clinical effectiveness of implant-supported removable ...cune.nl/index_bestanden/grossman et al...
TRANSCRIPT

Rstaf
m
H
m
s
I
r
U
S
I
D
t
©
0
d
J Oral Maxillofac Surg67:1941-1946, 2009
Clinical Effectiveness ofImplant-Supported Removable Partial
Dentures—A Review of the Literature andRetrospective Case EvaluationYoav Grossmann, DMD, MsHA,* Joseph Nissan, DMD,† and
Liran Levin, DMD‡
Purpose: To review the published data on the treatment outcomes of restoring the partially edentulouspatient with implant-supported removable partial dentures (ISRPDs) and describe the concept of ISRPDsand the clinical guidelines for placing implants for ISRPDs, and evaluate case series results.
Materials and Methods: For the review, a literature search was performed using the PubMed andOvid databases. Reports in English from 1969 to 2008 were considered. Also, 35 patients have had theirdentition restored with ISRPDs supported by 67 implants. These patients were evaluated in terms ofimplant and teeth survival.
Results: The data from the published reports and the presented case series suggest that the incorpo-ration of dental implants into removable partial dentures could be an optional treatment plan for thepartially edentulous patient to improve function and patient satisfaction.
Conclusions: ISRPDs provide patients with stable, long-term predictable prostheses. This treatmentalternative should be considered whenever fixed restorations are not a valid option. Strict maintenanceand a follow-up protocol are recommended to obtain satisfactory results. Longitudinal clinical studies arerequired for evaluation of ISRPDs.© 2009 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 67:1941-1946, 2009aoptttlr
tctoolceNctcat
emovable partial dentures (RPDs) are still exten-ively used for restoration of partially edentulous pa-ients. However, these prostheses have been associ-ted with poor patient acceptance, compromisedunction and esthetics, and an increased risk of caries
*Senior Prosthodontist, Maxillofacial Prosthetics Service, Depart-
ent of Oral and Maxillofacial Surgery, Sheba Medical Center, Tel
ashomer, Israel.
†Senior Lecturer, Director of Implant Prosthodontics, Depart-
ent of Oral Rehabilitation, The Maurice and Gabriela Gold-
chleger School of Dental Medicine, Tel Aviv University, Tel Aviv,
srael.
‡Clinical Instructor, Department of Oral Rehabilitation, The Mau-
ice and Gabriela Goldschleger School of Dental Medicine, Tel Aviv
niversity, Tel Aviv, Israel; and Department of Periodontology,
chool of Graduate Dentistry, Rambam Health Care Campus, Haifa,
srael.
Address correspondence and reprint requests to Dr Grossmann:
epartment of Oral and Maxillofacial Surgery, Sheba Medical Cen-
er, Tel Hashomer, Israel; e-mail: [email protected]
2009 American Association of Oral and Maxillofacial Surgeons
278-2391/09/6709-0023$36.00/0
Roi:10.1016/j.joms.2009.04.081
1941
nd periodontal disease.1-4 Therefore, it is the mutualbjective of the clinician and patient to restore theartially missing dentition with a fixed restorationhat exhibits better longevity.5 Implant-supported res-orations have become a predictable treatment modalityo obtain this desirable treatment outcome.6-8 Neverthe-ess, for various reasons, fixed implant-supported resto-ations might not be prescribed.
The treatment goals of restoring the partially eden-ulous patient with an RPD are to improve the masti-atory function and esthetics and to restore the pos-erior occlusal support and vertical dimension ofcclusion, all without compromising the patient’sral health. However, studies have shown that the
ong-term use of RPDs results in an increased risk ofaries, residual ridge resorption, and periodontitis,specially in patients with poor oral hygiene.1,2,9-11
o evidence has shown that the prosthesis per seauses the damage.9 Moreover, it has been reportedhat RPD wearers are more dissatisfied with their oralonditions than patients without a partial denture12
nd that RPDs are more inconvenient.12,13 In addi-ion, elderly patients were more satisfied with their
PD only when it added a significant number of
oapi
Rad(c
M
tffwca
R
vwiw
wsiRitrscttTiittupor
timM
PIhphiIei
gtptGI
aipiaathYsdaatemsmotu
etpum3
c(mmi(maw
1942 CLINICAL EFFECTIVENESS OF IMPLANT-SUPPORTED REMOVABLE DENTURES
cclusal units to their dentition.13 Clinicians shouldlso be aware that a significant proportion of RPDsrescribed for these patients are not used, especially
n Kennedy Class II patients.12
The combination of dental implants to support thePD might alleviate some of these problems associ-ted with conventional RPDs. The present reportescribes the concept of implant-supported RPDsISRPDs), the indications for their use, and thelinical parameters that dictate implant location.
