classificationsystemfor thesuddenunexpectedinfant...
TRANSCRIPT

Classification System for the Sudden Unexpected InfantDeath Case Registry and its Application
abstractSudden unexpected infant deaths (SUID) accounted for 1 in 3 postneo-natal deaths in 2010. Sudden infant death syndrome and accidentalsleep-related suffocation are among the most frequently reportedtypes of SUID. The causes of these SUID usually are not obvious beforea medico-legal investigation and may remain unexplained even afterinvestigation. Lack of consistent investigation practices and an autopsymarker make it difficult to distinguish sudden infant death syndromefrom other SUID. Standardized categories might assist in differentiat-ing SUID subtypes and allow for more accurate monitoring of the mag-nitude of SUID, as well as an enhanced ability to characterize thehighest risk groups. To capture information about the extent to whichcases are thoroughly investigated and how factors like unsafe sleepmay contribute to deaths, CDC created a multistate SUID Case Registryin 2009. As part of the registry, the Centers for Disease Control andPrevention developed a classification system that recognizes the un-certainty about how suffocation or asphyxiation may contribute todeath and that accounts for unknown and incomplete informationabout the death scene and autopsy. This report describes the classi-fication system, including its definitions and decision-making algo-rithm, and applies the system to 436 US SUID cases that occurredin 2011 and were reported to the registry. These categories, althoughnot replacing official cause-of-death determinations, allow local andstate programs to track SUID subtypes, creating a valuable tool toidentify gaps in investigation and inform SUID reduction strategies.Pediatrics 2014;134:e210–e219
AUTHORS: Carrie K. Shapiro-Mendoza, PhD, MPH,a LenaCamperlengo, DrPH,a Rebecca Ludvigsen, MPH,b CarriCottengim, MA,c Robert N. Anderson, PhD,d ThomasAndrew, MD,e Theresa Covington, MPH,f Fern R. Hauck, MD,MS,g James Kemp, MD,h and Marian MacDorman, PhDd
aDivision of Reproductive Health, Centers for Disease Control andPrevention, Atlanta, Georgia; bOak Ridge Institute for Science andEducation (ORISE) Research Participant Program, Division ofReproductive Health, Centers for Disease Control and Prevention,Atlanta, Georgia; cDB Consulting Group, Inc., Atlanta, Georgia;dDivision of Vital Statistics, National Center for Health Statistics,Centers for Disease Control and Prevention, Hyattsville,Maryland; eOffice of Chief Medical Examiner, State of NewHampshire, New Hampshire; fNational Center for Child DeathReview, Michigan Public Health Institute, Okemos, Michigan;gDepartments of Family Medicine and Public Health Sciences,University of Virginia, Charlottesville, Virginia; and hDivision ofPediatric Allergy, Immunology and Pulmonary Medicine,Washington University, St Louis, Missouri
KEY WORDSsudden infant death syndrome, sudden unexpected infant death,infant mortality, accidental suffocation, classification, child deathreview, surveillance
ABBREVIATIONSCDC—Centers for Disease Control and PreventionCDR—child death reviewICD-10—Tenth Revision of the International Classification ofDiseasesNCRPCD—National Center for the Review and Prevention of ChildDeath (formerly the National Center for Child Death Review)SIDS—sudden infant death syndromeSUID—sudden unexpected infant death
Dr Shapiro-Mendoza conceptualized and designed theclassification system, coordinated and supervised thedevelopment and revision of categorization instruments, led theactivities related to assignment of cases to categories, drafted,revised, and wrote the final version of the manuscript, andoversaw the project in general; Dr Camperlengo and Ms Ludvigsenparticipated in conceptualizing the categories, led activities tomodify data collection instruments, provided technical assistanceregarding review, data entry, and quality control for stategrantees, carried out the initial analyses, and critically reviewedthe manuscript; Ms Cottengim provided technical assistanceregarding review, data entry, and quality control for stategrantees, carried out the final analyses, and critically reviewedthe manuscript; Ms Covington participated in conceptualizing thecategories, designed the data collection instruments, providedtechnical assistance regarding review, data entry, and qualitycontrol for state grantees, carried out the initial analyses, andcritically reviewed the manuscript; Drs Anderson, Andrew, Hauck,Kemp, and MacDorman participated in conceptualizing thecategories and critically reviewed the manuscript; and all authorsapproved the final manuscript as submitted.
(Continued on last page)
e210 SHAPIRO-MENDOZA et al by guest on September 4, 2018www.aappublications.org/newsDownloaded from

In the United States, ∼1 in 7 infantdeaths and 1 in 3 postneonatal deathswere attributed to sudden unexpectedinfant death (SUID) in 2010.1 The mostfrequently reported causes of SUID aresudden infant death syndrome (SIDS),ill-defined and unknown cause ofmortality, and accidental sleep-relatedsuffocation.2 Differentiating betweenthese causes, especially SIDS and in-fant suffocation, can be challenging,because SUID case investigations arenot always conducted in a standardmanner, and universally accepted def-initions or biological markers to dis-tinguish SIDS from suffocation do notexist.3,4 To complicate matters, bothSIDS and accidental sleep-related suf-focations are frequently unwitnessedand occur in unsafe sleeping environ-ments. SIDS is reserved for deaths thatremain unexplained after a thoroughcase investigation.5 Accidental sleep-related suffocation relies on scene ev-idence of an infant being suffocated orstrangulated by items or persons ina sleep environment. A standardizedclassification system with carefullydelineated criteria that recognizes in-conclusive evidencemight assist in thisdifferentiation. Moreover, such a systemmay allow for improved monitoring ofSUID, enhance our ability to character-ize the highest risk groups, and identifypathophysiologic and genetic mecha-nisms underlying these deaths.
