clic sargent key worker education project june … · clic sargent key worker education project ......
TRANSCRIPT

CS evaluation report updated 20.1.15 1
CLIC Sargent Key Worker Education Project June 2012 – October 2014
EVALUATION REPORT Project Co-ordinators Angela Russell, Royal Hospital for Sick Children, Edinburgh Ali Hall, Yorkhill Children’s Hospital, Glasgow Carole Campbell, Royal Aberdeen Children’s Hospital

CS evaluation report updated 20.1.15 2
Content Introduction / aim / background Approach Methodology Data Collection Analysis Ethical considerations Results Recommendations / Action points Limitations Lessons learnt Coincidental outcomes of the project Dissemination Conclusion Acknowledgement We would like to thank our colleagues for their continued support throughout the development of the education package.
CS evaluation report updated 20.1.15 3
Introduction Aim The aim of this two year, pan Scotland project is to improve and enhance the overall and local support offered to children and young people with cancer in Scotland and their families. This project was enabled by funding from the CLIC Sargent Key Worker Project. Background In March 2012, the Scottish Government launched the first Cancer Plan for Children and Young People in Scotland (Scottish Government, 2012) with the aim of delivering a high quality, single and sustainable, specialist cancer service to ensure the best possible outcomes. The Managed Service Network (MSN) for Children and Young People in Scotland has been charged with delivering this vision and will require national multidisciplinary team working to ensure that care is coordinated to provide an efficient, effective and safe service for all children and young people in an age appropriate manner, regardless of where they live. It is envisaged that each child and young person will have a designated Key Worker who will be responsible for supporting the family and will play an integral role in coordinating the care pathways to ensure a continuum in quality from primary to tertiary care. The Scottish Cancer Plan aims to minimise disruption to normal family life and to limit time away from home, other children, from family support and from work, where possible, in order to help families cope. This will require improved networking, links and support between hospitals and all other children’s services to increase opportunities for specialist care to be provided in the community, (and will build upon the recommendation by The Scottish Executive National Delivery Plan for Children and Young People’s Specialist Services in Scotland (Scottish Government, 2009) ) This approach is echoed throughout the United Kingdom and in 2005, the National Institute for Health and Clinical Excellence (NICE) published guidance on how cancer services for children and young people in England should be delivered by the NHS. The guidance, “Improving Outcomes for Children and Young People” recommended that every child or young person with cancer and their family should have a key worker responsible for the coordination of their care and support in the community. Furthermore, supported by the NHS, CLIC Sargent conducted a full review into community based care and support needed by these children, young people and their families. This review, “More than My Illness: Delivering quality care for children with cancer” (2009), was undertaken with the aim of developing a model for future service delivery that, once implemented, should allow all children to have a key worker and equal access to good quality, holistic, community based care. Paediatric Oncology Outreach Nurse Specialists (POONS) have been identified as being best placed to act as the child and young person’s Key Worker in the first instance (although it is acknowledged that the Key Worker may change over

CS evaluation report updated 20.1.15 4
time). This project, which is supported by the Scottish Managed Service Network for Children and Young People with Cancer is about implementing these recommendations within Scotland and developing an educational resource package that the Key Worker will be able to use with any local services and community staff who may be involved in caring for a child or young person with cancer and his or her family. It is envisaged that any clinical care will be coordinated by the POONS with possible involvement from local community multidisciplinary teams (in the main, Community Children’s Nurses where they are available) An important element of the project will be collaborative working between the three principal treatment centres and shared care centres to examine, improve and standardise care pathways across Scotland. The success in changes in practice would be dependant upon the participation and involvement of all members of the multidisciplinary team. Approach The approach to be pursued in addressing the challenges of delivering care closer to home is to invest in creating greater capacity, knowledge and skills within communities to contribute to the care of children and young people undergoing treatment for cancer. To assist all POONS across Scotland to meet the criteria of working as the child and family’s key worker a 2 fold approach will be taken;
Development of an educational package
Development of shared care documentation The ultimate aim is these will be used by Primary Health Care Professionals so that the overall and local support offered to these children and families is enhanced. Methodology In order to develop an education resource package for use within the community and shared care centre, it is essential to determine the needs of service users and providers. A scoping exercise was conducted in the first year to identify the need for such a resource, its content and how training should be delivered, evaluated and sustained. The project was coordinated by CLIC Sargent funded nurses from Aberdeen, Edinburgh and Glasgow who all worked closely together to examine, improve and standardise care pathways across Scotland. The project was started in June 2012 with the nurses from Edinburgh and Glasgow and they were joined in January 2013 with the nurse from Aberdeen. Our initial brief was to develop an education package fit for purpose. We started with a brainstorming session which highlighted the areas for further exploration and development. This enabled us to clearly define the outcomes and develop a project plan which detailed the direction of the project. We then identified with our teams what links were already established, what works well and what needs
CS evaluation report updated 20.1.15 5
improved upon. This identified that there were links but no real structure in place or consistency to the referral process for community children’s nurses in particular. Therefore the first six months of the project was spent mainly networking with colleagues throughout Scotland including primary care, AHPs MSN group, MSN promoting the project and investing in their expertise and opinions. As the project progressed staff have engaged in the process and we have developed links that didn’t previously exist and strengthened those already there. Initial Plan First year - scoping exercise to:
1. Identify gaps in service – from a professional and child and family perspective
2. Identify what is already available – through questionnaire to professionals and networking face to face.
3. Identify what care and support is possible to deliver closer to home - networking
4. Identify training needs to enable care identified in 3 to be delivered closer to home
5. Review current training courses to ensure they meet staff needs
Second year - implementation
1. Delivery of training
2. Development of education resource package
3. Roll-out of education resource package
Data collection
We were tasked with the development of an education / resource package which could be utilized by all staff within primary care, community children’s nurses, shared care centres and other local services. Initially, a brainstorming session took place to determine what we wanted to achieve and how we envisaged getting there. Following that it was agreed that the best way to inform the development of the education package was to consult the key stakeholders. We achieved this by:
Networking with colleagues prior to sending out the questionnaires to raise awareness of the project.
Sending an invitation to complete a questionnaire to all children (with parent/carer), young people and families currently on treatment and those who had completed treatment within one year. We decided to limit the timescale for patients off treatment to one year in order to keep the data collection manageable. Advice was taken from the Paediatric Oncology Outreach Nurses with regards to patients receiving palliative care.
CS evaluation report updated 20.1.15 6
Inviting healthcare professionals who were currently involved in the care of children and young people with cancer or had been involved within the past year to complete a questionnaire via survey monkey
Family questionnaires (Children/parent or carer and young people)
Each questionnaire asked questions in relation to the following:
Demographics
Principal treatment centre
Outreach service
Shared care / Community
Information, advice and support
Further comments
The child or young person and families’ questionnaires were sent by post with a stamped addressed envelope for easy return. A collection box for the questionnaires was also put in the ward and Haematology out-patient clinic of each Principal treatment centre.
The survey monkey link was sent to professionals via a named individual with the intention of it being cascaded down to all relevant staff. Throughout this time we also met with various groups of staff; Community Children’s Nurses (CCNs), Allied Health Professionals (AHPs), GPs via the MSN interface meeting, MSN to promote the project and inform as many professionals as we could. This process proved to be invaluable and we felt much supported particularly by the MSN for children and young people’s cancer services in Scotland.
Analysis Child/Young Person and family questionnaires The questionnaires consisted of open and closed questions to enable participants to expand on their responses so we could gain as much information as possible. Clinical audit, Yorkhill Children’s Hospital, Glasgow assisted us with the analysis of the closed questions using an excel spreadsheet. Each project co-ordinator took responsibility for an area of Scotland (West of Scotland, South East Scotland and Grampian & Highlands) to collate the written comments.
Professional Questionnaires
Results were collated through survey monkey. Again, a lot of valuable information was received through additional comments which were collated by the project coordinators.
