clinical records management policy - east cheshire nhs trust records... · east cheshire nhs trust...
TRANSCRIPT
East Cheshire NHS Trust Clinical Records Management Policy – v.4 Information Governance Officer – September 2014 Page 1 of 55
Clinical Records Management Policy Incorporating Clinical Record Keeping Standards
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 2 of 55
Policy Title:
Clinical Records Management Policy Incorporating Clinical Record Keeping Standards
Executive Summary:
A definitive policy for the management of clinical records. A framework for improving quality, availability and effective use of records and the monitoring processes to effectively maintain records management standards. This policy also includes national guidance from the Royal College of Nursing and Royal College of Physicians in relation to the expected standards for clinical record keeping in the Trust.
Supercedes: Clinical Record Management Policy v 4
Description of Amendment(s):
Minor amendments to roles and responsibilities and reference to the NHS Code of Practice that has now been replaced by the Records Management Code of Practice for Health and Social Care 2016..
This policy will impact on: Clinical practices, administrative practices, employees.
Financial Implications:
Policy Area: Corporate Document Reference:
ECT002620
Version Number: V0.4 Effective Date: November 2016
Issued By: Director of Corporate Affairs & Governance
Review Date: November 2018
Author: Head of Integrated Governance
Impact Assessment Date:
November 2016
APPROVAL RECORD
Committees / Group Date
Consultation: Information Governance & Records Group
17/11/2016
Approved by Committees:
Approved by Director:
Information Governance & Records Group Director of Corporate Affairs & Governance
17/11/2016
17/11/2016
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 3 of 55
CONTENTS
1 Introduction .................................................................................................. 4
2 Scope and definitions .................................................................................. 4
3 Aims of records management systems ...................................................... 5
4 Roles and Responsibilities .......................................................................... 6
5 Legal and Professional Obligations ............................................................ 7
6 Retention and Disposal Schedules ............................................................. 7
7 Process for Management of Clinical Records ............................................ 8
8 Clinical Record Keeping Standards .......................................................... 10
9 Clinical Records Management Audit ........................................................ 13
10 Training ....................................................................................................... 13
11 Monitoring Performance ............................................................................ 13
12 Audit ............................................................................................................ 14
13 Review ........................................................................................................ 14
Appendix 1 ............................................................................................................. 15
Appendix 2 ............................................................................................................. 19
Appendix 3 ............................................................................................................. 22
Appendix 4 ............................................................................................................. 25
Appendix 5 ............................................................................................................. 30
Appendix 6 ............................................................................................................. 38
Appendix 7 ............................................................................................................. 45
Appendix 8 ............................................................................................................. 47
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 4 of 55
1 Introduction 1.1. Records management is the process by which an organisation manages all the
aspects of records whether internally or externally generated and in any format or media type, from their creation, all the way through their lifecycle to their eventual disposal.
1.2. The Records Management Code of Practice for Health and Social Care 2016 has
been published by the Information Governance Alliance as a guide to the required standards of practice in the management of records for those who work within or under contract to NHS organisations in England. It is based on current legal requirements and professional best practice.
1.3. Trust records are its corporate memory, providing evidence of actions and decisions
and representing a vital asset to support daily functions and operations. Records support policy formation and managerial decision making, protect the interests of the Trust and the rights of patients, staff and members of the public. They support consistency, continuity, efficiency and productivity and help deliver services in consistent and equitable ways.
1.4. Record keeping standards are the minimal requirements for all staff to adhere to in the
achievement of effective safe record keeping and documentation of clinical care. The Nursing and Midwifery Council and Royal College of Physicians have set out the minimum requirements for clinical records keeping and these are full endorsed by East Cheshire NHS Trust as the minimal standard for the organisation and all clinical staff.
2 Scope and definitions 2.1 This policy relates to all types of records including:
Patient health records (electronic or paper based concerning all specialties);
Accident and Emergency records;
Theatre registers and minor operations (and other related) registers;
X-ray and imaging reports, output and images;
Photographs, slides and other images;
Microform (microfiche/microfilm);
Audio and video tapes, cassettes, CD-ROM;
Computerised records;
Scanned records; And relates to all health records in use throughout the Trust including for those services based on the hospital site and in the community.
2.2 Records Management is a discipline which utilises an administrative system to direct
and control creation, version control, distribution, filing, retention, storage and disposal of records, in a way that is administratively and legally sound, whilst at the same time serving the operational needs of the Trust and preserving an appropriate historical record. The key components of records management are:
Record creation;
Record keeping;
Record maintenance (including tracking of record movements);
Access and disclosure;
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 5 of 55
Closure and transfer;
Appraisal;
Archiving; and
Disposal.
2.3 The term Records Life Cycle describes the life of a record from its creation/receipt through the period of its ‘active’ use, then into the period of ‘inactive’ retention (such as closed files which may still be referred to occasionally) and finally either confidential disposal or archival preservation.
2.4 In this policy, records are defines as ‘recorded information, in any form, created or
received and maintained by the Trust in the transaction of its business or conduct of affairs and kept as evidence of such activity.
2.5 Information is a corporate asset. The Trust’s clinical records are important sources of
administrative, evidential and historical information. They are vital to the Trust to support patient care and treatment and for purposes of accountability. The Trust holds an information asset register. More details relating to information assets can be found in the Information Governance Policy.
2.6 Record keeping is defined as “consisting of information about the physical or mental
health or condition of an identifiable individual made by or on behalf of a health professional in connection with the care of that individual”.
3 Aims of records management systems 3.1 The aims of our Clinical Records Management Systems are to ensure that:
records are available and can be accessed – records and the information within them can be located and displayed in a way consistent with its initial use and that the current version is identified where multiple versions exist;
records can be interpreted – the context of the record can be interpreted: who created or added to the record and in which location when, during which process, and how the record relates to other records;
records can be trusted – the record reliably represents the information that was actually used in, or created by, the clinical process, and its integrity and authenticity can be demonstrated;
records can be maintained through time – the qualities of availability, accessibility, interpretation and trustworthiness can be maintained for as long as the record is needed, perhaps permanently, despite changes of format;
records are secure – from unauthorised or inadvertent alteration or erasure, that access and disclosure are properly controlled and audit trails will track all use and changes. To ensure that records are held in a robust format which remain readable for as long as records are required;
records are retained and disposed of appropriately – using consistent and documented retention and disposal procedures, which include provision for appraisal and the permanent preservation of records with archival value; and
staff are trained – so that all staff are made aware of their responsibilities for record keeping and record management.
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 6 of 55
4 Roles and Responsibilities
4.1 The Chief Executive is the accountable officer and has overall responsibility for
ensuring that information governance is applied through the organisation 4.2 The Director of Corporate Affairs and Governance is the Trust’s Senior Information Risk Owner (SIRO) and has delegated accountability for:-
The Data Protection Act
IG Toolkit
Records Management
Information Security
Registration Authority activity 4.3 The Associate Medical Director – Clinical Effectiveness will act as the Caldicott
Guardian and will take a lead on Confidentiality issues.
a. To act as a champion for data confidentiality at Board level.
b. To develop a knowledge of confidentiality and data protection matters including links with external sources of advice and guidance.
c. To ensure that confidentiality issues are appropriately reflected in organisational strategies, policies and working procedures for staff.
d. To oversee all arrangements, protocols and procedures where confidential social care information may be shared with external bodies including disclosures to other public sector agencies and other outside interests
4.4 The Deputy Director of Corporate Affairs and Governance (Deputy SIRO) is
responsible for ensuring that systems and processes are implemented to ensure sound information governance across the Trust. This includes management of the information governance team budget.
4.5 The Head of Integrated Governance provides assurance reports to the
Information Governance & Records Management Group meeting, manages the information governance team, monitors compliance with the IG Toolkit and oversees the archiving and retention of records.
4.6 The Integrated Governance Manager has overall responsibility for operational
management of Information Governance and for the implementation and coordination of the information governance work programme across the Trust including providing guidance for good records management practice and promoting compliance with this policy although responsibility for specific requirements is devolved to specialist leads and service managers.
4.7 Operations Manager - Outpatients is responsible for the maintenance of the
patient casenote and has overall responsibility for the management of the health records library function and its procedures and will work with the Associate Medical Director, Clinical Effectiveness / Deputy Caldicott Guardian in this regard.
4.8 Managers and Supervisors will be responsible for ensuring the local
implementation of information governance and that they implement this and appropriate information policies within their sphere of responsibility. This includes taking appropriate management action should non-compliance arise. Clear
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 7 of 55
accountability arrangements will ensure that staff are held to account for the work that they do and this will be reinforced through contractual arrangements.
4.9 Employees, Volunteers, Contractors, sub-contractors all Trust staff, whether
clinical or administrative, employed, sub-contracted or volunteers, have a responsibility to ensure compliance with this and other Information Governance policies and procedures and must undertake annual training via the on line IG Training Toolkit.
5 Legal and Professional Obligations 5.1 All NHS records are public records and the Trust will take necessary actions to comply
with the legal and professional obligations set out in the Records Management Code of Practice for Health and Social Care 2016, in particular:
The Public Records Act 1958 – the Act sets out broad responsibilities for everyone who works with NHS records, defined as public records under the Act;
The Data Protection Act 1998 – regulates the management of personal information held both manually and on computer;
The Freedom of Information Act 2000 – provides a general right of access to recorded information held by public authorities;
The Common Law Duty of Confidentiality – based on precedent and case law, determines that healthcare providers must obtain patient consent to disclose personal information outside of the health care team;
NHS Confidentiality Code of Practice – offers guidance on protecting confidentiality, informing patients about uses of their personal information and the circumstances in which confidential information may be used or disclosed and any new legislation affecting records management that is subsequently agreed.
6 Retention and Disposal Schedules 6.1 It is a fundamental requirement that all health records are retained for a minimum
period of time for legal, operational, research and safety purposes. The length of time will depend on the clinical record type and its importance to business functions. The Trust has adopted the retention periods set out in the Records Management Code of Practice for Health and Social Care 2016:
6.2 Notes are retained within the Health Records Library for 12 months plus current year.
Deceased casenotes can be sent to Deepstore after 6 months. All case notes prior to this timeframe are available within the digital image system or available from off site storage at Deepstore. If casenotes are required from Deepstore there is a 24 hour turnaround in place should casenotes be required urgently.
6.3 Record Management & Storage of Child Health/School Health Records following
Death. Child Health/School Health record to be marked DECEASED clearly across the front of the file. Community record to be tracked on computer system by whoever is currently in possession and record returned to relevant Clinic/School Health Base. Record to be filed in mainstream filing to follow retention policy as for all child records.
6.4 Records are retained disposed and destroyed of appropriately - using consistent and
documented retention and disposal procedures, which include provision for appraisal and the permanent preservation of records with archival value. Detailed guidance on