aterials and Methods
For the review, a data search was performed usinghe PubMed and Ovid databases. Reports in Englishrom 1969 to 2008 were considered. Also, the datarom 35 patients who had had their dentition restoredith ISRPDs supported by 67 implants at 2 medical
enters were reviewed. Those patients were evalu-ted in terms of implant and teeth survival.
esults
Overall, from 1969 to 2008, the data search re-ealed 10 reports on ISRPDs. Most of the publicationsere single case reports.5,14-18 Two publications were
n vitro studies assessing the ISRPD design,19,20 and 3ere retrospective clinical studies.21-23
In a retrospective study,21 10 patients were treatedith unilateral and bilateral mandibular distal-exten-
ion RPDs supported by 16 posterior implants. Themplants were used alone as vertical stops to enhancePD support or with resilient retentive elements. The
nvestigators showed consistently increased satisfac-ion in all patients, minimal component wear, noadiographic evidence of excessive bone loss, andtable peri-implant soft tissues after at least 1 year oflinical follow-up. In another study, 15 partially eden-ulous patients with an unfavorable number and dis-ribution of abutments were treated with ISRPDs.22
he partially edentulous arch configuration was mod-fied by placing 33 implants into strategic sites. Themplant survival rate was 100%, with only minor pros-hetic complications and significantly improved pa-ient satisfaction. In a retrospective study of implantssed to restore the dentition of partially edentulousatients with ISRPD, an overall implant survival ratef 95.5% was reported during a mean follow-up pe-iod of 31 months.23
CASE EVALUATION
The study sample included 35 consecutivelyreated patients (26 men and 9 women; mean age atmplant placement 55.3 years, range 33 to 67) at 2
edical centers (Tel Aviv University School of Dental
edicine, Tel Aviv, Israel, and the Department of irosthodontics, Sheba Medical Center, Tel Hashomer,srael). The study subjects were partially edentulous,ad lost more than 5 teeth in either arch, and had norevious denture wearing experience. A smokingabit was reported by 12 patients (34.3%). Only med-
cally healthy patients who had been treated with anSRPD were included in the present study. No otherxclusion criteria were applied. All patients signed annformed consent statement.
All patients were examined clinically and radio-raphically before implant placement. Patients werereated with a 2-stage surgical procedure with im-lants from 3 different manufacturers (Zimmer Den-al, Carlsbad, CA; 3i Implant Innovations, Palm Beachardens, FL; and MIS Implants Technologies, Shlomi,
srael).In addition to the implants, teeth were selected as
butments to provide support for the ISRPDs accord-ng to their pulpal and periodontal condition, theresence and type of coronal restoration, the need for
ndirect retention, and the distribution and number ofbutments and implants in the arch. Guiding planesnd rest seats preparations were performed afterreatment planning and cast survey. All prosthesesad a rigid chromium-cobalt alloy (Dentorium, Nework, NY) major connector. The implants providedupport only using healing caps or retention withifferent resilient attachments, such as the Locatorttachment (Locator, Zest, Escondido, CA), the O-ringttachment (Zimmer Dental), or a bar and clip. Pa-ients were assessed 1 week postoperatively afterach surgical stage and at regular follow-up appoint-ents after prosthesis insertion. An implant was con-
idered a failure if it was removed because of clinicalobility; if it showed evidence of peri-implant radi-
lucency and/or persistent pain, discomfort, or infec-ion that was attributable to the implant; or if it wasnrestorable.24
A total of 67 implants were placed in 35 partiallydentulous patients who received ISRPDs from 1996o 2007. Overall, 35 ISRPDs were placed. Maxillaryrostheses were provided to 14 patients and mandib-lar prostheses to 21 patients. The postimplant place-ent follow-up period was 9 to 120 months (mean
5.4).Before implant placement, the most prevalent arch
onfiguration was Kennedy Class II in the mandible10 patients) followed by Kennedy Class I in theandible (8 patients) and Kennedy Class I in theaxilla (7 patients). The arch configuration was mod-
fied by implant placement in 18 patients (51.4%)Table 1). Of the 67 implants, 39 were placed in theandible (18 in the anterior area, 5 in the premolar
rea, and 16 in the posterior area), and 28 implantsere placed in the maxilla (9 in the anterior area, 13
n the premolar area, and 6 in the posterior area).

