clinical study of usre wazifi nazfe raham …
TRANSCRIPT
CLINICAL STUDY OF USRE WAZIFI NAZFE RAHAM
(DYSFUNCTIONAL UTERINE BLEEDING) AND ITS
MANAGEMENT WITH UNANI DRUGS
by
Salma Bano
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore.
In partial fulfillment
of the requirements for the degree of
Mahire Tib
M.D. (Unani)
in
Ilmul Qabalat wa Amraze Niswan
(Obstetrics & Gynaecology)
Department of Ilmul Qabalat wa Amraze Niswan
(Obstetrics & Gynaecology)
National Institute of Unani Medicine
Bangalore.
2007

CLINICAL STUDY OF USRE WAZIFI NAZFE RAHAM
(DYSFUNCTIONAL UTERINE BLEEDING) AND ITS
MANAGEMENT WITH UNANI DRUGS
by
Salma Bano
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore.
In partial fulfillment
of the requirements for the degree of
Mahire Tib
M.D. (Unani)
in
Ilmul Qabalat wa Amraze Niswan
(Obstetrics & Gynaecology)
Under the guidance of
Dr. Wasia Naveed
Department of Ilmul Qabalat wa Amraze Niswan
(Obstetrics & Gynaecology)
National Institute of Unani Medicine
Bangalore.
2007

I
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
KARNATAKA.
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation/thesis entitled “Clinical Study of
Usre Wazifi Nazfe Raham (Dysfunctional Uterine Bleeding) and its
Management with Unani Drugs” is a bonafide and a genuine research
work carried out by me under the guidance of DR. WASIA NAVEED,
Associate professor, Department of Qabalat wa Amraze Niswan,
Govt. Nizamia Tibbi College, Hyderabad.
Date: Signature of the Candidate
Place: (Dr. Salma Bano)

II
CERTIFICATE BY THE GUIDE
This is to certify that the dissertation entitled “Clinical Study of
Usre Wazifi Nazfe Raham (Dysfunctional Uterine Bleeding) and its
Management with Unani Drugs” is a bonafide research work done by
Dr. Salma Bano, in partial fulfillment of the requirements for the degree of
Mahire Tib (M.D.Unani) in Ilmul Qabalat wa Amraze Niswan.
Date: Signature of the Guide
Place: DR. WASIA NAVEED,
Associate professor,
Dept. Qabalat wa Amraze Niswan
Govt. Nizamia Tibbi College,
Hyderabad

III
ENDORSEMENT BY THE HOD, PRINCIPAL/HEAD OF THE
INSTITUTION
This is to certify that the dissertation/thesis entitled “Clinical Study of Usre Wazifi
Nazfe Raham (Dysfunctional Uterine Bleeding) and its Management with
Unani Drugs” is a bonafide research work done by Dr. Salma Bano under the
guidance of Dr.Wasia Naveed, Associate Professor, Dept. Qabalat wa Amraze
Niswan, Govt. Nizamia Tibbi College, Hyderabad.
Seal & Signature of the Seal & Signature of the
HOD Head of the Institution
Dr. K Tabassum Prof. M. A .Jafri
Incharge HOD, Director, NIUM,
Dept. Ilmul Qabalat wa Bangalore.
Amraze Niswan.
Date: Date:
Place: Place:

IV
COPYRIGHT
Declaration by the Candidate
I hereby declare that the Rajiv Gandhi University of Health Sciences,
Karnataka shall have the rights to preserve, use and disseminate this
dissertation/thesis in print or electronic format for academic/research purpose.
Date: Signature of the Candidate
Place: (Dr. Salma Bano)
© Rajiv Gandhi University of Health Sciences, Karnataka.

V
In loving
Memory of my
Beloved parents,
My inspiration,
Throughout.

VI
It is indeed my fortune to have carried out this dissertation work at National
Institute of Unani Medicine, Bangalore. In this regard, I would like to express my
heartfelt gratitude to Prof. M. A. Jafri, Director, NIUM, Bangalore, for his
courtesy, grace and blessings to carry out this work.
I express my sincere and deep sense of gratitude to Dr. Wasia Naveed,
Associate Professor, Dept of Qabalat wa Amraze Niswan, Govt. Nizamia Tibbi
College, Hyderabad, for her valuable guidance, encouragement incessant support
and selfless help in the preparation of this dissertation. I’m indebted to her for her
valuable suggestions and encouragement. I’m indeed privileged to have her as my
guide.
I wish to express my deep sense of gratitude and indebtedness to my co-
guide, Dr. Ismath Shameem, Lecturer, Dept of Ilmul Qabalat wa Amraze Niswan
NIUM, Bangalore, for all the valuable help and guidance in the preparation of this
dissertation. She has taken lots of pain and with patience has gone through this
dissertation a number of times. I express my humble thanks to her for the invaluable
consent.
I extent my gratitude to Dr. K. Tabassum, Reader, Incharge, Dept of Ilmul
Qabalat wa Amraze Niswan NIUM Bangalore, for her concern, meticulous approach
and keen supervision of this dissertation work.
I express my sincere gratitude to my teacher Dr. Wajeeha Begum, Lecturer,
Dept of Ilmul Qabalat wa Amraze Niswan NIUM, Bangalore, for permitting me to
utilize the cases from her unit and also for her valuable suggestions and
encouragement.
I take this opportunity to thank Dr. Md. Anwar Siddiqui Hospital incharge,
NIUM, Bangalore, for providing the facilities in the hospital for carrying out my
clinical study. He was magnimous in rendering his invaluable support and
cooperation.
I express my sincere thanks to all the professors, readers& lecturers of
NIUM, Bangalore for their invaluable support and advice.
I extend my whole hearted thanks to my teachers and collegues of Govt.
Unani Medical College, Bangalore for their well wishes

VII
I express my regards to Dr. Nafees Khan, Chief Pharmacist, Dr. Fazil
Ahmed, senior Pharmacist and other staff of Pharmacy Dept, NIUM, Bangalore, for
preparing and providing the medicines on time required for my clinical study.
I extend my regards to Dr. Sanjeeda Tabassum, Biochemist and other staff
of Pathology Dept. for helping me in my clinical study
I express my sincere thanks to Dr. Triveni. K. L Consulting Sonologist,
Triveni scanning Centre, Magadi Road, Bangalore, for her invaluable help in my
clinical study.
I extend my regards to Dr. Veena Baindur, Gynaecologist, visiting
consultant, NIUM, Bangalore, for her kind co-operation and help in my clinical
study.
.My association with the nursing staff and nursing assistance throughout my
clinical study has been of immense help. My sincere thanks to all of them.
I extend my thanks to the staff of library, NIUM, Bangalore for their
generous help during the course of my literary work.
.
I extend my thanks to all the Paramedical staff, NIUM, Bangalore.
Invaluable is the help rendered by my fellow PGs and as well as my juniors
in carrying out my clinical and literary work. My heartfelt regards to them. I express
my regards to all those who have directly or indirectly helped me in completing this
endeavor.
I’m highly indebted to my patients without whose cooperation; this work
would not have been possible.
Here are a few individuals whose help and support have been truly
significant, without their physical, intellectual and moral support, this book would
still have been in a conceptual stage. Naveed, Faizia, Zahoor, , Nikhath, Nadeem,
Farheen, Sameera, and my sisters Qamer Bano and Dr. Najma Bano.
Last but not the least; I thank my mother-in-law for her graceful blessings. I
wish to appreciate the immense and valuable support rendered by my life partner
Mr. Syed Ziaulla. I owe my highest regards to him for his good understanding and
maximum contribution in helping me to discover my potential. Words of gratitude
are inadequate to express my unbound thankfulness to him.
I owe my love and blessings to my kids, Tasneem, Umair and Zubair for
their cooperation and patience throughout the course of my study.
Date: Signature of the candidate
Place: (Dr. Salma Bano)

VIII
LIST OF ABBREVIATIONS USED
AUB: Abnormal Uterine Bleeding
BID: Twice daily
BT: Bleeding Time
CaCx: Cancer of Cervix
CVS: Cardiovascular System
COC: Combined Oral Contraception
CT: Clotting Time
CLPD: Corpus Luteal Phase Defect
DUB: Dysfunctional Uterine Bleeding
DHEA: Dehydroepiandrosterone
DC: Differential Count
D&C: Dilatation and Curettage
DM: Diabetes Miletus
E2: Ethenyl Estradiol
ESR: Erythrocyte Sedimentation Rate
FSH: Follicle Stimulating Hormone
FDA: Food and Drug Administration
GnRH: Gonadotrophins Releasing Hormones
HTN: Hypertension
HDL: High Density Lipoprotein
HRT: Hormonal Replacement Therapy
IUCD: Intra Uterine Contraceptive Device
IHD: Ischaemic Heart Disease
IPD: Inpatient Department
LFT: Liver Function Test
LNG-IUS: Levanorgestrel-Releasing Intrauterine System
LH-RF: Leutinising Hormone-Releasing Factor
LH: Leutinising Hormone
MBL: Menstrual Blood Loss
NSAID: Non-Steroidal Anti-Inflammatory Drugs

IX
OPD: Outpatient Department
PGE2: Prostaglandin E2
PCOD: Poly Cystic Ovarian Disease
PT: Prothrombin Time
PGI2: Prostaglandin I2
PGF2: Prostaglandin F2
PRL: Prolactin
PIF: Prolactin Inhibiting Factor
RBS: Random Blood Sugar
RS: Respiratory System
RFT: Renal Function Test
SGOT: Serum Glutamic Oxaloacetic Transaminase
SGPT: Serum Glutamic Pyruvic Transaminase
TB: Tuberculosis
T3: Triiodothyronine
T4: Thyroxine
TSH: Thyroid-Stimulating Hormone
TLC: Total Leucocyte Count
TXA: Thromboxane
UWNR: Usre Wazifi Nazfe Raham
USG: Ultrasonography
VDRL: Venereal Disease Research Laboratory test

X
ABSTRACT
Background and Objectives:
Paraceleus (1494-1541) called the uterus, “The smallest microcosm” in which all
the human life is reproduced. Of the many disorders involving the uterus which pose
the major health hazard in the life of women, DUB poses a major challenge to
gynecologists and forms about 10%-15% of gynae admissions.
With an objective to evaluate the efficacy of unani drugs in the management of
DUB, to provide cost effective, easily available, and safe remedy to the ailing
community, the present study was conducted at Department of Ilmul Qabalat wa
Amraze Niswan, NIUM Hospital, Bangalore.
Methods:
Standard controlled randomized single blind study was carried out by registering 60
clinically diagnosed cases of DUB were enrolled in both test group (30 patients) and
control group (30 patients) after getting their consent to participate in the study.
Treatment was given for 10 days or as per assessment of the patient for 3
consecutive menstrual cycles and evaluation of treatment was done by the
assessment of menstrual blood loss (MBL) using the Pictorial Bleeding Assessment
Chart before and after the treatment, relief of the associated symptoms and
regularity of menstrual cycles.
Results:
There was a significant reduction of MBL in both test group and control group
(P < 0.0001). The irregularity of menstrual cycles was rectified and menstrual cycles
were regular with duration of 24-30 days. Of the 30 patients in the test group, 21
(70%) were cured, 7 (23.30%) were relieved, and 2 (6.7%) were partially relieved.
Interpretation and Conclusion:
The Unani drugs in the test group were found to be effective as they are having
haemostatic, styptic, analgesic, and anti-inflammatory properties. The formulation is
rich in oxides of iron, calcium, and phosphorus, hence found to be beneficial in
replenishing the lost minerals in excessive menstrual flow.
Keywords:
Dysfunctional Uterine Bleeding, Menstrual Blood Loss, and Menstrual cycle.

XI
TABLE OF CONTENTS
1. Introduction 01
2. Objectives 05
3. Review of literature 06
4. Methodology 58
5. Results 83
6. Discussion 93
7. Conclusion 100
8. Summary 102
9. Bibliography 105
10. Annexures 112

XII
LIST OF TABLES
Sl. No. Tables Pages
1: Age Incidence in Test Group & Control Group 83
II: Marital Status incidence in Test Group & Control 84
Group
III: Pattern of Menstrual Cycle Incidence in Test 85
Group and Control Group
1V: Temperamental Incidence in Test Group and 86
Control Group
V: USG Findings Incidence in Test Group and 87
Control Group
V1: Endometrial Biopsy Findings Incidence in Test 88
Group
V11: Results: Duration of MBL Before and After 89
Treatment
V111: Results: Amount of MBL (pads per day) Before 90
and After Treatment
1X: Results: MBL Assessment Scores Before & After 91
Treatment in Test Group & Control Group
X: Results: Showing Overall Response 92

XIII
LIST OF FIGURES
Sl. No. Figures Pages
1. Fluctuation of different hormone levels 12
during menstrual cycle (ovulatory)
2. Endometrium in Proliferative Phase 19
3. Endometrium in Secretory Phase 19
4. Uterine multiple polyposis 44
5. Disordered proliferative endometrium 45
6. Benign endometrial hyperplasia 45
7. Geru 62
8. Gulnar 66
9. Dammul Akhwain 71
10. Barg Bartang 77

KEY WORDS TO MASTER CHART
♦ Reg no - Registration number.
♦ BPV - bleeding per vaginum.
♦ AOF (Pads per day) - Amount of flow.
♦ DOF (days) – Duration of flow.
♦ Dys – Dysmenorrhoea.
♦ GW – General Weakness.
♦ WD – White Discharge.
♦ BA – Back Ache.
♦ POC – Pattern of Cycle.
♦ AOM – Age of Menarche.
♦ P – Para, L – Live, A – Abortion, D – Died.
♦ HOS – History of Sepsis.
♦ Sur – Surgical.
♦ IUCD – Intra Uterine Contraceptive Device.
♦ Hor – Hormonal.
♦ P/S – Per Speculum.
♦ P/V – Per Vaginum.
♦ Vg – Vagina, Cx – Cervix, Ut – Uterus.
♦ TLC – Total Leucocyte Count.
♦ DLC – Differential Leucocyte Count, P – polymorphs,
L – Lymphocytes, E – Eosinophils, M – Monocytes, B – Basophils.
♦ ESR – Erythrocyte Sedimentation Rate.
♦ USG – Ultrasonography.
♦ Endo-Biop – Endometrial Biopsy.
♦ DM – Damavi, BL – Balghami, SF – Safrawi, SU – Saudawi.
♦ BT – Before Treatment, AT – After Treatment.
♦ NR – No Response, PR – Partially Relieved, R – Relieved,
C – Cured
♦ AV – Anteverted, RV – Retroverted, Ero – Erosion,
Htd – Hypertrophied, MEO – Mildly Enlarged Ovaries.
♦ Cy – Cystocele, Rec – Rectocele.
♦ NS – Normal Size, Bul – Bulky, M – Mobile, FF – Fornicess Free.
♦ NA – Not Applicable.
♦ IC – Infrequent Cycles, Menor – Menorrhagia,
Polym – Polymenorrhoea, Menomtrgia – Menometrrogia.
♦ Hyp. Plastic- Hyperplastic, Secr – Secretory, Prolif – Proliferative.











1
1. Introduction
“Hystera” or Uterus is considered to be a symbol of feminity in nature. The
medieval humanist Buonaccidi said of this unique female organ – “of all the
miracles which the human body shows us, none is more marvelous and admirable
than the womb of woman, from whence man in all his wondrous complexity, is most
ingeniously derived.”
A woman is one of the God’s greatest complex and beautiful creations on
earth. The gynaecological health of a woman depends to a large extend on the
normalcy or otherwise of her menstrual cycle.
The term menstruation is derived from the Latin word, ‘Menstruns’ meaning
monthly. (1)
Normal menstruation requires integration of the hypothalamic - pituitary -
ovarian axis with a functional uterus, a patent lower genital outflow tract and a
normal genetic karyotype of 46 XX. (2)
The normality of menstruation is subjectively determined by the amount and
duration of blood flow and by the intervals between menstrual cycles. The blood
loss in normal menstrual period varies from 25 -75 ml. (3)
Normal menstrual flow is defined as occurring at a mean interval of 28 days
(+/_ 7 days) with an average duration of 4 – 7 days. Although, it can be erroneous to
generalize research findings to study population of women (regardless of race,
ethnicity, weight, etc). Most studies from 1960’s and 1970’s found that mean MBL
in normal women is 35ml. approximately 95% of women lose less than 60ml of
blood during each menstrual cycle. Blood loss of >60 – 80ml per month is
associated with anaemia and iron deficiency. (4)

2
Menstrual disturbances can cause a lot of discomfort, inconvenience and can
also disrupt a normal healthy life style. Millions of women across the globe suffer
from this problem.
Menstrual dysfunction is the most common problem being encountered in
gynaecological practice. The earliest reference to the problem of menstrual
dysfunction is in Hindu literature dating back to 1400 B.C. (5)
The increasing anxiety with dysfunctional menstruation is specially a
problem of the 20th
century. Previously late menarche, early menopause and
prolonged periods of child bearing and lactational amenorrhoea reduced the number
of menses experienced by women in their life time. The reduction of family size, by
the wide spread use of contraception and sterilization has resulted in an
approximately ten fold increase in the number of periods that woman experience
during their reproductive life.(6) Women find menstruation as a source of
discomfort and inconvenience and this view is aggravated by the changing role of
women within society in which a more active role in occupations outside of the
house hold is being pursued, a place where episodes of flooding are even less
tolerable.(7)
The term dysfunctional uterine bleeding is defined as abnormal bleeding in
women between menarche and menopause that can not be attributed to medications,
blood dyscrasias, systemic diseases, trauma, uterine neoplasms or pregnancy, though
it is commonly applied to bleeding which is excessive either in amount, duration or
frequency.(8). In India, the incidence is reported to be 12.6 – 23.17% of all
gynaecological admissions. (9).
The term, ‘diagnosis of exclusion’ specified for DUB is more confusing than
enlightening. The evaluation of DUB mainly consists of recording a proper history,

3
thorough physical and pelvic examination and performing various investigative
procedures which explore the pathology in the pelvis and mainly in the uterine
cavity. (5)
In Unani Tib DUB is being mentioned and described under the heading of
Kasrate Tams from ancient times, but recently it is being mentioned as Usre Wazifi
Nazfe Raham. (10)
The basis of Unani Tib is laid on Humors and Temperament. Buqrat, the
father of humoral theory, states that any change or alteration in humors and their
temperament can affect the health of a person. Alteration or changes in sex, age,
food & drink, air, rest & physical and psychological activity, sleep & wakefulness
and retention & elimination disturbs the health and homeostasis of a person
resulting in dysfunction of body. (1, 11)
The etiology attributed to Kasrate Tams is Imtela (plethora), Sue Mizaj
(changes in temperament) of the body or the uterus Zofe Quwate Maseka (decrease
in the retentive power of uterine vessels), Maayiyate khoon (increased liquidity of
blood) and active congestion of blood resulting in increased tension in uterine
vessels. (12, 13, 14, 15, 16)
Hormonal therapy has its own side effects like nausea, vomiting, GIT
disturbances, obesity, sterility, hypertension, liver diseases etc. (17)
Hysterectomy which has been the ultimate cure, though a safe operation with
minimum morbidity and mortality has its own long term complications viz.,
premature ovarian failure, vault pro-lapse is quite disturbing. (5).
Therefore, despite a wide range of treatment options, for its management
which have been multiplied over the recent years, yet considering the factors such as
age, parity and wishes of the patients with regard to contraception, future

4
pregnancies etc., there is still an acute need to look for better option for its medical
management.
The present study was conducted on 60 clinically diagnosed patients of DUB
from IPD and OPD of Department of Ilmul Qabalat wa Amraze Niswan, NIUM
Hospital, Bangalore, and after obtaining their consent to participate in the study,
treatment was given for 3 consecutive menstrual cycles and no side effects were
noted.
There was a significant reduction of MBL in the control group (P<0.0001).
The irregularity of menstrual cycles was rectified and menstrual cycles were
restored to regular with duration of 24-30 days. Of the 30 patients in the test group,
21 (70%) were cured, 7 (23.30%) were relieved, and 2 (6.7%) were partially
relieved. There was a subjective relief in the associated symptoms viz backache,
general weakness, palpitation, etc.
Unani drugs are freely available, inexpensive, harmless, and efficacious and
have been abundantly used in Unani Tib.
The combination has no adverse action on consumption and does not create
any irritation. The drugs chosen in the study have haemostatic, styptic and
astringent effect which increases the constrictive power of the uterine vessels by
virtue of their cold and dry temperament.
Hence, it was envisaged to develop an indigenous therapy which is gentle,
non hormonal, practical, safe, yet effective alternative in the management of DUB
with the prime aim of benefiting the ailing community.

5
2. Objectives
1. To evaluate the efficacy of unani drugs in the management of Usre Wazifi
Nazfe Raham (UWNR).
2. To popularize the unani medicines in the management of DUB.
3. To prevent anaemia and its consequences caused by heavy bleeding.
4. To provide cost effective, easily available safe remedy to all suffering patients
of UWNR.
5. To prevent the complications of HRT and to avoid surgical treatment.

6
REVIEW OF LITERATURE
The ancient Greeks assumed that menstruation was a cleansing process and
the Bible refers to the woman as being “unclean” at that time (1).
In Arabic the words ‘pure’ and ‘impure’ originally referred to menstruation
and the term ‘taboo’ or ‘sacred’ entered the English language from the Polynesian
word tabu or menstruation (1).
Greeks observed that the menstrual blood was thinner at the beginning and at
the end of menstruation and that once begun the blood flowed quickly (1).
In Unani Tibb DUB is described under the heading of Kasrate tams, the other
synonyms are Ifrate Haiz, Istehaza etc. In recent times it is referred to as Usre
Wazifi Nazfe Raham (10).
The problem of excessive menstrual blood loss was also addressed by the ancient
Greeks and Romans.
Buqrat (Hippocrates of Cos) (460-377 BC): He advocated that treatment consisted
of cupping applied to the breast. Hippocrates is the father of humoral theory. The
basis of Unani Tibb is laid on Humours and Temperament. Any change or alteration
in the composition and preparation of all humours or any change in their
temperament due to dominancy of any humours in body fluids would alter the state
of health and lead to abnormalcy in normal functioning of the body. According to
the dominancy of khilt or humour the condition, Kasrate haiz is referred to as
damwi, balghami, safrawi or saudawi (1, 14).
Dioscorides (AD54-68): Has stated that Tukhme Bartang given as a food stops
excess menstruation. Joshanda Dana Anar helps in reducing excessive bleeding (1).

