clips word template -...
TRANSCRIPT
CHCPA301B Deliver care services using a palliative approach
Reading 5: Respond to signs of pain and other symptoms/discomfort
1© NSW DET 2009
Contents
Reading 5: Respond to signs of pain and other symptoms/discomfort 3
Introduction 3Observe client closely and identify pain and other symptoms in line with care plan directives 3Document observations of pain and other symptoms and promptly report to appropriate member of care team 5Implement strategies to promote comfort in line with care plan 7Regularly evaluate and document effectiveness of implemented strategies 9Refer to appropriate member of staff any misconceptions in the workplace surrounding the use of pain relieving medication 10
2© NSW DET 2009

Reading 5: Respond to signs of pain and other symptoms/discomfort
IntroductionWhen a person is at the end of his/her life and cure is unlikely, as carers we can offer him/her strategies which will minimise pain and other symptoms, such as anxiety, constipation, dyspnoea (difficulty breathing) and restlessness. This reading will show you how to assess and manage these symptoms so that your client is not distressed by them. The focus of this reading is the assessment of pain in both the verbal and non-verbal client through the use of specially designed assessment tools.
Observe client closely and identify pain and other symptoms in line with care plan directivesElderly people may be reluctant to report pain because they believe that having some pain is just a normal part of growing old. It isn’t! Untreated pain can lead to depression, decreased socialisation, decreased mobility, impaired ability to undertake personal tasks such as showering and toileting, and sleep disturbances. Pain is the most common symptom of a person who is in the terminal phase of life, regardless of the underlying disease. Pain is managed best by a process of assessment, intervention using an array of drug and non-drug therapies, and evaluation of the effectiveness of these.
Pain is common in older people and some studies have shown that 20% of older people take some medication for pain, usually for arthritis, bone and joint problems, back problems and other chronic conditions. Pain is common amongst residents of aged care facilities and often is untreated because of the high prevalence of dementia, sensory problems and disability in this population which makes assessment and management more difficult.
There are three basic categories of pain:
3© NSW DET 2009
1. Nociceptive pain may arise from tissue inflammation, mechanical deformation such as fractures, ongoing injury and destruction such as in arthritis or ischaemic disorders. These usually respond well to traditional approaches to pain management including common analgesic medications and non-pharmacologic strategies such as heat/cold therapy.
2. Neuropathic pain results from a process that involves the peripheral or central nervous system. Examples are diabetic neuropathy, post-amputation phantom limb pain, and neuralgia from herpes zoster (shingles). These problems do not respond predictably to conventional analgesics, but do respond to tricyclic antidepressants, anticonvulsants, or antiarrhythmic drugs.
3. Mixed or unspecified pain may have unknown mechanisms such as recurrent headaches. Treatment for this type of pain may require trials of different approaches.
Pain management is most successful when the underlying cause is identified and treated.
Pain is a subjective symptom and the most accurate evidence of pain is based on the individual’s description and self-reports.
A person who can describe the pain may say it is aching, burning, heaviness, sharp, ‘pins and needles’, tingling or tightness.
A person who is cognitively impaired eg from dementia, or who has communication difficulties eg from a stroke, may present with agitation, restlessness, changes in facial expressions such as frowning or grimacing, or making noises such as crying, groaning, and moaning.
There are a number of excellent pain assessment tools which can be used eg
The Functional Pain Scale (FPS).
The Numerical Rating Scales (NRS) where numbers are used to represent the strength of the pain where 0 represents no pain and 10 represents unbearable pain.
The Brief Pain Inventory (BPI).
The FACES Scale which has a number of faces drawn on its scale from a smiley face to a crying face. This is useful for people who cannot verbalise their pain.
Abbey Pain Scale. This is an Australian developed tool for people with dementia.
Pain Assessment in Advanced Dementia (PAINAD) Scale. Another useful tool for carers to assess pain in people with dementia.
