classification and management of acute and chronic pain in
TRANSCRIPT

Classification and Management of Acute and Chronic pain in Sickle Cell
Disease
1
Deepika S. Darbari, MDChildren’s National Medical Center
Professor of Pediatrics
George Washington University School of Medicine
and Health Sciences
Washington DC

Learning Objective:
• Pain in sickle cell disease can result from many underlying causes
• Phenotypes of pain in SCD may differ based on underlying mechanisms
• Pain taxonomy describing diagnostic criteria (AAPT and AAAPT) may be helpful in classifying pain phenotypes
• Understanding of pain phenotypes/mechanisms is crucial for selecting appropriate therapies for improving outcomes
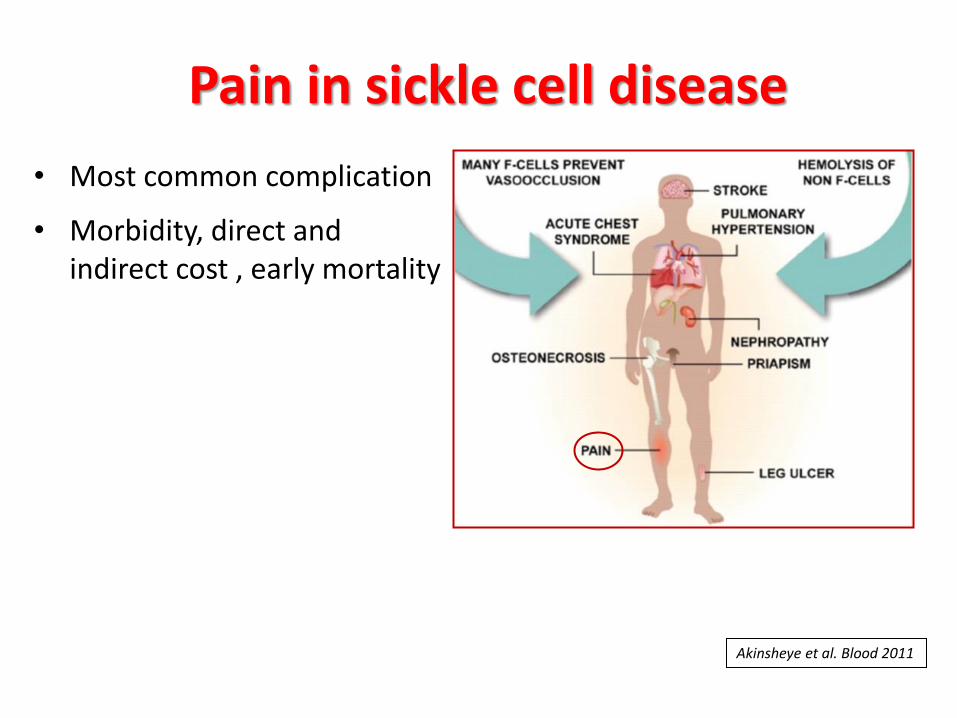
Pain in sickle cell disease
• Most common complication
• Morbidity, direct and indirect cost , early mortality
Akinsheye et al. Blood 2011

All pains in SCD are not created equal!

Acute vaso-occlusive episodes
• Hallmark manifestation
• Acute Pain (Dactylitis). 6-8 months
• 5 cardinal signs of acute inflammation : – rubor (redness),
– calor (increased heat),
– tumor (swelling),
– dolor (pain),
– functio laesa (loss of function)
– Ischemia- reperfusion physiology (reperfusion injury)
Ischemia-Reperfusion Injury
Two distinct phases of Ischemia/Reperfusion:
• 1. Ischemia caused by interruption of vascular supply leads to tissue injury
• 2. Reperfusion is associated with resolution of occlusion and resupply of oxygen →inflammatory phase → systemic inflammation→ remote organ injury/ multi-organ dysfunction syndrome

Zhang et al. Blood 2016
Vaso-occlusion in SCDA multicellular and multistep model

Zhang et al. Blood 2016
Vaso-occlusion in SCDA multicellular and multistep model

Cells involved
• Sickle RBC
• Platelets
• Neutrophils
• Monocytes
• Endothelial cells
• Mast cells
Molecules/mediators • Pro-inflammatory
cytokines through the NF-kB pathway (TNF-α, ILs, endothelin-1, PG E2.
• Chemokines• Coagulation cascade• HMGB
Vaso-occlusion in SCD A multicellular and multistep model

