clinical decision support to improve diabetes care: a search for unintended consequences randall d....
TRANSCRIPT

Clinical Decision Support Clinical Decision Support to Improve Diabetes Care:to Improve Diabetes Care:
A Search for Unintended ConsequencesA Search for Unintended Consequences
Randall D. Cebul, M.D.Center for Health Care Research & Policy
Case Western Reserve UniversityMetroHealth Medical Center
Cleveland
Center for
Health Care
Research &
Policy
www.chrp.orgSupported by grant R01-HS015123, AHRQ

Purpose/Overview
1. Describe aspects of a trial of real-time clinical decision support (CDS) to improve care and outcomes of patients with diabetes.
2. Describe analyses/preliminary results of Secondary Aim #4: “to examine general and intervention-specific unintended consequences of our intervention.”
The Search for Unintended Consequences
1. Has our focused attention on diabetes and glycemic control been associated with:
• Higher rates of clinically important hypoglycemia?• Inattention to/reduced quality for other conditions?
2. Has the CDS been associated with “Alert Fatigue”*? - do clinicians want to keep or eliminate the CDS at the end of the trial?
* Chronic Alert Fatigue Syndrome (CAFS) “is an insidious disorder, characterized by mental exhaustion and exasperation secondary to frequent, involuntary exposure to displays of alerts and reminders in computerized clinical information systems.” Greengold NL. P & T. 2005; 30: 506-511.
Diabetes Improvement Group – Diabetes Improvement Group – Intervention Trial (DIG-IT*): OverviewIntervention Trial (DIG-IT*): Overview
• Commercial EMR-facilitated: – study design (cluster randomized trial, or CRT)– real-time clinical decision support – performance measurement– Nurse Case Management
• Two health care systems 24 sites, 200 PCPs– Cleveland Clinic, MetroHealth
*Funded, in part, by grant R01-HS015123Agency for Healthcare Research and Quality
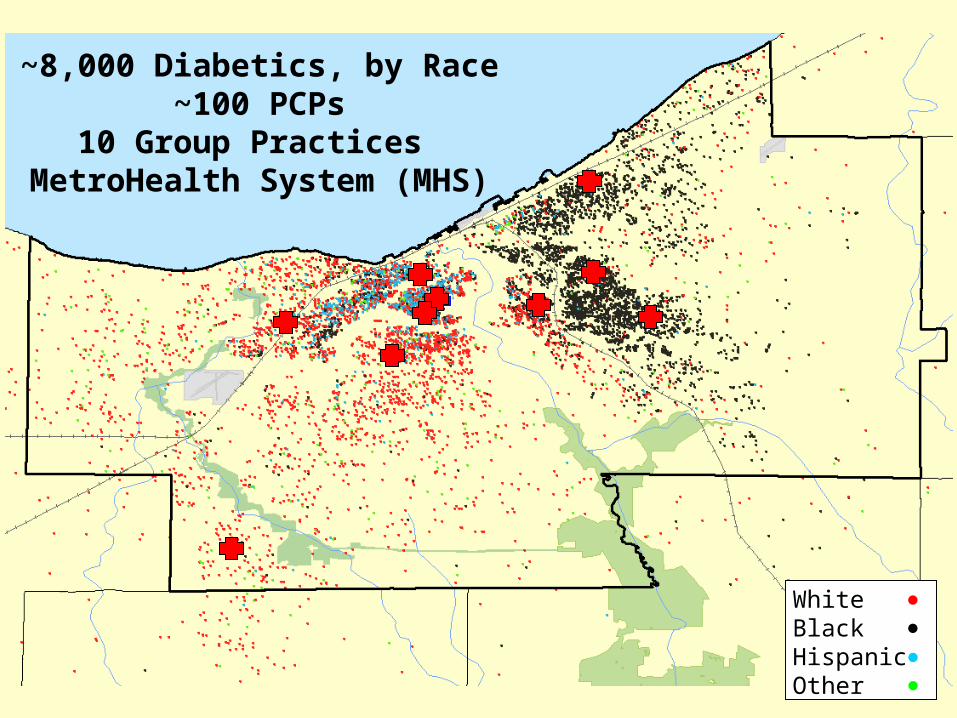
White BlackHispanicOther
~8,000 Diabetics, by Race~100 PCPs
10 Group Practices MetroHealth System (MHS)

