clinical pathways in emergency medicine
TRANSCRIPT

Clinical Pathways in Emergency Medicine
Suresh S. David Editor
Volume I
123

Clinical Pathways in Emergency Medicine


Suresh S. David Editor
Clinical Pathways in Emergency Medicine
Volume I
ISBN 978-81-322-2708-3 ISBN 978-81-322-2710-6 (eBook) DOI 10.1007/978-81-322-2710-6
Library of Congress Control Number: 2016931333
© Springer India 2016 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifi cally the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfi lms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. The use of general descriptive names, registered names, trademarks, service marks, etc. in this publication does not imply, even in the absence of a specifi c statement, that such names are exempt from the relevant protective laws and regulations and therefore free for general use. The publisher, the authors and the editors are safe to assume that the advice and information in this book are believed to be true and accurate at the date of publication. Neither the publisher nor the authors or the editors give a warranty, express or implied, with respect to the material contained herein or for any errors or omissions that may have been made.
Printed on acid-free paper
This Springer imprint is published by Springer Nature The registered company is Springer (India) Pvt. Ltd
Editor Suresh S. David , MBBS, MS, FRCP, FACEM, MPhil, PhD Pushpagiri Medical College Hospital Thiruvalla Kerala India
v
Pref ace
In the history of humankind, Medicine has never been more exciting and challenging than in the twenty-fi rst century. One of the great challenges of being a contemporary academic clinician is to fi nd ways to correlate pertinent Basic Sciences to clinical appli-cation, at the bedside. When I set out to prepare Clinical Pathways in Emergency Medicine , it evoked a thought for contemplation. ‘Do we need one more book in the specialty of Emergency Medicine?’ That helped to harness an unprecedented approach: from the perspective of a nascent, yet inquisitive emergency physician who is keen to understand the rationale of occurrence, manifestation, and management of acute clinical conditions. And this book differs signifi cantly by providing an algorithm at the end of each chapter, which, at a glance, provides a roadmap for the journey ahead.
Clinical Pathways in Emergency Medicine is an international congregation of contribu-tors, who have offered their expertise which has immensely fl avored the global approach to Emergency Medicine. The authors include a remarkable blend of colleagues, friends, former students, and new stars on the horizon of Emergency Medicine. A multi-author manuscript of this nature cannot be delivered without the dedication exhibited by them. In addition to being luminaries from around the globe, they are among the most progressive clinicians in various sub-specialties of Emergency Medicine. And I could not have wished for a better bunch of Section Editors, who superbly orchestrated the creation and revision of manuscripts. Each one of them is an enviable embodiment of clinical excellence.
Sound clinical experience, coupled with knowledge, based on authoritative books and peer-reviewed publications, remains the foundation, on which clinical management needs to be built. In my three decades of clinical practice, I have been humbled multiple times, by the way in which anecdotal experience and written literature is fl outed by the human body.
Today’s dogma becomes tomorrow’s heresy. Clinical Pathways in Emergency Medicine is a compendium of contemporary evidence-based knowledge. However, no book remains perfect and a shrewd clinician knows very well that the practice of medi-cine, based out of a book, has its own limitations. Nevertheless, I am optimistic that this edition of the book would facilitate satiation to the hunger for knowledge among increasing numbers of aspirants in the fi eld of Emergency Medicine.
Pushpagiri Medical College Hospital, Prof. Suresh S. DavidKerala, India


vii
Contents
Part I Resuscitation Section Editor: Raja Sekhar Maroju
1 Airway Management in ED . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 Venugopalan Poovathumparambil
2 Anaphylaxis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19 Rosie Furse
3 Cardiopulmonary Resuscitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31 Raja Sekhar Maroju
4 End of Life Care in the Emergency Department . . . . . . . . . . . . . . . . . . 45 Arti Baskaran
5 Fluid Resuscitation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57 Jonathan Leung and Derek Hicks
6 Post-cardiac Arrest Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73 Neal Durge and Chris Solomonides
7 Vascular Access . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 83 Mir Saaduddin Ahmad
Part II Cardiology Section Editor: Suresh S. David
8 Acute Cardiac Arrhythmias . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101 Rachel Gnanaprakasam and Suresh S. David
9 Acute Coronary Syndromes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 117 George Koshy and Raja Sekhar Maroju

