~clinical - uva health system department of anesthesiology clinic:alprivileges update form i have...
TRANSCRIPT









· r..w:=
, ~Clinical Privileges Update Form
DODald Mathes Department of Anesthesiology
I have reviewed the privileges previously granted to me and request the following changes to include any new therapies, procedures, or additional training necessary to perform new privileges requested. (please include supporting documentation to verify competency):
New Privileges to be Added (please indicate category level and type ofexperience):
:pf N~L~
Current Privileges not to be Renewed:*
__/..,..,ri. N l\ L~
j*Prlvlleges not renewed are not reported as being voluntarily relinquished unless this Is done while you are under Investigation; or, In return for not eonduetlng an Investigation or proeeeding. If privileges are to be reported IS voluntarily relinquished you will be notiDed and reeeive a eopy of the report to be ftled with the National Praetitloner Databank.
~.t).4i1A~DATE CLINICIAN S NATURE'-'t(. ~
As the Division Head/QI Liaison and Department ChajrlMedical Director, we have revie~ed the abovenamed clinician's level of experience, past performance and quality indicators (if renewing privileges) as related to requested privileges and agree that the above named clinician's qualifications are appropriate. Since the date of the last appointment, we have reviewed appHcable information from the following sources of quality and utilization data: '
We find as follows:
~Acceptable review with recommendation of reappOintment to the clinical staff with clinical privileges as requested
Concerns noted on review with corrective action plan In place with recommendation of reappointment to the clinical staff with privileges as requested, but subject to a review In __ months.
Should have clinical privileges granted but restricted as folio
~!41 (t,
~{, I ~ch
DATE
DATE

Mathes Department of Anesthesiology
Clinic:alPrivileges Update Form
I have reviewed the privileges previously granted to me and request the following changes to includeany new therapies, procedures, or additional training necessary to perform new privilegesrequested. (Please include supporting documentation to verify competency):
New Privileges to be Added (please indicate category level and type of experience):
Current Privileges not to be Renewed: *
• •••• ~. R', '.-_~ ~ ',.,. _~_~- ".__ ~'A~~_' .--.' , •••••""" ···~·.·4··-~-__ -.A-· .~ '_.~_.·_·.·.· .. h~,.·.·.~·~~"·'~~_~' ',_,~,'. ,-_., .' ..•. V._, v __ .•_v.·~ ~ , _••_._,'__ " •••• ~,., ", ••.__ •__
*Privileges not renewed are not reported as being voluntarily relinquished unless this is done while you are under investigation;~--'.or, in return for not conducting an investigation or proceeding. If privileges are to be reported as voluntarily relinquished you
vill be notified and receive a copy of the report to be filed with the National Practitioner Databank.
-.---z.LI{LL~__ --- . _DATE ~-~---
As the Division Head/QI Liaison and Department Chair/Medical Director, we have reviewed the above-named clinician's level of experience, past performance and quality indicators (if renewing privileges) asrelated to requested privileges and agree that the above named clinician's qualifications are appropriate.Since the date of the last appointment, we have reviewed applicable information from the following sources ofquality and utilization data:
We find a~ows:~_V;Acceptable review with recommendation of reappointment to the clinical staff with clinical privileges as
requested
Concerns noted on review with corrective action plan in place with recommendation of reappointmentto the clinical staff with privileges as requested, but subject to a review in __ months.
Should have clinical privileges granted but restricted as fo
DATE
DATE
Revised 3J1I2006

Donald Mathes Department of Anesthesiology
"U..NI..VER.SIT'x ..I.••. (I/\TIRGINIr\HEALTH SYSTEJ\1
Clinical Privih!ges Update Form
I have reviewed the privileges previously granted to me and request the following changes to includeany new therapies, procedures, or additional training necessary to perform new privilegesrequested. (Please include supporting documentation to verify competency):
New Privileges to be Added (please indicate category level and type of experience):
./)'\ 0 C\t'\0 (10ciL
Current Privileges not to he Renewed:*
/)'\{) C i/'\IAII\~
*Privileges not renewed are not reported as being voluntarily relinquished unless this is done while you are under investigation;or, in return for not conducting an Investigation or proceeding. If privileges are to be reported as voluntarily relinquished youwill be notified and receive a copy of the report to be filed with the National Practitioner Databank.
_'s 13'-"'-'-J-=.o----'o\'--'i ~~ /J/I.4....IL Y4()DATE CLINICIAN SIGNATURE 4~
As the Division Head/QI Liaison and Department Chair/Medical Director, we have reviewed the above-named clinician's level of experience, past performance and quality indicators (if renewing privileges) asrelated to requested privileges and agree that the above named clinician's qualifications are appropriate.Since the date of the last appointment, we have reviewed applicable information from the following sources ofquality and utilization data:
We fl2r'S follows:Acceptable review with recommendation of reappointment to the clinical staff with clinical privileges asrequested
D Concerns noted on re\liew with corrective action plan in place with recommendation of reappointmentto the clinical staff with privileges as requested, but subject to a review in __ months.
D Should have clinical privileges granted but restricted a
DATE
DATE
Revised 31112006