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 8 of 55
retention periods for a full range of NHS personal health and different types of business and corporate records is provided in the Information Lifecycle and Records Management Policy and staff are trained - so that all staff are made aware of their responsibilities for record-keeping and record management.
7 Process for Management of Clinical Records The organisation has approved documentation which describes the process for managing the risks associated with clinical records in all media.
7.1 Accurate recording and knowledge of the whereabouts of all records is crucial if the
information they contain is to be located quickly and efficiently. One of the main reasons why records get misplaced or lost is because the next destination is not recorded anywhere
7.2 Tracking mechanisms should record the following (minimum) information
The item reference number or other identifier
A description of the item (e.g. the file title)
The person, unit or department, or place to who it is being sent
The date of transfer to them 7.3 Process for tracking the main hospital record
There is an electronic process for tracking the main hospital record through the PAS system and all appropriate staff will receive training in using the electronic system. Ongoing support and training is available within the Trust by a dedicated trainer.
7.4 Process for tracking A&E Admissions Where an admission occurs as the result of an A&E attendance, the appropriate pro-
forma is to be completed (either medical or surgical). Where the casenote has arrived at A&E, the pro-forma is to be filed before transfer to the ward. Where the casenote is not available to A&E staff, the pro-forma is to accompany the patient to the ward whereby the admitting Ward staff to be responsible for ensuring that the admissions pro-forma is filed within the notes appropriately.
7.5 Manually operated tracking systems
The following methods for manually tracking the movement of active records are suggested (specifically for community health records or those records held within departments):
A paper register - a book, diary or index card to record transfers
File “ absence” or “tracer” cards put in place of absent files
Record on a computer data base
Those teams using such manual tracking process to produce and have available procedure/guidance documentation to detail the local process.
7.6 Process for creating hospital health records
The process for the creation of records within the organisation is as followed and is a set standard for the organisation and all staff creating clinical records:
Search the MPI (Master Patient Index) for the patient (see Patient Management System (PMS) procedure for Searching MPI)
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 9 of 55
If the patient is not already recorded on MPI interrogate the National Strategic Tracing Service (NSTS) database for NHS number
Search the MPI by NHS number to ensure the patient is not registered under a different name/address/date of birth
If patient not found on MPI, register patient using ORE function. The Basic Details screen must be completed in full
PMS will then require a casenote to be allocated. All casenotes should be allocated to “Main” file. NB: No physical record will be created until requested e.g.: by Emergency Admissions or Outpatients
The patient’ Registered GP details must be completed and any other Registration Details provided
To complete the process an episode must be opened (see PMS procedure)
To register a patient without an episode use PMI function following the above procedure. Use option 3 “casenotes” to allocate a casenote.
7.7 Process for creating community-based health record
Community services must adhere to the documented process for creating local health records. Copies of the local processes are available from the Service Lead.
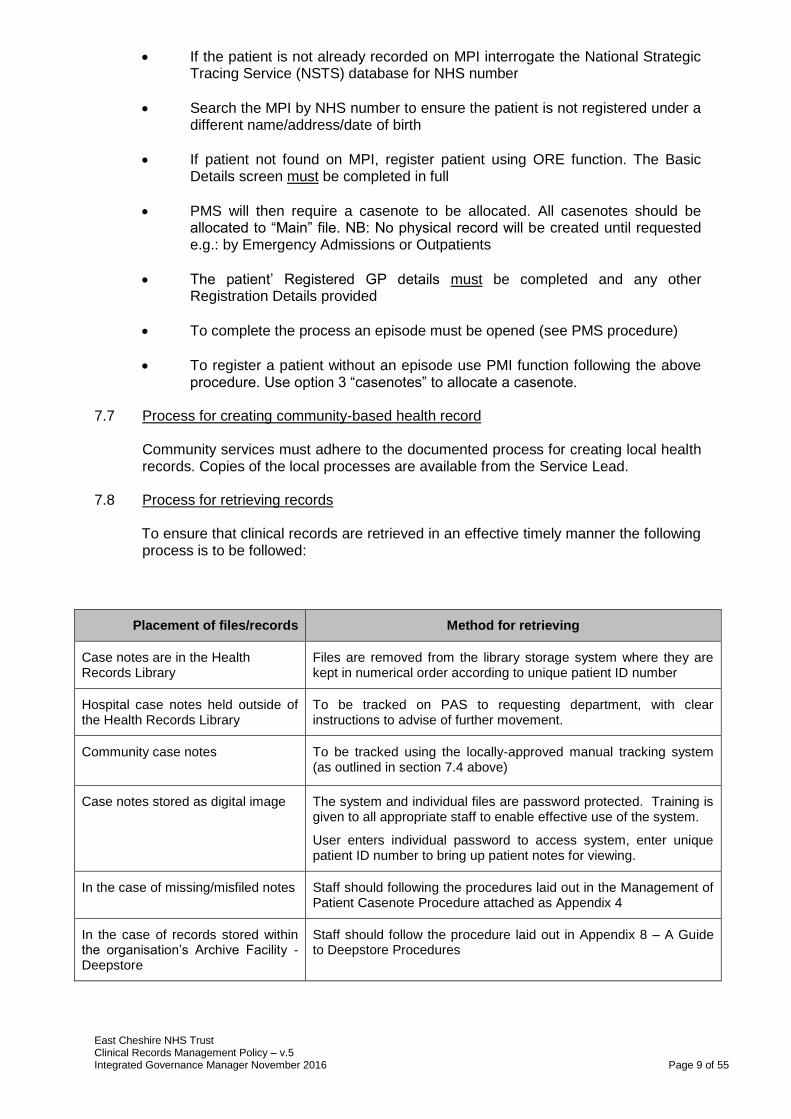
7.8 Process for retrieving records
To ensure that clinical records are retrieved in an effective timely manner the following process is to be followed:
Placement of files/records Method for retrieving
Case notes are in the Health Records Library
Files are removed from the library storage system where they are kept in numerical order according to unique patient ID number
Hospital case notes held outside of the Health Records Library
To be tracked on PAS to requesting department, with clear instructions to advise of further movement.
Community case notes To be tracked using the locally-approved manual tracking system (as outlined in section 7.4 above)
Case notes stored as digital image The system and individual files are password protected. Training is given to all appropriate staff to enable effective use of the system.
User enters individual password to access system, enter unique patient ID number to bring up patient notes for viewing.
In the case of missing/misfiled notes Staff should following the procedures laid out in the Management of Patient Casenote Procedure attached as Appendix 4
In the case of records stored within the organisation’s Archive Facility - Deepstore
Staff should follow the procedure laid out in Appendix 8 – A Guide to Deepstore Procedures
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 10 of 55
8 Clinical Record Keeping Standards 8.1 Good Record keeping is an integral part of the care of all patients and is essential to
the provision of safe and effective care. It is not an optional extra to be fitted in if circumstances allow.
8.2 Good record keeping, whether at an individual, team or organisational levels has
many important functions. These include a range of clinical, administrative and educational uses as well as legal ones.
8.3 The principles of good record keeping apply to all types of records, regardless of how
they are held. These can include:
Handwritten clinical notes
Emails
Letters to and from other health professionals
Laboratory reports
X-rays
Printouts from monitoring equipment
Incident reports and statements
Photographs 8.4 The basic principles of good record keeping are:
Every item1 will include the patients name, identification number (NHS Number), date of birth, location in hospital and consultant in charge of the care. This information should be specified each time an entry is made in the notes.
It is envisaged that staff will be working towards achieving the Royal College of Physician’s guidance to be followed in that patient identifying information to be included on every ‘side’ of every ‘page’ throughout the record and that the Trust’s paperwork will be amended to reflect this aspirational requirement. In addition, record keeping standards state that the following principles should apply to all health records:
Handwriting should be legible.
All entries to records should be signed. In the case of written records, the person’s name and job title should be printed alongside the first entry. The name and designation of the person making the entry should be legibly printed against their signature.
All entries will have the date and time recorded in 24 hour clock. This should be in real time and chronological order and be recorded as close to the actual time as possible. If there is a delay the time of the event and the delay should be recorded with the entry commencing with “Written in retrospect for ……..”.
1 An ‘Item’ can be:
- a standalone sheet whereby the ID should be placed on at least one side
- an integrated clerking proforma bundle
- charts/results
- X-ray reports
- E-mails printed off and included in the notes
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 11 of 55
Records should be accurate and recorded in such a way that the meaning is clear.
Records should be factual and only include approved abbreviations. The list of approved abbreviations is available on the Trust’s web-site. Health records should not contain jargon, meaningless phrases or irrelevant speculation.
Professional judgement should be used to decide what is relevant and what should be recorded.
Record details of any assessments and reviews undertaken and provide clear evidence of the arrangements which have been made for the future and ongoing care of the patient. This should also include details of information given about care and treatment.
Records should identify any risks or problems that have arisen and show the action taken to deal with them.
All staff have a duty to communicate fully and effectively with their colleagues, ensuring that they have all the information they need about the people in their care.
No staff must alter or destroy any records without being authorised to do so.
If you need to add something to a medical record or make a minor correction contemporaneously (e.g. correct a spelling error or insert/delete a word or two) then do not obliterate an entry that you wish to correct – run a single line through it so it can still be read and continue your sentence as usual.
If there is a need to insert using a caret (omission mark ^) , for example, a missed word, then do so and adhere to the following procedure.
a) Make the minor amendment unambiguously and transparently.
b) Put your initials clearly beside the entry in question.
c) Ensure that your full name, together with your initials, has been
documented in the records so that it is evident who made the amendments.
d) The date this took place should be inserted in the shortest form possible, besides your initials; e.g. 22/9/14 for 22nd September 2014 (even 22/9 if it is clear which year is referred to).
The above procedure is to amend minor imperfections during the completion of records. For anything more than minor changes to records the approach outlined below for retrospective amendments should be followed:
In the unlikely event that a staff member needs to alter their own or another healthcare professional’s records retrospectively2, they must give their name and job title, and sign and date the original documentation. They should make sure that the alterations they make, and the original record, are clear and auditable. All such deletions and alterations have to be countersigned by the member of staff making them and with a date and time (24hrs clock) entered when this occurred.
2 when an alteration / deletion has been made retrospectively in the case notes this should be stated and the reason for this
recorded
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 12 of 55
Where appropriate, the patient, or their carer, should be involved in the record keeping process.
Every entry in the medical record should identify the most senior healthcare professional present (who is responsible for decision making) at the time the entry is made.
On each occasion the consultant responsible for the patient care changes, the name of the new responsible consultant and the date and time of the agreed transfer of care should be recorded.
Advance decisions, consent and resuscitation status statements must be clearly recorded in the medical records.
Records should be readable when photocopied or scanned.
Coded expressions of sarcasm or humorous abbreviations to describe the people in your care should never be used in any circumstances.
All records must be written in black ink with the exception of operation / procedure notes.
No member of staff should ever falsify records.
The patient’s complete medical record should be available at all times during their stay in hospital.
The contents of the medical record should have a standardised structure and layout.
Documentation within the medical record should reflect the continuum of patient care and should be viewable in chronological order.
Data recorded or communicated on admission, handover and discharge should be recorded using a standardised proforma.
An entry should be made in the medical record whenever a patient is seen by a doctor. When there is no entry in the hospital record for more than four (4) days for acute medical care or seven (7) days for long-stay continuing care, the next entry should explain why.
The discharge record/discharge summary should be commenced at the time a patient is admitted to hospital.
Advance directives, consent and resuscitation status statements must be clearly recorded in the medical record. (These are to be recorded within the ALERTS section of ECNHST records)
8.5 Good record keeping standards for the safe, effective care of patients are endorsed
and supported by:
Nursing and Midwifery Council
Royal College of Physicians
The Chartered Society of Physiotherapy
College of Occupational Therapists
The Society of Radiographers
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 13 of 55
9 Clinical Records Management Audit 9.1 The Trust will regularly audit clinical records management practices for compliance
with this framework and establish an audit programme which is that each Service Area will audit an agreed number of case notes, as approved by the Information Governance and Records Management Group on an annual basis. Each Service Area to work with the Clinical Effectiveness Department to produce a work plan to ensure that their audit is representative. Each audit must be registered with Clinical Effectiveness who will support the Service Areas in the audit process.
9.2 The audit reports using the standard Trust audit documentation report will be agreed
by the Information Governance & Records Management Group and sent to Associate Directorates for action within each Service Area. Results and progress reports will be monitored by the Directorate SQS meeting and will inform future training requirements and highlight underperforming areas. Once action plans are agreed and completed a follow up audit must take place.
If the Trust compliance target is not achieved a re-audit will be carried out each year, using Trust approved pro-forma.
9.3 A combined audit report of all the Service Area casenotes audit will be presented to
the Information Governance and Records Management Committee on an annual basis
9.4 Managers will be responsible for regular, localised monitoring of the quality of
documentation and that standard good practice guidance is adhered to.
10 Training 10.1 All staff are obliged to undertake the annual IG Training Toolkit update which includes
standards of record keeping.
10.2 Line Managers will be responsible for arranging any ongoing training for applicable
staff in record keeping, case note handling and general clinical records practice in accordance with their personal development plan and departmental role requirements.
10.3 New staff will receive training through corporate and local induction.
10.4 All training provided to staff will be in line with the Data Protection Act 1998 and the Caldicott Report 1997.
11 Monitoring Performance 11.1 The trust will audit its records management practices which includes the audit
requirements for Service Areas as outlined in section 9 11.2 The audit will
Follow a mechanism of adapting the policy to cover missing areas if these are critical to the creation and use of records
Set and maintain standards by implementing new procedures, including obtaining feedback where the procedures do not match the desired levels of performance