rfsport
D
erauai
cf
flt
bmtsttffpposnmonpibol
cltam
1
GS
M
M
GS
Ff
GS
GROSSMANN, NISSAN, AND LEVIN 1943
Overall, 2 (2.9%) of the 67 inserted implants failed,esulting in a crude rate for implant survival of 97.1%or the present study. Both failures occurred in theame patient. This patient was a heavy smoker withre-existing periodontal disease. During follow-up,nly 1 abutment tooth was lost. All other abutmentsemained functional without need for retreatment athe last follow-up visit.
iscussion
Implants are used to improve the RPD support,nhance retention and stability, preserve the residualidge underneath the denture base, reduce the stresspplied on the abutment teeth, eliminate the need fornesthetic clasp assemblies, and modify unfavorablerch configurations. Most of the available data onmplant-tissue supported RPD or ISRPD is from clini-
Table 2. CLINICAL GUIDELINES FOR ISRPD
1. Place implants in area of second molars in distalextension patients
2. Place implants adjacent to distal abutment in casefuture fixed restoration is an option, distal abutmentsare poor, or patient is concerned about clasp showing
3. Place implants medially in Kennedy Class IV arch4. Use short or narrow-body implants if necessary5. Use resilient attachments on the implants6. Design a simple RPD; use rest seats and guiding plates
similar to conventional RPD7. Use rigid major connector design for maxillary arch8. Minimize mandibular lingual flange if difficult for
patient to adjust9. Incorporate retentive elements to denture base under
functional load0. Schedule patient for checkups and maintenance
appointments
Table 1. ARCH CONFIGURATIONS ACCORDING TOKENNEDY CLASSIFICATION BEFORE AND AFTERIMPLANT PLACEMENT
Arch ConfigurationBefore
Arch Configuration After
Class I Class II Class III
axillaClass I 3 4Class II 3Class III 3Class IV 1andibleClass I 3 5Class II 4 6Class III 1Class IV 2
rossmann, Nissan, and Levin. Clinical Effectiveness of Implant-upported Removable Dentures. J Oral Maxillofac Surg 2009.
firossmann, Nissan, and Levin. Clinical Effectiveness of Implant-upported Removable Dentures. J Oral Maxillofac Surg 2009.
al reports describing the use of posterior implantsor distal-extension RPDs.14-18
From our review of the published data, the keyactors to be considered when designing an ISRPD areisted in Table 2 and discussed in the following sec-ions.
KENNEDY CLASS I TISSUE ISRPD
The Kennedy Class I partially edentulous arch hasilateral distal extensions. The functional load is trans-itted to the teeth and the soft tissue. Implant loca-
ion depends primarily on the dimensions of the re-idual ridge and the biomechanical considerations ofhe RPD design. Two distally positioned implants inhe area of the second molars would effectively trans-orm the Kennedy Class I configuration to a moreavorable Kennedy Class III. Theoretically, the im-lants should be located as distally as possible torovide maximal support and stability (Fig 1). This isf special importance in the mandible because of theignificant displacement of the denture base that isot supported by the major connector. The implantsight be used for support only using healing caps
r for retention with resilient attachments con-ected to the implants. A low-profile attachment isreferred to decrease the off-load forces to the
mplants. Endodontically treated abutments woulde specifically beneficial when used for supportnly without direct retainers applying unfavorable
ateral displacing forces.25
However, an inadequate posterior ridge dimensionould restrict implant placement to a more anteriorocation, distally to the existing abutments. In addi-ion, the clinician should be aware that implant ther-py is versatile and that, in the future, the patientight select to restore the edentulous ridges with
IGURE 1. Kennedy Class I mandibular arch modified to moreavorable Kennedy Class III arch with 2 implants.
