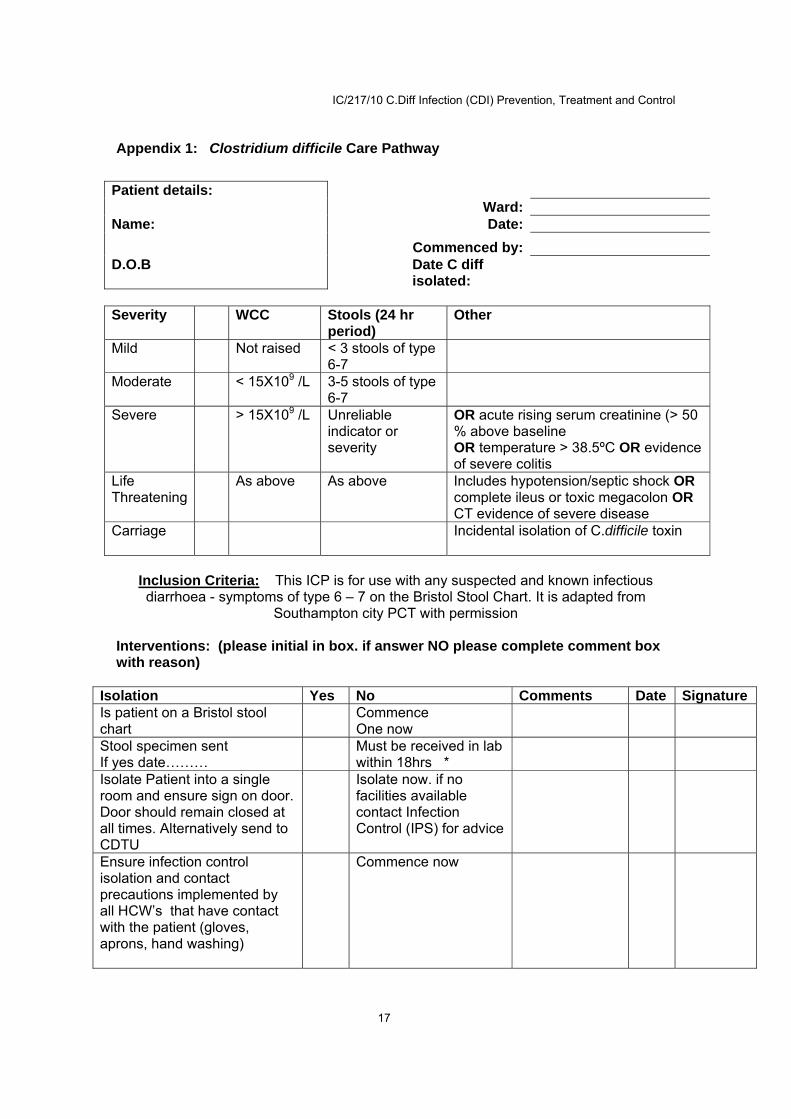
Appendix 1: Clostridium difficile Care Pathway
Patient details: Ward: Name: Date: Commenced by: D.O.B Date C diff
isolated:
Severity WCC Stools (24 hr
period) Other
Mild Not raised < 3 stools of type 6-7
Moderate < 15X109 /L 3-5 stools of type 6-7
Severe > 15X109 /L Unreliable indicator or severity
OR acute rising serum creatinine (> 50 % above baseline OR temperature > 38.5ºC OR evidence of severe colitis
Life Threatening
As above As above Includes hypotension/septic shock OR complete ileus or toxic megacolon OR CT evidence of severe disease
Carriage Incidental isolation of C.difficile toxin
Inclusion Criteria: This ICP is for use with any suspected and known infectious diarrhoea - symptoms of type 6 – 7 on the Bristol Stool Chart. It is adapted from
Southampton city PCT with permission Interventions: (please initial in box. if answer NO please complete comment box with reason)
Isolation Yes No Comments Date Signature Is patient on a Bristol stool chart
Commence One now
Stool specimen sent If yes date………
Must be received in lab within 18hrs *
Isolate Patient into a single room and ensure sign on door. Door should remain closed at all times. Alternatively send to CDTU
Isolate now. if no facilities available contact Infection Control (IPS) for advice
Ensure infection control isolation and contact precautions implemented by all HCW’s that have contact with the patient (gloves, aprons, hand washing)
Commence now
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
18
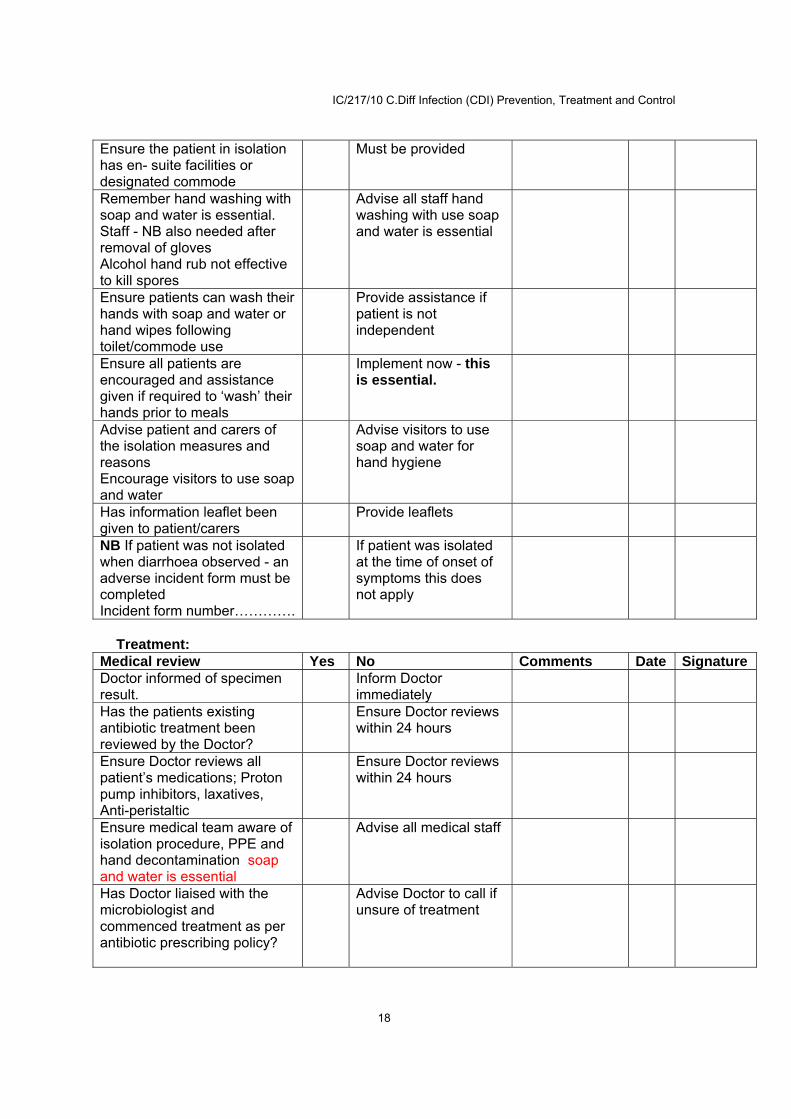
Ensure the patient in isolation has en- suite facilities or designated commode
Must be provided
Remember hand washing with soap and water is essential. Staff - NB also needed after removal of gloves Alcohol hand rub not effective to kill spores
Advise all staff hand washing with use soap and water is essential
Ensure patients can wash their hands with soap and water or hand wipes following toilet/commode use
Provide assistance if patient is not independent
Ensure all patients are encouraged and assistance given if required to ‘wash’ their hands prior to meals
Implement now - this is essential.
Advise patient and carers of the isolation measures and reasons Encourage visitors to use soap and water
Advise visitors to use soap and water for hand hygiene
Has information leaflet been given to patient/carers
Provide leaflets
NB If patient was not isolated when diarrhoea observed - an adverse incident form must be completed Incident form number………….
If patient was isolated at the time of onset of symptoms this does not apply
Treatment:
Medical review Yes No Comments Date Signature Doctor informed of specimen result.
Inform Doctor immediately
Has the patients existing antibiotic treatment been reviewed by the Doctor?
Ensure Doctor reviews within 24 hours
Ensure Doctor reviews all patient’s medications; Proton pump inhibitors, laxatives, Anti-peristaltic
Ensure Doctor reviews within 24 hours