Currently we rely on death certificatestomonitorpopulationestimates of SUIDmortality. Unfortunately our ability toaccuratelymonitor SIDS and other SUIDis hindered by situations in which thecause of death reported on the deathcertificate may not be classified andcoded as the certifier intended. Forexample, the Tenth Revision of the In-ternational Classification of Diseases(ICD-10) does not provide a uniquecodingcategory for the termSUID. Thus,reports of SUID are often coded as SIDS,even though certifiers may use them to
mean different things.6 As a result ofthese challenges in investigating, re-porting, and classifying deaths, wehave an incomplete understanding ofactual SUID trends and risk factors.Because vital records do not reveal theextent to which cases may have beenthoroughly investigated, or how factorslike unsafe sleep may contribute todeath, the Centers for Disease Controland Prevention (CDC) created the SUIDCase Registry in 2009.7–9
On January 1, 2010, the SUID CaseRegistry pilot program began activelycollecting data in 5 states (Colorado,Georgia,Michigan, NewJersey, andNewMexico) using methods described else-where.9 On January 1, 2011, 2 additionalstates (Minnesota and New Hampshire)began collecting data. These stateswere awarded cooperative agreementswith the CDC after a competitive pro-posal process. A major objective of thisnew SUID Case Registry was to createa classification system using standard-ized definitions to assign categories tocases reported in the case registry.Several SIDS and SUID definitions andclassifications have recently been pro-posed,10–18 although not universallyaccepted, underscoring the need forconsistent and standardized SUID re-porting practices. This report describesthe classification system used by theSUID Case Registry, including its stan-dardized definitions and decision-makingalgorithm, and applies the categoriza-tion process to 436 SUID cases. Thesewere cases that occurred in 2011 andwere reported to the registry fromparticipating states. The algorithmguides the assignment of cases intoexplained (“Suffocation with unsafesleep factors”) and unexplained cate-gories (“No autopsy or death sceneinvestigation,” “Incomplete case infor-mation,” “No unsafe sleep factors,”“Unsafe sleep factors,” and “Possiblesuffocation with unsafe sleep factors”).These categories are not intended to,
and do not, replace official cause-of-death determinations, but are meantto apply a common categorization pro-cess to cases to allow local and stateprograms to better track and un-derstand SUID.
FLOW OF DATA FROM CASEIDENTIFICATION TOCATEGORIZATION
The SUID Case Registry program andhow it builds on the infrastructure ofchild death review (CDR) teams hasbeen previously reported.9 Briefly, theRegistry is a population-based, multi-state surveillance program developedin partnership with the National Centerfor the Review and Prevention of ChildDeath (NCRPCD), formerly the NationalCenter for Child Death Review.9 Localand state CDR teams operate understate legislation and program policies.However, with funding from CDC forincreased staffing and resources alongwith technical assistance, grantees (ie,state health departments or their bonafide agents) comprehensively reviewall resident SUID cases.
Figure 1 describes the flow of the SUIDCase Registry data from the time of caseidentification to the time of SUID cate-gory assignment. SUID cases are identi-fied by CDR teams using severalmethods, including notification frommedical examiner or coroner offices andnotification from state vital statisticsoffices. For each case, the multidisci-plinary CDR team (including medicalexaminers, coroners, law enforcement,public health representatives, otherhealth care providers, and social servicerepresentatives) reviews and discussesSUID case information from retrospec-tively collected death scene inves-tigations, autopsies, medical records,and other medico-legal reports. The CDRteam also identifies actionable strate-gies to help prevent future deaths andimprove case investigation. The CDRteam enters this information in the web-
SPECIAL ARTICLE
PEDIATRICS Volume 134, Number 1, July 2014 e211 by guest on September 4, 2018www.aappublications.org/newsDownloaded from

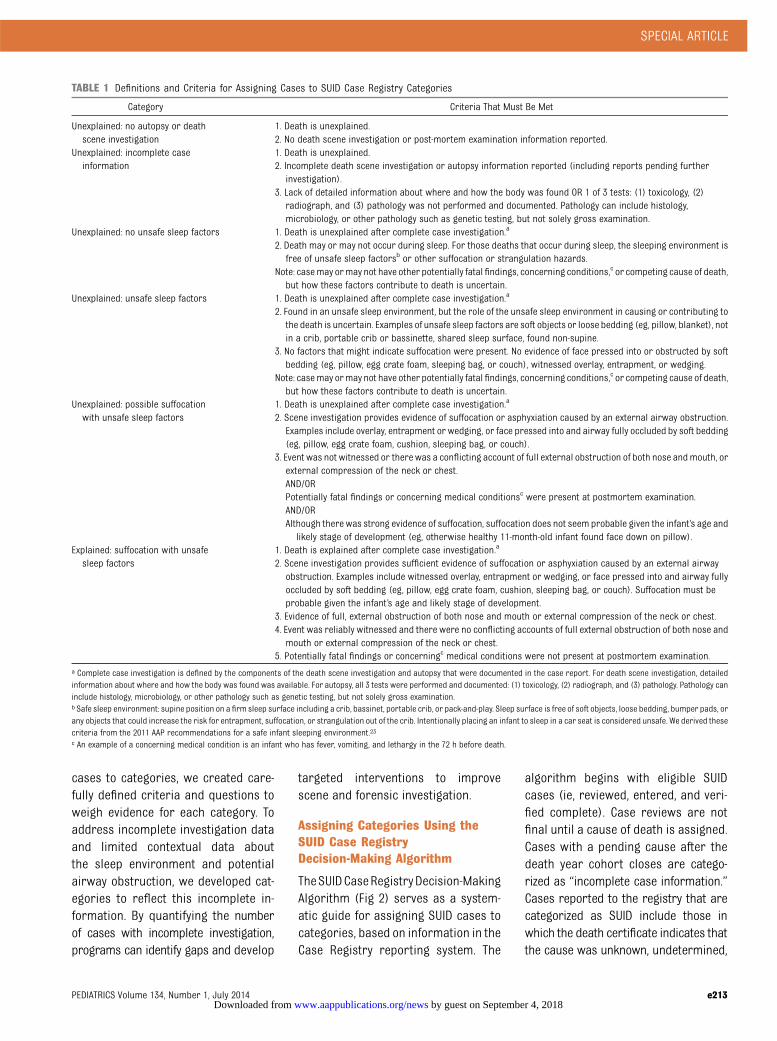
based NCRPCD Case Report,19 whichincludes a standard set of questionsdeveloped specifically to review SUIDcases.20 The CDC receives de-identifieddata for all SUID cases reported fromparticipating states and examines datafor completeness. States are asked toreconcile any missing and unknownvariables. Once the CDC receives themost complete information, CDC staffreview cases and assign categoriesusing the standardized definitions anddecision-making algorithm. An explana-tion of these SUID categories and crite-ria used to define these groupings aredescribed in Table 1. These categoriescan be used to identify risk factors andcharacteristics of infant deaths thatcould be potentially prevented, to im-prove scene investigation and autop-sies, and to identify potential cases for
clinical research. Personally identifyinginformation is not available aboutcases, and resulting categorizations donot alter previously ascribed officialcause-of-death determinations. In otherwords, these categories are strictly forsurveillance purposes and do not re-place official medical examiner or cor-oner cause-of-death determinations.
