clinicalsurvivalguide-2012-2013
TRANSCRIPT
ACADEMIC SOCIETIESFostering Professionalism and Instilling Pride...
Clinical Survival Guide2012-13
10th Edition

Copyright © 2005 by The Miller School of Medicine at the University of Miami Academic Societies
All rights reserved
Printed in the United States of America
Editors
Kevin Kadakia Class of 2013
Academic Societies Executive Staff 2012-2013
Academic Societies Clinical Survival Guide
10th Edition

Table of Contents
CHAPTERS:
Professionalism .............................................................................................ii
1. General Information..............................................................................................1
2. Systems to Know Before You Begin........................................................3
3. The In-Patient Wards.......……………………………………………….4
4. Writing Notes and Presentations............................................................................6
5. Family Medicine/GPC......……………………………………………………….8
1. OB/GYN………………………………………………………………….10
6. Pediatrics…………………………………………………………………..13
7. Internal Medicine ………………………………………………………….14
8. Surgery ............................................................................................................16
9. Neurology ........................................................................................................19
10.Psychiatry ........................................................................................................21
APPENDICES:
A. Important Locations...........................................................................................23
B. Clerkship Coordinators and Phone/Address Info……………………24
C. General Important Phone #s………………………………………………...25
D. Sample Notes……………………………………………………………….26
E. Oral Presentation Pearls……………………………………………………...31
F. Recommended Books ……………………………………………………...32
G. CXR……………………………………………………………………...33
H. Reading EKG‘s ……………………………………………………………34
I. Lab Values…………………………………………………………………36
J. Fluids, Electrolytes, and TPN ..................................................................38
K. Pediatric Tables……………………………………………………………...40
L. H&P Review………………………………………………………………41
M.Patient Record Sheets………………………………………………………43
N. Important Forms in Jackson
History and Physical Form........................................................................1
Order Form………………………………………………………………3
Parenteral Nutrition Order Form…………………………………………4
PCA Order Form........................................................................................5i

IV Antibiotics Form……………………………………………………...7
Insulin Administration Order Form…………………………………….9
Respiratory Treatment Order Form…………………………………...11
Consent for Procedure Form…………………………………………...12

Preface Professionalism
To the Class of 2014:
Congratulations! You have successfully passed the formidable challenges of your first 2 years, endured the torture of the USMLE step 1, and are now ready to officially don your white coat in the bold new role of CC-3! The years ahead of you will be filled with new challenges as you transition from student to professional. You will need to preserve the skills that helped you persevere through your first 2 years, while acquiring new talents to help you function as a valuable member of a medical team. Learning to be a team player is essential to the steep learning curve present throughout your third and fourth years and the lesson will remain worthwhile throughout your professional career.
You may find yourselves working with classmates who you feel lack these all important interpersonal skills. When faced with the pressures of performance, many of us feel that we must impress the house staff, even if this means inconveniencing our fellow students or diminishing them in the eyes of others. All of us have made certain sacrifices to get where we are. Success is important to all of us; we demand it of ourselves. However, the reality is that being a team player will make you look better to those who are evaluating you.
Learning to be a team player requires that you respect your colleagues and superiors. Additionally, don‘t forget to respect the most important teachers you will encounter on the wards—the patients! These individuals literally trust you with their lives on a daily basis and this trust deserves incredible respect. Treating even the most difficult patient is a privilege, not a right. As such, it is our duty to respect the rights and privacy of these individuals.
Here are just a few common sense tips:
1. Do not pre-round on other students‘ patients unless asked to do so by that student. This is often regarded as an attempt to make that other student look bad during ward rounds.
2. Do not jump on the questions asked by attendings to your fellow students unless cued to do so by the attending or that student.
3. If you want to round with the resident at the end of the day, make sure you invite your teammates; they may or may not choose to attend. Likewise if you are privy to knowledge about a change in the schedule of morning rounds, make sure you let your teammates know.
4. Share computers equally. Some floors have a limited number of HIS equipped terminals. Also, if a student needs just a single lab value, it is nice to offer to look it up for them while you are still logged on.
Remember above all to use common sense and follow common courtesy. Take some time to think about your behavior on the wards. Think to yourself, ―Is this the way I would want my teammates to act? Everyone will be looking forward to a learning curve when they get on the wards. Make it easier on yourself and others by being a good team member and your 3rd year will be a lot more enjoyable and a lot less stressful.
We know you all will do a great job and we look forward to working with you as fellow team members on your upcoming rotations! If you ever have any questions, feel free to use the upperclassmen as a resource—we‘ve been there and we‘d love to make the experience easier for you however possible. Remember, your academic society is built to help you throughout medical school—turn to your upperclassmen for advice and pass on your pearls to the classes below you. Enjoy your clinical experiences and good luck!
ii

Getting around the hospital : Each clinical rotation will take you to a different part of the hospital. While it is not necessary to know your way around the entire hospital on your first day, there are some places that you should be able to locate regardless of clerkship including the main radiology reading room and the all-important cafeteria. In Appendix A is a list of important locations throughout JMH.
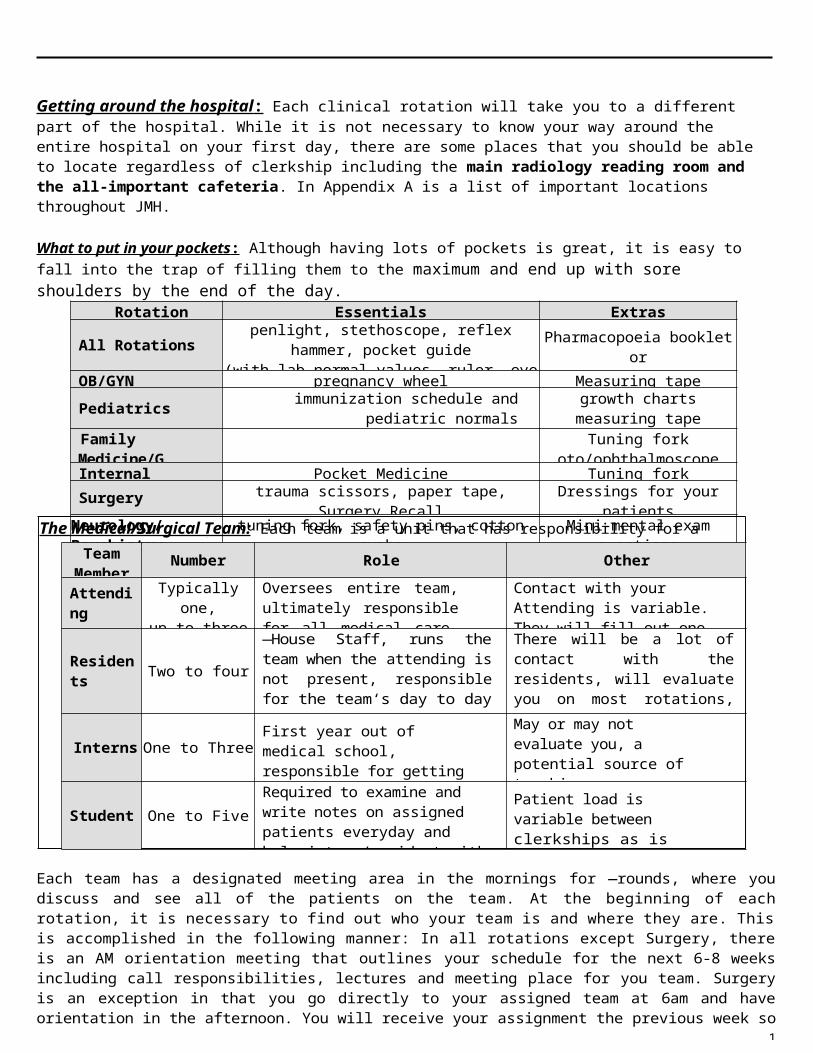
What to put in your pockets : Although having lots of pockets is great, it is easy to fall into the trap of filling them to the maximum and end up with sore shoulders by the end of the day.
Rotation Essentials Extras
All Rotationspenlight, stethoscope, reflex hammer, pocket guide
(with lab normal values, ruler, eye chart such asMaxwell‘s) and a pocket text/reference guide.
Pharmacopoeia booklet orEpocrates on PDA
OB/GYN pregnancy wheel Measuring tape
Pediatrics immunization schedule and pediatric normalsgrowth charts
measuring tapeFamily Medicine/GPC
Tuning forkoto/ophthalmoscope
Internal Medicine Pocket Medicine Tuning fork
Surgery trauma scissors, paper tape, Surgery RecallDressings for your patients
(ex: 4x4 gauze)Neurology/Psychiatry
tuning fork, safety pins, cotton swabsMini-mental exam questions
Each team has a designated meeting area in the mornings for ―rounds, where you discuss and see all of the patients on the team. At the beginning of each rotation, it is necessary to find out who your team is and where they are. This is
accomplished in the following manner: In all rotations except Surgery, there is an AM orientation meeting that outlines your schedule for the next 6-8 weeks including call responsibilities, lectures and meeting place for you team. Surgery is an exception in that you go directly to your assigned team at 6am and have orientation in the afternoon. You will receive your assignment the previous week so you know approximately where to go on that Monday morning.
Special Requests : With many of the rotations, there is an opportunity to request specific services, teammates and the like. Surgery and Internal Medicine have a formal request form that you will receive and must return the week before that
1
The Medical/Surgical Team: Each team is a unit that has responsibility for a certain subgroup of patients.
TeamMember
Number Role Other
AttendingTypically one,up to three in
surgery
Oversees entire team, ultimately responsible for all medical care, a faculty member
Contact with your Attending is variable. They will fill out one of your evaluation forms
Residents Two to four―House Staff, runs the team when the attending is not present, responsible for the team‘s day to day operations
There will be a lot of contact with the residents, will evaluate you on most rotations, the source of a majority of the teaching you will receive on the wards
Interns One to ThreeFirst year out of medical school, responsible for getting the work done on patients
May or may not evaluate you, a potential source of teachingdepending on how overwhelmed/worked your intern is
Student One to Five
Required to examine and write notes on assigned patients everyday and help intern/resident with getting work done on your patients
Patient load is variable between clerkships as is ―on-call" responsibilities
rotation begins. In Family Medicine/GPC, Neurology/Psychiatry, Pediatrics and OB/GYN, there are not formal request processes but most departments will try to honor requests if given to the course coordinators office prior to the start of the rotation. Appendix B has a list of the course coordinators and their secretaries. Invariably situations arise where you need to miss a few days of the rotation due to death of a family member, illness or weddings, etc. It is imperative that you let your course coordinator/team know ASAP so that arrangements may be made (even if this means notifying the course coordinator before you even begin the rotation). Some rotations are more flexible than others in this regard (eg. Psychiatry is very flexible while Neurology is not flexible at all).
Graduate Medical Education : In medical school terms, undergraduate medical education is considered to be the four years of medical school. Internship, Residency and Fellowships all comprise graduate medical education. Internship is the first year after medical school graduation and in many fields today is automatically combined with residency. One must complete at least one year, your internship year, in order to qualify to take Step 3 of the National Licensing Boards. You then go on to a residency and after that you are qualified to take the Boards for that specialty. You can go on to sub-specialize by applying for a fellowship with subsequent boards in that specialty area.
Mentors/Career Choice: As your third year progresses, it is important to keep your mind open to new experiences and different specialties as possible career paths. If you come across a field that is intriguing to you, do not be afraid to approach your residents and attendings. They can give you a broader perspective of what this field has to offer as a future career choice. They will often offer you great opportunities that can better orient you and provide you with a greater understanding of what life is like in that specialty. Close to the end of your third year, it is also a good idea to meet with the program director of the field you choose. They can provide you with invaluable advice that will make the application/interview process a smoother experience. For example, they can let you know how important research experience or clinical experience is and can connect you to ongoing research projects.
Hopefully, you have been introduced to the Careers in Medicine website on the AAMC web page [http://www.aamc.org/students/cim/]. The beginning of the third year is an excellent time to re-evaluate your career goals, or just to review your profile and interests. Remember that it is OK to change your mind 100 times during 3rd year concerning a specialty choice. Keep going back to the Careers in Medicine website throughout the year whenever you may be looking for some answers or guidance. In addition, visit the Office of Professional Development and Career Guidance. There you can meet Dr. Donald Temple and Dr. Hilit Mechaber or Mrs. Biederman. They can connect you with faculty members and doctors in almost every field have expressed interest in meeting with students to discuss their career choices. It might not be a bad idea to ask current 4 th years which attendings are good mentors. Also, be sure to take advantage of the various student-run interest groups which exist for most specialties.
Externships : Midway through your third year you should begin to consider where you would like to do externships during your fourth year. They are great opportunities to try out other programs, see cities you might want to live in and have the programs get a look at you. Most people go on externships in the fall of their 4th year to help them in the application process; it is a good idea to get an outside letter of recommendation to strengthen your application. Some students use this opportunity to see a new city for fun or to travel internationally.
Regardless of where you want to go or what you want to do, it is important to contact the programs to find out their schedule and their application dates. Nancy Cuevas in the Student Affairs office has a packet with all of the contact numbers and email addresses of all the US schools. By April you should begin applying. Italia Smith, Coordinator for Student Service in the Office of Academic Affairs, has the packet that is necessary to complete for international externships. In January of your third year, the Deans will have a class meeting to go over the timeline of requirements.
VSAS (Visiting Student Application Services) is a new online pilot program used by ten institutions for externship applications. You should visit their website to find out which schools utilize this service [http://www.aamc.org/programs/vsas/]. Italia Smith will email you your login code (which is the same as your other AAMC login credentials). Once you complete the application, Nancy Cuevas will be notified so that she can complete the institutional certification aspect, and then Italia Smith will release the application to the different schools.
Each institution has different requirements concerning immunizations and their health policies. It is important to read their instructions carefully to ensure that your application is processed in time. Early in the year, make sure to have your titers drawn at the Student Health Clinic (must make an appointment at 786-466-8381). Certain schools will require the actual lab report for the titers, but make sure to bring all necessary forms to the appointment so they can order everything you need. Some schools require a complete physical exam, which is NOT done at the Student Health Clinic.
2

JMH Electronic Medical Record System JACKS : During the orientation week for third year, you have a scheduled training session for the computer system. At this point, you will receive your login and password that will enable you limited use of the system. It is imperative that you attend this session as it outlines the important functions that you will need, including looking up a patient‘s lab results, future appointments and discharge summaries from previous in-patient stays. Take special note on how to set up patient lists. This will be very important; you will be able to generate a list of patients assigned to your team, and even a personalized list of your assigned patients. The training takes place in the Park Plaza West (Green Garage) basement, Rm L 202. Office hours are 7am -11pm, seven days a week.
The PACS system is essential for viewing radiology on any of the intranet equipped JMH computer terminals. There are no longer any plain film X-rays (except in trauma); almost everything is now on the computer. The username is your regular email logon ID, and the password is the same as the username. After you first logon to PACS, you will be asked to reset your password.
JMH Phone/Pager System : All phone numbers begin with the ―585‖ that within the hospital can be replaced with a ―5‖ followed by the four-digit extension. If a phone line‘s five-digit number begins with a ―6‖ this means it can only receive limited inbound calls. Therefore, if you are paging someone to a phone, be sure to page them to a ―5-xxxx‖ number. To dial outside of the hospital, one must first dial ―99.‖
The house staff at JMH all carry either a four-digit pager, their individual pager or a separate pager that is attached to a specific job. For example, the Trauma Blue intern pager is always carried by the intern currently on the Trauma Blue service. To Page: dial 5-2255 (or 585-2255 from a phone outside of JMH) and follow the instructions: enter the four-digit pager number at the tone, then enter the number you want that person to call followed by the pound key.
The page operator is 5-5400, this number is important when asked to page or call another service.Translator Pager-6921Procedure team- 0179
When paging someone to a JMH phone with multiple extensions, you must page them to the second number up from the bottom. That is usually the main number to the floor, and is the only number that will allow the phones on that floor to ring. The call may come in on any extension, but it is the only way the call will get through.
For a hospital phone directory, go to the 5th floor of the Annex Building down the hallway on the way to the cafeteria (it has a phone outside the door). These directories are updated yearly.
Chapter 2Systems to Know Before You Begin
2

