clinical considerations in the use of new migraine medications · migraine as head pain with...
TRANSCRIPT

In the last decade, a variety of newantimigraine compounds havebeen synthesized. At the same
time, existing agents have been refor-mulated to enhance their delivery,convenience, and effectiveness for themigraine patient. As a result, clini-cians today have the benefit of severalnew effective agents that are backedby extensive clinical testing but wereunavailable just 5 or 10 years ago.
The result is that patients whowere chronic users of the tertiaryheadache center or the emergencyroom are now being treated muchmore effectively. For many patients,these new agents are miracle drugs.
Even with an overall failure rate ofabout 20%, the new self-administeredparenteral therapies and nasal sprayshave truly revolutionized migrainetreatment.
The opportunity and the challengeis to educate physicians as to the bestuse of these revolutionary agents.Various national groups and societiesare now seeking consensus onheadache guidelines that explain theoptimal use of these new agents invarious patient scenarios. Managedcare plans are eager to adopt andimplement such guidelines.
Undoubtedly, this is the correctprocess, but managed care groups
Clinical Considerations in the Use of New Migraine Medications
Based on a presentation by Constance Johnson, MD
. . .SYMPOSIUM PROCEEDINGS . . .
Presentation Summary The opportunities for improv-
ing the lives of those with severemigraine have never been greater.Yet, even as physicians becomemore aware of today’s more effec-tive pharmacologic options, thetendency of this disease to mani-fest differently in individualpatients means that even theclearest treatment guidelines willrequire monitoring and cus-tomization. The main choices forpharmacologic treatment of acute
migraine include over-the-count-er combinations (for example,acetaminophen-aspirin-caffeineand nonsteroidal anti-inflamma-tory drugs), dihydroergotamine,and 5-hydroxytriptamine ago-nists. The efficacy of theseagents is approximately 60% to80%, and the choice of an agentfor an individual patient oftendepends on dosing convenience,administration options, side-effect profiles, and individualresponse.
VOL. 5, NO. 2, SUP. THE AMERICAN JOURNAL OF MANAGED CARE S79

S80 THE AMERICAN JOURNAL OF MANAGED CARE FEBRUARY 1999
. . . SYMPOSIUM PROCEEDINGS . . .
must realize that the final guidelineswill in all likelihood offer only generalinstruction in choosing the appropri-ate therapy. With limited head-to-head studies and a wide variation in
patients’ therapeutic response, guide-line modification is appropriate,because it will shift much of the man-agement burden back to the primarycare physician. So those who aredeveloping and implementing migraineguidelines should take into account theperspective of the busy physician whomanages headaches on a daily basis.Several common physician concernsinvolving migraine diagnosis andtreatment are presented to highlightthis practical perspective.
Defining HeadacheThe diagnosis of headache has not
changed in recent years. No test formigraine exists, only tests to excludeorganic headache disorders. The defi-nition of headache remains clinical.The International Headache Society(IHS) classification that definesmigraine as head pain with migrain-ous features remains the best guide(Table 1).1 However, even though thediagnosis of headache has notadvanced significantly, cliniciansmust pay more attention to their owntendency to classify the headache andthe patient.
Neurologists still do not agree onwhether all headaches are variationsof the same disorder or discrete man-ifestations of separate disorders. As aresult, the old “lumper vs splitter”debate goes on.
Although the debate at the patho-physiologic level may be academic,the very practical implications ofphysician and patient beliefs regard-ing headache origins should be recog-nized. For example, if a certain physi-cian believes that diet is a major trig-ger of headache, he or she may endup with patients for whom this is true.Similarly, a gynecologist who treatsmenstrual migraine may have a prac-tice that attracts women for whom atimed prophylactic treatment worksbest. There is referral bias at work,and the physician’s definition shapesthe treatment choice.
Table 1. International Headache Society (IHS) Criteria for Migraine
Source: See reference 1.
Migraine Without Aura
A. At least 5 attacks fulfilling criteria B through DB. Attacks lasting 4 to 72 hours (untreated or unsuccessfully treated)C. At least 2 of the following characteristics:
1. Unilateral locations2. Pulsating quality3. Moderate or severe intensity (inhibits or prohibits daily activities)4. Aggravated by climbing stairs or similar routine activity
D. At least 1 of the following:1. Nausea and/or vomiting2. Photophobia and phonophobia
E. At least 1 of the following:1. History, physical, and neurologic examinations do not suggest dis-
orders in groups 5 through 11 of the IHS classification [NOTE:These include headache associated with: 1) head trauma; 2)vascu-lar disorders; 3) nonvascular intracranial disorder; 4) substances ortheir withdrawal; 5) noncephalic infection; 6) metabolic disorder;and 7) facial pain associated with disorder of the cranium, neck,eyes, ears, nose, sinuses, teeth, mouth, or other facial or cranialstructures.]