viii
10 Heart Failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 129 Lakshay Chanana
11 Hypertensive Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 139 Ashish Nandy and Sanjukta Dutta
Part III Critical Care Section Editor: John Victor Peter
12 Acid-Base Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 155 Kishore Pichamuthu
13 Acute Respiratory Failure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167 John Victor Peter
14 Hypotension and Shock . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 179 John Victor Peter and Mathew Pulicken
15 Mechanical Ventilation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 191 Shivakumar S. Iyer and Jignesh Shah
16 Severe Sepsis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 207 Suhel Al-Soufi and Vineet Nayyar
Part IV Respiratory System Section Editor: Dhakshinamoorthy Vijayasankar
17 Acute Shortness of Breath . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 221 Seema O. Brij , Paul Bambrough , and D. Vijayasankar
18 Bronchial Asthma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 235 G. Krishna Prasad , Prakash E. George , and Jebu A. Thomas
19 Chronic Obstructive Pulmonary Disease (COPD) . . . . . . . . . . . . . . . . 245 Seema O. Brij , Sumit Chatterji , and Malcolm Marquette
20 Pulmonary Embolism . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 259 Dhakshinamoorthy Vijayasankar
Part V Environmental Medicine Section Editor: Jaybalan Allan Matthew
21 Accidental Hypothermia and Cold Injury . . . . . . . . . . . . . . . . . . . . . . 271 Seelan Pillay
22 Altitude Medicine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 285 Jaybalan Allan Matthew
23 Electrical Injuries . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297 Roshen Maharaj
Contents
ix
24 Heat-Related Illnesses . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 307 Ruvendra D. Shah
25 Submersion and Diving-Related Illnesses . . . . . . . . . . . . . . . . . . . . . . . 315 Jaybalan Allan Matthew
Part VI Gastrointestinal System Section Editor: Suresh S. David
26 Abdominal Pain . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 329 Harshil Mehta
27 Acute Pancreatitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 347 Ajay Kumar Mishra
28 Gastrointestinal Bleeding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 357 Sridhakshini Sathasivam
29 Intestinal Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 363 Dhavapalani Alagappan and Sathya Kaliannan
30 Jaundice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 375 Praveen Eadala
Part VII General Medicine and Allied Specialties Section Editor: Suresh S. David
31 Acute Thyroid and Adrenal Disorders . . . . . . . . . . . . . . . . . . . . . . . . . 387 P. E. Rama Subrahmanyam
32 Biomarkers in Emergency Medicine . . . . . . . . . . . . . . . . . . . . . . . . . . . 405 Anoop T. Chakrapani
33 Bleeding and Coagulation Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . 417 Rebecca Mathews and Reeba Mary Issac
34 Blood Transfusion Reactions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 429 Sajit Varghese
35 Dermatological Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 437 S. Senthilkumaran
36 Diabetic Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 457 Sandeep Balanrao Gore
37 Febrile Neutropaenia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 473 N.V. Maheshwari
38 Geriatric Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 485 Sethu Babu
Contents
x
39 Near Hanging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 497 T. V. Ramakrishnan
40 Oncological Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 503 Sameer Rathi
41 Pituitary and Parathyroid Disorders . . . . . . . . . . . . . . . . . . . . . . . . . . 513 Anoop James George and Suresh S. David
Part VIII Infectious Diseases Section Editor: Babu Urumese Palatty
42 Acute Fever of Indeterminate Cause . . . . . . . . . . . . . . . . . . . . . . . . . . . 529 Shashiraj Eswarappa and Babu Urumese Palatty
43 Dengue . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 539 Parvinder K. Chawla
44 Dog Bite . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 549 Suresh S. David
45 Emerging Respiratory Pandemics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 557 Seema Oommen
46 Food Poisoning . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 567 P. C. Rajeev and Jerry Johny
47 HIV-Related Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 577 Menon Sachin Venugopal and Vivek Gopinath
48 Malaria . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 591 Menon Sachin Venugopal and B. L. Harikrishnan
49 Standard Precautions Against Biohazardous Diseases . . . . . . . . . . . . 601 Sandeep Nathanael David
50 Varicella and Herpes Zoster Infections . . . . . . . . . . . . . . . . . . . . . . . . . 609 Binod Basheer and Salish Varghese
Part IX Nephrology Section Editor: Gopal Basu
51 Acute Kidney Injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 621 Sreejith Parameswaran
52 Electrolyte Imbalance: Potassium, Magnesium, Calcium and Phosphorous . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 637 Jacob K. Addo
Contents
xi
53 Electrolyte Imbalance: Sodium and Water . . . . . . . . . . . . . . . . . . . . . . 651 Gopal Basu
54 Emergencies of End-Stage Renal Disease and Kidney Transplantation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 669 Sishir Gang
Part X Neurology Section Editor: Shakuntala Murty
55 Altered Mental Status . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 681 Shakuntala Murty
56 Dizziness and Syncope . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 693 Girish Narayan
57 Headache . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 703 Thomas Mathew and Sagar Badachi
58 Neurosurgical Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 715 Ruth-Mary deSouza and Tony Elias
59 Seizures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 733 Raghunandan Nadig
60 Stroke . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 747 Praveen Kumar B. Gowder
Part XI Obstertics and Gynaecology Section Editor: Suresh S. David
61 Abnormal Uterine Bleeding . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 767 Devendra Naik
62 Assessment of Sexual Assault . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 775 Shweta Tyagi
63 First and Second Trimester Emergencies . . . . . . . . . . . . . . . . . . . . . . . 781 Rachel Gnanaprakasam
64 Gynaecological Infections . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 797 Benita Florence
65 Third Trimester Emergencies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 809 Suresh S. David and Harshil Mehta
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 823
Contents
Part I Resuscitation

