clinical aspects of congenital heart disease in mongolism
TRANSCRIPT

Clinical Aspects of Congenital Heart Disease in Mongolism
REDA M. SHAHER, MD MATTHEW A. FARINA, MD IAN H. PORTER, MD MONICA BISHOP, MD
Albany, New York
From the Departments of Pediatrics amnd Pathology, Albany Med,ical Center Hospital and Albany Medical College, Albany, N. Y. Manuscript received February 25’, 1971, re- vised manuscript received June 29, 1971, accepted July 23, 1971.
Address for reprints: R. M. Shaher, MD, Division of Pediatric Cardiology, Albany Medical Center, Albany, N. Y. 12208.
The clinical course of 39 children with mongolism and congenital heart disease is presented. In all the diagnosis was confirmed by cardiac catheterization, angiocardiography and chromosomal studies. Patients were classified into 3 groups according to the hemodynamic findings as follows: group I, 6 patients with right ventricular outflow tract obstruction; group II, 22 patients with pulmonary hypertension at systemic levels; and group Ill, 11 patients with normal or slightly increased pulmonary vascular resistance. The underlying cardiac pathologic findings in these 3 groups are presented. In group I, the mortality rate was 33 percent, and hypoxia was the major problem. Recurrent chest infections and congestive heart failure developed in patients in group II, and the mortality rate was 36.5 percent. Eisen- menger’s reaction developed by age 3 years in the majority in this group. Patients in group III did extremely well, and most were asymp- tomatic.
The occurrence of congenital heart disease in mongolism is well recognized. Most studiesl-* have dealt with the incidence and type of congenital heart disease in this condition ; very few5 have dis- cussed clinical and hemodynamic aspects. This paper reviews the clinical course and the hemodynamic findings of 39 children with mongolism and congenital heart disease seen at the Albany Medi- cal Center Hospital in the 4 years from 1967 to 1970.
Material
Thirty-nine children with mongolism and congenital heart disease underwent cardiac catheterization and angiography at Albany Medical Center Hospital between 1967 and 19’70. Chromosomal studies demon- strated trisomy 21 in all. There were 22 male and 17 female patients aged 1 day to 14 years. Eleven patients underwent heart surgery during the period of observation. Eleven patients died during the same time, and autopsy examination was performed in 8. Each patient was evalu- ated clinically, and a chest roentgenogram and electrocardiogram were obtained during each visit. The criteria employed for signs of right and left ventricular hypertrophy in the electrocardiogram are those sug- gested by Vince and Keith.6
All patients were studied by cardiac catheterization and angiocardi- ography. A left to right shunt at any level was considered present if there was a step-up in oxygen saturation of 7 percent or more. Shunt reversal was considered present if there was a difference of 5 perce,ntl or more in oxygen saturation between the pulmonary venous and sys- temic arterial blood samples. In many patients, dye-dilution curves ob- tained by injecting Cardio-Green@ dye into the right side of the heart were used to confirm the site of shunt reversal. The term Eisenmenger’s syndrome or reaction was used to signify shunt reversal at atrial, ven- tricular or pulmonary arterial levels secondary to pulmonary hyperten- sion. Whenever possible, patients were investigated by several injec-
VOLUME 29, APRIL 1972 497

SHAHER ET AL.
tions of contrast medium into the cardiac chambers and great vessels. According to the hemodynamic findings, patients were classified into 3 groups as follows :
Group I: Six patients with right ventricular out- flow tract obstruction: 4 with tetralogy of Fallot; 1 with double-outlet right ventricle and pulmonary ste- nosis; and 1 with pulmonary atresia and ventricular septal defect and patent ductus’arteriosus.
Group II: Twenty-two patients with pulmonary hy- pertension at systemic levels: 7 with complete atrio- ventricularis communis; 4 with ventricular septal de- fect; 4 with ventricular and atria1 septal defects ; 2 with ventricular septal defect and patent ductus ar- teriosus; 1 with ventricular and atria1 defects and patent ductus arteriosus ; 2 with common ventricle ; 1 with double-outlet right ventricle; and 1 with car pul- monale, ventricular septal defect and patent ductus ar- teriosus.
Group III: Eleven patients with normal or slightly increased pulmonary vascular resistance: 4 with ven- tricular septal defect; 1 with ventricular and atria1 sep- tal defects; 3 with patent ductus arteriosus; 2 with atria1 septal defect and patent ductus arteriosus ; and 1 with ostium primum atria1 septal defect.
Findings
Incidence of Cardiac Defects
Only 10 patients in this series had an isolated defect-a patent ductus arteriosus in 3, a complete atrioventricularis communis in 3, a ventricular septal defect in 3, and an ostium primum atria1 septal defect in 1. The remaining 29 patients had multiple defects. Sixty-six defects occurred in the 39 patients. The incidence of these defects was as follows : ventricular septal defect, 18 ; patent duc- tus arteriosus ; 15 ; atrioventricularis communis, 11; atria1 septal defect (primum in 1), 9 ; tetralogy of Fallot, 4 ; peripheral pulmonary arterial steno- sis, 4 ; double-outlet right ventricle (1 with pulmo- nary stenosis), 2 ; common ventricle, 2 ; pulmonary atresia, 1; and endocardial fibroelastosis, 1.