2. History and/or physical and/or neurologic examinations suggestsuch a disorder, but it is ruled out by appropriate investigations
3. Such a disorder is present, but attacks do not occur for the firsttime in close temporal relation to the disorder
Migraine With Aura
A. At least 2 attacks fulfilling criterion BB. At least 3 of the following characteristics:
1. One or more fully reversible aura symptoms indicating focal cere-bral cortical and/or brain stem dysfunction
2. At least 1 aura symptom develops gradually over more than 4 min-utes or 2 or more symptoms occur in succession
3. No aura symptom lasts more than 60 minutes. If more than oneaura symptom is present, the accepted duration is proportionallyincreased
4. Attack follows an aura with a free interval of less than 60 minutes(can also begin before or simultaneous with the aura)
C. At least 1 of the following:1. History, physical, and neurologic examinations do not suggest dis-
orders in groups 5 to 11 of the IHS classification (see note above)2. History and/or physical and/or neurologic examinations suggest
such a disorder, but it is ruled out by appropriate investigations3. Such a disorder is present, but attacks do not occur for the first
time in close temporal relation to the disorder
VOL. 5, NO. 2, SUP. THE AMERICAN JOURNAL OF MANAGED CARE S81
. . . CLINICAL CONSIDERATIONS IN THE USE OF NEW MIGRAINE MEDICATIONS . . .
Even the classification of headachesin terms as basic as frequency andseverity may not always be clear cut.For example, there are alwayspatients who have headaches that fitthe IHS classification of migraine onlyonce a year or every other year. Butperhaps these patients have tensionheadaches that require treatmentevery month. Many patients actuallypresent with this type of mixed disor-der. Should they be treated formigraine? The answer hinges on thephysician’s interpretation of the oftenvague patient-reported frequency.Severity alone cannot be the guide todefining migraine, because manypatients with mixed headaches havevery severe tension headaches.
In defining a patient’s migraine fre-quency over the longer term, the cli-nician often will identify periods ofremission and exacerbation. Over thecourse of a 15- to 20-year physician-patient relationship, there willundoubtedly be good migraine timesand bad migraine times. This has
implications for evaluating outcomesof both prophylactic and alternativetherapies. Is the patient getting betterbecause of therapy, or is it a sponta-neous remission? Such waxing andwaning of disease also has implica-tions for possibly tapering treatment.
Such practical diagnostic issuessuch as special patient populations,infrequent migraines, and long-termremissions have not been addressedin treatment trials and are difficult toincorporate in guidelines.
Pharmacologic TreatmentChoices of pharmacologic migraine
therapy can be divided into 3 types:acute symptomatic treatment, acuteabortive treatment, and prophylactictreatment. Because migraine is gener-ally a paroxysmal disorder, acutetreatments receive the most atten-tion. Recommendations regarding themainstays of acute therapy from sev-eral publications are highlighted, notso much to guide drug choice as toillustrate the similarity of results seen
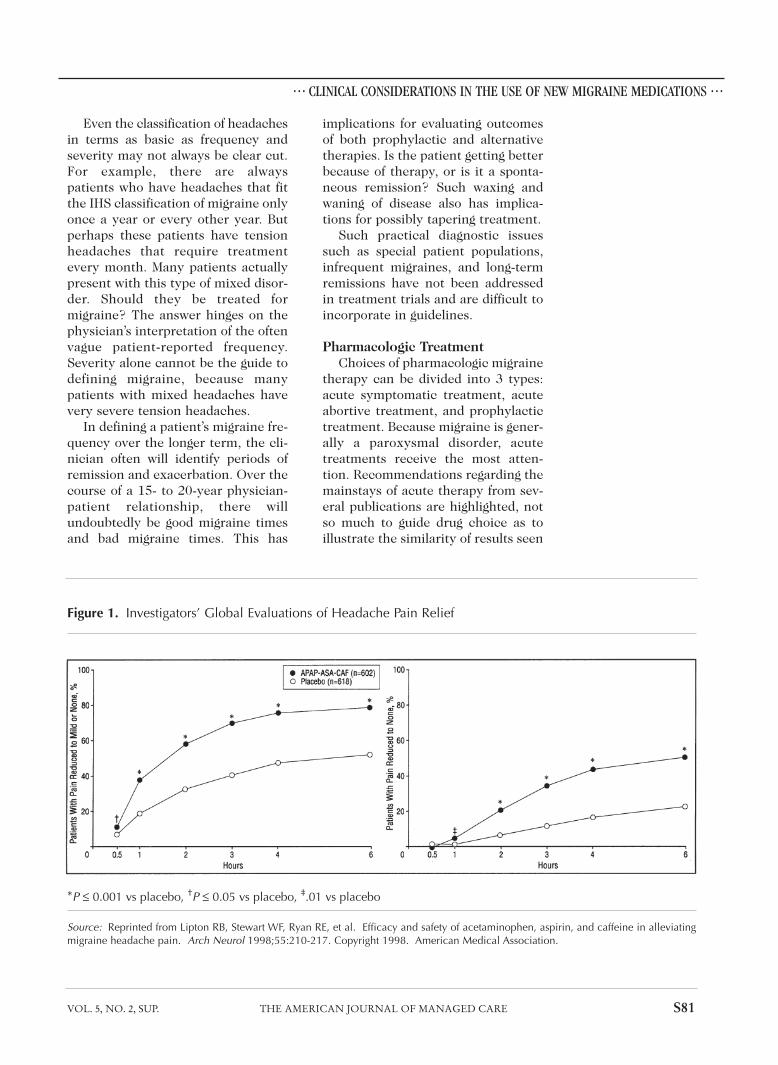
Figure 1. Investigators’ Global Evaluations of Headache Pain Relief
*P ≤ 0.001 vs placebo, †P ≤ 0.05 vs placebo, ‡.01 vs placebo
