clinical data to support the interpretation of susceptibility testing of anaerobes robin howe
TRANSCRIPT

Clinical data to support the interpretation of susceptibility
testing of anaerobes
Robin Howe

'Mixed anaerobessensitive to metronidazole'
(common practice in UK)
Pus from cerebral abscess
Primary plate after 5 days AnO2 incubation
Courtesy Val Hall

? But would we report:-
'Mixed aerobes sensitive to a cephalosporin'
'Fungus present, try Athlete's Foot powder'
'Virus detected, have a hot whisky and lemon'
And would we test them like this?…..
Courtesy Val Hall

'S.O.P.' for susceptibility testingof anaerobes
• Agar: Any (selective or non-selective)
• Inoculum: Direct sample, ?mixed, not standardised
• Antimicrobial agents: metronidazole
• Incubation: On bench till 5pm, then AnO2 18-72hrs
• Controls: None
• Interpretation:
– Any sized zone = mixed anaerobes, sens to MZ– No zone = no anaerobes isolated– Colonies within zone = aerobes
Courtesy Val Hall

Why is susceptibility testing of anaerobes not generally used in clinical decision-
making?• Technical issues with testing
– Slow growth– Lack of consensus regarding agar/method
• Anaerobic susceptibility patterns– Predictable– Unchanging over years
• Limited data to correlate in vitro results with outcome– Infections often polymicrobial– Outcome affected by multiple factors (eg surgery)
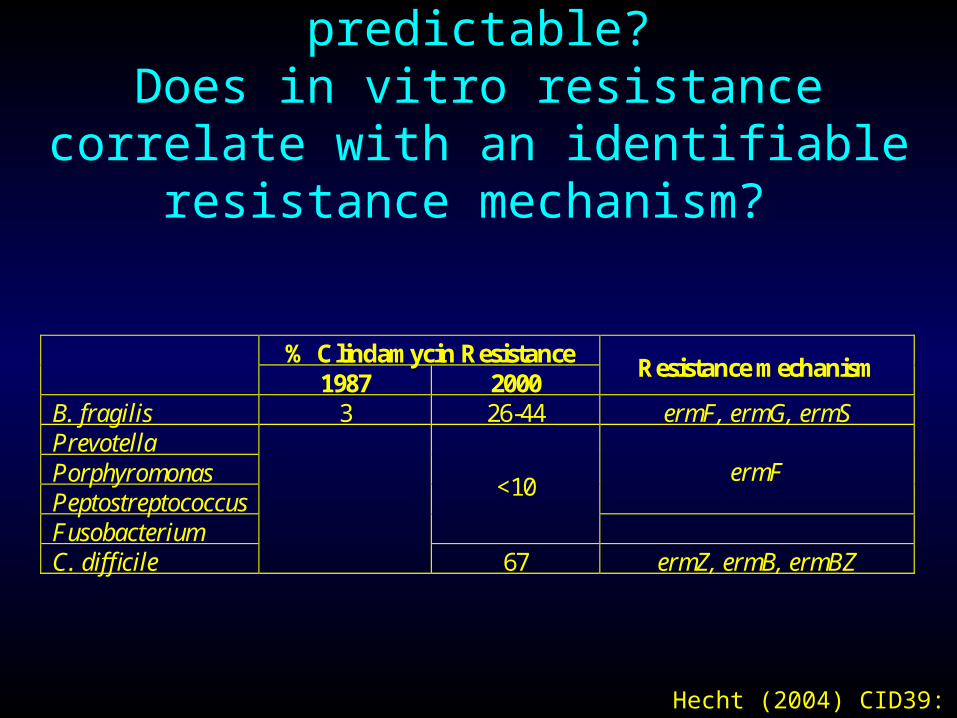
Are resistance rates predictable?Does in vitro resistance correlate with an
identifiable resistance mechanism?
% Clindamycin Resistance 1987 2000
Resistance mechanism
B. fragilis 3 26-44 ermF, ermG, ermS Prevotella Porphyromonas Peptostreptococcus
ermF
Fusobacterium
<10
C. difficile
67 ermZ, ermB, ermBZ
Hecht (2004) CID39: 92