Pathology
The pathologic findings in the 8 autopsy cases in this series were classified according to the ma- jor cardiac defect.
Atrioventricularis communis: Four patients were found to have complete atrioventricularis communis at autopsy. In all 4, there was a single atrioventricular (A-V) valve with an anterior and a posterior leaflet. Associated defects included pat- ent ductus arteriosus in 1, patent ductus arterio- sus and endocardial fibroelastosis of both ven- tricles in 1, common ventricle with a rudimentary outlet chamber and normally related great arteries and a small ductus in 1, and pulmonary infundibu- lar stenosis and origin of both aorta and pulmo- nary artery from the right ventricle in 1.
Ventricular septal defect: A ventricular septal defect as the major pathologic finding was present in 3. In 2 the defect measured more than 1 cm2 in
diameter; in 1 it was 1 by 1 mm. In 2 patients the ventricular septal defect was in the membraneous septum, and associated defects included patent ductus arteriosus in 1 and patent foramen ovale in 1. The third patient had a ventricular septal defect of the A-V canal type and an ostium secundum atria1 septal defect.
Atria1 septal defect: In 1 patient an ostium secundum atria1 septal defect, 4 by 4 mm, was the major abnormality in 1 patient who also had a small patent ductus arteriosus.
Prenatal and Family History
The mean age of the mothers, when this infor- mation was available, was 33 years. One mother was between 15 and 19 years, 14 were between 20 and 29 years, 12 were between 30 and 39 years, and 10 were over 40 years of age. The mean age of the fathers, when this information was available, was 33.7 years. Two were between 15 and 19 years, 11 were between 20 and 29 years, 14 were between 30 and 39 years, and 10 were over 40 years of age.
Four patients were first-born, 11 second-born, 8 third-born, 4 fourth-born, 2 fifth-born, 2 sixth- born, 3 seventh-born, 2 eighth-born, and 1 tenth- born. No information was available in 2 cases.
A positive history of congenital heart disease was present in 2 cases. One patient had a sibling with mild muscular aortic stenosis; another had a sibling who died at birth of congenital heart dis- ease. In 2 families another sibling had mongolism, and another patient had a cousin with mongolism. Cousins of 3 other patients had, respectively, men- tal retardation, cleft palate and muscular dys- trophy.
None of the mothers had diabetes, but a history of previous abortion was obtained in 10 families. During the first trimester of pregnancy, 3 mothers had been exposed to X-radiation and 8 had a posi- tive history of medication or an infection (not rubella), or both, and 3 bleeding during this pe- riod.
Clinical Features
Physical findings : At the initial evaluation most patients were small for their age. In height, 16 children were below the third percentile, 5 be- low the tenth, 2 below the twenty-fifth, 1 below the fiftieth, and 2 below the seventy-fifth percentile. In weight, 16 children were below the third percen- tile, 5 below the tenth, 5 below the twenty-fifth, and 1 below the fiftieth percentile. Most patients remained in the same group on subsequent evalua- tions.
A heart murmur had been detected at birth in 13 patients, during the first 3 months in 14, be- tween the fourth month and first year in 7, and after the first year in 3. One patient, who died at age 3 weeks, had no murmur ; in 2 others there was
498 The American Journal of CARDIOLOGY
CONGENITAL HEART DISEASE IN MONGOLISM
no record of the age at which the murmur had been discovered.
Permanent cyanosis or cyanosis of short dura- tion was observed in 21 patients and occurred only in groups I and II. It occurred at birth in ‘7 pa- tients. Cyanosis developed in 2 patients during the fir& year of life ; in 8 others, cyanosis became no- ticeable after this period. No information was available on the onset of cyanosis in the remaining 4.
Clubbing of the fingers was noted in 10 patients, 3 in group I and 7 in group II. The youngest pa- tient in group I in whom this sign was detected at the initial cardiac evaluation was 10 months of age. Of the 7 in group II, 1 had clubbing at 10 months; the remaining 6 were 3 years of age or older at the initial cardiac examination.
Heart failure developed in the first year of life in 14 patients; 1 was in group I and had acyanotic tetralogy of Fallot, 12 were in group II and 1 was in group III. In 1 patient in group II heart fail- ure developed at age 10 years, and the condition was precipitated by acute rheumatic fever (Case 27).
Recurrent bronchitis and pneumonia and pre- cordial bulging occurred in the majority of pa- tients in group II. Attacks of pneumonia were often complicated by heart failure and cyanosis. Precordial bulging was not seen in groups I or III.
Murmurs occurred in all but 1 patient, who died at age 3 weeks with a common ventricle and a complete atrioventricularis communis. The ma- jority of patients had ejection murmurs in the pulmonary area or a loud pansystolic murmur in the third or fourth left space ; a few had both mur- murs. A continuous murmur was present in 5 pa- tients, 4 with a patent ductus arteriosus and 1 with pulmonary atresia. In 3 patients with pulmonary hypertension a short mid-diastolic murmur was also present. An additional early diastolic murmur was present in 2 patients, 1 with pulmonary hyper- tension and shunt reversal, and 1 with tetralogy of Fallot after a Brock’s procedure.