The First Day: You are supposed to receive a packet or email with information about the first day of a rotation at least by the weekend before it begins. However, some secretaries are more organized than others in getting the information out to you. It is important to call and ask the secretary or your fellow students where to go and what time you need to be there if you don‘t get any notice. Some students would find or page the residents on the team they were assigned to and see what time rounds started and if they were expected to pick up a patient. (Highly Advised)
Your responsibilities on the first day of a rotation vary considerably. There is always an orientation. Most rotations require that you at least go and meet the team you‘re assigned to that day. Some teams will immediately give you patients or duties to fulfill, while others will let you start the next day. It‘s important to be in constant contact with any other medical students you may have on your team; the residents and attendings notice if there is good rapport and sharing between members of the team. Be sure to trade cell phone numbers with your teammates and get the pager numbers for your residents. Ask the resident or intern how to access the sign-out and add the census for your team to the patient tabs in Cerner. Also, important to add each patient you admit or participate in care to the My Patients tab in Cerner.
The Typical Day : What time your day begins is dependent upon how long it takes you to complete your pre-rounds and what time rounds begin. It is the medical student‘s responsibility to see his/her patients and write a progress note (pre-rounding) before rounds begin with the rest of the team.
Each morning you must do the following:1. Look up new or pending labs in the computer and check vitals which will also be in the computer. In's and Out's are
still located in the flow sheet that is located in the nursing station in trauma, but can sometimes be found in Cerner elsewhere. In Peds, I & O are always in Cerner. Please note, there is no such thing as a pending x-ray. If the computer reports it as pending, you can look at the film using the PACS system or go to the radiology reading room [Diagnostic & Treatment Center – JMH 2nd Floor] for additional help. The film may have been read and dictated, just not transcribed into JACKS. You can also call the dictation line for the dictated report [305-547-7900, then press 4444#1, then enter the MRN#; if you need to advance dictations, press 5]. Also, don‘t forget to look up older labs that might have been pending previously, such as blood and urine cultures and pathology reports , these return under the date they were ordered not when the result is back (these can take several days to show up in the computer) . For abnormal values, you may want to look at previous values to see their trends or the patient‘s baseline value. It may be beneficial to record al l re levant pat ient information in a template or ―scutsheet [some avai lable at http://www.medfools.com/downloads.php] because oftentimes residents/attendings will ask about previous labs/imaging reports to compare current values to.2. See your patient; ask them about their symptoms and how they are doing. Each service will also have certain specific
questions to ask (i.e. contractions on OB) – see later chapters of this guide.3. Examine them; every patient deserves a daily physical exam with greater focus on their admitting problem.4. Write a progress note or SOAP note in their chart (see chapter 3).
These basic steps are followed regardless of the rotation, although each rotation has a different focus and the notes tend to be different. Appendix D contains a sample admission note and sample progress note. Information concerning the focus of your exam and note on each rotation is included in that section.
Rounds : These take up a variable part of the morning and are attended by various team members. A majority of the time the entire team is present and the patients on the service are presented to the Attending, the patient is seen again and a plan is made for the day. Presenting is an important skill to master because this is the only time that the Attending might interact with you. They fill out your evaluation at the end of the rotation based on your presentations and what the residents have to say about you.
Floor work : By the end of rounds there is a list of work to be completed for the day. Make sure you have written downthe work list for your patients so you don‘t forget anything. The most common way to organize what needs to be done iswriting the To Do List on a census or sign-out. It is important to then get as much of the work done as possible before lunch
Chapter 3 The In-Patient Wards
4

because the afternoons go by fast and orders for specific labs need to be entered in the AM. Again, not only every service, but every team, runs things differently and it is important to find out on the first day of the rotation what the resident expects of you and what your duties are.
Some services might have afternoon rounds (notably Surgery and Ob/Gyn). On other rotations, you may be allowed to leave after the work for the day is done. In either case, don‘t leave until the chief resident or senior resident on your team gives you permission.
Excellent resource to help you with floor work: WWW.MEDFOOLS.COM – a great source for scutsheets, etc.
5
Chapter 4Writing Notes and Presentations
This section is intended to be a guide/template for all progress and admission notes. Keep in mind, however, that each service stresses different parts of the standard form, while others almost completely omit or add sections. For example, OB/GYN will add information about past pregnancies and GYN history, while a surgical progress note is not very interested in detailed problem lists. Also, neurology teams are very interested in a detailed neuro exam, and not as interested in the daily abdominal exam. Just like everything else in 3rd year, take a cue from your interns and residents to find out what the attending on the team prefers, and don‘t be afraid to ask questions.
Progress Note = SOAP Note It is always a good idea to begin a progress note with a one-sentence patient identification. For example: Patient is a (age) year old (race/gender), hospital day #X for (admitting problem) or Post-op day #X (for surgical patient). It is important to also include in this sentence the day number for antibiotics (abx) and for any central lines. Don‘t forget to check and record the medications that your patient is taking, The medications listed in the JACKS system are not always accurate as to what the patient is receiving in the hospital, so make sure to check the patient‘s MAR located with the patient‘s flow sheets in a binder at the nurse‘s station.
ID: Identifying Data: This should be short and sweet giving the most pertinent information on the patient that will allow someone reading the note know who the patient is. For example: 54 yo HF with h/o pancreatic adenocarcinoma s/p double bypass.
S: subjective : Here you write the patient‘s observations about theirillness, symptoms, and any developments or problems since theprevious day.
O: objective: Important vitals - Temp Max, HR (range), BP (range).If the patient has fluid ins and outs recorded(I/O), these are considered to be vital signs and should berecorded as 24-hour values. (On pediatrics they like the urine
output recorded as cc/kg/hr). Begins with a one phrase assessment of the patient‘s overalllook, e.g. NAD (no acute distress), A directed physical exam is thenrecorded followed by labs and imaging studies.
A/P: assessment and plan. Recap pt ID and what the working Dx is. Number eachproblem and write an assessment of the current status of theproblem and a plan for it. This is the area where you can shine.
Anyone can be a worker and report subjective and objective findings but a well thought out assessment and plan shows that you know the patient, the problem, and what to do about it. Always check with your resident and/or attending before writing your plan, as they have the final say on the patient. This does not mean you should not have a plan formulated. Once you present your patient, you will usually have the opportunity to share your ideas about what should be done next for the patient, and that is your time to shine.
Additionally, a well-written note should allow any other person reading the note to understand exactly what is going on with the patient and what the team is currently planning. This is especially important when you consult another specialty to see your patient and they are reading the chart for the first time. You will notice that the medical student note is typically much longer and more detailed than the resident and attending note, this is appropriate and shouldn‘t be shortened.
6
Presenting on daily rounds: This is essentially comprised of the same information in your progress note and in the same format. It is different because you often shorten what you report of the physical exam to include only the pertinent positives and negatives. The attending doesn‘t want to hear that the tympanic membranes were clear if this is someone in the hospital after a foot operation.
Admission Notes : The following format is standard wherever you go. All of this information is in Maxwell. ID/CC (identifying data); the same as mentioned above with the SOAP notes.HPI: the who, what, when, where, why, and how of the patient‘s problems that are requiring admission including
the ―seven dimensions of pain/any symptom‖ (OLDCARTS) and most importantly the time course of events. Thisalso includes pertinent PMH related to the chief complaint (i.e. if the pt has chest pain and had a MI 3 years ago).
PMH: list by problem, include duration, past or ongoing treatment, level of control, and any associated hospitalizations. PSHx: the surgery plus the reason and dateMeds: include dosing and complianceAllergies: include what the reaction wasFam Hx: include first-degree relatives, their age now or age at death along with cause, chronic/familial medical illnesses
Social Hx: who the patient lives with, occupation, education level. Some rotations put habits in the category also, asking only about EtOH, tobacco and illegal drugs. Include sexual history, if relevant.
ROS: The review of systems is a component of the admission note that is recorded but never presented. Do not repeat information already in the HPI, simply write ―see HPI‖ for those sections and continue with your complete ROS.PE: General Appearance, Vitals, HEENT, Lungs, CV, Abd ,Ext, neuro, other.Labs& Imaging: any x-rays or blood work done by the emergency room. If a lab was ordered but results are not back, write
―pending.‖
Assessment and Plan:The most important part of the note, the same approach is used as in the SOAP note. Number each problem and write a thorough assessment of what is going on. For the plan in an admission note, the purist approach is to first address the diagnostic plan and then a therapeutic plan.
The Formal Presentation : As with the daily progress presentation, the structure is that of the admission note: the same content, the same order, just no review of systems and no extraneous information. The key to a good presentation includes all pertinent information delivered in a smooth and concise manner. No one on the team wants to listen to a medical student take twenty minutes to present in a wandering way filled with lots of ―ums‖ and ―ahs‖. Certain phrases should never be used such as ―well basically what happened was‖ or ―essentially.‖ Terms like these tell the attending that you aren‘t comfortable presenting patients. Think of your presentation as a story in that it paints a picture of what happened in a clear and concise manner. Do not editorialize during the presentation on why you believe a certain problem exists present the facts and clarify the problems during the assessment. This takes practice and no one expects you to do it well from day one. Some pointers include:
- Do not include a review of systems on oral presentation.- As a student, you will have to include a differential diagnosis in the assessment.- Ask your intern/resident for help or advice; most are very willing to help.
Please refer to Appendix D for sample SOAP and admission notes, as well as some more presentation pearls.
7

Chapter 5Family Medicine/GPC
Family Medicine/ General Primary Care: This rotation might be completely different for those of you who take it first than for those that take it later.
Half of the rotation will be set in a private practice. Each student is assigned a community preceptor to work with. The workload on this course is extremely preceptor-dependent. Some clinics are 5 days a week, 8 AM – 5 PM; others are only three or four days a week with variable hours. What you are able to do at clinics depends on your preceptor. Some will allow you to examine patients, write notes, and formulate plans. Others might just have you act as an observer. As you can see, this experience is a lot like your preceptor experience during the first and second years of medical school. While your participation is dependant on the office setting, you can always try to take a pro-active role and do as much as your preceptor will allow.
The other part of the rotation will be set in various clinics/outpatient experiences around Miami. A typical day is divided into halves. For example in the morning, you may be assigned Jefferson Reaves and in the afternoon you will rotate through ACC or a public school clinic. By the end of the rotation, you will also turn in two write-ups from these clinics that you believe represent your best work. You will make photocopies of your write-ups which must be evaluated by an attending before being handed in.
It is extremely important to be on time and be present for the clinics you are assigned to on your schedule. Be sure to call the coordinator and clinic ahead of time if you are going to be late or are not able to attend clinic.
Jefferson Reaves: Take advantage of the learning opportunity offered at Jefferson Reaves. This is the one place in which patients are scheduled for students to see. Students will first see a patient by themselves, and then present the case to an Attending. You will be asked to do both problem-focused histories and physical exams as well as address any on-going chronic medical conditions. Many of these patients have elaborate past medical histories found in their charts. Unless it is a first-time visit, you are not required to get a complete history. Focus on the patient‘s chief complaint. Find out what information is pertinent to the chief complaint, and then do a focused exam. Try to develop an assessment in your mind by asking yourself: ―How is the patient doing in regard to the chief complaint?
For example: CC: ―My pressure‘s high. Assessment: 55 year-old black male with PMHx significant for HTN and DM presents with high BP due to noncompliance of meds x 2wks for financial reasons. Patient‘s BP is not well controlled, as evidenced by BP 150/90, +HA, +scotoma and noncompliance of meds x 2wks.
Having even these few sentences shows that you are acquiring information and analyzing the data. Next comes the plan. Give it a shot. Try to decide what meds the patient should be on. It‘s not important so much to know the specific drugs to use, but try to understand what class of drugs to use and why you are choosing that medication. Throughout the year you will get more familiar with actual drugs.
After seeing the patient, you will present the information to the Attending. Together you will review the Assessment and Plan. You will then both see the patient together, and provide the patient with prescriptions, education, and follow-up appointments. Make sure to review the topics of Hypertension, Diabetes Mellitus and Dyslipidemia in preparation for your time at Jefferson Reaves!!! Many of the patients also have concomitant social issues that can be addressed during their appointments.
STD Clinic: It sounds gross and disgusting, but it turns out to be everyone‘s favorite. You attend STD clinic at the Health Department for usually one week. The doctors, nurses and techs are extremely helpful and teach you a lot. You are taught to take a sexual history. You will get lots of practice with gyn and male exams. By the end of the week you are extremely comfortable doing these histories and physicals. You will learn all there is to know about STDs. You will get to see Giardia, Trichomonas and even Syphillis clinically and under the microscope.
Camillus House: Camillus house is a non-profit organization that provides care and shelter to poor homeless men, women, and children. This experience is unique in that you will most likely get to see more children and adolescents, and anything from management of hypertension to management of HIV. Chances are you will get to work with Dr. J. Hiriart, the director of student education, who specializes in Med/Peds. He is very student friendly and will have you see the patients, write the notes, and then present to him.
8

