clinical proof-of-concept of an anti- cd47 agent for the ... · this presentation may contain...
TRANSCRIPT

Clinical Proof-of-Concept of an Anti-CD47 Agent for the Treatment of CTCL:Data from Phase 1 Trials of TTI-621 Employing both Intravenous and Intralesional Routes of Administration
Yaping Shou, MD, PhD
Chief Medical Officer, Trillium Therapeutics
T-Cell Lymphoma Forum 2019: Industry Innovation

This presentation may contain forward-looking statements, which reflect Trillium's current expectationregarding future events. These forward-looking statements involve risks and uncertainties that may causeactual results, events or developments to be materially different from any future results, events ordevelopments expressed or implied by such forward-looking statements. Such factors include, but are notlimited to, Trillium's ability to obtain financing to advance the products in its development portfolio; changingmarket conditions; the successful and timely completion of pre-clinical and clinical studies; the establishmentof corporate alliances; the impact of competitive products and pricing; new product development risks;uncertainties related to the regulatory approval process or the ability to obtain drug product in sufficientquantity or at standards acceptable to health regulatory authorities to complete clinical trials or to meetcommercial demand; and other risks detailed from time to time in Trillium's ongoing quarterly and annualreporting. Forward-looking statements are made only as of the date of this presentation and except as requiredby applicable securities laws, Trillium undertakes no obligation to publicly update or revise any forward-lookingstatements, whether as a result of new information, future events or otherwise.
2

CD47 – An Innate Checkpoint that Inhibits Macrophage Phagocytosis
• CD47 is a widely expressed glycoprotein that delivers a “DO NOT EAT” signal to macrophages through SIRPα
• Binding of CD47 to SIRPα inhibits macrophage cytoskeletal activity and in turn phagocytosis
• Tumor cells frequently exploit the CD47-SIRPαaxis to evade immune surveillance by macrophages
• Many hematologic and solid tumors express high levels of CD47
• High CD47 expression often correlates with aggressive disease and poor clinical outcomes
3

Checkpoint Inhibition Against CD47 May Present Therapeutic Potential For T-Cell Lymphoma
4
Anti-CD47 Ab induces longer survival in transformed CTCL PDX (DFTL 22685)
Anti-CD47 mAb efficacy is macrophage and not neutrophil dependent in a TCL PDX model
S Jain, et al, Blood 2018 132:339
High CD47 expression in Sézary Cells
Akilov et al. 2017 EORTC CLTF
CD47 levels correlated to survival of patients with Sézary Syndrome

TTI-621: A Dual Function SIRPαFc Decoy Receptor that Blocks CD47 and Delivers an Activating Signal
5
Blocks the CD47 DO NOT EAT signal
Delivers an EATsignal through FcγRs
MacrophagePhagocytosis
Antigen Presentation & Adaptive Immunity

TTI-621 IgG1 Fc delivers a potent “eat” signal
6
CD47 Blocker* (Company) Isotype
TTI-621 (Trillium) IgG1
TTI-622 (Trillium) IgG4
Hu5F9 (Forty Seven) IgG4
CC-90002 (Celgene) IgG4
SRF231 (Surface Oncology) IgG4
ALX148 (ALX Oncology) Inert IgG1
Petrova et al. Clin. Cancer Res. 2017
*Clinical stage compounds
Advantages of an IgG1 Fc:• Maximizes potency by delivering an activating signal to
macrophages through Fc receptors• Higher likelihood of monotherapy activity - not dependent
upon a combination with another IgG1 antibody• Could be used to treat tumors where no anti-cancer
antibody is available

TTI-621 Does Not Bind Human RBCs
7
Petrova et al. Clin. Cancer Res. 2017
CD47 is associated with the Rh Ag complexand anchored to the cytoskeleton in RBCs TTI-621 does not bind human RBCs TTI-621 does not agglutinate human RBCs
Salomao et al. PNAS 2008
Why does TTI-621 not bind RBCs?• Moderate binding affinity – need bivalent interaction• Lack of CD47 mobility in the RBC membrane prevents
clustering and limits bivalent binding
Advantages of non-RBC binding:• Minimizes likelihood of anemia• Avoids drug removal by the “antigen sink”• Avoids interference with transfusion medicine testing