CS evaluation report updated 20.1.15 7
Ethical considerations
Advice was sought from the Scientific Officer, SESRES with regards to ethical implications. Individuals were anonymous and confidentiality was assured throughout.
Results
This is a summary of the results. If you would like further information / clarification please contact one of the project coordinators.
Family questionnaires
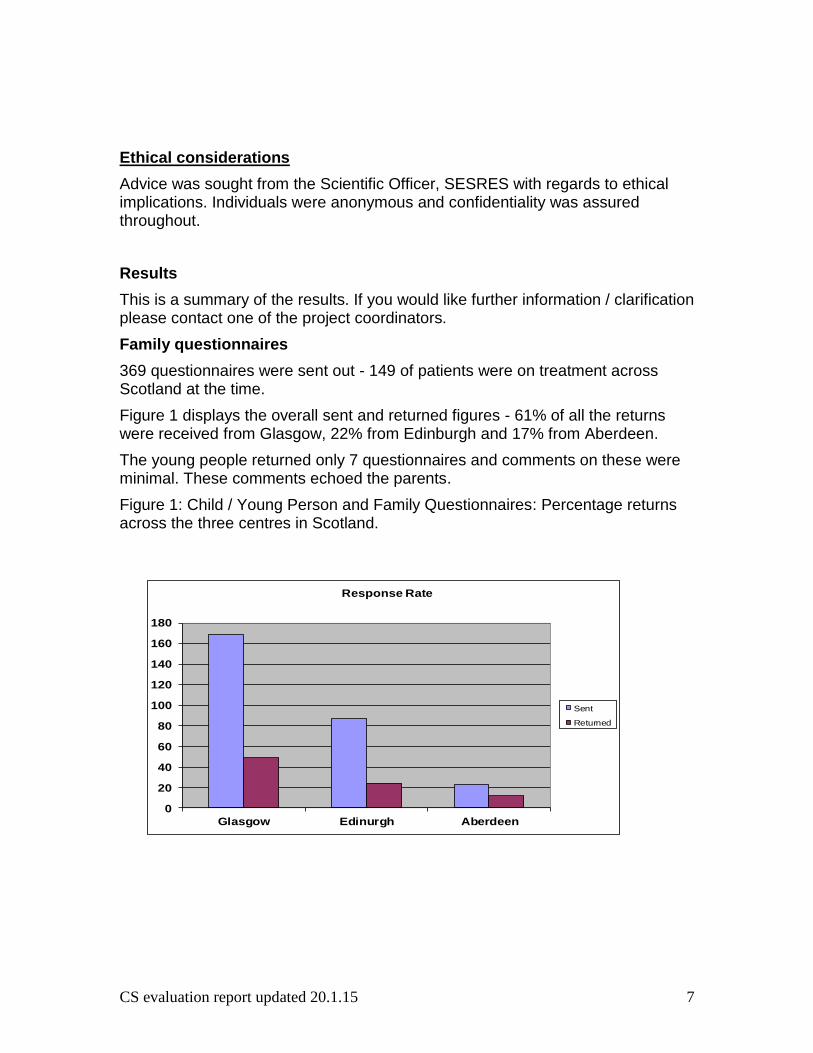
369 questionnaires were sent out - 149 of patients were on treatment across Scotland at the time.
Figure 1 displays the overall sent and returned figures - 61% of all the returns were received from Glasgow, 22% from Edinburgh and 17% from Aberdeen.
The young people returned only 7 questionnaires and comments on these were minimal. These comments echoed the parents.
Figure 1: Child / Young Person and Family Questionnaires: Percentage returns across the three centres in Scotland.
0
20
40
60
80
100
120
140
160
180
Glasgow Edinurgh Aberdeen
Response Rate
Sent
Returned
CS evaluation report updated 20.1.15 8
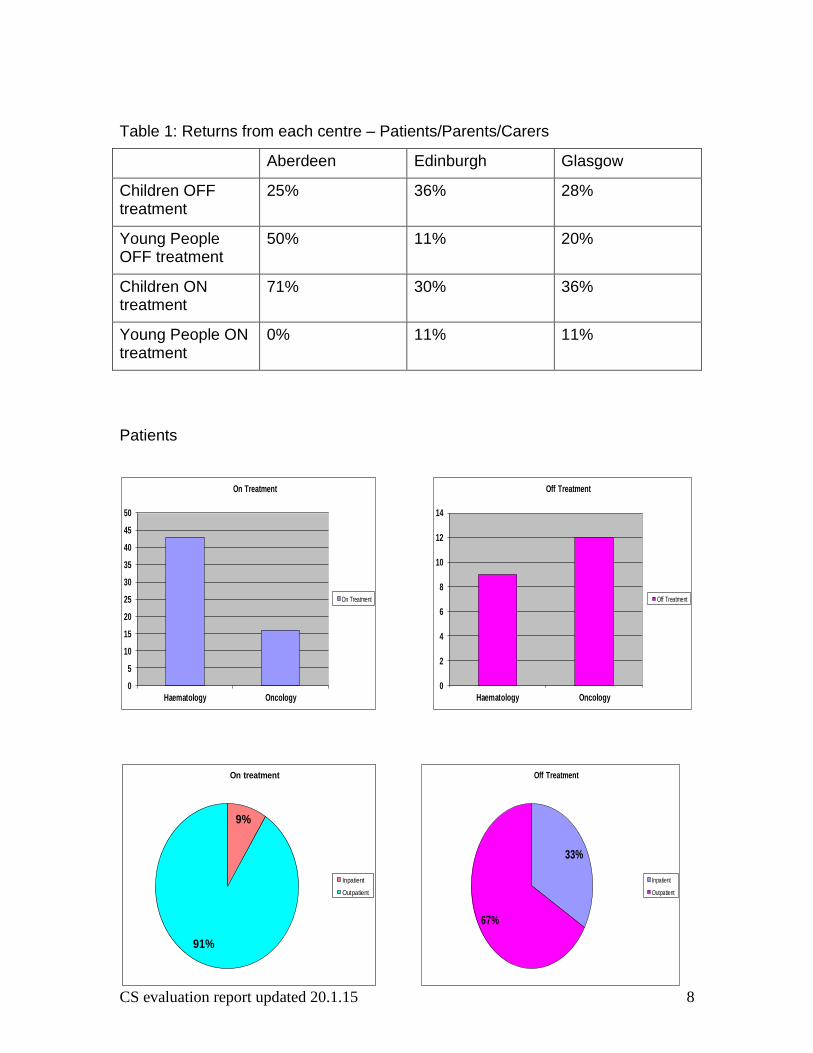
Table 1: Returns from each centre – Patients/Parents/Carers
Aberdeen Edinburgh Glasgow
Children OFF treatment
25% 36% 28%
Young People OFF treatment
50% 11% 20%
Children ON treatment
71% 30% 36%
Young People ON treatment
0% 11% 11%
Patients
0
5
10
15
20
25
30
35
40
45
50
Haematology Oncology
On Treatment
On Treatment
0
2
4
6
8
10
12
14
Haematology Oncology
Off Treatment
Off Treatment
9%
91%
On treatment
Inpatient
Outpatient
33%
67%
Off Treatment
Inpatient
Outpatient

CS evaluation report updated 20.1.15 9
23/44 questionnaires were from patients with Acute Lymphoblastic Leukaemia on maintenance.
The top 2 graphs demonstrate how often patients attend their Principal treatment centre (PTC). The bottom 2 graphs demonstrate travelling time to PTC. 68% of families have a more than 1hour round trip. Many of them were travelling on at least a weekly basis.