3© Springer India 2016 S.S. David (ed.), Clinical Pathways in Emergency Medicine: Volume I, DOI 10.1007/978-81-322-2710-6_1
Chapter 1 Airway Management in ED
Venugopalan Poovathumparambil
Introduction
• Airway management is considered a core responsibility of emergency physicians as airway assessment and management is the fi rst step in the management of any acutely unwell patient.
• Patients in extremis requiring resuscitation often have a compromised airway, usually due to decreased consciousness.
• Prompt airway management followed by adequate ventilation mitigates second-ary hypoxic damage to the brain and other vital organs.
Key Points • Hypoxia secondary to poorly managed airway leads to increased morbidity
and mortality. • Assess the patient to determine the type of airway intervention needed
based on the set of circumstances and presentation. • It is important to be conversant in the use of various anaesthetic agents. • Avoid hypoxaemia or hypercarbia while preparing or while intubating the
patient. • Always have a backup plan in case of a failed airway. It is important to be
conversant with the airway algorithms and also have the correct equipment available.
V. Poovathumparambil , DA, DNB, MNAMS, MEM [GWU] Aster DM Healthcare , Ernakulam , India e-mail: [email protected]

4
• Rapid sequence intubation is a key skill for any physician working in an emer-gency department.
• Mismanagement of the airway can lead to catastrophic and often devastating consequences for both the patient and the providers caring for them [ 1 ].
Signs and Symptoms of a Potential Airway Problem
A conscious patient who is able to speak is deemed to have a patent airway.
Threatened Airway
• Loud noisy breathing • Accessory muscles supported respiration • Abdominal muscle using expiration
Airway Management
Basic Airway Management
• Clear airway of any secretions and look for foreign bodies. • Head tilt and chin lift (not in trauma). • Jaw thrust (in trauma cases).
To continue patency of airway that is amenable to basic airway manoeuvres, one of the two basic airway adjuncts can be used.
• Oropharyngeal airway (OPA)
– The size an OPA by measuring the length from the angle of the mouth to the tragus of the ear. Stand at the head end of the patient. Open the mouth and insert gently behind the tongue. In adults, insert the OPA with the concave side facing the palate. Once the tip reaches the posterior end of the hard pal-ate, turn the OPA to have the concave surface in line with the tongue. Gently push it in until it sits comfortably on the tongue. Never force the OPA. It is not indicated if the patient is gagging on the airway. Alternatively, use tongue depressor or laryngoscope blade for OPA insertion. Tolerance of an OPA indi-cates loss of gag refl ex and becomes an indication for defi nitive airway management
• Nasopharyngeal airway (NPA)
– NPA is useful in patients who are not tolerating OPA. Size an NPA by measur-ing the distance between the tip of the nose to the tragus. Approximate the diameter of the NPA to the patient’s nostrils. Lubricate the NPA adequately
V. Poovathumparambil
5
and insert by facing the bevel to the septum in order to avoid turbinate injury. Assess patency of the nose and any signs of fracture to the base of the skull (like CSF leak, Battle sign, Raccoon eye). Basal skull or midfacial fractures are only relative contraindications, and an NPA can still be used albeit with caution.
Endotracheal Intubation
It is extremely important to assess the airway prior to intubation. LEMON is a use-ful mnemonic to perform this assessment which can predict a diffi cult airway:
(i) L – Look externally (ii) E – Examine 3-3-2 (iii) M – Mallampati score (iv) O – Obstructions (v) N – Neck mobility