Source: Reprinted from Lipton RB, Stewart WF, Ryan RE, et al. Efficacy and safety of acetaminophen, aspirin, and caffeine in alleviatingmigraine headache pain. Arch Neurol 1998;55:210-217. Copyright 1998. American Medical Association.

S82 THE AMERICAN JOURNAL OF MANAGED CARE FEBRUARY 1999
. . . SYMPOSIUM PROCEEDINGS . . .
with these classes of available agents.The over-the-counter (OTC) med-
ications are still the mainstays ofacute symptomatic treatment. Mostheadache patients have some person-al history of using aspirin and aspirin-caffeine combination products by thetime they visit a physician. Potentialoveruse of these products should bediscussed with patients who consulttheir physicians.
In a recent double-blind, placebo-controlled trial, the nonprescriptioncombination of acetaminophen,aspirin, and caffeine was highlyeffective in reducing migraineheadache pain as well as alleviatingnausea, photophobia, and phono-phobia (Figure 1).2 In this study ofmore than 100,000 migraineurs whosuffered moderate to severe pain,the pain was reduced to mild ormoderate after 2 hours in 59.3% ofthe 602 drug-treated patients vs
32.8% of the 618 placebo-treatedpatients (P < 0.001). The drug com-bination was well tolerated in thispopulation.
The nonsteroidal anti-inflammato-ry drugs (NSAIDs), which were intro-duced 10 to 20 years ago, led to thefirst revolution in acute migrainetherapy.3 Nonsteroidals such asibuprofen, naproxen sodium, andketorolac have now become staples ofmigraine management.
With the transition of severalNSAIDs to OTC status, many patientsnow present to the headache clinicwho are already self-medicating atprescription-level doses. With somany potent and potentially toxicOTC options for headache pain,patients should always be questionedabout any history or continuing pat-tern of self-medication.
For treatment of more severeheadaches, combination productsthat contain aspirin or acetamino-phen plus a sedative (for example,butalbital) or a mild vasoconstrictor(for example, isometheptene) areoften used.4 A mild sedative such asdichloralphenazone is also sometimespart of the combination. Becausethese combination products havebeen available for years, most physi-cians are familiar with their limita-tions, such as the addictive potentialof products containing barbituratesand the contraindications of prepara-tions containing isometheptene inpatients with glaucoma, hyperten-sion, or liver disease, as well as thosetaking monoamine oxidase inhibitors(MAOIs).
In terms of abortive therapies forsevere headaches, the main choicesare medications containing ergota-mine and the selective serotonin ago-nist medications. Algorithms havebeen created by many practitionersto aid in selecting particular agents atparticular times; one such algorithmis shown in Table 2. For the very busyprovider, such charts can be valuable
Table 2. Algorithm for Migraine Management
STAGE Mild Moderate Severe
CHARACTERISTICS Occasional Moderate or Severe headachemild headache, severe or frequentno nausea or headache moderate-severevomiting with or headache,
nausea or nausea +/orvomiting vomiting,
functionalimpairment
TREATMENT OTC analgesic Combination NSAIDNSAID analgesic Triptan
NSAID Ergot alkaloidTriptan AntiemeticErgot alkaloid Prophylactic Antiemetic medication

VOL. 5, NO. 2, SUP. THE AMERICAN JOURNAL OF MANAGED CARE S83
. . . CLINICAL CONSIDERATIONS IN THE USE OF NEW MIGRAINE MEDICATIONS . . .
in treating the majority of patients;however, they have major limitations.