Design: Random Assignment of Practices to Design: Random Assignment of Practices to CDS - Disease Management (DM CDS - Disease Management (DM22)) - MHS
5Groups
5GroupsDM2
Epic
Only
10 Practices, ~100 PCPs, ~8000 Patients
Primary Aims: Quality & Utilization (including sub-groups by insurance etc)
Secondary Aims: Adoption/Correlates; Unintended Consequences
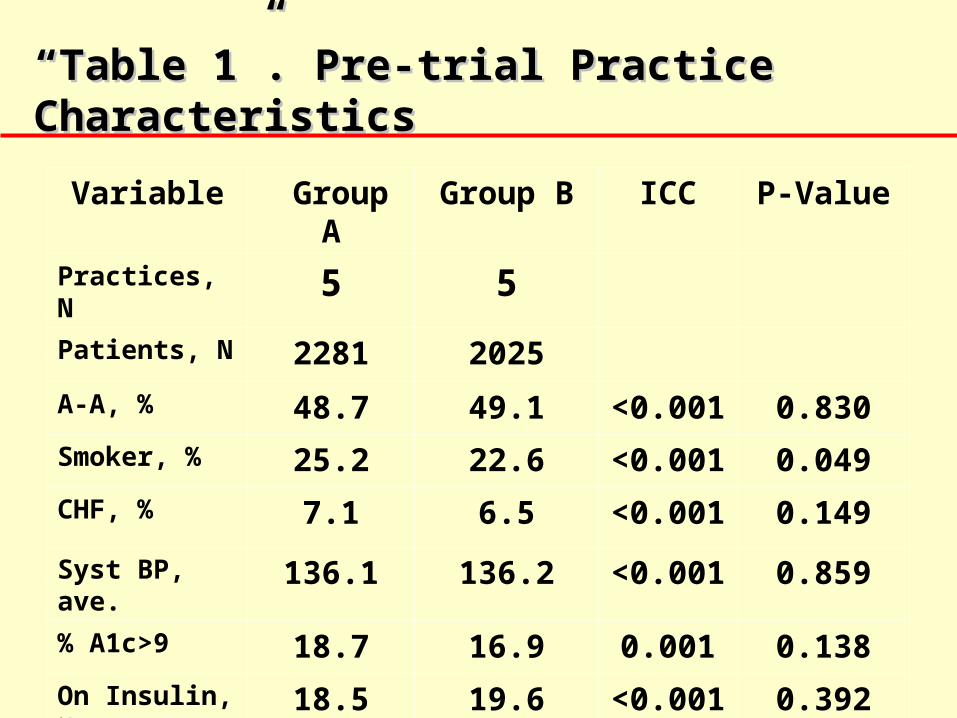
““Table 1”. Pre-trial Practice CharacteristicsTable 1”. Pre-trial Practice Characteristics
Variable Group A Group B ICC P-Value
Practices, N 5 5Patients, N 2281 2025
A-A, % 48.7 49.1 <0.001 0.830
Smoker, % 25.2 22.6 <0.001 0.049
CHF, % 7.1 6.5 <0.001 0.149
Syst BP, ave. 136.1 136.2 <0.001 0.859
% A1c>9 18.7 16.9 0.001 0.138
On Insulin, % 18.5 19.6 <0.001 0.392
ED visits, % 26.9 19.4 0.015 0.032
Clinical Decision Support – DMClinical Decision Support – DM22
• Alerts and Linked Order Sets
• Patient Lists/Registry
• Practice panel performance feedback
• Nurse Case Management
Practice Panel Tools
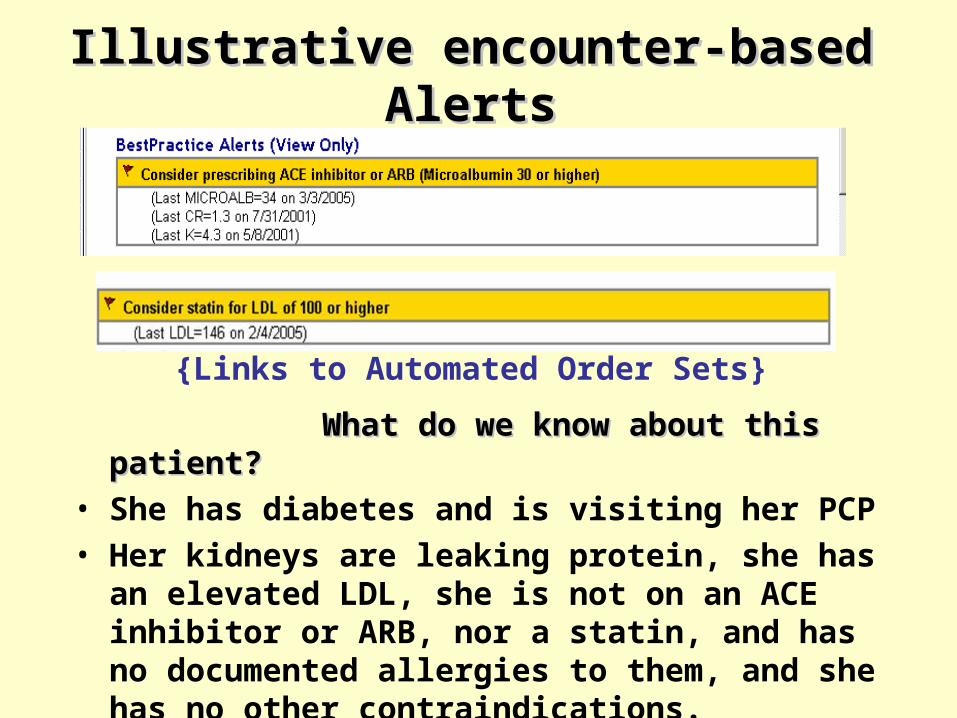
Illustrative encounter-based AlertsIllustrative encounter-based Alerts
What do we know about this patient?What do we know about this patient?• She has diabetes and is visiting her PCP• Her kidneys are leaking protein, she has an
elevated LDL, she is not on an ACE inhibitor or ARB, nor a statin, and has no documented allergies to them, and she has no other contraindications.
• There are several alternative drugs/doses
{Links to Automated Order Sets}