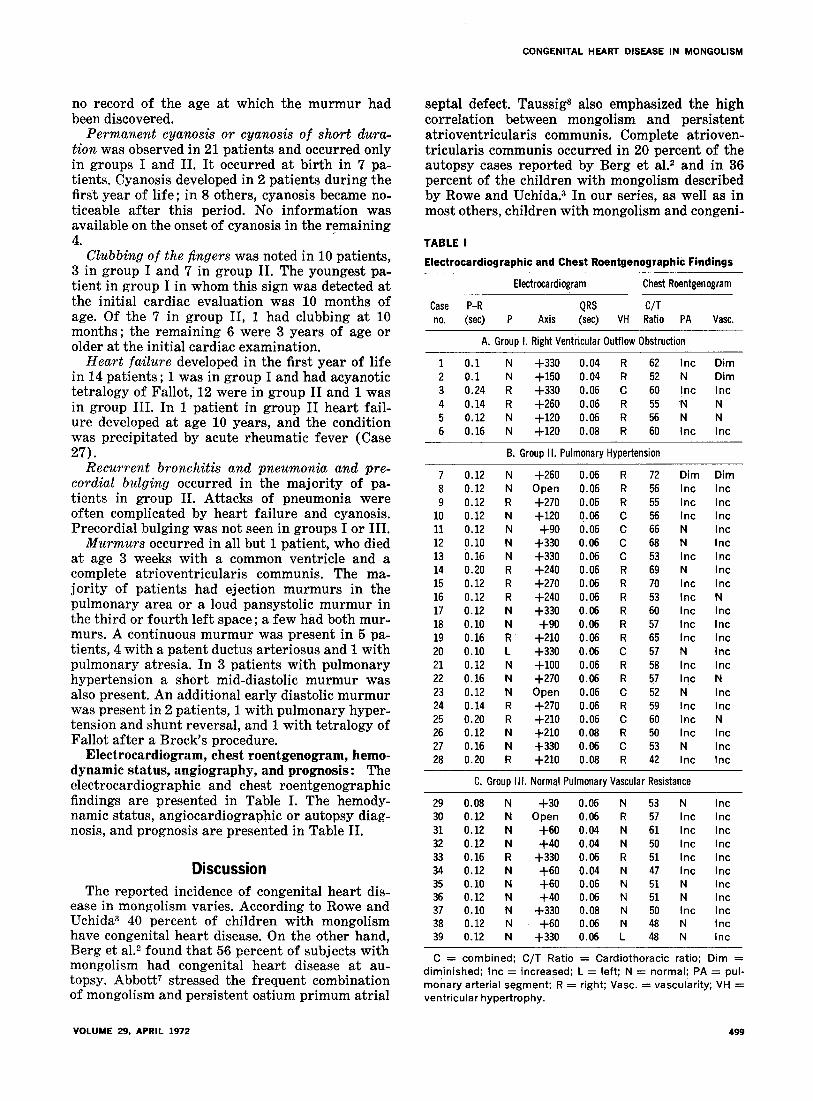
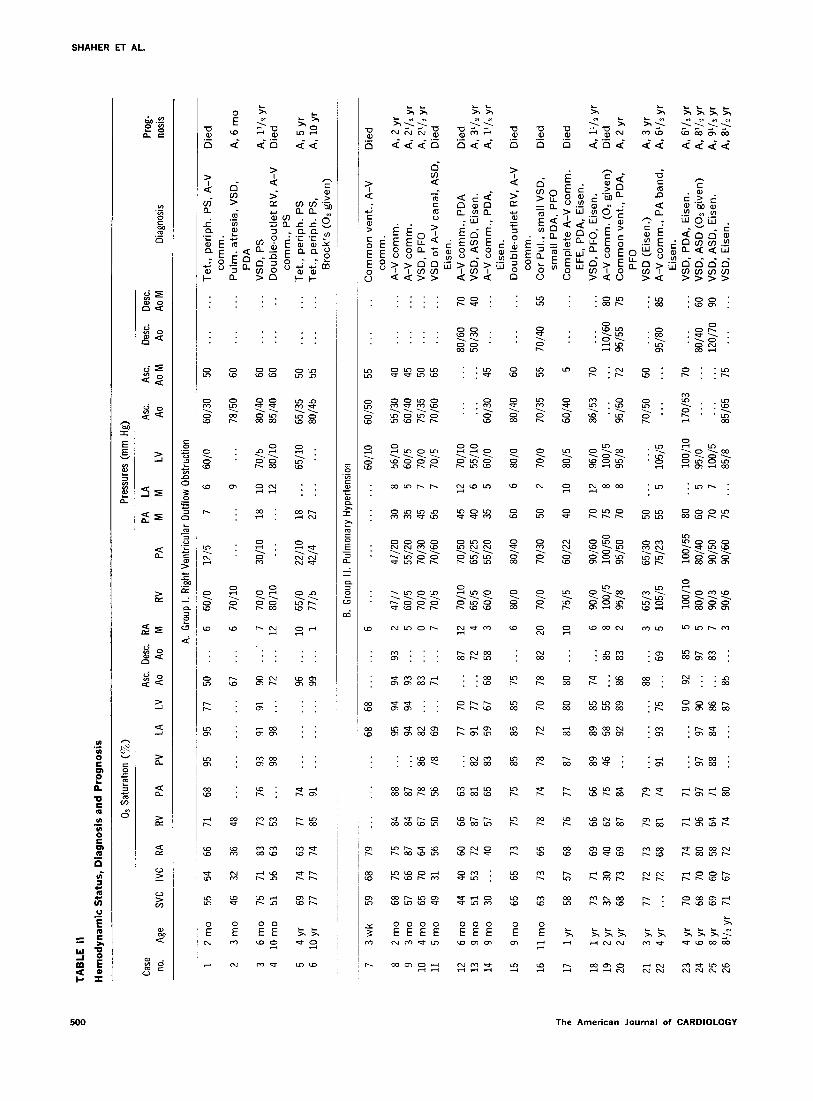
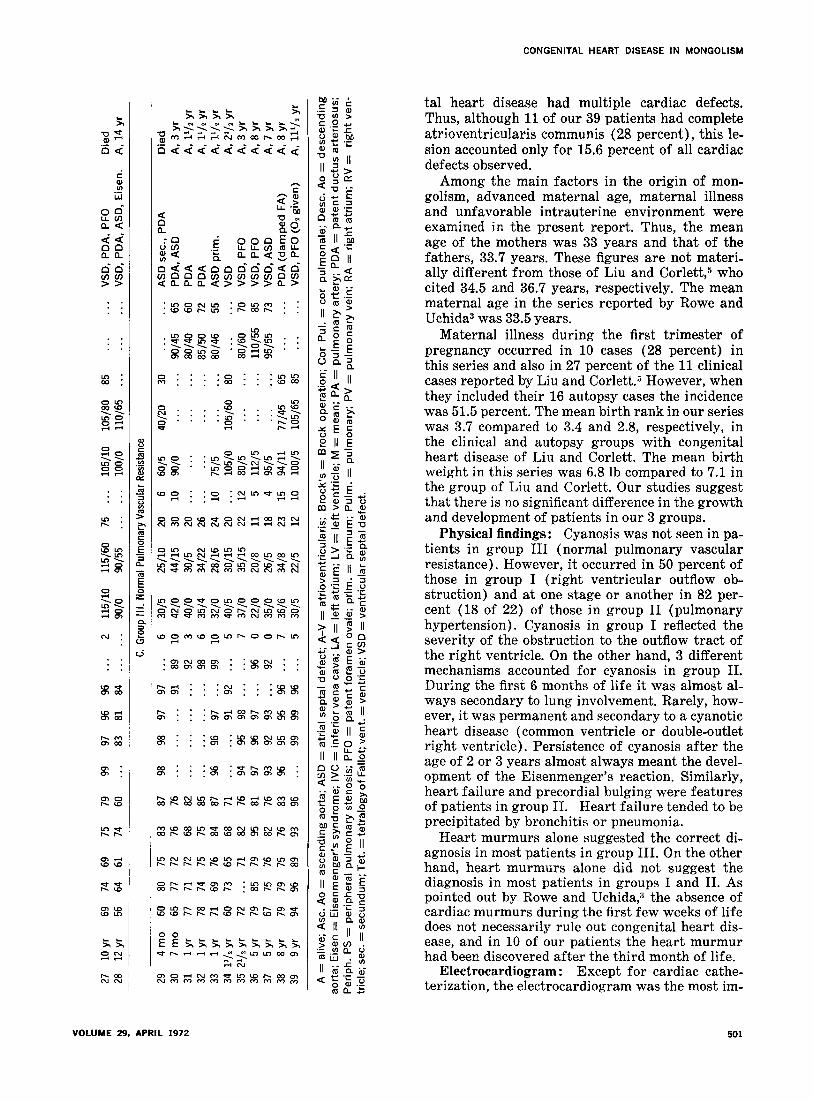
Electrocardiogram, chest roentgenogram, hemo- dynamic status, angiography, and prognosis: The electrocardiographic and chest roentgenographic findings are presented in Table I. The hemody- namic status, angiocardiographic or autopsy diag- nosis, and prognosis are presented in Table II.