For a descriptions of these and other pain scales, go your ‘My briefcase’ or to Geriatric Assessment Tools: Pain by Iowa Geriatric Education Center at:
4© NSW DET 2009

http://www.healthcare.uiowa.edu/igec/tools/categoryMenu.asp?categoryID=7
Other symptoms to be aware of are:
oral discomfort due to dehydration.
weakness and fatigue
dyspnoea (difficulty breathing)
anxiety and restlessness
constipation due to nutritional deficit and/or pain medication
anorexia (lack of appetite)
skin integrity problems due to the client becoming bed-bound, wound breakdown, oedema of limbs
nausea and/or vomiting.
Document observations of pain and other symptoms and promptly report to appropriate member of care teamWhenever you become aware of changes in symptoms, including pain, it is important that these are assessed, documented and reported according to the policies and practices of the organisation. Your organisation will have various methods of assessment and documentation of symptoms such as:
fluid balance charts to assess hydration
food intake charts to assess anorexia
bowel charts for assessment of daily bowel function
wound charts which identify breakdown in the skin and any infection
skin integrity charts which assess whether the client needs to be turned every two hours and/or have a special mattress which uses alternating air pressure to support different areas of the body or be nursed on a medical sheepskin.
When a symptom is recognised in your client, assessment of the symptom should take place. This should then be transferred to the client’s care plan and strategies developed to minimise the effects of the symptom. Implementation of these strategies occurs until they are reassessed for their success. If reassessment shows that the strategies have not been successful, then new strategies are tried.
5© NSW DET 2009
Case study
Mrs Bobbin had a stroke in the past week. Her general condition is poor and her family have been told that she will live only a few days. Mrs Bobbin has fragile skin which has already become reddened on her sacral area. Mrs Bobbin is incontinent of urine and faeces, cannot speak and has difficulty swallowing. The speech therapist has ordered only thickened fluids if Mrs Bobbin can tolerate them. Mrs Bobbin’s care plan should reflect her changed condition.
Care Plan Mrs. Bobbin
Need/Issue Goal Strategy Evaluation
Inability to swallow solids.
To provide whatever hydration is possible.
Offer level 2 thickened fluids by teaspoon, with resident sitting upright. Cease if gagging.
29/10/2009:
Mrs Bobbin continues to take small amounts of thickened fluids.
2/11/2009:
Mrs Bobbin is unconscious and cannot swallow thickened fluids. Cease giving fluids.
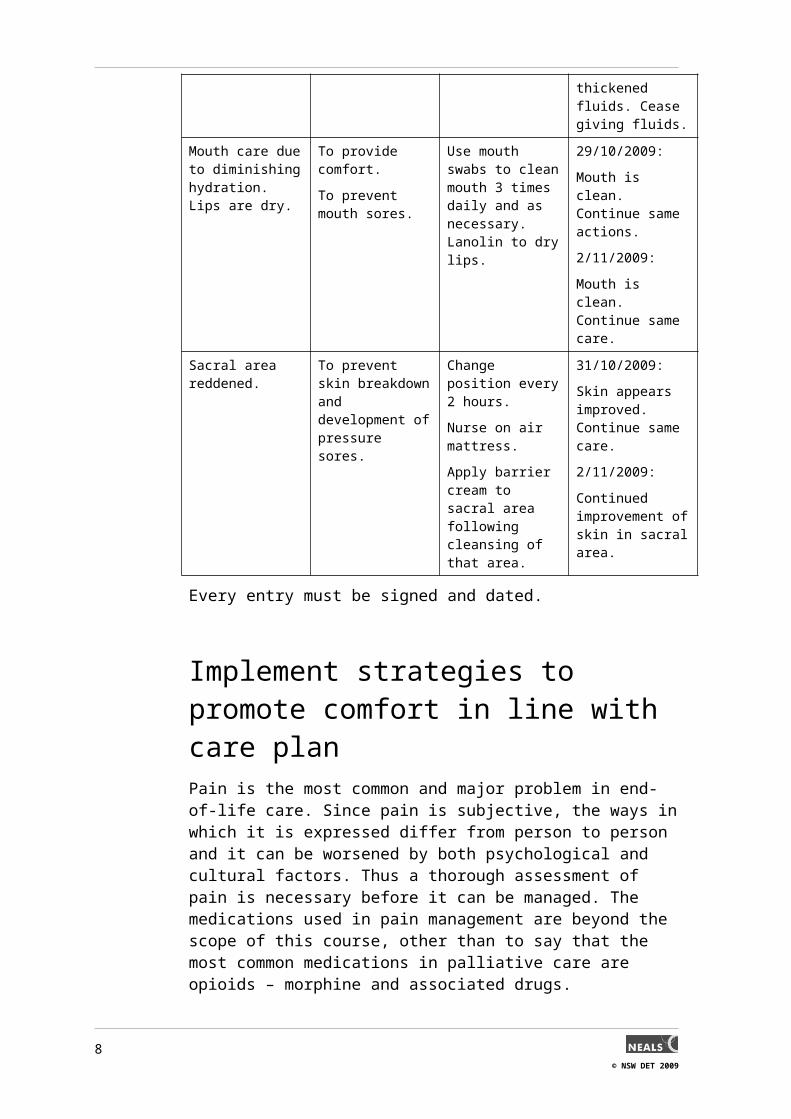
Mouth care due to diminishing hydration. Lips are dry.
To provide comfort.
To prevent mouth sores.
Use mouth swabs to clean mouth 3 times daily and as necessary. Lanolin to dry lips.
29/10/2009:
Mouth is clean. Continue same actions.