7
Soranus of Ephesus. (98AD – 138AD): He advised that ligatures should be
applied to the armpits and groins in an attempt to reduce blood flow to the body and
thus to the uterus (1).
Jalinoos (Galen) (130AD-200AD): Advised application of large cuppings beneath
the breasts in Kasrat e tams. He mentioned about simple drugs such as Khurfa,
Raswat, Gile Armani, Gulnar etc. he has quoted about use of decoction of Bartang
leaves in douche form and the patient was cured (14).
Zakriya Razi (C932AD): In his book Al Hawi, Vol 9 has mentioned about the
diseases of women and their management (14).
Majoosi (C930AD- 994AD); In his famous book Kamil us Sana has attributed the
etiology for excess menstruation as
• Zofe Quwate Maseka ie. Decrease in the retentive power of uterine vessels.
• Increased liquidity (maayiyat) of blood
• Active congestion of blood resulting in increased tension in uterine vessels
(15).
Ibne Sina (AD980-1037):
He treated excess menstruation in the same way as Soranus, although he
added opium to some of his prescriptions (1).
Ismail Jurjani (c1136-1140AD):
His book zakheere khwarizm shahi Vol VI mentioned about the position,
shape, size, structure of uterus in different stages of life. He has mentioned different
causes and management of menorrhagia (13).
Ajmal khan (1868-1927AD ):
Has described the cause of menorrhagia, as ingestion of hot and spicy food
that alters the temperament of blood to safrawi, increases the maayiyat of blood

8
making the blood vessels of uterus more dry and friable resulting in excess bleeding
(18).
Dysfunctional Uterine Bleeding:
Dysfunctional Uterine Bleeding best defined as abnormal bleeding from the
uterus in the absence of organic disease of the genital tract (19). The term DUB
applies to any abnormal bleeding including disturbances of the menstrual cycle,
regular and irregular uterine bleeding and alterations in the amount or duration of
menstrual loss, but most commonly implies excessive regular menstrual bleeding or
essential menorrhagia (7).
In the absence of gross or microscopic pelvic pathology, menstrual disorders
have been attributed to dysfunction of the hypothalamic - pituitary - ovarian -
uterine axis. The endocrine dysfunction may produce a wide spectrum of disorders
ranging from excessive cyclic or acyclic bleeding to infrequent or scanty bleeding
from the uterus (20).
Four separate conditions were discovered which were thought to be related
to D.U.B. in the history of menorrhagia (1).
The first of these, the anovulatory bleeding cycle was described in rhesus
monkey by Heape, (1897). Heavy menstruation occurs despite anovulation.
Emil Novak (1927 – 33) described the first instance in humans. (1)
The second abnormality (later) termed the luteal phase defect in which the
development of secretory phase was impaired, described by Jones (1949). (1)
A third condition termed irregular shedding of endometrium was recognized
by Driessen in 1914. (1)
The final disorder that of endometrial hyperplasia was thought to occur more
commonly described by Recamier (1850), Cullen in 1900 described hyperplastic

9
endometrium accompanied by uterine bleeding. However, Robert Schroder is
usually credited with a definitive early work on endometrial hyperplasia as a clinical
entity. (1)
The histologic appearance of large glands of irregular shape prompted Novak
and Martzloff (1924) to apply the term Swiss cheese pattern to cystic glandular
hyperplasia of endometrium (1).
Initial studies on this condition in the 1930s and 1940s were devoted to the
microscopic examination of the endometrium. Only 50% showed any histological
abnormality and in about 40% there were evidence of ovulation, both findings being
inconsistent with the theory that uninhibited prolonged oestrogen stimulation of the
endometrium is the main cause of DUB. With the improvement in hormone assay
techniques in 1960s, attention was directed to the study of oestrogen and
progesterone excretion levels in normal and abnormal menstruation. The results
however showed that the oestrogen excretion levels in DUB were consistent only in
their variability (20).
Based on endometrial histology, practical classification of DUB was
evolved, and the introduction of oral contraceptive steroids revolutionized its
treatment. However, many patients either failed to respond to hormones or had
contra-indications to their use (20).
In the 1970s the wide use of contraception, particularly mini pills, long
acting injectible steroids and IUCD added a new dimension to the problem of
Abnormal Uterine Bleeding (AUB). The study of endometrium in these cases by
electron microscope, histochemical and immuno fluorescent techniques threw more
light on the subject. These studies revealed the importance of fibrin, the platelets,

10
the lysosomal system and prostaglandins in the haemostatic control of menstrual
blood loss.
The recent work of Fritz and Speroff (1982) has stressed the role of the
ovary in controlling its own steroidogenic function and the ultimate endometrial
response via the oestrogen feedback mechanism (20).
Currently the emphasis has been on defining the parameters of DUB based
on objective methods of measurement of menstrual blood loss (MBL) (Cohen and
Gibor 1980) and in studying the phenomenon of haemostasis in the uterus, as it
differs from haemostasis in the peripheral blood (20). The upper limit of normal
menstruation is thus taken as 80ml per menses (Rybo 1966) (21).
“There is no significant difference in the plasma concentration of LH, FSH
and E2 or in the salivary concentration of progesterone between those with objective
heavy loss and those with normal loss” (22).
Latest Scientific Research:
With the development of gynecology, the introduction of anaesthetics and the
use of uterine curette from the mid-19th
century, the menstrual cycle became the
subject of scientific study. Abnormalities of endometrium were described by
Recamier (1850) and Olshausen (1875) and also by Cullen (1900-1908) highlighted
the histological characteristics of endometrial hyperplasia. (1)
Hallberg et al (1966) defined menorrhagia as menstrual blood loss of more
than 80 ml per menstruation from a normal secretory endometrium after a normal
ovulation.
Worry, Fright, Fatigue, nervous shock, sexual excess and perversions were all
thought to be causes of uterine hemorrhage – frank (1845) (1)

11
Prostaglandins were first discovered by Kurzrok and Lieb in 1930. (18) The
amounts of PGE2 and PGF2α in the endometrium in leutial phase are increased in
patients with menorrhagia and Dysmenorrhoea (Haynes et al 1980).(4,5)
Endometrial hyperplasia develops when unopposed oestrogen stimulation
persists, as in chronic anovulation. Women with high levels of oestrogen may have
an amenorrheic period followed by acute and heavy bleeding (5). The endometrial
histology is extremely useful in a management of DUB. A defective corpus luteum
would cause irregular ripening and premenstrual spotting while a persistent corpus
luteum would cause irregular shedding. (3, 23)
An endometrial biopsy done on 4th
day of cycle would reveal both
proliferative and secretory endometrium in the case of persistent corpus luteum (5,
23).
12
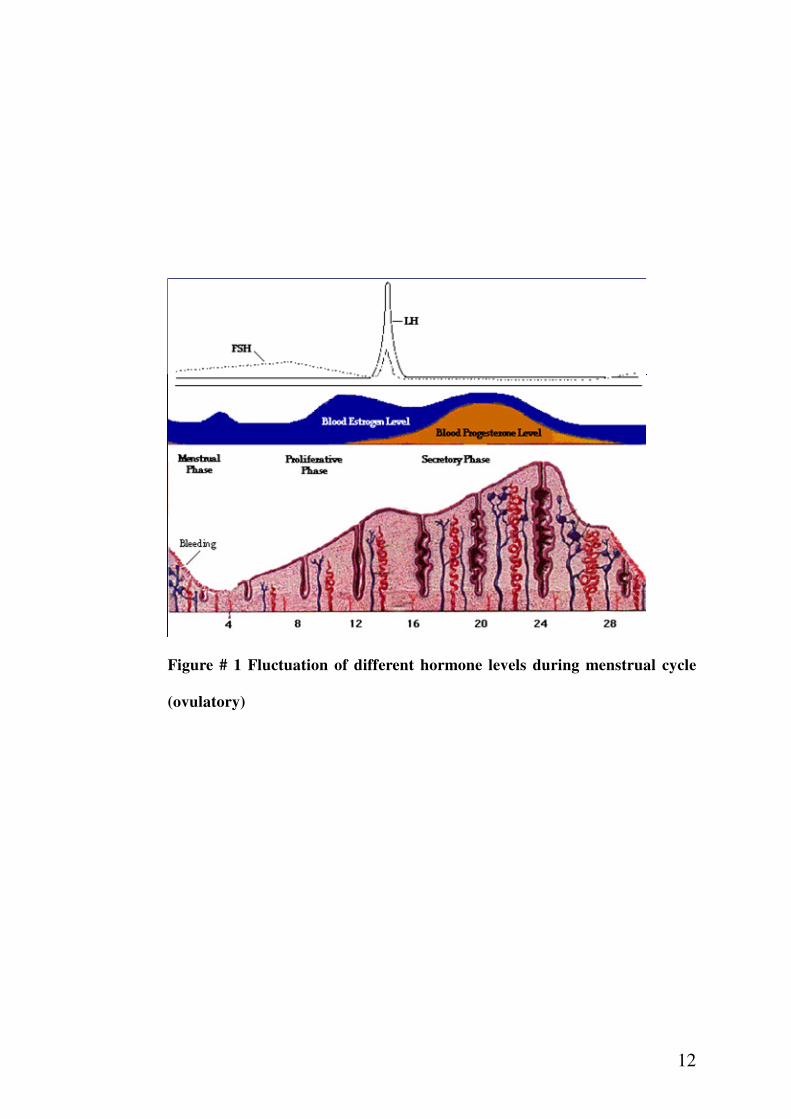
Figure # 1 Fluctuation of different hormone levels during menstrual cycle
(ovulatory)

13
PHYSIOLOGY OF MENSTRUATION (24, 25):
The female reproductive organs consist of internal genital organs and
external genital organs. The internal genital organs include vagina, uterus, fallopian
tubes, and the ovaries. These organs are placed internally and require special
instruments for inspection.
Menstruation is defined as a periodic and cyclic shedding of the
endometrium from menarche to menopause. Menstruation is the visible
manifestation of cyclic physiologic uterine bleeding due to shedding of the
endometrium following invisible interplay of hormones mainly through
hypothalamo-pituitary-ovarian-uterine axis.
A proper co-ordination in hypothalamo-pituitary-ovarian-uterine axis and
patent genitalia is conductive to the onset of menstruation and the maintenance of
the process of menstruation. A normal menstrual cycle lasts from 21-35 days with 2-
6 (4-5) days of flow and an average loss of 20-30 ml. It is made of blood (30-40
ml), stripped endometrium, mucus, leukocytes, neutrophils, and an unfertilized
ovum. Menstruation is absent before puberty, during pregnancy sometimes during
lactation and after menopause.
During each cycle, the uterine mucosa hypertrophies to provide a suitable
bed for the reception and implantation of the fertilized ovum. If pregnancy takes
place, the mucosa becomes converted to decidua. Otherwise, in the absence of
pregnancy, the hypertrophied mucosa sheds in the form of menstruation. Hence,
menstruation is defined as funeral of the unfertilized ovum or weeping of uterus for
the lost ovum. (24, 25)

14
The normal human menstrual cycle can be divided into two segments based
on the organ under examination.
• The ovarian cycle.
• The endometrial cycle.
The ovarian cycle may be further divided into follicular and luteal phases,
whereas the endometrial cycle is divided into corresponding proliferative and
secretary phases.
THE OVARIAN CYCLE (24)
:
The development and maturation of the follicle, ovulation, and formation of
corpus luteum and its degeneration constitute an ovarian cycle. All these events
occur within 4 weeks.
The ovarian cycle consists of
1. Recruitment of groups of follicles.
2. Selection of dominant follicle and its maturation.
3. Ovulation.
4. Corpus luteum formation
5. Demise of the corpus luteum.
Recruitment of groups of follicles:
The cohort of the growing follicles undergoes a process of development and
differentiation which takes about 85 days and spreads over 3 ovarian cycles.
The initial recruitment and growth of primordial follicles are not under the
control of any hormone. After a certain stage (2-5 mm size) the growth and
differentiation of primordial follicles are under the control of FSH.
There is a predominant change in the oocyte which is enlarged out of
proportion to the size of the follicle. The oocyte is surrounded by an acellular barrier

15
of glycoprotein called Zona pellucida. The outer single layer of flattened
pregrannulosa cells become cuboidal and multilayered called the granulosa cells.
The granulosa cells require FSH receptors.
Selection of dominant follicle and its maturation:
The granulosa cells grow faster than the theca cells. There is production of
follicular fluid which is primarily an ultra filtrate of blood from the vessels within
theca interna.
As early as day 5-7 of menstrual cycle, one of the follicles become dominant
and undergoes further maturation. It is probably that the one with highest antral
concentration of estrogen and lowest androgen\ estrogen ratio and whose granulosa
cells contain maximum receptors for FSH becomes the dominant follicle. The rest of
the follicles become atretic by day 8.
There is marked enlargement of the granulosa cells with lipid inclusion. The
granulosa cells surround the ovum to form cumulus oophorus which anchors the
ovum to the wall of the follicle.
At this stage, FSH induces LH receptors on the granulosa cells of the
dominant follicle. This induction is essential for the Midcycle LH surge to induce
ovulation, leutenisation of the granulosa cells to form corpus luteum, and secretion
of progesterone.
The fully mature graffian follicle just prior to ovulation measures about 20 mm.

16
Ovulation:
The dominant follicle shortly before ovulation reaches the surface of ovary.
The cumulus become detached from the wall so that the ovum with surrounding
cells floats freely in the liquor folliculi. The follicular wall near the ovarian surface
becomes thinner. The cumulus escapes out of the follicle by a slow oozing process
taking about 1-2 minutes along with varying amount of follicular fluid. The stigma
is soon closed by a plug of plasma.
Following ovulation, the follicle is changed to corpus luteum. The ovum is
picked up into the fallopian tube and undergoes either degeneration or further
maturation if fertilization occurs.
On day 22-23 of the cycle, retrogression of corpus luteum starts. The lutein
cells atrophy and corpus luteum become corpus albicans. Regression of corpus
luteum is due to withdrawal of tonic LH support.
ENDOMETRIAL CYCLE (UTERINE CYCLE) (2, 24)
The Endometrium (2, 25, 26)
:
The endometrium is the mucosal lining of the uterus. It has remarkable
ability to respond to the ovarian hormones in cyclic fashion, with resultant monthly
phenomenon known as menstruation. Endometrium has an excellent regenerative
capacity towards restoration after a normal slough. Endometrium varies in thickness
from 1 to 10mm according to the phase of menstrual cycle. It is covered by a single
layer of cuboidal and columnar epithelium which dips in to form simple unbranched
tubular and spiral glands some of which are so long that they extend from surface to
myometrium.
17
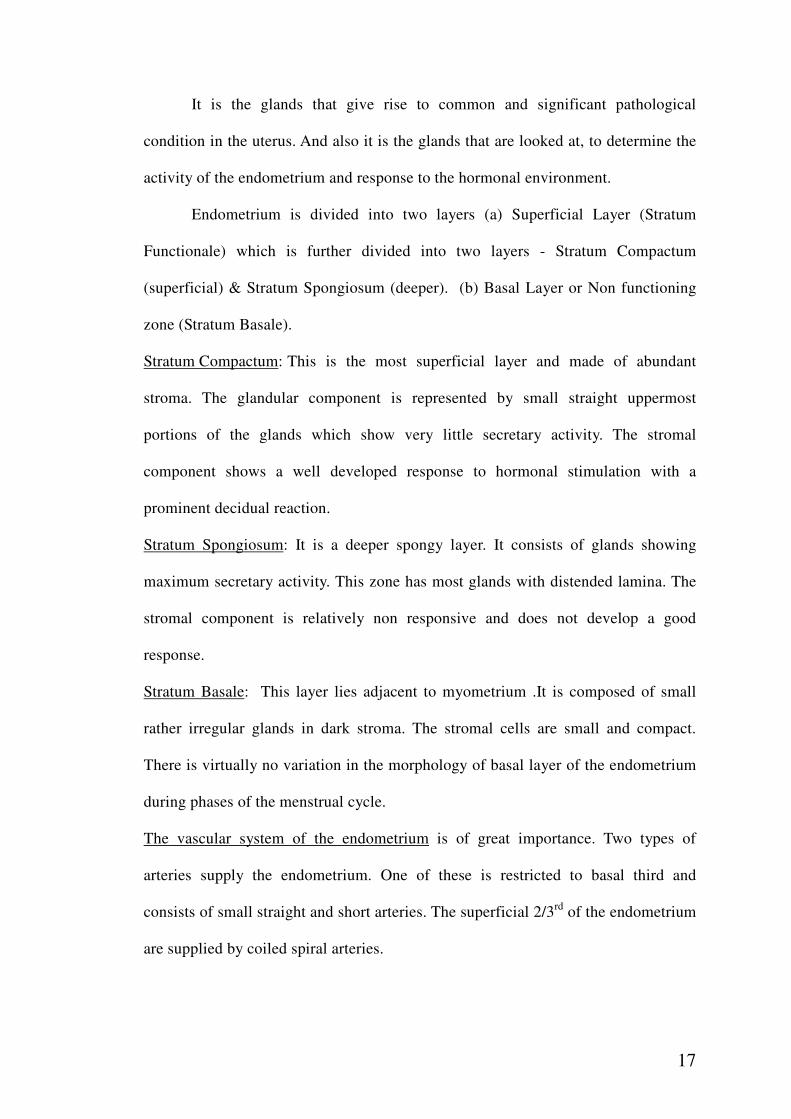
It is the glands that give rise to common and significant pathological
condition in the uterus. And also it is the glands that are looked at, to determine the
activity of the endometrium and response to the hormonal environment.
Endometrium is divided into two layers (a) Superficial Layer (Stratum
Functionale) which is further divided into two layers - Stratum Compactum
(superficial) & Stratum Spongiosum (deeper). (b) Basal Layer or Non functioning
zone (Stratum Basale).
Stratum Compactum: This is the most superficial layer and made of abundant
stroma. The glandular component is represented by small straight uppermost
portions of the glands which show very little secretary activity. The stromal
component shows a well developed response to hormonal stimulation with a
prominent decidual reaction.
Stratum Spongiosum: It is a deeper spongy layer. It consists of glands showing
maximum secretary activity. This zone has most glands with distended lamina. The
stromal component is relatively non responsive and does not develop a good
response.
Stratum Basale: This layer lies adjacent to myometrium .It is composed of small
rather irregular glands in dark stroma. The stromal cells are small and compact.
There is virtually no variation in the morphology of basal layer of the endometrium
during phases of the menstrual cycle.
The vascular system of the endometrium is of great importance. Two types of
arteries supply the endometrium. One of these is restricted to basal third and
consists of small straight and short arteries. The superficial 2/3rd
of the endometrium
are supplied by coiled spiral arteries.
18
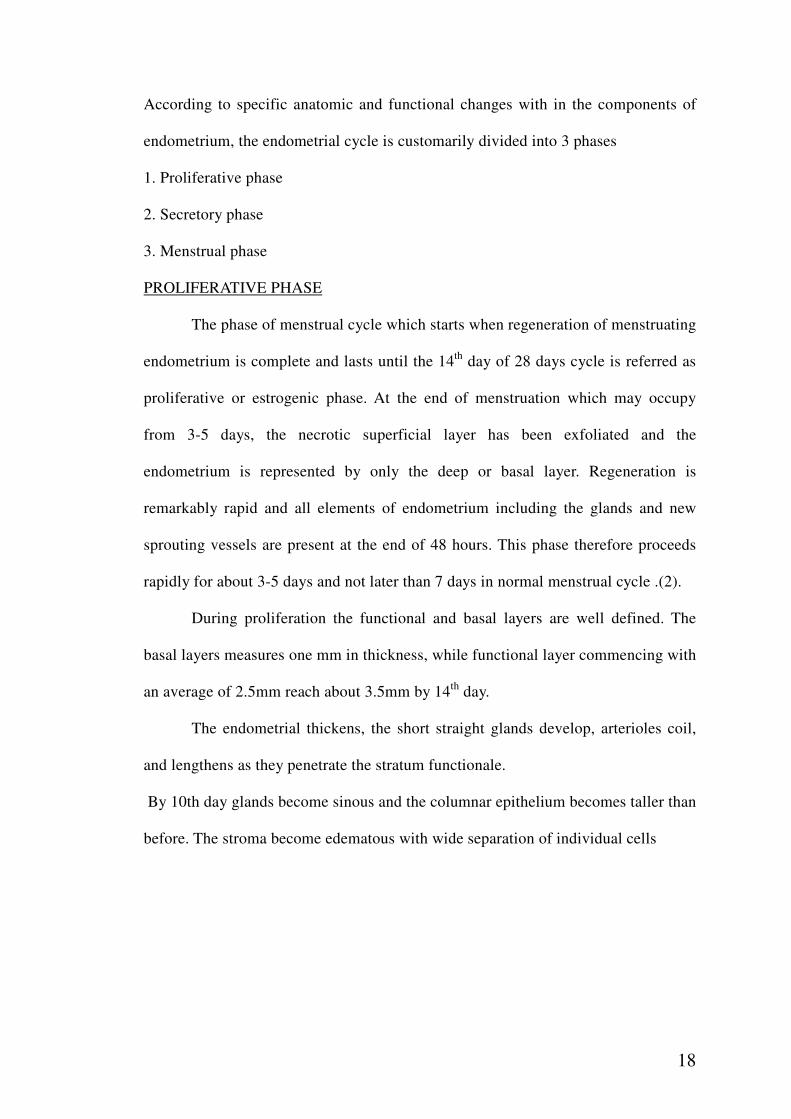
According to specific anatomic and functional changes with in the components of
endometrium, the endometrial cycle is customarily divided into 3 phases
1. Proliferative phase
2. Secretory phase
3. Menstrual phase
PROLIFERATIVE PHASE
The phase of menstrual cycle which starts when regeneration of menstruating
endometrium is complete and lasts until the 14th
day of 28 days cycle is referred as
proliferative or estrogenic phase. At the end of menstruation which may occupy
from 3-5 days, the necrotic superficial layer has been exfoliated and the
endometrium is represented by only the deep or basal layer. Regeneration is
remarkably rapid and all elements of endometrium including the glands and new
sprouting vessels are present at the end of 48 hours. This phase therefore proceeds
rapidly for about 3-5 days and not later than 7 days in normal menstrual cycle .(2).
During proliferation the functional and basal layers are well defined. The
basal layers measures one mm in thickness, while functional layer commencing with
an average of 2.5mm reach about 3.5mm by 14th
day.
The endometrial thickens, the short straight glands develop, arterioles coil,
and lengthens as they penetrate the stratum functionale.
By 10th day glands become sinous and the columnar epithelium becomes taller than
before. The stroma become edematous with wide separation of individual cells

19
Figure # 2. ENDOMETRIUM IN PROLIFERATIVE PHASE
Figure # 3. ENDOMETRIUM IN SECRETORY PHASE (19)

20
The coiled arteries extend through the endometrium and by first post
menstrual week they grow more rapidly than endometrium and become more coiled
and spiraled. In some cases the vascularity is so intense that blood oozes into uterine
cavity at the time of ovulation to be discharged from the vagina (2).
SECRETORY PHASE (2)
This phase begins on the 15th
day and persists until the onset of
menstruation. It represents the time between ovulation and the onset of menstruation
The most characteristic signs are found in glands. Their epithelial cells
develop spherical translucent areas between nuclei and basal membrane which
contain the precursors of glandular secretion, which persist until about 21st day of
cycle. Their characteristic corkscrew appearance is called sub nuclear vacuolation
and is presumptive evidence of progesterone activity and therefore of ovulation, the
fluid in these vacuoles consists of mucin and glycogen. The coiled arteries becomes
more spiral and form closely wound perpendicular columns through the mucosa.
The endometrium measures 8-10mm in thickness in the secretory phase.
About 24th
day of cycle, some shrinkage of glands is apparent, partly due to
the loss of their secretion into lumen and partly due to dehydration of stroma. The
corkscrew pattern now becomes saw toothed. No superficial necrosis has yet
occurred, but the superficial layers are noticeably less vascular. Just before
menstruation there is a well marked local leucocytic infiltration.
MENSTRUAL PHASE (2, 24, 25)
The fundamental cause of menstruation is degeneration of corpus luteum,
usually occurs 14 days after ovulation and it represents the breakdown and casting
off of an endometrium prepared for a pregnancy which does not materialize and so
is sometimes described as the weeping of disappointed uterus.

21
As a result of ovarian cycle the uterus is subjected initially of oestrogen
followed by combination of oestrogen and progesterone. Both of these are
withdrawn when corpus luetum degenerates and menstruation occurs within few
days. The endometrium shrinks. This causes the elongated spiral arterioles, which
have grown to the tip of the surface epithelium to coil and become compressed. This
elicits hypoxia, stasis and vasoconstriction. The inadequate lymphatic supply of
endometrium contributes to an accumulation of catabolic materials, which leads to
tissue destruction, infiltration of lysosomes of the cells, release of acid Phosphatase
and other powerful lytic materials causing digestion of endometrium resulting in
bleeding.
Eventually the entire stratum functionalis sloughs off. At this time the
endometrium is very thin as only the stratum basalis remains. The menstrual
bleeding passes from the uterine cavity to the cervix and through vagina to the
exterior.
Within 4-7 days after menstruation starts, the loss of blood ceases, because,
by this time the endometrium has become re-epithelialized.
MECHANISM OF NORMAL MENSTRUATION:
In normal menstruation 50-75% of the menstrual flow is blood, the rest being
fragments of endometrial tissue and mucus. Menstrual blood does not normally clot
and consists of aggregation of endometrial tissue, red cells, degenerated platelets
and some fibrin. It also contains fibrin degradation products as endometrium
releases fibrinolytic substances that cause any blood clot to disintegrate. These
substances are rapidly consumed and if the blood loss is greater than the amount of
lysine released, then clots may form in the vagina. The passage of blood clots
always indicates excessive menstrual blood loss (27).