Discussion The reported incidence of congenital heart dis-
ease in mongolism varies. According to Rowe and Uchida3 40 percent of children with mongolism have congenital heart disease. On the other hand, Berg et a1.2 found that 56 percent of subjects with mongolism had congenital heart disease at au- topsy. Abbott7 stressed the frequent combination of mongolism and persistent ostium primum atria1
VOLUME 29, APRIL 1972
septal defect. Taussig* also emphasized the high correlation between mongolism and persistent atrioventricularis communis. Complete atrioven- tricularis communis occurred in 20 percent of the autopsy cases reported by Berg et a1.2 and in 36 percent of the children with mongolism described by Rowe and Uchida.3 In our series, as well as in most others, children with mongolism and congeni-
TABLE I
Electrocardiographic and Chest Roentgenographk Findings
Electrocardiogram Chest Roentgenogram
Case P-R QRS C/T no. (set) P Axis (set) VH Ratio PA Vast.
A. Group I. Right Ventricular Outflow Obstruction
1 0.1 N +330 0.04 R 62 Inc Dim 2 0.1 N +150 0.04 R 52 N Dim
3 0.24 R +330 0.06 C 60 Inc Inc 4 0.14 R +260 0.06 R 55 N N 5 0.12 N +120 0.06 R 56 N N 6 0.16 N +120 0.08 R 60 Inc Inc
7 0.12 N 8 0.12 N 9 0.12 R 10 0.12 N 11 0.12 N 12 p.10 N 13 0.16 N 14 0.20 R 15 0.12 R 16 0.12 R 17 0.12 N 18 0.10 N 19 0.16 R 20 0.10 L 21 0.12 N 22 0.16 N 23 0.12 N 24 0.14 R 25 0.20 R 26 0.12 N 27 0.16 N 28 0.20 R
72 Dim Dim 56 Inc Inc 55 Inc Inc 56 Inc Inc 66 N Inc 68 N Inc 53 Inc Inc 69 N Inc 70 Inc Inc 53 Inc N 60 Inc Inc 57 Inc Inc 65 Inc Inc 57 N Inc 58 Inc Inc 57 Inc N 52 N Inc 59 Inc Inc 60 Inc N 50 Inc Inc 53 N Inc 42 Inc Inc
C. Group Ill. Normal Pulmonary Vascular Resistance
+260 0.06 R Open 0.06 R +270 0.06 R +120 0.06 c +90 0.06 C +330 0.06 c +330 0.06 c +240 0.06 R +270 0.06 R +240 0.06 R +330 0.06 R +90 0.06 R +210 0.06 R +330 0.06 c +100 0.06 R +270 0.06 R Open 0.06 C +270 0.06 R +210 0.06 C +210 0.08 R +330 0.06 C +210 0.08 R
B. Group II. Pulmonary Hypertension
29 0.08 N 30 0.12 N 31 0.12 N 32 0.12 N 33 0.16 R 34 0.12 N 35 0.10 N 36 0.12 N 37 0.10 N 38 0.12 N 39 0.12 N
+30 Open
+60 +40 +330
+60 +60 +40 +330
+60 +330
0.06 N 53 N Inc 0.06 R 57 Inc Inc 0.04 N 61 Inc Inc 0.04 N 50 Inc Inc 0.06 R 51 Inc Inc 0.04 N 47 Inc Inc 0.06 N 51 N Inc 0.06 N 51 N Inc 0.08 N 50 Inc Inc 0.06 N 48 N Inc 0.06 L 48 N Inc
C = combined: C/T Ratio = Cardiothoracic ratio; Dim = d$inished; Inc = increased; L = left; N = normal; PA = pul- monaryarterialsegment; R = right; Vast. = vascularity; VH = ventricularhypertrophy.
499
TAB
LE
II
Hem
od
ynam
ic
Sta
tus,
D
iag
no
sis
and
P
rog
no
sis
O2
Satu
ratio
n (T
O)
Pres
sure
s (m
m
Hg)
Cas
e A
sc.
Oes
c.
RA
PA
LA
A
sc.
Asc
. O
esc.
D
esc.
Pr
og-
no.
Age
SV
C
IVC
R
A
RV
PA
PV
LA
LV
Ao
Ao
M
RV
PA
M
M
LV
Ao
AoM
A
o A
o M
D
iagn
osis
no
sis
A.
Gro
up I
. R
ight
Ven
tric
ular
O
utflo
w
Obs
truc
tion
1 2
mo
55
54
66
71
68
95
95
77
50
. 6
60/O
12
15
7 6
60/O
60
/30
50
. . .
. . .
Tet.,
pe
riph.
PS
, A
-V
Die
d co
mm
.
2 3
mo
46
32
36
48
. . .
.
. 67
.
6 70
/10
. .
9 . .
78
/50
60
. .
. Pu
lm.
atre
sia,
VS
D,
A,
6 m
o PD
A
3 6
mo
75
71
83
73
76
93
91
91
90
. .:
7 70
/o
30/1
0 18
10
70
/5
80/4
0 60
. .
. . .
. VS
D,
PS
A,
l1lz
yr
4
10m
o 51
56
63
53
98
98
. .
72
.
. 12
80
/10
. .
12
80/1
0 85
/40
60
. . .
. .
Dou
ble-
outle
t R
V,
A-V
D
ied
com
m.,
PS
5 4
yr
69
74
63
77
74
. .
. .
. 96
. .
10
65
/O
22/1
0 18
. .
. 65
/10
65/3
5 50
. .
. . .
