chss review report - · pdf filethis document contains the draft report of the chss review...
TRANSCRIPT

DRAFT REPORT OF CHSS REVIEW COMMITEE
This document contains the draft report of the CHSS review
committee. As decided in the meeting held with recognised
Unions/Associations a copy of the report is made available in the web
site. All Office bearers of Associations and Unions are requested to
submit their suggestions/views on the report by 31st December, 2006.
Suggestions may be sent to:
Under Secretary (Administration), DAE
Anushakti Bhavan, CSM Marg, Mumbai 400 001
By normal mail or Email: [email protected] (please mark subject as
‘CHSS Review Committee’)
November 21, 2006

1
DRAFT REPORT OF THE CHSS REVIEW COMMITTEE
The Department of Atomic Energy vide its order No.7(4)/2004-
CHSS/IR&W/8067 dated 31st October, 2005 constituted a committee
consisting of the following members to review the existing provisions of
Contributory Health Services Scheme (CHSS).
1) Shri V.P. Raja - Chairman Additional Secretary (I&M), DAE
2) Shri P. Venugopalan - Member Controller, BARC
3) Dr. D.K. Jaitly - Member Head, Medical Division, BARC
4) Shri P.M. Pawar - Member Deputy Controller of Accounts, BARC
5) Shri V. Dayalan - Member Officer on Special Duty (R&D), DAE
6) Shri P.P. Madhavan Kutty - Member Secretary Under Secretary, DAE
Consequent on the transfer of Shri V. Dayalan as CAO, IGCAR,
Shri M. Venugopalan, Deputy Secretary (A / IR&W), DAE replaced
Shri Dayalan as a Member of the Committee.
The terms of reference to the committee are as follows:-
1) examine the issues relating to eligibility criteria of dependents in
terms of age, income, residence and relationship with the employee,
etc.
2) review the existing facilities for other systems of medicines vis-à-vis
CHSS facilities

2
3) review the eligibility of beneficiaries for different classes of
accommodation, revision of subscription, checks and balance to
prevent misuse of the facilities
4) examine the issue of the long term sustainability of the current
subscription based CHSS and explore the possibility of replacing it
with medical insurance scheme
5) work out the financial implication of its recommendations along with
a proposal to finance the same without adding to the cost to the
exchequer.
The committee may call for suggestions from the recognized
Service Associations/Unions of the Department and data, if any, required
from various authorities operating the scheme and will also invite any
officer to attend its meetings.
The Committee was required to submit its report to the Department
before March 31, 2006.
The salient features of the scheme are:
The CHSS was introduced in the Department in the year 1962 by
Late Dr. H.J. Bhabha, the founder of the Nuclear Research Programme in
the country. Although all other Central Government employees were
covered either under the CGHS or CS(MA) Rules, there was an
imperative need with a legal obligation for a unique and distinctly
different medical care having regard to the functional intricacies of the
organization and hence a separate scheme i.e. CHSS was set up
exclusively in the Department. This was especially taking into account
the fact that the nature of occupation of Scientists and other employees
demanded evolving a high level medical care system involving not only a

3
routine treatment facility but a sort of medical auditing supported with a
research input as a matter of abundant caution in the area of nuclear
radiation. In the initial stage the scheme had covered only Mumbai based
units. However, as the activities of the Department expanded and
laboratories and plants were set up at different units, the scheme was
extended mutatis mutandis to many other places. In fact, in tune with the
growth of the Department, the CHSS has also recorded a phenomenal
expansion as an inbuilt system of the whole set up as a pathway to health
care in the Department and at present the scheme is in operation in 13
places like Mumbai, Tarapur, Kota, Talcher, Chennai, Kalpakkam,
Vadodara, Hyderabad, Indore, Manuguru, Tuticorin, Kolkata and
Mysore. The scheme is being administered by the following authorities:
Place Administering Year of Authority introduction
Mumbai & Mysore - Director, BARC 1962/2002
Tarapur - Station Director, TAPS 1967
Kota - Station Director, RAPS 1965
Talcher/Manuguru - Chief Executive, HWB 1977/1988 Vadodara/Tuticorin 1998/1998
Kalpakkam/Chennai - Director, IGCAR 1993/1993
Indore - Director, CAT 1986
Kolkata - Director, VECC 1998
Hyderabad - Chief Executive, NFC 2003
Scope and Application
In addition to DAE employees, the scheme covers the staff of
NPCIL, TIFR, TMC, SINP, IMSc and AEES. Employees of ECIL, IRE,
UCIL, IOP, IPR and HRI are not covered under the scheme.