22
CHANGES IN THE ENDOMETRIUM:
In the proliferative phase, the spiral arterioles grow upwards from the basal
to the more superficial layers of the endometrium where a capillary network
develops.
In the luteal phase, there is a marked increase in length and coiling of the
spiral arterioles which also become much more dilated (27, 28).
Premenstrually, the endometrial glands are empty of secretion, the fluid from
the stroma is resorbed, the endometrium shrinks and the spiral arterioles become
even more coiled up to 8 loops being added at this stage. At the same time, gaps
appear between the endothelial cells of the spiral arterioles and leucocytes migrate
through the gaps into the stroma which appears to undergo disintegration.
Immediately before menstruation, the spiral arterioles constrict intensively for a
period of 4 - 24 hours and then dilate with a massive extravasation of erythrocytes
particularly in spongiosa layer. Numerous blood lakes appear and the areas of
hemorrhage coalace to lift off islands of devitalized endometrium (27, 28)
Blood initially spurts from the open ends of the spiral arterioles and also
from coalased lakes as well from torn ends of capillaries and veins.
Approximately, 75% of the menstrual blood is arterial and 25% is venous, though
the proportion may change, in women with menorrhagia (28)
Markee postulated that the key event in menstruation is the vasoconstriction
of the spiral arterioles due to liberation of unknown substances in the endometrium
produces vasoconstriction resulting in damage to the walls of spiral arterioles and
necrosis of superficial layer of endometrium (28).

23
ROLE OF PROSTAGLANDINS:
It is likely that the arteriolar constriction and endometrial necrosis are caused
by prostaglandins. They are synthesized from arachidonic acid in endometrium and
myometrium by the enzyme cyclo-oxigenase. Prostaglandin E2 produces myometrial
contraction and vasodilatation. PGI2 (prostacyclin) causes myometrial relaxation
and vasodilatation. It also inhibits platelets activity. PGF2 alpha produces
vasoconstriction as well as myocontraction, hence, PGE2 and PGF2 alpha produces
Dysmenorrhoea and PGI2 can cause menorrhagia (2, 24).
ROLE OF LYSOSOMES:
Lysosomes are intracellular granules that contain large number of enzymes
which initiates cellular digestion, hydrolyze the ground substance of the
endometrium and promote the degradation of collagen fibers (Shaw and Roche
1986).
Lysosomes increase in endometrium in the luteal phase (Wood 1973).
It is suggested that the release of autolytic enzymes on withdrawal of the
ovarian steroids, promotes the regeneration of endometrium in the premenstrual
period (Henzl et al 1972).
Phospholipase A2 enzyme present in lysosomes is important for synthesis of
prostaglandins (5).
HAEMOSTASIS AND ENDOMETRIAL REGENERATION:
Primary haemostasis in the spiral arterioles is achieved by the formation of
plugs of aggregated platelets and fibrin (Christian et al 1980). (27).
The haemostatic plugs which form superficially may be shed with fragments
of endometrium as they are lifted off with reopening of the spiral arterioles followed
by further bleeding and plug formation. About 24 hours after the onset of bleeding,

24
most of the superficial layers of the endometrium have been shed and very few
plugs are seen (27).
After 24 hours, the main mechanism ensuring haemostasis is constriction of
the spiral arterioles together with swelling of the endothelial cells which completely
occlude the arterioles.
Re-epithelialization commences from the basal glands from second day and
proceeds rapidly and is usually completed by third or fourth day (2, 24, 25, 27)
FIBRINOLYSIS AND LIQUIFACTION OF MENSTRUAL BLOOD:
The normally liquid nature of menstrual loss is believed to be an important
part of mechanism of menstruation, facilitating the passage of menstrual products
through the cervix. It also ensures easy and rapid discharge and prevents infections
and adhesions of the endometrium. The endometrium and cervix are sites of marked
fibrinolytic activity. Plasminogen activation has been demonstrated in the
myometrium, endometrium, and menstrual blood. The concentration of plasminogen
activators in menstrual blood is maximal on the first day of bleeding and is higher in
women with excess menstrual blood loss (Bonnar et al 1983). It is also much higher
in samples collected from the uterus than from the vagina, suggesting that the
activators are rapidly consumed and explaining why clots may form in the vagina
but rarely do so in uterus. (27)
Raes MP et al 1985 found that plasminogen and alpha 2 macroglobulin are
more on day 1. Heparin like activity has been demonstrated in uterine fluid and has
been found to increase in menstrual cycle but also to decrease at menstruation.
Menstrual blood contains aggregation of erythrocytes, degraded and exhausted
platelets, small amount of fibrin, and large amounts of fibrin degradation products
suggesting that the haemostatic plugs and any blood clots that may undergo

25
fibrinolysis and rapidly disintegrate. An excess of fibrinolytic activity in the
endometrium might well impair haemostatic plug formation in the spiral arterioles
and wound provide a ready explanation for excessive menstrual blood loss (27).
HORMONAL CONTROL OF MENSTRUAL CYCLE:
The proliferation phase of the endometrium represents the oestrogen part of
the menstrual cycle. It is initiated and controlled by progesterone, although the
effects of progesterone are obtained only after the endometrium has been sensitized
with oestrogen. (2).
These two hormones are secreted by ovary and ovary itself is activated by
the pituitary gland, the secretion of which is under the nervous control of the
hypothalamus. (2).
At puberty, the hypothalamus starts a pulsate secretion of GnRH, resulting in
an activation of H-P-O-uterine axis and in establishment of menstrual cycles.
The GnRH initiates the secretion of FSH and LH, FSH released from
anterior pituitary stimulates the growth of a few primordial follicles into graffian
follicles but only one dominate graffian follicles is selected which fully matures and
ovulates where as other follicles become atretic. The graffian follicles under the
influence of FSH together with only a minimal amount of LH secrete 17ß –
oestradiol. (2).
This 17 –oestradiol has 3 functions:
1. It produces proferalative changes in endometrium.
2. Inhibits further secretion of FSH from anterior pituitary.
3. Stimulates anterior pituitary to secrete LH
Inhibin produced by graffian follicle under estrogenic effect is also
responsible for a fall in the FSH level and stimulation of LH secretion

26
The maximum peak of oestrogen secretion is seen about 48 hrs before
ovulation whereas; LH peak occurs about 24- 36 hours before ovulation.
The LH serves two functions:
1) It stimulates graffian follicle to secrete 17 ß oestradiol.
2) It causes the follicle to rupture at ovulation and to form corpus luteum.
The corpus luteum secretes progesterone the level of which starts rising.
The progesterone has 2 functions,
1. It stimulates the endometrium to undergo secretory hypertrophy.
2. It inhibits further production of LH from anterior pituitary.
In absence of pregnancy both oestrogen and progesterone levels
decline gradually and the fall in the levels of these hormones brings about
menstruation following degeneration of corpus luetum (2).
In anovulatory cycles, fall in level of oestrogen alone can bring about
withdrawal bleeding in the form of menstruation. However the oestrogen
withdrawal bleeding is far heavier than progesterone withdrawal bleeding. (24).
USRE WAZIFI NAZFE RAHAM
The basis of Unani Tibb is laid on the concept of akhlat (humors) and their
respective mizaj (temperament). Buqrat, father of humoral theory states that, “any
change or alteration in humors’ and their temperament either in quantity or quality
will alter the health of a person.”(11).
These changes do occur even when there is change in relation to Asbabe
Sitta Zarooriya, the six basic principles needed for the maintainance of health. They
are ‘atmospheric air’, ‘food and drink’, ‘rest and activity of body’, ‘psychological
activity’, ‘sleep and wakefulness’ and ‘retention and elimination.’ (12).

27
IFRATHE HAIZ (13, 15, 16, 29, 30)
Our renowned unani physicians have described the etiopathology of ifrathe
Haiz under seven categories:
1. Galbae Khoon (excessive congestion of blood):
The increase in volume of blood (plethora) is either due to increase
production of blood or decrease utilization of blood by body tissues. Some times the
quality of blood is so altered that it is not utilized by the tissues, thereby increasing
its volume in blood vessels. Here the body defensive mechanism, Tabiyat plays its
part by eliminating the excess from the body either via nose, gums, and piles or in
females by Ifrathe Haiz.
2. Riqhat o Hiddate Khoon (excess in heat and liquidity of blood):
Sometimes the mizaj of blood increases in heat and becomes more liquefied.
This makes the uterine blood vessels more dilated and tortuous resulting in
excessive uterine bleeding
3. Galbae Safra: (dominance in yellow bile):
Sometimes the dominance of khilt safra alters the temperament of blood by
increase in heat, thereby making the blood vessels of uterus fragile.
4. Galbae Balgham: (dominance of phlegm):
When there is a dominance of khilte balgham in blood, it weakens the uterine
blood vessels and musculature. Khilte balgham by virtue of it mizaj “barid ratab”
increases the fluidity in blood. Hence results in excessive flow of menstrual
bleeding.

28
5. Galbae Sauda: (dominance of black bile):
Emotional disturbances, worry, fright, anxiety, depression etc. are due to
alteration of ones temperament to saudawi. These changes cause disturbance in
menstrual cycle.
6. Zofe Raham: (uterine debility):
Frequent pregnancies, abortions or excessive intercourse weakens the uterine
musculature. This alters the constricting power of uterine blood vessels thereby
resulting in excessive painless menstrual bleeding.
7. Sue Mizaje Raham:
The various pathological conditions in the genital tract such as polyps, ulcers,
injury, carcinoma of uterus or surgery alters the temperament of uterus. Sue Mizaje
Raham weakens the muscles and vessels of uterus resulting in excess menstrual
flow.
Clinical Features and Diagnosis
To know the predominant humor causing the irregular bleeding, the patient is
advised to keep a sterile cotton cloth or swab in the vagina for the whole night. Next
morning the cloth is dried and the colour of the stain is noticed, if it appears to be
yellowish the causative humor is safra; if it is whitish it is balghami and if the stain
is greenish black or banafshi, it is due to the dominancy of sauda in blood.
Along with this the other related clinical features as per the dominancy of each
humor are as follows:
♦ Galbae Khoon:
The plethora is characterized by feeling of heaviness in various parts
of body, redness of complexion, distension of vessels, tightness of skin, fullness of
pulse, high colour of urine, impaired appetite and defective vision (12, 30).

29
♦ Galbae Balgham:
The signs of phlegm being predominant are excessive pallor, flabbiness of
body, cold and moist skin, excessive salivation and viscid saliva. A weak digestion
with acid eructation, pale urine, excessive sleepiness, flabby muscles, mental
dullness and a soft pulse of slow rate and speed are characteristics of this condition
(12, 30).
♦ Galbae Safra:
This is characterized by rough and dry tongue, dry nostrils, excessive thirst,
rapid pulse, lack of appetite, irritative diarrhoea and frequent attacks of tingling in
the skin are the signs of bile being predominant(12, 30).
♦ Galbae Sauda:
The dry and dark skin, thick and dark blood, anxiety, burning in the
epigastrium, false appetite, thick and turbid urine, dark complexion and excessive
hairiness along with this, the patient exhibits the signs of psychosis such as
depression, anxiety, altered mood (12, 30)..
♦ Zofe Raham:
The patient will have painless bleeding along with:
a. History of post coital bleeding or
b. History of leucorrhoea or
c. History of recurrent abortions (14, 15, 16, 30).
♦ Sue Mizaje Raham:
The bleeding per vagina would be blackish in colour, painful, often
accompanied by pus (12, 30).
30
Complications
Due to excessive loss of blood, many conditions develop in the body such
as loss of appetite, zofe hazam, swelling or oedema in limbs and whole body and the
woman becomes pale. Sometimes it may lead to ascites.
Due to excessive loss of blood, safra predominates which cause rigors,
safrawi bakhar and back may ache by virtue of its mizaj (dryness) causing irritation
of local muscles.
Management of UWNR
General principles of treatment (Usoole Ilaaj):
Treatment is carried out by
a) General measures:
♦ Rest and reassurance (31, 32)
♦ Raise the foot end of the bed and apply cloth soaked in ice water on
the suprapubic region at the time of heavy bleeding per vaginum (31,
32).
b) Diet:
Food may be withheld, reduced or given in moderate quantity or purposely
increased depending upon the condition of the disease as well as of the patient (12).
In zofe raham, muqwi foods and drinks such as half boiled egg, red rice,
carbohydrates are advised. Avoid sour, hot and flatulent producing foods.
In galbae khoon, light foods are recommended, e.g., anar dana, kadu,
masoor, angoor, aashe jou, sagu dana, moong ki khichdi. Avoid hot and dry foods
(10, 31, 32).
In galbae safra, angoor, kishmish, abe anar tursh, chawal and moong are
adviced.

31
In galbae balgham, muragh, teetar with zeera and darchini, nukhudab are
adviced.
In galbae sauda, nukhudab along with sheere magze badam, maska and misri
are given.
c) Treatment by Simple and Compound Drugs:
Treat the causative factor using simple drugs along with astringent e.g.,
Bartang, Khurfa, kafoor etc. In compound formulations hakeems have included
astringent and styptics to control, the excessive bleeding. These medicines are given
orally as well as locally in the form of humool, farzaja, zimad etc.
d) Operative procedures (31, 32).
In classic unani literature, it is recommended that plethora can be rectified by
1. Venesection (Fasad):
Venesection Of Basalic Vein
Venesection of basalic vein is advised when the patient is strong and healthy.
In uterine inflammations, basalic vein venesection is comparatively not beneficial as
it draws the menstrual blood upwards and prevents from flowing. Hence,
venesection of leg vein is advised as it facilitates menstrual flow (Al fasad) (14).
Raban tabri advised to use cephalic vein (10).
2. Cupping (Pachne):
Application of large cups is advised below the breast region to divert the
flow of blood from uterus. Uterine blood vessels join the blood vessels of the breast
in the abdominal skin just below the breast (16).
In wet cupping scarifications are made deep enough to draw blood from
the deeper parts as it might be difficult to release the cup, a piece of linen or sponge

32
soaked in warm water should be packed around it to reduce swelling. This is
particularly necessary in the cuppings of breast for menorrhagia and epistaxis (12).
Dry cupping is employed for directing the flow of matter inn the opposite
direction e.g. cupping over the breast for checking menstrual bleeding (12).
Tightly binding at the breast region, helps in reducing the menstrual blood flow.
1. Treatment of anaemia-
Anaemia should be corrected energetically by diet and haematenics.

33
TYPES OF ABNORMAL UTERINE BLEEDING (5, 33)
Polymenorrhoea frequent irregular bleeding at less than 21 days intervals.
Infrequent Cycles Infrequent irregular bleeding at intervals longer than 35
(Oligomenorrhoea) days (25).
Metrorrhagia Intermenstrual bleeding between regular periods.
Menorrhagia Excessive uterine bleeding occurring regularly
(synonymous with the term hypermenorrhoea).
Hypomenorrhoea Decreased menstrual flow at regular intervals
Menometorrhagia Frequent irregular excessive and prolonged uterine
bleeding.

34
DEFINITION OF DYSFUNCTIONAL UTERINE BLEEDING
Dysfunctional uterine bleeding is defined as abnormal bleeding from the
uterus in the absence of organic disease of the genital tract. (7).
Dysfunctional uterine bleeding is the term used to describe abnormal
bleeding because of hormonal abnormalities in the absence of pregnancy, tumour,
infection, or coagulopathy (34).
Dysfunctional uterine bleeding describes the spectrum of abnormal
menstrual bleeding patterns that may occur in anovulatory women who have no
medical illness or pelvic pathology. Anovulatory bleeding can be effectively and
confidently managed with medical treatment regimens based on sound physiological
concepts (5).
According to Jeffcoat’s, the term has been used to cover all forms of
abnormal bleeding for which an organic cause cannot be found. The diagnosis can
only be made by excluding all other causes for bleeding; this means that the
frequency of the diagnosis depends on definition of organic lesions, and on the case
and trouble taken to exclude such a lesion. Dysfunctional uterine bleeding can be
classified according to whether it is ovulatory or anovulatory (25).
According to Shaws, in a larger number of patients, menorrhagia is not
associated with any structural abnormality, disease in the pelvis or evidence of
either general disease or endocrine disorder. If on bimanual examination the uterus
and appendages are found to be normal, the term Dysfunctional uterine bleeding is
used. The etiology is purely hormonal and that the hypertrophy and hyperplasia of
endometrium are induced by high titre of oestrogen in the circulating blood (2).

35
Robert W. Shaw - Dysfunctional uterine bleeding is defined as heavy and/or
irregular menses in the absence of recognizable pelvic pathology, pregnancy, or
general bleeding disorder. (21).
Incidence
DUB is one of the most frequently encountered conditions in gynaecological
practice and forms about 10% of gynae admissions, it may occur in any age between
puberty and menopause but is said to be frequent at the extremes of reproductive life
when menstrual function is being established or declining (20).
The younger the adolescent at menarche, the faster the ovulatory cycles will
occur. According to one study, the time interval from menarche to regular ovulatory
cycles depends on age of menarche. The time from menarche until 50% of cycles
are ovulatory is one year if menarche occurs between ages 12 and 13 years and 4.5
years if menarche occurs at 16 years or older In India the incidence is reported to be
12.6 – 23.17% of all gynaecological admissions (35).
The social and economic cost of menorrhagia is considerable, 28% of female
population consider their menstruation excessive and will plan their social activities
around their menstrual cycles and nearly 10% of employed women will need to take
time off work because of excessive menstrual loss (35, 36).
CLASSIFICATION OF DYSFUNCTIONAL UTERINE BLEEDING (19)
The clinical classification of dysfunctional uterine bleeding is as follows:
1. Ovulatory
a. Mixed Etiology
• Short proliferative and/or secretory phase
• Mid cycle spotting
• Polymenorrhoea

36
b. Corpus luteum insufficiency
• Luteal phase defect
• Premenstrual spotting
• Menorrhagia or hypermenorrhoea
c. Prolonged corpus luteum activity
• Persistent corpus luteum (Halban’s disease)
• Irregular shedding
• Menorrhagia
• Infrequent Cycles (Oligomenorrhoea)
2. Anovulatory
The bleeding pattern shows oligomenorrhoea, hypermenorrhoea,
menometrorrhagia.
CLINICAL VARIETIES OF DYSFUNCTIONAL UTERINE BLEEDING
1. Menorrhagia or hypermenorrhoea:
It is cyclical bleeding at normal intervals which is excessive in amount or
duration. It is most often due to anatomic abnormalities of the uterus, such as
myomas. It is caused by conditions affecting uterus and its vascular apparatus rather
than by any ovarian disturbance or increase in the bleeding surface such as uterine
fibroids and adenomyosis.
It may result from active or passive congestion of uterus or it can be a
manifestation of blood disease characterized by faulty clotting (2, 24, 25).
2. Polymenorrhoea or Epimenorrhoea:
It is cyclical bleeding which is normal in amount but which occurs at too frequent
intervals. Here the uterus is likely to be normal and the error in the cycle is the
result of disease or functional disturbance of the ovary. It occurs when pituitary-
ovarian relationship is upset and when there is active or passive congestion in the

37
ovaries associated with vasomotor disturbances, pelvic infection, and ovarian
endometriosis. (25)
3. Metrorrhagia:
The bleeding is acyclical, irregular or continuous bleeding of any amount. This
sometimes denotes a profound alteration in ovarian rhythm but is more often caused
by a surface lesion of genital tract e.g., Benign or malignant growth with ulceration.
It is also a feature of abnormal pregnancy states such as abortion and ectopic
pregnancy (25).
4. Infrequent Cycles: (Oligomenorrhoea)
Menstrual bleeding occurring more than 35 days apart and which remains constant
at that frequency (24, 25). The error is in the ovary and its controlling factors rather
than in the uterus (25).
5. Hypomenorrhoea:
When the menstrual bleeding in unduly scanty and lasts for less than 2 days. The
causes may be local (uterine synechiae or endometrial tuberculosis), endocrinal
(user o.c.pills, thyroid dysfunction and premenopausal) or systemic (malnutrition)
(24).
6. Menometorrhagia:
It is the term applied when the bleeding is so irregular and excessive that the
menses (periods) cannot be identified at all. The causes may be DUB- usually
during adolescence, following childbirth and abortion and preceding menopause,
sub mucous fibroid, uterine polyp and CaCx and endometrial carcinoma (24).

38
ETIOLOGY AND PATHOPHYSIOLOGY OF DUB:
The finding of the secretory endometrium in 88% of women with
dysfunctional bleeding suggests that anovulation is the exception rather than the
rule. It is concluded that no pituitary-ovarian abnormality is present in the majority
of women with menorrhagia and that bleeding is most likely to be due to local
causes within the uterus.
The postulated mechanisms are the following:
1. Failure in vasoconstriction due to excessive secretion of PGE2 and
increase in PGE2/PGF2 alpha ratio.
2. Failure in formation of adequate thrombotic plugs, perhaps due to
prostacyclin excess or increase in PGI2/TXA ratio.
3. Excessive fibrinolysis with failure in formation of secretory thrombotic
plugs.
4. Increase in vascular endothelial proliferation due to excessive formation
of prostanoids.
5. Failure in vascular endothelial proliferation due to decreased relaxin.
6. Delay in endometrial regeneration.
All these changes may occur as a primary defect in the endometrium or
secondary to changes in the ovary, pituitary, hypothalamus, and higher centers (19,
37)

39
OVULATORY DYSFUNCTIONAL UTERINE BLEEDING
Ovulatory oligomenorrhoea is usually due to a prolonged proliferative phase.
It most commonly occurs in adolescents and may be a normal feature of menarche.
In older women it may precede menopause.
Ovulatory polymenorrhoea is commonly due to a shortening of the
proliferative phase, particularly in adolescents when it is thought to be due to
hypersensitivity of the ovary.
Dysfunctional Bleeding with Corpus Luteum Abnormalities(23)
This is said to occur most commonly in the adult reproductive years.
Corpus luteum insufficiency is due to failure in the development of the
corpus luteum with a decreased secretion of progesterone and estrogen in the second
half of the cycle. Endometrial biopsy may show “irregular ripening” of the
endometrium which is associated with hypermenorrhoea and pre menstrual spotting.
Early involution of the corpus luteum may result in shortening of the menstrual
cycle and polymenorrhoea.
Prolonged activity of the corpus luteum results in “irregular shedding of the
endometrium” and may be associated with development of corpus luteum cyst. It
causes prolonged and excessive menstruation and possibly oligomenorrhoea due to
prolonged cycles.(23)
ANOVULATORY DYSFUNCTIONAL UTERINE BLEEDING (19)
Anovular menstruation occurs at the extremes of reproductive life as a rule
rather than the exception and should be regarded as normal.
Irregular shedding of the endometrium occurs due to progressive rise
followed by sudden decrease of estrogen secretion.

40
Threshold bleeding occurs due to estrogen increase just above the critical
threshold below which the endometrium cannot be maintained.
Metropathia haemorrhagica: This is the classical form of DUB. There is a
slow rise of estrogen and no feedback inhibition of the pituitary and hence
hyperplastic endometrium. This can be followed by either cyclical, continuous or
Acyclical bleeding. The graffian follicles presumably fail to rupture and continue
producing estrogen until the granulosa and theca cells degenerate (19).
PATHOPHYSIOLOGY (2, 24)
The current concept concludes that the abnormal bleeding is most likely due
to local causes in the endometrium. There is some disturbance of the endometrial
blood vessels and capillaries and coagulation of blood in and around these vessels.
These are probably related to alteration in the ratio of endometrial prostaglandins
which are delicately balanced in haemostasis of menstruation.
The endometrial abnormalities may be primary or secondary to
incoordination in the hypothalamo-pituitary-ovarian axis. It is thus more prevalent
in extremes of reproductive period- adolescence and premenopause or following
childbirth and abortion.
Emotional influences, worries, anxieties or sexual problems sometimes are
enough to disturb the normal hormonal balance. (24).
Dysfunctional uterine bleeding is classified into anovulatory (80%) and
ovulatory bleeding (20%), as this helps in understanding the underlined pathology
and its management. It is therefore grouped into:
• Ovular Bleeding
• Anovular Bleeding.(2,24)

41
OVULAR BLEEDING (2, 24, 25)
POLYMENORRHOEA OR POLYMENORRHAGIA
The condition usually occurs following child birth and abortion, during
adolescence, and premenopausal period and in pelvic inflammatory disease.
The follicular development is speeded up with resulting shortening of the
follicular phase. This is probably due to hyperstimulation of the follicular growth by
FSH. Rarely, the luteal phase may be shortened due to premature lysis of corpus
luteum. Sometimes, it is related to stress induced stimulation.
Endometrial study prior to or within few hours of menstruation reveals
secretory changes.
OLIGOMENORRHAGIA (INFREQUENT CYCLES)
Primary ovular oligomenorrhoea is rare. It may be met in adolescence and
preceding menopause. The disturbance may be due to ovarian unresponsiveness to
FSH or secondary to pituitary dysfunction. There is undue prolongation of the
proliferative phase with normal secretory phase.
Endometrial study prior to or within few hours of menstruation reveals
secretory changes.
FUNCTIONAL MENORRHAGIA
Ovular menorrhagia is quite uncommon. Two varieties are found:
� Irregular shedding of the endometrium
� Irregular ripening of the endometrium
The abnormality is usually met in extremes of reproduction period.
In irregular shedding, desquamation is continued for a variable period with
simultaneous failure of regeneration of the endometrium.