DEVELOPING STANDARDDEFINITIONS FOR SUID CASEREGISTRY SURVEILLANCE
Although we considered other SUIDclassification systems,10–18 none com-pletely fit the surveillance and pro-grammatic purposes of the SUID CaseRegistry. In 2010, Sidebotham21 en-couraged that any new categoricaldefinitions be simple and improve on
earlier classification systems. As such,our SUID Case Registry classificationsystem incorporates the contributionsof other colleagues.13,16,22 Similar toRandall et al16 and Pasquales-Styleset al,22 the SUID Case Registry systemrecognizes the importance of possibleasphyxia or suffocation in sudden un-expected and unexplained infant deathcases. Like Randall et al,16 our systemalso recognizes the degree of uncer-tainty that can accompany deaths inpotentially asphyxiating environments.Also like others,13,16,17 we acknowledgethe uncertainty resulting either frominadequate review of the death sceneor incomplete forensic examination,and incorporated this uncertainty inour category definitions. To that end,like the Krous et al13 system and theAvon system,17 we have included a cat-egory, “no unsafe sleep factors,” to ac-count for the proportion of unexplaineddeaths that occurred in an environmentin which unsafe sleep factors were notidentified. Our categories and defi-nitions overlap with many of Randallet al,16 although our labels and criteriawere created to meet the aims of theSUID Case Registry. Although we did notlimit definitional categories to specificinfant age groups (eg, postneonatalperiod or until 6 or 8months of age)13 orrequire that a death occur during sleeplike some earlier classifications,10,13,15
our categories allow further stratifica-tion by age and sleep status, dependingon analytic needs.
In creating categories, we also con-sidered the challenges reported withearlier categorization schemes.13,15–17
These challenges include reviewer di-agnostic preferences, incomplete sceneinvestigation and forensic investigationrecords, and lack of information aboutwhere and how the infant was found(including detailed factors about thesleeping environment), especially as re-lated to airway obstruction. To reduce in-consistency among reviewers in assigning
FIGURE 1Flow of SUID Case Registry data from case identification to categorization.
e212 SHAPIRO-MENDOZA et al by guest on September 4, 2018www.aappublications.org/newsDownloaded from
cases to categories, we created care-fully defined criteria and questions toweigh evidence for each category. Toaddress incomplete investigation dataand limited contextual data aboutthe sleep environment and potentialairway obstruction, we developed cat-egories to reflect this incomplete in-formation. By quantifying the numberof cases with incomplete investigation,programs can identify gaps and develop
targeted interventions to improvescene and forensic investigation.
Assigning Categories Using theSUID Case RegistryDecision-Making Algorithm
TheSUIDCaseRegistryDecision-MakingAlgorithm (Fig 2) serves as a system-atic guide for assigning SUID cases tocategories, based on information in theCase Registry reporting system. The
algorithm begins with eligible SUIDcases (ie, reviewed, entered, and veri-fied complete). Case reviews are notfinal until a cause of death is assigned.Cases with a pending cause after thedeath year cohort closes are catego-rized as “incomplete case information.”Cases reported to the registry that arecategorized as SUID include those inwhich the death certificate indicates thatthe cause was unknown, undetermined,
TABLE 1 Definitions and Criteria for Assigning Cases to SUID Case Registry Categories
Category Criteria That Must Be Met
Unexplained: no autopsy or deathscene investigation
1. Death is unexplained.2. No death scene investigation or post-mortem examination information reported.
Unexplained: incomplete caseinformation
1. Death is unexplained.2. Incomplete death scene investigation or autopsy information reported (including reports pending further
investigation).3. Lack of detailed information about where and how the body was found OR 1 of 3 tests: (1) toxicology, (2)
radiograph, and (3) pathology was not performed and documented. Pathology can include histology,microbiology, or other pathology such as genetic testing, but not solely gross examination.
Unexplained: no unsafe sleep factors 1. Death is unexplained after complete case investigation.a
2. Death may or may not occur during sleep. For those deaths that occur during sleep, the sleeping environment isfree of unsafe sleep factorsb or other suffocation or strangulation hazards.
Note: casemay ormay not have other potentially fatal findings, concerning conditions,c or competing cause of death,but how these factors contribute to death is uncertain.
Unexplained: unsafe sleep factors 1. Death is unexplained after complete case investigation.a
2. Found in an unsafe sleep environment, but the role of the unsafe sleep environment in causing or contributing tothe death is uncertain. Examples of unsafe sleep factors are soft objects or loose bedding (eg, pillow, blanket), notin a crib, portable crib or bassinette, shared sleep surface, found non-supine.
3. No factors that might indicate suffocation were present. No evidence of face pressed into or obstructed by softbedding (eg, pillow, egg crate foam, sleeping bag, or couch), witnessed overlay, entrapment, or wedging.
Note: casemay ormay not have other potentially fatal findings, concerning conditions,c or competing cause of death,but how these factors contribute to death is uncertain.