John F. Kennedy Middle School: If Miami-Dade Public Schools are in session during your rotation you may be assigned to this school clinic for one of the weeks of the rotation. Here you see both students and their family members. Many of the appointments are devoted to yearly school physicals.
9
Chapter 6OB/GYN
This 6-week rotation will place you for 3 weeks on a Generalist Team, 1 week on a Gynecology Oncology Team , and the other 2 weeks could include Maternal Fetal Medicine, Reproductive Endocrinology, or an off-campus private practice. Your Generalist weeks will be divided up into 1 day of OR, 1 day of Labor &Delivery, and 3 days of clinic. There is no option as to what team you are assigned to. On the first day of the rotation, you will receive a syllabus that will assign you to your team. In general, your days will start very early, and end very late. On either service, you will probably have to arrive at the hospital at 6 AM, and on some days be expected to stay until 8 PM. The hours are variable, especially depending upon the team you are assigned to.
Thursday is the academic day on OB/GYN. You will have to round in the morning, but after rounds, you will be expected to attend lectures. Sometimes they will finish around noon, while other days they will go well into the afternoon. Attendance is taken at all the lectures. Also, each Thursday, you will have a quiz from the Beckman textbook readings. The only lectures you are responsible for watching on your own time are Dr. Yasin‘s lectures, which are video-tapped. His lectures can be found on the mededu website, under MS-3 course listings, OB/GYN. Make sure to watch his lectures prior to your OB week because he WILL ASK YOU QUESTIONS, or at least ask you if you watched his lectures!
In addition to these lectures, you will have weekly small group meetings with an attending assigned to be your faculty mentor. These sessions usually involve student presentations and discussion about your case write-ups. You will have to hand in a written case report about halfway through the rotation. The format will be discussed at orientation, and you can get feedback and advice from your small group leader. You will then hopefully go over your reports at one of the later small group sessions. It is the only true assignment‘ for this rotation.
As for grading on this rotation, you will be evaluated by your residents/fellows/attendings on OB and GYN/GYO. Your small group leader will also evaluate you. There is an oral exam that you will take sometime during the 3rd or 4th week on the rotation. The oral exam covers several topics in OB/GYN and focuses mainly on how to convey information to patients. These oral exams are very low stress, and because they occur in the middle of the rotation, you do not need to worry about being tested on cases from services that you have not rotated through yet. The final written exam is a national Shelf exam that is given on the last Friday of the rotation. This is a difficult exam to prepare for, as you have very little background in OB/GYN from the first 2 years of school, and your free time is very limited. Traditionally, the exam has emphasized OB more than GYN and GYO is only minimally covered on the shelf so do not waste your time memorizing cancer stages for the shelf. Try to read through a book, whether it is Case Files, Blueprints, Beckmann‘s, or Hacker & Moore. Most people suggest Case Files. Dr. Estes has also ordered access to an online question database (known as the ACOG questions), which was helpful for the range of topics covered on the shelf exam.
During this rotation, you will have to spend a maximum of 2 nights on-call in Labor and Delivery. Your L&D call starts with evening board rounds. After that, it‘s pretty much the same as your day on the floor. Be prepared for no sleep, as there is usually very little free time or even a call room for the students. Feel free to participate in both deliveries and C-sections. Call will last until board rounds the next morning. If the night is slow the residents usually tell you to go home early.
Obstetrics
On OB, rounds can begin as early as 6 AM. You will usually see 1-2 patients and write notes for them before rounding with the resident and/or attending. The notes should include the following:
- Patient ID (GxPxxxx, CC, HD# or POD#)- Did the baby move overnight- Was there any uterine tenderness/contractions- Was there any vaginal discharge or blood- For pre-eclampsia patients, always ask about headaches, vision changes, or edema- Vital signs for the mother and baby (including fetal heart rate)- Always a thorough heart, lung and abdominal exam
After morning rounds, you will have to attend morning meeting with the OB residents and one of their attendings. This is a high-pressure situation for residents, but low-key for students. You are expected to observe, as residents will present interesting and/or new patients. Important words of advice are to not speak unless spoken to, and do not fall asleep!! It will be extremely difficult when you are post-call, but do your best.
10

After morning meeting, you will then head to clinic or Labor and Delivery (L&D). Your residents will tell you where to go. The 1st and 3rd year residents are on the labor floor, and the 2nd and 4th year residents are in the OR performing the C-Sections. During the week of L&D there is the potential to do a lot. There are board rounds in the morning, where one team signs out all the new patients to the new team. When you start your shift, the students should split up the patients on the floor, and follow their own patients. You are expected to check up on your patients periodically. As new patients come onto the floor, you should pick them up, and do an admitting H & P. There will be an opportunity to go to the OR for C-Sections. Be patient, as there is a lot happening on the labor floor. A word of advice about obstetrics: many of the attendings, residents and staff may seem intimidating at times. Do not let them walk all over you—stand up for yourself. If the problems ever get out of hand, you can always talk to your team‘s chief, your attending, and/or Dr. Estes who is very approachable. However, in order to get the most from the experience, you have to put yourself out there, otherwise you will be ignored. Constantly keep reminding the residents and the midwives that you want to be part of a delivery.
In clinic, you will see pregnant and/or post-partum patients, and check their labs. Ask the same types of questions you would ask your ward patients in the morning. On exam, you should measure fundal height, listen for fetal heart tones, and do a brief PE on the mother. In labs, look for protein, ketones, or glucose in the urine, check for last PAP, RPR, Hep B, GC/Chlamydia culture, H/H, as well as Hb electrophoresis. There is a standardized form in each patient‘s folders that will clue you in on the questions to ask and labs to look up; it is very helpful. Also, if they are past 20 weeks, check to make sure an ultrasound has been performed. These clinics are busy/hectic, so be patient as there are usually a lot of patients to see. In the mornings, it is usually a general prenatal clinic. In the afternoons, there are more high-risk clinics (HIV, Diabetes etc). There are endocrine OB clinics, as well as clinics for women with a history of substance abuse problems. Your role in these clinics may be diminished, but that is all dependent on the attending in charge.
GYO
On this half of the rotation, your ward responsibilities are very similar. You usually have to show up around 6 AM, and will see anywhere from 1 to 3 patients, depending upon your service. On GYN, the teams are similar in size with similar responsibilities. After rounds in the morning, you will then go to the OR or to clinic. Clinic times vary, but there can be clinic in both the morning and afternoon. There are usually 2 GYN teams and these teams alternate weeks in the OR and Clinics. On GYO, be sure to show up in dress clothes every morning. If you are scheduled to go to the OR that day, bring a change of scrubs.
For the OR, the best thing to do is to print out the schedule the day before. Split the cases up with your team, and try to read up on your patient‘s problem(s) and the relevant anatomy for the case. It‘s like your surgery rotation, where residents and attendings can and do ask you questions. Be prepared. And keep in mind, especially on GYO, some cases may last longer than 5 hours. Go to the bathroom and get something to eat before if there is a chance it may be a long case.
As for clinics, it is also very busy. The GYN history is a bit more extensive than a standard history. It must also include:
- Last Menstrual Period - Period Frequency - Menarche- Past OB Hx (G & P) - Past GYN hx - Family Hx- Social Hx - STD‘s - Meds/Allergies
At these clinics, you will have to do a pelvic exam (don‘t worry, you will practice it again during orientation). Remember that if you are to do the exam, you should wait for a resident or attending to be present. It is not right to ask a patient to wait on the exam table while you try to find someone to supervise. It‘s OK to get the history alone, and then return with a Dr. to perform the physical exam. These exams may include the chance to do a Pap Smear, colposcopy, biopsies, and various cultures. You need to document in the chart findings concerning the vagina, cervix, uterus, and adnexa. In addition, if a colposcopy and/or biopsy is done, the best way to document suspicious sites is to draw a picture.
Many times, you will also have rounds in the afternoon after clinics (especially on GYO). Always remember to check with your resident to see if you are going to round again later in the day. As in all rotations, you are not free to go until your residents give you permission to leave. Remember to always ask if there are any notes or work you can do for them, it shows interest. A valuable resource for any oncology service (med onc, rad onc or gyn onc) is Wikibooks radiation oncology. This is a free online book that covers every tumor site in the body and has important background information and treatments for each site with corresponding evidence. It can really help you understand the service and make you look very interested.
11
Chapter 7 Pediatrics
Pediatrics is divided into 2 weeks of wards, 1 week of the pediatric ER, 1 week of Neonatal Intermediate Care Unit (NICU), 1 week of outpatient pediatrics clinic and 1 week of subspeciality clinics. Unless you request to be on wards first (or last), the order in which you rotate through pediatrics is alphabetical, meaning if you're at the beginning of the alphabet, chances are you will be on wards first.
Regarding which books to buy, most people believe that Blueprints in Pediatrics, First Aid in Pediatrics, and Case Files in Pediatrics are very good books for this rotation. An alternative choice is Clinical Pediatrics and Child Health, which is a textbook out of the U.K. It is concise and easy to read without being as superficial as other books may be. As far as question books are concerned, Appleton & Lange Review and PreTest are equally effective.
On the wards, there are four teams to which you could be assigned to: red, orange, blue, or green. Red is the only generalist team. Orange is hematology and oncology;blue and green are other pediatric subspecialties. Understand that while the attending generally changes from month to month, there are a couple of constants. Dr. Tamer is always the attending on Team Red.. Dr. Tamer in particular is known to be an excellent teacher, and an excellent contact for those of you who wish to get a letter of recommendation. If you are interested in Pediatrics, I recommend inquiring ahead of time as to whether Dr.Tamer and/or Dr.Worley are on the wards during your rotation.
A day on wards generally lasts from 6:30am to 4pm. The mornings are spent rounding and during the afternoon you are responsible for following up on labs, procedures, etc. ordered during rounds. Always check in with your team while you are on the wards! On Saturdays, you are expected to come in and round from roughly 7 to 12pm. You are on call every fourth night while on the wards, and are required to admit one patient. While you could be lucky and get your one patient early in the day, chances are this will not always happen. If you don‘t get your one patient by 7 pm, you can go home. You are required to present your patients to the team the next morning, so be prepared. You are also required to write an admission note reminiscent of those write-ups you hated doing during 1st and 2nd year. It takes a lot longer than you think, especially when you get your patient late.
Every Thursday is an academic day, so for people on the Wards you round in the morning then leave for lecture whenever it begins that day. If you are not on the wards you can just show up for lecture but double check with the NICU attending as some of them may require you to round in the morning before leaving for lecture.
Finally, regarding the shelf exam, well, there is not much we can tell you, other than it is just like any other board exam – difficult!!! Do as many practice questions beforehand as you can, and you will do fine. Remember, there are also medicine questions on the shelf. There are some old shelf questions in the pediatric library in large black binder—hint hint.
12
Chapter 8 Internal Medicine
Along with surgery, internal medicine is one of the major rotations of 3rd year. No matter what specialty you eventually choose you will need to apply something that you will learn during these 8 weeks. The rotation itself is split into two 4- week blocks at either JMH, VA, Mt. Sinai, or UMH doing general medicine. There are also specialty services in Gastroenterology at UMH, Special Immunology, Cardiology, and Hematology/Oncology. You can make a request as to which hospital you are assigned and which student you may want on your team. The internal medicine administrative assistant will send out an email before you begin the rotation and ask for your request. Not everyone, however, will get everything they request.
At JMH, the 3rd year student plays a very active role on the team. Attending rounds vary by team, with most starting between 7-8 AM. You must see all of your patients before rounds, which includes: obtaining their vitals over the last 24 hours, new lab results, new imaging results, updates on any consults/studies done the day prior, any overnight incidents from the nurse, and brief history/physical. Notes are team dependent, with some requiring notes in the chart before rounds. The students are responsible for carrying 2-4 patients. Length of rounds is highly attending and census dependent. After rounds, you carry out the day‘s plan for each of your patients, including calling for consults, medication renewals, prioritizing radiology, calling for lab results, etc. Lectures and POPS sessions are in the afternoon on most days. Student report is held every Friday for those at JMH and the VA. Try to bring one patient to discuss, including all pertinent EKGs and films. It is moderated by the faculty, including Dr. Gardner, and is a great learning experience with a low-stress environment.
Call is every other day, and alternates between short call (until 2pm) and long call (until 6pm). You work under the intern and resident (2nd or 3rd year) and admit 1-2 patients each call and leave either after you are done with your admissions or at 10 PM, whichever comes first. Third year students do the history and physical, then (under ideal conditions) discuss their findings with the resident. For each patient, you come up with a differential diagnosis and write an assessment and plan. You will present your admissions at rounds the next morning You should also turn in your best write-ups to the course coordinator who requires that you submit 3 write-ups for grading. You are supposed to turn in one write up every 2 weeks, but you may want to get all of them done as soon as possible, so you don‘t need to be worrying about them when you are studying for the shelf.
The VA is somewhat similar to JMH. There is a computerized chart system into which you enter all your notes and get lab values, etc.; however, you are not able to write orders as you are able to at JMH. Students here follow the same lecture schedule as those at JMH.
At Mt. Sinai, the same principles apply. There is free breakfast and lunch everyday (a BIG plus), but lunch is almost always non-vegetarian (a heads up for some of you). Work rounds were with the residents in the cafeteria starting at 7am with attending rounds starting between 8-9. See your patients and get your note in the chart before resident rounds. Students here have a different lecture schedule, with POPS sessions every Monday, Wednesday, and Friday following lunch. Each student does one assigned presentation during the 4 weeks. Mt. Sinai is a private hospital and students here generally have a less active role in the team. However, because it is a smaller hospital and you have some more time, there are plenty of opportunities to see procedures done on your patients and others.
Sylvester is a newer service with only 1-2 students for each month. These students work directly with the attendings, and most of the patients are Hem/Onc patients. Rounds usually begin around 8am depending on the census and attending.
There are 2 oral exams and one shelf exam. The orals are 15 minutes each. You choose a card and whatever topic you get, you discuss. The possible topics are listed below and in the syllabus. These orals are VERY examiner dependent with respect to stress level, number of topics, and format of discussion, but the majority will just ask you to tell them what you know about the topic and will ask very few questions. The shelf is a very typical shelf exam, with the exam getting ―easier‖ the later in the year you take it because you generally know more stuff. It is almost impossible to study for everything on it. We recommend knowing your oral exam topics inside out, which prepares you for most of what is on the shelf. This can be done with textbooks, Blueprints, Step-Up to Medicine, Pocket Medicine, and listening on rounds... MKSAP for students 4 is the MUST HAVE TEXT! This book will by far prepare you for your shelf and oral exams BETTER than any other question book. The questions are very ―shelf-like‖ and totally worth the time. It also comes with a CD which you can use on your computer which is faster than flipping to the answers.
13