In an emergency, where a patient has not been prepared for anaesthetic, airway can be secured with some safety by performing a rapid sequence induction (RSI) for intubation.
Seven Ps of Intubation
1. Preparation 2. Preoxygenation 3. Premedication 4. Paralysis with sedation 5. Protection and positioning 6. Placement of tube and confi rmation 7. Post-intubation care
There are three axes, oral axis, pharyngeal axis and laryngeal axis, to consider for positioning of the patient during intubation Fig. 1.1 .
Ideally, these three axes should be aligned. In neutral supine position, these axes are in different directions. Recently, one of the most popular methods to improve the chances of successful airway management is called the ‘ramp’ posi-tion. This position is to align the auditory canal with the sternum in a straight line. This ‘ramp’ position has been studied and validated as one of the most important steps in enhancing the chances of successful airway management [ 2 ]. The most common mistake made during intubation is ‘cranking back’ on the laryngoscope handle to lever the top of the blade to provide better visibility. This manoeuvre may improve glottic visualisation; however, it restricts the operator’s ability to
1 Airway Management in ED

6
manipulate the tube by limiting the size of the oral opening and also jeopardises the teeth.
Check the following equipment for their availability and functioning before intubation :
• Suction, oxygen, BVM device and transportable ventilator • Airway adjuncts – appropriately sized OPA and NPA
Paralysing agents facilitate intubation and are benefi cial in :
1. Tight heads (head injury, ↑ ICP) 2. Tight hearts (CAD, vascular heart disease) 3. Tight lung (bronchial asthma, hyperreactive airway, COPD) 4. Tight vessels (HTN, coarctation of the aorta)
Fig. 1.1 Patient head position for intubation
V. Poovathumparambil

7
• Appropriately sized supraglottic airway devices (SGD) like laryngeal mask air-way (LMA0 or iGel)
• Laryngoscope with appropriate blade available and light source checked
• Spare laryngoscope handle • Appropriately sized ETT: cuff checked plus a size above and below • Stylet/bougie • Monitors including EtCO 2 monitor • Drugs
– Sedatives/anaesthetics – etomidate, midazolam, fentanyl, propofol, thiopen-tone and ketamine
– Paralytics – suxamethonium, pancuronium, vecuronium, atracurium and rocuronium
• Others – atropine, lignocaine, preservative free spray 4 % or 10 %, Lubricant
It is important to wear proper personal protection equipment like gloves, plastic apron and visors. Ideally, three assistants are required in performing an RSI: one person for managing the airway, second person for applying cricoid pressure and third person for drug administration. For crash intubation, even one assistant is acceptable.
Preoxygenation
This can be achieved by using BVM device with 100 % O 2 for 3–5 min or by 100 % O 2 through eight vital capacity breaths.
Premedication
This is best remembered by the mnemonic LOAD:
• L: Lignocaine 1–1.5 mg/kg • O: Opioid – Fentanyl 3 mcg/kg • A: Atropine 0.02 mg/kg • D: Defasciculating agents [1/8th of intubating dose of non-depolarising muscle
relaxants prior to suxamethonium will reduce the fasciculations]
Induction and paralytic agents Agents used to sedate and obtund refl exes prior to paralysis and intubation are called ‘induction’ agents – midazolam, fentanyl, propo-fol, etomidate, ketamine, thiopentone, etc. are agents currently available (Tables 1.1 , 1.2 and 1.3 ).
Suxamethonium is one of the best paralytic agents for emergency intubation. Rocuronium is another paralytic agent that gives equal intubating condition but within just 60 s and without any adverse effects of suxamethonium.
1 Airway Management in ED