Intravenous Administration Study (TTI-621-01)
8
Multicenter, open-label phase 1 study in patients with relapsed/refractory hematologic malignancies (NCT02663518)
Dose Escalation(0.05, 0.1, 0.2, 0.3 mg/kg)
MonotherapyIndications
Identified initial MTD(0.2 mg/kg) based on
conservative DLT criteria
Lymphoma
0.2 mg/kg (mono)0.1 mg/kg (combo)
Heme Malignancies
CD20+ NHL (Rituximab)cHL (Nivolumab)
0.2 to 0.5 mg/kg(Dose Ramp-up)
CTCL, PTCL
Dosing
CombinationIndications
OngoingSimon’s 2-stage Design
Dose Intensification at Investigator Discretion Made Permissible per
Protocol Amendment
Dose Escalation Initial Expansion Focused Expansion

Intravenous TTI-621 is Well Tolerated
9
• Most frequent AEs were low-grade infusion reactions, clinically managed by pre-medication and close monitoring
• ≥ Grade 3 thrombocytopenia occurred in 18% patients
• Diverse patient population from the following expansion cohorts: AML, MDS, MPN, B-NHL, T-NHL, HL, MM, CLL, SCLC
Based on Snapshot data, Nov. 26, 2018
Cohort(s): All Total
Grade 1-2 Grade ≥3 n=179
Infusion Related Reaction 69 (39) 3 (2) 72 (40)
≥ 15% Thrombocytopenia 11 (6) 33 (18) 44 (25)
Chills 34 (19) 34 (19)
Fatigue 27 (15) 27 (15)
Nausea 21 (12) 21 (12)
≥ 5% Anaemia 8 (4) 12 (7) 20 (11)
Pyrexia 18 (10) 18 (10)
Diarrhoea 16 (9) 1 (1) 17 (9)
Vomiting 14 (8) 1 (1) 15 (8)
Neutropenia 13 (7) 13 (7)
Headache 13 (7) 13 (7)
Hypotension 7 (4) 2 (1) 9 (5)
Source: 28 Nov 2018 DDLs
Related Adverse Events
n(%)
Adverse Event
Grades
0 25 50 75 100
AE Reports (%)
Gr 1-2
Grade ≥3

Transient Thrombocytopenia Not Associated with Increased Risk of Bleeding
10
Median Platelet Levels in All Subjects During Week 1 (N=179)
Pre-dose Platelet Levels in All Subjects Over 12 Weeks (N=179)
Bleeding Adverse Events in All Subjects (N=179)
Based on Snapshot data, Nov. 26, 2018
0
25
50
75
100
125
150
175
200
0 1 2 3 4 5 6 7 8
Pla
tele
ts (
x10
9/L
)
Day
183 168 181 166 159 161 169 177 161 181 173 167
0 (0) 3 (2) 4 (3) 8 (6) 5 (4) 7 (7) 5 (5) 4 (5) 3 (4) 2 (3) 1 (2) 3 (6)
0
50
100
150
200
250
300
1 2 3 4 5 6 7 8 9 10 11 12
Pla
tele
ts (
x 1
09/L
)
Week
Median
Gr 4 n(%)
Min
Median
75%
25% • Thrombocytopenia is likely an on-target effect resulting from CD47 blockade and the TTI-621 IgG1 Fc
• Thrombocytopenia is reversible within a week• Pre-dose platelet levels remain relatively stable over the course
of the study• Transient platelet decreases did not lead to an increased risk of
bleeding• Platelet decreases did not impact drug delivery – 1/179 patients
had dosing discontinued due to thrombocytopenia
All and Related Bleeding Adverse Eventsn (%)
Adverse Event Severity
Totaln=179
Grade 1 Grade 2 Grade 3
All Related All Related All Related
Any Bleeding Adverse Event 18 (10) 9 (5) 3 (2) 0 4 (2) 3 (2) 24 (13)
Epistaxis 9 (5) 5 (3) 2 (1) 2 (1) 11 (6)
Gastrointestinal haemorrhage 2 (1) 1 (1) 2 (1)
Haematuria 1 (1) 1 (1) 1 (1)
Haemorrhage 1 (1) 1 (1) 1 (1)
Menorrhagia 1 (1) 1 (1) 1 (1)
Purpura 1 (1) 1 (1) 1 (1)Unrelated Grade 1 events in 1 patient, each: Anal haemorrhage, Haematochezia, Haematoma, Haemoptysis, Periorbital haematoma, Petechiae, Rectal haemorrhage; Unrelated Grade 2 events in 1 Patient, each: Ecchymosis, Thrombotic thrombocytopenic purpura, Vaginal haemorrhage