42
The possible explanations are:
1. Incomplete withdrawal of LH even on 26th day of cycle –› incomplete
atrophy of corpus luteum –› persistent secretion of progesterone.
2. Persistent LH –› Inhibition of FSH –› suppresses ripening of the follicle
in the next cycle –› less oestrogen –› less regeneration.
3. Variation of the endometrial receptors which are sensitive to the
influence of oestrogen and progesterone.
Endometrial sampling performed on 5th or 6th day of the onset of
menstruation reveals a mixture of secretory and proliferative endometrium. There is
total absence of any surface epithelium.
IRREGULAR RIPENING OF THE ENDOMETRIUM
There is poor formation and inadequate function of the corpus luteum.
Secretion of both oestrogen and progesterone is inadequate to support the
endometrial growth. As such, slight bleeding occurs and continues prior to the start
of proper flow.
Endometrial study prior to or soon after spotting reveals patchy area of
secretory changes amidst proliferative endometrium.
ANOVULAR BLEEDING (2, 24, 25)
MENORRHAGIA:
Anovular bleeding is usually excessive in the absence of growth limiting
progesterone due to anovulation; the endometrial growth is under the influence of
oestrogen throughout the cycle. There is inadequate structural stromal support and
the endometrium remains fragile.

43
Thus, with the withdrawal of oestrogen due to negative feedback action of
FSH, the endometrial shedding continues for a longer period in asynchronous
sequences because of lack of compactness.
CYSTIC GLANDULAR HYPERPLASIA
(Metropathic haemorrhagia, Schroeder’s disease)
This type of abnormal bleeding is usually met in premenopausal women. As
there is no ovulation, the endometrium is under the influence of oestrogen without
being opposed by growth limiting progesterone for a prolonged period. After a
variable period however, the oestrogen levels falls resulting in endometrial shedding
with heavy bleeding. Bleeding also occurs when the endometrial growth have
outgrown their blood supply. Due to increased endometrial thickness, tissue
breakdown continues for a long time. Bleeding is heavy as there is no
vasoconstrictor effect of PGF2 alpha. Bleeding is prolonged until the endometrium
and blood vessels regenerate to control it. (24)
CHANGES IN THE UTERUS
There is a variable degree of myohyperplasia with symmetrical enlargement
of the uterus to a size of about 8-10 weeks due to simultaneous hypertrophy of
muscles. The endometrial changes are classical. On naked eye examination, the
endometrium looks thick, congested, and often polypoidal (multiple polyposes)

44
Figure # 4: UTERINE MULTIPLE POLYPOSIS

45
Figure # 5: DISORDERED PROLIFERATIVE ENDOMETRIUM
Figure # 6: BENIGN ENDOMETRIAL HYPERPLASIA

46
Microscopically,
a. There is marked hyperplasia of all the endometrial components. There is
marked disparity in sizes, some of the glands are small; others are large
giving the appearance of Swiss Chess pattern. The glands are empty and
lined by columnar epithelium.
b. Absence of secretory changes.
c. Areas of necrosis in the superficial layers with small haemorrhagic and
leucocytic infiltration.
CHANGES IN THE OVARY:
Cystic changes may be observed involving one or both the ovaries. The cyst
may be single or multiple and the fluid contains oestrogen. The cyst is of follicular
type. There is no evidence of corpus luteum (24).

47
PATTERNS OF DYSFUNCTIONAL UTERINE BLEEDING ASSOCIATED
WITH ENDOCRINE AND HISTOLOGICAL CHANGES (5)
Menstrual Pattern Ovulation Phase changes Endometrial
histology
Polymenorrhoea
Menorrhagia
Epimenorrhoea
Normal Shortened
follicular phase
Normal
Infrequent Cycles
(Oligomenorrhoea)
Menorrhagia
Normal Long follicular
phase
Normal
Premenstrual
spotting
Menorrhagia
Abnormal corpus
luteum
Short luteal phase Deficient secretory
endometrium
Prolonged cycles Persistent corpus
luteum
Long luteal phase Well-developed
secretory
endometrium
Polymenorrhoea
Menorrhagia
Anovulation
(insufficient follicles)
Short cycle Deficient
proliferative
endometrium
Infrequent Cycles
(Oligomenorrhoea)
Metropathica
haemorrhagica
Anovulation
(polycystic ovaries)
Prolonged cycle Proliferative or
hyperplastic
endometrium

48
CLINICAL FEATURES OF DYSFUNCTIONAL UTERINE BLEEDING (25)
Abnormal uterine bleeding is a symptom and not a disease. Exact details of
the amount, duration and frequency of bleeding must be ascertained. It occurs in
various forms:
� Cyclical bleeding at normal intervals which is excessive in amount or
duration
� Cyclical bleeding, normal in amount but occur at too frequent intervals
of less than 21 days.
� Cyclical bleeding which is both excessive and too frequent.
� Acyclic bleeding of any amount and which occurs irregularly or
continuously in between normal cycles
� Prolonged and irregular bleeding
ASSOCIATED SYMPTOMS AND CHARACTERISTIC FEATURE OF
OVULATORY AND ANOVULATORY DYSFUNCTIONAL UTERINE
BLEEDING (3, 21, 25)
OVULATORY DYSFUNCTIONAL UTERINE BLEEDING
� Regular periodicity
� BBT curve- Biphasic
� Midcycle spotting
� Breast fullness and/or tenderness
� Dysmenorrhoea/menstrual cramps
� Weight gain/Oedema
� Irritable bowel syndrome
� Mood changes
� Secretory endometrium on HPE

49
ANOVULATORY DYSFUNCTIONAL UTERINE BLEEDING
� Most common in postmenopausal and premenopausal periods
� Acyclical bleeding patterns
� Unpredictable as to the onset of bleeding
� Variation in duration of bleeding
� Painless nature of bleeding
� Frequent spotting
� BBT curve-Monophasic
� Non secretory pattern of endometrium on HPE
Other relative features in result of DUB are signs of anaemia-pallor, palpitation,
haemic murmur. Anxiousness, nervousness and depression are present.
DIAGNOSIS AND EVALUATION OF DYSFUNCTIONAL UTERINE
BLEEDING
A diagnosis of Dysfunctional Uterine Bleeding is a diagnosis of exclusion. A
well constructed history and physical examination are of paramount importance.
Organic lesions of the reproductive tract, coagulopathies and endocrinopathies must
be ruled out. Complication of early pregnancy should be considered and should be
excluded by serum ß human chorionic gonadotrophin (ßhCG) (33)
HISTORY (3, 24, 38)
The history includes a detailed menstrual pattern in terms of intervals,
duration, and amount of flow, a list of medications, obstetric history, sexual and
contraceptive histories, as well as general medical history. It should also show any
recent surgical or gyncaecological disorders.

50
PHYSICAL EXAMINATION:
A general examination should take note of signs of anaemia, hypothyroidism,
and clotting disorders.
PELVIC EXAMINATION (5, 24, 39)
A pelvic examination should be complete in both inspection and bimanual
palpation of the external and internal organs. A cervical smear should be taken if
suspicious of lesion. Examination should identify atrophy, cervical polyps,
erosions, cervicitis, or ominous lesions. Bimanual examination should note the size,
regularity of the uterine surface, tenderness, consistency and mobility. Irregularities
of the uterus suggest fibroids, tender fixed uterus suggest PID and endometriosis.
Uniformly enlarged uterus could be due to endometriosis (5).
INVESTIGATIONS (2, 3, 6, 16,):
Haematological investigations-Hb, TC, DC, ESR,
platelet count, BT, CT, RFT, LFT, TFT, and other hormone assay viz PRL, FSH and
LH.
DIAGNOSTIC PROCEDURES
1. Cervical cytology-Papanicolaou smear
2. Endometrial biopsy
3. Pelvic Ultrasonography
4. Hysteroscopy
5. D&C (optional) (8, 40)
DIFFERENTIAL DIAGNOSIS of DYSFUNCTIONAL UTERINE BLEEDING
(3,33,41)
1. Pregnancy complications
• Abortion
• Ectopic pregnancy
• Trophoblastic disease

51
2. Benign and malignant neoplasms of the genital tract
• Cervical polyp
• Vaginal adenosis
• Vaginal carcinoma
• Granulosa-theca cell tumours
• Endometriosis
• Leiomyoma
3. Genital Tract Infections:
• Vaginitis
• Cervicitis
• Vaginal foreign body
• IUCD
• Salpingitis
4. Endocrinopathies
• PCOD
• Hyperprolactinomas
• Hypothyroidism
• Hyperthyroidism
5. Administration of drugs or hormones (exogenous)
6. Trauma
7. Coagulation Disorders
• Idiopathic thrombocytic purpura
• Von Willebrand disease
8. Chronic systemic illness
• Liver cirrhosis
• Renal failure
TREATMENT :( 2, 3, 5, 14)
The objectives of treatment are:
� To control bleeding.
� To prevent recurrence.
� To preserve fertility if required.

52
� To correct associated conditions, e.g. hypothyroidism and liver disease.
� To induce ovulation if desiring conception (5).
The patient’s age, severity of bleeding, desire for future fertility and the
presence of associated problems influence the type of treatment.
Many types of medical and surgical treatment options are available.
Reassurance is one of the important aspects of treatment. Greenburg found
that 53% of women referred to a gynecological clinic had mild to moderate
depression. Women who score highly on psychiatric scores are more likely to
complain. Menses is often a reflection of mind is a well-known statement in Indian
thought (5).
MEDICAL TREATMENT:
Medical treatment is the preferred management for dysfunctional uterine
bleeding. The selection of treatment depends on whether it is used to stop an acute
heavy bleeding or to control recurrent episodes.
TREATMENT OF ACUTE BLEEDING:
Oral conjugated equine oestrogens 10 mg a day in four divided doses reduces
the bleeding within 24 hours. Even after the bleeding stops, oestrogen is continued
in a lower dose for 21 to 25 days and progesterone is administration for the last 7 to
10 days of a cycle.
A combined oral contraceptive pill with high oestrogen content is
administered in the dosage of four tablets per day in the treatment and once the
bleeding is under control, the number of pills may be gradually reduced to one pill
per day for another 20 days to finish the cycle. (36)

53
Instant control of bleeding can be achieved by inflating a Foley catheter 30
ml balloon inside the uterus. D and C is used in severe or persistent bleeding with
failure of other methods.
Drugs used during menstruation-Antifibrinolytics and nonsteroidal anti-
inflammatory drugs (NSAIDs) are effectively used with ovulatory dysfunctional
uterine bleeding (5, 22).
Antifibrinolytics (Tranexamic acid, epsilon-aminocaproic acid, ethamsylate,
dicynene)
Tranexamic acid acts by inhibiting plasminogen activator, which is increased
in dysfunctional uterine bleeding. The menstrual loss was reduced by 50% in
ovulatory menorrhagia as compared to norethisterone which in fact was found to be
associated with increased bleeding. The reduction is markedly seen in women who
exhibited the highest amount of menstrual loss. The most common side-effects are
nausea and vomiting. No increase in incidence of thromboembolism was
demonstrated in larger studies. Tranexamic acid is used in the dosage of 3-6 gm per
day, ethamsylate is the least effective though marketed most widely in developing
countries (5, 23, 34).
In a comparative study of Tranexamic acid and norethisterone in the
treatment of ovulatory menorrhagia it is found that Tranexamic acid is a safe and
effective medical therapy in menorrhagia and is likely to normalize blood loss in
women loosing 80 – 200ml prior to treatment. Norethisterone at this dose is not an
effective for ovulatory menorrhagia (42).
NSAIDs:
NSAIDs act by inhibiting cyclo-oxygenase, thereby reducing the production
of endoperoxides. The Fenamates also block the myometrial PGE2 receptors. The

54
NSAIDs also have an analgesic action and hence useful in patients with
dysmenorrhoea. Mefenamic acid 500 mg tds, Ibuprofen 400 mg tds, Naproxen
sodium 275 mg qid are useful in women with heavy menstruation, especially
ovulatory. The reduction in blood loss is 20-50% in about 75% of women.
In a randomized control trial of ethamsylate, Mefenamic acid and tranexamic
acid: Mefenamic acid is a NSAID which has been widely used for Dysmenorrhoea
and menorrhagia. Given at a dose of 500mg every 8 hours for 3 days, it resulted in a
20% decrease in blood loss however tranexamic acid, and antifibrinolytic agent
which is a competitive inhibitor of plasminogen activation, was most effective,
resulting in a 54% reduction in MBL (43).
DRUGS USED IN CYCLICAL FASHION
Combined Oral Contraceptive Pill
The mean blood loss with COC is reduced by 50%. Apart from reduction in
blood loss the pill has the advantage of regulating the cycle and providing
contraception. Thus, it is useful in both ovulatory and anovulatory haemorrhage. In
the absence of smoking and risk of thrombosis, it is an effective treatment. Low
dose pills with fourth generation progesterone can be used even in the elderly.
Caution should be taken in prescribing it to early teenagers since there is theoretical
possibility of causing early epiphyseal arrest. The mechanism of action is mainly
local with the inactivation of endometrium and in addition, reduction in
prostaglandin synthesis and impaired fibrinolysis.
Progesterones:
Norethisterone and Medroxyprogesterone acetate are most frequently
prescribed medical agents but without much effect in ovulatory cycles. The effects
may depend on duration and dose of drug administered. In anovulatory

55
menorrhagia, Medroxyprogesterone acetate 10 mg t.i.d used from day 12 of the
cycle for 14 days showed reduction of menstrual blood loss (MBL) of 50%.
Norethisterone, which is widely used, has adverse effects on lipid metabolism,
carbohydrate metabolism, and coagulation. Hence, it is better avoided in patients
with hypertension, diabetes, dyslipidaemia (4, 5, 23).
DRUGS USED THROUGHOUT THE CYCLE:
Danazol is a synthetic androgenic steroid, which is effective in inhibiting the
endometrial growth by acting at various levels. It blocks the androgen and
progesterone receptors, inhibits sex steroid synthesis and at higher doses inhibits
pituitary gonadotrophin.
The reduction in blood loss is proportional to the dosage use. With a dose of
400 mg, 50% of women become amenorrheic. There is a gross reduction in the
menstrual flow if the woman is menstruating. With 200 mg and 100 mg the blood
loss was reduced by 86 and 57% respectively. A carry over effect, i.e. decrease in
blood loss continued for many months after stopping the drug.
An overview: Levanorgestrel and Ethinyl Estradiol is one among other various
hormonal assays used as cycle-regulators that enable the application of correct
dosage and they bring about suitable hormonal levels in menstrual irregularities (23,
44)
GnRH:
Treatment with GnRH agonist results in medical menopause. After the
therapy is discontinued the menstrual blood loss returns to pretreatment levels. A
more useful application of this treatment is to suppress endometrial growth before
endometrial ablation (2, 3, 5, 23, 24).

56
Levanorgestrel-Releasing IUCD:
Anderson and Rybo reported a reduction in the menstrual loss by 86, 91, and
97% at 3, 6, and 12 months, respectively.
It is an effective nonsurgical treatment for the management of Menorrhagia
and Dysmenorrhoea that has additional benefit as a contraceptive and in relieving
premenstrual syndrome (45).
Intrauterine Progestins:
Intrauterine devices and systems were developed for contraceptive purposes,
but the hormone – containing devices also provide severe noncontraceptive health
benefits. Progesterone,” a uterine relaxing hormone”, was initially added to inert
contraceptive intrauterine coils to decrease expulsion and improve contraceptive
action. Subsequent experience in women using both the Progestasert (releasing
65mcg of progesterone a day) and Mirena (releasing 20mcg of Levanorgestrel a
day) for contraception demonstrated a significant decrease in menstrual flow. The
LNG-IUS (Mirena, Berlex) was approved by the Food and Drug Administration
(FDA) in 2000 as a contraceptive only.
The LNG-IUS has several noncontraceptive healthy benefits. It has been
shown to increase haemoglobin, decrease menstrual loss by 74% to 97% and
therefore anaemia, reduce bleeding caused by fibroids and adenomyosis, and
provide an acceptable alternative to surgery. A recent decision analysis showed that
the LNG-IUS ranks higher than all other medical treatments when effectiveness,
side effects, length of treatment and acceptability are considered (4, 34, 45).

57
SURGICAL MANAGEMENT:
About 15% of women seek surgical solution to menstrual dysfunction. The
surgical methods could be minimally invasive or hysterectomy. The minimally
invasive procedures are D and C and endometrial ablation.
Endometrial ablation:
Many methods of ablating the endometrium have been tried like Laser
ablation, Resectoscope, Microwave ablation, Thermal balloon, and Cryosurgery.
Although, these techniques cannot guarantee amenorrhoea, they are much more
effective than medical therapy.
The main advantages are short hospital stay, short postoperative recovery
time, and lower incidence of serious complications. Since the morbidity is low, it
could be performed in medically high-risk patients and obese patients (24, 35, 46).
Hysterectomy:
Hysterectomy should be the last resort of treatment of dysfunctional uterine
bleeding. It is indicated only when all methods fail or the woman has associated
symptomatic pelvic pathology. However, the use of Levanorgestrel IUCD and the
ablation procedure should reduce the rate of hysterectomy for dysfunctional uterine
bleeding (3, 4, 5, 24, 25 ).

58
MATERIAL AND METHODS:
The study was conducted during 2005 – 2007 in the dept Of Ilmul Qabalat
wa Amraze Niswan National Institute of Unani Medicine, Hospital, Bangalore, and
60 clinically diagnosed cases of DUB from both OPD and IPD were enrolled in the
study. Detailed complaints and specific history was entered in the specific proforma,
Annexure # 1.
Criteria for selection of patients:
In this study all patients with abnormal uterine bleeding were selected with
following
Inclusion criteria:
♦ Patients with abnormal uterine bleeding without any pelvic pathology.
♦ Patients able to participate in the study and ready to follow the instructions
and sign the consent form.
♦ Both married and unmarried.
♦ Both Nulliparous and Multiparous.
♦ Patients with extended duration of flow to their previous habits of 5-6 days
or bleeding for more than 9 days.
♦ Frequent / early menstrual cycle of less than 21 days.
♦ Infrequent cycles followed by heavy prolonged bleeding phase.
♦ History of one or more above complaints atleast for 2-3 cycles.
Exclusion criteria:
♦ Patients with organic lesions in the pelvis viz fibroids, adenomyosis,
endometrial polyp, carcinoma insitu of endometrium.
♦ Severe systemic diseases – DM, IHD, HTN, TB.
♦ Blood dyscrasias

59
Case Evaluation:
Clinical history of each patient was carefully recorded in detail. This includes:
♦ Age, socio economic status and parity.
♦ Amount, duration and pattern of uterine bleeding and its relation to last
menstrual period.
♦ The amount of bleeding judged by number of pads changed per day, by the
presence of clots and by the presence or absence of anaemia.
♦ Any symptom suggestive of bleeding disorders and endocrinological
disorders were noted.
♦ History of any intake of exogenous, sex steroids, anticoagulants, NSAIDs
was noted.
♦ The patient was asked for any significant past and family history.
♦ A detailed general and systemic examination was done. The pulse, blood
pressure was noted, the CVS and RS were examined, and breast and thyroid
were examined.
♦ Per abdomen examination was done to rule out any organomegaly.
♦ Per speculum examination was done to visualize the vagina, cervix and also
to rule out any local lesion.
♦ Bi manual examination was done to note the position, size, consistency and
mobility of the uterus and to rule out any adnexal mass.
♦ Per rectal examination was done wherever necessary.
♦ Temperamental evaluation was done as per Annexure # 3.(47)
♦ Assessment of menstrual blood loss is done by using the Pictorial Bleeding
Assessment Chart. (Annexure # 4) (48, 49) The patients of both Groups
were given the charts before and after treatment to assess the MBL of their
periods.

60
Investigations done
Routine investigations viz, complete blood count, BT, CT., RBS, LFT, RFT,
VDRL and specific investigations such as, USG to rule out Pelvic Pathology,
Hormone profile viz, T3, T4, TSH and PRL, FSH, LH, Endometrial biopsy and
Histopathology were done.
Study design: Standard control randomized single blind study.
Randomization was done by number method using probability sampling
method. (50)
Evaluation of result was done by,
� By relief of symptoms.
� By student’s paired t’ test.
� By chi-square test.
Sample size – 60 patients of clinically diagnosed DUB cases
30 patients in test group
30 patients in control group
Duration of therapy - 3 menstrual cycles – for 10 days in each cycle/as per the
assessment of the patient in 3 consecutive cycles.
Follow up – Every menstrual cycle during the study period.
Informed consent – Patients fulfilling the inclusion criteria were given full
information having details regarding the nature of study and those patients agreed to
participate in the study were enrolled after signing the informed consent form,
Annexure # 2.

61
PHARMACOGNOCY OF DRUGS:
The drugs selected in the test group have haemostatic, astringent, anti-
inflammatory and analgesic effect which may act locally on the uterine musculature
and uterine blood vessels to control the excessive menstrual blood loss from the
uterus. These drugs are cost effective, easily available and well tolerated by the
patients without any side effects.
Test group
1. GERU Red ochre 3gm
2. GULNAR Punica granatum linn 2gm
3. DAMMUL AKHWAIN Dracaena cinnabari 1gm
4. BARG BARTANG Plantago lanceolata 10gm
The first three drugs were finely powdered and made 2 doses of 3gms each.
Dosage – 3gms BID along with Joshanda Barge Bartang 50ml BID from the 3rd
day
of cycle for 10 days in each cycle / as per assessment of the patient.
Method of preparation of Joshanda Barg Bartang:
Mix 10gms of powder of Barge Bartang in 100ml of water, soak for 2 hours
and boil it and filter.
Control Group:
The standard drug tablet styptocid 1 BID was given from 3rd
day of the cycle
for 10 days in each cycle or as per the assessment of the patient in 3 consecutive
cycles.
Haematinic Qurs Kushta Foulad 1 BID for 90 days was given to the patients of
both groups.

62
Figure # 7: GERU (RED EARTH)

63
GERU (RED EARTH):
Pharmaceutical Name: Koalinum
Vernacular Names:(51, 52, 53, 54)
Arabic: Teene Ahmar
English: China clay/ Kaolinite/ red ochre
Hindi: Chiknimati/ Geru
Kannada: kempu mannu
Persian: Gile mugrah, Gile surkh
Tamil: Sona Geru, Hiringi powder
Habitat :
The term ‘Koalin’ derived from koaling, the name of a high ridge in Kiangsi,
China, where clay was mined centuries ago (55). Geru is a native white aluminium
silicate found in Ceylon, China etc. In India it is obtained in Gwalior and the
Baghdad variety is said to be of high quality which is reddish black in colour (54).
Description :
Geru is obtained by purifying native white feldspar or aluminium silicate by
elutriation which removes silica and undecomposed feldspar. Geru is a clay found in
lead and iron ore and contains an excess of oxide of iron over any other clay. There
are two varieties – bole (yellow) and red ochre. The red ochre contains more iron
than the bole and is used in medicine. It rapidly absorbs water if poured upon it (54).
Geru is of two types (1):-
1. Bright red and pure called as “Sona Geru” and (56)
2. Dull red in colour and impure form.
Best variety is that which is clean and swells in water (54).
Parts used: Clay
64
Parts under study: clay
Chemical constituents:
The Koalin group includes three minerals that have essentially the same
chemical composition (Al2O3: 3SiO2: 2H2O) but that differ in crystallization:
Kaolinite, dickite and nacrite.
Pure Koalin contains Alumina 70, silica 26 and iron oxide 4 % (54),
Mizaj (Temperament)
Cold 20 dry 2
0 (53, 54, 57)
Cold 10 dry 2
0 (54)
Af’aal (Actions and uses):
Haemostatic, anti- inflammatory,adsorbent (mughrey), antidiarrhoeal,
antipyretic and dessicant (mujaffif).
It is used as an antidiarrhoeal in dysentery, cholera, diarrhoea. It is beneficial
in healing of septic wounds (53, 54, 57).
Koalin probably owes its value to,
a) absorption on the surface of its fine molecules of toxins; thus it is of great
value in cases of food poisoning also.
b) Its mechanical protective coating of the acutely inflamed gut.
c) Finally the range of therapeutic application of kaolin is not confined to
intestinal disorders, and in relieving bleeding from internal organs. It is value in
infantile diarrhoea: as a local application in diphtheria of the throat and on burns; for
local treatment in leucorrhoea and in vaginal and uterine inflammation and lastly,
for disinfection of the surgeon’s hands before operation, where thorough rubbing of
the hands with purified kaolin will - it is believed - remove all septic infection
65
from the skin without causing the irritation of the skin so common with the use of
the usual surgical antiseptics (54)
It is beneficial in controlling excessive bleeding from uterus (53, 54, 56). It
enters into the composition of several compound formulations for relieving bleeding
from internal organs.
Geru and phitakri equal quantity; 6 masha of this powder is beneficial in controlling
excessive uterine bleeding and wakes the cycles regular.
Externally, as a zimad for its anti inflammatory effect and is useful in skin eruptions,
healing of wounds.
Badal: (Substitute) - Gile Armarni – equal dose
- Kateera - ¼th dose
Muzir:(Toxic) Produces sudda in intestines (53, 54,57,)
spleen (54)
Mus leh:(Corrective) sharbat banafsha
sugar syrup
Miqdaare khorak:(Dose) – 1 - 3 masha powder form
1 tola as nukhu (58)
2 - 3 masha (53)
7 – 9 masha (54)
Compound formulations:
Safoofe istehaza
Safoofe teen
Geru is used along with other styptics like sange jarahat, kahroba, dammul akhwain,
mazu, phitakri, locally in the form of intravaginal douche and as well orally in tablet
or powder form to control excessive blood loss from the uterus ( 54, 56).