8
Table 1.1 Sedative induction agents
Agent Dose Induction Duration Benefi ts Caveats
Thiopental 3–5 mg/kg IV
30–60 s 10–30 min ↓ ICP ↓ BP
Methohexital 1 mg/kg IV <1 min 5–7 min ↓ ICP short duration
BP seizure, laryngospasm
Ketamine 1–2 mg/kg IV
1 min 5 min Bronchodilator, ‘dissociative’ amnesia
↑ Secretions, ↑ ICP emergence phenomenon
Etomidate 0.3 mg/kg IV
<1 min 10–20 min ↓ ICP Myoclonic excitation, vomiting, no analgesia
↓ IOP, neutral BP
Propofol 0.5–1.5 mg/kg IV
20–40 s 8–15 min Antiemetic, anticonvulsant
Apnea, ↓ BP, no analgesia
↓ ICP Fentanyl 3–8 μg/kg
IV 1–2 min 20–30 min Reversible
analgesia, neutral BP
Highly variable dose ICP: variable effects, chest wall rigidity
Table 1.2 Succinylcholine
Adult dose 1.0–1.5 mg/kg Onset 45–60 s Duration 5–9 min Benefi ts Rapid onset, short duration Complications Bradyarrhythmias
Masseter spasm Increased intragastric, intraocular and possibly intracranial pressure Malignant hyperthermia Hyperkalaemia Prolonged apnea with pseudocholinesterase defi ciency Fasciculation-induced musculoskeletal trauma Histamine release Cardiac arrest
Table 1.3 Non-depolarising muscle relaxants
Agent Adult intubating IV dose Onset Duration Complications
Vecuronium (intermediate/long)
0.08–0.15 mg/kg 2–4 min 25–40 min Prolonged recovery time in obese or elderly or if there is hepatorenal dysfunction
0.15–0.28 mg/kg (high-dose protocol)
60–120 min
Rocuronium (intermediate/long)
0.6 mg/kg 1–3 min 30–45 min Tachycardia
Atracurium (intermediate)
0.4–0.5 mg/kg 2–3 min 25–45 min Hypotension Histamine release Bronchospasm
V. Poovathumparambil
9
Intubation
Proper laryngoscope technique is essential for successful placement of endotracheal tube (ETT). Failure to intubate is usually due to wrong or poor technique. One of the more common mistakes made during laryngoscopy is of not having adequate control of the tongue. Human tendency is to tilt the laryngoscope blade forward. It results in not only damaging the incisors but also decreasing the chances of having an unobstructed view of the larynx.
• Straight blades : The tip should extend underneath the epiglottis and lift it. • Curved blades : The tip should extend into the vallecula with the action of
upward movement on the hyoepiglottic ligament exposing the glottic opening.
Optimal External Laryngeal Manipulation (OELM)
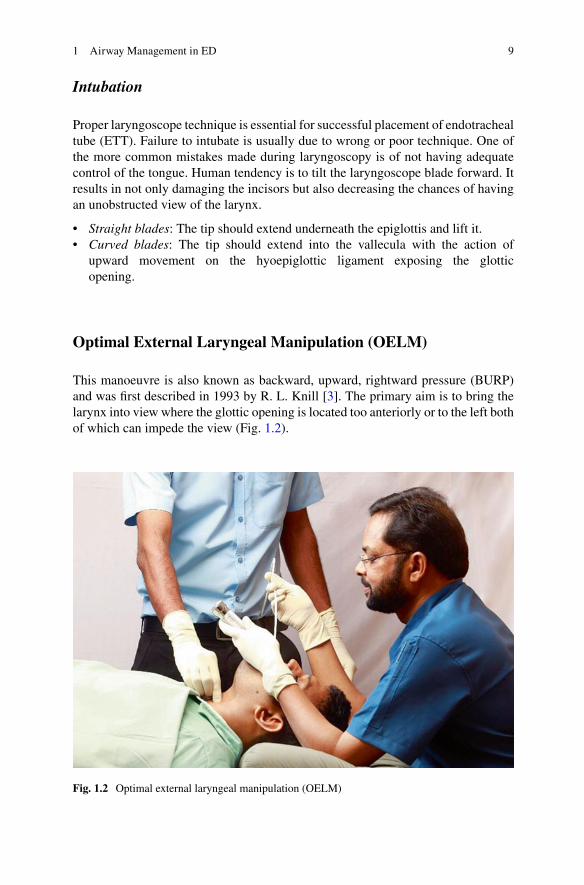
This manoeuvre is also known as backward, upward, rightward pressure (BURP) and was fi rst described in 1993 by R. L. Knill [ 3 ]. The primary aim is to bring the larynx into view where the glottic opening is located too anteriorly or to the left both of which can impede the view (Fig. 1.2 ).
Fig. 1.2 Optimal external laryngeal manipulation (OELM)
1 Airway Management in ED
10
Two methods have been described:
1. The assistant should know the principle and place pressure on the thyroid carti-lage (upwards and to the right).
2. The person performing the laryngoscopy should guide the assistant into the opti-mal direction and with a degree of pressure that yields the best glottic view.
It is important to note that BURP manoeuvre is not the same as cricoid pressure. Cricoid pressure is applied usually during RSI, where the patient has not been fasted prior to intubation. The usefulness of cricoid pressure during intubation is question-able [ 4 ].
Cricoid Pressure
Cricoid pressure is a direct posterior pressure applied over the cricoid ring, by which the oesophagus will be occluded between the cricoid cartilage and vertebral column to prevent regurgitation and aspiration of gastric contents.
Confi rmation of Tube Position
Confi rmation of a properly placed tube is as important as intubation. A wrongly placed tube in the oesophagus will kill the patient within minutes. An endobronchial intubation will cause hypoxia and contralateral lung collapse.
Primary Confi rmation of Tube
1. Intubation under direct vision 2. Chest movement 3. Five-point auscultation 4. Bag compliance 5. Fogging in the tube
All primary confi rmation methods are not absolute and sometimes misleading.
Secondary Confi rmations
1. ETCO 2 – All intubations should be confi rmed by ETCO 2 . This is now considered as a gold standard.
V. Poovathumparambil