Many migraine patients have mild,moderate, and severe headacheepisodes rather than stages character-ized by increasing headache severity.The patient may require medicationfrom each category to manage indi-vidual migraines. “Staged” is a termused in managed care to indicate thetypes of treatment to be covered at agiven stage of a disease. It is not wellsuited to migraine, where the numberof exceptions approaches the rule.The primary care practitioner mustappreciate the potential need to pre-scribe numerous migraine medica-tions for an individual patient.Because of the explosion of new trip-tan medications, another layer ofcomplexity arises. The following twosections review the new medicationsand summarize their similarities anddifferences.
ErgotaminesErgot alkaloids have been used as
antimigraine therapy for more thanhalf a century. Patients can now takedrugs containing ergotamines orally,sublingually, rectally, intramuscular-ly, intravenously, or intranasally.Some products are combined withcaffeine or a barbiturate. Because oftheir long history of use, most physi-cians know that the ergotamines arerelatively nonselective pharmacologicagents that affect adrenergic anddopaminergic receptors as well asserotonergic sites. Nausea and vomit-ing, symptoms that are already pres-ent in many patients with severemigraine, occur in one or two of every10 patients who take ergotamine andremain a major drawback.4
Because of the erratic gastroin-testinal absorption of oral ergotamineproducts, injectable or nasal forms ofdihydroergotamine (DHE) are oftenpreferred in severe migraine. DHEnasal spray is a unique way to deliverDHE intranasally and has long been
available for parenteral administra-tion. Although DHE is effective whenit is given to the patient intramuscu-larly, the injection site is usuallypainful, making this method unac-ceptable for many patients.
DHE nasal spray was evaluated in adouble-blind, placebo-controlled studyin which 70% of the patients reportedthat their headache had resolved at 4hours. Only 14% of the patients inwhom the headache had completelyresolved reported a recurrence within24 hours. The rates of nausea withthe 2-mg dose of DHE were notmarkedly higher than those seen inthe placebo group.5
DHE spray offers migraine patientsan important option for aborting orgreatly ameliorating migraine pain byproviding once-a-day dosing with alow recurrence rate. Use of the pres-ent DHE delivery system is awkwardcompared with sumatriptan nasalspray. An improved nasal deliverydevice could further improve the easeof self-administration.
TriptansThe selective 5-HT1 agonists have
been designed to target the subset ofneurotransmitter receptors implicat-ed in migraine pathophysiology with-out disturbing noninvolved receptors.Although the vascular and neurogenicactions of these drugs are still beingdebated, these new agents havedemonstrated efficacy in relievingacute migraine pain and decreasingnausea and vomiting.
There are now 4 triptans on themarket (Table 3). The first triptan tobe approved by the Food and DrugAdministration (FDA) was sumatrip-tan, which was released in 1993. Itwas evaluated in a double-blind,placebo-controlled clinical trial as a6- or 8-mg subcutaneous injection.Pain severity was assessed at 30, 60,and 120 minutes after treatment,which produced statistically signifi-cant response rates of about 50%,

S84 THE AMERICAN JOURNAL OF MANAGED CARE FEBRUARY 1999
. . . SYMPOSIUM PROCEEDINGS . . .
70%, and 90%, respectively. The differ-ence between the 6- and 8-mg dose wasnot significant,6 and the drug wasapproved by the FDA at the lower dose.
Trials with the oral tablets demon-strated similar efficacy with a sloweronset of action.7,8 The optimum doseof oral sumatriptan was recently eval-uated in a controlled study involving1003 patients that compared 25-, 50-,and 100-mg doses. Both the 50- and100-mg doses were more effectivethan the 25-mg dose, and the 50-mgdose was associated with fewer sideeffects than the 100-mg dose.9 Asmight be expected, the nasal sprayhad a more rapid onset than thetablets, but it was less than theinjectable. The 5-mg dose is lesseffective than the 20-mg dose, 45% to49% vs 60% to 64% (PI Imitrex NasalSpray), making the higher dose com-parable to the injectable or the 50-mgoral dose. The newer triptans are alloral preparations, of which naratrip-tan has the longest half-life. The effi-cacy was 68%, compared with placebo
4 hours after a dose in a double-blindtrial.10 Zolmitriptan and rizatriptanhave also been evaluated in double-blind, placebo-controlled trials anddemonstrated efficacy similar to thatof sumatriptan and naratriptan.11,12
Rizatriptan is available as a tablet anda melt, the MLT. The melt disinte-grates quickly when placed on thetongue, which does not result in morerapid absorption but increases theease of administration.