rossmann, Nissan, and Levin. Clinical Effectiveness of Implant-upported Removable Dentures. J Oral Maxillofac Surg 2009.
xed implant-supported restorations. In this case also,
tcdpts
awjmfw
wKtca
eplpTm
amitltKd
FiOp
GS
FbiwauR
GS
1944 CLINICAL EFFECTIVENESS OF IMPLANT-SUPPORTED REMOVABLE DENTURES
he implants should be located more medially, adja-ent to the existing abutments, to allow future prostho-ontic use (Fig 2). Moreover, when implants arelaced adjacent to the distal abutments, the unes-hetic retentive clasp on the distal abutments could bepared.
KENNEDY CLASS II TISSUE ISRPD
The Kennedy Class II partially edentulous arch hasunilateral distal extension. An ISRPD should be usedhen the tooth loss is extensive (Fig 3). Otherwise,
ust as when only the molars are missing, the patientight not use the prosthesis. When the patient has no
unctional problem, a shortened dental arch concept,ith no prosthesis, should be considered.26,27
Placing a single implant in the posterior regionould modify the Kennedy Class II configuration to aennedy Class III and increase the stability and reten-
ion of the prosthesis. The same considerations dis-ussed for the Kennedy Class I tissue ISRPD alsopply.
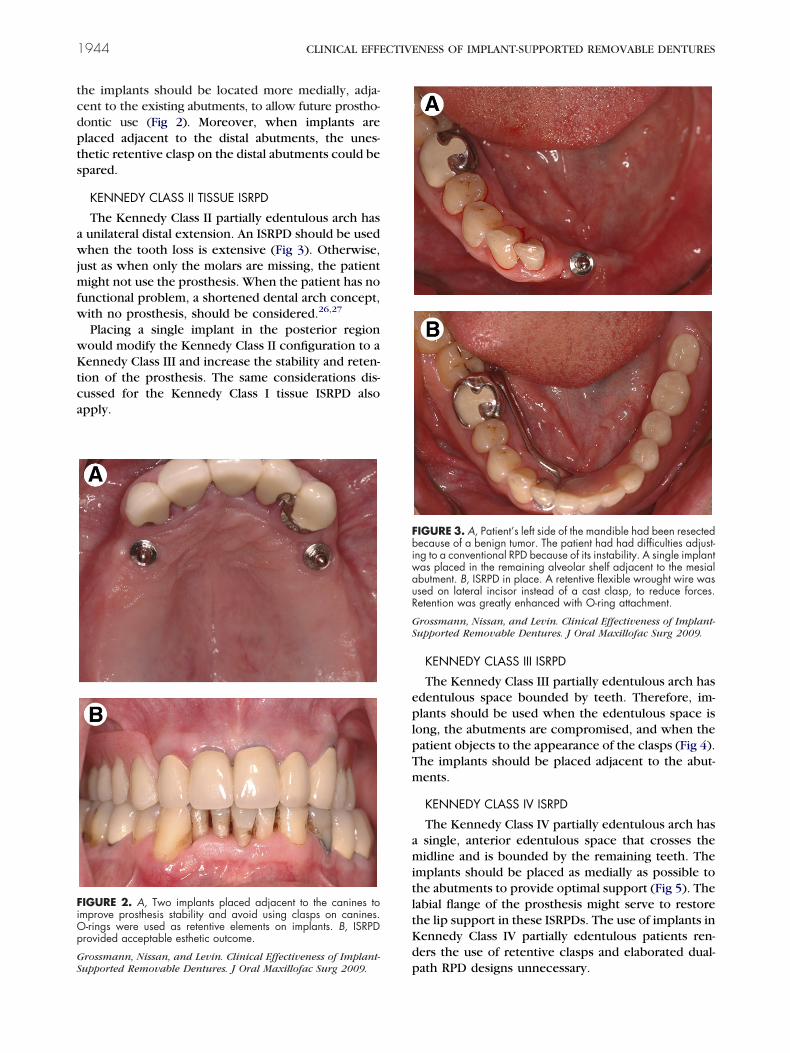
IGURE 2. A, Two implants placed adjacent to the canines tomprove prosthesis stability and avoid using clasps on canines.-rings were used as retentive elements on implants. B, ISRPDrovided acceptable esthetic outcome.