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 14 of 55
Highlight where non-conformance to the procedures is occurring and suggest a tightening of control and adjustments to related procedures
11.3 All incidents relating to records management and or clinical record keeping will be
reported via the Trust incident reporting system and reviewed in line with the Trust processes.
12 Audit 12.1 This policy will be audited in line with the KPI’s identified in section 9 and 11 as a
minimum on an annual basis and reported to the Information Governance and Records Management Group. Any action plans developed from this audit will be agreed by the Group with a quarterly review of progress.
12.2 All audits should be registered with the Trust Department for Clinical Effectiveness.
13 Review 13.1 This policy will be reviewed by the Information Governance & Records Management
Group as a minimum every 2 years or sooner if new legislation, codes of practice or national standards is introduced.
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 15 of 55
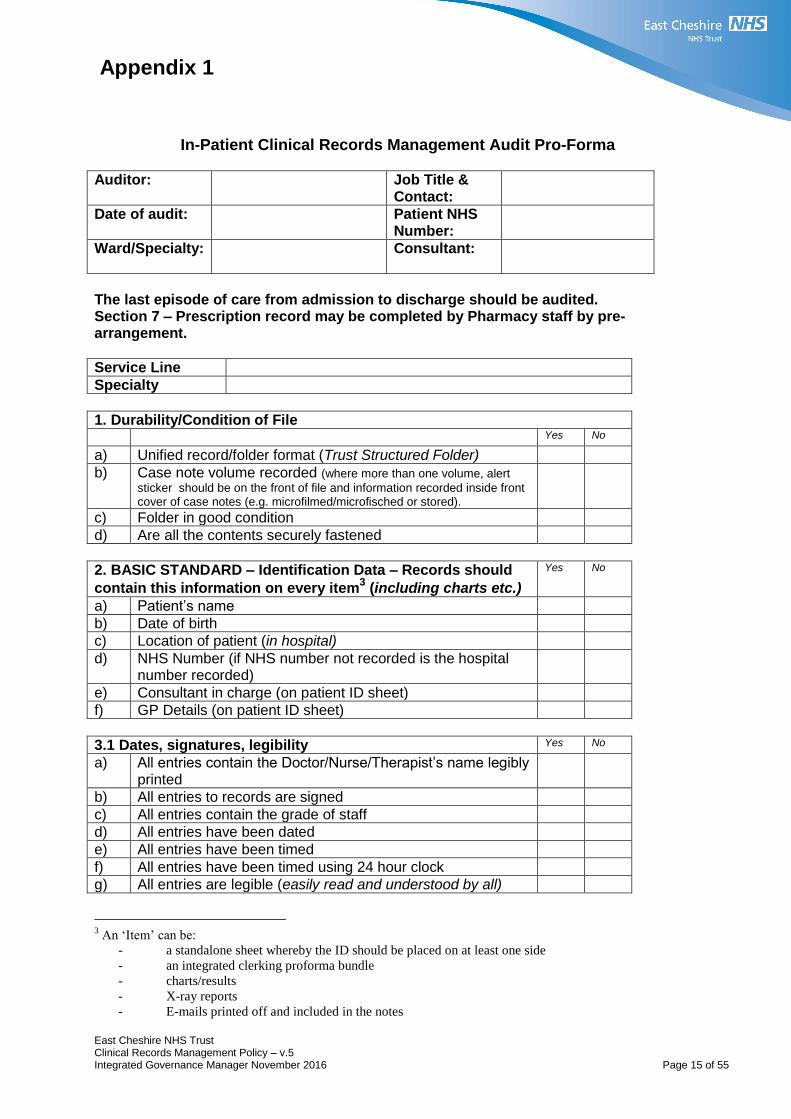
Appendix 1
In-Patient Clinical Records Management Audit Pro-Forma
Auditor:
Job Title & Contact:
Date of audit:
Patient NHS Number:
Ward/Specialty:
Consultant:
The last episode of care from admission to discharge should be audited. Section 7 – Prescription record may be completed by Pharmacy staff by pre-arrangement.
Service Line
Specialty
1. Durability/Condition of File
Yes No
a) Unified record/folder format (Trust Structured Folder)
b) Case note volume recorded (where more than one volume, alert
sticker should be on the front of file and information recorded inside front cover of case notes (e.g. microfilmed/microfisched or stored).
c) Folder in good condition
d) Are all the contents securely fastened
2. BASIC STANDARD – Identification Data – Records should
contain this information on every item3 (including charts etc.)
Yes No
a) Patient’s name
b) Date of birth
c) Location of patient (in hospital)
d) NHS Number (if NHS number not recorded is the hospital number recorded)
e) Consultant in charge (on patient ID sheet)
f) GP Details (on patient ID sheet)
3.1 Dates, signatures, legibility Yes No
a) All entries contain the Doctor/Nurse/Therapist’s name legibly printed
b) All entries to records are signed
c) All entries contain the grade of staff
d) All entries have been dated
e) All entries have been timed
f) All entries have been timed using 24 hour clock
g) All entries are legible (easily read and understood by all)
3 An ‘Item’ can be:
- a standalone sheet whereby the ID should be placed on at least one side
- an integrated clerking proforma bundle
- charts/results
- X-ray reports
- E-mails printed off and included in the notes

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 16 of 55
3.1 Dates, signatures, legibility Yes No
h) All entries are written in black ink (with the exception of operative notes)
i) Do entries comply with Trust abbreviations
3.2 Alterations Inserted/Deleted that have been made Contemporaneously (at the time)
Yes No No Errors
a) Have alterations inserted/deleted been scored through using one line so that the original record is still legible.
b) Have alterations inserted/deleted been initialled/signed
c) Has a name and initials been given on the record to identify who made the alterations inserted/deleted
d) Have alterations inserted/deleted been dated
3.3 Alterations/Deletions that have been made retrospectively2
Yes No No Errors
a) Have alterations/deletions been scored out so that the original record is still readable.
b) Have alterations/deletions been signed
c) Has a name and job title been given on alterations/deletions
d) Have alterations/deletions been timed in 24 hour clock format
e) Have alterations/deletions been dated
f) Have alterations/deletions been countersigned where a staff member has altered their own or another healthcare professional’s records retrospectively
g) Has a statement been recorded to state why the alteration/deletion was made
2 When an alteration/deletion has been made retrospectively in the case notes this should be
stated and the reason for this recorded.
4. Alert Notification Yes No N/A
a) Is a Patient Alert Record filed in the casenotes - IF NO – go to 4c
b) Does the Patient Alert Record contain the patient details
c) Is an allergy/intolerance recorded in the casenotes (e.g. on prescription record)
d) If yes, is this information recorded on the Patient Alert Record
e) ALERT sticker/notification is on the front of the file (if appropriate) *COMPLETE INCIDENT FORM IF ALLERGY/ALERT RECORDED IN FILE, BUT NO ALERT STICKER ON FRONT OF FILE
f) If alert sticker on front of file, is there an entry on alert record (inside file)
g) Advanced directives statements are recorded on the Alert Record (if appropriate)
h) Consent status statements are recorded on the Alert Record if identified by an Advanced directive
i) During the last episode of care is there a Do not attempt cardio-pulmonary resuscitation decision documented in the case notes
j) If yes, is there a red Do not attempt Cardio-pulmonary resuscitation (DNACPR) form filed at the front of the case notes
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 17 of 55
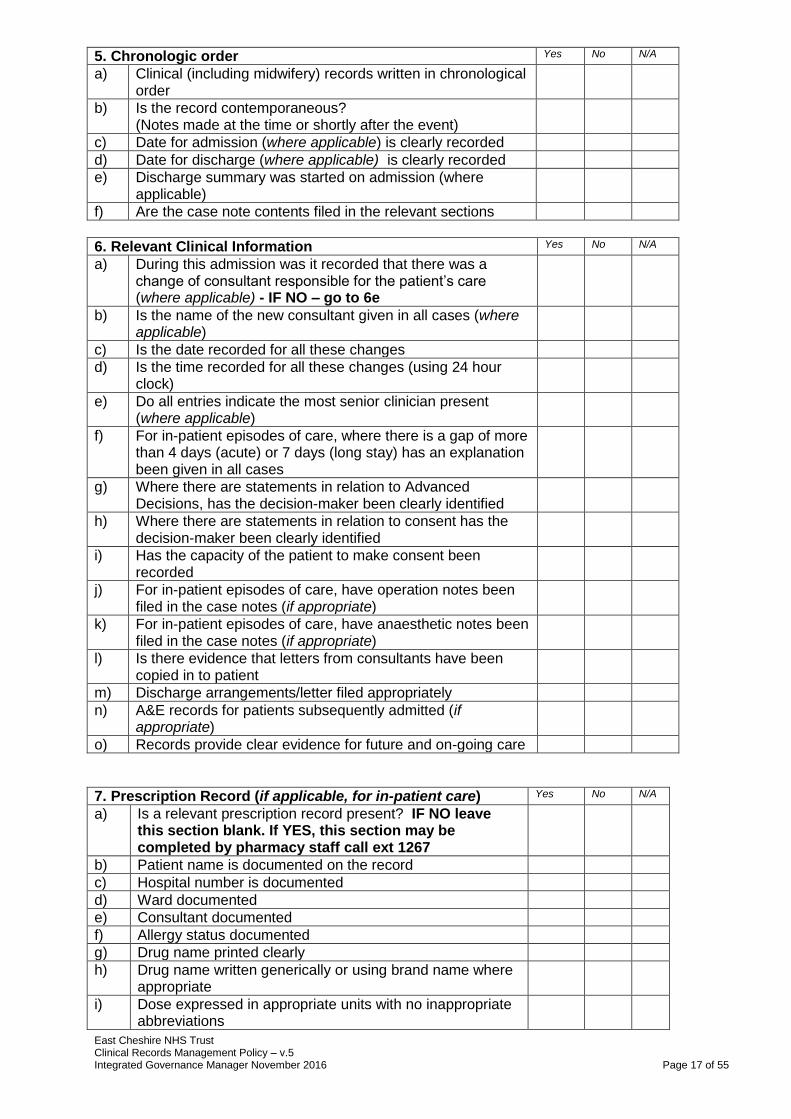
5. Chronologic order Yes No N/A
a) Clinical (including midwifery) records written in chronological order
b) Is the record contemporaneous? (Notes made at the time or shortly after the event)
c) Date for admission (where applicable) is clearly recorded
d) Date for discharge (where applicable) is clearly recorded
e) Discharge summary was started on admission (where applicable)
f) Are the case note contents filed in the relevant sections
6. Relevant Clinical Information Yes No N/A
a) During this admission was it recorded that there was a change of consultant responsible for the patient’s care (where applicable) - IF NO – go to 6e
b) Is the name of the new consultant given in all cases (where applicable)
c) Is the date recorded for all these changes
d) Is the time recorded for all these changes (using 24 hour clock)
e) Do all entries indicate the most senior clinician present (where applicable)
f) For in-patient episodes of care, where there is a gap of more than 4 days (acute) or 7 days (long stay) has an explanation been given in all cases
g) Where there are statements in relation to Advanced Decisions, has the decision-maker been clearly identified
h) Where there are statements in relation to consent has the decision-maker been clearly identified
i) Has the capacity of the patient to make consent been recorded
j) For in-patient episodes of care, have operation notes been filed in the case notes (if appropriate)
k) For in-patient episodes of care, have anaesthetic notes been filed in the case notes (if appropriate)
l) Is there evidence that letters from consultants have been copied in to patient
m) Discharge arrangements/letter filed appropriately
n) A&E records for patients subsequently admitted (if appropriate)
o) Records provide clear evidence for future and on-going care
7. Prescription Record (if applicable, for in-patient care) Yes No N/A
a) Is a relevant prescription record present? IF NO leave this section blank. If YES, this section may be completed by pharmacy staff call ext 1267
b) Patient name is documented on the record
c) Hospital number is documented
d) Ward documented
e) Consultant documented
f) Allergy status documented
g) Drug name printed clearly
h) Drug name written generically or using brand name where appropriate
i) Dose expressed in appropriate units with no inappropriate abbreviations