21%
24%
17%
11%
19%
4% 4%
On Treatment
More than once a week
Weekly
Every 2nd week
3 weekly
Monthly
Every few months
Yearly
38%
31%
0%
31%
0% 0%0%
Off Treatment
More than once a week
Weekly
Every 2nd week
3 weekly
Monthly
Every few months
Yearly
0
5
10
15
20
25
0-30minutes
31-60minutes
60-120minutes
> 120minutes
> 180minutes
On Treatment Travel Time
On Treatment
0
1
2
3
4
5
6
7
8
0-30minutes
31-60minutes
60-120minutes
> 120minutes
> 180minutes
Off Treatment Travel Time
Off Treatment
CS evaluation report updated 20.1.15 10
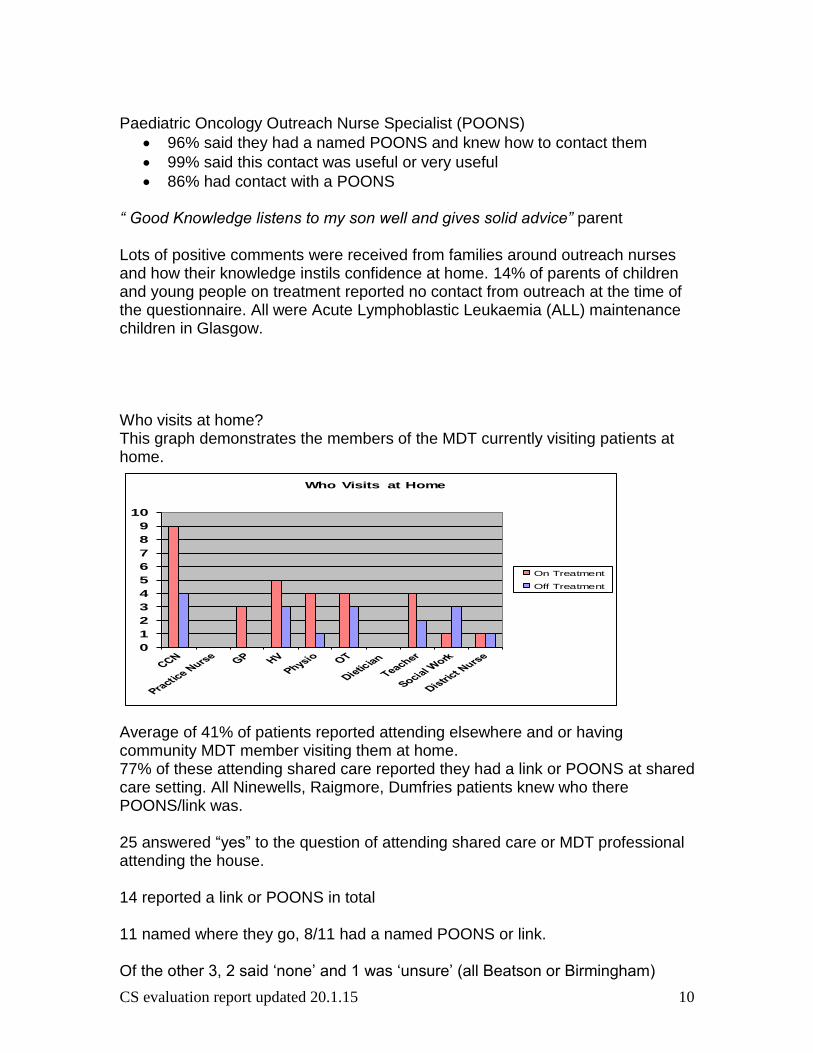
Paediatric Oncology Outreach Nurse Specialist (POONS)
96% said they had a named POONS and knew how to contact them
99% said this contact was useful or very useful
86% had contact with a POONS “ Good Knowledge listens to my son well and gives solid advice” parent Lots of positive comments were received from families around outreach nurses and how their knowledge instils confidence at home. 14% of parents of children and young people on treatment reported no contact from outreach at the time of the questionnaire. All were Acute Lymphoblastic Leukaemia (ALL) maintenance children in Glasgow. Who visits at home? This graph demonstrates the members of the MDT currently visiting patients at home. Average of 41% of patients reported attending elsewhere and or having community MDT member visiting them at home. 77% of these attending shared care reported they had a link or POONS at shared care setting. All Ninewells, Raigmore, Dumfries patients knew who there POONS/link was. 25 answered “yes” to the question of attending shared care or MDT professional attending the house. 14 reported a link or POONS in total 11 named where they go, 8/11 had a named POONS or link. Of the other 3, 2 said ‘none’ and 1 was ‘unsure’ (all Beatson or Birmingham)
0
1
2
3
4
5
6
7
8
9
10
Who Visits at Home
On Treatment
Off Treatment
CS evaluation report updated 20.1.15 11
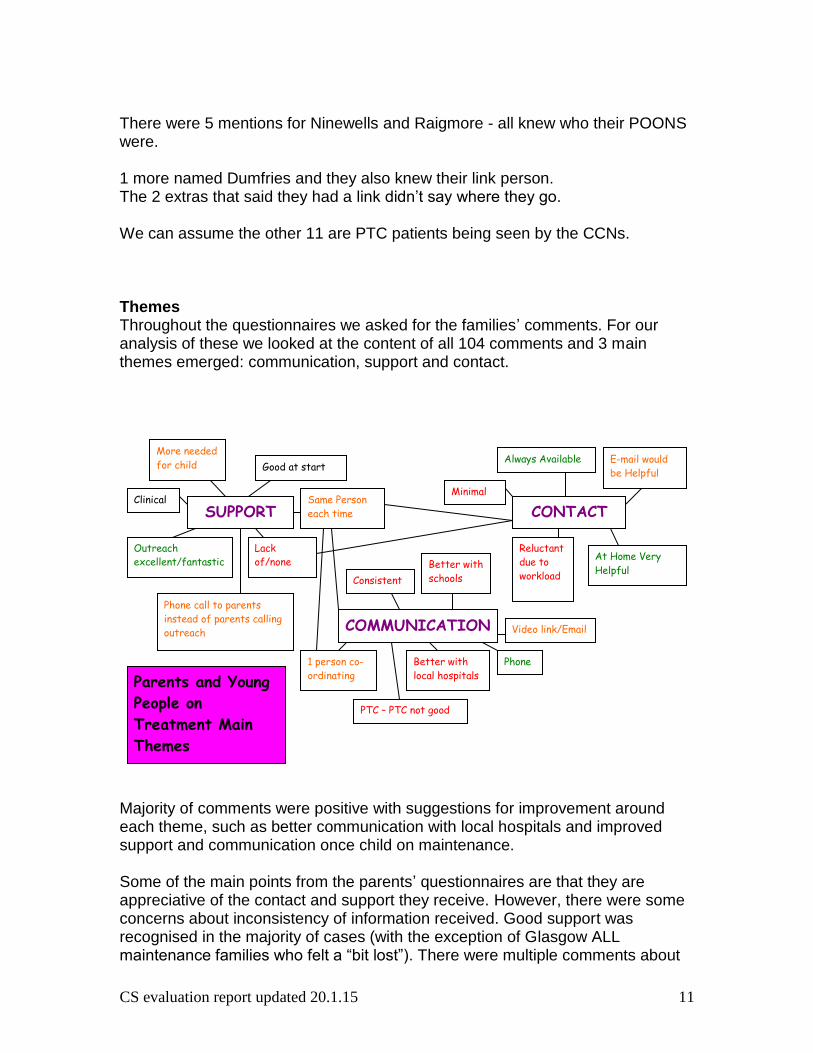
There were 5 mentions for Ninewells and Raigmore - all knew who their POONS were. 1 more named Dumfries and they also knew their link person. The 2 extras that said they had a link didn’t say where they go. We can assume the other 11 are PTC patients being seen by the CCNs. Themes Throughout the questionnaires we asked for the families’ comments. For our analysis of these we looked at the content of all 104 comments and 3 main themes emerged: communication, support and contact.