Unexplained: possible suffocationwith unsafe sleep factors
1. Death is unexplained after complete case investigation.a
2. Scene investigation provides evidence of suffocation or asphyxiation caused by an external airway obstruction.Examples include overlay, entrapment or wedging, or face pressed into and airway fully occluded by soft bedding(eg, pillow, egg crate foam, cushion, sleeping bag, or couch).
3. Event was not witnessed or therewas a conflicting account of full external obstruction of both nose andmouth, orexternal compression of the neck or chest.AND/ORPotentially fatal findings or concerning medical conditionsc were present at postmortem examination.AND/ORAlthough there was strong evidence of suffocation, suffocation does not seem probable given the infant’s age and
likely stage of development (eg, otherwise healthy 11-month-old infant found face down on pillow).Explained: suffocation with unsafe
sleep factors1. Death is explained after complete case investigation.a
2. Scene investigation provides sufficient evidence of suffocation or asphyxiation caused by an external airwayobstruction. Examples include witnessed overlay, entrapment or wedging, or face pressed into and airway fullyoccluded by soft bedding (eg, pillow, egg crate foam, cushion, sleeping bag, or couch). Suffocation must beprobable given the infant’s age and likely stage of development.
3. Evidence of full, external obstruction of both nose and mouth or external compression of the neck or chest.4. Event was reliably witnessed and there were no conflicting accounts of full external obstruction of both nose and
mouth or external compression of the neck or chest.5. Potentially fatal findings or concerningc medical conditions were not present at postmortem examination.
a Complete case investigation is defined by the components of the death scene investigation and autopsy that were documented in the case report. For death scene investigation, detailedinformation about where and how the body was found was available. For autopsy, all 3 tests were performed and documented: (1) toxicology, (2) radiograph, and (3) pathology. Pathology caninclude histology, microbiology, or other pathology such as genetic testing, but not solely gross examination.b Safe sleep environment: supine position on a firm sleep surface including a crib, bassinet, portable crib, or pack-and-play. Sleep surface is free of soft objects, loose bedding, bumper pads, orany objects that could increase the risk for entrapment, suffocation, or strangulation out of the crib. Intentionally placing an infant to sleep in a car seat is considered unsafe. We derived thesecriteria from the 2011 AAP recommendations for a safe infant sleeping environment.23c An example of a concerning medical condition is an infant who has fever, vomiting, and lethargy in the 72 h before death.
SPECIAL ARTICLE
PEDIATRICS Volume 134, Number 1, July 2014 e213 by guest on September 4, 2018www.aappublications.org/newsDownloaded from

SIDS, SUID, unintentional sleep-relatedasphyxia /suffocation/strangulation,unspecified suffocation, cardiac or re-spiratory arrest without other well-defined causes, or unspecified causeswith potentially contributing unsafesleep factors. Cases in which mannerof death is reported as homicide, areexcluded. Two trained members of the
CDC’s SUID Case Registry program staffreview and categorize each case byapplying the algorithm that consistsof a series of questions (Fig 2). Staffmembers work together to reach con-sensus about the assignment of a par-ticular category. This process can becompleted in∼7 minutes. In those casesin which the 2-member review team
cannot concur, the case is conservativelygrouped in the category reflecting themost uncertainty, eg, “Unexplained:Possible suffocation with unsafe sleepfactors” versus “Explained: Suffocationwith unsafe sleep factors.” After theinitial review, all cases that are catego-rized as “Explained: Suffocation withunsafe sleep factors” and the few cases
FIGURE 2Decision-making algorithm for assigning SUID case registry categories. *Category includes cases that may or may not have other potentially fatal findingsconcerning conditions, or competing cause of death, but how these factors contribute to death is uncertain.
e214 SHAPIRO-MENDOZA et al by guest on September 4, 2018www.aappublications.org/newsDownloaded from

(,10 of those reported for our analy-sis) that cannot be reconciled arereviewed by 2 other program staff anda category is assigned by group con-sensus. The former cases are reviewedbecause of the high degree of difficultyof distinguishing these cases from un-explained, possible suffocation withunsafe sleep factors (see below). Thissecondary review takes ∼5 minutes.Data are received quarterly and casesare categorized on an ongoing basis.
To use the algorithm (Fig 2), one mustapply the SUID Case Registry’s defini-tion for a complete case investigation(includes both death scene investiga-tion and autopsy) and a safe sleep en-vironment (Table 1). At a minimum, thedeath scene investigationmust providesufficiently detailed information for thereviewers to envision where and howthe body was found. For an autopsy tobe considered complete, it must in-clude evidence that the following testswere performed and documented: (1)toxicology, (2) radiograph, and (3) pa-thology. Pathology can include histol-ogy, microbiology, or other pathologysuch as genetic testing, but not solelygross examination. These minimal cri-teria were based on expert opinionand a National Association of MedicalExaminers white paper.8 A safe sleepenvironment is 1 where: (1) the infantis found supine on a firm sleep surfaceincluding a crib or bassinet mattress,portable crib, or pack-and-play, and (2)the sleep surface is free of soft objects,loose bedding, bumper pads or anyobjects that could increase the risk forentrapment, suffocation, or strangula-tion. We derived these criteria from the2011 AAP recommendations for a safeinfant sleeping environment.23
Categories are based on the com-pleteness of the case investigation, in-cluding death scene investigation,autopsy, and medical history. Catego-ries are used to distinguish accidentalsleep-related suffocations from other
SUID groupings. Categories are furthersubdivided as “Explained” and “Un-explained” (Table 1 and Fig 2).
The 2 categories, “No autopsy or deathscene investigation” and “Incompletecase information,” are the easiest todistinguish (Table 1 and Fig 2). Theremaining categories, which aim todistinguish how or if an unsafe sleep-ing environment contributed to thedeath, are more difficult to differenti-ate, although each has complete caseinformation by definition.