2/11/2009:
Mouth is clean. Continue same care.
Sacral area reddened. To prevent skin breakdown and development of pressure sores.
Change position every 2 hours.
Nurse on air mattress.
Apply barrier cream to sacral area following cleansing of that area.
31/10/2009:
Skin appears improved. Continue same care.
2/11/2009:
Continued improvement of skin in sacral area.
Every entry must be signed and dated.
6© NSW DET 2009

Implement strategies to promote comfort in line with care planPain is the most common and major problem in end-of-life care. Since pain is subjective, the ways in which it is expressed differ from person to person and it can be worsened by both psychological and cultural factors. Thus a thorough assessment of pain is necessary before it can be managed. The medications used in pain management are beyond the scope of this course, other than to say that the most common medications in palliative care are opioids – morphine and associated drugs.
One of the major considerations in using opioids in the elderly is the difference in the way the drug is used by the body from that of a young person. Liver and kidney function in the elderly is reduced which causes opioids to accumulate in the plasma and have a higher chance of side-effects. Opioids also affect the central nervous system which is altered with age, resulting in an increased risk of side effects.
As a result of coexisting disease, the elderly often take a number of other medications which can interact with opioids causing adverse reactions. In summary, use of opioids in the elderly requires caution and regular review.
If a person is experiencing mild pain, it is recommended that non-opioid analgesia such as paracetamol is given on a regular basis, such as four times daily. The side effects of paracetamol are minimal and it is generally effective in mild pain. The next step for pain is a mild opioid such as codeine, which is about one-tenth as powerful as morphine. The third step is the use of a strong opioid such as morphine. These three steps are recommended by the World Health Organisation.
Morphine can be given in a number of forms including tablets and liquid, injection, and via patches on the skin. Signs of morphine toxicity include drowsiness, hallucinations, and confusion.
When the person is approaching death and is unable to swallow, morphine and other drugs may be given via a syringe driver which is a battery operated pump which provides a stated amount of medication continuously via a needle which is placed under the skin.
7© NSW DET 2009
Photograph of a syringe driver
Syringe driver
However, there are a number of non-drug therapies where you can assist the client to be more comfortable. You should read the care plan and discuss comfort strategies with your supervisor before undertaking them. The client will gain much support from your reassuring tone of voice, gentle touch and time spent with him/her and these will assist with comfort.