Survival tips:1. Know your patients! This cannot be stressed enough. It looks very impressive if you can give history tidbits,
radiological findings, or lab values on the spot. Know what medications and dosages they are on.2. Read up on your patients. You will be pimped. Again, very impressive if you get it right. The problem lists are
extensive, so try to read up on all your patients‘ problems. This will also help with shelf and oral exam studying.3. When presenting in attending rounds, be concise and present PERTINENT positives and negatives. All pertinent
findings are in the HPI, including ROS. Don‘t tell the attending the patient denies eye irritation for an acute MI admission.
4. Discharge planning. Once again, it looks impressive if you can say you‘ve talked to the social worker about the possibility for at-home nursing when needed. Many JMH patients will need special outpatient care. Doing this is helpful to the team.
5. Admission write-ups are very thorough, but daily progress notes are very concise SOAP notes.6. Make a COPY of ALL admission write-ups to turn in. You get to choose which ones are handed in so the more you
have to choose from the better.
Oral exam topics: You can find outlines of each of these topics on the Academic Societies website.
-Myocardial infarction -COPD/Asthma -Hepatitis-Anemia -SLE -CHF-Pneumonia -Acute/Chronic Renal Failure -DKA-Acute Arthritis -Hypertensive emergencies -Upper GI bleed-Venous thrombosis/emboli -HIV/AIDS complications -Altered mental status
Example of studying:
For SLE know epidemiology, etiology, signs and symptoms, physical findings, tests and results, various treatments, differential diagnosis, natural history of disease, complications, and the 11 criteria for diagnosis. For example, one of the criteria is a positive ANA, so know what else can give you a positive ANA. Pericarditis may also occur in SLE, so know what else can cause pericarditis, signs and symptoms, treatments, etc. This will help with both oral and shelf exam studying.
14
Chapter 9Surgery
Surgery will probably be the most demanding rotation you have, in terms of time commitment and material to be learned. Your time here is split between Trauma Surgery and General/Elective Surgery. Both are busy schedules, but only Trauma has call. Your grade in surgery is comprised of many different parts: an evaluation from each service you are on (20% each), a final oral exam (20%), the Surgery shelf exam (25%), weekly quizzes (10%), and clerkship director discretionary points (5%) . Read as much as you can whenever you have time, as there is a lot of material to be learned and little free time to learn it.
Over the course of the rotation, you will have lectures once a week, currently on Thursdays from 3:30-5 pm. Attendance is mandatory. After each lecture you have a short 10-question quiz. All the quiz questions come directly out of the reading from Lawrence, not from the lecture itself, although a few lecturers basically give you a lot of the answers in their presentations.
Trauma Surgery
Surgery is split into two segments, trauma surgery and elective surgery. Everyone will spend four weeks on a trauma team. Being on Trauma consists of dividing all the patients on the census amongst the medical students and rounding on them in the mornings, helping at Trauma Clinic, students taking turns carrying the Trauma pager and running down to the resuscitation bay or “resus” when a trauma is coming in, and taking turns scrubbing in on surgeries. You will also have scheduled overnight calls where you will stay overnight in trauma resuscitation bay and work with the resident covering that night.
Keep in mind you have a list of things you have to get signed off by the end of the rotation, like “suture removal, placed a foley, etc.” Keep that form on you so you can get it signed as you do these things and don’t have to scramble near the end.
In terms of exam preparation, you will be expected to submit a list of 6 cases that you are familiar with from your 4 weeks on trauma. That list will compile potential starting points for your oral exam. However, know that the exam can go anywhere. It is very important to know your anatomy concerning certain procedures, especially hernias. This exam is more of a focus on the procedure and surrounding medical concerns of the disease process, but know your patients as well. Unlike the medicine orals, surgeons love to ask questions so be ready for anything. The best piece of advice I heard about surgery and surgeons is that while surgeons may not be correct all the time, they are certain about whatever they say. The take-home message here is that when on rounds, in the OR, or at your oral exam, be confident. While you may not know an exact lab value, you should always have a good idea of the range of that value, and report it confidently. Instead of I think, report an answer as It is.
Remember, surgeons are always in a rush, and therefore want your notes and presentations to be succinct and to the point. Therefore, your write-ups will be VERY FOCUSED. Still use the main admit/progress notes as a guide, but make your note directed. Here are some pointers/examples:
· Get the low down on the case from your resident, and then find the consultation form filled by the requesting physician.
· Chief complaint· HPI: Always ask about the following
Onset Duration Frequency QualityAlleviating Factors Exacerbating Factors Severity (1-10) Assoc. SymptomsFever Meds for symptoms Nausea/Vomiting Last BM
It is important to have a good handle on the sequence of symptom onset, as it helps delineate etiology. **Be succinct yet complete
· PMHx, PSurgHx, Meds, and Allergies are all important· SHx (Tobacco, EtOH, drugs, transfusions) and FamHx should focus on suspected problem· PX: usually very directed with the following always performed
VITALS!!!! Tm, Tc, BP, HR, RRHEENT-note oral mucosa (for hydration)Heart and Lungs (auscultate)Abdomen (auscultate, palpate, rebound?, masses?)
15

Extremities (cyanosis?, clubbing?, edema?) Rectal (tone?, heme?, masses?)
· Labs: You may see some radiological studies that have been performed and results always seem to be pending. Your job is to get the official reading of that film by tracking the film down and reading the report scribbled by the radiologist. If a US or CT scan was performed, the radiologists usually jot their findings in a logbook that is sitting in the trauma radiology reading room (ask your resident where you can find this book).
· A/P: Think about everything for a second and put it all together. Think of a few things the patient may have and why/why not? Is the history consistent with the physical? Do you need to perform some more lab/radiological studies to differentiate causes? If so, what would they be and how could they help? If you feel comfortable with the above questions, then you are ready to present to your resident. Hurry up!
In the mornings you will be pre-rounding on patients who are post-op or post trauma. It is MOST important that you have their vitals and INS/OUTS. You should also look at the patients wound and know if they are getting PT/OT because these are the things that slow down discharge.
On-Call/Resus
When you are on-call with your team, one student will carry the trauma pager. When it goes off, make sure you are back at the resus area. If the patient is coming by air, you can go up to the roof to help bring the patient in. Once in the trauma bay, your responsibilities are ABC (Ass, Blood, Catheter):
1) Remove the patient‘s clothes (conventionally or with trauma scissors)2) Rectal exam to check for blood, tone, and a high-riding prostate in males3) Femoral stick for ABG and whatever blood-work is needed4) Foley Catheter placement in those patients who need it
This is the minimum a student is expected to do. If you have any questions, ask the nurses, as they are usually very helpful. While on-call, you can also help suture patients in the holding area, as well as see consults in the hospital and ER. In addition, if any traumas go to the OR, it is expected that one student will scrub in on that case. This is the day for you to see cases in the OR as well. It is up to the students on call to decide who will scrub in on what cases. Make sure you see a variety of cases, as your oral exam topics are generated from cases you will see in the OR. It is a good idea to look at the OR schedule the day before elective day, split up the cases then, and the night before read about the procedure you will observe. Residents and attendings love to pimp students while they are scrubbed in to cases.
ClinicTrauma clinic is typically a very fast-moving clinic. You are seeing patients for either pre-op evaluation or for follow-up after a certain procedure. Your progress notes should be concise, yet thorough. Surgeons are very ‗to the point‘ people, and like notes as such. You will be shown a pre-op packet that you will complete with those patients, and follow-ups may need dressing changes or suture/staple removal. This clinic is run by the senior resident or fellow, and the attending will be there to evaluate all the pre-op patients at the end of clinic. The good news is after that, you should be able to go home!!!!
Take advantage of the days you are done at NOON on trauma. This is great time to study for the shelf and prepare your oral topics. There is much less time on the elective services.
Elective Surgery
There are 5 different general surgery teams you can be on. What follows is a brief summary of each team. Remember, read up on the cases you will be scrubbing in on, and your hours will be long regardless of the team you are on. And always keep in mind, you will be required to know 6 cases from your time on this service for your oral exam. So it is to your benefit to know as much as possible about your cases beforehand, and milk as much info from the residents and attendings as you can while scrubbed in on the cases. But beware, asking questions may set you up to do more research. If you demonstrate some basic knowledge about the patient, the anatomy, and the procedure, your questions should be answered.
There are clinics interspersed with OR days. These are your pre-op/post-op clinics, and they many be long. Sometimes students did not get to eat lunch until 2. A good rule of thumb for your entire Surgery rotation is to carry snacks with you at all times.
16
Chapter 9Surgery
There are afternoon/early-evening rounds as well. Many times students would get frustrated because the residents arrived much later than the scheduled time. It is a good idea to carry a book with you, as there are periods of time between cases and while waiting for your team when you can catch up on your reading. There always needs to be a student present on the weekends to help round. Students generally will split up the weekends giving you at least some time off.
EI – Surgical OncologyAs the name implies, this service deals with surgical intervention of many types of cancers (especially breast cancer). There is some general surgery as well. Rounds begin at 6 AM in WW 10. There are some long cases, and some cases start very late. There are many mastectomy cases. Remember to print up the schedule ahead of time to fairly split the cases up. Also Dr. Livingstone, the chair of the department of surgery, is the head of the E1 service. Therefore, this is a great opportunity for those interested in a surgical career and possibly a letter from Dr. Livingstone.
E2 – Endocrine/Hepato-biliaryThis is traditionally the most challenging team, but is very resident dependent. You will work insanely long hours (some surgeries will go in excess of 9 hours), but it is also the team where you will be rewarded with excellent learning experiences as well as a good evaluation if you do what is expected of you. Many of these cases are extremely long, so be prepared (eat and go to the bathroom before scrubbing in). Rounds also start for this team at 6 AM in WW 10; in addition, you will round in the evening with Dr. Levi on his patients (typically later in the evening than earlier). I‘ve heard the census can get very large, so be prepared to work hard.
E3 – ColorectalSimilar to the other JMH elective services. Rounds also begin at 6AM on WW10. You are in the OR all day Monday and Wednesday and doing colonoscopies on Friday. You have an all-day clinic on Tuesday where you will see a variety of patients and then post-op clinic on Thursday. The surgeries range from 20-minute anal cases to 5-hour open abdomen cases so there is a lot of variety.
Pediatric SurgeryThis is a slightly different type of service. This is a general pediatrics surgery team. If you want experience monitoring and caring for peds patients, this is a good team to be on. Students are responsible for monitoring the PSSC patients each AM. 2 days each week are spent in the clinic, and 3 days are spent in the OR. You will get excellent experience monitoring fluids and electrolytes on this service.
VA SurgeryThis is the broadest of the elective surgery teams. You will have the opportunity to see almost every type of surgery as a member of this team You will also be doing a variety of “surgical” clinics, including pre-op clinic, vascular surgery clinic, and proctology clinic. Rounds typically begin at 6:30 AM at the VA SICU.
Vascular and Transplant SurgeryThese are new services for students. These are very focused electives and are very similar to working on any other E service. You typically begin between 6-7AM.
17
Chapter 10Neurology
Neurology is a 4-week course. Two weeks are spent on the wards on the general neurology service. The remaining two weeks are either spent on the stroke service or on the consult service. Lectures are held in the afternoons on Fridays- you are REQUIRED to be at these lectures and DO NOT BE LATE! They are actually worthwhile and generally well taught. At the end of each lecture is a short quiz that can be difficult; to do well, go over all of the assigned slides and focus on the ones that will not be reviewed in the the lecture. They represent easy points for you to earn toward your final grade.
The 2 weeks spent on the general service is on WW11 if you are at JMH. If you are at the VA, the residents room is on the 12th floor. Three PGY-2 residents manage patients on this service. Students are encouraged to follow 1 or 2 patients and write notes in the morning. Each morning the team of residents and students round with the attending. These rounds are benign and students are usually allowed to present if so desired. Once or twice a week the team will go to neuro-radiology rounds at 8am. Usually, after rounds or neuro-radiology rounds, the students are generally free until the afternoon lectures. This time can be spent writing notes on patients, researching a presentation topic, or studying neurology. Students don‘t come in to round on Saturday or Sunday unless you are on call.
Students on stroke service will learn the most during the rotation. Be sure to study your neuroanatomy/vasculature. These students follow patients admitted for strokes with a resident, the stroke fellow, and one of the stroke attendings. Rounds last a little longer on this service, but less is expected of the student. Some patients will be in the neurosurgery or stroke ICU and are more challenging to follow. After morning rounds, the day is usually free until afternoon lecture.
Students on consult service spend the morning following the PGY-3 resident around the hospital seeing all patients on other services for which a neuro consult was ordered. The attending will usually round briefly with the team in the mornings. You generally do not pre-round on this service and will rarely present to the attending in the morning. There are no morning notes to write on this service. Students are usually done by lunch but may have to stay till four when the on call resident takes over.
Students are required to take call 3 times during this rotation. Call involves working with the PGY-3 resident on call, seeing all neurology consults in the hospital. Call starts at 4PM. Page the resident when you‘re ready to start and they‘ll usually tell you where to meet. Call lasts until 11pm, and the residents have been warned repeatedly by faculty not to let students out early! Weekend call is quite long, starting at 8am for morning rounds and finishing at 11pm as well. You will almost never be let out early and there can be a lot of down time if there are no consults, so come prepared with study materials, etc.
You will participate in WBT, or Ward Based Teaching.. You will write up one of your patients, ON PROGRESS NOTE PAPER, from presentation to hospital course – like an extensive admit note. You will present the patient in full to your chief resident. Your grade for this exercise will be based on both your presentation and the write-up.
There is an essential neurological findings quiz, which is a web based training involving localizing lesions given a patient’s clinical findings. There is also a neuroanatomy radiology powerpoint, and there will be a quiz halfway through rotation on the anatomical structures. For now, spelling does count.
In general, this is not a difficult rotation, it is very structured and has a lot of busy work. The final exam includes information from the lectures, and since each lecture has an extensive handout, no outside reading is required for the exam. The final also includes neuro-radiology, so the student should find time to review the radiology posted on the web. You will also be expected to perform a neuro exam on a normal patient in 10 minutes - the examiners are VERY picky about details, so be sure to practice performing the exam ahead of time. Make sure to go to the OSCE review; it is very helpful.
For each 2 weeks, you will also be asked to write a concise presentation of 2 patients. Again, this is not an exercise on writing every detail; rather it is to show you are capable of summarizing a patient in 200 words or less. You will also be asked to turn in a relevant article for each patient. Be sure to always designate HANDEDNESS of your patients.
18
For writing notes on your patients, the emphasis will be the neuro exam. All the other aspects of a standard write-up are the same, with a thorough neuro exam on all admission notes. You will receive a card on the first day of the rotation that lists out the complete neuro exam. Use it as a guide, as it is the neuro exam you will have to perform at the end of the rotation. It includes:
- Mental Status - Reflexes- Cranial Nerves - Coordination- Motor - Gait and Station- Sensation
Students are evaluated by 2 attendings (1 general service, 1 stroke or consult) and 2 residents. These evaluations only count for 10% of the grade! Any student who shows up when and where they are supposed to be will do fine on this rotation.
19

Chapter 11Psychiatry
During the 6-week psychiatry clerkship, you will spend 3 weeks on one service and 3 weeks on another. The services you can work on are the VA, health and recovery, adult inpatient (2 units-adult intensive and BT2), child inpatient, geriatric psych, and inpatient consult.
A typical day on psychiatry begins between 6 and 9, depending on the service, and you will be busy at least through the morning and into the afternoon. You can expect your days to end latest at 5pm. Lectures are held on Thursdays for about four hours. However, most services will require you to be present before you head to lectures. Pay attention at orientation to get the details! These lectures will cover the core topics in psychiatry that are the focus of your shelf exam at the end of the 6-week rotation. 40 % of your grade is from that exam, 50% from your attendings‘ evaluations, and 10 % from attendance, patient write-up, etc. The patient write-up is discussed with you on the first day, and Dr. Sotelo will hand out a sample write-up. It is a standard psych write-up, with a major emphasis on mental status exam and multiaxial diagnosis.
In addition to your ward responsibilities, you will also have to take call in the crisis ER. You will take 2 weekend calls (either 8-1, or 1-6) and 3 weekday calls (form 3-10). You will interview patients who present to the ER, and discuss findings with the resident on-call. During your interview please be sure to sit on the side of the desk that is closest to the door. If the patient is admitted, you will have to do most of the paperwork, lab work and physical exam necessary for admission.
In terms of books, most people use First Aid for Psychiatry. It is key; Case Files is good as well. Dr. Sotelo does not recommend Blueprints. Students also find Lange Q&A helpful as well as USMLE World for practice questions. On the first day of the rotation Carrie will also give you a master key, which will open all the doors in the psychiatry building.
The tools that you will utilize on this rotation are a little different than the others. Most information you will gather on Psychiatry will occur during the patient interview. The key is learning what questions to ask and how to ask them. The emphasis will be on the mental status exam. What follows below is the important aspects of obtaining a psych history when a patient presents to your service or crisis. Remember, it is a unique exam because the ―exam‖ is not a physical exam but is an interpretation of the patient‘s mental status.
HPI: Focus on when the episode started triggers, changes in emotions, duration, habits, depressive symptoms (SIGECAPS), manic, hallucinations, paranoia, and delusions
Past Psychiatric History: hospitalizations, outpatient treatment, medications and responses to individual meds.
Development/Social History:· Birth city· Childhood: any abuse? Who were they raised by?· Relationship with family· Highest level of education· Occupation(s) – past and present· Financial support· Marital status· Children
Family History: Psychiatric, medical, depression, learning problems, mental hospitalization, anyone treated with medications and if so which ones and what responses.
Mental Status Exam:General Appearance: posture, older/younger than stated age, attentiveness, cooperative or not, rate of behavior –hypo/hyperkinetic, psychomotor retardation/excitation, speech, attitude towards examiner.
Mood and Affect: Mood is subjective, affect is how patient demonstrates mood or verbal versus non-verbal. i.e. flat, blunted, normal (=wide range), congruent or incongruent to mood, appropriate/inappropriate affect.
Perceptual Disturbances: hallucinations – olfactory, tactile (formication can occur with DTs), visual, and auditory (how many voices, what do they say, for how long)Thought Processes: Determined entirely via speech. Organized versus disorganized.
20