. Te
t.,
perip
h.
PS
A,
5 yr
6
10 y
r 77
77
74
85
91
. .
99
. .
1
7715
42
14
27
. . .
. . .
80/4
5 55
. .
. . .
Te
t.,
perip
h.
PS,
A,
10 y
r B
rock
’s
(02
give
n)
B.
Gro
up I
I. Pu
lmon
ary
Hyp
erte
nsio
n
7 3w
k 59
68
79
.
68
68
. . .
. 6
. .
. .
60/1
0 60
/50
55
Com
mon
ve
nt.,
A-V
co
mm
. A
-V
com
m.
A-V
co
mm
. VS
D,
PFO
VS
D
of
A-V
ca
nal,
ASD
, Ei
sen.
A
-V
com
m.,
PDA
VS
D,
ASD
, Ei
sen.
A
-V
com
m.,
PDA
, Ei
sen.
D
oubl
e-ou
tlet
RV,
A
-V
com
m.
Cor
Pu
l.,
smal
l VS
D,
smal
l PD
A,
PFO
C
ompl
ete
A-V
co
mm
. EF
E,
PDA
, Ei
sen.
VS
D,
PFO
, Ei
sen.
A
-V
com
m.
(0,
give
n)
Com
mon
ve
nt.,
PDA
. PF
O
VSD
(E
isen
.) A
-V
com
m.,
PA
band
, Ei
sen.
VS
D,
PDA
, Ei
sen.
VS
D,
ASD
(0
, gi
ven)
VS
D,
ASD
, Ei
sen.
VS
D,
Eise
n.
Die
d
8 2
mo
9 3m
o 10
4m
o 11
5
mo
68
75
75
84
88
. .
95
94
94
93
2 57
66
87
84
87
. .
. 94
94
93
. .
5
65
70
64
67
78
86
82
. 83
. .
0
49
31
56
50
56
78
69
_..
71
. 7
4717
47
120
60/5
55
120
70/o
70
/30
7015
70
/60
30
8 56
/10
35
5 60
/5
45
7 70
/o
55
7 70
15
55/3
0 40
...
...
60
/40
45
...
...
7513
5 50
...
...
70
/60
65
...
...
A,
2 yr
A
, 2V
z yr
A
, 2V
2 yr
D
ied
70/1
0 70
/50
45
12
7011
0 .
6515
65
125
40
6 55
/10
. . .
. .
60/O
55
120
35
5 60
/O
60/3
0 45
80/6
0 70
50
/30
40
. . .
. . .
12
6 m
o 13
9m
o 14
9
mo
44
40
60
66
63
. .
77
70
. . .
87
12
51
53
72
87
81
82
91
77
. .
72
4 30
. .
40
57
65
83
59
67
68
58
3
Die
d
A,
3’1%
yr
A,
llln
yr
Die
d 15
9
mo
65
65
73
75
75
85
85
85
75
. . .
6 80
/40
60
6 80
/O
80/4
0 60
50
2 16
11
mo
63
73
65
78
74
78
72
70
78
82
20
70/3
0 70
/o
7013
5 D
ied
17
1 yr
58
57
68
76
77
87
81
80
80
. .
. 10
75
15
60/2
2 40
10
80
15
60/4
0 5
. . .
. . .
Die
d
73
71
69
66
66
89
89
85
74
. .
6 32
30
40
62
75
46
58
55
. .
. 85
8
68
73
69
87
84
. . .
92
89
86
83
2
W/O
90/60
70
12
96/O
86
153
70
100/
5 10
0/50
75
8
100/
5 . ,
. . .
. 95
/8
95/5
0 70
8
9518
95
/50
72
A,
l1lz
yr
D
ied
A,
2 yr
18
1 yr
19
2
v 20
2
yr
3 yr
4
yr
. . .
. . .
110/
60
80
9515
5 75
21
22
77
72
73
79
79
, . .
. . .
. . .
88
. .
3
. . .
72
68
81
74
91
93
75
. .
69
5 65
13
65/3
0 50
. .
. . .
10
5/5
7512
3 55
5
105/
5 70
/50
60
. . .
. . .
A,
3 yr
A
, @
I2
yr
. . .
. . .
95/8
0 85
lOO
/lO
170/
53
70
95/o
.
. . .
100/
5 . .
. . .
. 85
18
8516
5 75
23
4 yr
24
6
yr
25
8 yr
26
8l
l2
yr
70
71
74
71
71
. . .
. . .
90
92
85
5 68
70
80
96
97
97
97
90
.
97
5 69
60
58
64
71
88
84
86
. .
83
7
71
67
72
74
80
. . .
. . .
87
85
. .
3
lOO
/lO
100/
55
80/O
80
/40
90/3
go
/50
90/6
90
/60
80
. . .
60
5 70
7
75
. .
A,
S1iz
yr
A,
8112
yr
A,
9112
yr
A,
8112
yr
. . .
. . .
80/4
0 60
12
0/70
90
. .
. . .
.