These triptan studies exemplifythe best and worst that published evi-dence can offer the busy practitioner.On the one hand, they clearlydemonstrate that the new agents areeffective in about 60% to 80% ofpatients, which is about double theefficacy of placebo, and that themigraineur’s quality of life can beimmensely improved; on the otherhand, they offer little guidance interms of which agent to choose andwhat to do when it fails.
Despite differences in receptor-binding affinities and pharmacokinet-
Table 3. Triptans 5 HT1 Agonists
*The maximum in 24 hours is twice the maximal initial dose with the exception of rizatriptan.
t 1/2 (hours) Cost Maximal Initial Dose Maximal in 24 Hours
Sumatriptan (Imitrex)
injection s.c. 6 mg 2 $$$ 6 mg 12 mg
tablets 25, 50 mg 2 1/2 $ 100 mg 200 mg
nasal spray 5, 20 mg 2 $ 20 mg 40 mg
Zolmitriptan (Zomig)
tablets 2.5, 5.0 mg 3 $ 5 mg 10 mg
Naratriptan (Amerge)
tablets 1, 2.5 mg 6 $ 2.5 mg 5 mg
Rizatriptan (MAXALT) 2-3 $ 10 mg *30 mg
tablets, MLT (5, 10mg)

VOL. 5, NO. 2, SUP. THE AMERICAN JOURNAL OF MANAGED CARE S85
. . . CLINICAL CONSIDERATIONS IN THE USE OF NEW MIGRAINE MEDICATIONS . . .
ic distribution, the selective serotoninagonists appear to be very similar interms of clinical effectiveness and tol-erance. They are similar with regardto side effects, contraindications, andprescribing limitations when used inpregnant women, the elderly, andthose with renal failure or liver dis-ease. The use of selective serotoninagonists is contraindicated in thepresence of coronary artery diseaseor in patients who are at risk for coro-nary artery disease. Similarly, effica-cy distinctions between members ofthis class are difficult to make at thistime.
Recent publications that providedirect comparative data suggest thatthe oral agents are quite similar interms of efficacy and side effects.13,14
In terms of cost, injectable sumatrip-tan is the most expensive.
Because of a lack of consensusregarding the differences betweenproducts, most physicians now relyon their own experiences withpatients to guide drug selection. Inmost cases, the choice among triptanagents is less important than that ofthe route of administration. Thetradeoffs involve the fast action ofthe injectables and the nasal sprayscompared with their slightly higherlevels of side effects. Many patientsreport more intense paresthesia, tin-gling, and tightness in the chest, aswell as intensification of theheadache when the injectable andspray routes are used. On the otherhand, the tablets produce fewer sideeffects, but they take longer to pro-vide relief.
At present, primary care physi-cians are trying to keep up with anexplosion of knowledge in all areas ofmedicine, of which headache is justone small niche. Whereas most physi-cians are very comfortable advisingpatients on the use of OTC analgesicsand NSAIDs, they increasingly ask forhelp in the selection and use of thenew DHE spray and the 5-HT1 ago-
nists. Physicians who do not see largenumbers of patients with severeheadaches often are especially hesi-tant to prescribe these new products.A consensus on treatment guidelineswill be especially useful in encourag-ing such physicians to treat moderateto severe headaches more responsive-ly at the primary care level.
Dosing is another problem thatmust be addressed by clear guide-lines. Primary care physicians oftendose the new agents inadequately andthen seek a referral through theirmanaged care group when drug ther-apy fails. The typical patient com-plaint related to underdosing is thatthe headache went from a level 8 to alevel 4, but then it returned to level 8at 4 hours. Because migraines areknown to last from 4 to 72 hours andthe half-lives of these drugs are only1.5 hours to 6 hours for the triptansand about 10.5 hours for DHE, theneed for multiple dosing in manypatients should be no surprise. Insuch a common situation, the criticalmessage for physicians involves notthe particular agent selected but ade-quate dosing and redosing with thatagent. Many patients require multipledosing, while at the same time dosage
“Dosing is another problem that must beaddressed by clear guidelines. Primary carephysicians often dose the new agents inadequately and then seek a referralthrough their managed care group whendrug therapy fails.”
—Constance Johnson, MD

limits must be observed. For busypractitioners who are struggling toremember all this dosing information,an easy reminder is that the maxi-mum triptan dose in 24 hours is 2times the maximal initial dose, withthe exception of rizatriptan, thenewest product, for which the maxi-mum dose is 3 times the maximuminitial dose.