Non-drug strategies for pain relief may be:
change of position – place pillows between knees, behind back and front
gentle massage of sore areas
heat or cold packs
physiotherapy
hypnosis (by a qualified psychologist)
relaxation techniques
acupuncture
transcutaneous electrical nerve stimulation (tens) machine
distraction techniques such as music.
Shortness of breath can be frightening for both the client and the family members. Dyspnoea (shortness of breath) can be due to medical problems,
8© NSW DET 2009
psychological issues such as anxiety, or poor lung function from the disease process.
Comfort strategies for the person experiencing dyspnoea are:
oxygen is a great comfort to people who are short of breath and takes away the feeling of suffocation
sitting upright supported by pillows helps with breathing
verbal reassurance is important.
One of the most remarkable aspects of the dying process is the loss of appetite and weight loss that many people experience. This has an effect on the morale of the family members who may demand that the dying person be fed or given fluids beyond his/her ability to swallow. They may say that the person is ‘starving to death’ and demand that they be hospitalised for artificial feeding. Research has shown that a person who is dying does not experience hunger and thirst.
Comfort strategies for the person experiencing anorexia and dehydration are:
If a person is still capable of eating, he/she should be offered food that he/she enjoys. Ice-cream and ice-blocks soothe a sore mouth and are easily swallowed.
Keeping the mouth clean and moist is essential. Lanolin to lips can be applied. Lips can be moistened with ice chips.
Anxiety and restlessness are common as clients face their fears and concerns about their impending death. Poorly managed symptoms such as pain, constipation, anorexia and dyspnoea can cause anxiety and restlessness. The focus should be on managing these symptoms well and providing good communication with the client and family.
Regularly evaluate and document effectiveness of implemented strategiesIt is necessary to regularly evaluate whether or not strategies for symptom relief are working as they should. Verbal communication with the client, observation of facial expressions, movement, respirations etc, as well as asking family members for their observations of the client will inform the carer of symptom relief. These observations should be documented and, if necessary, new strategies put in place.
If the strategies for symptom management are not successful, think about what might be contributing to the symptoms eg pain may be worsened by anxiety or by lying in the same position. Constipation may be a result of the
9© NSW DET 2009

opioids given for pain management and inadequate fluid intake. Anorexia may be caused by poor oral hygiene leading to sores or thrush in the mouth. Each of these can be managed effectively.
Strategies which are trialled should be added to the care plan, written in client’s progress notes and in the staff communication book, depending on the protocols in your organisation. Discussions at staff shift handover on strategies which work are ideal, as everyone then has an opportunity to discuss quality care for the client.
Refer to appropriate member of staff any misconceptions in the workplace surrounding the use of pain relieving medicationThe management of pain is just one aspect of palliative care which addresses the broad goal of the relief of suffering. One barrier to good pain management at the end-of-life occurs when there are misconceptions about the use of opiates (the morphine group of drugs). Sometimes a family member may not want these to be used, because they have the belief that by doing so, the person is being euthanised.
The use of opioids (the morphine group of drugs) for non-cancer pain is becoming more acceptable. True drug addiction in older patients is rare, and not a reason for failing to use opioids to relieve pain. Research which asked carers, patients and health professionals about their concerns over commencing and continuing the use of morphine and other opioids, found that the introduction of morphine is seen as representing worsening disease and death. It is seen as the last resort in the disease process. Terms used to describe the commencement of morphine were ‘a death sentence’, ‘hastening death’ and having a strong stigma associated with its use.
When health professionals administer pain medications and other palliative therapies for the dying patient, the intent is explicitly on relief of symptoms, even if the possibility exists that such treatments could hasten death. Communication with the family must stress this goal. Teamwork between nurses, doctors, patients, and their care workers is crucial to successful management of pain.
10© NSW DET 2009