66
GULNAR
Figure # 8: Gulnar

67
GULNAR
Botanical name: Punica granatum linn (52,59)
Family: Punicaceae; Lythraceae
Vernacular names: (58)
Arabic: Julnar
English: Pomegranate (wild)
Hindi: Anar, Dhalim
Kannada: Dalimba
Persian: Gulnar
Urdu: Gulnar
Tamil: Madalai
Habitat:
The tree is found wild in Persia, Arabia, Afghanistan and Baluchistan and
cultivated nearly all over India, Himachal Pradesh. It grows in the vast tract of the
hill slopes of Jammu and Kashmir and Himachal Pradesh (55, 59).
One of the important centers of wild pomegranate in Himachal Pradesh is
Darlaghat; literally it means a place of wild pomegranate trees (55).
Description:(51, 52, 54, 60 )
An attractive shrub or small tree 20 – 30 ft height, bark smooth grey, thin,
branched, more or less spiny. Leaves are evergreen or deciduous, opposite or in
whorls of 5 or 6, short stemmed, oblong, lanceolate 3/8 to 4 inch long and leathery.
Flowers are borne on the branch tips singly or as many as 5 in a cluster.
Fruit 3.5 – 7.5cm in diameter, globose, tipped with the calyx, rind
coriaceous, woody, the interior septate with membranous walls of the carpels, each

68
carpel containing numerous seeds, angular from mutual pressure. Seeds with a
watery outer coat contain pink juice and a horny inner coat.
Parts used: flower, rind of fruit, fresh fruit juice, dried bark of stem and root (53,
57, 58, 61).
Part under study: flower.
Morphology of flower:
Flowers are 3.8 – 5cm long and as much across, mostly solitary, sometimes 2
– 4 together, terminating short shoots, sometimes apparently axillary sessile or
nearly so. Calyx-tube campanulate, adnate to and produced beyond the ovary,
coriaceous, lobes 5-7, valvate. Petals 5-7, obovate, scarlet, wrinkled, inserted
between the calyx lobes. Stamens are numerous, inserted on the calyx below the
petals at various levels; anthers elliptic, dehiscing longitudinally. Ovary inferior,
many celled, the cells arranged in two concentric circles; style long, bent; stigma
capitate. Carpels early coalescing and owing to unequal growth becoming arranged
in 2 tiers, 3 in the lower and 5-9 in the upper (52).
Chemical constituents:
The fresh rind of the fruit contains wax, 0.8; resins, 4.5; mannitol, 1.8; non-
crystallized sugars, 2.7; gums, 3.2; insulin, 1.0; mucilage, 0.6; tannin, 10.4; Gallic
acid, 4.0; and calcium oxalate, 4.0% (51).
Tannin occurs in all parts of the tree, particularly in fruit rind (up to 26% in
dried rind), stem bark (10-25%, root bark (28%), and leaves (11%).
The yield a light red dye, they contain the pigment pelargonidin 3,5 –
diglucoside (51).
The rind also contains isoquercetrin (51).

69
The bark of the stem and roots contains a number of alkaloids belonging to
the pyridine group. They are pelletierine, isopelletierine, pseudopelletierine,
methylpelletierine and methyl isopelletierine (51).
Mizaj (Temperament) Cold 10 dry 2
0 (53, 54)
Cold 20 dry 2
0 (57, 59)
Cold 30 dry 3
0 (59)
Af’aal: (Actions and uses)
Astringent, haemostatic, antihelminthic, stomachic (51), dessicant (53, 57,
58, 59).
Flowers are used as astringent in diarrhoea, dysentery. They control the
bleeding from internal organs (53, 57, 58); used in epistaxis;
The flowers are styptic to the gums, check vomiting, useful in biliousness,
sore eyes, ulcers, sore throat. It is used as a good astringent injection in leucorrhoea
and uterine hemorrhages’, ulcer of uterus and of the rectum. The powdered flower
buds are used in bronchitis (51, 53, 57, 58, 59, 60).
Unripe flowers are dried and powdered to make a snuff, a best astringent in
nasal haemorrhage while internally it is effective in infantile diarrhoea and dysentry
( 54, 58, 59). Taking three small buds avoids conjunctivitis (Kertitis) for duration of
one year (54).
*Gulnar with other styptics is recommended in excessive menstrual flow (30)
*Gulnar is used locally in the form of Zimad, Farzaja, Humool, Aabzan & Hukhna
in Kasrat - Tams (14, 16, 18, 29, 30, 62)
*Gulnar is one of the effective ingredients in oral formulation used in Kasrat Tams.
(14, 13, 16, 18, 29, 30, 31, 32)

70
Badal: (Substitute) Buds, bark of Punica granatum
Jufth balooth (53, 56, 57, 58, 59)
Muzir: (Toxic) produces headaches, sudda ( 55, 57, 59)
Mus leh:(Corrective) kateera ( 55, 57, 59)
Miqdaare khorak:(Dose) 3 - 5 masha (flowers)(57)
6 or 7 masha (53, 59)
7 masha (seeds)(53, 59)
Compound formulations:
Sharbat Haabis
Qurs Kahroba
Majoon Busud
Qurs Gulnar
Advanced research:
♦ “Whole plant paste of Doob and buds of Punica granatum is taken with
filtrate of rice in scanty and irregular periods” (63).
♦ “Flowers of Gulnar farsi, Punica granatum linn are reported for astringent
and styptic properties and are also beneficial in the treatment of diarrhoea and
dysentry.(64, 65)
♦ Following administration of cholesterol-4-14
C to leaves of Punica granatum
plants, radioactive pregnenolone was isolated and identified by thin-layer and
gas chromatography and the formation of the acetate derivative.(66)
Estrone was isolated from pomegranate seeds and its identity was confirmed by thin-
layer chromatography in three solvent systems and by four color reactions. Three
derivatives were prepared and had the same chromatographic characteristics in three
solvent systems as the corresponding derivatives from authentic estrone. The
biological potency of this material was also comparable to that of estrone.
Pomegranate seeds are the richest plant source of steroidal estrogens yet found.(67)

71
DAMMUL AKHWAIN
Figure # 9: Dammul Akhwain (70)

72
DAMMUL AKHWAIN
Botanical name: Dracaena cinnabari (59)
Family: Dracaenaceae / Ruscaceae
Vernacular names: (53)
Arabic: Dammul akhwain
English: Dragon’s blood
Hindi: Heera dhan / rang barat
Persian: khoon siyashan
Urdu: damm ul akhwain
Habitat:
Dracaena draco, a native of Canary islands and Morocco, the resin is exuded
from the wounded trunk or branches of the tree. Dragon’s blood is also obtained by
the same way from Dracaena cinnabari which is endemic to the islands of Socotra
east of Somalia.(51, 68)
Description: (68)
Dragon’s blood is a bright red resin that is obtained from different species of
four distinct plants genera – Croton, Dracaena, Daemonorops and Dterocarpus.
Both Dracaena and Daemonorops are still often marked in contemporary times as
Dragon’s blood with little or no distinction between the plant sources.
Dracaena draco, a native of Canary Islands and Morocco, the resin is exuded
from the wounded trunk or branches of the tree. Dragon’s blood is also obtained by
the same way from Dracaena cinnabari which is endemic to the islands of Socotra
east of Somalia.
Dragon’s blood is also produced from the rattan palms of the genus
Daemonorops of the Indonesian islands. It is gathered by breaking off the red resin

73
encasing the unripe fruit the rattan. The collected resin is then rolled into solid balls
before being sold.
Daemonorops draco
The long slender stems of the genus are flexible and the older trees develop
climbing propensities. The leaves have prickly stalks which often grow into long
tails and the bark is provided with many hundreds of flattened spines. The berries
are about the size of a cherry and pointed. When ripe they are covered with a
reddish, resinous substance which is separated in several ways, the most satisfactory
being by steaming, or by shaking or rubbing in coarse, canvas bags.(68).
Dracaena cinnabari
Dracaena is a genus of about 40 species of trees and succulent shrubs in the
family Dracaenaceae / Ruscaceae or in Agavaceae.
Dracaena species is divided into two groups or genera:
1. A group of tree-size species with stout trunks and stiff, broad-based leaves,
growing in arid semi-desert areas, and known as dragon trees.
2. A group of smaller shrubby species with slender stems and flexible strap-
shaped leaves, growing as under storey plants in rainforests (and very popular
as houseplants), and known collectively as shrubby Dracaenas.
Although a monocotyledon Dracaena stem shows secondary growth
different from the secondary thickening found in dicot plants and is termed as
dracaeraid thickening.(68)
Parts used: Resinous exudation
Part under study: Resin

74
Morphology of resin:
Resin form an ill defined group of products, which are produced normally
during growth or secreted as a result of injury to the plant. As a class, resin is related
to one another more by their physical properties and appearance than by any
similarity in chemical composition. They are usually brittle amorphous solids, which
fuse readily on heating, after passing through a preliminary stage of softening. They
are insoluble in water but dissolve in alcohol or other organic solvents which on
evaporation; deposit the resin, as a varnish like film. Resin burn with a characteristic
smoky foam giving an aroma of Loban (58)
Chemical constituents:
Several analyses of Dragon’s blood have been made with the following
results:
1. 50 – 70 percent resinous compound of benzoic and benzoyl-acetic acid, with
dracoresinotannol, and also draco alban and dracoresene.
2. 56.8 percent of red resin compounded of the first three mentioned above, 2.5
percent of the white, amorphous dracoalban, and 13.58 of the yellow, resinous
dracoresene, 18.4 vegetable debris and 8.3 percent ash.
3. 90.7 percent of red resin, draconin, 2.0 of fixed oil, 3.0 of benzoic acid, 1.6 of
calcium oxalate and 3.7 of calcium phosphate.
4. 2.5 percent of dracoalban, 13.58 of draco resin, 56.86 of dracoresin, benzoic
dracoresinotannol ester and benzoylaceticdracoresinotannol ester with 18.4 of
insoluble substances (56).
5. It also contains cinnamic acid. (68).

75
Dragon’s blood is not acted upon by water, but most of it is soluble
in alcohol. It fuses by heat. The solution will stain marble a deep red,
penetrating in proportion to the heat of the stone.(56)
Mizaj (Temperament) Cold 30 dry 3
0 (53, 57, 59, 61)
Cold 20 dry 2
0 (59)
Cold 10 dry 3
0 (59)
Cold 30 dry 2
0 (58)
Af’aal: (Actions and uses)
Haemostatic, strong Astringent,
It promotes healing of wounds and to stop bleeding. It is used as haemostatic to stop
external as well as internal bleeding. Cooling effect on stomach and liver cures in
dysentery, diarrhoea, for ulcer of mouth, throat, intestine and stomach (53, 55, 57,
59).
As surma increases the vision and helps in healing of ulcers of eyes. As manjan
(tooth powder) strengthens the gum (52, 53, 55, 59).
Used in haemoptysis, menorrhagia and bleeding piles to control bleeding (52, 53,
55, 54, 59).
It is a strong astringent, hence used in Kasrat Tams caused by infections and
ulceration of uterus. (13).
It is also used locally as pessary, Zimad etc. in Kasrat-Tams.(29, 30, 62)
Dioscorides – use the dragon’s resin as a sort of cureall, for general wound healing,
a coagulant, curing diarrhoea, lowering fevers, dysentery diseases, for ulcers of
mouth, throat, stomach, intestine, antiviral for respiratory viruses, stomach viruses
and for skin disorders as eczema.(56)

76
In folk medicine - it is used as a wash to promote healing of wounds and to stop
bleeding. Used internally for chestpain, postpartum bleeding, internal trauma and
menstrual irregularities (wikipedia).(56)
Badal (Substitute) : Kaju, Usara Kahu, Shadnaj, Akhakhia.
Muzir (Toxic) : Kidney
Mus leh (Corrective): Kateera, Gond babul.
Miqdaare khorak (Dose) : 1 - 1½- masha (57)
2 - 4½ masha (53)
1 – 4 masha (59)
Compound formulations:
Safoof Istehaza Majoon Busud (13)
Qurs Kaknaj Hab Habis suddam (54)
Qurs Bawaseer
Majoon Tewaaj

77
BARG BARTANG
Figure # 10: BARG BARTANG

78
BARG BARTANG
Botanical name: Plantago lanceolata (55, 60)
Family: Plantaginaceae
Vernacular names (52, 53, 59)
Arabic: Lissanul hamal
English: Rib grass / ripple grass / snake plantain.
Hindi: Baltanga
Persian: Bartang
Urdu: Bartang
Habitat:
Western Himalayas from Kashmir to Simla about 5000 – 8000ft salt range,
Waziristan, Ceylon (introduced) Europe and North Asia, hills of south India (51,
59).
Description:
This is a very dark green slender perennial herb. The leaves are lanceolate
about an inch in breadth and 3-4 inches long, 3-5 ribbed and narrowing into petioles.
The leaves contain good fiber.(58).
The flower stalks are longer than the leaves, often more than 2ft long,
furrowed and angular, terminating in cylindrical plant, dense spikes about ½ - 3 or 4
inches long. Two lower sepals usually united. Stamens far protruding, Capsule
containing 2-4 oblong seeds. (52, 56)
The seeds are covered with a coat of mucilage, which separates readily
when macerated in hot water. (56)
The leaves of Bartang resembles wolf’s tongue, hence the name Lisanul
Hamal in Arabic (57)

79
Parts used: Roots leaves and seeds.
Part under study: Leaves.
Chemical constituents:
Leaves contain tannin (2.1%), carotene (0.56mg/100gm), thiocyanogen
20mg/100gm of leaf juice, alkaloids (0.26%), protein (8.5%), calcium (1.56%) and
phosphorus (0.88%)(51).
Galactose (44.0%), arabinose (32.0%), glucose (9.0%), rhamnose (7.0%),
mannose (4.0%) along with xylol and fucose obtained by complete hydrolysis of
total mucilage(69);
Crude polysaccharide from leaves composed of galacturonic acid (31.0%),
Galactose (28.0%), arabinose (20.0%), glucorunic acid (7.0%), glucose (6.0%),
rhamnose (4.0%), mannose (2.0%), fucose and xylose.(69)
A glucoside aucubin C13 H19O8H2O has been isolated from the leaves, roots
and seeds. (54,59)
Mizaj (Temperament) cold 20 dry 2
0 (12, 53, 57, 58, 59)
cold 30 dry 3
0 (Jalinoos)
Af’aal (Actions and uses)
The leaves are : Astringent, haemostatic, analgesic, controls internal
bleeding.
Seeds are: Diuretic, purgative and haemostatic.
The leaves are used in diarrhoea, piles.
They are considered cooling, alternative, and diuretic.
In Europe the leaves are considered astringent and useful for healing sores (52, 53,
59).

80
It is used in hemoptysis, tuberculosis, pulmonary ulcers. Extract of leaves is
beneficial for spleen and kidney diseases.
It is used for piles, menorrhagia, chronic fevers, and mumps and relieves dyspepsia.
Aab Bartang Sabz used in the form of Douche and found to be very effective in the
treatment of Kasrat Tams (Jalinoos) (14, 16)
Aab Bartang/ Joshanda Bartang is given as a vehicle (Badrakha) along with other
astringents (13).
Bartang is beneficial in Har Nazf hence used locally as a douche in chronic and non
chronic hemorrhages’ (Avicenna) (30).
Bartang is included in zimadath, Farzajat and Humool preperations for controlling
bleeding from Uterus (58)
Badal: (Substitute) - Barge-hamaz bustani (53, 59).
Seeds are used as substitute for leaves and vice versa.
Muzir: (Toxic) - lungs and spleen
Mus leh:(Corrective) - honey, mastagi, banafsha (52, 53, 57)
Miqdaare khorak:(Dose) -5-7 tola of Aab murrawikh(52, 53,57, 59)
- 7 masha of seeds
Latest research:
New compound plantamajoside has also been isolated which showed
antibacterial activity against E. coli and Staphylococcus aureus. (69)
Plantago lanceolata - All the plantains contain high level of tannins. The astringent
property of the leaves due to the tannin makes the leaves useful for all types of sores
on the skin, cuts, bites and various inflammations. (68)
Compound drugs
Safoof Teen
Safoof Istehaza

81
Phi STYPTOCID
COMPOSITION:
Each Tab Contains:
1. Adrenochrome Monosemicarbazone 0.5mg
2. Menadione Sodium Bisulphite IP 10mg
3. Rutin N.F.XI – 50mg.
4. Ascorbic Acid IP 37.5mg
5. Cholecalciferol IP 200 IU
6. Calcium Phosphate IP 125mg.
INDICATION:
Epistaxis, Secondary Haemorrhage, Haemoptysis,
Menorrhagia, Metrorrhagia, Retinal haemorrhage. Prior to surgery to reduce bleeding
FUNCTION:
Promotes physiological haemostasis by causing constriction of cut capillary
ends.
DOSAGE: 1-2 tab TID
MECHANISM OF ACTION:
The drug acts as a haemostatic agent by reducing capillary fragility. It
controls oozing from raw surfaces and prevent bleeding from
microvasculature.
CONTRAINDICATION: Hypersensitivity.
PRECAUTION:
Use with caution in children, patients over 60, in pregnant women and in
lactation.
DRUG INTERACTIONS: Antihistamines reduce the efficacy of the drug.

82
QURSE KUSHTA FOULAD (71)
Ingredients:
Burada foulad (Iron filings) 100gms
Gandhak amla sar (Sulphur) 60gms
Tirphala (Emblica officinalis, Terminalia belerica ,Terminalia chebula) 50gms
Hathisundi buti ka pani (Heliotropium indicum) 1 Litre
Aab ghaikwar (Aloe barbedensis) 50ml
Uplav (Cow dung pieces) 25kgs
Preparation:
The Tirphala is ground, sieved and triturated in a mortar containing the Aab
ghaikwar. When the juice dries, 10gmslozenges are made, dried and subjected to the
gil hikmat process. When dry, they are heated in a pit containing 10 kg of dung. On
cooling, the cakes are removed from the urn, the Sulphur is added and the mixture is
triturated in a mortar containing 250ml of the Hathisundi buti ka pani. 10gms tablets
are made, placed in an earthenware vessel, and submitted to gil hikmat, after which
they are heated in 5kg. of the dung. On cooling the lozenges are triturated in the
Hathisundi buti ka pani and heating is repeated two more times. Thus there will be
five heating’s in all. After the fifth heating Kushta which is reddish black would be
ready; this is sieved and preserved in a bottle.
Dosage:
60mg or 2 tablets per day.
Indications:
Tonic against general debility and anaemia, liver stimulant, tonic during
convalescence and curative for impotency if due to anaemia.

83
7
2
6
11
7
910
8
0
2
4
6
8
10
12
No of
patients
11 to 20 21 to 30 31 to 40 41 to 50
Age in Years
Age Incidence in Test Group and
Control Group
Test Group Control Group
1
OBSERVATIONS AND RESUTLS
TABLE No 1: Age Incidence in Test Group & Control Group
Analysis of the results showed that age groups of patients in the study varied from
11 – 50 years. In Test Group maximum incidence is between 41 – 50 years age
group i.e., 35%. In Control Group maximum incidence is between 21 – 30 years
age group i.e., 36%. It shows that DUB can occur at any age group.
Age
Group
(Years)
Test Group
n=30
Control Group
n=30
Total
n=60
Total
Percentage
No of
patients
% of
patients
No of
patients
% of
patients
No of
patients
% of
patients
11-20 7 23.33% 2 6.66% 9 30.00%
21-30 6 20.00% 11 36.00% 17 56.66%
31-40 7 23.33% 9 30.00% 16 53.33%
41-50 10 33.33% 8 26.66% 18 60.00%
Total= 30 30 60
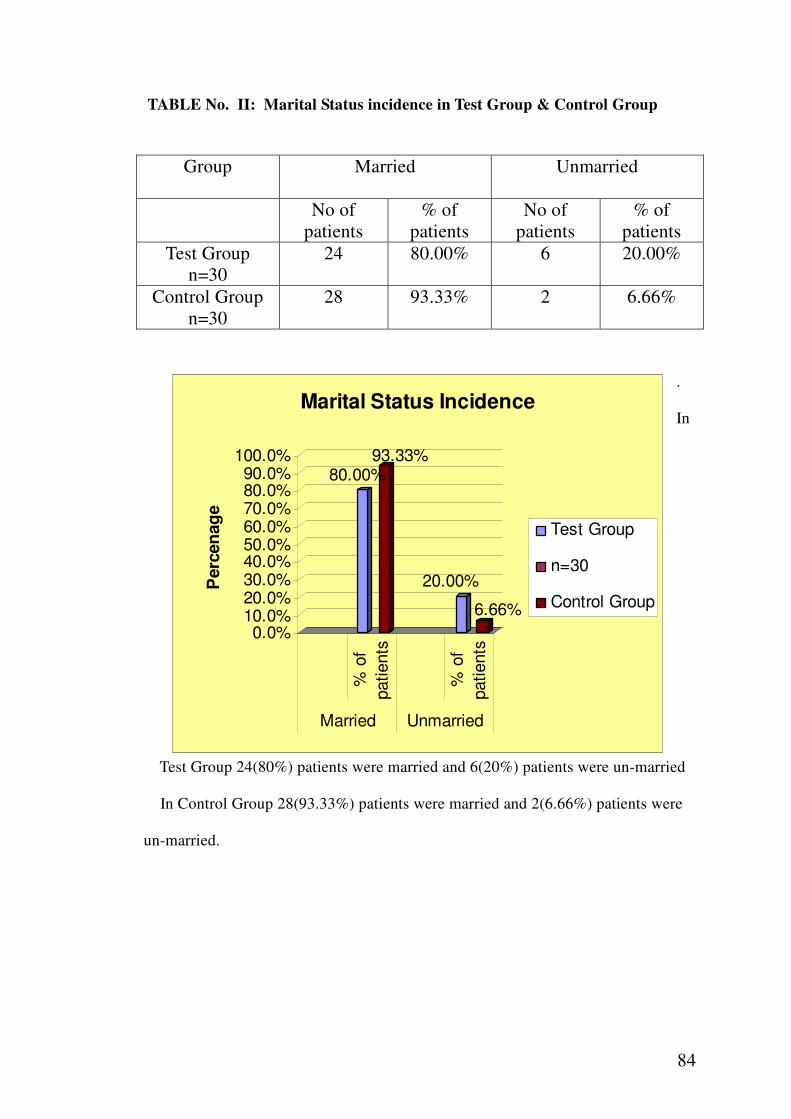
84
80.00%93.33%
20.00%
6.66%
0.0%10.0%20.0%30.0%40.0%50.0%60.0%70.0%80.0%90.0%
100.0%
Perc
en
ag
e
% o
f
patients
% o
f
patients
Married Unmarried
Marital Status Incidence
Test Group
n=30
Control Groupn=30
TABLE No. II: Marital Status incidence in Test Group & Control Group
.
In
Test Group 24(80%) patients were married and 6(20%) patients were un-married
In Control Group 28(93.33%) patients were married and 2(6.66%) patients were
un-married.
Group
Married
Unmarried
No of
patients
% of
patients
No of
patients
% of
patients
Test Group
n=30
24 80.00% 6 20.00%
Control Group
n=30
28 93.33% 2 6.66%