prossmann, Nissan, and Levin. Clinical Effectiveness of Implant-upported Removable Dentures. J Oral Maxillofac Surg 2009.
KENNEDY CLASS III ISRPD
The Kennedy Class III partially edentulous arch hasdentulous space bounded by teeth. Therefore, im-lants should be used when the edentulous space is
ong, the abutments are compromised, and when theatient objects to the appearance of the clasps (Fig 4).he implants should be placed adjacent to the abut-ents.
KENNEDY CLASS IV ISRPD
The Kennedy Class IV partially edentulous arch hassingle, anterior edentulous space that crosses theidline and is bounded by the remaining teeth. The
mplants should be placed as medially as possible tohe abutments to provide optimal support (Fig 5). Theabial flange of the prosthesis might serve to restorehe lip support in these ISRPDs. The use of implants inennedy Class IV partially edentulous patients ren-ers the use of retentive clasps and elaborated dual-
IGURE 3. A, Patient’s left side of the mandible had been resectedecause of a benign tumor. The patient had had difficulties adjust-
ng to a conventional RPD because of its instability. A single implantas placed in the remaining alveolar shelf adjacent to the mesialbutment. B, ISRPD in place. A retentive flexible wrought wire wassed on lateral incisor instead of a cast clasp, to reduce forces.etention was greatly enhanced with O-ring attachment.
rossmann, Nissan, and Levin. Clinical Effectiveness of Implant-upported Removable Dentures. J Oral Maxillofac Surg 2009.
ath RPD designs unnecessary.
sisptw
etmgrfl
li
oh
R
Fant
GS
FmKbTipw
GS
GROSSMANN, NISSAN, AND LEVIN 1945
The ISRPD serves as a cost-effective, prostheticolution for partially edentulous patients who are notmmediate candidates for extensive, fixed implant-upported restorations. Incorporation of dental im-lants to improve the RPD support and retention ando enhance patient acceptance should be consideredhen treatment planning for RPD.As mentioned, a high incidence of periodontal dis-
ase and dental caries has been reported in conven-ional RPD wearers, attributed mainly to a lack ofotivation and compliance with adequate oral hy-
iene. Therefore, patients should be advised of theirole in the maintenance of the ISRPD, and a definiteollow-up protocol is mandatory to obtain satisfactoryong-term results.