Dose Intensification is Well Tolerated
11
• Dose intensification at Investigator’s discretion allowed per protocol; later standardized in Amendment 8 (Ramp up from 0.2 to 0.5 mg/kg within 5 weeks)
• Included in this analysis were 22 patients dose intensified; 15 dose intensified to 0.5 mg/kg between Week 5-30.
• No worsening of post-dose platelet decrease was observed at 0.5 mg/kg
• No apparent differences in other AEs were seen between patients receiving stable dose of 0.2 mg/kg and patients dose intensified on study
Pre-Post Dose Pre Post Pre Post
Visit (mg/kg) Week 1 (0.2) Weeks 5-30 (0.5)
Patients (n) 22 22 15 15
0
100
200
300
400
500
600
Plt
(x1
09/L
)
Pre- and Post-Dose Platelets
Investigator Discretion (ID) Amendment 8 (A8) N
Median Plts 244 131 234 188
Pre-Post Dose Pre Post Pre Post
Patients (n) 22 22 15 15
Visit (mg/kg) Wk (0.2) Wks 5-30 (0.5)
0
100
200
300
400
Pla
tele
ts (
x 1
09 /
L)
Min
Median
75% Quartile
25% Quartile
Visit (mg/kg) Wk 1 (0.2) Wks 5-30 (0.5)
Pre-Post Dose Pre Post Pre Post
Patients (n) 22 22 15 15
0
20
40
60
80
100
Pat
ien
ts (
%) Grade 4
Grade 3
Grade 2
Grade 1
Grade 0
Pre- and Post-Dose Platelet Counts
Based on Snapshot Data, Nov. 26, 2018

IV TTI-621 Has Single Agent Activity in T-Cell Lymphoma Patients
12
• Monotherapy ORR by the data cut: 17% in MF, 20% SS, and 18% in PTCL
• 5/7 responses observed in patients receiving weekly doses of 0.2 mg/kg
• One Sezary patient achieved CR after 48 weeks of study treatment, showing the possibility of a slow response to the study drug.
Based on Snapshot data, Dec. 26, 2018
TTI-621-01: T-Cell
LymphomaN
Response
n(%)
Objective Response (days)
med (range)
CR PR Total Time to Response Treatment Duration
Mycosis Fungoides 24 --- 4 (17) 4 (17) 49 (23-51) 103 (47-281)
Sezary Syndrome 5 1 (20) --- 1 (20) 336 (336-336) 387 (387-387)
Peripheral TCL 11 --- 2 (18) 2 (18) 50 (20-79) 314 (127-500)
Total / Overall 40 1 (3) 6 (15) 7 (18) 50 (20-336) 135 (47-500)
Ongoing →
Ongoing →
Ongoing →
Ongoing →
Ongoing →
0 90 180 270 360 450 540
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
MF
Sezary
Sezary
Sezary
Sezary
Sezary
PTCL
PTCL
PTCL
PTCL
PTCL
PTCL
PTCL
PTCL
PTCL
PTCL
PTCL
CT
CL
Pe
riph
era
l T
CL
Days
TTI-621-01: T-Cell Lymphoma (n= 40)
CR PR SD PD NA