CONGENITAL HEART DISEASE IN MONGOLISM
tal heart disease had multiple cardiac defects. Thus, although 11 of our 39 patients had complete atrioventricularis communis (28 percent), this le- sion accounted only for 15.6 percent of all cardiac defects observed.
Among the main factors in the origin of mon- golism, advanced maternal age, maternal illness and unfavorable intrauterine environment were examined in the present report. Thus, the mean age of the mothers was 33 years and that of the fathers, 33.7 years. These figures are not materi- ally different from those of Liu and Corlett,6 who cited 34.5 and 36.7 years, respectively. The mean maternal age in the series reported by Rowe and Uchida3 was 33.5 years.
Maternal illness during the first trimester of pregnancy occurred in 10 cases (28 percent) in this series and also in 27 percent of the 11 clinical cases reported by Liu and Corlett.5 However, when they included their 16 autopsy cases the incidence was 51.5 percent. The mean birth rank in our series was 3.7 compared to 3.4 and 2.8, respectively, in the clinical and autopsy groups with congenital heart disease of Liu and Corlett. The mean birth weight in this series was 6.8 lb compared to 7.1 in the group of Liu and Corlett. Our studies suggest that there is no significant difference in the growth and development of patients in our 3 groups.
Physical findings: Cyanosis was not seen in pa- tients in group III (normal pulmonary vascular resistance). However, it occurred in 50 percent of those in group I (right ventricular outflow ob- struction) and at one stage or another in 82 per- cent (18 of 22) of those in group II (pulmonary hypertension). Cyanosis in group I reflected the severity of the obstruction to the outflow tract of the right ventricle. On the other hand, 3 different mechanisms accounted for cyanosis in group II. During the first 6 months of life it was almost al- ways secondary to lung involvement. Rarely, how- ever, it was permanent and secondary to a cyanotic heart disease (common ventricle or double-outlet right ventricle). Persistence of cyanosis after the age of 2 or 3 years almost always meant the devel- opment of the Eisenmenger’s reaction. Similarly, heart failure and precordial bulging were features of patients in group II. Heart failure tended to be precipitated by bronchitis or pneumonia.
Heart murmurs alone suggested the correct di- agnosis in most patients in group III. On the other hand, heart murmurs alone did not suggest the diagnosis in most patients in groups I and II. As pointed out by Rowe and Uchida,3 the absence of cardiac murmurs during the first few weeks of life does not necessarily rule out congenital heart dis- ease, and in 10 of our patients the heart murmur had been discovered after the third month of life.
Electrocardiogram : Except for cardiac cathe- terization, the electrocardiogram was the most im-
VOLUME 29. APRIL 1972 501

SHAHER ET AL.
portant investigation in identifying our 3 groups of patients. Thus, whereas no evidence of abnor- mal axis deviation or atria1 or ventricular hyper- trophy occurred in 64 percent (7 of 11) of patients in group III, all patients in groups I and II had ab- normal electrocardiographic findings ; significant changes affected the P-R interval, the electrical axis, and atria1 and ventricular hypertrophy pat- terns singly or in combination. Thus, of the 3 pa- tients in group I with left axis deviation (Cases 1, 3 and 4) selective left ventricular angiogram showed the goose-neck deformity of cushion defect in 2 (Cases 1 and 4) and was inconclusive in the 1 (Case 3). Of the various anatomic abnormalities that occurred in group II, the pattern was uniform in the ‘7 patients with complete atrioventricularis communis. Thus, 6 had extreme right or left axis deviation and 1 had an open loop. Six had signifi- cant right ventricular hypertrophy and 1 showed combined enlargement. The P-R interval was pro- longed in 3. Regardless of the underlying patho- logic lesion all of the remaining 15 patients in group II had either right or combined ventricular hypertrophy. None had a normal pattern or left ventricular enlargement alone. The electrical axis of these 15 patients ranged from +90 to f330”. A complete atrioventricularis communis was present in 2 with left axis deviation; in the remaining 4 patients with such an electrical axis a cushion de- fect could not be demonstrated angiocardiographi- tally or at post-mortem study. In group III, 64 per- cent (7 of 11) had a normal electrocardiogram. The only patient with an ostium primum atria1 septal defect in this series had the typical electro- cardiographic changes, namely, incomplete right bundle branch block and left axis deviation. The remaining 3 patients had an open loop or left axis deviation which suggested a cushion defect. How- ever, this diagnosis has not been confirmed angio- cardiographically.
Chest roentgenogram: We have found the chest roentgenogram helpful in making a rough assessment of the severity of congenital heart dis- ease in mongolism. The cardiothoracic ratio and the pulmonary vascularity have been fairly reli- able in this regard. On the other hand, cardiac con- figuration, the position of the aortic arch, the purr monary arterial segment and left atria1 size have generally not been particularly helpful. The find- ing of skeletal deformity in the chest roentgeno- gram of a cyanotic patient should raise the possi- bility of hypoxic car pulmonale, since in 1 of our 2 patients with such findings pulmonary hyperten- sion and pulmonary venous desaturation were found at cardiac catheterization.