Disorganized speech can consist of flight of ideas (still connected) versus looseness of associations, tangential, circumstantial or racing thoughts. Assess presence of neologisms or any other language impairments. All are aspects of speech that cannot be better explained by a pure cognitive defect – e.g., Wernicke‘s aphasia.
Thought Content: Preoccupations, thought disturbances consisting of delusions/paranoias or ideas of reference (one notch below a delusion). Is delusion congruent to mood?
Judgment and Insight: ability to understand self, illness and emotions.
Cognition and Sensorium: memory – remote, recent, immediate, intelligence, concentration
Further Diagnostic Studies: Psychological testing, scales for baseline anxiety, depression.
Multiaxis Diagnosis:Axis I: Clinical syndromeAxis II: Personality disorders and mental retardationAxis III: Physical disorders or conditionsAxis IV: Psychosocial and environmental problemsAxis V: Global Assessment of functioning (GAF) scale from
1-100 (100 – superior functioning, 70 – mild symptoms or difficulty in social functioning, 50 – serious symptoms, 20 – danger to self or others.)
For those who want to perfect their mental stats exam (and know what you‘re talking about when presenting to Dr. Henry) a small, cheap, pocket-sized book ―The Mental Status Exam Explained‖ is very helpful.
Appendix AImportant Locations
General InformationMain Radiology Reading Room = DTC 2nd FloorUltrasound = DTC 2nd Floor (OB Ultrasound ACC 2nd Floor) Emergency CT = behind Surgical ER, reading room in main ER hallway Inpatient CT = Central 2Inpatient MRI = 1st floor between Central and DTCCafeteria = 1st floor Central (by atrium)
Family MedicineClerkship orientation/Friday Lectures = Highland Building 4th Floor Geriatrics - VAMC
GPCClerkship orientation/Wed. Morning Lectures = Rosenstiel (auditoriums/ GEM rooms)
Internal MedicineEach team meets in different designated areas each morningER-E = across the hall and beyond Surgical and Medical ER entrances on the right and radiology on the left GI Station = South Wing 2Cardiac Cath = North WingBronchoscopy = North Wing
NeurologyWards = all teams meet on West Wing 11Case-Based Teaching, orientation, and others = all at GCRME Building Clinic = ACC West 3C
OB/GYNLabor Floor = East Tower 4GYN/GYO, Ante-partum = East Tower 7 Post-Partum/nursery = East Tower 3 Clinic = ACC West 4th floor
PediatricsWards = East Tower 5 or 6 (morning work rounds with teams on 6) Library = East Tower 6 code- 6042NICU = Central 5Clinic = ACC West 5th floor
PsychiatryAll activities and most services in Mental Health Building across the street from BPEI. You need a key to get
around.
Surgery Trauma = Ryder Center 3rd Floor
Trauma Clinic = Ryder 3rd Floor ―A‖ sideE1 = WW 10 with surgeries in Main ORE2 = WW 10 with surgeries in Main ORE3 = Rounds in WW 10 with surgeries in Main ORPedi Surgery = meet at PSSC on East Tower 6 VA = VA SICUTransplant- WW15 or otherwise specified Vascular- Page resident
22
Appendix D
Junior Clerkship Coordinators
Clerkship Coordinator Address Phone Fax
Family MedicineDr. Gervais
Andrea Santo
HighlandProfessional Bldg
#470243-2763 243-2905
GPCDr. D. Weiner
Ashley ManuelRMSB #2167 243-3186 243-1814
Geriatrics Dr. Palacios VAMC 2nd fl nursing home #NH207
575-3388 575-3365
Internal MedicineDr. Lowery
Angelica Escalante 243-2218
Neurology Dr. J. Maldonado Gordon Center for
Research for Medical Education D-41
243-6491 243-3347
Ob/Gyn Dr. Estes
Tameka Collins
JMH East Tower #7007
Clinic
585-5610
243-5175325-1282
Pediatrics Dr. A. Tamer JMH East Tower #6006
585-6364 325-0293
PsychiatryDr. Sotelo
Cary Fratacci MHC #3308 355-9146 355-9187
SurgeryDr. L. Sands
Evelyn GoteraSylvester Cancer
Center #3524243-4255 243-4221
AnesthesiologyDr. C. Diez
Victor ChaconJMH Ryder Trauma
2nd Floor585-7015 585-8359
Radiology Dr. H. Martinez JMH West Wing 279 585-7497 585-8591
23

Appendix D
Department Person Phone Fax email
Admission Office Dr. Weiss 243-3234 243-6548
Medical Education 243-2003
Financial AssistanceLaura Kasperski
Maggie Gomez243-6211 243-8398 [email protected]
Curriculum Dr. Mechaber 243-6499 [email protected]
Student Affairs Dr. Ana Campo
Office of Professional Development
Dr. Hilit Mechaber [email protected]
Risk Management Steve 585-7352
Needle Stick Alma Breeden 305-750-0525 p 939-7061
JMH Page Operator 5-5400
Cardiac Arrest 5-6123
Emergency/
Fire5-6123
Security 5-6111
VA Cardiac Arrest 2
Fire/Security 3322
Needle Sticks: If you are accidentally stuck with a needle:– If you are wearing gloves and were stuck in the hand, immediately remove the gloves and rinse your hands with hydrogen
peroxide. Do NOT squeeze the wound.
– Notify the Head Nurse immediately; she will call Employee Health Services.
You should call the Needlestick emergency phone number immediately:
1-866-7-Needle (24 hrs/day; 7 days/week): the nurse will direct you about the next appropriate step, depending on the day
– You will be given the option to take Combivir beginning immediately.– You will have to go to Employee Health Services when they are open to fill out an ―Exposure on Duty‖ form and recall
exactly what happened. They will consent the patient for HIV testing at this time.
24
General Important Phone Numbers
Appendix D
Please note: the following Appendix is a work in progress and is comprised of notes from students. The enclosed data is not necessarily inclusive and every Attending wants something different. There is no real standard - some Attendings are looking for less or more information in different areas. This appendix is meant only as a guideline to help you get the ball rolling. Please feel free to submit well-written notes to the Academic Coordinator for future guides.
AbbreviationsHD- hospital day SOB- shortness of breathPOD- post-op day N/V- nausea and vomitingS/P-status post B-bilaterallyBM- black male HA- headacheLF- Latin female Tm- max temp for 24 hrsPMH- past med history Tc- current tempHTN- hypertension I- total inputDM-diabetes O- total outputC/o- complains of FS- finger stick, blood sugarCP- chest pain CTA- clear to auscultationNSR- normal sinus rhythm NT- non-tenderLAD- lymphadenopathy ND- non-distendedM/R/G- murmurs, rubs, gallops HSP- hepatosplenomegalyNBS- normal bowel sounds R/G- rebound tenderness, guardingC/C/E- clubbing, cyanosis, edema PERRLA- pupils equal, round, reactive to light andAAO- awake, alert, oriented to accommodation
person, place, & time ISS- Insulin Sliding ScaleC/W-consistent with EOMI-extraocular movements intactPO- by mouth PR- per rectumW/R/R-wheezes, rales, rhonchi
Sample Admission Note
Admission Note
CC: ― My chest hurts‖
HPI: 49 y/o woman complaining of chest pain that started approximately 2 hours ago. She describes the pain as starting in the substernal region and radiating to her left shoulder. The pain is stabbing in nature and is rated as 8/10. The pain has not changed since it started and she has not taken any medications to try to alleviate the pain. The patient does not associate anything with the onset of the pain, including exercise, trauma, or food. She denies shortness of breath, nausea, vomiting or diaphoresis associated with the pain.Past Medical Hx: Migraine headaches since the age of 35 that are managed with over the counter meds.
Surgical Hx: Tubal ligation approximately 15 years ago
Family Hx: Father- deceased at age 79, cerebral vascular accident x2 and kidney disease Mother- HTN, Hypercholesterolemia, MI at age 7311 siblings- all in good health according to patient
Social Hx: unemployed, married, son (28), daughter (21), Denies smoking, drugs, 3 beers/month x 20 yrs.
ROS: general- denies significant weight change, fatigue, or night sweats Skin- denies rashes, sores, or discolorations
Head- admits to headaches, denies changes in visionEyes- denies blurring, itching, or irritationEars- denies earache, tinnitus, or discharge
25
Sample Notes & Clerkship Pearls
Nose- admits to sneezing and runny nose for past weekThroat- denies sore throat or hoarsenessRespiratory- admits to cough, denies shortness of breath, hemoptysis, or
wheezingCardiac- denies palpitations, dyspnea on exertion, orthopnea, or edema
GI- denies change in appetite, abdominal pain, indigestion, diarrhea, hematochezia, or melena
Urinary- denies frequency, urgency, or dysuriaGenital- last menses approximately 2 weeks agoMusculoskeletal- denies weakness or joint stiffness
PE: Vitals BP-137/79 HR- 69 T- 98 RR- 14General- 49 y/o woman appearing her stated age in moderate discomfort,
well developed with good hygiene and cooperative with exam Skin- no scars, tattoos, rashes or sores. 5 cm by 5 cm hematoma over
spine at T5 levelHEENT- normocephalic, atraumatic, pupils equal round reactive to light,
extraoccular movements intact, sclera white, conjunctiva clear, facial features symmetric, gross hearing intact, no sinus tenderness, no nasal discharge, buccal mucosa moist and pink with no ulcers or sores
Neck- supple, no lymph nodes appreciated, trachea midline, thyroid not palpable, no JVD, no carotid bruits
Heart- PMI at 5th intercostal space in midclavicular line, no thrills or lifts, S1 and S2 heard, no murmurs, rubs, or gallops, no pain to Palpation of chest wall
Lungs- symmetric expansion, no wheezes or crackles, clear to auscultation in all fields
Abd- no surgical scars, normal active bowel sounds, no tenderness topalpation, non-distended, no masses felt, tympanic in all quads
Musculoskeletal- normal range of motion, strength symmetric in upper andlower extremities, +2 pulses throughout
Neuro- alert and oriented x3, CN II-XII intact bilaterally, strength 5/5 throughout, sensation intact to light touch and temperature
Labs:
EKG- normal sinus rhythm X2Cardiac enzymes:
06:27 13:17 19:12CPK 371 277 213CPK-MB 11.1 7.8 4.4Troponin SC 0.5 0.6
Problem List:1. Left-sided chest pain
Assessment and Plan:1. Chest Pain- Patient‘s pain is not typical of ischemic myocardial pain. While some aspects of the pain are consistent,
acute onset substernal in origin and radiating to left arm, she did not describe typically associated symptoms and quality of pain is not what would be expected. All patients complaining of chest pain without an obvious cause must be ruled out for MI. This patient being female makes this step very important since women commonly have atypical presentations of acute ischemia. High on my differential is esophageal spasm as pain in appropriate location for this cause. This can be considered after cardiac origin is evaluated. Patient has no history of trauma and pain is not reproducible with palpation directing my differential away from a musculoskeletal source. A pulmonary source is also a possibility but is unlikely as patient has no pulmonary symptoms and pain is not pleuritic in nature. A chest x-ray is needed to assess this.
1. admit to telemetry2. get 3rd set of cardiac enzymes3. chest x-ray4. morphine 1-2mg Q4-6 hours prn chest pain
26

5. Tylenol extra strength prn headache6. nitroglycerin sublingual up to 37. aspirin 325mg8. fasting lipid panel to establish cardiac risk
The key to this note is the discussion of the possible causes of the patient’s chief complaint.
CXR- negCardiac Enz- T, CK, CK-Mb neg x 3EKG- NSR with ST segment depression in AVF, II, IIIECHO- dec movement of the inf wall, with ejection fraction (Ef) of 22%
A/P1. Ischemia- Con‘t telemetry. Pt scheduled for cardiac cath tomorrow. Con‘t Nitro PRN, Aspirin, and
Labetalol.2. HTN- Suboptimally controlled, elevations most likely due to episodes of CP. Con‘t HCTZ and
Lopressor. Add Catapress if SBP >180 or DBP >100.3. DM- follow ISS4. Hyperlipidemia- order lipid profile for tomorrow‘s AM labs. Con‘t Lipitor.
* Leave room for resident to add stuff
Signature and CC-3 Print Last Name
Hints· Write in black in;, start your note at the second vertical line (not at the M.D. line)· S (subjective) is what the patient tells you. O (objective) is the flow sheet and your exam.· Vital Signs- are usually recorded in ranges and the current measurement· Problem List includes all the patient’s medical problems. The A/P problems are only those that are pertinent to the
patient’s reason for being admitted.· Meds are the medications the patient is currently taking in the hospital. If the patient is on antibiotics, list the number
of days completed over the number prescribed (ex. Bactrim 4/7)
27