Intratumoral Administration Study (TTI-621-02)
Multicenter, open-label phase 1 study of direct intratumoral injection of TTI-621 in patients with relapsed/refractory mycosis fungoides (MF) or percutaneously accessible solid tumors (NCT02890368)
13
*10 mg 3x/wk for 2 wks then 10 mg weekly
^Combinations: IFN-α, anti-PD-1/PD-L1, T-vec (melanoma only), radiation (plasmacytoma only)
Single injection(1, 3 or 10 mg)
Multiple Injection(10 mg 3x/wkfor 1 or 2 wks)
Induction*+ continuation
(monotherapy or combinations^)
Dose Expansion
• Advantages of direct injection:• Obtain very high local drug
concentrations
• Avoid systemic antigen sink
• Rapid responsesDose Escalation

Intralesional TTI-621 Injections Were Well Tolerated in CTCL Patients
• Related adverse events (AEs) all Grade 1 or 2; no Grade ≥3 AEs
• Common related AEs include chills, injection site pain, and fatigue
• No related serious adverse events or dose-limiting toxicity
14Querfeld et al. ASH 2018
Related Adverse Eventsn (%)
Grade Total*1-2 ≥ 3 (N=27)
Any Adverse Event 19 (70) 0 19 (70)
Chills 8 (30) 0 8 (30)
Injection site pain 8 (30) 0 8 (30)
Fatigue 6 (22) 0 6 (22)
Erythema 3 (11) 0 3 (11)
Nausea 3 (11) 0 3 (11)
Diarrhea 2 (7) 0 2 (7)
Headache 2 (7) 0 2 (7)
Myalgia 2 (7) 0 2 (7)
Pyrexia 2 (7) 0 2 (7)
* TEAEs in 1 subject, each: arthralgia, decreased appetite, dizziness, flatulence, flushing, hyperhidrosis, inflammation, influenza like illness, insomnia, local swelling, mycosis fungoides lesional swelling, neutrophil count increased, edema, pain, palpitations, penile swelling, pruritus, pruritus generalised, thrombocytopenia, uncoded, white blood cell count increased.
0 25 50 75Patients (%) Grade 1-2 AEs