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 18 of 55
j) Route documented and legible
k) Signed by prescriber
l) Surname legibly printed
m) Date treatment to commence (including year)
n) Numbers used (NOT Roman numerals)
o) English instructions are used
p) Times of administration annotated
q) With stop or review dates for anti-infectives
r) Maximum dose documented where applicable
s) Line through discontinued item
t) Discontinuation signed
u) Discontinuation dated
v) If prescription chart is full/messy, has a new prescription chart been written?
w) If more than one prescription chart in use is this clearly indicated at the top of each chart i.e. 1 of 1, 1 of 2
Additional Comments
Thank you for your time completing this form Please send the completed proformas to:
Clinical Effectiveness Team
Top Floor, New Alderley House Macclesfield Hospital
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 19 of 55
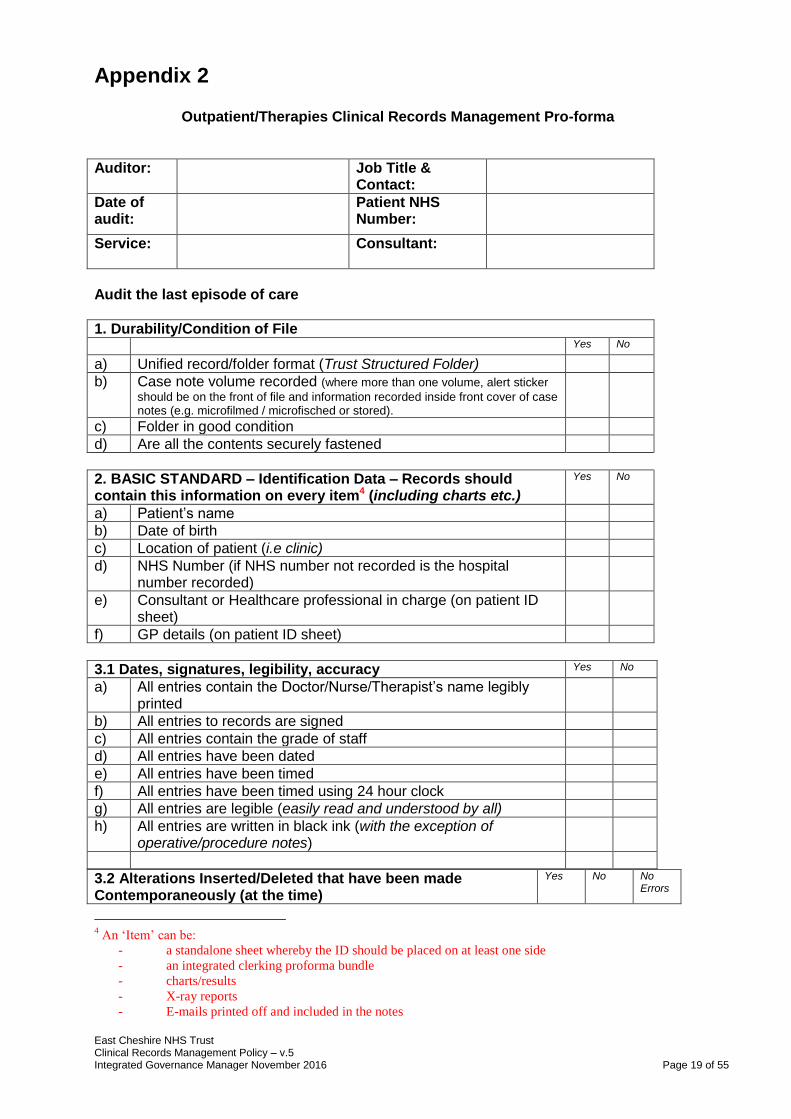
Appendix 2
Outpatient/Therapies Clinical Records Management Pro-forma
Auditor:
Job Title & Contact:
Date of audit:
Patient NHS Number:
Service:
Consultant:
Audit the last episode of care
1. Durability/Condition of File
Yes No
a) Unified record/folder format (Trust Structured Folder)
b) Case note volume recorded (where more than one volume, alert sticker
should be on the front of file and information recorded inside front cover of case notes (e.g. microfilmed / microfisched or stored).
c) Folder in good condition
d) Are all the contents securely fastened
2. BASIC STANDARD – Identification Data – Records should contain this information on every item4 (including charts etc.)
Yes No
a) Patient’s name
b) Date of birth
c) Location of patient (i.e clinic)
d) NHS Number (if NHS number not recorded is the hospital number recorded)
e) Consultant or Healthcare professional in charge (on patient ID sheet)
f) GP details (on patient ID sheet)
3.1 Dates, signatures, legibility, accuracy Yes No
a) All entries contain the Doctor/Nurse/Therapist’s name legibly printed
b) All entries to records are signed
c) All entries contain the grade of staff
d) All entries have been dated
e) All entries have been timed
f) All entries have been timed using 24 hour clock
g) All entries are legible (easily read and understood by all)
h) All entries are written in black ink (with the exception of operative/procedure notes)
3.2 Alterations Inserted/Deleted that have been made Contemporaneously (at the time)
Yes No No Errors
4 An ‘Item’ can be:
- a standalone sheet whereby the ID should be placed on at least one side
- an integrated clerking proforma bundle
- charts/results
- X-ray reports
- E-mails printed off and included in the notes
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 20 of 55
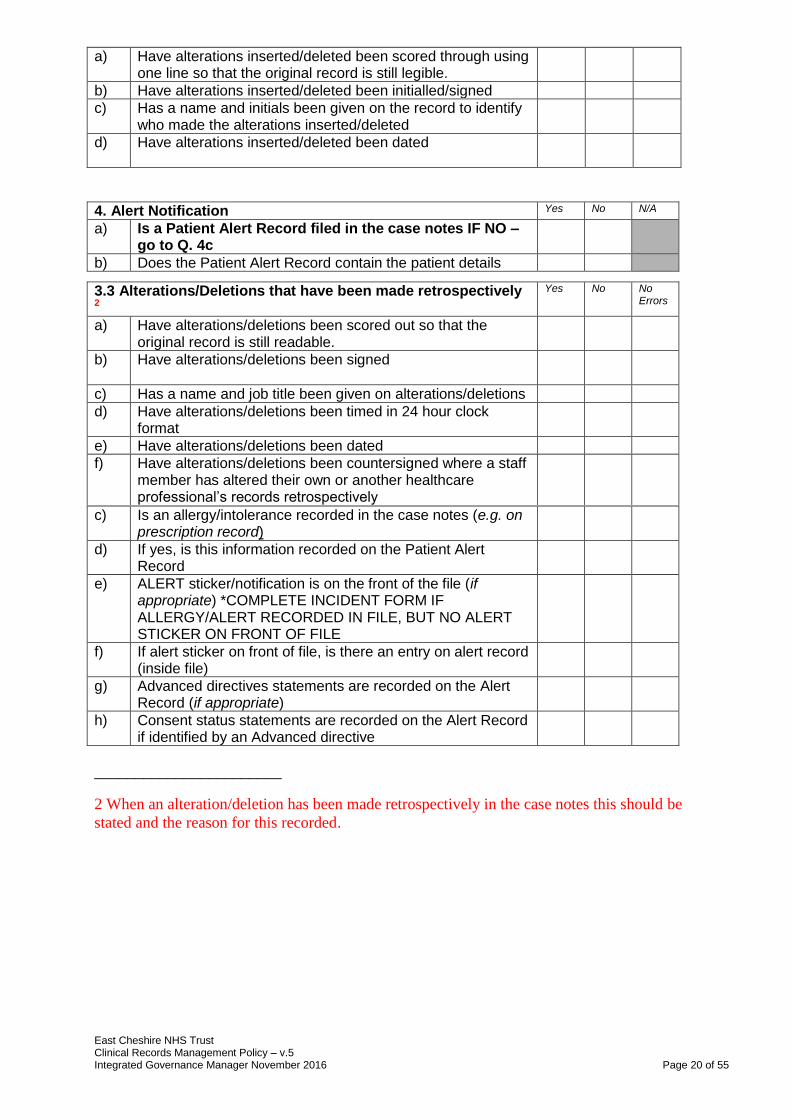
a) Have alterations inserted/deleted been scored through using one line so that the original record is still legible.
b) Have alterations inserted/deleted been initialled/signed
c) Has a name and initials been given on the record to identify who made the alterations inserted/deleted
d) Have alterations inserted/deleted been dated
4. Alert Notification Yes No N/A
a) Is a Patient Alert Record filed in the case notes IF NO – go to Q. 4c
b) Does the Patient Alert Record contain the patient details
c) Is an allergy/intolerance recorded in the case notes (e.g. on prescription record)
d) If yes, is this information recorded on the Patient Alert Record
e) ALERT sticker/notification is on the front of the file (if appropriate) *COMPLETE INCIDENT FORM IF ALLERGY/ALERT RECORDED IN FILE, BUT NO ALERT STICKER ON FRONT OF FILE
f) If alert sticker on front of file, is there an entry on alert record (inside file)
g) Advanced directives statements are recorded on the Alert Record (if appropriate)
h) Consent status statements are recorded on the Alert Record if identified by an Advanced directive
_______________________
2 When an alteration/deletion has been made retrospectively in the case notes this should be
stated and the reason for this recorded.
3.3 Alterations/Deletions that have been made retrospectively 2
Yes No No Errors
a) Have alterations/deletions been scored out so that the original record is still readable.
b) Have alterations/deletions been signed
c) Has a name and job title been given on alterations/deletions
d) Have alterations/deletions been timed in 24 hour clock format
e) Have alterations/deletions been dated
f) Have alterations/deletions been countersigned where a staff member has altered their own or another healthcare professional’s records retrospectively