This is the framework for your standard clinic note, specifically geared towards primary care visits. You will get a lot of experience with clinic notes on all rotations, but it is the only format you will use on GPC and Family Medicine. Keep this in mind for pediatrics as well, since outpatient peds is really a primary care clinic. Just remember that health maintenance in peds patients mainly consists of vaccinations, and there are developmental milestones you should screen for at annual physical visits.
Chief Complaint: record whether it is a first time visit (with complaint), or for follow-upPatient is a 40 y.o. white Cuban male with a history of diabetes, hypertension and hyperlipedemia.1.Any new problems2.Diabetes-3.hypertension-4.hyperlipedemia-5.Health Maintenance-women: last pap, mammogram, bone density (if post-menopausal)men: last PSA, DREboth: last hemoccult, colonoscopy or flex siglipid profile (if not addressed previously)other appropriate health maintenance for particular disease processes, i.e.last optho exam, HbA1C, microalbumin and vaccines in a diabetic patient
current meds- drug allergies-
If first visit:med hx, surg hx, social hx
P/E: Vitals-Unless its the first visit, do a focused physical exam. Cardiac, pulmonary and abdominal exams are always included.
A/P:(Assessment and Plan)
1.Assess any new problems-explain what you think is going on and why. What labs/studies you'll need in order to confirm or refute your hypothesis. Whatare you doing about it today?
Assess old problems one at a time-Is the patient optimally or suboptimally controlled and why? Are you making any changes in their current regimen? Include any labs, studies, referrals that are needed.
2.Diabetes-3.Hypertension-4.Hyperlipedemia-5.Health Maintenance 6.Return to Clinic (RTC)-
Specific Specialty Considerations for Your Notes See each specialty chapter for more information.
OB/GYN- Obstetric history:
G=Gravida: the number of total pregnancies (twins count as a single pregnancy)P=Para: pregnancy outcomes described as FP And L(HINT: as in Florida Power And Light)
Full term deliveries (pregnancies > or = to 37 wks)Pre-term deliveries (viable pregnancies <37 wks)Abortions (spontaneous or medical; includes ectopic)Live births (only place where twins are counted separately)
28
Sample Clinic Note
In addition, movement of baby, vaginal bleeding/discharge, STD history, and screening tests must be recorded. See OB/GYN section for more details about prenatal care/screening.
- Obstetric physical: must include Fetal Heart Rate, fundus height (if > 16 weeks), and possible pelvic exam if warranted by symptoms- GYN/GYO history: again, you want to ask about the general obstetric history, as well as history on GYN problems, including last period, if they are regular, if they are heavy/moderate/light (# of pads used/day is a good way to quantify), history of STD‘s, and when their last Pap and Mammogram was.- GYN/GYO physical: will mainly constitute a pelvic exam, assessing the vagina, cervix, uterus, and adnexa, all of which should be mentioned in the clinic note
Surgery
- Regardless of your service, like everything else on surgery, these notes should bedirected towards the patient‘s problems, whether it is pre-op or post-op.- For pre-op visits, make sure that the patient does not have any medical problems that will require an evaluation for clearance for surgery. If so, you will most likely have to refer them to a medicine clinic for clearance. Those details will be determined by your team.- Post-op: Note antibiotic day number out of total days (ex: Keflex day 3/7), infection screening (ex: wound clean/dry/intact), N/V, flatus/bowel movements, fever/chills. Many of these factors are important on the inpatient wards.
Pediatrics-As mentioned above, pediatrics clinic notes will not differ that much. Remember the vaccination schedule, and remember to screen for developmental milestones. In addition, you will have to counsel parents concerning their child‘s illness, as well as anticipatory guidance for what to expect over the next year from their child. That includes warnings about potential dangers around the home, and safety precautions parents should take.
29

Appendix E Oral Presentation Pearls
During your clerkship, it is important to master the delivery of a focused, fluent, and concise oral presentation. When done effectively, the oral presentation leaves your audience with a solid comprehension of your patient‘s health care issues. Take the time to really understand what is going on with your patient and to organize and synthesize the data into a story that your audience will also understand. Furthermore, body language, eye contact, posture, etc. all contribute to a polished presentation.
The formal presentation (admission presentation) : The structure of your formal oral presentation is the same as your admission note, though no time should be wasted on superfluous information. More emphasis should be given to the patient‘s current state (CC, HPI, PE, labs, A/P) than to past events (PMH, FH, SH), unless they are relevant to the current state. The review of systems is a component of your written note that is not presented orally. Anything in the ROS worth reporting should have already been mentioned in the HPI. This presentation is longer than your daily presentation, as it is the first time the audience is learning about the patient.
Presenting on daily rounds: This presentation recounts the information in your daily progress note, in the same format. Often you present only pertinent positives and negatives in the physical exam.
Each rotation will have specifics they will want you to include in your notes as well as in your oral presentation. These are usually outlined in your formal orientation to each area. Above all, listen to the interns and residents on your team to get an idea of what your attending wants to hear in your presentation. This is also a good way to learn how not to present a patient! Remember, the oral presentation takes lots of practice. No one expects you to be perfect the first few times you present-- just take a deep breath and do your best!
30
Course Texts Pocket Reference Q&As
Surgery Lawrence, NMSSurgery Recall,Surgery Secrets
Lawrence, A&L, Pretest
Medicine
Cecil‘s Essentials of Medicine,
**Pocket MedicineWashington Manual
Mosby‘sA&L, Pretest
Harrison‘s Principles of InternalMedicine, NMS, MKSAP, Erbella, RapidInterpretation of EKG‘s (Dubin), CaseFilesCurrent Medical Diagnosis & Treatment
NeurologyNeurology: an Illustrated Colour Text Neurology in Clinical
PracticeSimon‘s: Clinical NeurologyCollins: Neurology
PsychiatryBRS, Kaplan and Sadock, First Aid, Case Files
CurrentClinical Strategies:
PsychiatryA&L, BRS, Pretest
GPCSyllabus contains latest treatment guidelines
Family Medicine
Essentials of Family Medicine NMS questions
OB/GYN Beckman‘s, Blueprints, Case Files
Current ClinicalStrategies:
Gynecology andObstetrics
A&L, Lipincott‘s,Not Pretest
Pediatrics Blueprints, Nelson‘s Essentials of Clerkship Series:Pediatrics
A&L, PretestPediatrics, Case Files, First AidGeriatrics Syllabus
AnesthesiologyThe ―Anesthesia‖ chapter from Lippincott‘s Pharmacology
Step II Review Books
Prescription for the BoardsSecrets for Step IIBoards & WardsNMS Question BookCrush Step II (Bochert)UCV Step IISome used Blueprints for Peds & OB/GYN for more of a review
Boards and Wards is a good pocket reference, as is the Scutmonkey series.
Maxwell‘s Pocket Reference Guide is extremely useful to have in your pocket for quick reference for lab values, equations, format for notes, etc. Spend some time looking through it before putting it in your pocket and forgetting about it!
Additionally, many people use Erbella for oral exams although care must be taken as some of the information is outdated. Just make sure you edit it as you study.
In many rotations you have to present topics to the team. Many people find good information on-line: MD Consult and on-line journals. Emedicine is good. Medline will be useful. Uptodate is now available through Calder Library. If you are on campus you can simply go to the website www.utdol.com . This source will be extremely valuable to you during your rotations and your career.
Appendix F Recommended Books
31

Chest FilmsApproach:
Marker: Locate and verify position with the apex of the heartInspiration: Need at least 9 ribs showing for an adequate view of lung fields Exposure: Underexposed – too bright and cannot see spine behind heart
Overexposed – too black and cannot see vessels in lungsRotation: Distance between medial ends of clavicles and spinous process should be equal Search Pattern:
1. Bones2. Begin at the lower left diaphragmatic recess and travel up the
left heart border, aortic knob to trachea and then down the ride side of the mediastinum to the right diaphragm. Then arch around the edges paying attention to the apices.
3. Examine lung fields and correlate anatomy from AP view with lateral view
Findings:1. Silhouette Sign: water density (pneumonia) overlaps heart border, so you lose the silhouette.
Right heart border: RMLLeft Heart Border: Lingula (LUL)Right Hemidiaphragm: RLLLeft Hemidiaphragm: LLLDescending Aorta: LLL
1. Air BronchogramsAir in bronchi is seen because surrounding alveoli are full of Pus/Blood/Fluid (pneumonia, hemorrhage, pulmonary edema)
2. Kerly B Sign (Line):Horizontal water density lines at periphery always extending to the pleura that is representative of increased fluid density in the interlobular septa. Think pulmonary edema (CHF) or lymphatic system tumor (lymphangitic carcinomatosis)
3. SnowBall: if fully round probably something originating in the lung; if splattered against the side most likely originating from an extra-pulmonic source such as the chest wall, pleura, or mediastinum.
Lung Disease PatternsInterstitial: innumerable thin white linesAirspace: patch of white opacity – consolidationHoneycomb: long standing interstitial lung diseaseMiliary: innumerable pellet sized white densities bilaterallyAtelectasis: collapse of lobes, white patchy density secondary to obstruction, compression or traction.
Widened Mediastinum:Aortic Aneurysm/Mediastinal Hematoma. Blurred aortic arch, bilateral apical caps, displaced mainstem bronchus downwards.
Increased Heart shadow: cardiomegaly secondary to CHF, cardiomyopathy or pericardial effusion.
Appendix G Reading CXR‘s
32
1. RATE"300, 150, 100" ..."75, 60, 50" but for bradycardia:· Cycles/6 second strip X 10 = Rate·Tachycardia = more than 100/min·Bradycardia = less than 60/min· Dissociated Rhythms: rhythms may co-exist
2. RHYTHMIdentify the basic rhythm, then scan tracing for prematurity, pauses, irregularity, and abnormal waves.
· Check for: P before each QRS. QRS after each P.· Check: PR intervals (for AV Blocks). QRS
interval (for BBB).If Axis Deviation, rule out Hemiblock.
3. AXISFor Axis in degrees, find isoelectric QRS in a limb lead of Axis Quadrant using the "Axis in Degrees" chart.
4. HYPERTROPHYCheck P Wave for atrial hypertrophy.Check R wave for Right Ventricular Hypertrophy.S wave depth in V1+ R wave height in V5 if >35mm = Left Ventricular Hypertrophy.
5. INFARCTIONScan all leads for: Q waves, inverted T waves, ST segment elevationQ wave = Necrosis
A significant Q wave is 0.04 seconds in duration (one small square wide) or is 1/3 the amplitude of the QRS complex.
Old infarcts: significant Q waves remain for a lifetime.Acute Injury: ST segment elevation or depression (ST segment returns to baseline with time.)T wave inversion = Ischemia
Appendix H Reading EKG's
33

Always obtain patient's previous EKG's for comparison
34

Appendix ILab Values
______________________________________________________________________________
BloodNormals Normals Endocrinology Normals
WBC 4.5 – 11 PT 11-15 Aldosterone 3-10 supine5-30 upright
Hgb 13.5 –17.5 (M)12.0 – 16.0 (F)
PTT 20-35 Cortisol 0800h 6-231600h 3-15
2200h 50%of 0800 hHct 39-49 (M)
35-45 (F)Bleeding Time
2-7 min Estrogen Follicular 60-200Luteal 160-400
Menopausal <130Plt 150-450 TT 6.3-11.1 FSH Follicular 1-9
Ovulation 6-26Luteal 1-9
Menopausal 30-118MCV 80-100 ESR M<15 F<20 Gastrin <100Na 135-145 ALK P 38-126 (M)
70-230 (F)GH <2 (M)
<10 (F)K 3.5-5.1 SGOT 7-40 LH Follicular 1-12
Midcycle 16-104Luteal 1-12
Menopausal 16-66Cl 98-106 SGPT 7-40 Progesterone Follicular 0.15-0.7
Luteal 2.0-25HCO3 22-29 GGT 9-50 (M)
8-40 (F)Prolactin <20
BUN 7-18 CPK MB
<5% PTH 10-65
Cr 0.6-1.2 Fe 65-175 (M)50-170 (F)
Testosterone Free-52-280Total 300-1000
Glu 70-115 TIBC 250-450 T4 Total 5.0-12.0Ca total 8.4 – 10.2 Fe sat 20-50 (M)
15-50 (F)T4 Free 0.8-2.3
Ca ionized 4.65-5.28 Ferritin 20-250 (M)10-120 (F)
T3 100-200
Phos 2.7-4.5 Vit B12 100-700 TBG 15-34Magnesiu m
1.3-2.1 Folate 3-16 TSH <10
Protein 6.0-8.0 PSA <4.0Albumin 3.5-5.5 Acid
P<0.8
Alpha- fetoprotein
<10 Cu 70-140 (M)80-155 (F)
Synovial Fluid
Bilirubin, total
0.2 –1.0 CA-125 <35 WBC <200
Bilirubin, direct
0-0.2 CEA <2.5 Trauma/OA/SL E
<3000>4000
Gout/RA >60000Septic
Lipase 10-140 Lithium 0.6 – 1.2 Protein <3.0Amylase 25-125 Vanco 20-40 Glucose >40C-peptide 0.7-1.89 Digoxin 0.8 – 2.0 Uric Acid <8.0T Chol <200 Urine LDH <Serum LDH
35
Cl
NCO2K
BUN Glu WBC Hgb PltCr Hct

LDL <130 Min volume
0.5-1.0mL/h
HDL >35 SG 1.002-1.030Trigs <100 Osmol 50-1400Lactate 5.0-20.0 Cr
mg/kg/d14-26 (M)11-20 (F)
Uric Acid 3.5-7.2(M)2.6-6.0 (F)
Urea Nitroge n
12-20 g/d
Ammonia 10-50 Na 40-220LDH 90-190 K 25-125
Appendix JFluids, Electrolytes and TPN
Daily requirements: Na+ 1-2 mEq/kg/dayK+ 1 mEq/kg/dayWater 1500cc per m2 or 100cc/kg/day for the first 10kg
50cc/kg/day for the second 10 kg10 cc/kg/day for each kg after that(some people like to use 20cc/kg/day for after the first 20kg)
After calculating the maintenance fluids and electrolytes, one must add the losses.Mild Moderate Severe
Percent dehydrated <5% 7-10% 12-15%MEq/L Na depleted 6 9 12
HR nl
RR nl
BP nl nl nlpreshock HTNshock hypoTN
Sensorium Nl Lethargic Coma/semicomaSkin Turgor (abdominal) Nl Poor
DrySunken2-3 sec.
Very poorParched
Very sunken>3 sec.
Mucosa Nl/dryNl
<2sec
NlNl
Eyes/fontanelCapillary Refill
(big toe)Urine Volume
Urine Concentration
For each liter of NG tube suction: 70 mEq/L of Na and 20mEq/L of K needs to be replaced For each liter of diarrhea: 40 mEq/L of Na and 40 mEq/L of K needs to be replaced
Add up total water, Na and K needed for maintenance and replacement and divide by 24 to get the number of cc/hr and what amount of electrolytes per hour. The amount of electrolytes needed will dictate which fluid to use.
For TPN nutrition:25 calories per kg1-2gm protein30% of calories from fat (40% if patient has COPD or CHF for a lower respiratory
quotient, 20% if liver disease or septic)
Example: 100kg patient who has lost 1.5L from NGT and 1.0L of diarrhea that requires TPN.2.4 L (given) 1.5 L NGT 1.0 L Diarrhea/T- 4.9 L fluid
Tube150 Na 1.5 x 70 = 105 1.0 x 40 = 40 295 mEq/L Na100 K+ 1.5 x 20 = 30 1.0 x 40 = 40 170 mEq/L K
100 kg x 25 cal/day = 2500 calories 100 kg x 2gm protein = 200
Total Calories Fluids3500 4900
37

Step 1: Calculate number of calories from fat. In this case 30% of 3500 = 1050 calories from fat. Since lipids comes as 20% lipid emulsion which is 2 calories per cc, 1050 calories / 2cal/cc is 525 cc of fluid. Divide this by 24h to get 22cc/hr of 20% IL.Subtract the calories and volume from fat from the running total:
2450 cal 4375 cc
The rest of the fluid will contain the AAs, glucose and electrolytes
Step 2: Calculate the percentage of amino acids that will be needed in the TPN, in this case 200 grams divided by the remaining 4375 cc equals 45g/L. TPN uses old nomenclature for AAs of percentage of 100cc – so 45g/L equals 4.5% (grams per 100cc).
Step 3: Subtract the calories of the amino acids from the total calories remaining: 4375 –200g(4cal/gram) = 2450 – 800 = 1650.
1650 cal 4375cc
Step 4: Remaining fluid and calories are given in the form of dextrose. 1650 cal/ 3.4cal/gm glucose = 485 gm of carbohydrates. 485cal/4375 cc fluid = 110g/L of sugar. This is also written in the old nomenclature of %g/100cc , therefore 110g/L = 11g/100cc = D11. The volume, 4375/24hr, gives the run rate of 180cc/hr.
Step 5: Calculate the amount of electrolytes to be added. Then taking into account the electrolytes needed: 295 of Na into aprox 5L total fluid = 60mEq/L Na, 170 of K into 5L = 40mEq/L.
TPN orders= D11 with 4.5%AA TRA (to run at) 180cc/hr, 22cc/hr of 20%IL plus 60mEq/L Na and 40mEq/l of K
Common Replacement Fluids:
Glucose (g/L)
38
Fluid mEq/L N a K C l H C O3
Ca Kcal/L