Ensure medical team aware of isolation procedure, PPE and hand decontamination soap and water is essential
Advise all medical staff
Has Doctor liaised with the microbiologist and commenced treatment as per antibiotic prescribing policy?
Advise Doctor to call if unsure of treatment

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
19
Ensure the patient’s fluid balance and electrolytes are monitored. NB Fluid balance chart required If bloods taken enter date here…………..
Ensure patient’s fluid balance is reviewed daily Commence fluid chart
Has the doctor prescribed electrolyte replacement medication - Diorolyte
Ensure doctor prescribes this medication
Cleaning:
Housekeeping Yes No Comments Date Signature Have team been advised of need for enhanced isolation cleaning three times daily
Advise housekeeping immediately
Designated bucket and mop &/or disposable cloths
Ensure relevant equipment is obtained
If patient has been moved to isolation room after experiencing symptoms ensure previous bed space is deep cleaned and curtains changed before being re occupied. Use enhanced cleaning using hypochlorite solution
Ensure bed space is cleaned prior to new occupant
Staff: Yes No Comments Date Signature Staff aware of need to clean toilet facilities or commode following each bowel action and wipe over with hypochlorite ‘1000’ppm solution twice a day or as per advice
Ensure cleaning is undertaken.
Designated /single use equipment should be available for patient in isolation e.g. slings NB If not possible ensure item cleaned as above before using with another patient eg hoists, blood pressure monitors
Designated or single use slings must be available Equipment removed from the room must be cleaned with soap and water, and the wiped over with hypochlorite solution.

IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
20
Transfer or discharge:
Planning Yes No Comments Date Signature Has receiving ward or ward at transfer hospital been informed of infective diarrhoea status?
Ensure receiving staff aware, including treatment given and when patient last symptomatic
Has the patient been 48 hours free of symptoms and passed a normal stool?
Patient should not be transferred
Has the Nursing or Rest home been informed of infective diarrhoea status?
Ensure receiving staff aware, including treatment given and when patient last symptomatic
Has the patient’s GP/district nurse been informed?
Ensure handover of patient’s care includes treatment given/ongoing and current status
A patient can be transferred to another hospital, or nursing home if they have been 48 hours free of symptoms.
Terminal Clean Post Discharge/Transfer Yes Date Signature Pathway discontinued
Housekeeping has been informed of the need for the single room/bay to have a deep thorough clean and curtains to be changed. See isolation policy
Ensure all pieces of patient equipment in isolation room have been decontaminated as discussed above.
IC/217/10 C.Diff Infection (CDI) Prevention, Treatment and Control
21
Appendix 2: Bristol Stool Chart