SmartSet Linked to ACE/ARB AlertSmartSet Linked to ACE/ARB Alert
Patient name
Patient name
Re-cap of indications
Choice of Rxs/doses
Follow-up testing

Practice Performance Feedback Practice Performance Feedback
“My panel” vs. Comparator

Individual Practice RegistryIndividual Practice Registry
Physician name
Patient name, hosp number and phone #
Click on tab to sort
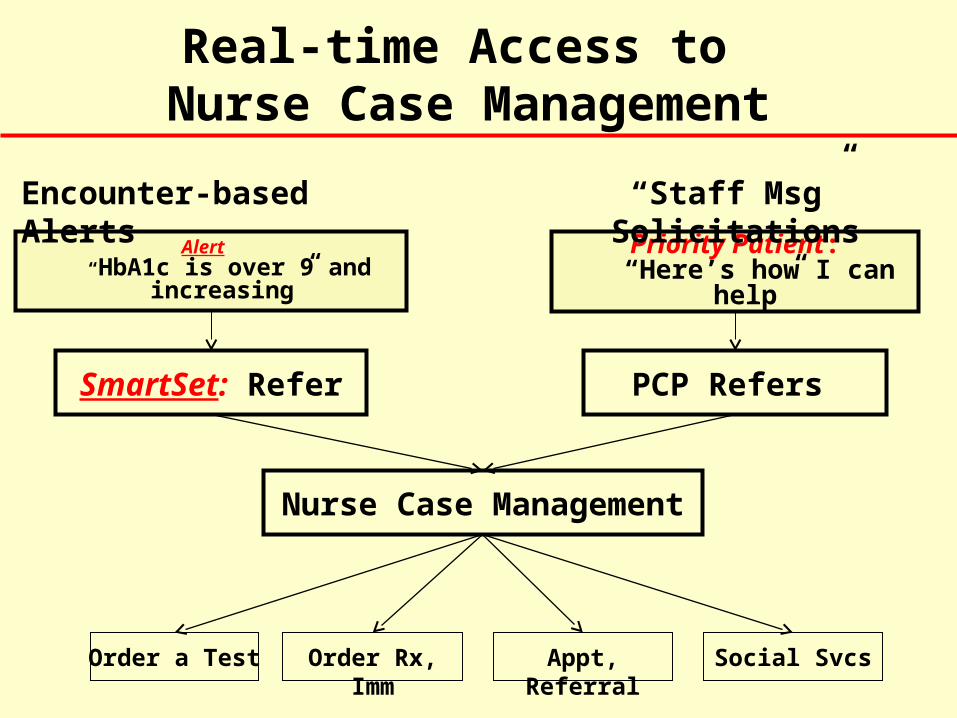
Alert: “HbA1c is over 9 and
increasing”
SmartSet: Refer
Priority Patient: “Here’s how I can help”
PCP Refers
Nurse Case Management
Real-time Access to Nurse Case Management
Encounter-based Alerts
“Staff Msg” Solicitations
Order a Test Order Rx, Imm Appt, Referral Social Svcs

Unintended consequences
• Has our focused attention on diabetes and glycemic control been associated with:
• Higher rates of clinically important hypoglycemia?• Outpatient visits with documented hypoglycemia?• ED Visits or hospitalizations for hypoglycemia?
• Inattention to other conditions?• Preventive services: mammograms and pap smears?• Diagnosis or management: asthma and CHF?