85
TABLE No. III: Pattern of Menstrual Cycle Incidence in Test Group and
Control Group
37% 36.66% 36%
16.66%
7%
33.34%
20%
13.34%
0%
5%
10%
15%
20%
25%
30%
35%
40%
PE
RC
EN
TA
GE
Menor Pmn Mnmt IC
TYPE OF MENSTRUAL CYCLE
PATTERN OF MENSTRUAL CYCLE
Test Group
Control
Group
In this study 36% of the women had Polymenorrhoea and 30% had Menorrhagia in
Test Group and in Control Group 37% of the women had Menorrhagia and 33% had
Polymenorrhoea, hence, the commonest pattern of AUB are Polymenorrhoea and
Menorrhagia followed by infrequent cycles.
Menstrual Cycle
(Type)
Test Group
n=30
Control Group
n=30
No of
patients
% of
patients
No of
patients
% of
patients
Menorrhagia 11 37.00% 11 36.66%
Infrequent Cycles 6 20.00% 5 16.66%
Polymenorrhoea 11 36.00% 10 33.33%
Menometorrhagia 2 7.00% 4 13.33%

86
TABLE No.1V: Temperamental Incidence in Test Group and Control Group
23.33%
56.67%
13.34%
6.66%
40.00%
60.00%
0.00% 0.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
PERCENTAGE
Test Group Control Group
TEMPERAMENT INCIDENCE
TEMPERAMENTAL INCIDENCE IN TEST GROUP
AND CONTROL GROUP
Damwi
Balghami
Safrawi
Saudawi
Analysis of the temperamental incidence showed that maximum percentage of
patients belongs to Balghami Mizaj in both Test Group (56.67%) & Control Group
(60%); Damwi Mizaj in Test Group (23.33%) & Control Group (40%); Safrawi
Mizaj in Test Group (13.34%) & Control Group (0%) and Saudawi Mizaj in Test
Group (6.66%) & Control Group (0%).
Temperament
(Type)
Test Group
n=30
Control Group
n=30
No of
patients
% of
patients
No of
patients
% of
patients
Damwi 7 23.33% 12 40.00%
Balghami 17 56.67% 18 60.00%
Safrawi 4 13.34% 0 0.00%
Saudawi 2 6.66% 0 0.00%
Total= 30 30

87
TABLE No: V - USG Findings Incidence in Test Group and Control Group
53.34%
70.00%
30.00%30.00%
6.66%
0.00%
10.00%
0.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
PE
RC
EN
TA
GE
Norm
al
Bulk
y U
teru
s
PC
OD
Sim
ple
Ovarian C
yst
USG FINDINGS
Test Group % ofpatients
Control Group % ofpatients
In the present study, in Test Group, 16 patients (53.34%) had normal pelvic scan; 9
patients (30%) had bulky uterus; 2 patients (6.66%) & 3 patients (10%).
In Control Group, 21 patients (70%) had normal pelvic scan and 9 patients (30%)
had bulky uterus.
USG
Findings
Test Group
n=30
Control Group
n=30
No of
patients
% of
patients
No of
patients
% of
patients
Normal 16 53.34% 21 70.00%
Bulky Uterus 9 30.00% 9 30.00%
PCOD 2 6.66% 0 0.00%
Simple Ovarian
Cyst
3 10.00% 0 0.00%
Total= 30 30
USG
Findings
Test Group
n=30
Control Group
n=30
No of
patients
% of
patients
No of
patients
% of
patients
Normal 16 53.34% 21 70.00%
Bulky Uterus 9 30.00% 9 30.00%
PCOD 2 6.66% 0 0.00%
Simple Ovarian
Cyst
3 10.00% 0 0.00%
Total= 30 30

88
Table No.V1: Endometrial Biopsy Findings Incidence in Test Group
Endometrium
(Type)
No. of cases
n=16
Percentage
Simple
Hyperplasia
5 31.25%
Secretory 4 25.0%
Proliferative 4 25.0%
Cystic Glandular 2 12.50%
Disordered 1 6.25%
31.25%
25.00% 25.00%
12.50%
6.25%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
PE
RC
EN
TA
GE
Simple
Hyperplasia
Secretory Proliferative Cystic
Glandular
Disordered
ENDOMETRIUM
ENDOMETRIAL BIOPSY FINDING
In the present study the commonest pattern of endometrium was simple hyperplasia
(31.25%), secretory endometrium (25%), proliferative endometrium (25%), cystic
glandular type (12.50%) and disordered endometrium in (6.25%) in test group

89
Table No.V11: Results: Duration of MBL Before and After Treatment
No. of Cases Before
Treatment
No. of Cases After
Treatment Duration
(Days) Test
Group
Control
Group
Duration
(Days) Test
Group
Control
Group
3-6 2 3 3-6 19 18
7-9 5 10 7-9 10 11
10-12 7 9 10-12 1 1
13-15 5 3 13-15 0 0
16 and
> 11 5
16 and
> 0 0
Total 30 30 30 30
In the study, before treatment, duration of menstrual flow (DOF) in Test Group
was; 11 patients had more than 16 days DOF, 5 patients had 13- 15 days of flow, 7
patients had 10-12 days, 5 patients had 7-9 days DOF & 2 patients had 3-6 days of
flow. In Control Group DOF before treatment was; 5 patients had more than 16
days, 3 patients had 13-15 days of flow, 9 patients had 10-12 days of flow, 10
patients had 7-9 days of flow, & 3 patients had 3-6 days of flow.
After treatment the duration of menstrual flow was regularized showing good
response; in Test Group 19 patients had 3-6 days of flow, 10 patients had 7-9 days
of flow and 1 patient had 10-12 days of flow. In control group DOF after treatment
was 18 patients had 3-6 days of flow, 11 patients had 7-9 days of flow & 1 patient
had 10-12 days of flow.

90
Table No.V111: Results: Amount of MBL (pads per day) Before and After
Treatment
There was a significant reduction of amount of flow after treatment in the present
study.
In test group according to number of pads used per day, 2 patients used > 8
pads per day, 25 patients had used 5-7 pads per day & 3 patients had used 2-4 pads
per day ( with DOF was > 20 days). After treatment, 28 patients had MBL as 2-4
pads per day & 2 patients had 5-7 pads per day.
In control group 15 patients had used> 8 pads per day amount of flow, 14
patients had used 5-7 pads per day & 1 patient had 2-4 pads per day ( with DOF was
> 20 days). After treatment 18 patients had 2-4 pads per day & 12 patients had 5-7
pads per day of MBL.
No. of Cases Before
Treatment
No. of Cases After
Treatment Amount
of flow
(pads/
day)
Test
Group
n=30
Control
Group
n=30
Amount
of flow
(pads/
day)
Test
Group
n=30
Control
Group
n=30
2-4 3 1 2-4 28 18
5-7 25 14 5-7 2 12
8 &
above 2 15
8 &
above 0 0

91
Table No.1X: Results: MBL Assessment Scores Before & After Treatment in
Test Group & Control Group
MBL Assessment Score Test Group
0100200300400500600700800
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
No. of Patients
Sc
ore
s
Series1
Series2
Before Treatment
After Treatment
In the present study there was significant reduction of menstrual blood loss after
treatment as per the assessment scores in pictorial chart of MBL.and it was evaluated
by statistical analysis using the paired t-test.
In test group, before treatment Mean was 506.433; SD 104.72; SEM 19.119 and after
treatment the values observed are: Mean 245.1; SD 53.637 SEM 9.79; P Value is <
0.0001, considered extremely significant.
In control group, before treatment values are; Mean 438.13; SD 92.77; SEM 16.938,
and after treatment Mean 231.3; SD 51.74; SEM 9.448; P Value is < 0.0001,
considered as extremely significant.
Hence it shows that test drug is clinically as significant as the standard drug.
MBL Assessment Score Control Group
0 100200
300400
500600700800
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 No. of Patients
Scores
Series1 Series2
Before Treatment
After Treatment

92
Table No. X: Results: Showing Overall Response
Group Cured Relieved Partially
Relieved
No
Response
Test Group
n=30
21 (70%) 7 (23.33%) 2 (6.70%) -
Control
Group
n=30
12 (40%) 11 (36.66%) 7 (23.33%) -
In the study, in Test Group out of 30 patients 21 patients (70%) were cured, 7
patients (23.33%) were relieved and 2 patients (6.70%) were relieved partially.
In Control Group 12 patients (40%) were cured, 11 patients (36.66%) were
relieved and 7 patients (23.33%) were partially relieved.
Statistical analysis of overall response between two groups was done by chi square
test and values observed are, 6.121 and the P value is 0.0469, showing that both
drugs are clinically significant.

93
DISCUSSION
Bleeding disorders are one of the commonest ailments among the gynaecological
problems. Apart from menorrhagia, other menstrual disorders are infrequent cycles,
polymenorrhoea, dysmenorrhoea, etc.
Excessive bleeding disorders may cause various other problems like anaemia,
palpitations, anxiety, mood depression, and cardiovascular problems.
DUB is defined as abnormal bleeding from the uterus in the absence of organic
disease of the genital tract. It is classified as:
Ovulatory including polymenorrhoea and menorrhagia and Anovulatory where the
bleeding is always painless and bleeding should be from the endometrium and not
from the cervix or lower genital tract.
It includes all the disturbances of menstrual cycle-regular or irregular with
alternations in amount and duration of flow.
The earliest reference to the problem of menstrual dysfunction is in Hindu literature
dating back to1400 BC. Menstruation is referred to as “unclean taboo” and impure in
the Greek and Arabic literature.
Unani physician viz Hippocrates, Dioscorides, Galen, Avicenna, etc. and later
physicians have also mentioned about the excess flow of menstrual blood and its
management.
The incidence of DUB is about 10%-15% of all gynaecological problems in the globe
and in India; it is 12.6% to 23.17%. It is equally common in the whole reproductive
life.
In the present study, vide table I and II, there is increasing incidence between 31-50
years i.e. 56.60%. It may be due to the fact that during this reproductive life, the

94
disease is preceded by abnormal handling and infection inoculation during abortions,
MTPs, Labour, and above all due to more stressful life.
The etiological factors as described by unani physicians were according to four
humours and derangement of temperament and also due to uterine debility and
weakness.
The present study which was conducted on 60 patients showed that the highest
incidence about 60% among the Balghami mizaj ladies vide table VII and VIII. It is
due to the fact that when excess of balgham or phlegm alter the temperament of the
uterus, weakens the uterine blood vessels, and tonicity of muscles resulting in loss of
blood due to poor constricting ability (Zofe Quwate Maseka) and also excess of
balgham may be a factor facilitating organisms to inhabit in the genital tract.
The plethora (imtila ba hasbul quwa) can be correlated with excess of oestrogens and
prostaglandins PGE2 and PGI2 in the blood thereby resulting in excessive menstrual
flow. The plethora due to imtila ba hasbul oyiya can be correlated with increase in the
size of the uterus. In the present study, USG findings showed that 30% of the patients
had bulky uterus. Hence, increase in the surface area of the endometrium results in
excess bleeding and delay in regeneration of the endometrium resulting in prolonged
duration of menstrual flow.
The etiopathology of DUB may be due to excessive proliferation in the endometrium
in result of multiple follicular ripening resulting in menstruation of every 2 or 3 weeks
or excessive pituitary-ovarian activity as occurs in following menarche or preceding
menopause.
Anovulatory cycles are usually encountered during postmenarche and premenopausal
period. The unopposed excessive oestrogen levels in these stages results in heavy

95
bleeding compared to ovulatory cycles. It is due to immaturity of the H-P-O axis in
puberty cases and regression of H-P-O axis in menopausal women.
DUB among 30-40 years of age is related to child bearing and stress factors. These
women also suffer from premenstrual syndrome. The stress-induced situations are due
to higher cortical effect on hypothalamic releasing factors or the effect of neuro-
hormonal substances from the CNS directly on the uterine musculature.
Menorrhagia can be the result of corpus luteum defect, irregular ripening of the
endometrium due to poor corpus luteum which is evident by low serum progesterone
level during the second phase of menstrual cycle.
Irregular shedding of the endometrium is due to incomplete or slow degeneration of
the corpus luteum (Halban’s disease). An anovulatory bleeding is due to absence of
active corpus luteum though oestrogen is produced but unopposed by progesterone. In
this type, the endometrium is hyperplastic, cystic type (Swiss chess occasionally
adenomatous). Bleeding is acyclical, continues for 2-8 weeks and is painless.
In the present study, serum estimation of thyroid profile was done in all 60 patients
and all are within the normal range.
Serum estimation of FSH, LH, and PRL was done and all were found to be within
normal range. This shows that there is no significant abnormal change in the levels of
the above hormones in patients with excessive bleeding in comparison to normally
menstruating women.
This study is correlated by the study done by John M. Eldred in 1994 which shows
“there does not appear to be a relation between ovarian and pituitary hormones and
menstrual loss.”
96
The study of endometrial histology is useful in the management of DUB, which is
done to differentiate between the benign and malignant condition and also functional
and organic disease.
In the present study, HPE of the endometrium is done on 16 patients of test group vide
table V1. In the study, the commonest type of endometrium among test group was
simple hyperplasia-23%, secretory phase-18%, proliferative phase-18%, cystic
glandular hyperplasia-5%, disordered endometrium-5% vide table V1.
In a study by Ganga S. Pillai and colleagues, “the spectrum of histopathological
changes in DUB” in 2002-commenest pattern of endometrium was endometrial
hyperplasia and associated incidental organic pathology was found in 15% cases.
A careful detailed history of medical and neuroendocrinal disorder along with
obstetric and gynaecological problems was questioned.
Detailed physical and pelvic examination was done along with routine hematological
exam and hormonal assay and endometrial biopsy.
Endometrial biopsy was performed on the married patients of the test group. It was
not applied to unmarried patients.
USG was done on all patients before the treatment to rule out any pelvic pathology. It
was found that 30% of the patients had bulky uterus and 8.3% had PCOD and rest of
the patients had normal uterus.
The evaluation of result was also done using the Menstrual Blood Loss Assessment
scoring system vide table V11.
Medical treatment is the best treatment for management of DUB to restore the normal
functioning of reproductive life. Most of the doctors prefer hormonal therapy.
NSAIDs are also recommended. These drugs reduce the production of endoperoxides

97
and block the myometrial PGE2 receptors. Along with NSAIDs, antifibrinolytics are
also recommended.
These standard medications have one or other drawbacks like GIT disturbances,
headaches, dizziness, abdominal cramps, and thromboembolic phenomenon is
common with antifibrinolytics. Hormones are not suitable for patients with cardio
vascular problems and it also impacts systemic effects on long use.
The other modern treatments are cryotherapy, direct circulation of heated saline,
phototherapy, microwave, radio infrequency, hyperthermia, and laser interstitial
therapy. These forms of therapy are costly and still in infantile stage.
D&C is a temporary therapeutic measure in severe menorrhagia.
Levanorgestrel releasing IUCD is however getting popularized but cannot be afforded
by all patients. Though there is no significant morbidity but unscheduled bleeding and
contraception among the young ladies, it is not accepted by many patients.
Among the surgical treatments, hysterectomy is the last option. It should be employed
when the patient does not respond to any type of treatment.
After careful study, it was decided to evaluate the efficacy of unani drugs in the
management of DUB which is most popular and ancient system of medicine and it is
also aimed to reduce the use of hormone therapy and to avoid hysterectomy.
The formula was selected from the used known drugs of ancient Hakims which have
least side effects. The ancient physicians have described apart from the herbal drugs
other operative procedures to divert the blood flow from the uterus. These are
‘venesection’ of basalic or cephalic vein, ‘cupping’ both dry and wet.
In the present study, 2 groups were planned. In the Group A, unani drugs were used as
test group and in Group B, the standard drug Styptovit was used.

98
The study was carried out on patients with identical features in respect of age, signs
and symptoms excluding systemic diseases, cardio vascular disorders, malignant
diseases, and organic lesions.
Endometrial biopsy was performed as a diagnostic procedure to rule out malignancy
in women of reproductive life particularly those who were at premenopausal age.
Endometrial biopsy was not applicable for unmarried patients (5).
Results: The result of the whole study was graded as
� Cured – Regularization of menstruation
Reduction in duration of flow
Reduction in amount of flow
Reduction in clots
Reduction in associated symptoms
� Relieved – Reduction in amount of flow along with normalization of any 2
characteristics of menstruation viz. duration, interval, clots and the associated
symptoms
� Partially Relieved- reduction of amount of flow only but persistence of
abnormalcy of interval, duration, clots, & associated symptoms.
� No Response- There is no response to treatment along with persistence of
most of the associated symptoms.
In the present study, in Test Group, 21 cases (70%) got cured, 7 cases (23.33%)
got relieved, and 2 cases (6.70%) were partially relieved.
In Control Group, 12 cases (40%) got cured, 11 cases (36.66%) got relieved, and
7 cases (23.33%) were partially relieved.
This overall response between two groups was analyzed statistically using chi-
square test: 6.121 and the P value are 0.0469.

99
There was a significant decrease in the bleeding volume as observed by the
Pictorial Menstrual Bleeding Assessment Chart before and after the completion of the
therapy for 3 months. There was a significant reduction in the menstrual bleeding and
it was evaluated by statistical analysis using the paired t-test.
The values observed are:
In Test Group, Before treatment, Mean -506.433, SEM-19.119, SD-104.72; After
treatment, Mean- 245.1, SEM-9.79, SD-53.637.and P value is <0.0001. It is
considered extremely significant.
In Control Group, Before Treatment, Mean -438.113, SEM-16.938, SD-92.775;
After treatment, Mean-231.3, SEM-9.448, SD-51.748.and P value is <0.0001. It
is considered extremely significant.
This shows that the Test Drug is as significant as the Standard Drug in controlling
the excessive loss of menstrual blood.
100
CONCLUSION
A woman presenting with abnormal uterine bleeding is a common problem seen
by many clinicians. Improved and sophisticated diagnostic tools allow us to
identify many causes of bleeding that were previously undetected.
After the detailed literary work it comes to conclusion that DUB is the
commonest cause of abnormal uterine bleeding but remains a diagnosis of
exclusion. In the present study the incidence is more common between 31-50
years.
DUB is a benign yet debilitating condition. Women of today are more employed
outside home or places where episodes of flooding are even less tolerable. The
victimized patients end up with debility, anaemia and psychological upsets.
Women thus require a safe and effective non surgical remedy for their menstrual
problems.
After the initial history taking and clinical examination, when the USG findings
are of normal uterine cavity the necessity for D and C and histopathology is
minimal.
The drugs included in test group were found to be cheaper, easily available,
effective and well tolerated by the patients without side effects.
As an affirmative to the mode of action as per the available research data, it may
be concluded:
Action on small blood vessels due to its haemostatic property, anti inflammatory
activity styptic action in Geru, Gulnar, Damul-Akhwain & Bartang
Geru, rich in oxides of iron, calcium restore the mineral loss caused by excessive
bleeding as observed by improvement in Hb% after the therapy and as a
haemostat controls the menstrual bleeding.

101
Gulnar is an astringent and may have the hormonal effect which needs to be
further evaluated.
Dammul Akhwain is a reputed resin for controlling bleeding for chronic
dysentery, diarrhea, piles and menorrhagia. Hence, found to be beneficial in
controlling the excessive MBL in DUB.
Barg Bartang controls internal bleeding and has antibacterial property.
There was a significant reduction in MBL (<50%) with P value < 0.0001 and
restoration of menstrual cycles to normal and there was no relapse or recurrence
of symptoms after the withdrawal of treatment. There was no significant change
in TLC, DC, RBS, RFT, LFT at the three month review after the completion of
the therapy showing that there were no adverse effects of the test drug on the
patients.
These drugs do not interfere with fertitility; can be combined with other therapies,
and have a fast onset of action, making them suitable in an acute bleeding.
This option may be particularly well suited for younger patients who wish to
preserve fertility and desire effective long term nonsurgical control of their
symptoms
From the above observation we can safely conclude that all the drugs taken in the
present study are pure, gentle, non-hormonal, safe and effective in the
management of DUB and hysterectomy should no longer be the only treatment
option presented to women with abnormal uterine bleeding.

102
SUMMARY
In the present study an attempt has been made to evaluate the efficacy of unani
drugs in the management of Usre Wazifi Nazfe Raham (DUB) and a detailed
comprehensive literary study carried out about DUB and unani and modern concepts
are thoroughly studied.
In this study, a total of clinically diagnosed 60 cases of DUB were registered from
the OPD/IPD of NIUM Hospital, Bangalore; 30 in test group and 30 in control
group.
The patients with abnormal uterine bleeding without any pelvic pathology, bleeding
disorder or any systemic disease, were included after getting their consent to
participate in the study.
The patients of all age groups during the reproductive life from menarche to
menopause were enrolled in the study.
A detailed medical, menstrual, and obstetrical history was taken. A detailed clinical
systemic examination was done to rule out any organic systemic disease. Pelvic
examination, both per speculum and bimanual was done to rule out any local
pathology viz malignancy, ulcer, etc, and was confirmed by pelvic ultrasonography
in all the enrolled 60 patients.
Routine hematological investigation including CBP, BT, CT, RBS, thyroid profile,
LFT, RFT was carried out. Patients with hepatic, renal or heart disease were
excluded from the study.
Hormone profile including FSH, LH, and PRL was performed. Endometrial biopsy
was performed to rule out any malignancy. The study showed that there are no
significant abnormal changes in hormone levels (FSH, LH, PRL) in DUB patients in

103
comparison to normally menstruating women. This was correlated with the study
done by John M. Eldred, “there does not appear to be a relation between ovarian and
pituitary hormones and menstrual loss.”
In the present study, the HPE done on patients of the test group showed that the
commonest type of endometrium was simple hyperplasia 34% followed by secretory
endometrium 20% and proliferative 17%. The endometrial biopsy was not done on
unmarried patients.
According to the pattern of cycle, 36% of patients had polymenorrhoea and 30% had
menorrhagia in the test group.
In the present study, the temperament of the patients was analyzed as per annexure #
1 and it was found that the highest incidence of DUB was found in patients with
Balghami mizaj (58.3%) followed by damwi mizaj (31.3%).
Assessment of Menstrual Blood Loss (MBL) was done by giving the patients
annexure # 2, the Pictorial Menstrual Bleeding Assessment Chart before and after
the completion of the therapy for 3 months. Evaluation of MBL was done by noting
the scores and statistical analysis done using students paired t’test.
Treatment: In the present study, the patients of the test group were given the unani
formulation and the patients of the control group, the standard drug Styptovit, was
given.
Test group contains Geru, Gulnar, and Dammul Akhwain in powdered form along
with Joshanda Barg Bartang. These drugs are given for 10 days in each menstrual
cycle or as per the assessment of the patient for 3 consecutive menstrual cycles. All
these drugs have haemostatic, styptic, astringent, anti-inflammatory, and analgesic
properties.

104
Geru has haemostatic and anti-inflammatory effect and contains excess of oxides of
iron, hence, beneficial in replenishing the lost iron in the menstrual blood loss.
Gulnar may have the hormonal effect as oestrone has been isolated from its seeds
and confirmed by thin layer chromatography. Hence, there is a need for further
evaluation of Gulnar for the presence of phytohormones. Gulnar has haemostatic
and astringent effect.
Dammul Akhwain is a strong astringent and is rich in calcium, phosphorus, etc.
which helps in coagulation of blood.
Barg Bartang has astringent, analgesic, and haemostatic effects. It has antibacterial
activity against E. coli and staphylococcus aureus. E. coli is the normal inhabitant of
female genital tract. Hence, Bartang has a beneficial effect.
The Control Group was given the standard drug, Styptovit, 1 tablet b.i.d. for 10 days
or as per the assessment of the patient in each menstrual cycle for 3 consecutive
cycles.
Comparative study was done and it was observed that there was a significant
decrease in bleeding volume (P<0.0001) and length of menstruation was reduced to
normal in the test group comparing to the standard drug. More than 90% of the
patients were relieved of excessive MBL during menstruation and those patients
who had irregular cycles before treatment showed good response and they had
regular cycles of 25 to 30 days after treatment.
Of the 30 cases registered in the test group, 21 cases (70%) got cured, 7 cases
(23.30%) got relieved, and 2 cases (6.70%) were partially relieved.
Hence, it is concluded that the Unani formulation is gentle, practical, safe, and
effective in the management of DUB; thus, the women can lead a normal healthy
life actively in occupations outside of the household without any inconvenience and
discomfort.