The category, “no unsafe sleep factors,”includes cases that may or may nothave occurred during sleep or ina sleeping environment (Table 1 andFigure 2). For deaths occurring duringsleep or in a sleeping environment, nopotentially asphyxiating hazards werereported. In contrast, cases assigned“Unsafe sleep factors” are those foundin an unsafe sleep environment, but therole of the potential suffocation orstrangulation hazards relative to deathis uncertain. This category includescases in which the scene investigationdoes not provide any evidence of air-way obstruction. For example, if an in-fant is sharing a sleep surface with anadult and there is no documentationthat the adult overlaid the infant or thatthe infant’s airway was obstructed, thedeath is called “Unsafe sleep factors.”In such cases, the evidence about theairway is insufficient to categorize asexplained or possible suffocation.
The most difficult task is distinguishingbetween “Unexplained: Possible suffoca-tion with unsafe sleep factors” and“Explained: Suffocationwith unsafe sleepfactors.” To categorize a case as “Ex-plained: Suffocation with unsafe sleepfactors,” there must be strong evidenceof suffocation (eg, report of full ob-struction of nose and mouth or externalcompression of the neck or chest). Also,the event must be reliably witnessedwith no conflicting reports or docu-mented potentially fatal findings or otherconcerning medical conditions. Someexamples are: (1) a 1-month-old infantfound face down in a pillow with hernose and mouth fully obstructed; (2) a 2-month-old infant found with her headand face wedged between the cushionsat the back of the sofa; and (3) a 4-month-old who is found lifeless in a twin bedwith his head and body underneath hismother. On the other hand, deaths cate-gorized as “Unexplained: Possible suffo-cation with unsafe sleep factors,” havesome evidence that suffocationmay haveoccurred, but information about a fullyobstructed airway is weak or not basedon a reliable witness account, or there isevidence of potentially fatal findings orother concerning conditions. An exampleof a case that would be assigned to“Unexplained: Possible suffocation withunsafe sleep factors” is an infant pre-viously assumed to be healthy, but whohas an atrial septal defect found at au-topsy and was found face down on top of
TABLE 2 Definitions of Mechanisms for Suffocation or Possible Suffocation
SUID Category Definition
Mechanisms forsuffocation
Factors in the sleep environment that caused or may have caused suffocation.
Overlay Shared sleep surface with other person overlaying or rolling on top of or againstinfant while sleeping and obstructing airway or compressing the neck or chestarea and preventing respiration.
Soft bedding Soft or loose bedding, pillows, or stuffed toys on sleep surface obstructing airway.Infant found face down or other position with airway obstruction.
Wedging orentrapment
Wedging and entrapment of an infant between 2 objects such as a mattress andwall, bed frame, or furniture causing airway obstruction or compressing chestand preventing respiration.
Other Other factors in thesleepenvironmentcausinganairwayobstruction, forexample,a situation inwhich an infant is sleeping in a car seat or stroller and the infant’sface or neck position results in an airway obstruction.
SPECIAL ARTICLE
PEDIATRICS Volume 134, Number 1, July 2014 e215 by guest on September 4, 2018www.aappublications.org/newsDownloaded from

a pillow. Although the infant was foundface down on a pillow with his nose andmouth obstructed, evidence of a compet-ing potentially fatal finding (i.e, atrialseptal defect) precludes assignment tothe explained suffocation category. Im-portantly, in instances in which thereviewers cannot concur when differ-entiating between explained suffocationand unexplained possible suffocation,the case is assigned as an unexplainedpossible suffocation.
Mechanisms of AccidentalSuffocation in a Sleep Environment
Cases categorized as possible and ex-plained suffocation with unsafe sleepfactors are further grouped by mecha-nism (Table 2). These mechanisms in-clude: (1) overlay by a person, (2) softbedding, (3) wedging/entrapment, and(4) others, such as suffocation by aplastic bag. When a single mechanismcannot be assigned for a particular case,more than 1 option may be selected andsuch cases are grouped togetheras “2 ormore mechanisms identified.” Analysisof themechanisms attributed to possibleor explained suffocation might providefurther insight into modifiable risk fac-tors in the sleep environment andquantify the contribution of differentmechanisms to suffocation deaths.
Development of theDecision-Making Algorithm
The development of the algorithmwas aniterative process and was conductedbetween 2009 and 2013. During its de-velopment, we applied the category def-initions and algorithm to nearly 1000cases reported in the SUID Case Registrysystem data files. In assigning cases tocategories, the algorithm highlightedlimitations in theability of thecasereportto fully capture where and how a bodywas found and whether there was anyobstruction of the airway, especially thenose and mouth. Because of this limita-tion, we modified the case report formwith improved questions and wording
and trained grantees how to incorporatethese changes. Before finalizing, we ap-plied the algorithm and category defi-nitions to all cases reported to theregistry in 2011 (the most recent yearwith completed data) that met the casedefinition. Minor revisions to wordingwere made to improve clarity.
Application of the ClassificationSystem
Table 3 shows the aggregated data fromthe initial 7 SUID Case Registry states(Colorado, Georgia, Michigan, Minnesota,New Hampshire, New Jersey, and NewMexico) and the categories to which thecases were assigned. Of the 436 SUIDcases identified in 2011, most (n = 382;88%) were classified as unexplainedSUID and most occurred in an unsafesleep environment (n = 320; 73%). “Suf-focation with unsafe sleep factors” wasassigned to 54 cases (12%), and 95 cases(22%) were assigned to “Possible suffo-cation with unsafe sleep factors.” In 5
states with 35 or more reported cases(Colorado, Georgia, Michigan, Minnesota,and New Jersey), the proportion of caseswithout a documented complete investi-gation varied, ranging widely from 5% to55%. Also in these states, the highestproportion of deaths (with complete in-formation) were assigned to the cate-gory “Unsafe sleep factors” (range, 45%–63%), followed by “Possible suffocationwith unsafe sleep factors” (range, 20%–36%), “Suffocation with unsafe sleepfactors” (range, 15%–25%), and “No un-safe sleep factors” (all states had ,5deaths in this category). Of the 66 pos-sible and explained suffocation deathsin these states, the mechanism mostfrequently reported was soft bedding(n = 63), followed by overlay (n = 29),wedging/entrapment (n = 18), and other(10) (Table 4).