Are resistance rates predictable?Does in vitro resistance correlate with an
identifiable resistance mechanism? % Resistance to -lactams
Penicillin Cephamycins
-lactam/ -lactamase inhibitors
Carbapenems
B. fragilis >97 8-22 5 <0.2 Prevotella 83 Fusobacterium 9 Porphyromonas 21 Peptostreptococcus 6
0-5 0-5
Non-perfringens Clostridia
0-88 0-5
C. perfringens 0-10?
0 0
Hecht (2004) CID39: 92

• Baquero (1992)– 10% C. perfringens in
Spain resistant to pen (MIC >0.5 mg/L)
BSAC BP 0.12 mg/L
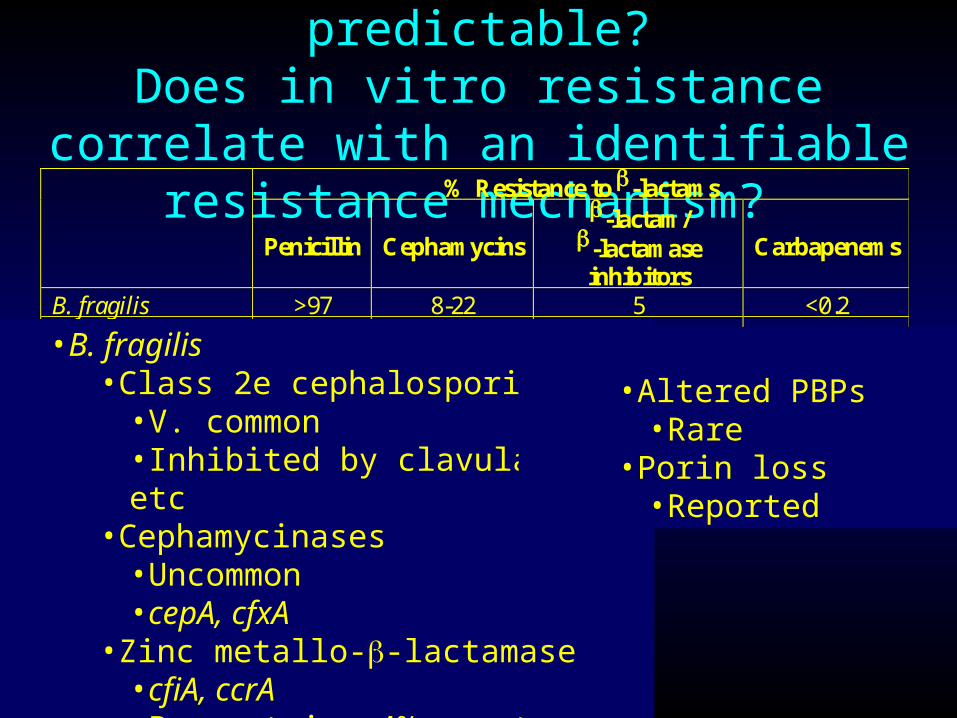
Are resistance rates predictable?Does in vitro resistance correlate with an
identifiable resistance mechanism? % Resistance to -lactams
Penicillin Cephamycins
-lactam/ -lactamase inhibitors
Carbapenems
B. fragilis >97 8-22 5 <0.2 Prevotella 83 Fusobacterium 9 Porphyromonas 21 Peptostreptococcus 6
0-5
0-5
Non-perfringens Clostridia
0-88 0-5
C. perfringens 0-10?
0 0
•B. fragilis•Class 2e cephalosporinase
•V. common•Inhibited by clavulanate etc
•Cephamycinases•Uncommon•cepA, cfxA
•Zinc metallo--lactamase•cfiA, ccrA•Present in ~4% - not usually expressed
•Altered PBPs•Rare
•Porin loss•Reported

Are resistance rates predictable?Does in vitro resistance correlate with an
identifiable resistance mechanism?
• Reduced susceptibility to metronidazole– Common in
• Propionibacteria & actinomycoses
– Rare in• B. fragilis
– nim genes
• C.difficile
REFERRALS TO ARU •Bacteroides spp. n=78
(5% of all Bacteroides)
• Clostridium paraputrificum n=5 (4%)
• Clostridium ramosum n=3 (1%)
nim genes
• Nim = nitro-imidazole reductase
• Types A – G found in Bacteroides spp.
• Detected by PCR-RFLP
• Chromosomal / plasmid-borne
• Absent from some MZ resistant orgs
• Probable alternative mechanisms
• High level MZ resistance can be induced in some nim-containing strains
Courtesy Val Hall

