clinical and pharmaceutical aspects of the use of antibacterial drugs in the clinic of internal...
TRANSCRIPT

Clinical and pharmaceutical aspects of the use of
antibacterial drugs in the clinic of internal diseases

Actions of antibacterial drugs on bacterial cells
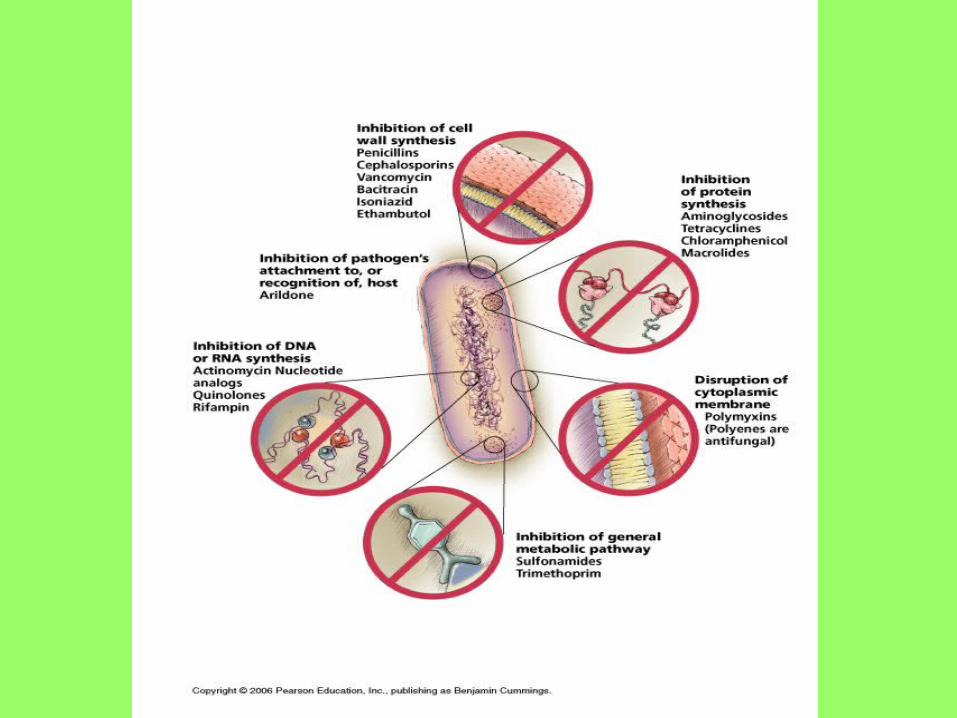

Mechanisms of Action 1. Inhibition of bacterial cell wall synthesis or activation of enzymes that
disrupt bacterial cell walls (eg, penicillins, cephalosporins, vancomycin)
2. Inhibition of protein synthesis by bacteria or production of abnormal bacterial proteins (eg, aminoglycosides, clindamycin, erythromycin, tetracyclines). These drugs bind irreversibly to bacterial ribosomes, intracellular structures that synthesize proteins. When antimicrobial drugs are bound to the ribosomes, bacteria cannot synthesize the proteins necessary for cell walls and other structures.
3. Disruption of microbial cell membranes (eg, antifungals)4. Inhibition of organism reproduction by interfering with nucleic acid
synthesis (eg, fluoroquinolones, rifampin, anti–acquired immunodeficiency syndrome antivirals)
5. Inhibition of cell metabolism and growth (eg, sulfonamides, trimethoprim)


Antibiotic Combination Therapy Antibiotic Combination Therapy Antimicrobial drugs are often used in combination. Antimicrobial drugs are often used in combination.
Indications for combination therapy may include:Indications for combination therapy may include:• • Infections caused by multiple microorganisms (eg, Infections caused by multiple microorganisms (eg,
abdominal and pelvic infections)abdominal and pelvic infections)• • Nosocomial infections, which may be caused by many Nosocomial infections, which may be caused by many
different organismsdifferent organisms• • Serious infections in which a combination is synergistic Serious infections in which a combination is synergistic
(eg, an aminoglycoside and an antipseudomonal (eg, an aminoglycoside and an antipseudomonal penicillin for pseudomonal infections)penicillin for pseudomonal infections)
• • Likely emergence of drug-resistant organisms if a single Likely emergence of drug-resistant organisms if a single drug is used (eg, tuberculosis). Although drug drug is used (eg, tuberculosis). Although drug combinations to prevent resistance are widely used, the combinations to prevent resistance are widely used, the only clearly effective use is for treatment of tuberculosis.only clearly effective use is for treatment of tuberculosis.
• • Fever or other signs of infection in clients whose immune Fever or other signs of infection in clients whose immune systems are suppressed. Combinations of antibacterial systems are suppressed. Combinations of antibacterial plus antiviral and/or antifungal drugs may be needed plus antiviral and/or antifungal drugs may be needed