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 21 of 55
5. Chronologic order Yes No N/A
a) Clinical (including midwifery) records written in chronological order
b) Is the record contemporaneous? (Notes made at the time or shortly after the event)
c) Date for discharge (where applicable) is clearly recorded
d) Are the case notes contents filed in the relevant sections
6. Relevant Clinical Information Yes No N/A
a) Is the name of the new healthcare professional given in all cases (where applicable)
b) Is the date recorded for all these changes
c) Is the time recorded for all these changes (using 24 hour clock)
d) Where there are statements in relation to Advanced Decisions, has the decision-maker been clearly identified
e) Where there are statements in relation to consent has the decision-maker been clearly identified
f) Has the capacity of the patient to make consent been recorded
g) Discharge arrangements/letter filed appropriately
h) Records provide clear evidence for future and on-going care
Additional Comments
Thank you for your time completing this form Please send the completed proformas to:
Clinical Effectiveness Team
Top Floor, New Alderley House Macclesfield Hospital
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 22 of 55
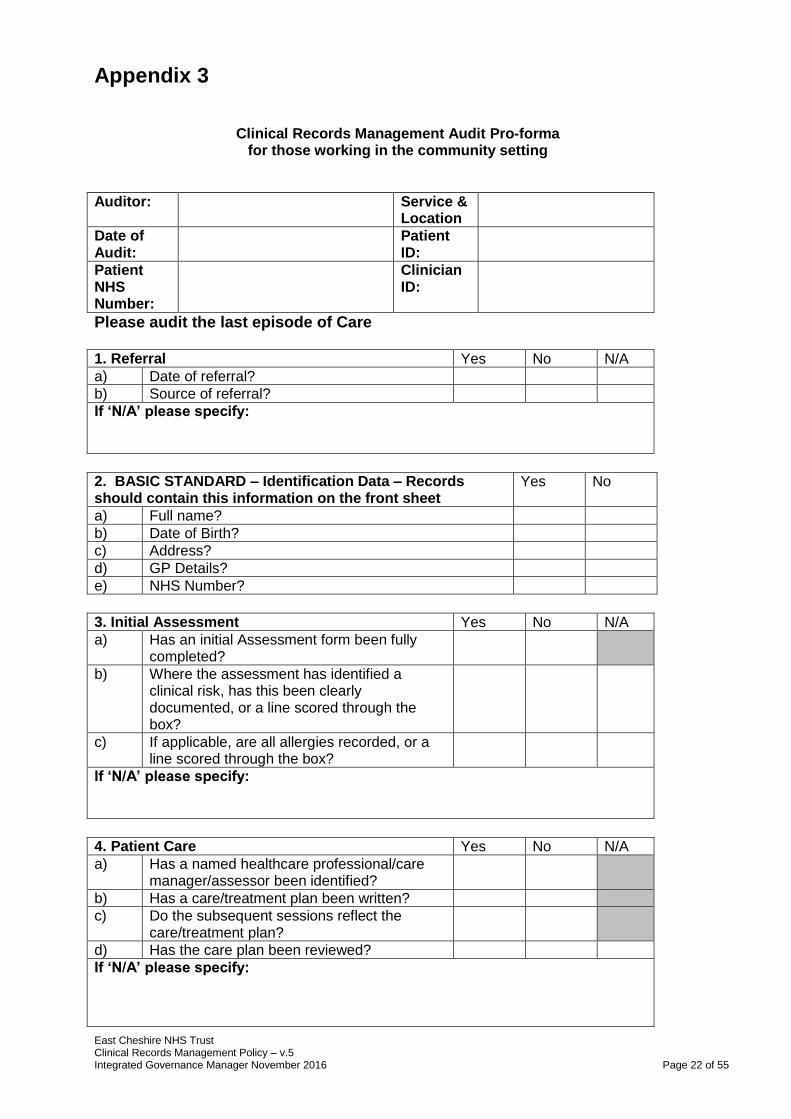
Appendix 3
Clinical Records Management Audit Pro-forma for those working in the community setting
Auditor:
Service & Location
Date of Audit:
Patient ID:
Patient NHS Number:
Clinician ID:
Please audit the last episode of Care 1. Referral Yes No N/A
a) Date of referral?
b) Source of referral?
If ‘N/A’ please specify:
2. BASIC STANDARD – Identification Data – Records should contain this information on the front sheet
Yes No
a) Full name?
b) Date of Birth?
c) Address?
d) GP Details?
e) NHS Number?
3. Initial Assessment Yes No N/A
a) Has an initial Assessment form been fully completed?
b) Where the assessment has identified a clinical risk, has this been clearly documented, or a line scored through the box?
c) If applicable, are all allergies recorded, or a line scored through the box?
If ‘N/A’ please specify:
4. Patient Care Yes No N/A
a) Has a named healthcare professional/care manager/assessor been identified?
b) Has a care/treatment plan been written?
c) Do the subsequent sessions reflect the care/treatment plan?
d) Has the care plan been reviewed?
If ‘N/A’ please specify:

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 23 of 55
5. Consent Yes No N/A
a) Where applicable has the Consent form been completed and signed?
b) For children under 16, has the parent/guardian given written consent to the treatment plan?
If ‘N/A’ please specify:
6. Discharge from Service Yes No N/A
a) Date of discharge?
b) Reason for discharge?
If ‘N/A’ please specify:
7. Confidentiality Yes No N/A
a) Are all the records stored in a place that ensures confidentiality i.e. a locked cupboard or a locked room?
If ‘N/A’ please specify:
8. Record Management Standards Yes No No Error
a) Are all entries written in black ink?
b) Are abbreviations used as in the Trust glossary?
c) Have all the assessment notes been signed and dated?
d) Was the signature legible?
e) Were all assessments timed, using the 24 hour clock?
f) Was the designation stated?
Alterations/Deletions that have been made Contemporaneously/retrospectively 2
g) Have alterations/deletions been scored out so that the original record is still readable.
h) Have alterations/deletions been signed
i) Has a name and job title been given on alterations/deletions
j) Have alterations/deletions been dated
k) If the alteration/deletion is retrospective in the case notes, has a reason for the alteration / deletion been stated
2 When an alteration/deletion has been made retrospectively in the case notes this should be stated and the reason
for this recorded.

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 24 of 55
8. Record Management Standards Yes No No Error
l) Have alterations/deletions been countersigned where a staff member has altered their own or another healthcare professional’s records retrospectively
m) Are all the contents securely fastened?
n) Is the record contemporaneous? (Notes made at the time or shortly after the event)
o) Is the record legible?
p) Is the record in chronological order?
q) Are there any gaps between each written session?
r) Do the records contain inappropriate judgemental statements/opinions?
s) Is the patient’s NHS number on every side of every page?
t) Is the patient’s name on every side of every page?
u) Is the patient’s date of birth on every side of every page?
Additional comments:
Thank you for your time completing this form Please send the completed proformas to:
Clinical Effectiveness Team

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 25 of 55
Appendix 4 Standard Operating Procedure Template
Title of Standard Operation Procedure:
Storage & Retention of all Medical Casenotes
Reference Number: Version No: 3
Issue Date: Review Date:
Purpose and Background
To provide operational guidance on storage of Medical Casenotes that are no longer current either physically (off site), or electronically
Scope (i.e. organisational responsibility) Vital functions affected by this procedure:
The Trust has legal responsibility arising from the Data Protection Act 1998 to make sure that its information is available and secure, and that it is not kept for longer than is necessary. All users of medical case notes
Monitoring Compliance
Requirement to be monitored. Must include all requirements within NHS LA Standards
Process to be used for monitoring e.g. audit
Responsible individual/ committee for carrying out monitoring
Frequency of monitoring
Responsible individual/ committee for reviewing the results
Responsible individual/ committee for developing action plan
Responsible individual / committee for monitoring action plan
1.7 – Health Records Management
b) legal obligations that apply to records
e) how health records are
retrieved from storage f) process for retention,
disposal and destruction of records
g) how the organisation
monitors compliance with all of the above.
Audit of Deepstore Destruction Schedules
Information Governance Manager
4 x annually
Health Records Management Sub-Group
Information Governance Manager
Health Records Management Sub-Group
East Cheshire NHS Trust Clinical Records Management Policy – v.4 Information Governance Officer – September 2014 Page 26 of 55
Escalations (if you require any further clarification regarding this procedure please contact):
Information Governance Officer
Committees / Group
Date
Consultation: Health Records Management Sub-Group
Approval Committee
Information Governance & Records
Management Group
Ratified by Committee: Information Governance & Records
Management Group
Received for information:
Trust Internet
1 INTRODUCTION
The Trust currently stores approximately 250,000 sets of case notes in paper format. In addition, archived records are stored either physically or electronically, with on-line retrieval functionality which is operational 24/7, (EDM) or Physically within secure storage (Deepstore)
2 GUIDANCE
The minimum period of retention of personal health records, no longer required for clinical purposes, should be determined in accordance with the Records Management Code of Practice for Health and Social Care 2016. The guidance is applicable to all NHS records and details the recommended minimum retention period for each record type.
Full details of the retention schedule are outlined in the Trust Corporate Records Management Strategy (Information Lifecycle Policy) available on the intranet.
Further advice can be sought from the Information Governance Officer.
THE PUBLIC RECORDS ACT All NHS records, and those of NHS predecessor bodies, are public records under the terms of the Public records Act 1958. The Act sets out broad responsibilities for everyone who works with such records, and provides guidance and supervision by the keeper of Public Records. It requires that those records that have been selected for archival preservation are transferred to The National Archives or a Place of deposit appointed under the Act. The maximum period for which records can be kept prior to transfer is usually 30 years (any NHS body that feels it needs to hold records for a longer period must consult with The National
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 27 of 55
Archives).
STANDARD PROCEEDURE
In line with the guidance and in order to reduce unnecessary storage, the guidelines for retention and destruction of medical casenotes is as follows:- 1. All medical casenotes relating to patients with a current episode of care will be retained
on Trust premises. This will include casenotes from all specialties. Where additional records are identified, for example occupational therapy, existence of these records must be cross-referenced to the hospital casenote using the alert system.
2. All medical casenotes relating to one year after discharge will be retained on Trust
premises. The Health Records Library will be the only main storage area with all other departments using a loan facility tracked on the PAS system to track records to individual areas.
3. Any medical casenotes relating to patients whose last episode of care is greater than
one year will be culled and tracked to Deepstore for storage. 4. All deceased casenotes will be stored one year after date of death and will be made
available to the appropriate bodies requiring access e.g. Cancer registry, Clinical Effectiveness.
5. All medical casenotes relating to a Legal case or Complaint must be marked “not
to be destroyed”. The Legal Services department or PALS department are to advise the Health Records Library when the do not destroy mark can be removed and the culling process can be followed.
9. Where there are multiple volume casenotes, volumes other than the current can be
stored within the Deepstore facility and tracked on PAS and with Deepstore appropriately.
10. All medical casenotes identified for destruction should be:-
Checked by the appropriate Health Records Library staff
Comply with legislation
Comply with local policies
Be kept secure whilst awaiting destruction
Be destroyed as confidential waste, with an appropriate destruction certificate obtained.
11. Costs incurred for retrievals will automatically be charged to individual Business Units.
Records of retrieval transactions will be maintained by the Health Records Library and re-charged on a monthly basis.
APPENDIX 1 - Outlines East Cheshire NHS Trust Records Management Destruction Guidelines in line with the Department of Health reviewed retention schedule. DESTRUCTION OF CONFIDENTIAL PATIENT RECORDS
Destruction of confidential medical casenotes must ensure that their confidentiality is fully maintained. Normally destruction should be by incineration or shredding. Where this service is provided by a contractor it is the responsibility of the Trust to satisfy itself that the methods used throughout all stages including transport to the destruction site provide satisfactory safeguards against accidental loss or disclosure.

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 28 of 55
Additional Information (if appropriate) See Appendix 1 (below) – Retention Schedule guidance
Back up information (if appropriate) Document Change History Roles and Responsibilities Abbreviations References
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 29 of 55
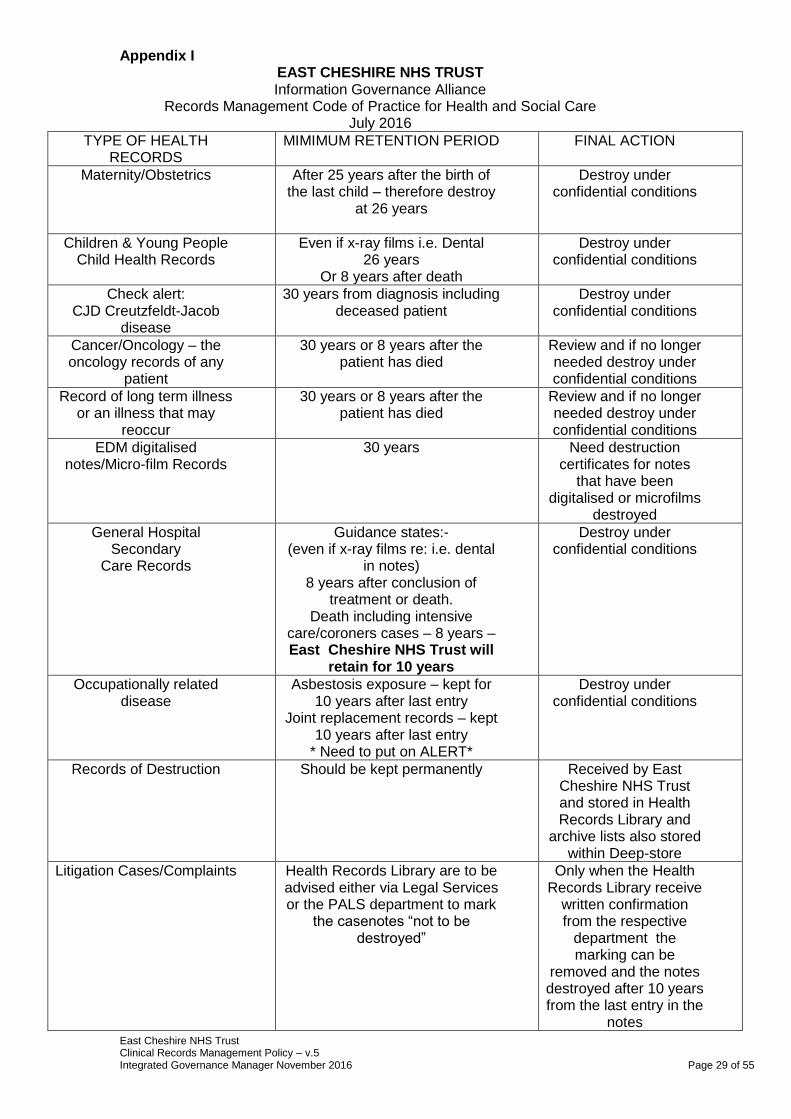
Appendix I EAST CHESHIRE NHS TRUST Information Governance Alliance
Records Management Code of Practice for Health and Social Care July 2016
TYPE OF HEALTH RECORDS
MIMIMUM RETENTION PERIOD FINAL ACTION
Maternity/Obstetrics After 25 years after the birth of the last child – therefore destroy
at 26 years
Destroy under confidential conditions
Children & Young People Child Health Records
Even if x-ray films i.e. Dental 26 years
Or 8 years after death
Destroy under confidential conditions
Check alert: CJD Creutzfeldt-Jacob
disease
30 years from diagnosis including deceased patient
Destroy under confidential conditions
Cancer/Oncology – the oncology records of any
patient
30 years or 8 years after the patient has died
Review and if no longer needed destroy under confidential conditions
Record of long term illness or an illness that may
reoccur
30 years or 8 years after the patient has died
Review and if no longer needed destroy under confidential conditions
EDM digitalised notes/Micro-film Records
30 years Need destruction certificates for notes
that have been digitalised or microfilms
destroyed
General Hospital Secondary
Care Records
Guidance states:- (even if x-ray films re: i.e. dental
in notes) 8 years after conclusion of
treatment or death. Death including intensive
care/coroners cases – 8 years – East Cheshire NHS Trust will
retain for 10 years
Destroy under confidential conditions
Occupationally related disease
Asbestosis exposure – kept for 10 years after last entry
Joint replacement records – kept 10 years after last entry
* Need to put on ALERT*
Destroy under confidential conditions
Records of Destruction Should be kept permanently Received by East Cheshire NHS Trust and stored in Health Records Library and
archive lists also stored within Deep-store
Litigation Cases/Complaints Health Records Library are to be advised either via Legal Services or the PALS department to mark
the casenotes “not to be destroyed”
Only when the Health Records Library receive
written confirmation from the respective
department the marking can be
removed and the notes destroyed after 10 years from the last entry in the
notes