Cardiac catheterization : Our findings demon- strated that pulmonary hypertension at systemic levels occurred in 56 percent of the children with mongolism. Our data also suggested that Eisen-
menger’s reaction and shunt reversal develop early in those with pulmonary hypertension. Thus, of the 13 patients over the age of 6 months who did not have a common ventricle (Case 20) or a double-outlet right ventricle (Case 15) or car pul- monale (Case 16), 10 (76 percent) were found by dye-dilution curves or pulmonary venous and sys- temic arterial blood samples to have shunt rever- sal. In addition, of the 10 patients who were 1 year of age or less and who did not have a double-outlet right ventricle (Case 15) or a common ventricle (Case 7), 5 were found to have shunt reversal. Moreover, whereas no patient without pulmonary hypertension (groups I and III) had pulmonary venous desaturation, 10 (76 percent) of the 13 pa- tients with pulmonary hypertension (group II) in whom a pulmonary venous sample was obtained had pulmonary venous desaturation. This finding demonstrated that patients with pulmonary hy- pertension are susceptible to lung infections or congestive heart failure, or both. Although it is reasonable to suggest that the early development of shunt reversal in this group could be in part sec- ondary to lung damage, it is difficult to rule out excessive reaction of the pulmonary vascular bed to pulmonary hypertension or anoxia, or both, in mongolism. Although pulmonary hypertension and the Eisenmenger’s complex have been known to occur in mongolism,“,” the incidence of these 2 con- ditions is difficult to assess owing to the paucity of hemodynamic data in published reports. Moreover, the term “Eisenmenger’s” has not always been clearly defined in these studies. A patient with idiopathic pulmonary hypertension has been re- ported on.”
Angiocardiography : This procedure estab- lished the anatomic diagnosis in all of our patients. We have found that hemodynamic data alone will not establish a complete anatomic diagnosis, espe- cially in patients in groups I and II, unless sub- stantiated by selective angiocardiography in the cardiac chambers or great vessels.
Prognosis: It would seem that the prognosis of any patient with mongolism and congenital heart disease is determined by the age and the severity of the underlying lesion. Thus, 11 of our 39 pa- tients died, 9 during the first year of life and 2 in subsequent years. Of these 11 patients, 2 had ob- struction of right ventricular outflow, 8 had pul- monary hypertension and 1 had normal pulmonary vascular resistance. The mortality rate in these groups, therefore, was 33, 36.5 and 10 percent, re- spectively. The major cause of death in group I was anoxia secondary to diminished pulmonary blood flow. On the other hand, recurrent pneu- monia and congestive heart failure developed in patients in group II. These 2 factors were the main cause of death in this group during infancy. It also appears that those who survive the first year of
502 The American Journal of CARDIOLOGY

CONGENITAL HEART DISEASE IN MONGOLISM
life do fairly well although the threat of pneu- monia and congestive heart failure remains. The Eisenmenger’s reaction occurs in the majority by age 3 years, and in 1 patient it occurred as early as age 5 months. In this series 5 patients with pul- monary hypertension were 8 years of age or older. Only 1 died (at age 10 years, secondary to rheu- matic fever). The remaining 4, all with cyanosis secondary to shunt reversal, are being followed up regularly in our clinic. Patients in group III had the best prognosis; only 1 died during the first year of life, and the remaining 10 are doing well and have had no major problems. Three of them underwent successful surgery, ligation of a patent
ductus arteriosus in 2 and closure of an ostium primum atria1 septal defect in 1.
Indications for surgery: Our data suggest that all patients in group II should be considered for early surgery. Palliative surgical therapy should be considered during the first year of life, particu- larly if there is recurrent lung infection or conges- tive heart failure. The high incidence of the Eisen- menger’s reaction after the first year suggests that total corrective surgery should be performed dur- ing the first 2 or 3 years of life. On the other hand, patients in groups I and III should be considered for surgery on an individual basis, and surgery recommended whenever indicated.
References
Evans PR: Cardiac anomalies in mongolism. Brit Heart 5. Liu MC, Corlett K: A study of congenital heart defects in J 12:258-262, 1950 mongolism. Arch Dis Child 34:410-419, 1959 Berg JM, Crome L, France NE: Congenital cardiac mal- 6. Vince DJ, Keith JD: The electrocardiogram in ventricu’la’r formations in mongolism. Brit Heart J 22:331-346, 1960 septal defect. Circulation 23:225-240, 1961 Rowe RD, Uchida IA: Cardiac malformation in mongo- 7. Abbott ME: New accessions in cardiac anomalies: pul- lism. A prospective study of 184 mongoloid children. Amer monary atresia of inflamatory origin; persistent ostium J Med 31:726-7315, 1961 primum with mongolian idiocy. Bull Int Assn Med Mus 10: Cullum L, Liebman J: The association of congenital heart 111-116, 1924 disease with Down’s syndrome (mongolism). Amer J 8. Taussig HB: Congenital Malformations of the Heart, Vol Cardiol 24:354-357, 1969 1. New York, Oxford University Press, 1947, p 13
VOLUME 29, APRIL 1972 503