Were there more clinically important episodes of hypoglycemia in the CDS group?
2.22.8
3.42.8
0
1
2
3
4
5
6
7
8
9
10
ED or Hospitalization O.P. Hypoglycemia
% o
f P
ts w
ith
1 o
r m
ore
ep
iso
des
ControlCDS
(Documented glucose<60mg/dl)(DM-related hypoglycemia)
(P=0.01) (P=0.96)

Were there fewer indicated mammograms, Pap smears, or evaluations for CHF in the CDS group?
62.8
45.9
68.2
57.2
44.9
66.1
0
10
20
30
40
50
60
70
80
Mammograms Pap Smears Echos for CHF
% o
f w
om
en w
ith
In
dic
ated
Tes
t
ControlCDS
(Women 18-75)(Women 50-75)
(P=0.21) (P=0.55)
(All pts with dx CHF)
(P=0.78)
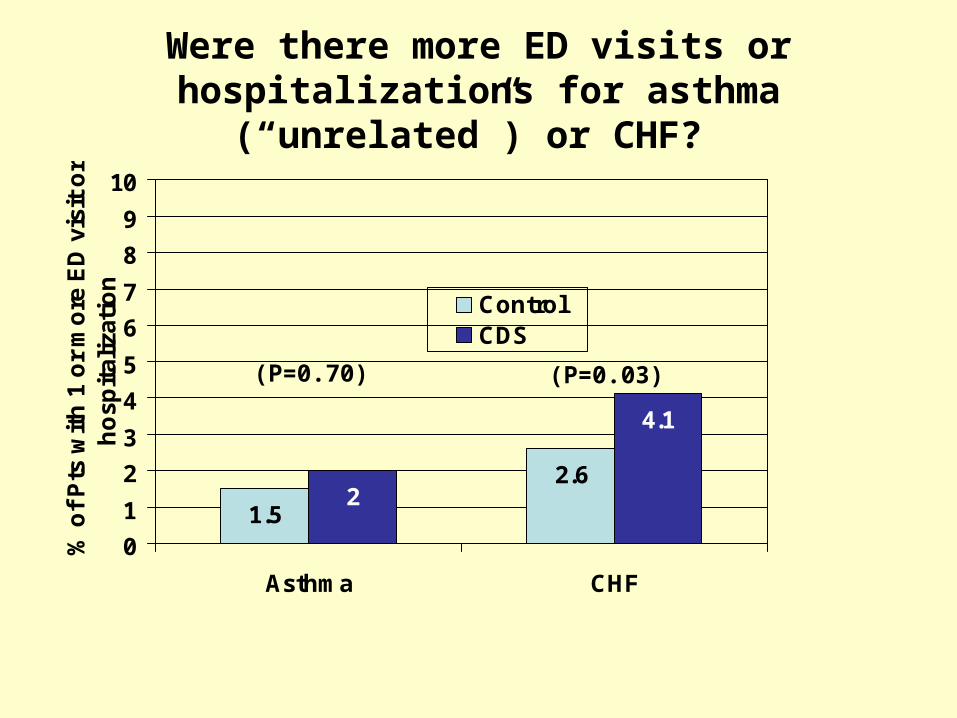
Were there more ED visits or hospitalizations for asthma (“unrelated”) or CHF?
1.5
2.62
4.1
0
1
2
3
4
5
6
7
8
9
10
Asthma CHF
% o
f P
ts w
ith
1 o
r m
ore
ED
vis
it o
r h
osp
ital
izat
ion
ControlCDS
(P=0.70) (P=0.03)

Planned Safety Comparisons Related to Alerts and Order sets
• Differences in proportions of patients:– Prescribed ACE inhibitors or ARBs in face of
relative contraindications (K+, renal function) or documented allergy
– Prescribed statins with relative C/I or allergy – Obtaining appropriate follow-up testing for Rx
side effects (kidney, liver function)

Alert Fatigue?PCP Satisfaction with CDS (n=51)
Re: 1) Alerts; 2) Practice Panel tools; and 3) Nurse Case Management:– “How often do you use”…?– “How useful do you find”…?– “Should “X” remain in Epic after the trial?”