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 30 of 55
Appendix 5 Standard Operating Procedure Template
Title of Standard Operation Procedure:
MANAGEMENT OF PATIENT CASENOTES (THERAPY SERVICES)
Reference Number: Version No: 3
Issue Date: Review Date:
Purpose and Background
This procedure is meant to outline a general standard practice when creating, tracking, discharging and managing the disposal of Therapy Services patient records.
Scope (i.e. organisational responsibility) Vital functions affected by this procedure:
The Trust has legal responsibility arising from the Data Protection Act 1998 to make sure that its information is available and secure, and that it is not kept for longer than is necessary. All staff involved in creating patient records
Monitoring Compliance
Requirement to be monitored. Must include all requirements within NHS LA Standards
Process to be used for monitoring e.g. audit
Responsible individual/ committee for carrying out monitoring
Frequency of monitoring
Responsible individual/ committee for reviewing the results
Responsible individual/ committee for developing action plan
Responsible individual / committee for monitoring action plan
1.8 Health Record-Keeping
Standards
a) basic record-keeping standards, which must be used by all staff
b) process for making sure a contemporaneous record of care is completed
c) how the organisation trains staff, in line with the training needs analysis
d) how the organisation monitors compliance with all of the above.
Escalations (if you require any further clarification regarding this procedure please contact):
PAS System Manager
Committees / Group: Date:
Consultation: Data Quality Group
Approval Committee
Information Governance & Records Management Group
Ratified by: Committee Information Governance & Records Management Group

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 31 of 55
Received for information:
Internet
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 32 of 55
Operating Procedure This procedure is meant to outline a general standard practice when creating, tracking, discharging and managing the disposal of Therapy Services patient records. This procedure does not include information on the Episoding, Transfer or Grading of New Patient referrals, but should be used in conjunction with additional procedures where necessary. Registering a Patient – Acute Upon the receipt of a patient referral: 1. Search the Master Patient Index (MPI) of the Patient Administration System
(PAS) for a patient with a matching NHS Number, if one is stated in the referral.
2. If the patient cannot be found, search the MPI of PAS for a patient with
matching Surname, Forename and Date of Birth as the patient stated in the referral.
Searches should be carried out in either the ‘RBA – Refer and Book Appointment’ or ‘EPI – Episode Enquiry’ screens of PAS. 3. If the patient cannot be found on the MPI, contact the Data Quality
Department on extension 1289, who will register the patient on PAS. Please note that notes are electronically allocated by the Data Quality Department, a hard copy of “MAIN” medical casenotes will not be created by the medical records library. In order to create Therapy Services specific casenotes, follow the procedure below. Patient Checks Before Creating New Casenotes Upon the receipt of a patient referral and before creating a new set of casenotes: 1. Use the ‘APE – Appointment Enquiry’ and ‘EPI – Episode Enquiry’ functions
of PAS to check the patient’s recent history. 2a. If the patient has outstanding activity that matches the new referral (i.e. recent
physiotherapy treatment upon receipt of a physio referral or recent Occupational Therapy treatment upon receipt of an O.T. referral) then additional patient records should not be created. The new referral letter should be passed to the treating clinician for assessment, or the Senior Therapist in the case of a patient currently on an outpatient waiting list. If the treating clinician is unavailable, amalgamate the new referral with the existing patient casenote and mark the front of the casenote with a dated note to alert the therapist that additional information that has been received.
2b. If the patient has recently discharged activity, the new referral letter should be assessed by the previously treating clinician. Follow the outcomes below; if the letter:
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 33 of 55
Is for therapist information only Amalgamate the new letter with the discharged notes Advises that treatment is still required for the same problem
Amalgamate the letter with the previous casenote, reopen the patient’s previous Episode of care and organise a further appointment for the patient to be seen. Continue to use the previous casenote during the patient’s treatment
Advises that treatment is required for a different problem
Amalgamate the letter with the previous casenote, open a new Episode of care and take the relevant action (such as booking an appointment or adding the patient to a waiting list). Continue to use the previous casenote during the patient’s treatment
2c. When it is clear that the referral letter is unrelated to a previous problem and
that the patient has no recent Therapy Services casenotes, a new Episode of care should be created on PAS (see the ‘Episoding New Referrals’ procedure) and a new set of casenotes created.
Creating New Therapy Services Casenotes - Acute 1. Physiotherapy casenotes are made up of a Therapy Services Casenote Front
Sheet, accompanying referral letter and a Casenote Tracking Card. Occupational Therapy casenotes are made up of a Therapy Services Casenote Front Sheet, accompanying referral letter, an Occupational Therapy Treatment Pack and a Casenote Tracking Card.
2a. Using the ‘PMI – PMI Add / Revise’ function of PAS, cross-check all patient
details between PAS and the referral and update the electronic record where appropriate. All details should be checked, including:
Title Full Name Sex Date of Birth Address Contact Numbers
NHS Number Hospital Number G.P Details Date of Referral Referrer Ethnicity
Once all details have been confirmed and an Episode of care opened on PAS, print the PAS document ‘THERAPYCN’ to your local PAS printer to create a Therapy Services Casenote Front Sheet. If there are any queries with patient’s personal information, please contact the Data Quality Department on extension 1289. 2b. In the case of Occupational Therapy referrals, Therapy Services Casenote
Front Sheets are to be combined with an Occupational Therapy Treatment Pack, available in the Admin Office, which are also for clinician completion.
2c. The Casenote Front Sheet, referral letter (and Occupational Therapy
Treatment Pack, where appropriate) are combined into a coloured plastic wallet to create a Therapies Casenote. The colour of the wallet denotes the referral’s speciality, as shown below:
Musculoskeletal Physio - Yellow Wallet Women’t Health Physio - Red Wallet Rheumatology Physio - Clear Wallet Neurology Physio - Clear Wallet Light Therapy - Blue Wallet Occupational Therapy - Green Wallet
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 34 of 55
2d. The newly created casenote should then placed in the appropriate place for
assessment or booking (see the ‘Episoding New Referrals’ procedure). The Tracking Card should be completed, stating the records whereabouts (see ‘Tracking Casenotes’ below) and immediately filed in the main file.
Creating New Therapy Services Casenotes - Community Community Services to adhere to locally documented process for creating and tracking casenotes. Copies of such procedures are available from the Associate Director’s office. Tracking Casenotes In order to maintain the quality of patient care and minimise the risk of clinical incidents, it is important to have the ability to check the whereabouts of any set of casenotes within the department at any time. Services (specifically those based in the community) must have locally documented tracking procedures that facilitate the requirements of good record keeping with the needs of the service. Services operating on the acute site, to use the following manual tracking system: 1. Whenever a patient casenote is removed from the main file, the Casenote
Tracking Card is to be completed and left in place of the casenote to show where the records have been taken. All Tracking Card entries are to be initialled so as to create an audit trial should the casenote be misplaced.
It is the responsibility of the person removing the casenote from the main file to complete the Casenote Tracking Card. 2. When the casenote is returned, the Tracking Card should be amalgamated
back with the patient record. No entry on the Tracking Card is required when returning casenotes to the main file.
3. Upon a patient’s discharge from the Therapy Services department, the
patient’s casenotes (Tracking Card included) are removed from the main file and stored, ready for destruction, in the Therapy Services Records Office. See ‘Records Storage and Destruction’ below for further information.
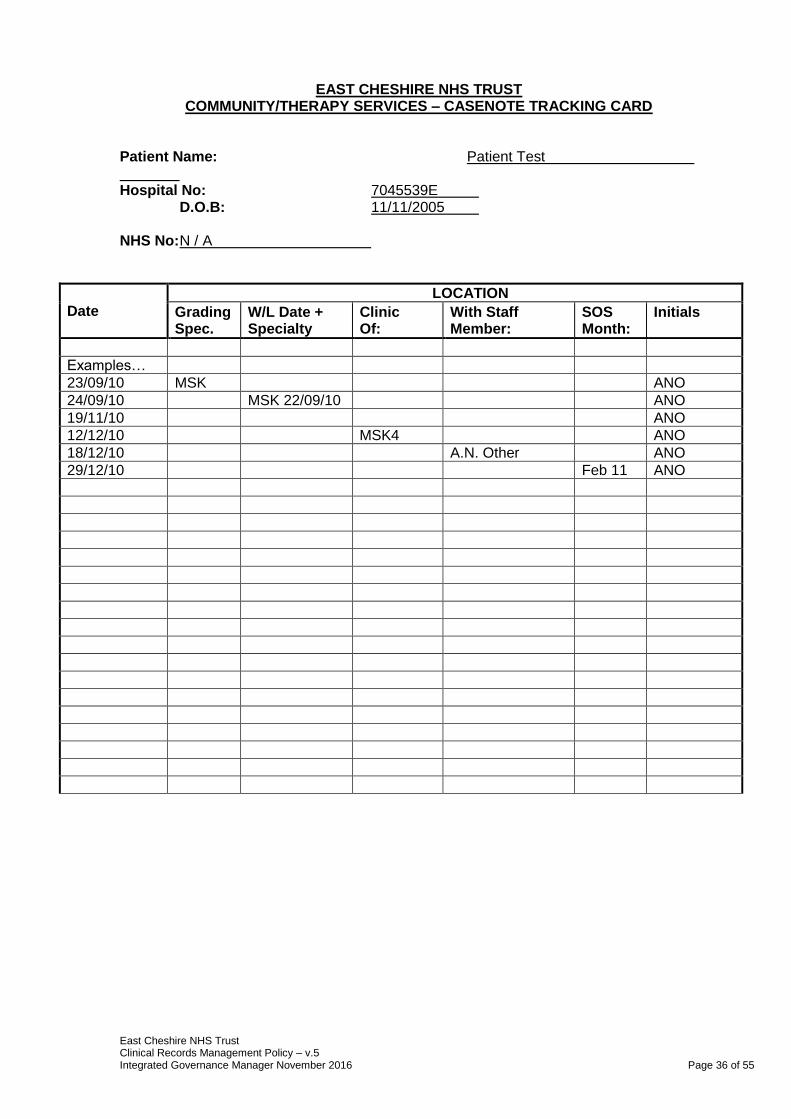
An example completed Casenote Tracking Card can be found below, along with a description of use for each column on the card for reference at the end of this document. Casenote Tracking Card Reference 1. Date
Completed to show the date that the patient casenote was removed from the main file
2. Grading Spec.
Completed to show that the patient casenote has been placed in an admin tray awaiting triage by a Senior Therapist. Mark with an abbreviation to show the speciality of the patient’s problem, e.g. MSK, RHEUM, O.T.
3. W/L Date + Specialty Completed to show that the patient casenote has been triaged by a Senior Therapist and has been placed on an outpatient waiting list. Mark with an abbreviation to show the specialty of the waiting list entry and the date that the patient’s referral was received, e.g. MSK 24/09/10
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 35 of 55
4. Clinic Of:
Completed to show that the record was removed and sent to the gym area for a clinic appointment. Mark with the PAS initials (Doctor Code) of the therapist treating the patient, e.g. MSK4 for Matt Hurst or WMH1 for Ros Hope
5. With Staff Member:
Completed to show that a specific member of staff has removed the casenote for their own review or use. Mark with the full name of the staff member holding the record.
6. SOS Month:
Completed to show that the patient has been placed on a delayed discharge until the end of a specific month, after which they are to be discharged if they suffer no further problems. Mark with the month and year that the patient’s SOS comes to and end, e.g. Oct ’10 or Jan ’11
7. Initials
Mark with the initials of the staff member removing the patient casenote from the main file.
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 36 of 55
EAST CHESHIRE NHS TRUST COMMUNITY/THERAPY SERVICES – CASENOTE TRACKING CARD
Patient Name: Patient Test Hospital No: 7045539E D.O.B: 11/11/2005 NHS No: N / A
Date
LOCATION
Grading Spec.
W/L Date + Specialty
Clinic Of:
With Staff Member:
SOS Month:
Initials
Examples…
23/09/10 MSK ANO
24/09/10 MSK 22/09/10 ANO
19/11/10 ANO
12/12/10 MSK4 ANO
18/12/10 A.N. Other ANO
29/12/10 Feb 11 ANO
East Cheshire NHS Trust Clinical Records Management Policy – v.4 Information Governance Officer – September 2014 Page 37 of 55
Records Storage and Destruction Therapy Services casenotes are kept in the department for a 3 year period post-discharge. After this period the casenotes are transferred to an external archive (Deepstore) for a further number of years, as outlined by the ‘Department of Health Records Management – NHS Codes of Practice – 2nd Edition’. A brief breakdown of these holding periods can be found below. 1. Adult patient’s casenotes are to be held for 8 years prior to destruction 2. Paediatric patient’s casenotes are to be held until the date of their 25th
birthday or 8 years after death 3. Obstetric patient’s casenotes are to be held until the date 25 years after
birth of their last child
Following these dates casenotes are to be destroyed.
Additional Information If Required:
Back up information (if appropriate) Document Change History Roles and Responsibilities Abbreviations References
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 38 of 55
Appendix 6
FILING INSTRUCTIONS
(STRUCTURED CASENOTE)
HEALTH RECORDS
SEPTEMBER 2014
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 39 of 55
GOOD RECORD KEEPING IS ESSENTIAL Records should be filed in accordance with the instructions outlined in this procedure document. Everything written should be in BLACK PEN, dated (including year) and signed legibly. The casenote is designed without a pocket; there is a place for everything within the sections identified. This will make searching within the notes easier and improve efficiency. It is the responsibility of each individual to ensure all documentation is filed appropriately within the casenote before forwarding to any other department or speciality. The casenote complies with Audit Commission guidance. Anita Thorpe Outpatient Administration Manager
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 40 of 55
STRUCTURE OF THE MEDICAL RECORD
INSTRUCTIONS FOR FILING
The structure of the main casenote comprises a cream folder with five cream dividers. There are six coloured dividers representing the following specialities to be used as and when appropriate Surgical 1 - Buff Gen Surg Oncology Urology Surgical 2 - Orange ENT Maxillofacial Ophthalmology Medicine 1 - Green Gen Med Cardiology Respiratory Medicine 2 - Grey Rheumatology Dermatology Haematology Obs/Gynae/Paeds - Blue Gynae Obstetrics Paediatrics SCBU Orthopaedic - Yellow A&E Trauma & Ortho Pain management These colours have been specifically chosen to co-ordinate with the colours of the new consultant header sheets. Each colour has been tested for suitability to photocopy black, blue and red ink for the purposes of litigation. FIRST SPINE: PATIENT ALERT RECORD: Patient Alert Record should always be the first document visible when opening the record. It is clearly identified by a patient identification label and should be used to record any important information including patient wishes and choices. Patient Identification Sheet (PID) The Patient Identification sheet should be filed behind the patient alert record. This provides all relevant information about the patient and previous and ongoing activity within the Trust. Where the patient is under the care of a specialist nurse (i.e. Macmillan nurse a multi-disciplinary case/information sheet will also be inserted. SAFEGUARDING DIVIDER: Documentation/correspondence relating to any safeguarding are to be placed behind this divider. EXCEPTION: The PURPLE FORM used to identify patient not for resuscitation should be filed in this section. When the expiry date has passed it should be scored through and filed behind the patient identification sheet. The forms MUST NOT be destroyed. CLINICAL TRIALS INSERT: This is not a standard insert and is only added if required. This insert sits inbetween the clinical notes divider and correspondence divider
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 41 of 55
Clinical Notes (Divider 1) The separate speciality dividers should be inserted here. They are colour coded and have general headings of MEDICINE, SURGICAL, ORTHOPAEDIC, OBS/GYNAE/PAEDS and include lists of specialities to be filed in that area. Where a typed letter forms part of the clinical note this should also be filed within this section . Any separate letters must be filed in the correspondence section. The clinical notes should be filed within the appropriate speciality in strict chronological order (reading like a book) and headed by a colour coded consultant identification sheet. Care Pathways Where the treatment plan of a patient is subject to a care pathway, all documentation relating to that period of treatment must be stored together throughout the admission. Following discharge, information will be transferred to the relevant section of the case note. Examples of documents to be filed in this section: Operation Notes Anaesthetic Records Consent Form Copy of Casualty Card Letters which form part of Clinical Notes Care Pathways (significant documents will be transferred to the relevant section of the record) Correspondence (Divider 2) (Referral letters, discharge summaries etc) All correspondence should be filed in strict chronological order Examples of documents to be filed in this section: Referral Letters (including Rapid Access proformas Discharge Summaries Letters from other hospitals SECOND SPINE Investigations (Divider 3) All results should be suitably mounted and filed on the appropriate sheet. Full sheet reports should be filed as one document. CTG’s and continuous tracings must be secured in an appropriate envelope, which can be sealed and is easily identifiable. Examples of documents to be filed in this section: ECG’s and Cardiography – (continuous reports will be filed in a plastic wallet EEG’s