105
BIBLIOGRAPHIC REFERENCES
1. Michael .J. O’dowd, the History of Obstetrics and Gynaecology, pg – 292 –
302.
2. Padubidri .V. G; Hawkins and Bourne Shaw’s text book of Gynaecology 13th
edition, pg- 25-47,291-299.
3. Larry.J.Coopeland, M.D, text book of Gynaecology, 2nd
edition 2000; W.B.
Saunders company pg- 391-397
4. Rameet.H. Singh, M.D, M.P.H, Paul Blumenthal, M.D, M.P.H; ‘Harmonal
Management of Abnormal uterine Bleeding’, Clinical Obstretrics and
Gynaecology, Vol 48 No. 2 June 2005
5. Sulochana Gunasheela, practical Management of Gynaecological problems,
Jaypee Brothers, pg – 23 – 32
6. John Studd, progress in Obstetrics and Gynaecology, Vol 5, Churchill
Livingstone, pg – 293 – 305
7. Cardoso.P.M, D Silva.E.A, DUB A REVIEW, Obstretrics and Gynaecology,
Vol IX No. 1 Jan 2004.
8. Neville. F. Hacker, MD, George Moore. J, MD, Joseph Gambone. C, DO,
MPH, Essentials of Obstetrics and Gynaecology, 4th
edition, 2004, pg – 409
– 412
9. Dalal Nilesh, Obstetrics and Gynaecology, M.G. M. Medical college & M. Y.
Hospital, Indore, Vol 4, No. , July 1999
10. Khurshid Ahmed Shafaqat Aazmi, Amraazunnisa, pg – 488 – 503
11. Syed Mohammed Kamaluddin Hussain Hamdani, Usoole Tibb, edition –
1980, pg - 33 – 34.

106
12. Mazhar. H. Shah TPK, the general principle of Avicenna’s Cannon of
Medicine, pg – 156
13. Ismail Jarjani, Zakheera Khwarizm, Vol. 6, pg – 590 – 598.
14. Abubakar Mohammed Bin Zakriya Razi, Kitabul Hawi, Vol No. 9, central
council for research in Unani Medicine, New Delhi 2001, pg – 7 – 52
15. Ghulam Hussain- Ali bin Abbas Majoosi, Kamilus Sana, Munshi Naval
Kishor, pg – 534
16. Abu Al Mansoorul Hassan Al Qamri, Gana Mana, pg – 340 – 342,
Nizami Press, Victoria Street, Lucknow
17. Seth A. Stabinsky, Mark Einstein et al. “ Modern Treatments of Menorrhagia
Attributed to Dysfunctional Uterine Bleeding “ Vol 54 No. 1 Obstetrical &
Gynecological survey 1998.
18. Ajmal Khan HK, Al Haziq 1983, pg – 465 – 467
19. Kamal Buckshee, vasant.B. Patwardhan, Rustom.P. Soonawala, principles
and practice of obstetrics and Gynaecology; Jaypee brothers, pg-244-249.
20. Krishna Menon.M.K, Devi.P.K, Bhasker Rao.K, post graduate Obstretrics
and Gynaecology, 4th
edition, Orient Longman, pg – 315-323
21. Robert.W.Shaw, Patrick Soutter.W, Stuart.L.Stanto, Gynaecology, Churchill
livingstone, pg – 189-196.
22. John.M.Eldred, Eric.J.Thomas. Pituitary and Ovarian harmone levels in
unexplained menorrhagia, Obstretrics and Gynaecology, Vol 84, No. 5, Nov
1994
23. Tank D. K, Vinita Salvi, Mumbai, Management of DUB, Journal of
Obstetrics and Gynaecology, India
107
24. Dutta D C, Textbook of Gynaecology including contraception, 4th
edition,
New central Book Agency, pg – 5-12,59-86,175-186.
25. Tindall.V.R, Jeffcoate’s principles of Gynaecology, Butterworth Heinemann
edition, pg- 25 – 30, 53 – 79, 512 –531
26. Grey’s Anatomy, D. V. Devis, MA, BSc, MBBS, pg – 1334 –1335
27. Keith Edmunds.D., Dewhursts textbook of Obs & Gynae for postgraduates,
Chapter 40, pg – 590 – 608, 5th
edition; Chapter 34, pg – 410 – 414, 6th
edition
28. Jonathan. S. berck, Novak’s Gynaecology, 13th
edition, Lippincott Williams
and Wilkins, pg-365-370.
29. Abul Razack HK Talimul Qabla, Vol 6, pg – 186 – 193
30. Syed Ghulam Hussain – Urdu translation of Al - Qanoon Sheikh bu Ali
Sina Vol 3, pg – 331 – 337
31. Shamshul Afaque Siddiqui HK, Deputy advicer (Unani), dept of HFW, govt
of India, New Delhi, Shifaul Amraz (clinical medicine), pg – 277 – 279
32. Mohammed Kabiruddin HK, Bayaze Kabeer, pg – 191, Hikmat Book Depot,
Hyderabad
33. John. A. rock, Advances in Obstetrics and Gynaecology, Vol. 3, Mosby,
pg – 230 – 245
34. Erinn Wolff, MD and Antoni Duleba, MD, Seeking Medical Options For
Abnormal Uterine Bleeding, Comtemporary OB/GYN, Nov 2005
35. Kenneth. J. Ryan, Ross. S. Berkowitz, Robert. L. Barbieri, Kirtner’s
Gynaecology , Principles and Practice, 6th
edition, Mosby, pg – 41 – 44
36. Monika Malhotra, Dysfunctional Uterine Bleeding in Adolescants, Obs &
Gynae, Vol 5, No. 5, may 2000, pg – 294 – 297

108
37. Akas Jain, MD and Nanette Santaro, MD, Clinical Obstetrics and
Gynaecology, Vol 48, No. 2, June 2005, Lippincott Williams & Wilkins, pg –
295 – 311
38. Wallis. L. A, Daniel. W. Levine, MD, Paula. J. A. Hillard, MD, FACOG, Text
book of Women’s Health, Chapter 75, pg – 601 – 610
39. Alexander. F. Burnett, MD, Clinical Obstetrics and Gynaecology – A
Problem based approach, Blackwell Science, pg – 286 – 290
40. Leon Speroff, MD, Marc. A. Fritz, MD, Clinical Gynecologic Endocrinology
and infertility, 7th
edition, Indian Edition, Lippincott Williams & Wilkins, pg
– 547 – 567
41. Sharma J. B, Dysfunctional Uterine Bleeding, Obs & Gynae, Vol 5, No. 11,
Nov 2000, pg – 684 – 685
42. Preston. J. T, Cameron. I. T, Adams. E. J, Smith. S. K, Comparative study of
tranexamic acid and norethisterone in the treatment of ovulatory
menorrhagia, British Journal of and Gynaecology, May 1995, Vol 102, Pg-
401 – 406
43. John Bonnar, Brain. L. Sheppard, Treatment of Menorrhagia during
Menstruation: Randomized Controlled trial of Ethamsylate, Mefenamic
Acid, and Tranexamic acid, Br Med J 1996; 313: 579 – 582.
44. Aarti Malik, Levanorgestrel and ethinly oestradiol in menstrual irregularities:
An Overview, & Gynae today, Vol 10, No. 9, Sep 2005
45. Barrington. J. W, Bowen Simpkins. P, The Levanorgestrel intrauterine
system in the management of menorrhagia, British Journal of and
Gynaecology, May 1997, Vol 104, pg – 614 – 616

109
46. Gerald. J. Shirk, MD, ACOG, Minimally Invasive Surgery for Ablation of the
Endometrium, Clinical Obstetrics and Gynaecology, Vol 48, no. 2, June 2005
47. Zulkifle Mohd. “Physicochemical Basis of Temperament”, Thesis submitted
to the Department of Kullyat, AKTC, AMU, Aligarh, U.P.
48. Higham JM, O’Brien PMS, Shaw RW. Assessment of menstrual blood loss
using a pictorial chart, Br J Obstet Gynaecol. 1990:97:734-739
49. Janssen CA, Scholten PC, Heintz APM. A simple visual assessment
technique to discriminate between menorrhagia and normal menstrual blood
loss. Obstet Gynecol. 1995; 85:977-982
50. Kothari C R, Research Methodology, methods and techniques , Probability
sampling, pg-60.
51. Kirtikar Basu. The Wealth of India. CSIR, New Delhi, Pg: 112,146,147, 317-
324
52. Kirtkar K.R., Basu B.D.,Indian Medicinal Plants: Vol.8,9.
Pg :1508-1513,2802,2806-2808
53. Mohammed Abdul Hakeem,Bustanul Mufradat Jadeed,
Pg: 114,115,269,270,486,510
54. Nadkarni K.M., Nadkarni A.K, Indian Materia Medica.Bombay Popular
Prakashan. Vol. 1 Pg: 464,986,1031-1035.Vol.2 Pg: 7-11
55. Chopra R.N., Chopra I.C., Verma B.S., Supplement to Glossary of Indian
Medicinal Plants. Pg: 81, 84 .National Institute of Science Communication
CSIR
56. www.wikipedia.com,http:/www.erowid.org/chemicals/opiates
57. Kabiruddin Hk. Maqznul Mufradat,Kitabul Advia,Ajaaz Publication
Pg: 113,114,283,494,495,504,505

110
58. Ibne Betaar, Al Jaameul Mufradat wa Al Advia wa Al Aqzia
Pg: 199,200,300-304
59. Chopra R.N., Nayar S.L., Chopra I.C., Glossary of Indian Medicinal Plants,
Pg: 196, 207, 282,National Institute of Science Communication &
Information Resources, New Delhi
60. Krishnan Marg K.S., National Institute of Science Communication. New
Delhi, ‘The Useful Plants of India’. Pg: 183,466,505
61. Najmul Ghani Rampuri Hk, Khazae nul Advia,
Pg:326,327,692,693,1138,1169,1170.
62. Mohammed Kabiruddin. H.K, Al Akseer, Vol 2, pg – 1364 – 1372, edition
2003
63. J.P.Yadav, Suresh kumar, Priyanka Siwach.- “Folk Medicine used in
Gynaecological and other related problems in rural population of Haryana”
March 24,2005.
64. Pamar C.,Kushal M.K.,Punica granatum,in wild fruits, Kalyani Publishers,
New Delhi. Pg: 74-77.
65. Aleem Khan M., Naeem A. Khan, Iqbal A. Qasmi. et.al-“Antidiarrhoeal
activity of antidiarrhoeal unani formulations in rats”
66. Anthony M. Gawienowski, Carol C. Gibbs-“ Journal of phytochemistry-
Biosynthesis of pregnenolone from cholesterol in Punica granatum”. March
2,2001
67. Erich Heftmann, Shui-Tze Ko, Raymond D. Bennett-“Journal on
Identification of estrone in pomegranate seeds”. April 23, 2001.
68. http://www.dracaenacare.
69. Compendium of Indian Medicinal Plants: Vol.4 Pg: 575,576,611,612

111
70. http://en.wikipedia.org/wiki/Image:Dracaena_reflexa.JPG
71. Md. Said H K, Hamdard Pharmacopoeia of Eastern Medicine, 2nd
Edition
1997. Pg-230-231.

1
NATIONAL INSTITUTE OF UNANI MEDICINE, BANGALORE
DEPARTMENT OF AMRAZ-E-NISWAN-WA-QABALAT
TOPIC: USRE WAZIFI NAZFE RAHAM (DUB)
GUIDE:-DR.WASIA NAVEED, B.U.M.S. MD (Niswan-o-Qabalat) GNTC, Hyderabad.
P.G SCHOLAR:-DR.SALMA BANO, B.U.M.S.
CASE -PROFORMA
Sl.No.of Case:
OPD/IPD No.\ Date
Patient’s Name:
D\O , W\O
Age:
Address with Contact No.
Qualification Uneducated \ Preschool\ High School\University
Marital Status Married \ Unmarried \ Widow \ Divorcee
Social Status Low class \ Middle class \ high class
Religion:
Date of Admission
Date of Discharge
Provisional Diagnosis:
Final Diagnosis:
Result:

2
1. Chief Complaints With Duration
1. Bleeding per vaginum
� Amount of flow
� Duration of flow
� Presence of clots
2. Pain abdomen
2. History of Present Illness with Duration:
3. Past History
History of any major illness:
(HTN, DM, TB, HIV, Bleeding Disorder, etc.)
Any Drugs taken-cortisones, sex steroids, anticoagulants, NSAID
History of any operation:
4. Family History
History of any major illness:
(HTN\ DM\ TB)
History of any endocrine abnormalities:
Malignancy
� Breast
� GIT
� Genital Organs
5 a) .Present Menstrual History
1. Duration of flow
2. Amount & frequency of cycles
3. LMP
4. Painful or Painless bleeding
5. Other associated complaints like:

3
•••• Generalized weakness
•••• White discharge
•••• Backache, etc.,
History of Previous Treatment for Menstrual Disorder and Its Effect
5 b) Past Menstrual History
Age of Menarche
Menstrual Period (Duration)
Menstrual Flow & Amount
Cycles-regular\irregular
History of Dysmenorrhoea
History of Intermittent Bleeding
or Pain
6a). Obstetrics History
� P L A D
� M. L:-
� L.C.B:-

4
Sl.no.
Year &
Date
Duration
Of
Pregnancy
Mode of
Delivery
Puerperium
Events
During
Pregnancy\
Labour
1
2
3
4
HISTORY OF ABORTIONS: - Present\ absent
[A] Induced:-
[B] Spontaneous:-
6b). HISTORY OF CONTRACEPTION
&
STERLIZATION
7). History of any Psychosomatic Disorders
8). Personal History
Diet: Micturition
Appetite: Bowel
Sleep Mood
Environment/Surroundings Habits
9). General Physical Examination
Build:
Nourishment\ Weight
Pallor\Ictrus
Oedema\Puffiness
Lymphadenopathy\Thyroid

5
Vitals
Pulse Rate: Temperature:
Blood Pressure Respiratory Rate
Breast Examination:
Examination of Secondary Sexual Characters:
Signs of any other Endocrine Disorders:
Signs of any Vitamin deficiency:
Systemic Examination
Cardiovascular System:
Respiratory System:
Gastro-intestinal System:
Local Examination:
Inspection of Vulva
Per Speculum Examination of:
o Vagina:
o Cervix:
Bi-Manual Examination:
Uterus
� Shape and size
� Position
� Mobility
� Surface (Regular or Irregular)
� Tenderness
� Consistency

6
Cervix
� Shape and size
� Mobility
� Surface (Regular or Irregular)
� Tenderness
� Consistency
� Any contact bleeding
Fornicess
� Tenderness
� Mobility
� Adenaxal Mass
� Palpable Ovaries
Per-Rectum Examination:
Investigations:
� Haemoglobin %:
� Total Leucocyte count:
� Differential Leucocyte count:
� Platelet count
� Bleeding Time:
� Clotting Time:
� Blood V.D.R.L.
� Blood Sugar
� Blood Urea
� S. Creatinine
� SGOT
SGPT
� Thyroid Profile
• T3

7
• T4
• TSH
� Hormone Profile
• FSH
• LH
• Prolactin
� Ultrasonography
� Biopsy of Endometrium (D&C) , Histopathology of Endometrium
Final Diagnosis:--
Treatment Given: Group A Medicine \ Group B Medicine
Dose:
Duration:
Result: Cured \ Relieved \ Partially Relieved \ No Response
Treatment Given For Three Cycles
Sl.No.of
cycle
Date of
reporting
LMP Duration
Of flow
Amount
Of flow
Investigations
If done
1st. Cycle
2nd.Cycle
3rd.Cycle
Follow-up Sheet without Treatment
Sl.No.of
cycle
Date of
reporting
LMP Duration
Of flow
Amount
Of flow
Investigations
If done
1st. Cycle
2nd.Cycle
3rd.Cycle
Conclusion:
Signature of PG Scholar

8
Assessment Criteria
The parameter of assessment criteria are graded as follows:
Menstrual Bleeding:
1) Duration of menstrual flow –
• 1 to 5 days
• 6 to 9 days
• 10 to 14 days
• 15 to 19 days
• 20 days & above
2) Interval between two menstrual cycles:
• Normal – 28 to 32 days
• Frequent – Menstrual bleeding occur at 21 days or less.
• Inter-menstrual bleeding – menstrual bleeding occur at 15 to 16 days
cycle or in between two menstrual cycle .
• Delayed – menstrual bleeding occurring > 35 days.
3) Amount of menstrual blood loss: 1 – 3 pads per day – 1
4 – 6 pads per day – 2
7 – 9 pads per day – 3
10 – 12 pads per day -- 4
> 12 pads per day – 5
4) Consistency of bleeding: Watery - 1
Watery+ Clots - 2
Clots (mild) - 3
Clots (moderate) 4
Clots (severe) - 5
5) Staining: Positive - 1
Negative - 0
6) Odour:
Positive - 1
Negative - 0

9
Intensity Of Pain During Mensus:
• Absent = 0
• Mild – Patient able to tolerate, subsides with rest.= 1
• Moderate – pain subsides with analgesics.= 2
• Severe – pain not subsides with use of analgesics.= 3
Remarks of Co-Guide:
Signature of Co-Guide
Remarks of Guide
Signature of Guide

NATIONAL INSTITUTE OF UNANI MEDICINE
BANGALORE
PATIENT CONSENT FORM
TOPIC: CLINICAL STUDY OF USRE WAZIFI NAZFE RAHEM
(DYSFUNCTIONAL UTERINE BLEEDING) AND ITS MANAGEMENT WITH
UNANI DRUGS
Patient OPD \ IPD.NO. ……………………………………………..…...
Name of the patient ………………………………………………….
Address …………………………………………… ……..
…………………………………………… ..……
……………………………………………………
I have been told and I understand that my participation in this clinical
research study is voluntary. I may decide not to participate or withdraw my
consent and discontinue my participation at any time. I understand that the
investigator incharge of this study may stop the study or stop my participation
in the study at any time for any reason without my consent.
By signing this form, I authorize the institution to access and obtain
information that is required for the study. This may include my medical
records and laboratory investigation reports. Before giving consent by signing
this document, the nature and purpose, procedure risks and benefits of this
research study have been explained to me. I have been given the opportunity to
review this document and ask questions, which have been answered to my
satisfaction. I am consenting to participate in research study.
Patient’s signature / Thumb impression Signature of the investigator
Name of patient…………………………
Date………………………………………
Place…………………………………….

Pictorial Assessment Chart- Scoring System
Name of the Patient:
Day Start:
Before Treatment Score:
Score PADS 1 2 3 4 5 6 7 8 9 10
1
5
20
1
5
CLOTS:
Small
Large
After Treatment Score:
Score PADS 1 2 3 4 5 6 7 8 9 10
1
5
20
1
5
CLOTS:
Small
Large


AOMYrs
P L A D HOS BT ATSl No. Reg No. Name of the Patient Age Date Marital Status BT AT BT AT BT AT BT AT BT AT BT AT BT AT Sur IUCD Hor Nil Vg Cx Vg Cx Uterus Uterus BT
1 21793 Nasreen Begum 39 1/3/2007 Married 7 3 6 5 A A P A A A P A IC Normal 14 6 4 2 0 P P A A A Healthy Healthy Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 102 31626 Shakeela Begum 42 3/3/2007 Married 9 5 7 6 P A A A A A P A Menor Normal 14 6 6 0 0 A A A P A Healthy Ero+Htd Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 103 31853 Noor Jaan 40 6/12/2006 Married 9 4 60 7 A A P A A A P A Menor Normal 11 8 6 0 2 A A A P A Healthy Healthy Healthy Healthy ut, RV.Bulky.M. FF ut, RV.Bulky.M. FF 74 32268 Zarin taj 44 1/12/2006 Married 4 3 15 6 A A A A A A P A Menor Normal 12 4 3 1 A A A A P A Pallor Pallor Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 115 32747 Padma M 33 19/12/06 Married 6 3 20 5 A A P A A A A A IC Normal 12 2 2 0 0 A P A A A Healthy Healthy Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 136 33205 Nuzhat 15 25/1/2007 Unmarried 7 4 10 4 P A P A A A A A Menor Normal 11 NA N A NA NA NA NA NA NA NA NA NA NA NA NA NA 127 35410 Noorie 20 7/2/2007 Married 5 3 20 7 A A A A P A P A Polym Normal 14 0 0 0 0 A A A A A Healthy Ero,Htd Healthy Healthy Ut -AV, NS, M FF Ut -AV, NS, M FF 128 36489 Sadia 18 26/02/07 Married 7 5 10 7 P A P A A A A A Polym Normal 14 0 0 0 0 A A A A A Healthy Healthy Healthy Healthy Ut -AV, NS, M FF Ut -AV, NS, M FF 109 36573 Ishrath 14 26/02/07 Unmarried 6 4 10 5 P A P A P A P A Polym Normal 12 NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA 12
10 37635 Haleema 17 12/3/2007 Unmarried 7 3 15 5 P A P A A A P A Menor Normal 11 NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA 911 37803 Laxmama 46 14/03/07 Married 6 2 20 8 A A P A P A P A Menomtrgia irregular 15 2 2 0 0 A P A A A Healthy Ero+ Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 1112 38215 shahnaaz 27 19/05/07 Married 7 3 9 7 A A P A P P P P Polym Normal 11 3 3 0 0 A A A A A Healthy Healthy Healthy Healthy Ut -AV, NS, M FF Ut -AV, NS, M FF 913 38943 Ishrath Taj 30 2/4/2007 Married 6 3 9 4 P A P A A A A A Polym Normal 13 3 3 0 0 A P A A A Pallor Pallor Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 714 39406 Razeena Khatoon 50 9/4/2007 Married 7 3 15 6 A A P A A A P A Menor Normal 13 7 7 0 0 A P A A A Pallor Pallor Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 8.515 40511 Hafeeza 40 6/6/2007 Married 5 3 15 7 A A P A P A P A Polym Normal 11 2 2 0 0 A P A A A Pallor Ero,Htd Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 8.516 41560 Farooq Unnisa 36 25/06/07 Married 4 3 18 6 A A P A A A A A Polym Normal 12 3 3 1 0 P P A A A Normal Ero + Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 8.517 41830 Farhat Javeria 32 17/05/07 Married 6 3 12 5 A A P A A A P A Menor Normal 12 4 2 0 2 A P A A A Pallor Ero + Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 1018 42176 Reshma Bano 25 22/05/07 Married 5 3 22 11 A A P A A A P A IC Normal 13 1 1 0 0 A A P A A Healthy Healthy Healthy Healthy Ut -AV, NS, M FF Ut -AV, NS, M FF 1019 42239 Asgari Begum 35 23/05/07 Married 7 2 20 6 A A P A A A P A IC Normal 14 6 4 2 0 A A A A A cy+rec+ Ero+ cy+rec+ Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 1020 42867 Arshiya 22 1/6/2007 Unmarried 4 2 20 7 A A P A P A P A IC Normal 17 NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA 7.521 42916 Hina 13 2/6/2007 Unmarried 5 3 10 5 P A P A P A P A Menor Normal 12 NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA 1222 42927 Nigar 28 12/6/2007 Married 7 3 12 5 A A P A P A A A Menor Normal 13 5 3 2 0 A P A A A Healthy Healthy Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 1023 43451 Gayatri 47 5/7/2007 Married 6 2 20 7 A A P A A A P A Menomtrgia Normal 14 3 3 0 0 A A A A A Healthy Htd Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 824 44267 Asmat Unnisa 42 21/06/07 Married 7 3 7 5 A A P A A A P A Polym Normal 13 5 5 2 A P A A A A Pallor Htd Healthy Healthy UT-AV-Bul.M-RF tender LUt-AV,Bul,M,FF 9.525 44561 Reshma Sultana 25 4/7/2007 Married 7 3 20 7 A A P P A A P A IC Normal 11 0 0 0 0 A A A A A Pallor Pallor Healthy Healthy Ut -AV, NS, M FF Ut -AV, NS, M FF 826 44836 Gulzar 42 2/6/2007 Married 6 3 10 5 A A P A A A P A Menor Normal 13 4 4 0 0 P P A A A Pallor Neboth + Healthy Healthy Ut -AV, NS, M FF Ut -AV, NS, M FF 7.527 45063 Waheed Unnisa 43 5/7/2007 Married 6 3 12 5 P A P A P A P A Polym Normal 11 8 6 2 1 P A A A A Pallor Pallor Healthy Healthy Ut-AV,Bul,M,FF Ut-AV,Bul,M,FF 1228 45155 Arshiya 15 5/7/2007 Unmarried 6 3 8 5 P A P A P A A A Polym Normal 14 NA NA NA NA NA NA NA NA NA NA NA NA NA NA NA 9.529 45724 Roohi Zaman 32 12/7/2007 Married 6 4 11 6 A A A A P A P A Menor Normal 15 3 3 A A P P A A A Healthy Ero + Healthy Healthy Ut -AV, NS, M FF Ut -AV, NS, M FF 1230 47263 Afroz Bano 36 2/8/2007 Married 7 4 20 8 A A P A A A P A Polym Normal 12 2 2 0 0 A P A A A Healthy Healthy Healthy Healthy Ut -AV, NS, M FF Ut -AV, NS, M FF 9.9
Chief Complaints Associated Complaints POC Obstetrical History Gynaecological ExaminationBPV P/S P/V
AOF(P/day) Dof (days) Dys GW WD BA Contraception BT AT Hb gm