CAILS Reductions in Injected Lesions Were Observed in the Majority of Patients
15
*Composite Assessment of Index Lesion Severity, a measure of local lesion responses
6* 6 7* 1 4 6 9* 5* 1 6 1 5* 3 1 6* 6 10* 1 6 1 14* 12*
IB IIB IA IIB IIB IIB IIB IB IVB IB IIB IIB IIA IVA IA IIB IIB IIB IIB IA IA IIB
†
-100
-50
0
50
CA
ILS
Ch
ange
(%
) fr
om
Bas
elin
e 1 mg 3 mg 10 mg
Injections
Stage
† received TTI-621 + PEG-IFN-α2a
* injections across up to 3 lesions
CAILS scores were available in 22patients:• 20 (91%) patients had decreased
CAILS scores.
• 9 (41%) patients had a reductionin CAILS scores by ≥ 50%.
• CAILS score reductions occurredat all dose levels, following singleand multiple injections, in allstages (IA to IVB), and in all lesiontypes (plaques, tumors, etc.).
15Querfeld et al. ASH 2018
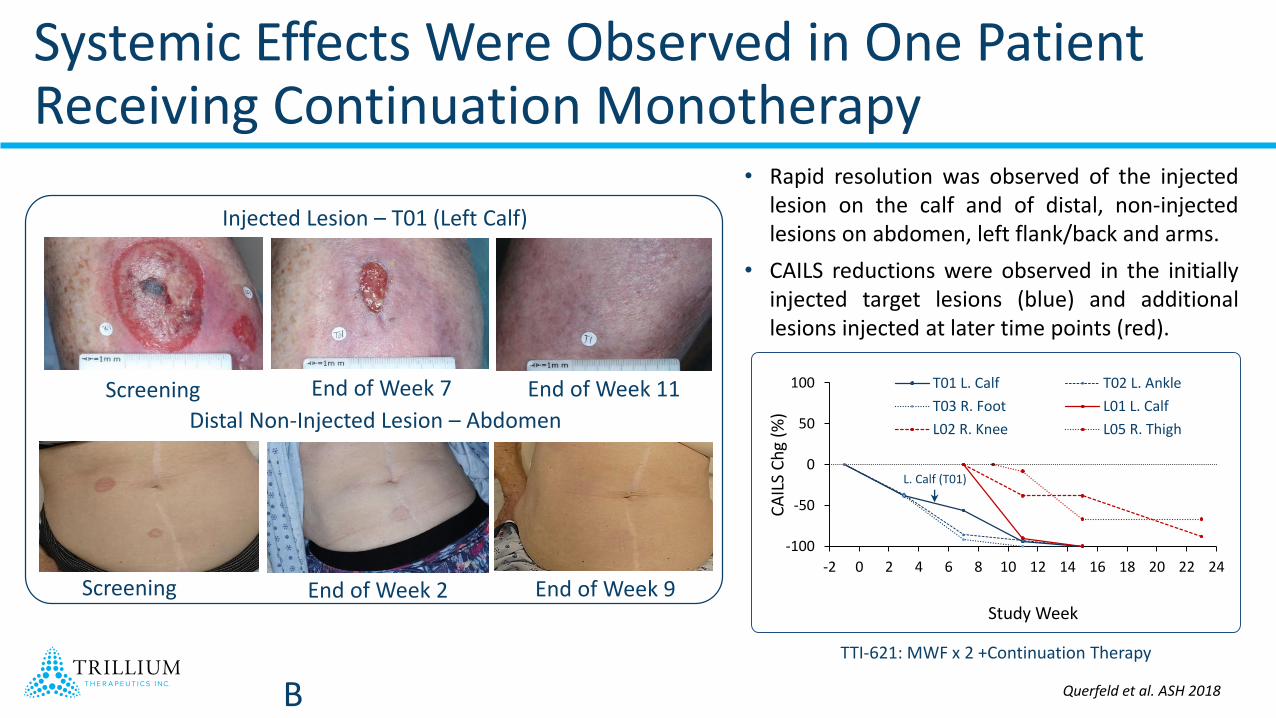
Systemic Effects Were Observed in One Patient Receiving Continuation Monotherapy
TTI-621: MWF x 2 +Continuation Therapy
Screening End of Week 2 End of Week 9
Distal Non-Injected Lesion – Abdomen
Injected Lesion – T01 (Left Calf)
Screening End of Week 7 End of Week 11
B
-100
-50
0
50
100
-2 0 2 4 6 8 10 12 14 16 18 20 22 24
CA
ILS
Ch
g (%
)
Study Week
T01 L. Calf T02 L. Ankle
T03 R. Foot L01 L. Calf
L02 R. Knee L05 R. Thigh
L. Calf (T01)
• Rapid resolution was observed of the injectedlesion on the calf and of distal, non-injectedlesions on abdomen, left flank/back and arms.
• CAILS reductions were observed in the initiallyinjected target lesions (blue) and additionallesions injected at later time points (red).
Querfeld et al. ASH 2018