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 42 of 55
Audiology Photographs Haematology Biochemistry Microbiology/Cytology/Histology/Serology Radiology CTG’s Drug and Therapies (Divider 4) This section should include any records of contact with therapies when entries are made separately from the clinical notes. All copies of prescriptions, drug cards etc. Examples of documents to be filed in this section: Drug Cards Blood Transfusion Records Anti-coagulant Charts Nursing Records/Charts (Divider 5) To include all nursing cardex and any charts recording details of care ie. Fluid Balance, TPR etc. Examples of documents to be filed in this section: Patient Property Forms Charts – Temperature Blood Pressure Pulse Respiration Urine Fluid Balance Position Electrolytes Typical Example of a Structured Casenotes For a patient referred to Mr Kokan, Out Patient Clinic: Patient Alert Record Patient I.D. Sheet Clinical Notes (Cream divider) Speciality Divider (Surgical 1 – Buff) JSK Header Sheet (Cream paper) Continuation Sheet (White paper) Correspondence (Referral letter) Investigations (Required Mount Sheets) ALERT STICKERS Allergies/Adverse Reactions to Drugs and other Important Information ie safeguarding. Due to its potential confidential nature, all alerts and important information must be recorded on the Patient Alert record on the inside of the case note. All details of allergies/drug reactions etc. should be listed here. Responsibility for completion of this information remains with the clinical staff. Therefore, where secretarial/clerical personnel identify a risk or a patient wishes to document a
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 43 of 55
choice. It MUST be brought to the attention of the Consultant or nominated deputy and the relevant signature obtained. Patients who have previous case notes stored off site ‘Deep stored or microfilmed’ will also have information recorded within the case notes. This information is completed by the Health Records Library case notes will also carry a white sticker alongside the year sticker To alert users of the case note that the patient has a risk or choice, an “ALERT” label should be struck to the front cover. These “Alert” labels are available from the records Library and should be held in all patient areas. Confidential information should not be written on the outside cover of a set of case notes. Please note that these labels MUST NOT be removed and that all subsequent volumes must also be marked accordingly. FOR THE PURPOSE OF INFECTON CONTROL When cases of infection have been resolved the relevant entry in the risk table should be removed or deleted. Authorisation to do this will be given by the Infection Control Team. LABEL STORAGE The small plastic wallet attached to the inside of the back cover is to be used for patient identification labels only. VOLUMISATION OF CASENOTES When multiple volumes of casenotes are required, ALL entries must be written in the current volume to maintain the chronological order of the record. Individual specialties MUST NOT adopt a specific volume, as the casenotes should reflect the overall picture of patient care. It is important that multiple volume case notes are NOT separated. THE MEDICLIP For secure, flexible filing of medical records The Mediclip fastener is recognised as a major innovation in the filing of medical record. It can be incorporated into almost any file or folder. The illustration below shows a medical record file with four tabbed dividers inserted for 4-sectional filing, together with detailed instructions in the use of the Mediclip fitting. This clearly demonstrates how easily papers can be inserted or extracted at any point without disturbing other papers, yet leaving all documentation secure, and in its original order.
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 44 of 55
INSTRUCTIONS IN USE OF THE MEDICLIP FASTENER (I) Illustrates documentation In clamped position when File is not in use. (ii) (iii) Shows clamp released for To insert documents:- Easy viewing of all con- Release clamp as Fig (ii) , open Tents in open position. File to position required, Separate clip, insert or extract Required paperwork, re- connect clip and close clamp (as Fig (i) Simclip In response to a requirement from the commercial market we have developed and are able to offer the Gazerbo Simclip which is similar in style to the Mediclip, performs essentially the same functions, and is more competitively priced. Alternatively see the following page for details of the new, self-adhesive, Easyfix fastener.
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 45 of 55
Appendix 7
NOTIFICATION PATHWAY FOR CHILD DEATHS
CHILD HEALTH COMPUTER DEPARTMENT INFORMED OF DEATH FROM VARIOUS SOURCES:
Maternity Unit / SCBU
A&E Department
Paediatric Ward / Paediatric Consultant
GP
Another Hospital
Social Services/Access Team
Health Visitor
School Nurse
School Health Assistant
Clinic Clerk
Registrar of Births and Deaths (usually a delay)
David Bourne – Senior Mortuary Technician
CHILD HEALTH COMPUTER DEPARTMENT CHECK FOR OUTSTANDING APPOINTMENTS, CLOSE RECORD & SEND NOTIFICATION TO: Secretaries to all Paediatric Consultants
Manager of Maternity Unit / SCBU
Medical Records Library MDGH
GP
Health Visitor
School Nurse
Head Teacher (if relevant)
Clinical Governance – Lead Midwife
Paediatric Liaison Health Visitor
Wendy Moss – New Born Hearing Screener
Safeguarding Children Team
Mel Barker – Named Nurse Acute Trust
Alder Hey Children’s Hospital (babies up to one year old)
CDOP NURSE / SAFEGUARDING TEAM TO NOTIFY: Designated Doctor for Safeguarding Children – Dr K Marinaki / Dr B Singh
Designated Nurse – Moira McGrath
Designated Nurse for Provider Services – Fiona Field / Kath Senior
Specialist Child Death Overview Panel Nurse – Janice Bleasdale
SECRETARIES TO PAEDIATRIC CONSULTANTS TO INFORM OUTSIDE AGENCIES AS APPLICABLE Child health/School Health record to be marked DECEASED clearly across the front of the file. Community record to be tracked on computer system by whoever is currently in possession and record returned to relevant clinic/School Health