Majority of comments were positive with suggestions for improvement around each theme, such as better communication with local hospitals and improved support and communication once child on maintenance. Some of the main points from the parents’ questionnaires are that they are appreciative of the contact and support they receive. However, there were some concerns about inconsistency of information received. Good support was recognised in the majority of cases (with the exception of Glasgow ALL maintenance families who felt a “bit lost”). There were multiple comments about
SUPPORT
COMMUNICATION
CONTACT Same Person
each time
Lack
of/none Outreach
excellent/fantastic
Good at start
Phone call to parents
instead of parents calling
outreach
More needed
for child
Clinical
PTC – PTC not good
Better with
schools
1 person co-
ordinating
Consistent
Video link/Email
Phone Better with
local hospitals
Always Available
Minimal
At Home Very
Helpful
E-mail would
be Helpful
Reluctant
due to
workload
Parents and Young
People on
Treatment Main
Themes
CS evaluation report updated 20.1.15 12
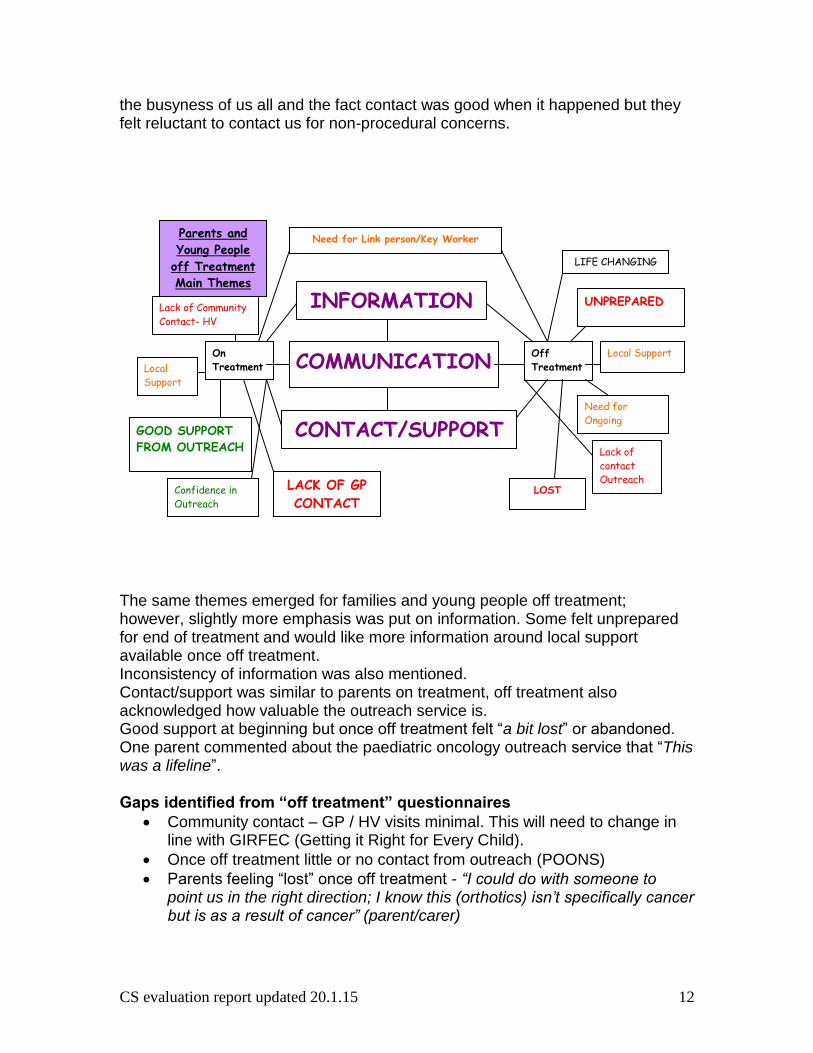
the busyness of us all and the fact contact was good when it happened but they felt reluctant to contact us for non-procedural concerns. The same themes emerged for families and young people off treatment; however, slightly more emphasis was put on information. Some felt unprepared for end of treatment and would like more information around local support available once off treatment. Inconsistency of information was also mentioned. Contact/support was similar to parents on treatment, off treatment also acknowledged how valuable the outreach service is. Good support at beginning but once off treatment felt “a bit lost” or abandoned. One parent commented about the paediatric oncology outreach service that “This was a lifeline”. Gaps identified from “off treatment” questionnaires
Community contact – GP / HV visits minimal. This will need to change in line with GIRFEC (Getting it Right for Every Child).
Once off treatment little or no contact from outreach (POONS)
Parents feeling “lost” once off treatment - “I could do with someone to point us in the right direction; I know this (orthotics) isn’t specifically cancer but is as a result of cancer” (parent/carer)
CONTACT/SUPPORT
On
Treatment Off
Treatment
t
LACK OF GP
CONTACT
Lack of Community
Contact- HV
GOOD SUPPORT
FROM OUTREACH
Confidence in
Outreach
UNPREPARED
LOST
Lack of
contact
Outreach
COMMUNICATION
Need for
Ongoing
INFORMATION
Need for Link person/Key Worker Parents and
Young People
off Treatment
Main Themes
Local Support Local
Support
LIFE CHANGING
CS evaluation report updated 20.1.15 13
Parents feel local professionals are not aware of where they are in their journey - “My GP never contacted us about my son when he was diagnosed and still has not been in touch” (parent/carer)
“Very poor service from HV said she would see my son for an extended time because of illness, then just no contact, we presume we are discharged” (parent/carer)