Additional research is warranted to evaluate theong-term survivability of the implants, the long-termnfluence on the abutment prognosis, and the effects
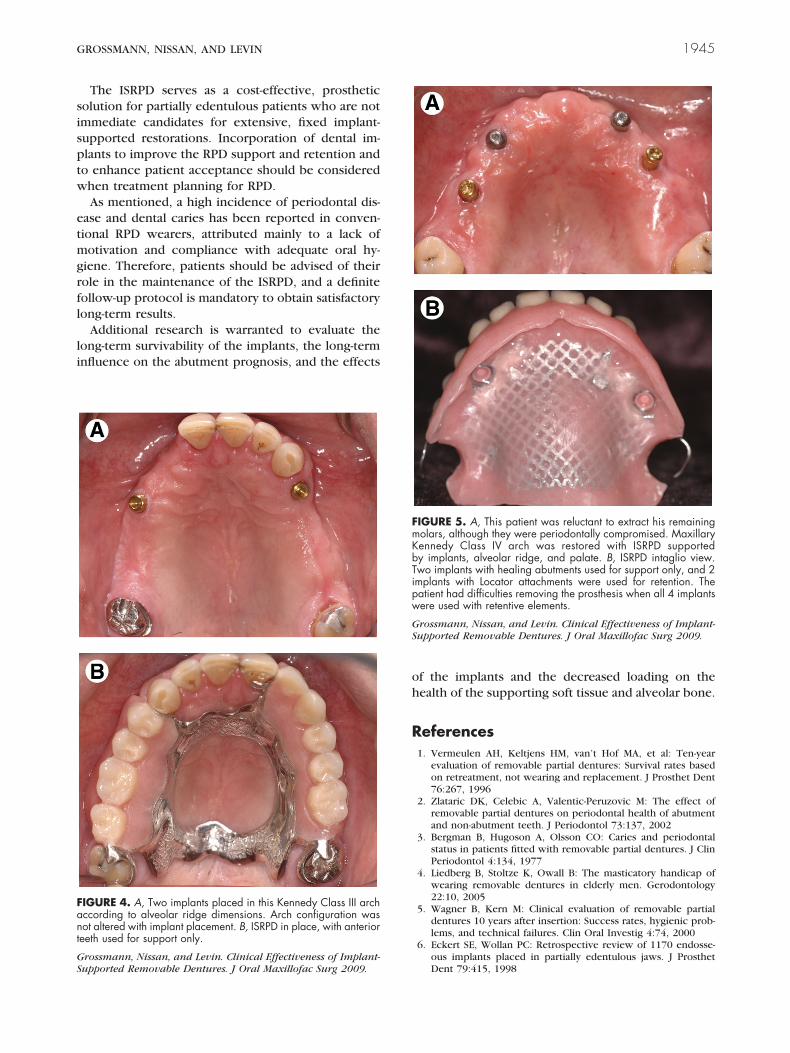
IGURE 4. A, Two implants placed in this Kennedy Class III archccording to alveolar ridge dimensions. Arch configuration wasot altered with implant placement. B, ISRPD in place, with anterioreeth used for support only.
rossmann, Nissan, and Levin. Clinical Effectiveness of Implant-upported Removable Dentures. J Oral Maxillofac Surg 2009.
f the implants and the decreased loading on theealth of the supporting soft tissue and alveolar bone.
eferences1. Vermeulen AH, Keltjens HM, van’t Hof MA, et al: Ten-year
evaluation of removable partial dentures: Survival rates basedon retreatment, not wearing and replacement. J Prosthet Dent76:267, 1996
2. Zlataric DK, Celebic A, Valentic-Peruzovic M: The effect ofremovable partial dentures on periodontal health of abutmentand non-abutment teeth. J Periodontol 73:137, 2002
3. Bergman B, Hugoson A, Olsson CO: Caries and periodontalstatus in patients fitted with removable partial dentures. J ClinPeriodontol 4:134, 1977
4. Liedberg B, Stoltze K, Owall B: The masticatory handicap ofwearing removable dentures in elderly men. Gerodontology22:10, 2005
5. Wagner B, Kern M: Clinical evaluation of removable partialdentures 10 years after insertion: Success rates, hygienic prob-lems, and technical failures. Clin Oral Investig 4:74, 2000
6. Eckert SE, Wollan PC: Retrospective review of 1170 endosse-
IGURE 5. A, This patient was reluctant to extract his remainingolars, although they were periodontally compromised. Maxillaryennedy Class IV arch was restored with ISRPD supportedy implants, alveolar ridge, and palate. B, ISRPD intaglio view.wo implants with healing abutments used for support only, and 2mplants with Locator attachments were used for retention. Theatient had difficulties removing the prosthesis when all 4 implantsere used with retentive elements.
rossmann, Nissan, and Levin. Clinical Effectiveness of Implant-upported Removable Dentures. J Oral Maxillofac Surg 2009.