Local-Regional Responses Were Observed in Non-Injected, Adjacent Control Lesions
17
All CAILS scores: Injected vs Non-Injected Control Lesions
Querfeld et al. ASH 2018
• 9 patients with reduced CAILS had a paired CAILS assessments in an adjacent non-injected lesion
• Injected lesion CAILS decreased -6% to -95% in all patients
• Non-injected lesions CAILS decreased -12% to -67% in 7/9 patients
• Median distance between paired injected and non-injected lesions is estimated to be 5.3 cm (range 0.2 – 15+ cm)
Non-Injected Control Lesions
Injected Target Lesions
-100
-50
0
50
100
CA
ILS
Ch
g (%
)
-100
-50
0
50
100
-13 -6 1 8 15 22 29 36 43 50 57 64 71 78
CA
ILS
Ch
g (%
)
Study Day

Peripheral Responses Were Observed Following Local Injections
18
Screening Day 8
P r e - T r e a t m e n t D a y 8
0
5 0 0
1 0 0 0
1 5 0 0
C D 4 :C D 8
CD
4:C
D8
Screening Day 8Screening Day 8
Single 1 mg Injection Single 1 mg Injection Single 3 mg Injection
P r e - T r e a t m e n t D a y 3 D a y 8
0
5
1 0
1 5
2 0
2 5
S e z a r y C e ll C o u n t
V
9+
of
CD
4+
(%
)
P r e - T r e a t m e n t D a y 8
0
1 0
2 0
3 0
4 0
5 0
6 0
C D 4 :C D 8
CD
4:C
D8
Querfeld et al. EORTC CLTF 2018

Summary
• TTI-621 is a novel dual function decoy receptor that blocks the CD47 “do not eat” signal and delivers an activating signal through FcRs
• TTI-621 is differentiated from other CD47 blocking agents by its potent IgG1 Fc and lack of RBC binding
• Intratumoral delivery of TTI-621 has been shown to be well tolerated and results in responses in injected and non-injected MF lesions
• Intravenous TTI-621 is well tolerated, activity observed as a single agent in CTCL, PTCL and DLBCL (Not shown) patients and in combination with rituximab in DLBCL patients (not shown) at relatively low doses; dose intensification ongoing
• Clinical POC of TTI-621 has been demonstrated for the treatment of CTCL from IV and IL drug delivery route
• Clinical program is moving forward in three distinct areas:
• Intratumoral mono- and combination-therapy in CTCL
• IV monotherapy in both CTCL and PTCL
• IV combination therapy in B-cell lymphoma
19

Acknowledgements
• Patients and their families
• Staff members who contributed to the TTI-621 clinical studies:• BC Cancer Agency• City of Hope• Cleveland Clinic• Colorado Blood Cancer Institute• Columbia University• Hackensack University Medical Center• Mayo Clinic – Rochester• Mayo Clinic - Jacksonville• Memorial Sloan Kettering Cancer Center• New York University• Oregon Heath & Sciences University• Princess Margaret Hospital• Seattle Cancer Care Alliance• Stanford University• Tennessee Oncology• University of Pittsburg
20

Trillium Therapeutics Inc. (NASDAQ/TSX:TRIL) is an immuno-oncology company dedicated to the discovery &development of novel and innovative cancer therapies

CAILS Responses Occurred Rapidly Within the 2-Week Induction Period
22Querfeld et al. ASH 2018
-100
-75
-50
-25
0
25
CA
ILS
Ch
g (%
) Single Injection, Single Lesion Cohort 1 (1 mg, n=2)
Cohort 2 (3 mg, n=1)
Cohort 3 (10 mg, n=3)Induction Period Single
-100
-75
-50
-25
0
25
CA
ILS
Ch
g (%
) Multiple Injections, Single Lesion Cohort 4 (10 mg, n=1) Cohort 5 (10 mg, n=5) Cohort 6 (10 mg, n=1)Induction
Period MWF x1 (4)
-100
-75
-50
-25
0
25
-13 1 15 29 43 57 71 85 99 113 127
CA
ILS
Ch
g (%
)
Study Day
Multiple Injections, Multiple Lesions Cohort 7 (10 mg, n=3)
Induction Period
Rapid and sustained reductions in CAILS scores were observed following both single and multiple injections in patients who only received induction therapy of ≤2 weeks