Appendix JFluids, Electrolytes and TPN
1/2 NS (0.45%) 77 7
170
50NS 154 154
D5W3403 9
100LR 130 4 110 28
D10W
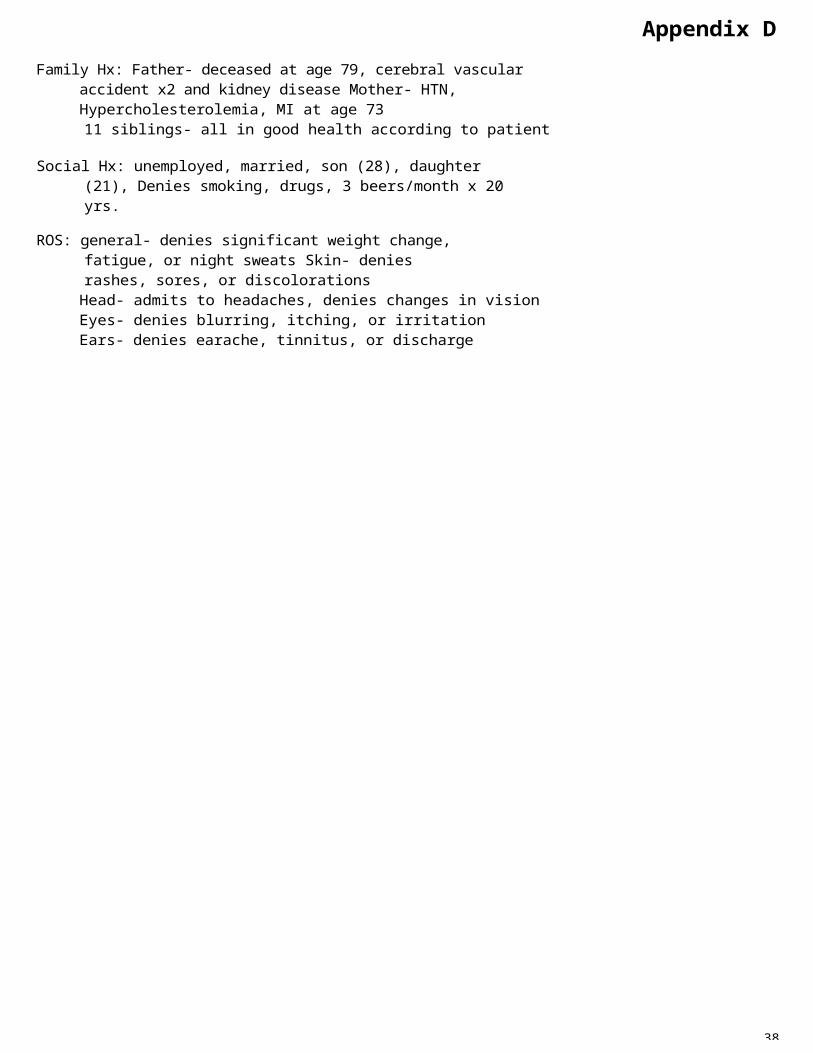
CSF WBC (polys) Glucose Protein Opening Pressure
Preterm 0 – 25 (<35%) 25 – 70 60 – 140
Infant 0 – 35 (<35%) 35 – 110 30 – 160 75 – 120
Child >4 weeks 0 - 5 ( 0%) 40 - 75 10 - 45 70 - 180
Total Bilirubin (mg/dL) Preterm Term
Day 1 <8 - 9 <6
Day 2 <12 <9
Week 1 <15 <10
Weeks 2-4 <10 - 12 <6
Osm = 2(Na) + (Glu/18) + (BUN/2.8) = 274 – 296
Appendix K Pediatric Tables
41
Pulse BP Resp Wt(kg)
WBC Hbg Hct
Preemie 130-160 45-60 40-60 <3 28 wk 14.5 45
Term 120-150 60-70 30-60 3-4 32 wk 15 47
3 mos 120-140 60-100 30-50 5-6 Term 8 - 30 13-20 40-58
6 mos 120-140 65-120 25-35 7 1-3 day 9 - 32 14 – 22 45 – 60
1 year 120-140 70-120 20-30 10 2 wk 5 - 20 10 - 20 40 – 58
1 1/2year
110-135 110-135 20-30 11 1 mos 5 – 19.5 11-18 32 - 54
2 year 110-130 110-130 20-28 12 2 mos 5 - 19 10 – 15 28 - 44
3 year 100-120 100-120 20-28 14-15 6 mos 6 - 18 10 - 14 30 - 42
4 year 95-115 95-115 20-28 16-17 6 mos – 2year
5 - 18 10 - 13 32 - 40
6 year 90-110 90-110 20-25 20 2 – 6 year 5 - 15 11 -14 33 - 40
10 year 75-95 75-95 16-24 30-32 6 – 12 year 4 - 14 11-15
14 year 60-90 60-90 15-20 45 12-18 year
SGOT (AST) LDH
Term 25 – 125 150 – 600
20 – 60 140 – 350Infant
Child 10 - 40 140 - 280

Appendix L H&P Review
42
HISTORY
ID age, sex, DOB, medical #Source & Reliability of Info SELF, FAMILY,
MEDICAL RECORDCC reason for seeking careHPI chronological order; setting/ location/timing (onset, duration, frequency) /quality/severity/ aggravating or alleviating factors/ associated Sx; evaluation/treatment; pertinent negatives/relevant FHx, risk factors, and lab valuesPMH general health/ childhood illnesses and complications/adult illnesses/ hospitalizations/accidentsPSH type, date, reason and outcome, transfusions, complications MED‘S:name/dose/frequency/ duration/reason/complianceALLERGIES med‘s/ rxn‘sFH (1st degree = parents, sibs, kids) age and health statusSH birthplace/cultural background/education/marital status/occupation/ religion/ living environment/hobbies/ economic resourcesHEALTH HABITS (type, amount, frequency, duration, rxn‘s, Tx) tobacco/alcohol/illicit drugs/diet/ exercise/toxins/sexual lifestyle (gender, STD‘s, #)PGYNH menarche/LMP/menses (frequency, duration, amount, dysmenorrhea)/menopause (age, Sx,HRT)/ contraception/sexual lifestyle (gender, STD’s, #)POBH: gravida, parity/type of delivery/birth weights/ complicationsHEALTH MAINTENANCE last PE & labs/self-exams/Pap/ MMG/hemoccult/sig or col/PSA/DRE/ immunizations/ lipids/PPD
* PEDIATRICS developmental milestones pmh (prenatal hx, birth hx, neonatal hx)/feeding
General weight change, fatigue/energy, fever, chills, weakness, night sweats, desired weightSkin, Hair, Nails changes, rashes, itching, sores, lumps, moles, pigment changesHead trauma, headaches, dizziness, N/V, loss of consciousnessEyes glasses/contacts, visual changes, trauma, blurriness, double vision, itchingEars hearing loss, pain, discharge, tinnitus, vertigoNose congestion, rhinorrhea, sneezing, itching, epistaxis, postnasal drip Mouth, Throat, Neck bleeding gums, sore throat, hoarseness, ulcers, tooth problems, swollen neck, neck pain Respiratory cough, sputum, SOB, dyspnea on exertion, wheezing, hemoptysis, TB exposureCardiac chest pain, palpitations, orthopnea, paroxysmal nocturnal dyspnea, # of pillows, exercise toleranceGI difficulty eating, abdominal pain, heartburn, N/V, dysphagia, bowel regularity/changes, stool color, diarrhea, constipation, bleeding (hematemesis, hemorrhoids, melena), jaundiceMusculoskeletal joint pain, stiffness, muscle weakness, range of motion, instability, swelling, redness, warmth Neurologic loss of sensation, numbness, tingling, tremors, weakness, fainting, seizures, loss of coordination/falls
ROS
Lymph tenderness, enlargementVascular edema, claudication, varicose veinsBreasts skin changes, masses/lumps, pain, dischargeUrinary frequency, hesitancy, urgency, polyuria, dysuria, straining to void, hematuria, nocturia, incontinence, stones, flank pain, dribbling Genital Male – penile discharge or sores, testicular pain or masses, hernias, libido, infertility, erectile problemsFemale – itching, bleeding, discharge, sores, sexual interest and functionEndocrine heat/cold intolerance, weight change, xs sweating, polyuria, polydipsia, polyphagia, hair changes Hematologic anemia, easy bruising/bleeding, petechiae, transfusions Psychiatric depression and other mood disorders, anxiety disorders, personality disorders, cognitive disorders (dementia, delirium), psychotic disorders, memory, concentration, sleeping, socialization, suicidal

PHYSICAL EXAMINATION * R Side (Pt sitting, supine, L lateral decubitus, sitting, standing)VITAL SIGNS height, weight, BP, HR, CARDIAC rate, rhythm/ murmurs, RECTAL perianal, anus/ sphincterRR, temp gallops, rubs, clicks/ tone, rectal walls, masses/FOBT/GENERAL APPEARANCE sex, race, age, weight, state of health, stature, gait, development, dress, hygiene, affect
S1, S2, splitting/precordial movements (PMI, lifts, thrills)/ JVD/carotid pulses and bruits
Male – prostate consistency/Female – uterus, rectovaginal septum LYMPHATIC adenopathy: size,
SKIN, HAIR, & NAILS color, integrity, hygiene, turgor, hydration, lesions, scars, rashes, bruises, tattoos/hair distribution, texture/ nail texture, clubbing, pitting
BREASTS (sitting and lying)skin changes, symmetry, tenderness, masses, dimpling, discharge, nipples, areolae, axillary nodes, infra and
shape, warmth, tenderness, mobility, consistency (occipital, posterior auricular, cervical – anterior, posterior, infra and
HEAD size, shape, trauma, deformities, symmetry/sensation (CN V)/temporal arteries/glands (parotid, submandibular, sublingual)/jaw, masseter muscle (CN
supraclavicular nodesVASCULAR cyanosis, clubbing, edema/pulses – amplitude, symmetry (carotid, radial, femoral, popliteal,
supraclavicular, axillary, epitrochlear, inguinal) NEUROLOGIC mental status /cranial nerves (I-smell; II-visualV)/sinuses (maxillary, frontal)/CN VII posterior tibial, dorsalis pedis)/JVD, acuity, fields, fundoscopy;
NECK supple or firm/trachea/ROM/ carotid bruits/varicose veins III,IV,VI-eyelid opening, pupilspine/CN XI/thyroid/cervical nodes/ masses
ABDOMEN contour, symmetry, scars, reflexes/bowel sounds, bruits,
constriction, EOM; V-facial sensation, corneal reflex, jaw
EYES external ocular structures(eyelids, conjunctivae, sclera, cornea)/red light reflex/pupils (symmetry, shape, size, direct
hum/aortic pulsation/ percussion tone opening, bite strength; VII-eyebrow raise, eyelid close, smile, frown, pucker, ant taste; VIII-auditory
(tympany, shifting dullness, liver span, liver border, spleen)/palpate
and consensual constriction – CN II liver, kidneys, spleen, masses/ acuity, Rinne, Weber, reflexes; IX,&III)/EOM‘s (CN III, IV, VI)/corneal reflex (CN V & VII)/visual acuity (CN
consistency (soft, firm)/ tenderness (guarding, light, deep, rebound,
X-gag reflex, palate elevation, swallowing, post taste, phonation;
II)/visual fields/accommodation and referred)/CVA tenderness/femoral XI-lateral head rotation, neckconvergence/funduscopy/nystagmus pulses/ inguinal nodes flexion, shoulder shrug; XII-tongueEARS symmetry, shape, deformities/ lesions, tenderness, discharge/ auditory acuity (watch, rubbing, whisper -- CN
MUSCULOSKELETAL (back, hips, knees, feet, ankles, shoulders, elbows, fingers) posture/spine alignment and
protrusion, lateral deviation strength)/reflexes(biceps, triceps, brachioradialis, patellar, ankle,
VIII)/lateralization (Weber)/bone vs. air conduction (Rinne)/otoscopy (external canal, TM)
tenderness/CVAtenderness/symmetry/ paraspinous muscles/joint heat, swelling,
plantar)/sensation (light touch, dull, pain, temperature, vibratory, proprioceptive – Romberg, position
NOSE symmetry/tenderness/ discharge/mucosa/turbinates/ septum
color/muscle tone, atrophy/ROM/strength
sense, stereognosis, two point discrimination)/strength/
MOUTH & THROAT hygiene/ dentures/lips, teeth, gums, buccal mucosa, palate/erythema, exudates/ tongue (CN
GENITOURINARYMale – rashes, ulcers, scars, nodules, masses induration, urethral discharge/pubic
cerebellum(finger-to-nose, heel-to-shin, rapid alternating movements)/ gait(straight line, tandem, heels,
XII)/tonsils/palatal elevation (ah, CN IX & X)/uvula/gag reflex (CN IX, X)
hair/glans, penis, testis, scrotum, epididymis/hernias
toes)
CHEST & LUNGS (post, lateral, ant)respirations (rate, rhythm)/shape, symmetry, chest expansion/ accessory muscles/tactile fremitus, vocal fremitus, whispered pectoriloquy,egophony/crepitus/ percussion tone/diaphragmatic excursion/auscultation (clear, wheezes, crackles, rhonchi, rubs)
Female – vulva & vagina (rashes, lesions, inflammation, discharge, bleeding, ulcers, nodules, masses, introitus, vaginal walls)/ Bartholin and Skene glands/ urethra/cervix (position, lesions, discharge, CMT)/uterus (size, tenderness, masses)/adnexae (size, tenderness)/bimanual andrectovaginal palpation
* PEDIATRICS measurements (height/length, weight, head circumference + growth curve)
43