DISCUSSION
We have built on and strengthened thework of other investigators in defining
TABLE 3 Number and Percentage of the 436 Cases Occurring in 2011 and Reported to the SUIDCase Registry by SUID Category, by All Cases, and by Those With Complete CaseInformation Only
SUID Category Total Cases Percentage of Cases by Statea
Number % A B C D E
All categoriesTotal n 436 100% b b b b b
UnexplainedNo death scene investigation or autopsy 11 3 0 3 10 0 3Incomplete case information 101 23 5 33 27 55 8No unsafe sleep factors 4c ,1 2 0 2 0 3Unsafe sleep environment 171 39 51 30 40 21 44Possible suffocation with unsafe sleep factors 95 22 23 23 13 14 28
ExplainedSuffocation with unsafe sleep factors 54 12 18 11 10 11 15
Incomplete informationd 112 26 5 36 37 55 10
Categories with complete information onlyUnexplainedNo unsafe sleep factors 4c 1 2 0 3 0 3Unsafe sleep environment 171 53 54 46 63 45 49Possible suffocation with unsafe sleep factors 95 29 25 36 20 30 31
ExplainedSuffocation with unsafe sleep factors 54 17 19 17 15 25 17
a States are represented by letters to maintain confidentiality. Percentages for states with fewer than 35 reported deaths arenot calculated owing to small numbers and resulting unstable estimates.b The 436 cases reported by state in 2011 include: CO (44), GA (111), MI (142), MN (39), NH (6), NJ (63), and NM (31).c Three deaths occurred during a sleeping period and 1 did not.d Incomplete information: no death scene investigation or autopsy plus incomplete case information.
e216 SHAPIRO-MENDOZA et al by guest on September 4, 2018www.aappublications.org/newsDownloaded from

and categorizing SIDS and other SUIDfor the purposes of the SUID CaseRegistry.10–17,19–21 Our classificationsystem emphasizes the uncertaintyabout how suffocation or asphyxiationmay have contributed to death and alsoaccounts for unknown and incompleteinformation about the death scene andautopsy. Until comprehensive sceneinvestigations are conducted on allSUID cases and standardized criteriaare universally accepted by death cer-tifiers, states and local public healthprograms can use information gath-ered from the SUID Case Registry andits classification system as a supple-ment to death certificate surveillance.We estimate that the current 9 statesparticipating in the registry capture∼13% of all US SUID. The registry’sstandardized categories allow pro-grams to quantify the number of cases
that: (1) have incomplete investiga-tions; (2) occur in an unsafe sleep en-vironment such as with soft bedding orwith a shared sleep surface; and (3)are possible or explained suffocationcases by mechanism. By identifyingand quantifying incomplete case in-formation, local and state jurisdictionscan identify strategies and target ap-propriate resources to improve sceneand forensic investigations, as well aschild death review programs. Addi-tionally, these categories may helpprograms better understand the cir-cumstances that potentially contributeto or actually cause suffocation or as-phyxiation, which could lead to morestrategic interventions.
Strengths
The SUID Case Registry’s process forassigning cases to categories of
explained and unexplained SUID hasseveral strengths. First, program staffand collaborators built on the work ofother investigators10–17,19–21 and cre-ated categories that meet local andstate surveillance and program needs.Second, categorization relies on stan-dardized definitions of SUID subtypesand a simple decision-making algo-rithm with explicitly defined criteriawith labels that are descriptive andeasy to distinguish from 1 another. Fi-nally, the system has been applied tohundreds of cases with assignment ofcategories based on group consensusby trained reviewers.
Another potential strength of thesestandardized categories may extendbeyond the registry and its surveillancepurposes. The categories could be usedby researchers conducting epidemio-logic and biomarker studies to definecases according to the degree of cer-tainty about potentially contributing as-phyxiation factors. Researchers couldalso use these categories to identifynew mechanisms and factors associ-ated with SUID. In addition, the SUIDCase Registry categories can be easilygroupedunderexisting ICD-10 codes forcomparison with vital statistics datafrom death certificates. Specificallythe categories “No autopsy or deathscene investigation” and “Incompletecase information” could be groupedunder the ICD-10 code R99, “Ill-definedand unknown cause of mortality.” The“explained” category, “Suffocation withunsafe sleep factors,” correspondswith ICD-10 code W75, “Accidental suf-focation and strangulation in bed.” Theremaining categories, all with com-plete case investigations but withvarying degrees of uncertainty aboutcontributing factors, could be groupedunder the ICD-10 code R95, “SIDS.” Fi-nally, if death certifiers eventually ac-cepted these categories or a modifiedversion, the categories could be usedas a future rubric to make and report
TABLE 4 Number of Cases Categorized as “Possible Suffocation With Unsafe Sleep Factors” or“Suffocation With Unsafe Sleep Factors” by Mechanism, SUID Case Registry, 2011 Deaths
Number of Casesa by Mechanismb
Soft Bedding Overlay Wedging orEntrapment
Other 2 or More
All casesc
Possible suffocation with unsafe sleep factors(n = 95)
49 17 6 7 4
Suffocation with unsafe sleep factors (n = 54) 17 12 12 3 5Cases by stateState APossible suffocation with unsafe sleep factors
(n = 26)1 0 4 2 0
Suffocation with unsafe sleep factors (n = 20) 3 3 1 1 3State BPossible suffocation with unsafe sleep factors
(n = 33)27 1 4 2 2
Suffocation with unsafe sleep factors (n = 16) 7 4 6 0 1State CPossible suffocation with unsafe sleep factors
(n = 8)5 3 1 1 2
Suffocation with unsafe sleep factors (n = 6) 2 3 2 0 1State DPossible suffocation with unsafe sleep factors
(n = 6)6 0 0 0 0
Suffocation with unsafe sleep factors (n = 5) 2 1 0 2 0State EPossible suffocation with unsafe sleep factors
(n = 11)6 1 2 2 0
Suffocation with unsafe sleep factors (n = 6) 3 0 3 0 0a Because fewer than 35 deaths were reported in NH and NM in 2011, data are not presented.b Multiple mechanisms can be assigned per case, but none of the 100 cases categorized had .2 mechanisms identified.Because each case can be assigned.1 mechanism, the sum of the mechanisms is greater than the total number of cases.c “All cases” includes reported cases from CO, GA, MI, MN, NH, NJ, and NM.