PENICILLINSPENICILLINS Indications for Use Indications for Use
• Clinical indications for use of penicillins include Clinical indications for use of penicillins include bacterial infections caused by susceptible bacterial infections caused by susceptible microorganisms. As a class, penicillins usually microorganisms. As a class, penicillins usually are more effective in infections caused by gram-are more effective in infections caused by gram-positive bacteria than those caused by gram-positive bacteria than those caused by gram-negative bacteria. However, their clinical uses negative bacteria. However, their clinical uses vary significantly according to the subgroup or vary significantly according to the subgroup or individual drug and microbial patterns of individual drug and microbial patterns of resistance. The drugs are often useful in skin/ resistance. The drugs are often useful in skin/ soft tissue, respiratory, gastrointestinal, and soft tissue, respiratory, gastrointestinal, and genitourinary infections. However, the incidence genitourinary infections. However, the incidence of resistance among streptococci, staphylococci, of resistance among streptococci, staphylococci, and other microorganisms continues to grow. and other microorganisms continues to grow.

AminopenicillinsAminopenicillins

PiperacillinPiperacillin

Augmentin Augmentin contains contains amoxicillin and clavulanate. amoxicillin and clavulanate. It is available in 250-, 500-, It is available in 250-, 500-, and 875-mg tablets, each of and 875-mg tablets, each of which contains 125 mg of which contains 125 mg of
clavulanate. clavulanate.

MACROLIDES

CephalosporinsCephalosporinsIndications for Use Indications for Use
Clinical indications for the use of cephalosporins include surgical Clinical indications for the use of cephalosporins include surgical prophylaxis and treatment of infections of the respiratory tract, skin prophylaxis and treatment of infections of the respiratory tract, skin and soft tissues, bones and joints, urinary tract, brain and spinal and soft tissues, bones and joints, urinary tract, brain and spinal cord, and bloodstream (septicemia). In most infections with cord, and bloodstream (septicemia). In most infections with streptococci and staphylococci, penicillins are more effective and streptococci and staphylococci, penicillins are more effective and less expensive. In infections caused by methicillin-resistant less expensive. In infections caused by methicillin-resistant S. S. aureus, aureus, cephalosporins are not clinically effective even if in vitro cephalosporins are not clinically effective even if in vitro testing indicates susceptibility. Infections caused by testing indicates susceptibility. Infections caused by Neiserria Neiserria gonorrhoeae, gonorrhoeae, once susceptible to penicillin, are now preferentially once susceptible to penicillin, are now preferentially treated with a third-generation cephalosporin such as ceftriaxone. treated with a third-generation cephalosporin such as ceftriaxone.
Cefepime is indicated for use in severe infections of the lower Cefepime is indicated for use in severe infections of the lower respiratory and urinary tracts, skin and soft tissue, female respiratory and urinary tracts, skin and soft tissue, female reproductive tract, and infebrile neutropenic clients. It may be used reproductive tract, and infebrile neutropenic clients. It may be used as monotherapy for all infections caused by susceptible organisms as monotherapy for all infections caused by susceptible organisms except except P. aeruginosa; P. aeruginosa; a combination of drugs should be used for a combination of drugs should be used for serious pseudomonal infections.serious pseudomonal infections.
Aminoglycosides Aminoglycosides Contraindications to UseContraindications to Use
Aminoglycosides are contraindicated in Aminoglycosides are contraindicated in infections for which less toxic drugs are infections for which less toxic drugs are effective. The drugs are nephrotoxic and effective. The drugs are nephrotoxic and ototoxic and must be used very cautiously ototoxic and must be used very cautiously in the presence of renal impairment. in the presence of renal impairment. Dosages are adjusted according to serum Dosages are adjusted according to serum drug levels and creatinine clearance. The drug levels and creatinine clearance. The drugs must also be used cautiously in drugs must also be used cautiously in clients with myasthenia gravis and other clients with myasthenia gravis and other neuromuscular disorders because muscle neuromuscular disorders because muscle weakness may be increased.weakness may be increased.