11
2. X-ray chest – Though this cannot rule out oesophageal intubation, it helps con-fi rm endobronchial intubation.
3. SPO 2 – This is useful to detect misplaced tube in the late phase only. 4. Oesophageal tube detection device [EDD] – This helps to rule out oesophageal
tube placement. 5. Ultrasound – This modality can also be used to help confi rm correct tube
placement. 6. Fibre-optic laryngoscopy and bronchoscopy – These are absolute ways to con-
fi rm tube position.
Post-intubation Care
Once the correct tube placement is confi rmed, secure the tube to prevent tube migra-tion or accidental extubation. The most common method is with adhesive tape; however, in individuals who have excessive secretions or have full beards, a circum-ferential tape around the neck has been recommended. Various products available commercially that combine the features of adhesive and nonadhesive methods are available. If the patient is in a hard C-collar, tie ETT over the collar. Manually ven-tilate patient to achieve EtCO 2 of 35–40 mmHg. Give post-intubation sedation for tube tolerance as required. Continue comprehensive monitoring including ETCO 2 .
Plan B
If plan A fails, rapidly move to alternate plans. Plan B must be a diffi cult airway plan.
Diffi cult Airway
Diffi cult airway is not just synonymous with diffi culty with laryngoscopy and endo-tracheal intubation but rather is a continuum of degrees of diffi culty with:
Standard timeline for rapid sequence intubation
T – 10 min Prepare T – 5 min Preoxygenate T – 3 min Pretreat T = 0 Paralysis with induction T + 30 s Protection T + 45 s Placement T + 90 s Post-intubation management
1 Airway Management in ED

12
• Bag mask ventilation (BMV) • Conventional direct laryngoscopy/intubation (DL) • Video laryngoscopy Intubation • Supraglottic airway placement • Surgical (invasive) airway access.
The diffi culty may be provider dependent, situation dependent, patient depen-dent, equipment and/or device dependent or a combination of these factors.
The ‘ can’t ventilate and can’t intubate ’ situation is the most diffi cult and disas-trous in airway management.
Can’t Ventilate Situation: Plan B
• Change BMV unit. • Use OPA and NPA. • Use two-hand ventilation. • Use two-person ventilation technique. • Use gauze around the mouth – useful in oedematous patient. • Use two pillows or remove pillow. • Use ramp position.
Can’t Intubate: Plan B
• Use BURP. • Release cricoids. • Release C-collar and change to manual in-line stabilisation. • Use two pillows, no pillow or pillow under the shoulder. • Use ramp position and align external auditory canal and sternal angle in the same line. • Change laryngoscope blade to the next size. • Change Macintosh to Miller blade or use McCoy laryngoscope blade. • Use SGD, Combitube or King’s airway. • Use stylet- or bougie-assisted intubation. • Use video laryngoscope.
Always do call for expert help . Switch to plan C.
Plan C
Urgent surgical airway:
• Needle cricothyrotomy • Surgical cricothyrotomy
V. Poovathumparambil