ESRPelvic USG Endo-Biop NR PR R C
AT BT AT BT AT BT AT BT AT BT AT BT AT BT AT LH-mIU/mL FSH-mIU/mL PRL-ng/mL DM BL SF SU BT AT AOF DOF AOF DOF AOF DOF
10.5 5000 6800 56 56 42 40 2 2 0 0 0 0 15 10 Bul.Ut.M.E.O N D 10.06 4.04 6.76 P A A A 409 185 6 5 4 4 3 4 0 0 0 111 5800 5000 48 48 34 48 4 2 6 2 0 0 10 20 bul.ut M. Hyp. Plastic 4.36 9.57 5.7 A P A A 593 274 5 9 4 7 3 5 0 0 0 111 5000 5000 40 60 54 40 6 0 0 0 0 0 20 15 bul.ut S.Hyp. Plastic ND ND ND A P A A 506 300 7 12 6 10 4 7 0 0 0 1
11.5 9650 4800 66 50 32 38 2 6 0 6 0 0 10 10 bul.ut Secr. Phase 1.81 7.64 10.45 A P A A 336 163 4 12 3 10 3 6 0 0 0 113 6800 6800 58 60 42 40 2 0 0 0 0 0 30 10 Normal Secr. Phase 6.85 5.42 6.78 P A A A 629 296 6 10 4 8 3 5 0 0 0 1
12.5 5500 4300 58 60 32 34 6 6 2 0 0 0 10 10 Normal NA 3.16 2.29 8.28 P A A A 423 167 6 6 4 5 4 5 0 0 0 114 8600 5000 60 56 26 36 14 4 0 4 0 0 10 20 Normal Prolif. Phase 33.07 5.39 5.53 A P A A 728 340 5 9 4 7 3 5 0 0 0 112 4010 6000 46 58 48 36 6 4 0 2 0 0 10 15 PCOD ND ND ND ND A P A A 546 275 6 10 5 8 3 7 0 0 1 0
14.5 5300 4800 54 60 44 40 2 0 0 0 0 0 20 25 Normal NA 5.23 3.04 11.1 P A A A 435 207 6 9 5 7 4 5 0 0 0 110 5600 4900 52 56 42 38 4 6 2 0 0 0 20 5 PCOD NA 9.93 5.17 7.15 P A A A 448 212 7 10 6 7 3 5 0 0 0 1
12.5 7400 6000 64 60 32 40 4 0 0 0 0 0 45 15 Bulky Uterus ND ND ND ND A P A A 554 344 6 15 5 12 2 8 0 1 0 013 5600 4900 56 48 40 48 4 2 0 2 0 0 20 10 Normal Prolif. Phase 5.8 4.69 4.27 A P A A 465 226 6 9 5 8 4 7 0 0 1 011 4600 6800 62 58 30 40 8 2 0 0 0 0 15 20 Bulky Uterus ND 5.33 8.8 3.2 A P A A 648 303 5 8 4 6 3 4 0 0 1 0
10.5 4020 4800 44 56 56 38 0 4 0 2 0 0 20 10 Bulky Uterus Prolif. Phase 6.79 16.36 7.59 A P A A 512 248 7 12 5 9 3 6 0 0 0 111.5 4800 5700 54 50 46 46 0 4 0 0 0 0 38 25 Normal Secr. Phase 1.86 2.8 4.55 A P A A 527 216 5 15 4 12 3 7 0 0 1 011 5150 6000 74 76 24 24 2 0 0 0 0 0 30 25 Bulky Uterus Cystic glandular hyperplasia 3.06 8.62 5.04 P A A A 436 216 4 10 3 6 2 6 0 0 0 111 5200 5800 58 62 34 36 6 2 2 0 0 0 30 20 Bulky Uterus Secr. Phase 5.95 10.3 7.51 A P A A 396 183 6 7 5 6 3 5 0 0 0 112 6500 4600 51 48 44 48 2 2 2 2 1 0 20 10 Normal ND ND ND ND A P A A 261 138 5 10 4 10 3 5 0 0 1 0
10.5 4900 5200 70 60 30 40 0 0 0 0 0 0 10 15 NS, L. O.simp,cyst Simple hyperplasia 9.14 23.64 4.86 A P A A 567 287 6 10 5 7 2 6 0 0 0 110.5 5060 4500 56 56 42 38 2 4 0 2 0 0 25 20 Normal NA ND ND ND A P A A 376 183 4 12 3 10 2 7 0 0 0 111 4800 4800 42 56 58 44 0 0 0 0 0 0 5 10 Normal NA 4.01 6.34 5.77 A P A A 574 267 5 8 4 6 3 5 0 0 0 111 5900 5800 72 60 24 40 4 0 0 0 0 0 10 15 Bulky Uterus Disordered Prolif. Phase 0.88 4.37 7.82 P A A A 520 245 5 10 4 8 3 5 0 0 0 1
10.5 5400 6000 56 60 42 40 2 0 0 0 0 0 20 15 bul.ut. Cx Htd.LOC ND ND ND ND A P A A 604 285 6 15 3 9 2 7 0 1 0 011 5800 5300 52 60 48 38 0 2 0 0 0 0 20 15 N S Cx HTD Simple hyperplasia 5.8 9.83 5.37 A P A A 504 267 7 7 5 5 4 5 0 0 0 110 5300 5500 48 60 42 36 6 4 0 0 0 0 40 15 Normal ND 14.52 6.32 8.39 A P A A 543 258 6 13 5 11 3 7 0 0 1 010 5300 5200 50 48 46 46 2 3 2 1 1 1 30 20 Normal ND ND ND ND A P A A 682 309 6 10 5 8 4 7 0 0 0 1
12.5 4400 6000 70 58 30 38 0 4 0 0 0 0 10 15 Normal Mid secretary phase 4.73 10.21 8.39 A P A A 580 284 6 10 5 8 5 5 0 0 0 110 6500 6000 44 50 52 46 4 4 0 0 0 0 10 20 Normal NA 1.54 4.03 7.6 A P A A 546 262 6 8 4 7 3 5 0 0 0 1
12.5 5800 5900 66 60 30 38 4 2 0 0 0 0 25 20 Normal Cystic glandular hyperplasia 8.45 4.94 2.77 A P A A 442 192 4 9 4 7 3 5 0 0 1 011 7200 5800 65 66 28 34 3 0 4 0 0 0 15 20 Normal Simple hyperplasia ND ND ND A P A A 403 222 6 15 5 12 4 8 0 0 0 1
Investigations Temperament Assesment chart Treatment Chart ResultsTLC DLC
ms % (cells/cumm) P L E M B 2nd cycle 3rd cyclemm/hr Hormone Profile Total Score Ist cycle

Sl No. Reg No. Name of the Patient Age Date Marital Status BT AT
1 28277 Shabana 27 6/1/2007 Married 4 32 33326 Amuda 33 3/1/2007 Married 8 53 35414 Laxmamma 48 7/2/2007 Married 8 44 35557 Rasheeda Parveen 35 9/2/2007 Married 8 55 35651 Akkayamma 37 13/02/07 Married 8 56 35943 Shamshad 30 17/02/07 Married 8 57 35956 Tasleem Firdose 37 17/92/07 Married 12 68 35817 Taranum Sultana 18 22/2/07 Un married 6 49 36497 Nasreen Taj 42 26/02/07 Married 7 510 37676 Rehana 46 13/03/07 Married 7 411 37711 Najmunnisa 42 14/3/07 Married 7 412 37716 Sayeeda Bano 42 13/03/07 Married 9 613 37812 Saira Bano 37 14/3/2007 Married 7 314 38501 Rihana Bee 33 1/4/2007 Married 8 415 38829 Naushad 32 2/4/2007 Married 8 516 41233 Qamrunissa 35 6/7/2007 Married 9 417 41541 Qamrunissa 50 14/05/07 Married 8 518 41903 Shahnaaz 28 14/6/07 Married 6 419 41950 Reshma 26 16/06/07 Married 7 420 41989 Thangamani 43 7/7/2007 Married 9 621 42421 Kantamma 46 16/07/07 Married 7 522 42887 Zeenath Kouser 30 17/07/07 Married 8 523 44179 Pavitra 15 2/7/2007 Un married 6 424 44335 Jabeen Taj 30 10/7/2007 Married 6 425 44634 Zeenat kouser 21 27/06/07 Married 8 426 45156 Laxmamma 30 7/7/2007 Married 7 427 45408 Hafeeza 28 9/7/2007 Married 8 428 45918 Naseeba 40 16/7/07 Married 5 329 46067 Shameem Taj 30 17/07/07 Married 5 430 46982 Mubeen Taj 30 31/7/07 Married 6 4
BPAOF(P/day)

BT AT BT AT BT AT BT AT BT
15 7 A A P A A A P10 7 P A P A A A P7 5 P A P A A A P7 6 A A P A P A P10 6 A A P P A A P6 6 A A P A A A P10 7 A A P A A A P9 5 P A P A A A P8 6 A A P A A A A20 8 A A P A A A P10 5 A A P A A A P6 5 A A P A A A A20 5 A A P A A A A9 5 A A P A P A P7 5 A A P A A A P5 4 A A P A A A P20 8 A A P A A A P15 7 P A P A P P P9 5 A A P A A A A10 5 P A P A A A P10 7 A A P A P A P20 6 P A A A A A A10 7 P A P A A A P10 6 A A P A A A A9 7 A A P A A A P10 7 A A P A A A P7 5 A A P A P A P7 5 P A P A A A A20 10 A A P A P A P15 8 P A P A P P P
PVChief complaints Associated complaints
BAGW WDDysDof (days)

AOMYrs
P L A D HOSAT BT AT
A Menor Normal 12 2 2 0 0 AA Menor Normal 13 3 3 0 0 AA IC IC 13 4 3 0 1 PA Menor Normal 12 2 2 0 0 AP IC IC 13 2 2 0 0 AA Menor Normal 13 2 2 0 0 AA Menor Normal 12 3 3 2 0 PA Polym Normal 15 NA NA NA NA NAA Menor Normal 12 5 5 2 0 PA IC IC 11 3 3 0 0 AA IC IC 13 6 6 0 0 AA Menomtrgia Normal 12 7 5 2 0 AA Polym Normal 13 5 5 0 0 AA Menor Normal 11 6 6 0 0 AA Polym Normal 13 4 4 0 0 AA Menor Normal 11 3 3 1 0 PA IC IC 14 6 6 2 0 AP Polym Normal 13 2 2 1 0 AA Polym Normal 13 2 2 0 0 AA Polym Normal 10 3 3 2 0 AA Polym Normal 13 4 4 1 0 AA Menomtrgia Normal 13 0 0 0 0 0A Menor Normal 12 NA NA NA NA NAA Polyrn Normal 12 3 3 0 0 AA Menor Normal 15 1 1 0 0 AA Menor Normal 12 2 2 0 0 AA Polyrn Normal 11 3 3 0 1 AA Polym Normal 11 4 4 0 0 AA Menomtrgia Normal 12 2 2 0 0 AA Menomtrgia Normal 12 0 0 4 0 A
Obstetrical His
A
POC

Sur IUCD Hor Nil Vg Cx Vg Cx
A P A A Healthy Healthy Healthy HealthyP A P A Healthy Healthy Healthy HealthyA A P A Pallor Pallor Healthy HealthyP A A A Healthy HTD Healthy HealthyP A A A Healthy Healthy Healthy HealthyA A P A Healthy Htd,Ero Healthy HealthyA A A A Healthy Healthy Healthy Healthy
NA NA NA NA NA NA NA NAP A A A Healthy Healthy Healthy HealthyA A P A Healthy Healthy Healthy HealthyA P A A Healthy Healthy Healthy HealthyA A A A Healthy Healthy Healthy HealthyA A P A Healthy Healthy Healthy HealthyA A A A Healthy Htd,Ero Healthy HealthyP A A A Healthy Htd,Ero Healthy HealthyP A A A Healthy Healthy Healthy HealthyA P A A Healthy Htd,Ero Healthy HealthyA A P A Healthy Ero Healthy HealthyA P P A Healthy Healthy Healthy HealthyP A A A Healthy Healthy Healthy HealthyA A A A Healthy Htd,Ero Healthy HealthyA A A A Healthy Healthy Healthy Healthy
NA NA NA NA NA NA NA NAP A A A Healthy Healthy Healthy HealthyA A A A Healthy Healthy Healthy HealthyP A A A Healthy Healthy Healthy HealthyP A A A Healthy Healthy Healthy HealthyP A P A Healthy Healthy Healthy HealthyP A A A Healthy Htd,Ero Healthy HealthyA A A P Healthy Htd,Ero Healthy Htd,Ero
story GynaecologicP/S
Contraception BT AT

BT ATUterus Uterus BT AT BT AT BT
Ut -AV, NS, M FF Ut -AV, NS, M FF 12 14.5 5200 4800 52Ut -AV, NS, M FF Ut -AV, NS, M FF 11.5 12 5650 5600 50Ut -RV, NS, M FF Ut -RV, NS, M FF 11 12.5 6780 6000 38Ut.AV. Bulky. M . FF Ut.AV. Bulky. M . FF 12.5 12.5 4800 5000 52Ut.AV. Bulky. M . FF Ut.AV. Bulky. M . FF 10 13 5060 8000 50Ut.AV. Bulky. M . FF Ut.AV. Bulky. M . FF 11.5 12.5 4100 5000 42Ut.AV. Bulky. M . FF Ut.AV. Bulky. M . FF 13 13 5000 4800 60NA NA 13 14.5 6900 5600 46Ut -AV, NS, M FF Ut -AV, NS, M FF 10 12.5 6000 5800 60UT -RV, Bulky, M FF UT -RV, Bulky, M FF 9 10.5 6600 6000 60Ut -AV, NS, M FF Ut -AV, NS, M FF 9 12.5 7800 6300 58Ut -AV, NS, M FF Ut -AV, NS, M FF 10.5 11.5 5850 5050 34Ut.AV. Bulky. M . FF Ut.AV. Bulky. M . FF 9 12.5 5620 5000 56UT -RV, Bulky, M FF UT -RV, Bulky, M FF 9 10.5 6000 6000 60Ut -AV, NS, M FF Ut -AV, NS, M FF 10 12 4000 4020 56Ut -AV, NS, M FF Ut -AV, NS, M FF 12.5 13 5700 6000 54Ut.AV. Bulky. M . FF Ut.AV. Bulky. M . FF 8.5 10.5 6000 5300 56Ut -AV, NS, M FF Ut -AV, NS, M FF 12 13 6600 4900 60Ut -AV, NS, M FF Ut -AV, NS, M FF 8 13 4300 5300 60Ut.AV. Bulky. M . FF Ut.AV. Bulky. M . FF 13 12.5 4000 6600 32Ut.AV. Bulky. M . FF Ut.AV. Bulky. M . FF 10 12 4350 6000 40Ut -AV, NS, M FF Ut -AV, NS, M FF 12 13.5 4700 6000 52NA NA 9.5 10.5 5500 4500 40Ut -AV, NS, M FF Ut -AV, NS, M FF 9 12.5 6150 5600 60Ut -AV, NS, M FF Ut -AV, NS, M FF 9.5 10.5 4080 5020 52Ut -AV, NS, M FF Ut -AV, NS, M FF 11.5 13 7500 4500 48Ut -AV, NS, M FF Ut -AV, NS, M FF 10.5 12.5 4100 5800 54Ut -AV, NS, M FF Ut -AV, NS, M FF 8 12 5000 6000 50Ut.RV. Bulky. M . FF Ut.RV. Bulky. M . FF 13 13 9000 7300 50Ut.AV. Bulky. M . FF Ut.AV. Bulky. M . FF 9 11 5600 4800 56
TLC cal Examination
P/VP(cells/cumm)Hb gms %
MASTER CHART - Control Group

AT BT AT BT AT BT AT BT AT
50 44 40 4 6 0 4 0 050 44 46 6 4 0 0 0 060 52 40 6 0 0 0 0 058 46 40 2 2 0 0 0 060 49 36 1 4 0 0 0 064 64 32 8 4 4 0 0 056 40 36 0 3 0 3 0 250 48 44 8 4 0 2 0 056 40 40 0 2 0 2 0 058 38 36 2 4 0 2 0 058 36 42 4 0 2 0 0 056 64 40 2 2 0 2 0 052 40 38 4 6 0 4 0 058 38 36 2 4 0 2 0 052 40 40 4 4 0 2 0 260 44 40 2 0 0 0 0 058 44 38 0 4 0 0 0 048 34 48 4 2 2 2 0 056 36 42 4 2 0 0 0 056 66 44 2 0 0 0 0 060 52 40 8 0 0 0 0 058 42 38 6 2 0 2 0 050 54 48 6 2 0 0 0 056 34 40 2 4 4 0 0 050 44 46 4 2 0 2 0 050 46 48 6 2 0 0 0 050 42 46 4 2 0 2 0 048 38 48 2 2 0 2 0 058 40 40 6 2 4 0 0 058 36 38 6 2 2 2 0 0
InvestigationsDLC
E M BLP
- Control Group
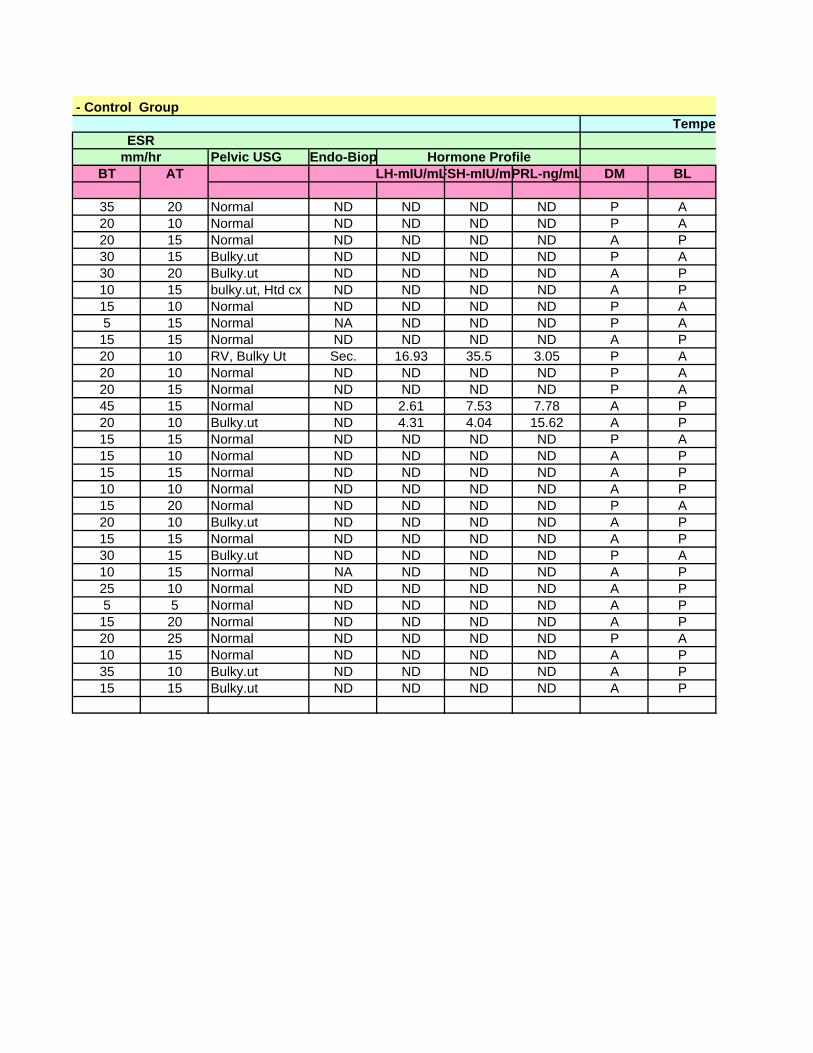
Pelvic USG Endo-BiopBT AT LH-mIU/mLFSH-mIU/mPRL-ng/mL DM BL
35 20 Normal ND ND ND ND P A20 10 Normal ND ND ND ND P A20 15 Normal ND ND ND ND A P30 15 Bulky.ut ND ND ND ND P A30 20 Bulky.ut ND ND ND ND A P10 15 bulky.ut, Htd cx ND ND ND ND A P15 10 Normal ND ND ND ND P A5 15 Normal NA ND ND ND P A15 15 Normal ND ND ND ND A P20 10 RV, Bulky Ut Sec. 16.93 35.5 3.05 P A20 10 Normal ND ND ND ND P A20 15 Normal ND ND ND ND P A45 15 Normal ND 2.61 7.53 7.78 A P20 10 Bulky.ut ND 4.31 4.04 15.62 A P15 15 Normal ND ND ND ND P A15 10 Normal ND ND ND ND A P15 15 Normal ND ND ND ND A P10 10 Normal ND ND ND ND A P15 20 Normal ND ND ND ND P A20 10 Bulky.ut ND ND ND ND A P15 15 Normal ND ND ND ND A P30 15 Bulky.ut ND ND ND ND P A10 15 Normal NA ND ND ND A P25 10 Normal ND ND ND ND A P5 5 Normal ND ND ND ND A P15 20 Normal ND ND ND ND A P20 25 Normal ND ND ND ND P A10 15 Normal ND ND ND ND A P35 10 Bulky.ut ND ND ND ND A P15 15 Bulky.ut ND ND ND ND A P
ESRHormone Profilemm/hr
- Control Group Tempe

SF SU BT AT AOF DOF AOF DOF AOF
A A 321 195 4 15 4 12 3A A 421 206 8 9 6 8 5A A 480 261 7 7 5 7 4A A 383 263 8 7 7 7 5A A 402 218 8 9 6 7 5A A 367 183 8 6 6 6 5A A 696 392 10 9 9 8 6A A 378 182 6 9 6 8 4A A 572 281 7 8 6 7 5A A 426 217 7 12 6 10 4A A 352 158 7 9 5 7 4A A 353 268 8 6 7 6 5A A 559 286 6 12 5 9 3A A 496 253 7 9 6 7 4A A 436 240 8 7 7 7 6A A 469 238 7 5 5 5 4A A 351 169 8 12 6 9 5A A 486 251 6 12 5 9 4A A 352 158 7 9 5 7 4A A 616 305 7 9 7 8 6A A 405 198 7 9 6 9 5A A 405 231 8 12 7 7 5A A 451 252 6 10 5 9 4A A 473 230 6 8 5 7 4A A 417 198 8 9 6 9 4A A 457 268 6 8 5 8 4A A 317 163 7 6 5 5 4A A 324 182 5 7 4 5 3A A 580 288 5 18 5 12 4A A 399 205 6 12 5 10 4
Assesment chart- Control Group
Treatment Chart
Ist cycle 2nd cycle 3rd c
rament
Total Score

NR PR R CDOF
7 0 0 0 17 0 0 0 15 0 1 0 06 0 0 0 16 0 1 0 06 0 0 0 17 0 0 0 15 0 0 1 06 0 0 0 18 0 1 0 05 0 1 0 05 0 0 1 05 0 0 1 05 0 0 0 15 0 0 1 04 0 0 0 18 0 1 0 07 0 0 1 05 0 0 1 05 0 0 1 07 0 0 1 06 0 1 0 07 0 0 0 16 0 0 1 07 0 0 0 17 0 0 0 14 0 0 1 05 0 0 1 010 0 0 0 18 0 1 0 0
Results- Control Group
cycle