ous implants placed in partially edentulous jaws. J ProsthetDent 79:415, 1998

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
1946 CLINICAL EFFECTIVENESS OF IMPLANT-SUPPORTED REMOVABLE DENTURES
7. van Steenberghe D, Lekholm U, Bolender C, et al: Applicabilityof osseointegrated oral implants in the rehabilitation of partialedentulism: A prospective multicenter study on 558 fixtures.Int J Oral Maxillofac Implants 5:272, 1990
8. Levin L, Sadet P, Grossmann Y: A retrospective evaluation of1,387 single-tooth implants: A 6-year follow-up. J Periodontol77:2080, 2006
9. Wostmann B, Budtz-Jorgensen E, Jepson N, et al: Indications forremovable partial dentures: A literature review. Int J Prosth-odont 18:139, 2005
0. Bergman B, Hugoson A, Olsson CO: Caries and periodontalstatus in patients fitted with removable partial dentures. J ClinPeriodontol 4:134, 1977
1. Jepson N, Allen F, Moynihan P, et al: Patient satisfactionfollowing restoration of shortened mandibular dental archesin a randomized controlled trial. Int J Prosthodont 16:409,2003
2. Witter DJ, van Elteren P, Kayser AF, et al: The effect of remov-able partial dentures on the oral function in shortened dentalarches. J Oral Rehabil 16:27, 1989
3. Van Waas M, Meeuwissen J, Meuwissen R, et al: Relationshipbetween wearing a removable partial denture and satisfactionin the elderly. Community Dent Oral Epidemiol 22:315, 1994
4. Keltjens H, Kayser A, Hertel R, et al: Distal extension remov-able partial dentures supported by implants and residual teeth:Considerations and case reports. Int J Oral Maxillofac Implants8:208, 1993
5. Kuzmanovic DV, Payne AG, Purton DG: Distal implants tomodify the Kennedy classification of a removable partial den-ture: A clinical report. J Prosthet Dent 92:8, 2004
6. Uludag B, Celik G: Fabrication of a maxillary implant-supportedremovable partial denture: A clinical report. J Prosthet Dent
95:19, 20067. Ganz SD: Combination natural tooth and implant-borne remov-able partial denture: A clinical report. J Prosthet Dent 66:1, 1991
8. Giffin KM: Solving the distal extension removable partial den-ture base movement dilemma: A clinical report. J Prosthet Dent76:347, 1996
9. Ohkubo C, Kurihara D, Shimpo H, et al: Effect of implantsupport on distal extension removable partial dentures: In vitroassessment. J Oral Rehabil 34:52, 2007
0. Maeda Y, Sogo M, Tsutsumi S: Efficacy of a posterior implantsupport for extra shortened dental arches: A biomechanicalmodel analysis. J Oral Rehabil 32:656, 2005
1. Mitrani R, Brudvik JS, Phillips KM: Posterior implants for distalextension removable prostheses: A retrospective study. Int JPeriodontics Restorative Dent 23:353, 2003
2. Mijiritsky E, Ormianer Z, Klinger A, et al: Use of dental implantsto improve unfavorable removable partial denture design.Compend Contin Educ Dent 26:744, 2005
3. Grossmann Y, Levin L, Sadan A: A retrospective case series ofimplants used to restore partially edentulous patients withimplant-supported removable partial dentures: 31-Month meanfollow-up results. Quintessence Int 39:655, 2008
4. Zarb GA, Albrektsson T: Consensus report: Towards optimizedtreatment outcomes for dental implants. J Prosthet Dent 80:641, 1998
5. Wegner PK, Freitag S, Kern M: Survival rate of endodonticallytreated teeth with posts after prosthetic restoration. J Endod32:928, 2006
6. Witter DJ, de Haan AF, Kayser AF, et al: 6-Year follow-up studyof oral function in shortened dental arches. Part I: Occlusalstability. J Oral Rehabil 21:13, 1994
7. Meeuwissen JH, van Waas MA, Meeuwissen R, et al: Satisfactionwith reduced dentitions in elderly people. J Oral Rehabil 22:
397, 1995