PRINCIPLES OF THERAPY WITH TETRACYCLINES
1. Culture and susceptibility studies are needed before tetracycline therapy is started because many strains of organisms are either resistant or vary greatly in drug susceptibility. Cross-sensitivity and cross-resistance are common among tetracyclines.
2. The oral route of administration is usually effective and preferred. Intravenous (IV) therapy is used when oral administration is contraindicated or for initial treatment of severe infections.
3. Tetracyclines decompose with age, exposure to light, and extreme heat and humidity. Because the breakdown products may be toxic, it is important to store these drugs correctly. Also, the manufacturer’s expiration dates on containers should be noted and outdated drugs should be discarded.

LLincosamiincosamiddes es
Clindamycin is indicated for treatment of Clindamycin is indicated for treatment of anaerobic infection caused by anaerobic infection caused by bacteroides and other anaerobes that bacteroides and other anaerobes that often participate in mixed infections. often participate in mixed infections. Clindamycin, sometimes in combination Clindamycin, sometimes in combination with an aminoglycoside or cephalosporin, with an aminoglycoside or cephalosporin, is used to treat penetrating wounds of the is used to treat penetrating wounds of the abdomen and the gut; infections abdomen and the gut; infections originating in the female genital tract, eg, originating in the female genital tract, eg, septic abortion and pelvic abscesses; and septic abortion and pelvic abscesses; and aspiration pneumonia. Clindamycin is aspiration pneumonia. Clindamycin is now recommended rather than now recommended rather than erythromycin for prophylaxis of erythromycin for prophylaxis of endocarditis in patients with valvular endocarditis in patients with valvular heart disease who are undergoing certain heart disease who are undergoing certain dental procedures. Clindamycin plus dental procedures. Clindamycin plus primaquine is an effective alternative to primaquine is an effective alternative to trimethoprim-sulfamethoxazole for trimethoprim-sulfamethoxazole for moderate to moderately severe moderate to moderately severe Pneumocystis jiroveciPneumocystis jiroveci pneumonia in AIDS pneumonia in AIDS patients. It is also used in combination patients. It is also used in combination with pyrimethamine for AIDS-related with pyrimethamine for AIDS-related toxoplasmosis of the brain.toxoplasmosis of the brain.

Chloramphenicol Because of potential
toxicity, bacterial resistance, and the availability of many other effective alternatives, chloramphenicol is rarely used. It may be considered for treatment of serious rickettsial infections such as typhus and Rocky Mountain spotted fever. It is an alternative to a b-lactam antibiotic for treatment of meningococcal meningitis occurring in patients who have major hypersensitivity reactions to penicillin or bacterial meningitis caused by penicillin-resistant strains of pneumococci. The dosage is 50-100 mg/kg/d in four divided doses.

OXAZOLIDINONESOXAZOLIDINONES

Antibiotic resistance


Factors that encourage the spread of resistance
The emergence and spread of antimicrobial resistance are complex problems driven by numerous interconnected fac tors, many of which are linked to the misuse of antimicrobi als and thus amenable to change. In turn, antimicrobial use is influenced by an interplay of the knowledge, expectations, and interactions of prescribers and patients, economic in centives, characteristics of a country's health system, and the regulatory environment.
Patient-related factors are major drivers of inappropriate antimicrobial use. For example, many patients believe that new and expensive medications are more efficacious than older agents. In addition to causing unnecessary health care expenditure, this perception encourages the selection of re sistance to these newer agents as well as to older agents in their class.
Self-medication with antimicrobials is another major factor contributing to resistance. Self-medicated antimicrobials may be unnecessary, are often inadequately dosed, or may not contain adequate amounts of active drug, especially if they are counterfeit drugs. In many developing countries, antimi crobials are purchased in single doses and taken only until the patient feels better, which may occur before the patho gen has been eliminated. Inappropriate demand can also be stimulated by marketing practices. Direct-to-consumer advertising allows pharmaceu tical manufacturers to market medicines directly to the public via television, radio, print media, and the Internet. In par ticular, advertising on the Internet is gaining market pen etration, yet it is difficult to control with legislation due to poor enforceability.