SPECIAL ARTICLE
PEDIATRICS Volume 134, Number 1, July 2014 e217 by guest on September 4, 2018www.aappublications.org/newsDownloaded from

cause-of-death determinations on thedeath certificates.
Challenges in Categorizing Deaths
Although this classification system islargely automated, the qualitative partof the review issubjectiveandcannotbeautomated. To reduce potential biasfrom this qualitative analysis, our sys-tem applies standardized definitions,has trained reviewers who agree oncategories through consensus, has asecondary review process, and relies ona guiding principle to err on the side ofcaution (ie, when in doubt, choose thecategory thatreflects the leastcertainty).
Thegreatest challenge ingroupingSUIDcases into defined categories is havingsufficient evidence available about thesleep environment and airway. CDRteams must rely on retrospectivelycollected information about the deathscene investigation. Of the 436 casesreported in 2011 to our surveillancesystem, 190 had a report of a scene re-enactment. Case reports with missingor unknown information for variablescompromise data quality and com-pleteness. In our data, one-quarter ofthe cases had incomplete information,although this varied widely betweenstates. Missing and unknown infor-mation can lead to a different catego-rizationoutcomethan the truecategory.
Because the states participating in theregistry likely have greater access tocritical death scene investigation dataand are able to use more resources toeliminate missing information thannon-fundedstates, generalizationaboutthe distribution of deaths in each cat-egory relative to other US states orpopulations may be limited. The CDC’sSUID Case Registry now operates in 9states: Arizona, Colorado, Louisiana,Michigan, Minnesota, New Hampshire,New Jersey, NewMexico, and Wisconsin.If the registry were to become a na-tional surveillance system, the qualityof data about circumstances sur-rounding SUID could be enhanced inmore states, and investigators andprograms could have a deepened un-derstanding of the magnitude of andcharacteristics associated with SUID.
CONCLUSIONS
The SUID Case Registry’s classificationsystem has built on the work of otherinvestigators in defining and categoriz-ing SIDS and other SUID cases, whilerecognizing the uncertainty about thecontribution of asphyxiation to the deathand also accounting for variations incase investigations. This new system hasbeen tested with hundreds of cases andhas performed well when categorizingchallenging cases. Finally, the systemhas
key implications for both public healthand clinical research. For public health,the classification system allows localand state programs to more accuratelytrack the magnitude of specific types ofSUID over time, creating a valuable toolto identify gaps in case investigation ofSUID and an enhanced ability to identifythe highest risk groups who mightbenefit from focused interventions orincreased services. For clinical inves-tigation, consistent reporting of SIDS andother SUID is crucial for identifyingpathophysiologic and genetic mecha-nisms underlying these deaths.
ACKNOWLEDGMENTSWe acknowledge the following contribu-tors for their critical input and advice inconceptualizing this project: Kim Collins,MD,TimothyE.Corden,MD,JohnFudenberg,D-ABMDI, Geoffrey Smith, MD, Bradley T.Thach,MD, andGregoryWyatt. Also, spe-cial thanks to Shin Kim, MPH, for hercontributions in conceptualizing theclassification system and reviewingan early draft, and to Alexa Erck, MPH,for her assistance with analysis andthoughtful review of the final draft ofthe manuscript. Finally, we thank theNCRPCD and the CDR coordinators inthe participating states for their sup-port of this project by allowing accessto the data contained in this report.
REFERENCES
1. United States Department of Health and Hu-man Services (US DHHS), Centers for DiseaseControl and Prevention (CDC), National Centerfor Health Statistics (NCHS). CompressedMortality File (CMF) on CDC WONDER OnlineDatabase. CMF 1999–2010, Series 20, No. 2P,2013. Available at: http://wonder.cdc.gov/mortsql.html. Accessed May 2, 2014
2. Shapiro-Mendoza CK, Tomashek KM, AndersonRN, Wingo J. Recent national trends insudden, unexpected infant deaths: moreevidence supporting a change in classifi-cation or reporting. Am J Epidemiol. 2006;163(8):762–769
3. Camperlengo LT, Shapiro-Mendoza CK, KimSY. Sudden infant death syndrome: di-agnostic practices and investigative poli-cies, 2004. Am J Forensic Med Pathol. 2012;33(3):197–201
4. Randall BB, Paterson DS, Haas EA, et al. Po-tential asphyxia and brainstem abnormalitiesin sudden and unexpected death in infants.Pediatrics. 2013;132(6). Available at: www.pe-diatrics.org/cgi/content/full/132/6/e1616
5. Willinger M, James LS, Catz C. Defining thesudden infant death syndrome (SIDS):deliberations of an expert panel convenedby the National Institute of Child Health and
Human Development. Pediatr Pathol. 1991;11(5):677–684
6. Kim SY, Shapiro-Mendoza CK, Chu SY,Camperlengo LT, Anderson RN. Differentiatingcause-of-death terminology for deaths codedas sudden infant death syndrome, accidentalsuffocation, and unknown cause: an inves-tigation using US death certificates, 2003–2004. J Forensic Sci. 2012;57(2):364–369
7. Shapiro-Mendoza CK, Kim SY, Chu SY, KahnE, Anderson RN. Using death certificates tocharacterize sudden infant death syn-drome (SIDS): opportunities and limi-tations. J Pediatr. 2010;156(1):38–43
e218 SHAPIRO-MENDOZA et al by guest on September 4, 2018www.aappublications.org/newsDownloaded from

8. Corey TS, Hanzlick R, Howard J, Nelson C,Krous H; NAME Ad Hoc Committee on SuddenUnexplained Infant Death. A functional ap-proach to sudden unexplained infant deaths.Am J Forensic Med Pathol. 2007;28(3):271–277
9. Shapiro-Mendoza CK, Camperlengo LT, KimSY, Covington T. The sudden unexpectedinfant death case registry: a method toimprove surveillance. Pediatrics. 2012;129(2). Available at: www.pediatrics.org/cgi/content/full/129/2/e486