Appendix MPatient Record Sheets
Name:ID #: Age/Race/Eth: Room #:
HPI:PMH:
PSH:SH: FH:
MED’s:All:
Dx/Surgery:
/ /
POD#
/
POD#/ /
POD#/ / /
POD#Tm @
BPr
HRr
RRr
I/O
Sub
PE
Labs
A/P
Tc
BPc
HRc
RRc
Tm
BPr
HRr
RRr
I/O
Sub
PE
Labs
A/P
@ Tc
BPc
HRc
RRc
Tm
BPr
HRr
RRr
I/O
Sub
PE
Labs
A/P
@ Tc
BPc
Tm @
BPr
HRr
RRr
I/O
Sub
PE
Labs
A/P
Tc
BPc
HRcRRc
HRc
RRc
43
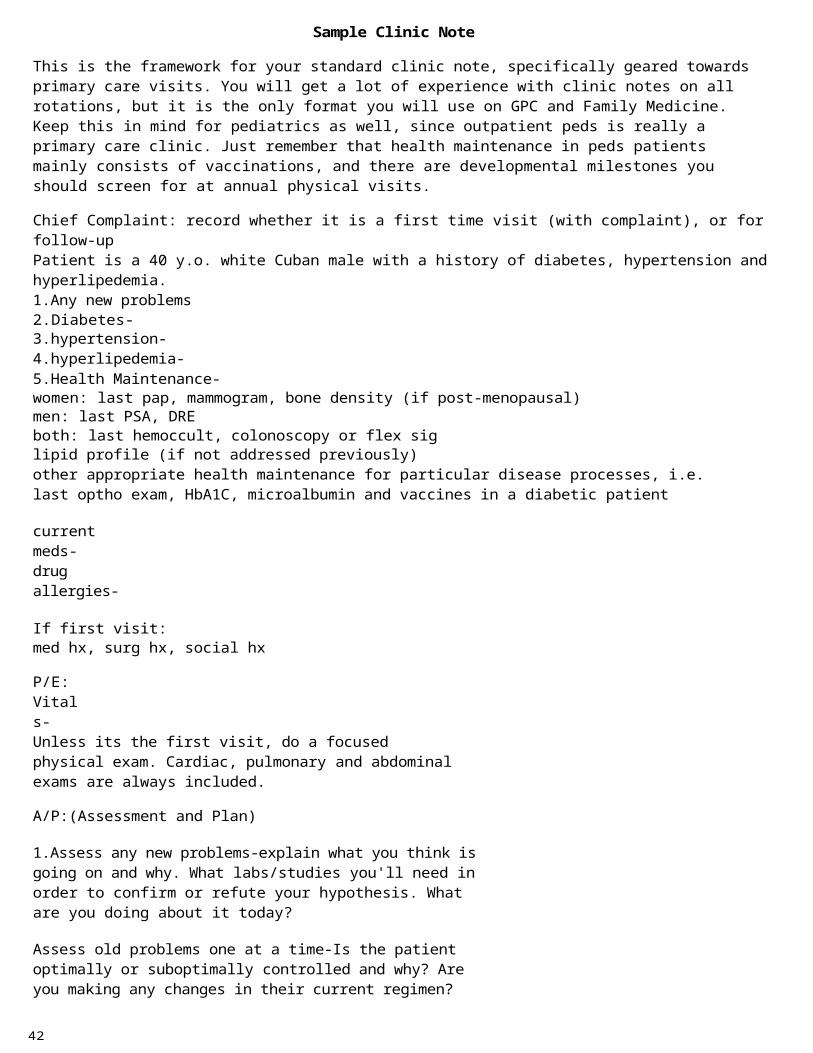
Pt. Identification: MR#: Room#:
S/P secondary to:
Date:HD/PODAbx Day
Tmax/TcBPHR/RRIns (IV type)Nutrition REG
NPOOutsFoley
Drainage Tubes NG Tube
BM/FlatusN/VTolerates DietLungs Cardio Abdomen
Wound ExtremitiesOther(Spirometry)Labs:CBC
P7
X-ray/CT/US
Assessment
Plan
Work List
44

NAME: ID #: ROOM
AGE: G P GA: LMP:
ALLERGIES:
MED'S:
U/S:
CC/Admitted For: PNC:
POBH:
PMH:
PSH:
FH:
SH:
HPI:
/ / D# GA / / D# GA / / D# GAS> S> S>
Tm
BPr
HR
FHR
@ Tc
BPc
RR
Wt
Tm @
BPr
HR
FHR
Tc
BPc
RR
Wt
Tm @
BPr
HR
FHR
Tc
BPc
RR
Wt
Bld Gluc
Bld Gluc Bld Gluc
Urine Urine UrineI/O> I/O> I/O>
PE> PE> PE>
LABS> LABS> LABS>
A: A: A:
P: P: P:
To Do: To Do: To Do:
45

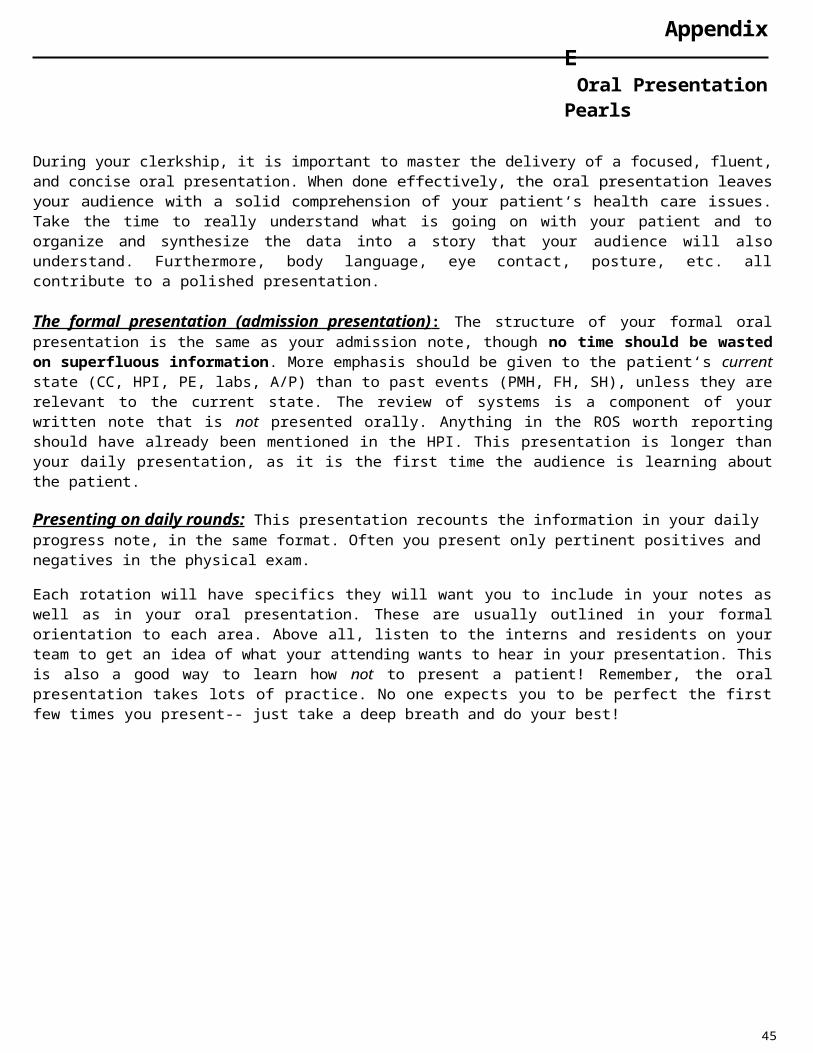
Important Forms in Jackson
1

2

3

4

5
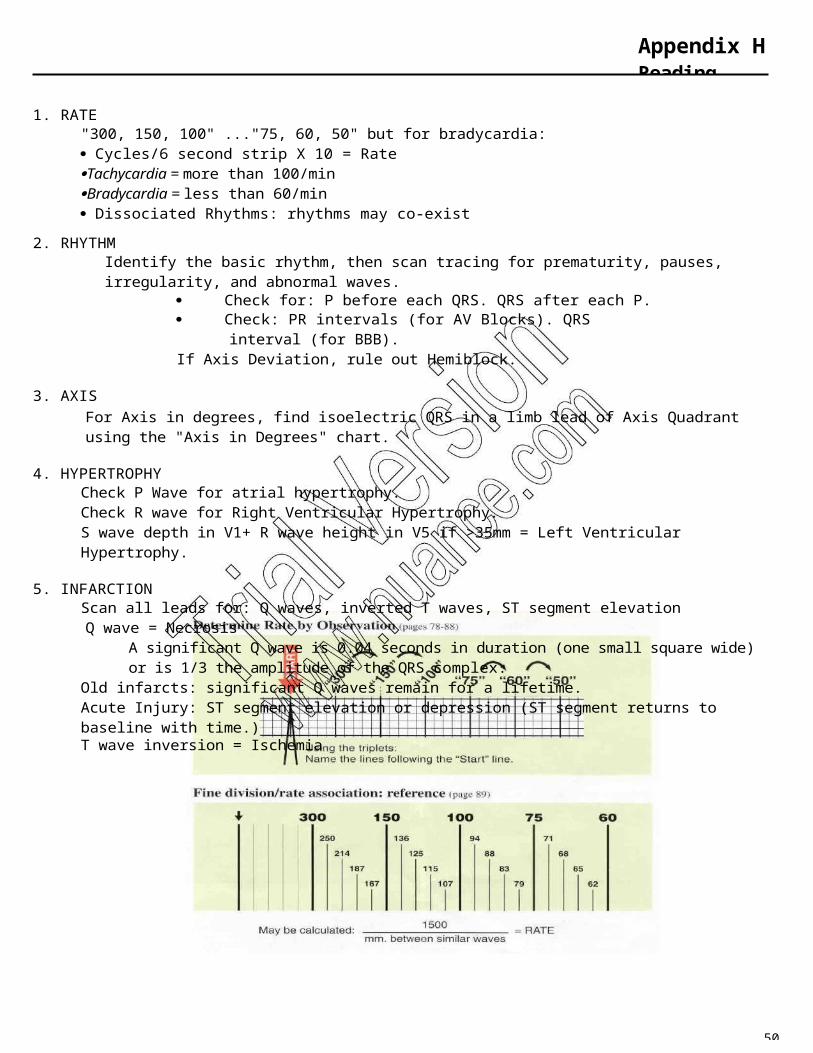
66
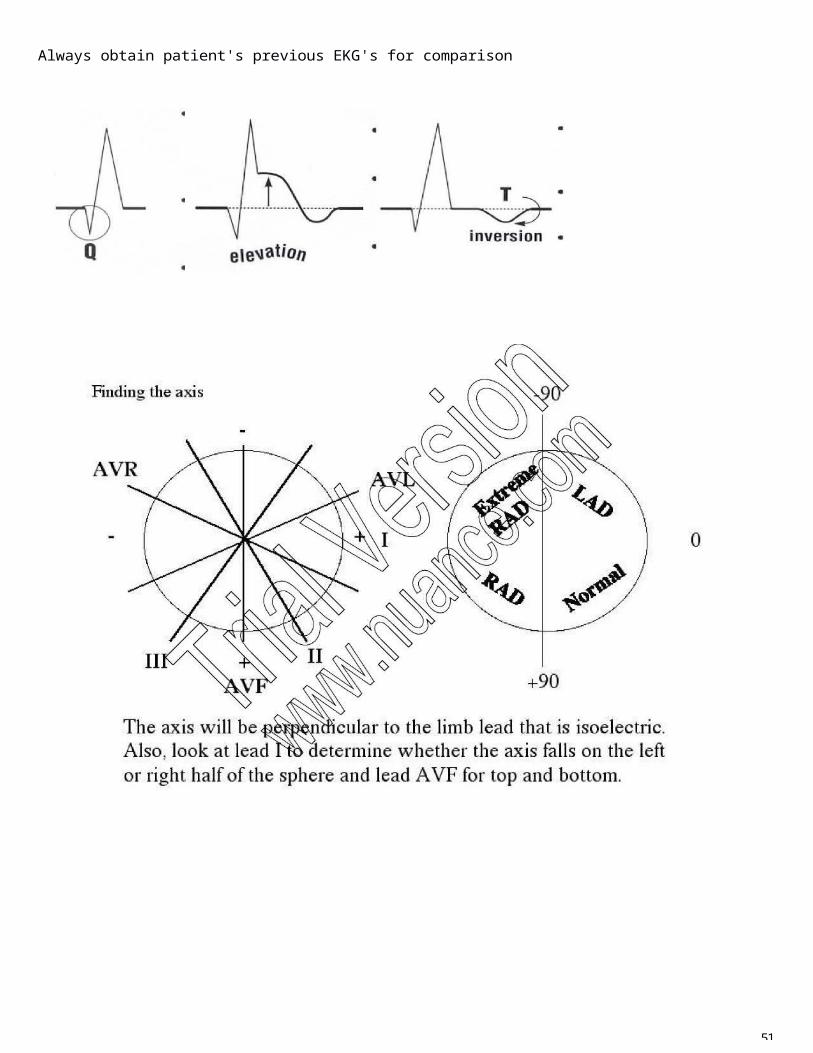
7

8

9
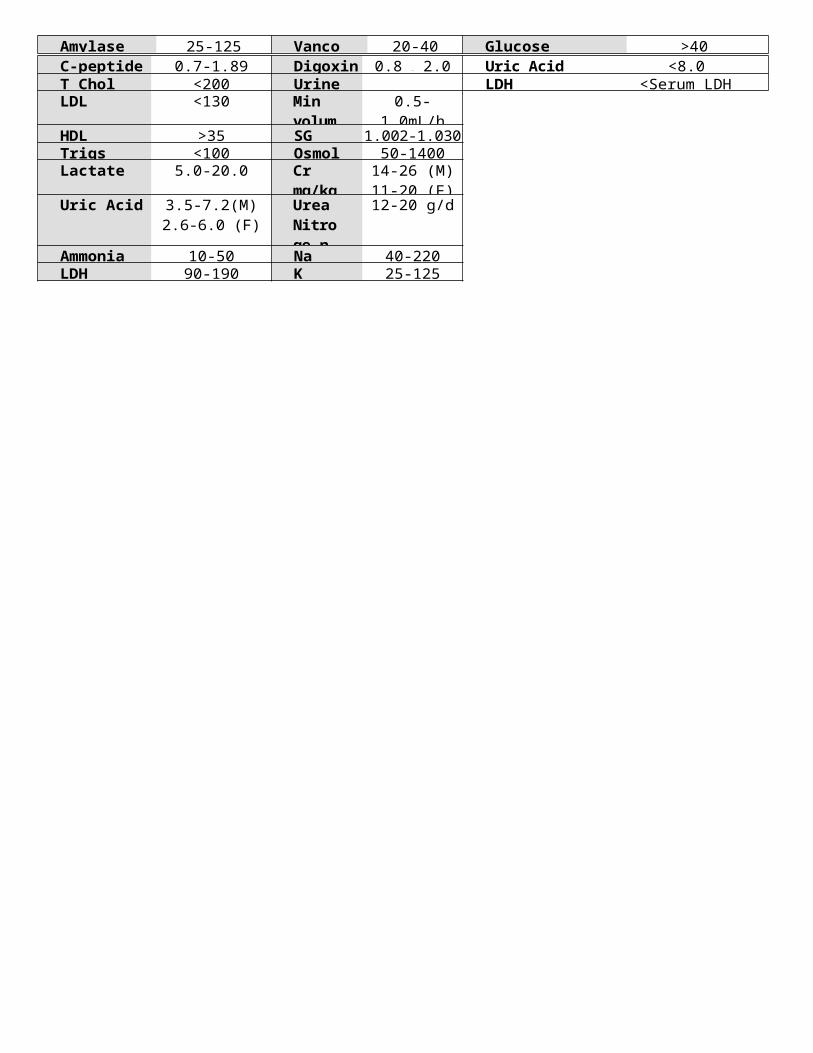
10

11
12