Prescribers' perceptions regarding patient expectations and demands substantially influence prescribing practice. Physi cians can be pressured by patient expectations to prescribe antimicrobials even in the absence of appropriate indications. In some cultural settings, antimicrobials given by injection are considered more efficacious than oral formulations. Such perceptions tend to be associated with the over-prescribing of broad-spectrum injectable agents when a narrow-spec trum oral agent would be more appropriate. Prescribing “just to be on the safe side" increases when there is diagnostic uncertainty, lack of prescriber knowledge re garding optimal diagnostic approaches, lack of opportunity for patient follow-up, or fear of possible litigation. In many countries, antimicrobials can be easily obtained in pharmacies and markets without a prescription.
Patient compliance with recommended treatment is another major problem. Patients forget to take medication, interrupt their treatment when they begin to feel better, or may be unable to afford a full course, thereby creating an ideal envi ronment for microbes to adapt rather than be killed. In some countries, low quality antibiotics (poorly formulated or manu factured, counterfeited or expired) are still sold and used for self-medication or prophylaxis.
Hospitals are a critical component of the antimicrobial re sistance problem worldwide. The combination of highly sus ceptible patients, intensive and prolonged antimicrobial use, and cross-infection has resulted in nosocomial infections with highly resistant bacterial pathogens. Resistant hospital-acquired infections are expensive to control and extremely dif ficult to eradicate. Failure to implement simple infection control practices, such as handwashing and changing gloves before and after contact with patients, is a common cause of infection spread in hospitals throughout the world. Hospi tals are also the eventual site of treatment for many patients with severe infections due to resistant pathogens acquired in the community. In the wake of the AIDS epidemic, the preva lence of such infections can be expected to increase.
Adverse Effectsof Sulfonamides Adverse effects can result from oral and sometimes topical
sulfonamides; effects include Hypersensitivity reactions, such as rashes, Stevens-Johnson
syndrome (see Hypersensitivity and Inflammatory Disorders: Stevens-Johnson Syndrome (SJS) and Toxic Epidermal Necrolysis (TEN)), vasculitis, serum sickness, drug fever, anaphylaxis, and angioedema
Crystalluria, oliguria, and anuria Hematologic reactions, such as agranulocytosis, thrombocytopenia,
and, in patients with G6PD deficiency, hemolytic anemia Kernicterus in neonates Photosensitivity Neurologic effects, such as insomnia, and headache Hypothyroidism, hepatitis, and activation of quiescent SLE may
occur in patients taking sulfonamides. These drugs can exacerbate porphyrias.

FLUOROQUINOLONES ciprofloxacin (Cipro, Ciloxan), gatifloxacin (Tequin)levofloxacin (Levaquin, Tavanic), lomefloxacin (Maxaquin)moxifloxacin (Avelox), norfloxacin (Noroxin), ofloxacin (Floxin, Tarivid)


ANTIVIRAL DRUGS

ANTIVIRAL DRUGS

Antiretrovirals

Therapy of HIV Infection: Nucleoside-Analog Reverse Transcriptase Inhibitors (NRTI). These
drugs inhibit viral RNA-dependent DNA polymerase (reverse transcriptase) and are incorporated into viral DNA (they are chain-terminating drugs).
Zidovudine (AZT = ZDV, Retrovir) first approved in 1987 Didanosine (ddI, Videx) Zalcitabine (ddC, Hivid) Stavudine (d4T, Zerit) Lamivudine (3TC, Epivir)
Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs). In contrast to NRTIs, NNRTIs are not incorporated into viral DNA; they inhibit HIV replication directly by binding non-competitively to reverse transcriptase.
Nevirapine (Viramune) Delavirdine (Rescriptor)
Protease Inhibitors. These drugs are specific for the HIV-1 protease and competitively inhibit the enzyme, preventing the maturation of virions capable of infecting other cells.
Saquinavir (Invirase) first approved in 1995 Ritonavir (Norvir) Indinavir (Crixivan) Nelfinavir (Viracept)

Antifungal Drug Mechanisms