Early Returns (71% response):“Should “X” remain after the trial?”
90%
72%
81%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Alerts & Order Sets Panel Tools Nurse Case Management
% Y
es

Summary: Work-in-Progress
• CDS intervention appears to be associated with:– Significant although small increases:
• ED visits for hypoglycemia - unintended but not unexpected.
• ED visits for CHF - ?related to use of TZDs– No significant differences:
• Preventive services (mammograms, pap smears)• Appropriate testing among patients with CHF• ED visits for unrelated condition (asthma)
• CDS-related alert fatigue did not occur, at least as measured by PCPs’ desires to retain the Alerts as the trial period ends.

Unintended Consequences: Closing Thoughts
• Don’t assume that well-intentioned and well-designed CDS is without unintended adverse consequences.
• Unintended consequences may relate:– directly from the activity that we are trying to improve (e.g.,
hypoglycemia; ? CHF from TZDs?)– to seemingly unrelated conditions (e.g., screening)
• Controlled trials are the best way to test for these “side effects”, and can be facilitated by using EMR-facilitated balancing of sites before assignment.
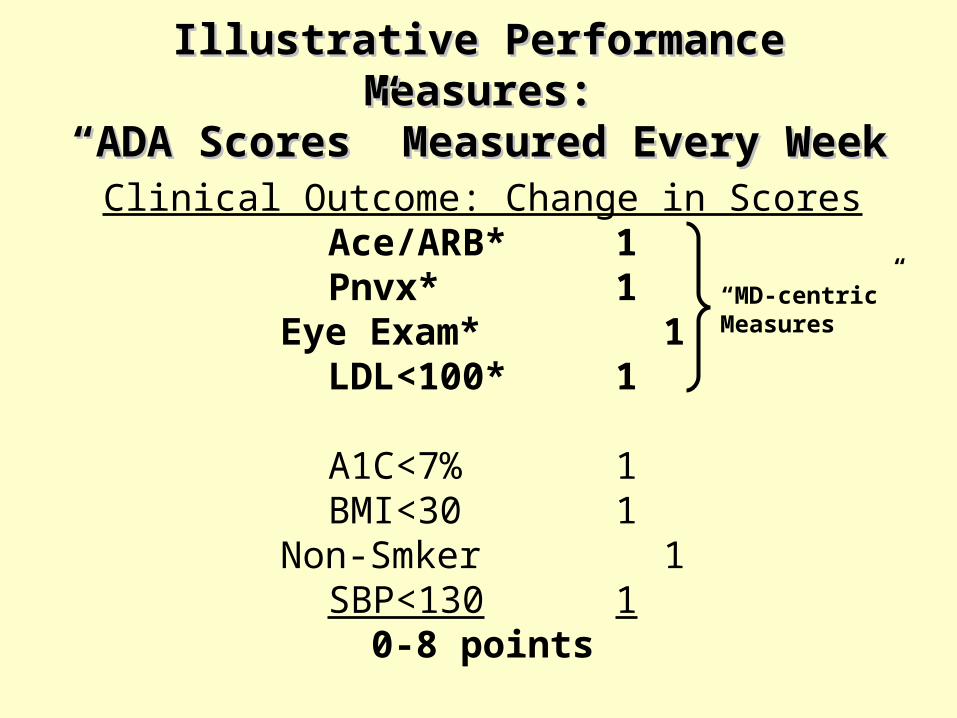
Illustrative Performance Measures:Illustrative Performance Measures:“ADA Scores” Measured Every Week“ADA Scores” Measured Every Week
Clinical Outcome: Change in ScoresAce/ARB* 1Pnvx* 1Eye Exam* 1LDL<100* 1
A1C<7% 1BMI<30 1Non-Smker 1SBP<130 1
0-8 points
“MD-centric” Measures

Changes in ADA Scores for MHS Experimental Group Patients (n=5288)
Percent ADA Score by Patient Week
Overall ADA MD-Centric ADA
40
45
50
55
60
65
70
75
80
Patient Week0 10 20 30 40 50 60 70 80 90 100
% of All ADA Measures Met% of All ADA Measures Met
% of 4 MD-Centric Measures Met% of 4 MD-Centric Measures Met