Donald Mathes Department of Anesthesiology
U~RSITY•• q;_VIRGINIA_ HEALTH SYsTEM
Clinical PriviIE~gesUpdate Form
I have reviewed the privileges previously granted to me and request the following changes to includeany new therapies, procedures, or additional training necessary to perform new privilegesrequested. (please include supporting documentation to verify competency):
New Privileges to be Added (please indicate category level and type of experience):
Current Privileges not to he Renewed: * .
No c\'\ ~d'\~
*Privileges not renewed are not reported as being voluntarily relinquished unless this is done while you are under investigation;or, in return for not conducting an lnvestigatlon or proceeding. If privileges are to be reported as voluntarily relinquished youwill be notified and receive a copy of the report to be filed with the National Practitioner Databank.
\- \"2.. -0 &DATE
As the Division Head/QI Liaison and Department Chair/Medical Director, we have reviewed the above-named clinician's level of experience, past performance and quality indicators (if renewing privileges) asrelated to requested privileges and agree that the above named clinician's qualifications are appropriate.Since the date of the last appointment, we have reviewed applicable information from the following sources ofquality and utilization data:
We find as follows:~ Acceptable review with recommendation of reappointment to the clinicalstaff with clinical privileges as
requested
D Concerns noted on review with corrective action plan in place with recommendation of reappointmentto the clinical staff with privileges as requested, but subject to a review in __ months.
o Should have clinical privileges granted but restricted as foil
[!}A"(v~ ~--------------~----------------------------
DATE ,
r~- __ ±Ut10gDATE
Revised 31112006