Preparation for the end of treatment - “It is very hard after treatment getting back to normality…more prepared for what happens after treatment i.e. local GP should be involved” (Parent/carer)
Family recommendations
Improved preparation for end of treatment
GP / community staff should be included from diagnosis to aid transition back at end of treatment - “…there has never been any contact between the GP and us since… diagnosis …which I think is wrong therefore I would not feel confident in taking him to the GP when they don’t know anything about him or what treatment he has had” (parent/carer)
Wider MDT to be kept up to date.
Key Worker for each child
Regular follow up / contact by POONS / Key worker / Late Effects practitioner
Professional questionnaire - results 3 survey monkey questionnaires were distributed:
MDT Health & education sectors external to PTC
PTC Haematology / Oncology MDT
Children’s hospital non Haematology / Oncology staff Survey monkey link was sent to key people within each group to cascade to relevant colleagues. All GPs off patients on and off treatment (for one year) were invited to complete the survey monkey. Each questionnaire asked questions in relation to the following:
Demographics
Involvement – past or present
Support received from PTC
Communication with PTC; method, frequency
Education; received and would like to receive
Gaps in service
CS evaluation report updated 20.1.15 14
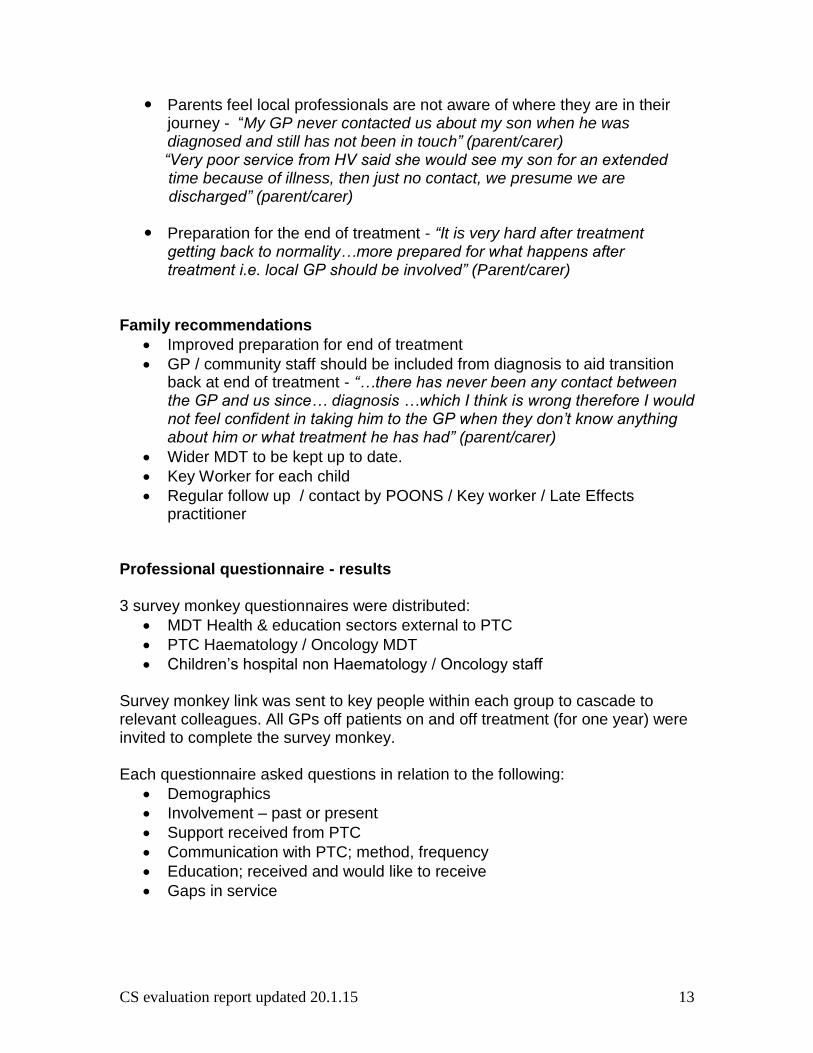
External questionnaire – 88 returns Percentage of returns is impossible to calculate due to nature of cascade of survey monkey link. Representatives from each group identified:
AHP (14) Doctors (27) Education (16) Nurses (31)
OT 1 Associate Specialist 1 Teachers 16 CHAS 1
Physio 11 GP 23 Practice nurse 2
Pharmacist 1 Practice manager 1 School nurse 1
Paediatrician 2 CCN 14
DN 5
HV 3
MacMillan nurse 3
Charge Nurse, DGH 1
Nurse Practitioner 1
0
5
10
15
20
25
30
Number of Professionals
CS evaluation report updated 20.1.15 15
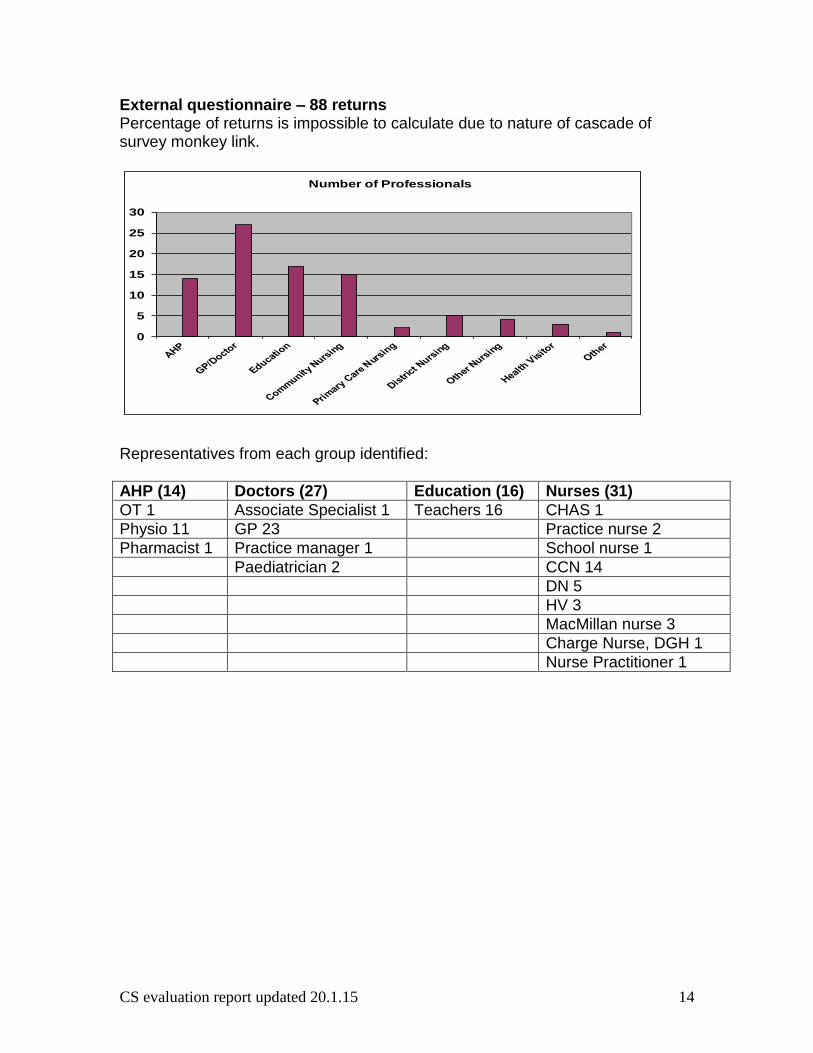
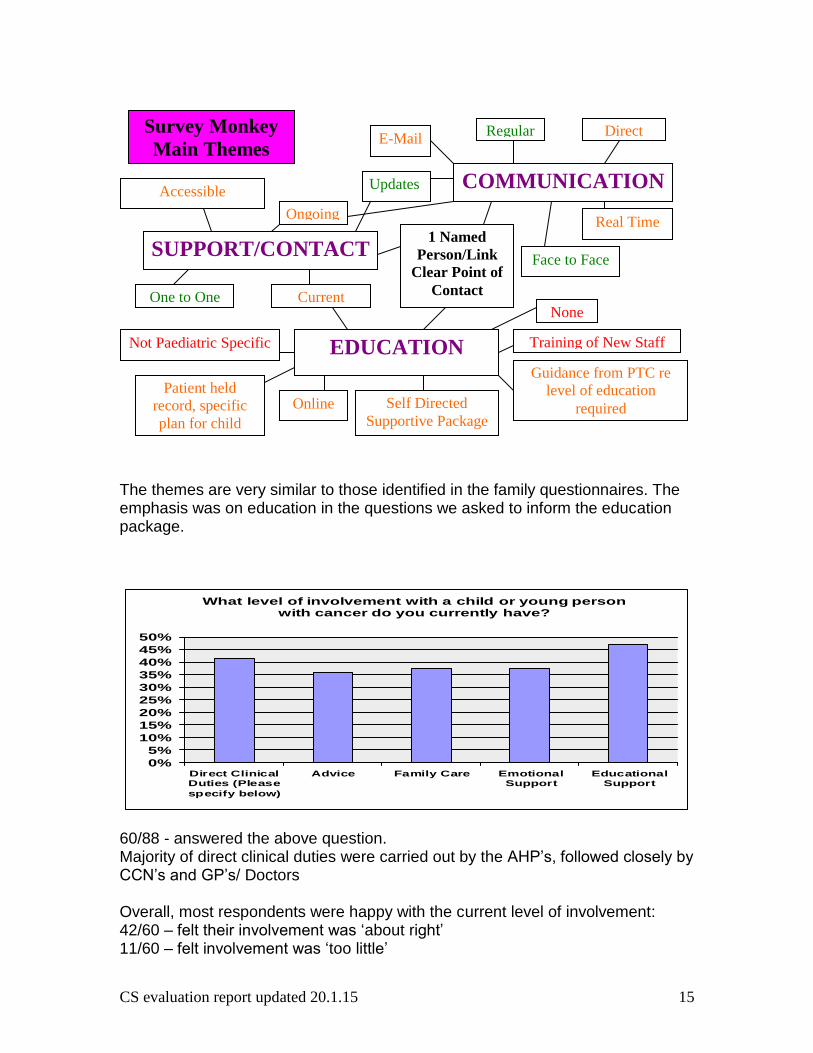
The themes are very similar to those identified in the family questionnaires. The emphasis was on education in the questions we asked to inform the education package. 60/88 - answered the above question. Majority of direct clinical duties were carried out by the AHP’s, followed closely by CCN’s and GP’s/ Doctors Overall, most respondents were happy with the current level of involvement: 42/60 – felt their involvement was ‘about right’ 11/60 – felt involvement was ‘too little’
SUPPORT/CONTACT
EDUCATION
COMMUNICATION
Survey Monkey
Main Themes
Regular Direct
Real Time
Face to Face
Updates
1 Named
Person/Link
Clear Point of
Contact
Accessible
One to One
Guidance from PTC re
level of education
required Online
Ongoing
Not Paediatric Specific
Self Directed
Supportive Package
Current None
Patient held
record, specific
plan for child
Training of New Staff
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Direct ClinicalDuties (Please
specify below)
Advice Family Care EmotionalSupport
EducationalSupport
What level of involvement with a child or young person with cancer do you currently have?