13
Anticipated Diffi culty
• Call expert help. • Awake intubation under local anaesthesia. • Blind nasal intubation. • Retrograde intubation. • Fibre-optic laryngoscopy. • Surgical airway – tracheostomy.
Yes
No
Yes
No
Yes
No No
Yes
No
Needs intubation
Unresponsive ?Near death?
Predict difficultAirway ?
RSI
AttemptIntubation
Successful?
Failure to maintainOxygenation?
≥ 3 attempts at OTI by Experienced operator?
Crash Airway
Difficult Airway
From DifficultAirway
Post intubation management
Failed Airway
MAIN EMERGENCY AIRWAY ALGORITHM
1 Airway Management in ED

14
Yes Fails
No
Yes Fails
No
Fails
UnresponsiveUnreactive
Near Death?
Crash Airway
Algorithm
DifficultAirway?
DifficultAirway
Algorithm
FailedAirway
Algorithm
RSI
UNIVERSAL EMERGENCY AIRWAY ALGORITHM
V. Poovathumparambil
15
Yes
No
Yes
No
Yes
No
Yes
No
No
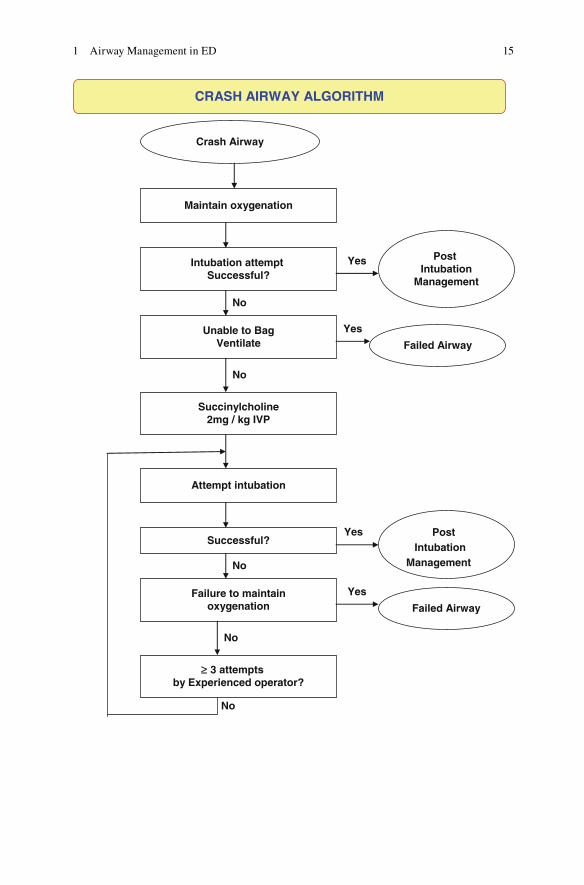
CRASH AIRWAY ALGORITHM
Crash Airway
Maintain oxygenation
Intubation attempt Successful?
Unable to BagVentilate
Succinylcholine2mg / kg IVP
Attempt intubation
Successful?
Failure to maintainoxygenation
Post Intubation
Management
Failed Airway
Post Intubation
Management
Failed Airway
3 attempts by Experienced operator?
£
1 Airway Management in ED