Other Current Issues• The use of DHE and the triptans is
contraindicated in patients whohave coronary artery disease orcoronary vasospasm. Chest symp-toms and coronary vasoconstric-tion occur with the use of DHEand triptans.15 Migraine can per-sist to age 50, 60, or 70, at whichpoint coronary artery disease isalready rampant. Given thispotential for coronary vasocon-striction, how can a physicianmanage the patient who continuesto suffer migraines during thesehigher-risk years?
• At the other end of the age scale,data are beginning to emergeregarding the use of triptans inchildren. A downward adjustmentof doses, for example use of suma-triptan 25-mg tablets and 5-mgnasal spray, appears to providethe needed benefit.
• Although current package insertrecommendations advise thattriptans should not be mixed witheach other or with ergotamine,many migraine clinics are usingthese agents in close proximity.For example, if a patient is given asumatriptan injection for a rapidlyaccelerating headache and theheadache recurs, some cliniciansmay give naratriptan tablets anhour or two after the injection.
• One of the widest gaps in ourknowledge of dosing concerns theupper limit of triptans or DHE. Wesee no physical or psychologicaltolerance to these drugs, so howmany doses can a patient take in aweek or a month? Even in theabsence of evidence, many healthplans are arbitrarily allowing onlytwo treatments per week or 6 to 8per month. This can be a seriousproblem for many lower incomemigraine patients.
• Paradoxically, this same healthplan may allow the patient to takepropranolol for prophylaxis everyday. Certainly, this beta-blockerhas a lower cost per pill, but theevidence for its efficacy in preven-tion is slim, and there may beother considerations, such as a
S86 THE AMERICAN JOURNAL OF MANAGED CARE FEBRUARY 1999
. . . SYMPOSIUM PROCEEDINGS . . .
Figure 2. The Physician’s Dilemma: Moving From Core Concepts
Although most primary care physicians are aware of the core concepts in the diag-nosis and treatment of migraine, effective treatment is often stymied by the lack ofanswers to complex questions involving individual patients. Practical treatmentguidelines, while not answering all questions, should encourage improvedheadache therapy in primary care and prompt referral when appropriate.
Mild Moderate Severe
Analgesics Rx NSAIDs DHEOTCs Combinations Triptans↔ ↔

VOL. 5, NO. 2, SUP. THE AMERICAN JOURNAL OF MANAGED CARE S87
. . . CLINICAL CONSIDERATIONS IN THE USE OF NEW MIGRAINE MEDICATIONS . . .
reduction in the patient’s exercisetolerance, which are completelyoverlooked.
• In women who suffer menstrualmigraines and are able to predicttheir migraines, prophylactic useof triptans may be indicated.Sumatriptan 25 mg 3 times a dayled to a marked reduction in fre-quency.16
• Finally, should triptans be usedfor moderate and severe tensionheadache? Many migrainepatients report pain relief whenthey use triptans for their tensionheadaches.17
The foregoing are just a few of theissues that practicing physicians mustaddress today. Although most careproviders are aware of the core con-cepts in the diagnosis and treatmentof migraine, truly effective treatmentis often stymied by a lack of answersto these types of complex questionsas they relate to individual patients(Figure 2). Consensus-based practiceguidelines may address some of theseissues, but a continued dialoguebetween specialists and primary carephysicians will be necessary to fill inthe remaining gaps as experiencewith the new agents grows.
. . . DISCUSSION HIGHLIGHTS . . .
At the conclusion of Dr. Johnson’spresentation, symposium participantsdiscussed the use of the new migrainemedications.
Dr. Brown: If a patient is not respond-ing to sumatriptan despite adequatedosages over a 2-month period, wouldyou switch to another triptan? Or arethe triptans all alike?
Dr. Johnson: If my patients are on 50mg of sumatriptan and I take them toa 100-mg dose and they still do notrespond, I would consider switchingto another triptan. Some patients
respond to a different member of thesame class.
Dr. Gallagher: We just completed astudy of more than 1600 patients thatcompared sumatriptan and zolmitrip-tan and showed some differencesbetween the agents. The average fam-ily doctor might not recognize thesedifferences, but the neurologist orspecialist would.
Dr. Mondell: What is the current sta-tus of the warning to reduce the doseof rizatriptan in patients who are alsotaking propranolol?
Dr. Brown: Apparently this warningwas added because propranololdecreases the hepatic clearance of thetriptan by about 70%. The recommen-dation is to use a 5-mg tablet insteadof a 10-mg one. We may learn moreabout this interaction in the future,including whether other beta-blockersand triptans share this interaction,but for now that is the recommenda-tion. The other precaution in copre-scribing concerns the triptans and theselective serotonin reuptakeinhibitors (SSRIs).