CS evaluation report updated 20.1.15 16
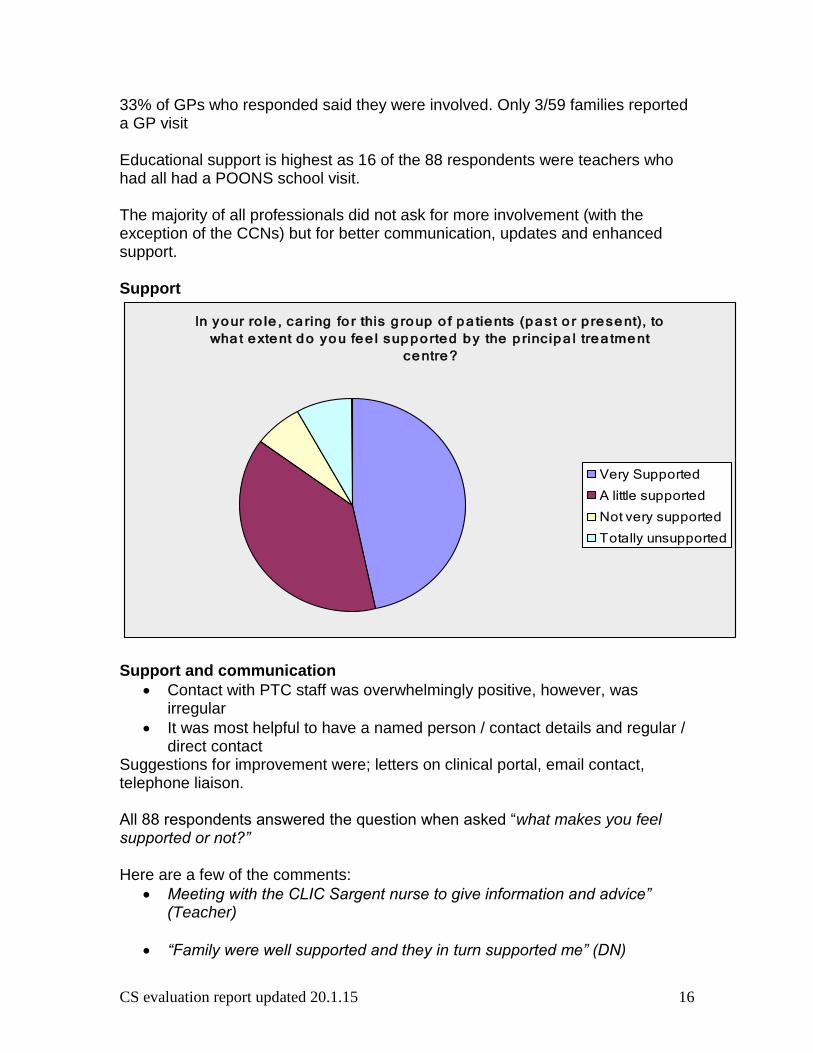
33% of GPs who responded said they were involved. Only 3/59 families reported a GP visit Educational support is highest as 16 of the 88 respondents were teachers who had all had a POONS school visit. The majority of all professionals did not ask for more involvement (with the exception of the CCNs) but for better communication, updates and enhanced support. Support
Support and communication
Contact with PTC staff was overwhelmingly positive, however, was irregular
It was most helpful to have a named person / contact details and regular / direct contact
Suggestions for improvement were; letters on clinical portal, email contact, telephone liaison. All 88 respondents answered the question when asked “what makes you feel supported or not?” Here are a few of the comments:
Meeting with the CLIC Sargent nurse to give information and advice” (Teacher)
“Family were well supported and they in turn supported me” (DN)
In yo ur ro le , ca ring fo r this g ro up o f p a tie nts (p a st o r p re se nt), to
wha t e xte nt d o yo u fe e l sup p o rte d b y the p rinc ip a l tre a tme nt
ce ntre ?
Very Supported
A little supported
Not very supported
Totally unsupported
CS evaluation report updated 20.1.15 17
“We would feel more supported if there was a link member of staff to contact if there were problems to give progress reports during treatment”
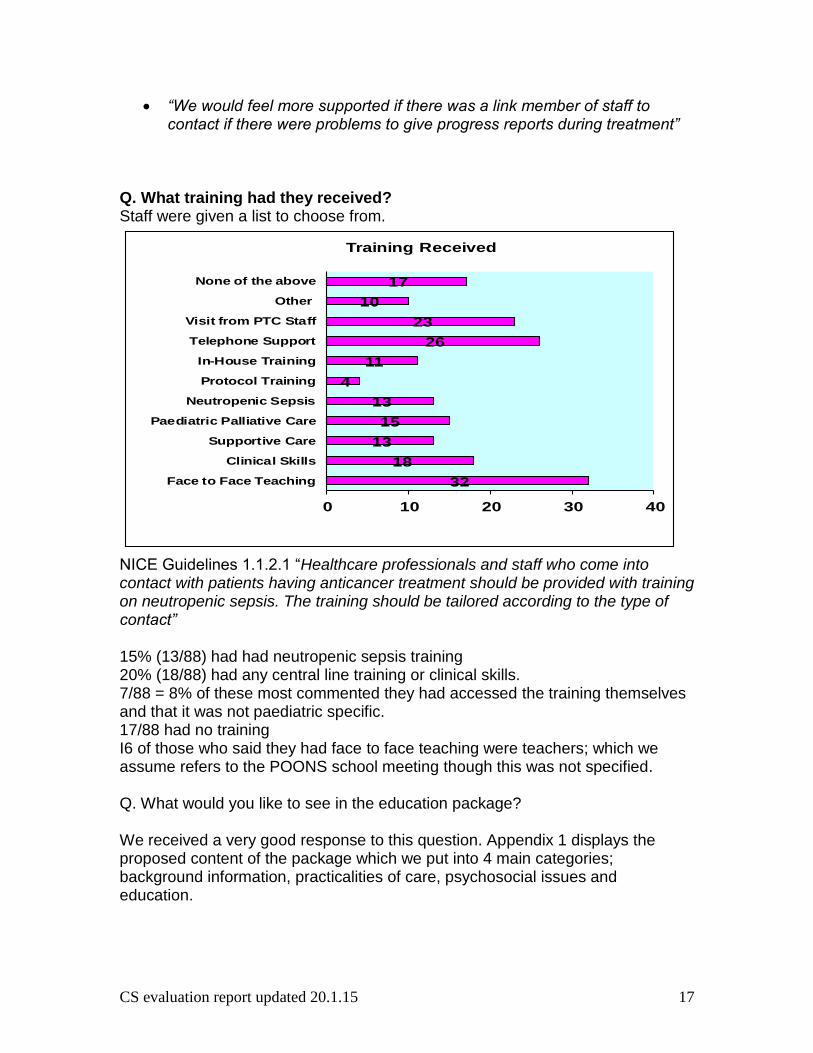
Q. What training had they received? Staff were given a list to choose from. NICE Guidelines 1.1.2.1 “Healthcare professionals and staff who come into contact with patients having anticancer treatment should be provided with training on neutropenic sepsis. The training should be tailored according to the type of contact” 15% (13/88) had had neutropenic sepsis training 20% (18/88) had any central line training or clinical skills. 7/88 = 8% of these most commented they had accessed the training themselves and that it was not paediatric specific. 17/88 had no training I6 of those who said they had face to face teaching were teachers; which we assume refers to the POONS school meeting though this was not specified. Q. What would you like to see in the education package? We received a very good response to this question. Appendix 1 displays the proposed content of the package which we put into 4 main categories; background information, practicalities of care, psychosocial issues and education.