16
Yes
No
Yes Yes
Yes
Difficult AirwayPredicted
Call for assistance
Failure to maintainOxygenation?
BMV or EDG Predicted to be
successful?
Awake DL, FO orVL Successful?
ILMOFO or VL
CricothyrotomyBNTI
Lighted stylet
DIFFICULT AIRWAY ALGORITHM
Failed Airway
Intubation PredictedTo be successful?
RSI
Post intubationManagement or
RSI
Go to mainAlgorithm
V. Poovathumparambil
17
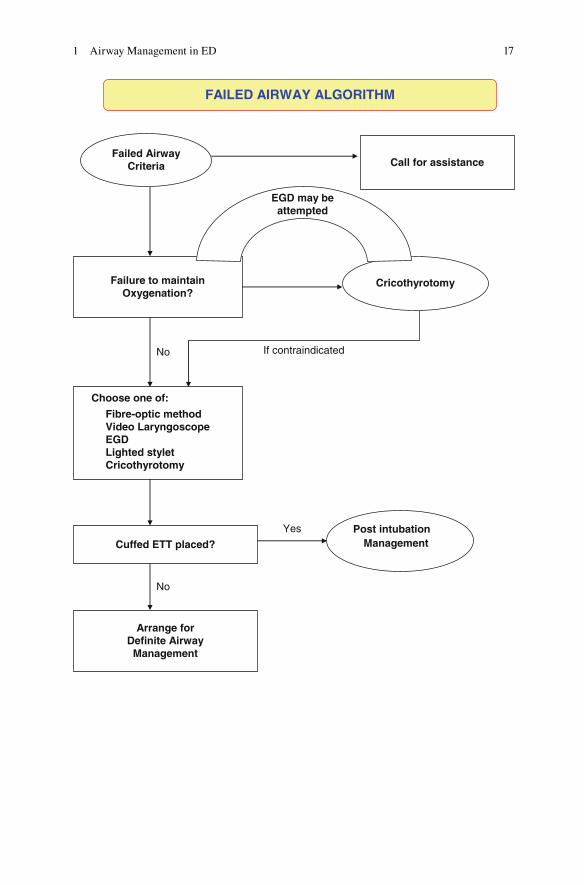
If contraindicatedNo
Yes
No
FAILED AIRWAY ALGORITHM
Failed AirwayCriteria Call for assistance
Failure to maintainOxygenation?
Cricothyrotomy
EGD may beattempted
Choose one of:
Fibre-optic methodVideo LaryngoscopeEGDLighted styletCricothyrotomy
Cuffed ETT placed?
Arrange forDefinite Airway
Management
Post intubation Management
1 Airway Management in ED

18
References
1. Urdaneta F. Emergency airway management airway workshop: January 2009. http://felipeair-way.sites.medinfo.ufl .edu .
2. Rao SL, et al. Laryngoscopy and tracheal intubation in the head- elevated position in obese patients: a randomized, controlled. Equivalence Trial Anesth Analg. 2008;107(6):1912–8.
3. Knill RL. Diffi cult laryngoscopy made easy with a “BURP”. Can J Anaesth. 1993;40(3):279–82.
4. Bhatia N, Bhagat H, Sen I. Cricoid pressure: where do we stand? J Anaesthesiol Clin Pharmacol. 2014;30(1):3–6.
V. Poovathumparambil

19© Springer India 2016 S.S. David (ed.), Clinical Pathways in Emergency Medicine: Volume I, DOI 10.1007/978-81-322-2710-6_2
Chapter 2 Anaphylaxis
Rosie Furse
Introduction
• Anaphylaxis is a severe, potentially life-threatening, generalised, hypersensitiv-ity reaction that is characterised by a rapid onset of airway and/or breathing and/or circulatory problems usually associated with skin or mucosal changes [ 1 ]. These occur in response to exposure to a precipitant (e.g. food, insect venom, drugs or exercise) and can be either allergic (IgE mediated) or non-allergic.
• Irrespective of this underlying pathophysiology, the clinical features, investiga-tions and acute treatment are the same, and all of these patients should be given a diagnosis of ‘anaphylaxis’ or ‘suspected anaphylaxis’. Terms such as ‘anaphy-lactoid’ or ‘severe allergic reaction’ are confusing and should be avoided.
Key Points 1. Anaphylaxis is a generalised reaction. However, its effect on skin and
mucosal changes, hypotension and respiratory compromise are noteworthy.
2. The mainstay of treatment is intramuscular epinephrine plus intravenous fl uids if hypotensive. All other drug interventions are secondary measures.
3. Detailed history is the key for diagnosis. 4. Serial mast cell tryptase levels will be helpful to the allergy specialist at
follow-up.
R. Furse , MBBS, MRCP, FCEM Department of Emergency Medicine , Royal United Hospital , Bath BA1 3NG , UK e-mail: [email protected]