Mechanisms underlying vaso-occlusion
• Vaso-occlusion in SCD arises from a complex cascade of interactions among RBCs, neutrophils, and endothelial cells
• Blockage of vasculature through multiple adhesive events
• Ischemia-reperfusion injury secondary to ongoing intermittent microvascular occlusions promotes chronic inflammation

Field et al. J pain. 2019
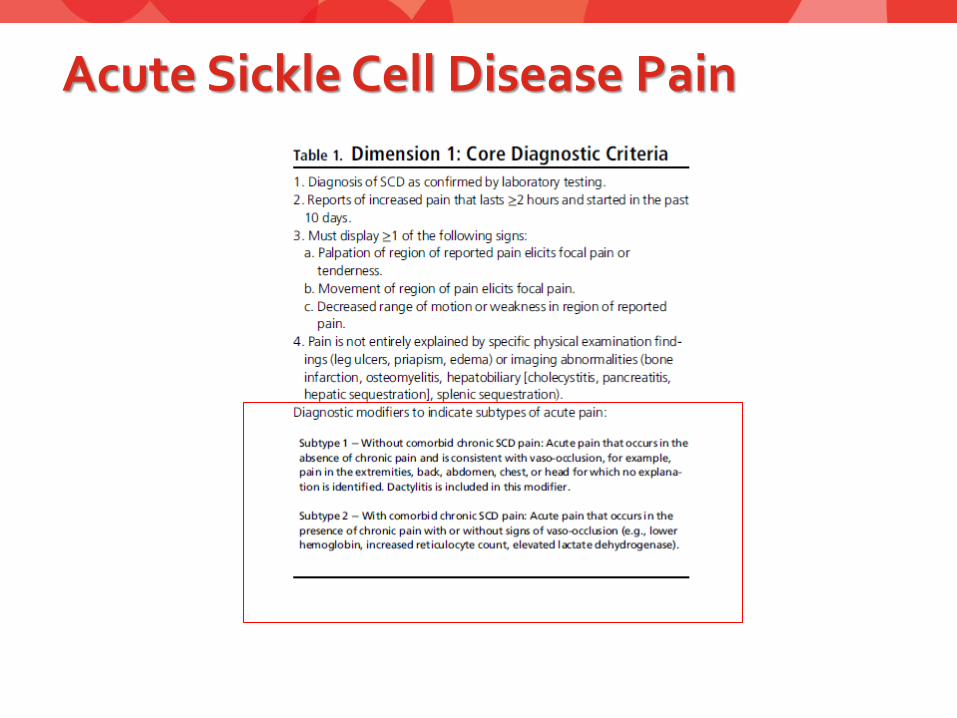
Acute Sickle Cell Disease Pain

Burden of Pain Increases with Age
Smith. Am Soc Hematol Education Program 2010

Vaso-occlusive episodes vs. daily pain
Smith et al Annals Int Med 2008

Smith W R et al. Ann Intern Med 2008;148:94-101
> 50% of patients experienced pain on >50% of the days;
30% experiened pain > 95% of the days
Episodes of daily pain

Chronic pain in sickle cell disease

Chronic SCD Pain
• Presence of SCD• Pain on most days in past 6
months• Display a sign on
exam/imaging• Not explained by other
diagnosis
• Modifiers: Chronic SCD Phenotypes
1) The Chronic SCD pain without contributory disease complications
2) Chronic SCD pain with contributory disease complications
3) Mixed pain type



Neuroplasticity/ Central sensitization
Latremoliere and Woolf. J Pain. 2009
Central sensitization: Increased responsiveness of nociceptive neurons in the central nervous system (increased sensitivity)
Characterized by reduction in pain thresholds and expansion of receptive field of the motor neurons
Changes occur in - Neurons in the dorsal horn cells-Spinal nucleus pars caudalis-Thalamus, amygdala and - Ant. cingulate cortex
Could be triggered by inflammation

Multiple Cellular Processes that Lead to Central Sensitization
Latremoliere and Woolf. J Pain. 2009

Hyperalgesia and after sensations in patients with SCD vs. matched non-SCD controls
Darbari et al. Scan J Pain 2017