• nim genes identified in 2% of 1,502 B. fragilis from 19 European countries
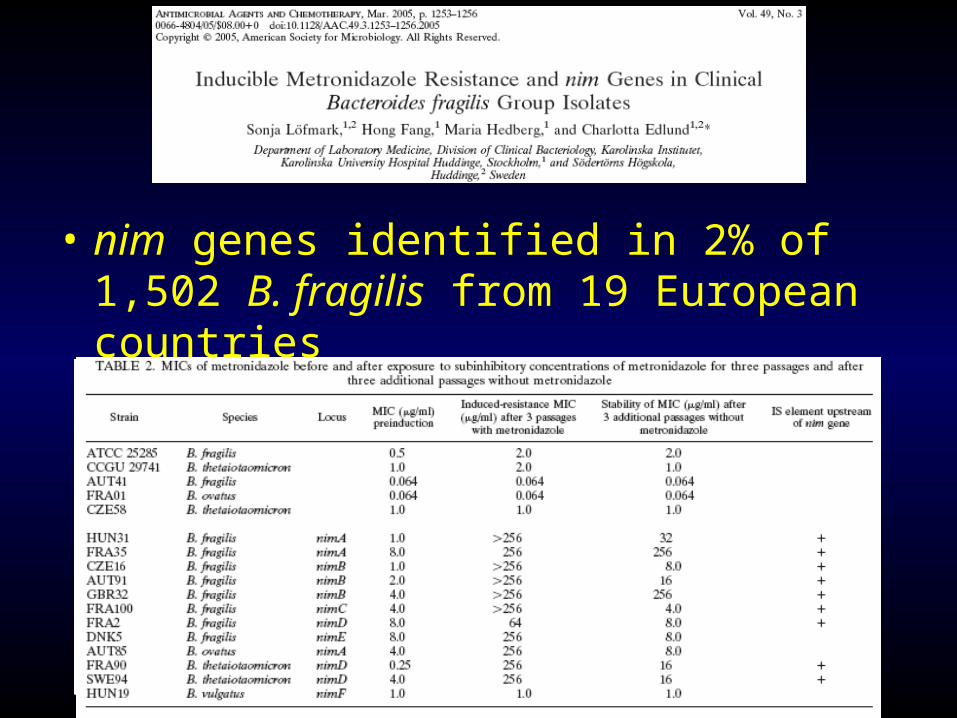
• nim genes identified in 2% of 1,502 B. fragilis from 19 European countries

Animal studies
• Rat model of secondary peritonitis– Pooled faecal emulsion intraperitoneally
– initially E. coli predominates with often fatal bacteraemia
– If survive abscesses with B. fragilis
– Early gentamicin no bacteraemia but late abscesses
– Early clindamycin no effect on bacteraemic mortality but reduced late abscesses in survivors
Onderdonk et al (1974) Infect Immun 10:1256
The role of anti-anaerobic therapy

Animal studies

?synergistic infection
• IP injection of mixtures of three orgs
FOX Cefotetan Amp/sul B. fragilis 8 8 2 B. thetaiotaomicron 16 64 4 B. ovatus 8 128 2 B. distasonis 8 128 4 E. coli 2 0.5 8
Bacterial counts
No deaths
No with abscesses in
survivors E. coli B.
fragilis B.
theta Saline 13 17/17 7.4 8.7 8.3 Cefoxitin 4 3/26 4.8 4.7 3.9 Cefotetan 0 3/30 4.5 4.0 3.6
E. coli B. fragilis B. theta
Amp/sul 7 4/23 5.4 3.2 2.8
Brook (1994) JAC 34: 791


Reports of clinical failure associated with resistance
• Penicillin vs C. perfringens– NIL
• Metronidazole vs Bacteroides spp– YES

Rotimi et al (1999)CMI 5: 166
• 3 case reports– 75 yrs female
• post op Hartmann’s treated with CAZ/MTZ• Readmitted with paracolic abscess• B. frag isolated (MTZ MIC >32 mg/L)• Cured with drainage + IMI
– 40 yrs male• Gangrenous appendix (mixed B. frag/E. coli/Pseudomonas)• CXM/MTZ started• Day 5 - Wound infection
– B. frag + B. ovatus (MTZ MIC >32mg/L)– Cured with co-amox
– 37 yrs male• Post renal transplant• cholecystitis cholecystectomy necrotising pancreatitis• Multiple Abs – CTX/MTZ/AMIK – MEM/AMIK/CPM• Mixed isolates from lap inc B. distasonis (MIC MTZ >32 mg/L, MEM >32 mg/L)• Pt died