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 46 of 55
base. Record to be filed in mainstream filing to follow retention policy as for all child records.
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 47 of 55
Appendix 8 Standard Operating Procedure
Title of Standard Operation Procedure:
Casenote Tracking Following A&E Attendance
Reference Number: SOP/A&E/Sept 14/2 Version No: No. 2
Issue Date: Sept 2014 Review Date: Sept 2016
Purpose and Background
To provide guidance to staff to ensure that information following an A&E attendance is included within the main hospital record.
Scope (i.e. organisational responsibility) Vital functions affected by this procedure:
All staff working in clinical environment/Health Records staff
Monitoring Compliance
Requirement to be monitored. Must include all requirements within NHS LA Standards
Process to be used for monitoring e.g. audit
Responsible individual/ committee for carrying out monitoring
Frequency of monitoring
Responsible individual/ committee for reviewing the results
Responsible individual/ committee for developing action plan
Responsible individual / committee for monitoring action plan
1.7 –
a) duties
b)legal obligations that apply to records
c)how a new record is created
d)how health records are tracked when in current use
e)how health records are retrieved from
Record keeping audit
Information Governance & Records Management Group
Annually Information Governance & Records Management Group
Information Governance & Records Management Group
Information Governance & Records Management Group
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 48 of 55
storage
f)process for retention, disposal and destruction of records
g)how the organisation monitors compliance with all of the above.
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 49 of 55
Escalations (if you require any further clarification regarding this procedure please contact):
Information Governance Officer x 3608
Committees / Group
Date
Consultation: Information Governance & Records
Management Group
Approval Committee
Information Governance & Records
Management Group
Ratified by Committee: Information Governance & Records
Management Group
Received for information:
All staff/Trust Internet
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 50 of 55
Operating Procedure 1. Discharging and Tracking of Case Notes Following A & E Attendance This process ensures the timely filing and discharging of Case Notes following a patient’s admission to the Emergency Department.
Case Notes already in department – File paperwork in clinical section and track notes to relevant secretary.
No Case Notes available - Photocopy CAS cards and Consultant History Sheets. Request case notes file paperwork in clinical notes and send to relevant secretary.
Patient seen by A & E Doctors only – return to previous secretary. 2. Additional steps required prior to filing paperwork and tracking Case
Notes:
Referral request from one specialty to another – fax referral request to relevant secretary with a copy of the CAS Card.
If referral request is written in the CAS card with no other specialty referral or proforma available; a copy of the CAS card would be faxed to the relevant secretary.
Patient transferred from one specialty to another – Track Case Notes and paperwork to last consultant responsible for patient care to the relevant secretary. Check whether patient has been given an appointment for the following day, if so track Case Notes to clinic and arrange notes to be delivered by porter,
DVT patients reports – Case Notes, (if available) and paperwork to be left in DVT tray in main Reception. Track Case Notes, (if available), to Medical Day Case Unit, (MDCU), in comments type ‘For Collection’.
TIA patients fax and forward paperwork FAO Steve – Stroke co-ordinator c/o Ward 11. If no notes available, notes to be requested from tracking location to be sent to stroke co-ordinator Ward 11.
Urology patients transferred to SHH, forward paperwork to Mrs Kujawa’s secretary at MDGH. If no notes available, notes to be requested from tracking location to be sent to the relevant secretary.
Patients with first seizures – forward copy of CAS card and relevant paperwork to Dr P Clough’s secretary. If no notes available, notes to be requested from tracking location to be sent to the relevant secretary.
Pregnant patient’s copy of CAS card and paperwork sent to relevant Obstetrician secretary. Notes are often held with Ante Natal or
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 51 of 55
Obstetrician’s secretary for the duration of the pregnancy. If notes are tracked to another location, notes to be requested from tracking location to be sent to the relevant secretary.
Gynaecology patient’s copy of CAS card and paperwork sent to relevant On Call Gynaecology secretary. If no notes available, notes to be requested from tracking location to be sent to relevant secretary.
Psychiatric patient’s original paperwork stays with the CAS card, including any DSH (deliberate self harm) forms
Back-Up Information Abbreviations: CAS DVT MDCU – Medical Day Case Unit TIA FAO – For the Attention of
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 52 of 55
Equality Analysis (Impact assessment) Please START this assessment BEFORE writing your policy, procedure, proposal, strategy or service so that you can identify any adverse impacts and include action to mitigate these in your finished policy, procedure, proposal, strategy or service. Use it to help you develop fair and equal services. Eg. If there is an impact on Deaf people, then include in the policy how Deaf people will have equal access. 1. What is being assessed?
A definitive policy for the management of clinical records.
Details of person responsible for completing the assessment:
Name: Kathryn Hepplestone
Position: Information Governance Officer
Team/service: Information Governance
State main purpose or aim of the policy, procedure, proposal, strategy or service: (usually the first paragraph of what you are writing. Also include details of legislation, guidance, regulations etc which have shaped or informed the document)
A framework for improving quality, availability and effective use of records and the monitoring processes to effectively maintain records management standards. This policy also includes national guidance from the Royal College of Nursing and Royal College of Physicians in relation to the expected standards for clinical record keeping in the Trust.
2. Consideration of Data and Research To carry out the equality analysis you will need to consider information about the people who use the service and the staff that provide it. Think about the information below – how does this apply to your policy, procedure, proposal, strategy or service 2.1 Give details of RELEVANT information available that gives you an understanding of who will be affected by this document Cheshire East (CE) covers Eastern Cheshire CCG and South Cheshire CCG. Cheshire West & Chester (CWAC) covers Vale Royal CCG and Cheshire West CCG. In 2011, 370,100 people resided in CE and 329,608 people resided in CWAC. Age: East Cheshire and South Cheshire CCG’s serve a predominantly older population than the national average, with 19.3% aged over 65 (71,400 people) and 2.6% aged over 85 (9,700 people). Vale Royal CCGs registered population in general has a younger age profile compared to the CWAC average, with 14% aged over 65 (14,561 people) and 2% aged over 85 (2,111 people). Since the 2001 census the number of over 65s has increased by 26% compared with 20% nationally. The number of over 85s has increased by 35% compared with 24% nationally. Race:
In 2011, 93.6% of CE residents, and 94.7% of CWAC residents were White British
5.1% of CE residents, and 4.9% of CWAC residents were born outside the UK – Poland and India being the most common

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 53 of 55
3% of CE households have members for whom English is not the main language (11,103 people) and 1.2% of CWAC households have no people for whom English is their main language.
Gypsies & travellers – estimated 18,600 in England in 2011. Gender: In 2011, c. 49% of the population in both CE and CWAC were male and 51% female. For CE, the assumption from national figures is that 20 per 100,000 are likely to be transgender and for CWAC 1,500 transgender people will be living in the CWAC area. Disability:
In 2011, 7.9% of the population in CE and 8.7% in CWAC had a long term health problem or disability
In CE, there are c.4500 people aged 65+ with dementia, and c.1430 aged 65+ with dementia in CWAC. 1 in 20 people over 65 has a form of dementia
Over 10 million (c. 1 in 6) people in the UK have a degree of hearing impairment or deafness.
C. 2 million people in the UK have visual impairment, of these around 365,000 are registered as blind or partially sighted.
In CE, it is estimated that around 7000 people have learning disabilities and 6500 people in CWAC.
Mental health – 1 in 4 will have mental health problems at some time in their lives. Sexual Orientation:
CE - In 2011, the lesbian, gay, bisexual and transgender (LGBT) population in CE was estimated at18,700, based on assumptions that 5-7% of the population are likely to be lesbian, gay or bisexual and 20 per 100,000 are likely to be transgender (The Lesbian & Gay Foundation).
CWAC - In 2011, the LGBT population in CWAC is unknown, but in 2010 there were c. 20,000 LGB people in the area and as many as 1,500 transgender people residing in CWAC. Religion/Belief: The proportion of CE people classing themselves as Christian has fallen from 80.3% in 2001 to 68.9% In 2011 and in CWAC a similar picture from 80.7% to 70.1%, the proportion saying they had no religion doubled in both areas from around 11%-22%.
Christian: 68.9% of Cheshire East and 70.1% of Cheshire West & Chester
Sikh: 0.07% of Cheshire East and 0.1% of Cheshire West & Chester
Buddhist: 0.24% of Cheshire East and 0.2% of Cheshire West & Chester
Hindu: 0.36% of Cheshire East and 0.2% of Cheshire West & Chester
Jewish: 0.16% of Cheshire East and 0.1% of Cheshire West & Chester
Muslim: 0.66% of Cheshire East and 0.5% of Cheshire West & Chester
Other: 0.29% of Cheshire East and 0.3% of Cheshire West & Chester
None: 22.69%of Cheshire East and 22.0% of Cheshire West & Chester
Not stated: 6.66% of Cheshire East and 6.5% of Cheshire West & Chester Carers: In 2011, nearly 11% (40,000) of the population in CE are unpaid carers and just over 11% (37,000) of the population in CWAC. 2.2 Evidence of complaints on grounds of discrimination: (Are there any complaints or concerns raised either from patients or staff (grievance) relating to the policy, procedure, proposal, strategy or service or its effects on different groups?)
No
East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 54 of 55
2.3 Does the information gathered from 2.1 – 2.3 indicate any negative impact as a result of this document?
No
3. Assessment of Impact
Now that you have looked at the purpose, etc. of the policy, procedure, proposal, strategy or service (part 1) and looked at the data and research you have (part 2), this section asks you to assess the impact of the policy, procedure, proposal, strategy or service on each of the strands listed below.
RACE:
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, racial groups differently? Yes No Explain your response: This procedure has no impact on different racial groups
GENDER (INCLUDING TRANSGENDER):
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, different gender groups differently? Yes No Explain your response: This procedure has an impact on different gender groups
DISABILITY
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, disabled people differently? Yes No
Explain your response: This procedure may have an impact on members of staff who are suffering from back problems etc. However in these instances no boxes will be lifted and this will be outlined in training sessions.
AGE:
From the evidence available does the policy, procedure, proposal, strategy or service, affect, or have the potential to affect, age groups differently? Yes No Explain your response: This procedure has no impact on different age groups
LESBIAN, GAY, BISEXUAL:
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, lesbian, gay or bisexual groups differently? Yes No Explain your response: This procedure has no impact on lesbian, gay or bisexual groups
RELIGION/BELIEF:
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, religious belief groups differently? Yes No Explain your response: This procedure has no impact on those with different religious beliefs

East Cheshire NHS Trust Clinical Records Management Policy – v.5 Integrated Governance Manager November 2016 Page 55 of 55
CARERS:
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, carers differently? Yes No Explain your response: This procedure has no impact on carers
OTHER: EG Pregnant women, people in civil partnerships, human rights issues.
From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect any other groups differently? Yes No Explain your response: This procedure has no impact on any other groups
4. Safeguarding Assessment - CHILDREN
a. Is there a direct or indirect impact upon children? Yes No
b. If yes please describe the nature and level of the impact (consideration to be given to all children; children in a specific group or area, or individual children. As well as consideration of impact now or in the future; competing / conflicting impact between different groups of children and young people:
c. If no please describe why there is considered to be no impact / significant impact on children This procedure has no impact on children
5. Relevant consultation Having identified key groups, how have you consulted with them to find out their views and that the made sure that the policy, procedure, proposal, strategy or service will affect them in the way that you intend? Have you spoken to staff groups, charities, national organisations etc?
No
6. Date completed: 5.12.16 Review Date: November 2018 7. Any actions identified: Have you identified any work which you will need to do in the future to ensure that the document has no adverse impact?
Action Lead Date to be Achieved
N/A
8. Approval – At this point, you should forward the template to the Trust Equality and Diversity Lead [email protected]
Approved by Trust Equality and Diversity Lead: Date: 5 December 2016