---<Privilege List for Clinical Staff08-Sep-OO DEPARTMENT OF ANESTHESIOLOGY
Name: ~o"""J...\J. -(\(\c..~(, 0,-0 1Date:
PLEASE MARK AS REQUESTED ONLY THOSE AREAS WHERE YOU ARE REGULARLY ASSIGNED TO PRACTICE;EMERGENCY PRIVILEGES SHOULD BE MARKED WHERE YOU ARE THE DESIGNATED PERSON TO COVER ANAREAIN WHICH YOU DO NOT REGULARLY PRACTICE. AREAS IN WHICH YOU DO NOT REGULARLY PRACTICE SHOULDBE LEFT BLANK
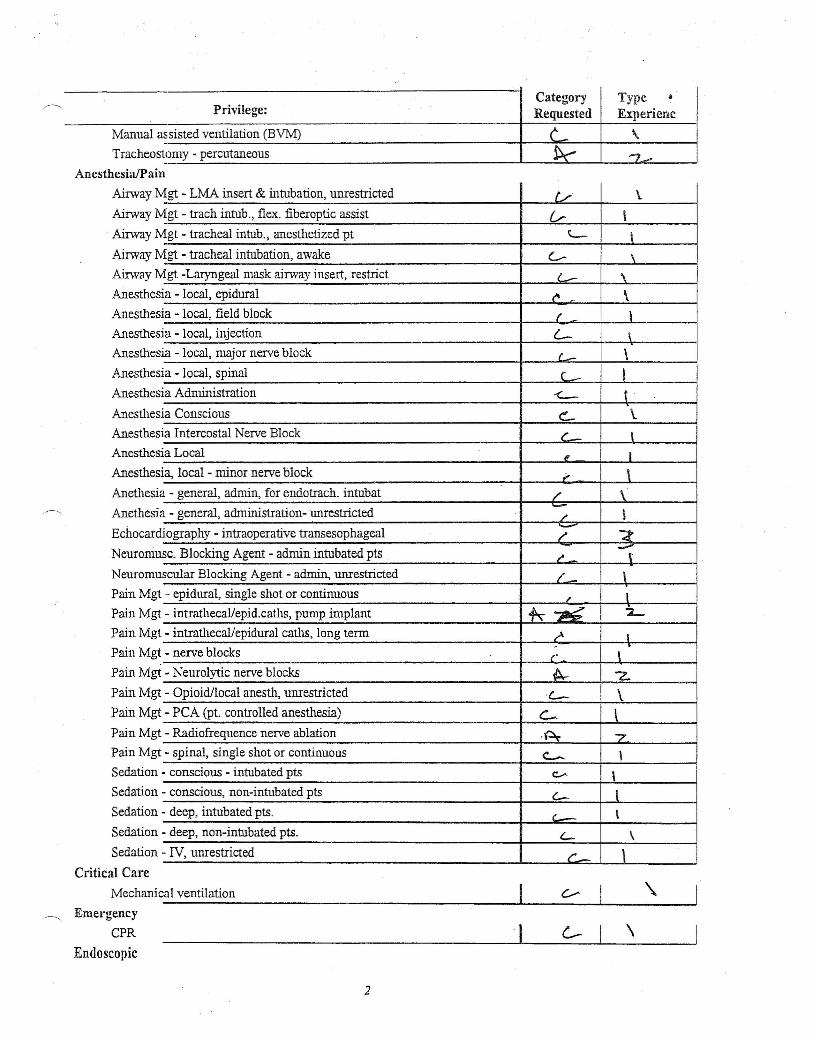
ACCORDING TO CATEGORY, ENTER A, B, OR C IN THE REQUESTED COLUMN NEXT TO THE LISTED PRIVILEGE:
A The applicant will not undertake patient m:mngemenUprocedure except in emergency.
B The applicant will occasionally manage patients or assist in management/perform the procedure/assist in the performance, Consultation will besought in the event of antlcipated or actual difficulties.
C The applicant will independently m:mage patients/perfonn the procetlure. The applicant would be expected to request consultation onlyoccasionally.
ACCORDING TO TYPE, ENTER 1, 2, OR 3 IN THE COLUMNS IN THE E}''PERIENCE COLUMN:Completed Formal Training Program.
2 Limited Experience - without formal training.
3 Extensive Experience - without formal tr:rilling.
UVA Outpatient Surgery Center Privileges ~es o No
. ~~----------~--------------------------~--------~--------~Privilege: .
CategoryRequested
TypeExperienc
Medical
AnesthesiaIPain
HemodynPain Consul
PainDiff.. Pain Man
Pain Man
Periop- UPostopera
Preoperati
Critical CareCritical C
lCU - UnNeonate iPIC intub
PIC sedati
GeneralPharmacologic Mgt
antic Support Consults (
tation a. ,Dx&Tx
.•.~ 2.agement - acute L \agement - chronic ~ -z...nrestricted med assess & mgt r: \tive Assess L \ve Assess '- \
are - Neurology . R L.restricted Care ~ Z.ntubation & mech vent (2... 1-..-ation & mech vent a. --z-on, pain control ~ ~
\Procedure
Ainvay Control
1
Category Type *Privilege: Requested Experienc
Manual assisted ventilation (BVM) c \Tracheostomy - percutaneous k '7~....
Anesthesia/Pain
AirwayM
AirwayM~Airway M
AirwayMAirwayMAnesthes
Anesthes
AnesthesAnesthes
Anesthes
Anesthes
AnesthesAnesthes
Anesthesi
Anesthesi
Anethesia.--------. Anethesia
Echocardi
Neuromus
NeuromuPainMgt
PainMgtPainMgtPain Mgt
PainMgt
PainMgtPain MgtPainMgtPain MgtSedation
Sedation
Sedation
Sedation
Sedation
Critical Care
Mechanical ventilation I----------------- --J
Emergency
CPR I__ C--_' __ \__ ----'
Endoscopic
gt - LMA insert & intubation, unrestricted (j \.--gt - trach intub., flex. fiberoptic assist V- Igt - tracheal intub., anesthetized pt L- \-gt - tracheal intubation, awake c- \-gt -Laryngeal mask airway insert, restrict c.: \
ia - local, epidural t" \ia - local, field block I Iia - local, injection L- \ia - local, major nerve block ('- \ia - local, spinal c_ Iia Administration <- tia Conscious c, \.
ia Intercostal Nerve Block c__ Ia Local , Ia, local - minor nerve block ., \- general, admin, for endotrach. intubat / \- general, administration- unrestricted - \/
.ography - intraoperative trans esophageal ;- "::tc. Blocking Agent - admin intubated pts ,. '\
seular Blocking Agent - admin, unrestricted / \- epidural, single shot or continuous " I- intrathecal/epid.caths, pump implant ~~ 2-
- intrathecal/epidural caths, long term r" I
- nerve blocks.
\r:- Neurolytic nerve blocks -A-
"'Z.- Opioid/local anesth, unrestricted 'L- \- PCA (pt. controlled anesthesia) C- \- Radiofrequence nerve ablation .~ "7
- spinal, single shot or continuous <:.-.. \- conscious - intubated pts c:.,.... \- conscious, non-intubated pts C- l- deep, intubated pts. '--- \- deep, non-intubated pts. '- \- IV, unrestricted C- \
2

'1
Privilege:Type ~Experienc
CategoryRequested
Bronchoscopy~~------------------------------------------~--------~--~~----~Vascular
Central Venous Catheter
Invasive Monitor. - arterial catheters
Invasive Monitor. - central venous catheterInvasive Monitor. - vascular, umestricted
\
DATE
As the Division Head/QI Liaison and Department Chair/Medical Director, we have reviewed the above-named clinician's level of experience and training as related to requested privileges and agree that theabove named clinician's qualifications are appropriate. Therefore, we r ommend the appintment to theClinical Staff with the clinical privileges as requested.
__ ---'lP {?-l ( ./7" (),,--sfcJ)
DATE RE
DATE
3