32
18
13
15
13
4
11
26
23
10
17
0 10 20 30 40
Face to Face Teaching
Clinical Skills
Supportive Care
Paediatric Palliative Care
Neutropenic Sepsis
Protocol Training
In-House Training
Telephone Support
Visit from PTC Staff
Other
None of the above
Training Received

CS evaluation report updated 20.1.15 18
Haematology / Oncology staff questionnaires – 27 returns Questions asked: Q1. Can you think of anything else we should include in the Education Package? 17/27 responses Responses received include:
Dietary advice
Emotions support
Advice
Supportive care
Information on the role of the Key Worker and GIRFEC All of the above have been incorporated into the final package contents in Appendix 1 Q2. What do you think works well in terms of communication with services external to the PTC? 25/27 responses “Good information once correct professional is identified and contacted” “Having a relationship with named person” “Direct communication with community staff, face to face visits, telephone calls” Q3. How do you think this could be improved? 23/27 responses Suggestions for improvements from PTC – shared care:
Ongoing support, particularly with the neuro-oncology patients
Greater communication with primary care GPs and local DGH
Shared care patient held documentation
A clear link to a single person in each PTC with up to date information on specific child
Documenting in case notes when other teams have been contacted, Printing email correspondence for filing
End of treatment summary
Clarity of responsibility during follow-up
1 named / link person
Support off treatment
Late effects
Transition to GP Q4. Thinking in terms of Key Working, do you see any gaps, areas for development or improvement in the care of children and young people in the community on treatment? 23/27 responses
CS evaluation report updated 20.1.15 19
Answers to this question suggested there was still confusion about the role of the key worker.
Communication
Named person/contact
“Patients discharged with no notice therefore takes time to put supportive care in place. Very distressing for parents, patients and staff”
“Need admin support to do effective key working, clear plans and evidence they are created. I think it will be interesting to see what families identify as areas they need support with”
Q5. Thinking in terms of Key Working, do you see any gaps, areas for development or improvement in the care of children and young people in the community off treatment? 18/27 responses
End of treatment summary with follow up plan
Lack of clarity about follow up and shared care – who is responsible for what?
Transition care
Maintaining good lines of communication
Need for late effects nurse to offer support and advice
Keeping local GP surgeries up to date
Developing links with educational system
“More involvement for those who may be left with some disability” Q6 Any other comments or suggestions? 8/27 responses
Shared documentation. Could current MDT be used as a forum for updates on routine info e.g. someone travelling home, parents struggling with home issues in PTC after new diagnosis and dilemmas are discussed?
Main issue is PTC – shared care communication pathways that are not reliant on anxious families. Duty bound to use GIRFEC documentation as pan-Highland.
Support for bereaved siblings
It would be good if there could be a process for regular feedback from the community to nursing staff on the ward about how children are doing who are not in-patients, not just when they have to come in to hospital for treatment”
Conclusions from scoping exercise
Following the survey it was reassuring to discover that the majority of staff would appreciate an education package. We asked for ideas for the content of the package and the results were divided into 4 main categories (Appendix 1). The information from all the surveys influenced the development of the education package. As well as the questionnaires we have examined all the available information and education resources

CS evaluation report updated 20.1.15 20
around the country. The end result will be a comprehensive sign-posting system so that information about all the various aspects of childhood cancer that has been requested will be easily accessible.
Initially, we envisaged the education package would be a hard copy. However, when asked how the package should be delivered the response overwhelmingly asked for it to be electronic as it would be easily accessible and updated. The MSN for children and young people cancer services agreed early on in the project that they would host it on their website. This would be accessed by professionals using an Athens password. Other methods of education delivery suggested were; self-directed, on-line, face to face, facilitated sessions, in-house training, tele-medicine and 1:1 meetings.
From a parent / carer and professional perspective, communication needed to be improved. To address this we developed a family held treatment record to be used between centres. We consulted staff and parents in the development of this and CLIC Sargent assisted us with the design. Initially, it was designed for use in Scotland however, CLIC Sargent are adapting it for use throughout the UK.
As a result of a GP interface meeting we developed a standard letter which will be personalised by the POONS and sent to the child / young person’s GP/HV shortly after diagnosis. This letter has been approved by the MSN.
Overall recommendations from scoping exercise
Regular and ongoing contact between all healthcare professionals and a named person is imperative
Regular and ongoing contact between the families and their Key Worker / POONS particularly during maintenance
Improved clarity of Key Worker role is required
MSN and project team working in unison throughout the project and beyond
Any recommendations / developments need to be in line with GIRFEC
Development of shared care documentation and education package
Continued pan Scotland working beyond project – development of MSN nurses’ group
Limitations
Wording of some questions made analysis tricky, e.g. when asked the purpose of a visit by the POONS, the majority of parents answered clinical where these visits also involve support.
Limited IT skills of project co-ordinators meant relying on clinical effectiveness which was time consuming and led to a delay in original timeline.
Many families were very specific about diagnosis which meant their anonymity was compromised therefore this information was blacked out..
CS evaluation report updated 20.1.15 21
Cascade effect of survey monkey questionnaire to professionals meant we were reliant on others to act.
Pan-Scotland working – geography. Initially this was a concern, however, we, as a team have worked well, building on each other’s strengths. We met regularly and communicated via telephone and email.
Lessons learnt
Development of questionnaires took a lot longer than initially anticipated due to consultation process, pilot of survey monkey and reliance on clinical effectiveness team.
Wording in parent / young person questionnaires could have been worded better to capture relevant information.
We under estimated the amount of time it would take to gather the contact details for all patients and GPs to send out the questionnaires by post (patients) and email (staff).
Cascading of professional survey monkey meant reliance on others which led to key staff being missed. This was picked up after the survey monkey was closed when one of the project coordinators was networking. That particular group of staff were then given the opportunity to contribute in person with one of the project co-ordinators. This made us question how many others have been missed.
We underestimated the time it would take to manually collate the written comments from both family and professional questionnaires.
Initial timeframe of two years was breached due to the amount of work the scoping exercise generated – the secondment was extended by three months for one coordinator
IT Company employed by the MSN were slow in delivering service which impacted on the completion date for the package. Final package should be on the MSN website by January 2015.
Evaluation of the seconded Educator posts CLIC Sargent provided £167,798 over three years for three nurses to be seconded from the NHS to complete this project supporting both the CLIC Sargent Key Worker agenda and the NHS Scotland agenda for children’s cancer services. In parallel CLIC Sargent provided £210,512 funding over three years for three Key Workers in Edinburgh, Glasgow and Aberdeen. This education project has strengthened collaborative working throughout Scotland by the project co-ordinators liaising closely with the POONS from the beginning of the project. This education package will assist the Key Worker in their role as networking across Scotland has been improved; educational resources will be able to be accessed quickly for community teams and can be tailored to the needs of the child. It is envisaged that more care closer / at home can be organised due to increased support networks.
CS evaluation report updated 20.1.15 22
This was a fantastic development opportunity for the project co-ordinators, enabling them to work at national level. As we were from different posts within paediatric oncology (outreach, ward and education) we complimented each other and utilised our individual strengths and experience to successfully complete the project. This project has given the project co-ordinators the opportunity to utilise and enhance their project management skills, improve communication links and networking opportunities. Leading a project at national level has been a learning curve for all three co-ordinators and has equipped us with transferrable skills and increased confidence. As a result of this project we feel that communication links have been improved pan-Scotland and will continue with the development of the MSN nurses group. We will all be returning to our roles within Paediatric Haematology / Oncology however, we will continue to communicate with each other and promote the education package and future developments that may arise through the MSN nurses group. Throughout this project we have shared our resources; e.g. clinical policies, learning contracts and orientation programmes for new staff nurses and raised awareness of learning opportunities which we will continue to do. It has been a great professional development opportunity for us and we hope we can encourage others to take advantage of future opportunities. Coincidental outcomes of the project
Networking at the beginning of the project led to collaborative working between the project co-ordinators and the MSN AHP group who have contributed to certain aspects of the education package. Now these links have been made they will be strengthened in the future.