Reports of clinical failure associated with resistance
• Penicillin vs C. perfringens– NIL
• Metronidazole vs Bacteroides spp– YES
• Penicillin vs Bacteroides spp.– YES
Brook (1984) Arch Otolaryngol 110: 228Gudiol (1990) Arch Intern Med 150: 2525

Reports of clinical failure associated with resistance
• Penicillin vs C. perfringens– NIL
• Metronidazole vs Bacteroides spp– YES
• Penicillin vs Bacteroides spp.– YES
• Β-lactam/β-lactamase inhibitors vs Bacteroides spp.– NIL
• Carbapenems vs Bacteroides spp.– YES

• 38 year old female– Elective laparotomy for adhesions
– Post-op IA collection treated with co-amox
– Day 13 - surgical drainage & change to CTX + MTZ
– BC grew B. fragilis (isolate 1)
– Changed to imipenem
– 2 weeks later persistent empyema drained (isolate 2)
– Cured with drainage/clindamycin/gentamicin
Turner et al (1995) Lancet 345: 1275
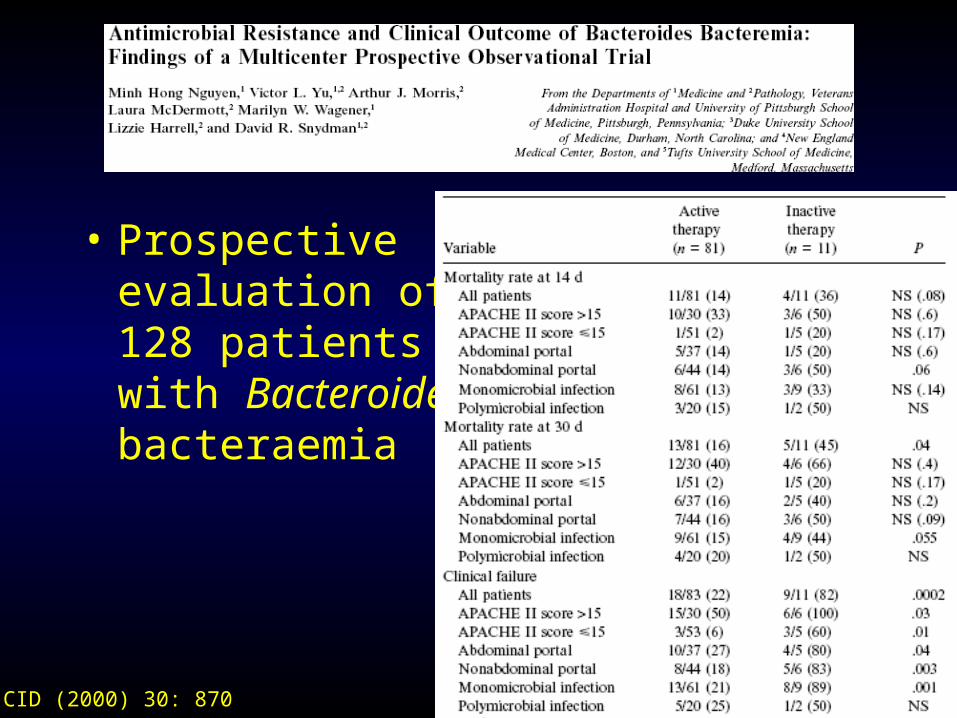
• Prospective evaluation of 128 patients with Bacteroides bacteraemia
CID (2000) 30: 870

Any data relating level of resistance to outcome?
• NO
Conclusions
• Antimicrobial resistance is variably predictable• Resistance rates are increasing
– CLD – becoming common– MTZ + carbapenems – emerging
• Inducibility is a concern
• Correlation between in vitro resistance and outcome has not been established for many anaerobic infections– The role of surgery should not be forgotten

Finegold 1989
• Susceptibility testing of anaerobes should be done in 4 settings:– Determine patterns of susceptibility to new agents
– Monitor susceptibility patterns Nationally
– Monitor susceptibility patterns locally
– Assist in the management of individual patients• Persistence of infection/ failure of usual regimes/ difficulty
making decisions based on precedent
• Brain abscess/ endocarditis/ osteomyelitis/ prosthetic device infection/ septic arthritis