Differences in brain connectivity patterns by pain burden
24
High pain group: Greater pronociceptive connectivity (Panel A)
• Greater connectivity between pro-nociceptive structures such as the insula and secondary somatosensory cortex.
• Greater connectivity between DMN regions and pro-nociceptive pain structures
Low pain group: Greater antinociceptive connectivity (Panel B)
• Greater connectivity between the primary somatosensory cortex and an antinociceptive region of the cingulate (subgenual) (associated with endogenous analgesic mechanisms)
Darbari et al. J Pain 2015

Chronic persistent/daily pain of SCD • Chronic (> 3 months) pain is common
• Starts in adolescents and young adult years
• Comorbidities (poor sleep, anxiety, depression)
• SCD complications +/- (avascular necrosis, leg ulcer)
• Poor response to standard therapy
• Underlying mechanisms are not completely clear: recurrent VOC, neuropathic pain, sensitization of central/peripheral nervous system →altered pain processing/ perception → spontaneous pain

Field et al. J pain. 2019
Mechanisms and modulators of acute and chronic SCD pain

SCD Pain Phenotypes
Peripheral
(nociceptive)
Peripheral
neuropathic/
sensitization
Central neuropathic/
sensitization
Underlying
mechanism
Inflammation or
mechanical damage of
tissues
Damage or dysfunction of
peripheral nerves
Altered central pain processing
Pain
characteristics
Throbbing, sharp,
pounding, dull
Local
Burning, heavy sensation, or numbness along the path of the affected nerve. Allodyniaand hyperalgesia
Hyperalgesia/allodynia
Diffuse pain
Response to
therapy
NSAID, opioid responsive Responds to both peripheral
and centrally acting
pharmacological therapies,
gabapentinoids
Responsive to neuroactive
compounds altering levels of
neurotransmitters of pain
Classic
examples
Osteoarthritis
Rheumatoid arthritis
? SCD acute VOC
Diabetic neuropathic pain
Post-herpetic neuralgia
SCD -related
peripheral
neuropathies
? SCD persistent pain
Fibromyalgia
Irritable bowel syndrome
TMJD, Tension headache
? SCD chronic pain
Darbari et al. EJH.2014
Suggested Management of Pain by Phenotypes

Evidence-based management of sickle cell disease: expert panel report, 2014
Acute Pain
Management
Guidelines 2014
• Treat promptly/ aggressively
• Reassess and individualize
• Non-opioids (anti-inflammatory)
• Opioids/ PCA
• Use non-pharmacologic
modalities (heat)

Chronic Pain
Management
Guidelines
Evidence-based management of sickle cell disease: expert panel report, 2014
• Etiology of pain
• Believe patient report
• Individualize
treatment plan with
the patient
• Evaluate patient
regularly
• One primary provider
for opioids
• Manage opioid side
effects
• Treat comorbidities:
Psychiatrist, addiction
specialist, social
worker
• Non-pharmacologic
adjuvant therapy

Chronic pain in SCD • While many patients may have chronic pain associated with
AVN/ leg ulcers etc. there is often no anatomic correlate to explain the pain
• Likely due to a different mechanism than vaso-occlusion/ disease complication alone
• Pathophysiology not completely clear but could be related to nerve damage, sensitization, inflammation, and/or opioid use
• Central sensitization associated with opioid use and psychological comorbidities and traits can contribute to a chronic pain phenotype.
• Patients may report exacerbations (or “crises”)

Field JJ 2017 ASH
1. Focus resources on adults with chronic pain (high rates of utilization for pain)
2: Aggressively treat SCD/ any underlying causes of pain- AVN- HU- Chronic transfusion
3: Apply principles of chronic pain management/ opioids.
Higher doses/ larger quantities of oral opioids do not help

Managing comorbidities
• Psychological co-morbidities are common in patients with chronic diseases including SCD
• Depression, anxiety, poor sleep quality are often present especially in patients with high pain burden
• Certain traits such as catastrophizing can make individuals at higher risk for developing chronic pain
• Parents with catastrophizing can increase the risk of high pain burden in child in SCD
• Co-morbidities can contribute and make pain worse
• Managing comorbidities is necessary