Dr. Johnson: But that is a very idio-syncratic reaction, as in the case ofselegiline and the SSRIs. Certainly, ifyour patient is on an SSRI and youadd a triptan and they get flushingand weakness and so forth, the inter-action is there. However, practicallyspeaking, this is not a big issue.
Dr. Brown: We caution physiciansabout using MAOIs with the triptans,but we do not say they cannot givethem together. However, concomi-tant use of MAOIs is contraindicat-ed with all the triptans except nara-triptan (Amerge), because MAOIscan reduce the clearance of triptans,resulting in increased plasma con-centrations and prolonged elimina-tion from the body. Concurrentadministration of MAOIs or their use

S88 THE AMERICAN JOURNAL OF MANAGED CARE FEBRUARY 1999
. . . SYMPOSIUM PROCEEDINGS . . .
within 2 weeks of their discontinua-tion is contraindicated. MAOIs do notsignificantly affect the elimination ofnaratriptan; however, their use is notcontraindicated with this specifictriptan.
Dr. Lake: From our perspective in acomprehensive/tertiary care headachecenter, we are seeing an increasingnumber of patients using sumatriptandaily. As an extreme example, we hadone cluster headache patient taking itevery 3 to 4 hours for 2 years, as wellas prednisone bursts every 2 weeks.His initial request for referral to ourcenter at the beginning of this 2-yearspan had been denied by the insur-ance company, which continued topay a large amount of money to med-icate a patient who remained disabled.Our perspective is that these drugsmay actually contribute to recurrent,rebound pain in some patients, andthat this overreliance on acute careactually crosses over into prophylacticcare in an intractable case. Inpatienttreatment for triptan withdrawal andappropriate prophylactic medicationled to a significant reduction inheadaches, improved functioning, andreduced costs over the long term.
Dr. Johnson: There is no evidencethat the acute treatment agents do ordo not cause rebound. Clearly, weshould not think about them in thesame way as we think about narcotics.However, we all see that small per-centage of patients who blur the linebetween acute and prophylactic care.Of course, 2 or 3 years from now wemay have a triptan that possesses nocardiac effects and can be used safelyevery day, cost issues aside. In addi-tion, if our guidelines set usage limitson triptan, we need to provide physi-cians with longer time frames. Somepatients tend to have 5 attacks con-centrated in 1 month and then noattacks for 2 months. Perhaps we needto specify an average number of doses
over several months rather than somany doses in 1 week or 1 month.
Dr. Gallagher: Keep in mind as wellthat the earlier the intervention, theless likelihood of the need for a repeatdose. If we can educate the patient torecognize and treat headaches at themoderate stage, he or she might needonly one pill instead of two.
Dr. Lake: Beyond the pharmaceuticaloptions, there may be some patientswho require a multidisciplinary sys-tem of care. We are beginning to rec-ognize this progression of cases inwhich the intractable patient con-tributes more than might be expectedto the overall impact on productivityand healthcare costs. The multidisci-plinary approach, including the psy-chological aspects, may very well fitwithin a new cost-justified diseasemanagement approach.
Dr. Gallagher: Many of us have men-tioned the need for head-to-headstudies. These studies are very costlyand not above criticism in terms ofdesign. An alternative to large, expen-sive, head-to-head trials is to use the“numbers needed to treat” approach,which essentially permits comparisonof the package insert study data andother studies with data on the place-bo controls.
Dr. Mondell: I believe it is dangerousto compare package inserts; it is likecomparing apples and oranges, withdifferent populations being treated.
Dr. Gallagher: Admittedly, it is notideal. However, for managed carecompanies or physicians who need tocompare drugs and lack the head-to-head data, it is valuable as a practicalcomparison.
Dr. Schweitzer: Even if we assumethat we see differences in efficacy orsafety between two treatment options,

VOL. 5, NO. 2, SUP. THE AMERICAN JOURNAL OF MANAGED CARE S89
. . . CLINICAL CONSIDERATIONS IN THE USE OF NEW MIGRAINE MEDICATIONS . . .
will the ideal managed care protocolthen mandate use of the most effec-tive agent?
Ms. Bowman: New drugs come alongevery day. Isn’t there a place for steptherapy here?
Dr. Ward: Tailored therapy, ratherthan step therapy, is probably morecost effective for these migrainepatients. Not every migraine patienthas the same kind of attack eachtime, so you must tailor treatment towhatever is going on. If the attack ismild and the patient is not sick,maybe acetaminophen-aspirin-caf-feine (Excedrin Migraine) wouldwork. However, if the patient wakesup with the headache from hell andhe or she is in the bathroom vomiting,then maybe the patient wants asumatriptan injection or a nasal spraythat contains sumatriptan or DHE. Ifyou start with a “one-size-fits-all”protocol, many patients will be dissat-isfied.