10. Beckwith JB. Defining the sudden infantdeath syndrome. Arch Pediatr Adolesc Med.2003;157(3):286–290
11. Fleming PJ, Blair PS, Sidebotham PD, HaylerT. Investigating sudden unexpected deaths ininfancy and childhood and caring for be-reaved families: an integrated multiagencyapproach. BMJ. 2004;328(7435):331–334
12. Hanzlick R, Hunsaker JC III, Davis GJ. AGuide for Manner of Death Classification.Atlanta, GA: National Association of MedicalExaminers; 2002
13. Krous HF, Beckwith JB, Byard RW, et al.Sudden infant death syndrome and un-classified sudden infant deaths: a defini-
tional and diagnostic approach. Pediatrics.2004;114(1):234–238
14. Randall BB, Wadee SA, Sens MA, et al. Apractical classification schema incorpo-rating consideration of possible asphyxiain cases of sudden unexpected infantdeath. Forensic Sci Med Pathol. 2009;5(4):254–260
15. Shields LB, Hunsaker JC III, Corey TS,Stewart D. Is SIDS on the rise?? J Ky MedAssoc. 2007;105(8):343–353
16. Randall B, Donelan K, Koponen M, Sens MA,Krous HF. Application of a classificationsystem focusing on potential asphyxia forcases of sudden unexpected infant death.Forensic Sci Med Pathol. 2012;8(1):34–39
17. Blair PS, Byard RW, Fleming P. Proposal foran international classification of SUDI.Scand J Forens Sci. 2009;2009(1):6–9
18. Blair PS, Byard RW, Fleming PJ. Suddenunexpected death in infancy (SUDI): sug-gested classification and applications tofacilitate research activity. Forensic SciMed Pathol. 2012;8(3):312–315
19. The National Center for Child Death Review.Child Death Review Case Reporting System:
Case Report 2.0. Available at: www.child-deathreview.org/reports/CDRCaseReport-Form02202008.pdf. Accessed March 27,2014
20. Covington TM. The US National Child Deathreview case reporting system. Inj Prev.2011;17(suppl 1):i34–i37
21. Sidebotham P. Do we need a new definitionfor SIDS?: Commentary on “Sudden un-expected death in infancy and the dilemmaof defining the sudden infant death syn-drome” by Henry Krous. Curr Pediatr Rev.2010;6(1):13–14
22. Pasquale-Styles MA, Tackitt PL, Schmidt CJ.Infant death scene investigation and theassessment of potential risk factors forasphyxia: a review of 209 sudden un-expected infant deaths. J Forensic Sci.2007;52(4):924–929
23. Moon RY, Darnall RA, Goodstein MH, et al;Task Force on Sudden Infant Death Syn-drome. SIDS and other sleep-related infantdeaths: expansion of recommendations fora safe infant sleeping environment. Pedi-atrics. 2011;128(5). Available at: www.pedi-atrics.org/cgi/content/full/128/5/e1341
(Continued from first page)
This work was presented in abstract form at the American Association of SIDS Prevention Physicians 22th Annual Conference, Naples, Florida, September 19 to 21,2013.
The findings and conclusions in this paper are those of the authors and do not necessarily represent the official position of the Centers for Disease Control andPrevention.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-0180
doi:10.1542/peds.2014-0180
Accepted for publication Apr 7, 2014
Address correspondence to Carrie K. Shapiro-Mendoza, PhD, MPH, Maternal and Infant Health Branch, Division of Reproductive Health, Centers for Disease Controland Prevention, Mailstop F-74, 4770 Buford Highway NE, Atlanta, GA 30341-3717. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: Ms Covington’s agency, the Michigan Public Health Institute, received funds from EGS that originated at the Centers for Disease Controland Prevention in the amount of $233,076.48 for the period April 1, 2009 to May 31, 2011, to develop and support components of the SUID Case Registry described inthe article (reference 09FED907750, contract GS07F67053R). The other authors have indicated they have no financial relationships relevant to this article todisclose.
FUNDING: This work was supported in part by the Maternal and Infant Health Branch, Division of Reproductive Health, National Center for Chronic DiseasePrevention and Health Promotion, Centers for Disease Control and Prevention, and in part by Federal funds from the Centers for Disease Control and Preventionunder contract GS07F67053R.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
COMPANION PAPER: A companion to this article can be found on page e240, online at www.pediatrics.org/cgi/doi/10.1542/peds.2014-0602.
SPECIAL ARTICLE
PEDIATRICS Volume 134, Number 1, July 2014 e219 by guest on September 4, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-0180 originally published online June 9, 2014; 2014;134;e210Pediatrics
Hauck, James Kemp and Marian MacDormanCottengim, Robert N. Anderson, Thomas Andrew, Theresa Covington, Fern R.
Carrie K. Shapiro-Mendoza, Lena Camperlengo, Rebecca Ludvigsen, Carriits Application
Classification System for the Sudden Unexpected Infant Death Case Registry and
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/134/1/e210including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/134/1/e210#BIBLThis article cites 20 articles, 5 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/public_health_subPublic Healthhttp://www.aappublications.org/cgi/collection/sids_subSIDSsubhttp://www.aappublications.org/cgi/collection/fetus:newborn_infant_Fetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on September 4, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-0180 originally published online June 9, 2014; 2014;134;e210Pediatrics
Hauck, James Kemp and Marian MacDormanCottengim, Robert N. Anderson, Thomas Andrew, Theresa Covington, Fern R.
Carrie K. Shapiro-Mendoza, Lena Camperlengo, Rebecca Ludvigsen, Carriits Application
Classification System for the Sudden Unexpected Infant Death Case Registry and
http://pediatrics.aappublications.org/content/134/1/e210located on the World Wide Web at:
The online version of this article, along with updated information and services, is
ISSN: 1073-0397. 60007. Copyright © 2014 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on September 4, 2018www.aappublications.org/newsDownloaded from