Networking at the MSN / GP interface meeting early on in the project led to the development of a standard letter which will be sent out by the POONS following diagnosis to improve timely communication.
The drug information is not there as the CCLG pharmacy group has agreed to take this on so that the information given to parents would be the same throughout the UK. The CCLG heard about the work the project co-ordinators were doing through the MSN pharmacy group as we initially approached them for advice and support.
Establishment of the MSN Nurses group – whilst networking at the beginning of the project it was evident we needed a nurses group as part of the MSN. This group now meets three times a year with representatives from all over Scotland.
Dissemination
CS evaluation report updated 20.1.15 23
Eductaion package will be launched as part of the MSN website at the MSN education day
Project co-ordinators will present / promote the education package in their area
The link to the education package will be on the GP/HV letter initially sent out by the POONS on diagnosis.
Flier or business like card with link on it to be given to any professional caring for a child or young person with cancer
Poster presentation at relevant conferences
Evaluation report will be available to all staff within project co-ordinators’ area.
Conclusion A scoping exercise was carried out to inform the development of the education package. It is envisaged that within the next few months it will become standard practice for the GP contact letter and shared care document (parent held treatment record) to be utilised throughout Scotland. The first print of the parent held treatment record was funded by NHS Lothian. The education package will be hosted on the MSN website and accessed by many professionals and in these ways, the overall and local support for professionals, children and young people with cancer and their families will be enhanced. References CLIC Sargent (2009) More than my illness: Delivering quality care for children with cancer. <www.clicsargent.org.uk CLIC Sargent (2010) More than my illness: Delivering quality care for young people with cancer. <www.clicsargent.org.uk National Institute for health and Excellence (2005). Guidance on Cancer Services. Improving Outcomes in Children and Young People with cancer. The Manual. www.nice.org.uk Scottish Government. GIRFEC (Getting it Right for Every Child http://www.edinburgh.gov.uk/info/20170/girfec
CS evaluation report updated 20.1.15 24
Appendix 1 – Content of Education Package Introduction to CYP cancer services in Scotland Fact sheets on ‘Things you should know’
Leukaemia
Solid tumours
Palliative care
Introduction to cancer in children and young people (General Information) The team supporting the CYP with Cancer and their family.
CYP with cancer hospital services PTC and Shared Care Current literature patients and families receive Information on local resources and services available Getting it Right for Every Child (GIRFEC) Play preparation Hospital Passport Beads of Courage / Rainbow Trail
Glossary of terms Background Information
Cancer types in the CYP (Leuk ALL AML) Presentations of common cancers in the CYP Understanding treatment Chemotherapy Surgery Radiotherapy Immunotherapy Stem cell transplantation Clinical trials Regimens Prognosis
Drug Information
Supportive Care Febrile Neutropenia Central line care Pain relief Nutritional support / dietary information Chemotherapy induced nausea & vomiting (CINV) Side-effects of treatment Generic side-effects of chemotherapy (Pharmacy sheet) Mucositis Infection (Chicken pox, measles and shingles) PCP prophylaxis Immunisations
CS evaluation report updated 20.1.15 25
Side-effects secondary to steroids Corticosteroids Steroid myopathy Avascular necrosis Weight gain Challenges Coping with invasive procedures Taking medicines Hairloss and Body Image Limb sparing surgery and amputation Regression / enforced dependency Changes in behaviour Sleeping Fatigue Psychosocial Care Staff support Financial support Communication How to talk about diagnosis Advice on telling other children Supporting the family: what can you do? Supporting normal life Integration back to school Transitional care Late effects and survivorship Pets Palliative Care Background statistics Children’s and Young People’s Acute Deterioration Management Plan (CYPADM) Regional services information Managing symptoms Talking about Death and Dying / Preparation for loss Bereavement care Health Professional Education available in Scotland Courses Clinical Skills updates
26
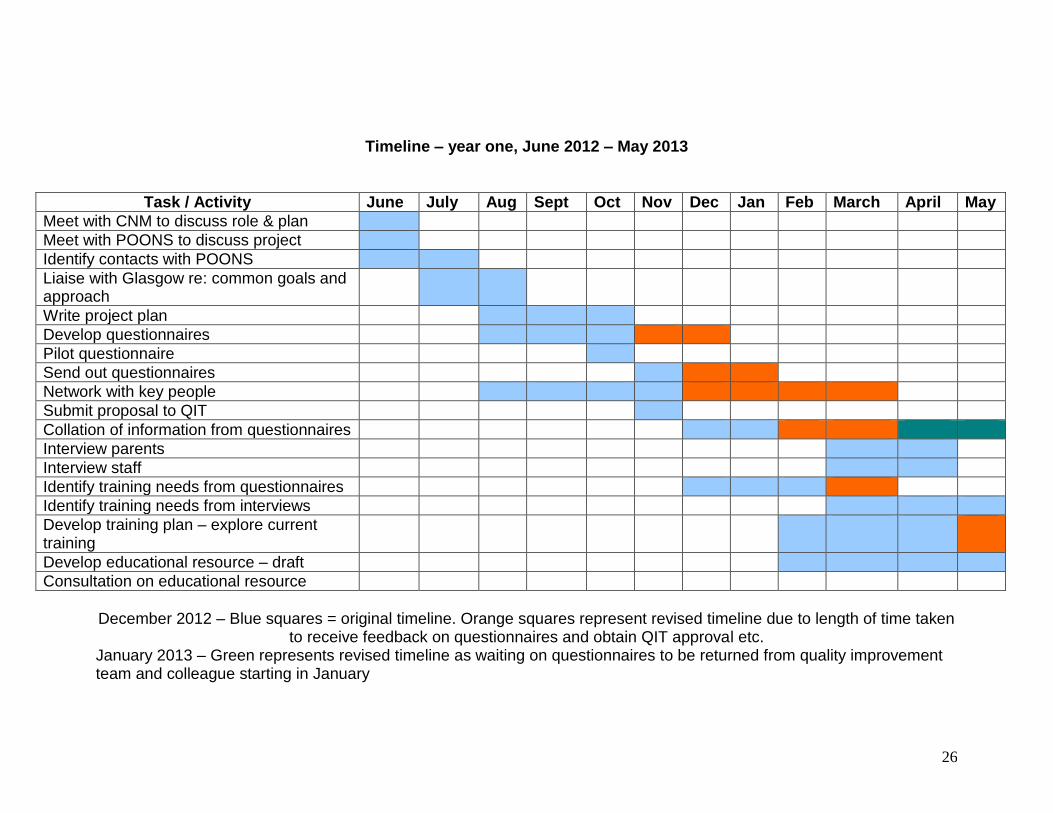
Timeline – year one, June 2012 – May 2013
Task / Activity June July Aug Sept Oct Nov Dec Jan Feb March April May
Meet with CNM to discuss role & plan
Meet with POONS to discuss project
Identify contacts with POONS
Liaise with Glasgow re: common goals and approach
Write project plan
Develop questionnaires
Pilot questionnaire
Send out questionnaires
Network with key people
Submit proposal to QIT
Collation of information from questionnaires
Interview parents
Interview staff
Identify training needs from questionnaires
Identify training needs from interviews
Develop training plan – explore current training
Develop educational resource – draft
Consultation on educational resource
December 2012 – Blue squares = original timeline. Orange squares represent revised timeline due to length of time taken
to receive feedback on questionnaires and obtain QIT approval etc. January 2013 – Green represents revised timeline as waiting on questionnaires to be returned from quality improvement team and colleague starting in January

27
Year two – June 2013 – June 2014
Task / Activity June July Aug Sept Oct Nov Dec Jan Feb March April May
Interview parents
Interview staff
Develop educational resource – draft
Consultation on educational resource
Printing
Education delivery
Launch educational resource

28