Dr. Mondell: But simple guidelinescan work well. I am not suggestingthat you should always start withdrug X for a headache of Y intensity.The ideal guideline would generallyinclude suggested classes, the timingof dosage, and the routes of adminis-tration. For example, if a patient hassignificant nausea and emesis, youwould want to use the parenteralforms, such as nasal sprays. We arenot talking about a complex algo-rithm.
Dr. Parham: When we apply a set ofrecommendations to local practices,we need things that are consistentand nationally recognized as beingvalid. The recommendations alsoneed to be flexible enough to allowfor repeated application during apatient’s natural history and to per-mit the introduction of new thera-pies as they become available.
Dr. Mondell: Obviously, the recom-mendations need to be fluid. Thepoint is that we need to start some-where. We do not have such a set ofrecommendations now. We need toinitiate a habit of consistent therapyso we can validate it and move on.
. . . REFERENCES . . .
1. Headache Classification Committee of theInternational Headache Society. Classificationand diagnostic criteria for headache disorders,cranial neuralgias and facial pain. Cephalalgia1988;8(suppl 7):1.2. Lipton RB, Stewart WF, Ryan RE, et al.Efficacy and safety of acetaminophen,aspirin, and caffeine in alleviating migraineheadache pain: three double-blind, random-ized, placebo-controlled trials. Arch Neurol1998;55:210-217.3. Pradalier A, Clapin A, Dry J. Treatmentreview: Non-steroid antiinflammatory drugsin the treatment and long-term prevention ofmigraine attacks. Headache 1988;28:550-557. 4. Peroutka SJ. Drugs effective in the therapyof migraine. In: Hardman JG, Limbird LE, eds.Goodman & Gilman’s The PharmacologicalBasis of Therapeutics, 9th ed. New York:McGraw-Hill, 1996:487-502.5. Gallagher MR, for the DihydroergotamineWorking Group. Acute treatment of migrainewith dihydroergotamine nasal spray. ArchNeurol 1996;53:1285-1291.6. The Subcutaneous SumatriptanInternational Study Group.Treatment ofmigraine attacks with sumatriptan. N Engl JMed 1991;325:316-321.7. Pramod R, Saxena PR, Tfelt-Hansen P.Sumatriptan. In: Olesen J, Tfelt-Hansen P,Welch KMA, eds. The Headaches. NewYork: Raven Press, 1993:329-341.8. Salonen R, on Behalf of the Study Group,Glaxo Wellcome OY and Turku HeadacheCenter, Turku, Finland. Patient preferenceamong 25 mg, 50 mg, and 100 mg oraldoses of sumatriptan. EFNS Symposium,Rome, Italy, 1996.9. Pfaffenrath V, Cunin G, Sjonell G,Prendergast S. Efficacy and safety of suma-triptan tablets (25 mg, 50 mg, and 100 mg)in the acute treatment of migraine: defining

S90 THE AMERICAN JOURNAL OF MANAGED CARE FEBRUARY 1999
. . . SYMPOSIUM PROCEEDINGS . . .
the optimum doses of oral sumatriptan.Headache 1998;38:184-190.10. Mathew NT, Asgharnejad M, PeykamianM, Laurenza A, on behalf of the NaratriptanS2WA3003 Study Group. Naratriptan iseffective and well tolerated in the acutetreatment of migraine: Results of a double-blind, placebo-controlled,crossover study.Neurology 1997;49:1485-1490. 11. Ferrari MD. 311C90: Increasing theoptions for therapy with effective acuteantimigraine 5HT1B/1D receptor agonists.Neurology 1997;48(suppl 3):S21-S24.12. Kramer MS, Matzura-Wolfe D, GetsonA, et al. Placebo-controlled, double-blindstudy of rizatriptan in multiple attacks ofacute migraine. Neurology 1997;48(suppl2):A68-A69.13. Visser WH, Teall JH, Malbecq W, et al.
Early onset of action of rizatriptan versussumatriptan in the acute treatment ofmigraine. Headache 1997;37:334-335.14. Lines C, Visser WH, Vandormael K, et al.Rizatriptan 5 mg versus sumatriptan 50 mg inthe acute treatment of migraine. Headache1997;37:319-320. 15. VanDenBrink AM, Reekers M, Bax WA,Ferrari MD, Saxena PR. Coronary side-effectpotential of current and prospective antimi-graine drugs. Circulation 1998;98:25-30.16. Newman LC, Lipton RB, Lay CL,Soloman S. A pilot study of oral sumatritpanas intermittent prophylaxis of menstruation-related migraine. Neurology 1998;51:307-309. 17. Packheiser A, Levien T. Features of avail-able triptans. Pharmacist's Letter 1998:Doc140809.