Chronic pain in SCD: Current gaps
- Risk factors / predictors of chronic pain
- Mechanisms/ central sensitization
- Role of opioid
- Long term effect of therapy on development of chronic pain (HU, Chronic transfusion, opioids)
- Impact of early HSCT
- Role of adjuvant therapies
- Non-pharmacologic approaches
- Endpoints/ biomarkers for therapeutic trials ( PRO/non-PRO)

Integrative Approaches for Managing pain

CDC data:Nationwide opioid crisis
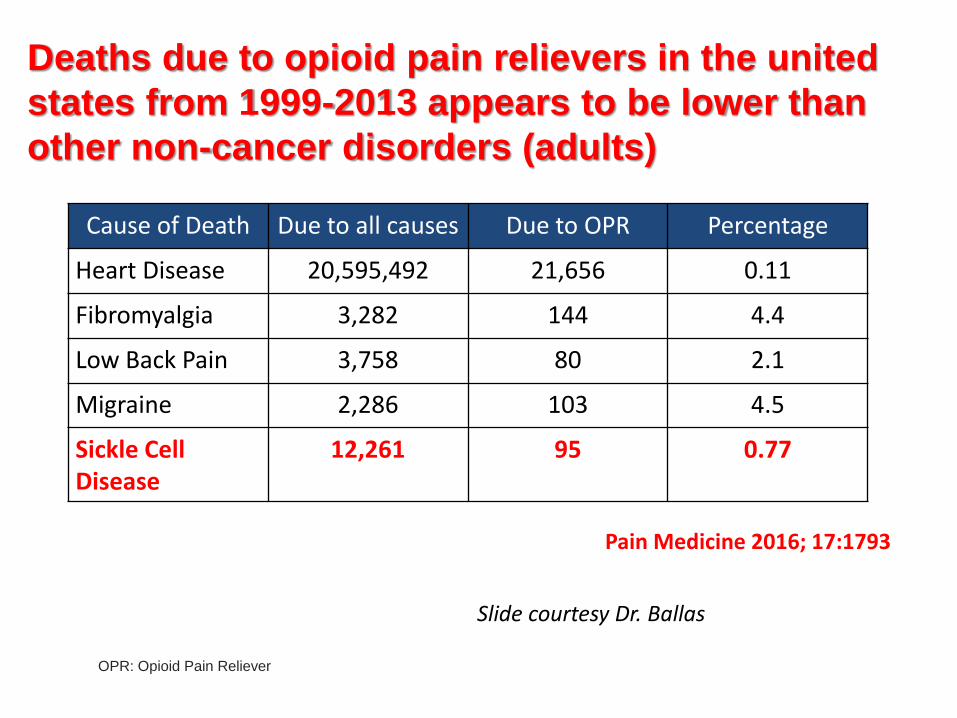
Deaths due to opioid pain relievers in the united
states from 1999-2013 appears to be lower than
other non-cancer disorders (adults)
OPR: Opioid Pain Reliever
Cause of Death Due to all causes Due to OPR Percentage
Heart Disease 20,595,492 21,656 0.11
Fibromyalgia 3,282 144 4.4
Low Back Pain 3,758 80 2.1
Migraine 2,286 103 4.5
Sickle Cell Disease
12,261 95 0.77
Pain Medicine 2016; 17:1793
Slide courtesy Dr. Ballas

J Natl Compr Canc Netw. 2020 Apr;18(4):392-399 2020

Integrative Medicine Clinic for SCD
• Multi-disciplinary clinic held in the division of Hematology
• Comprehensive Services:
• Hematology
• Pain management
• Psychology
• Social work
• Physical therapy
• Healing touch
• Aromatherapy
• Massage therapy
• Acupuncture/Acupressure
Disease modifying
Rx
Counselling
Physical therapy
AcupunctureAroma
Psychosocial
Mind body
Integrative care for sickle cell
pain
Complement Ther Med. 2020;49:102287.

Summary and conclusions
• Pain/chronic pain is common in sickle cell disease
• Pain phenotypes may vary based on underlying etiology
• One or more mechanisms may be active at a given time in a patient ( AAPT modifiers)
• Management of chronic pain is a long process
• Be cognizant of opioid related comorbidities
• Use principles of managing sickle cell disease and chronic pain to effectively manage a patient with SCD and chronic pain