4
Beneficiaries of the scheme shall not be entitled to claim
reimbursement under Central Services (Medical Attendance) Rules, 1944
for treatment availed under the modern systems of medicare while in their
concerned CHSS station.
The Scheme covers both the serving and retired employees and
their family members. Family for the purpose include employee’s
wife/husband as the case may be, dependent children upto 25 years and
dependent parents. The Scheme also provides for inclusion of one of the
dependent relatives of an employee on payment of additional contribution
equal to the average per capita expenditure. Under the Scheme, a
beneficiary is entitled to medical treatment both as an out patient and
inpatient in the Departmental Hospitals or referral hospitals recognized
under the Scheme. Treatment under the Scheme includes for both
ordinary ailments and also for specialized treatment for acute and chronic
diseases like cancer, heart ailments etc. and no cost ceiling limits have
been prescribed for any treatment. The Scheme also provides for
Pathological investigations and X-rays examinations, maternity facilities,
reimbursement of expenses incurred in medical emergencies etc.
The Committee was constituted to examine in depth the issues
listed on pages 1-2 and suggest improvements for running the scheme and
also examined the financial viability of the scheme. In other words, the
main task assigned to the Committee was to come up with suggestions/
recommendations to make the Scheme to offer better services and at the
same time make it financially more viable by generating the required
funds to meet its running cost, on a sustained basis. The “cost-
effectiveness” of various facilities provided under the scheme was also to
be looked into by the Committee.

5
As a first step towards modification of the provision of the
Scheme, a statement on about 30 points based on the queries/
clarifications sought by various units in the past was prepared. The
statement was sent to the Heads of Units eliciting their comments and
also suggestions, if any, to improve the Scheme for the consideration of
the Committee. The Committee also collected various statistical
information from the offices concerned relating to CHSS. The data so
collected and tabulated in a statement form are furnished as Annexures.
The committee held seven meetings. After detailed deliberations,
the Committee recommends the following additions/modifications/
amendments to be made in the Scheme:-
Point-1. Inclusion of dependent relatives on payment of normal contribution at 1% of the pay in lieu of per capita expenditure as existing in Clause 18.1.
Existing provision (Clause 18.1)
The employees are not ordinarily permitted to register their
dependent relatives. Notwithstanding what has been stated above, in
extra-ordinary cases the administering authorities may allow an employee
to register under the scheme, one of his/her relatives, who is entirely
dependent upon and residing with him/her on payment of an additional
contribution, at a rate equal to the average per capita expenditure (without
any element of subsidy) borne by the scheme in the preceding year. This
additional contribution would be payable for a minimum period of one
year, even when benefits are availed of for a period shorter than this.
Further, before the request for registration in this regard is entertained,
the relative must have actually been staying with the employee concerned
6
for a minimum period of 60 days. Benefits of the scheme will be allowed
to relatives on the same scale as admissible to members of family.
The term, relative, for the above purpose, would be restricted to
brothers and unmarried and widowed sisters and such near relatives only.
Recommendation
After detailed discussion, it was decided that the existing provision on this can continue having regard to the following facts:
1. The contribution is payable by the employees concerned based on per-capita expenditure, i.e. without the element of subsidy.
2. The number of employees availing of this facility is very negligible.
3. It ensures medi-care facility to the dependent brothers, sisters, etc. which otherwise sometimes would be an handicap for certain young scientists even to continue their services in the Department.
Point 2. Inclusion of a provision for medical coverage to the Scientists/Engineers visiting foreign countries on deputation or tour. Existing provision
No provision
Recommendation
It is noted that one of the conditions for travel abroad covers taking
medical insurance and as such it was decided not to make any specific
provision in this regard in the Scheme. Moreover the scheme is only for
treatment within the Country.

7
Point 3. Extension of coverage to dependent daughter/son after completion of 25 years of age and reviewing the provisions regarding registration of children/parents with regard to computation of income, staying together etc.
Existing provision (Clause 4.1(b)
Children, step-children or legally adopted children upto 25 years of
age restricted to two. Addition in the number of children can be allowed
on payment of extra contribution in respect of each child in multiples of
one extra rate for each additional child. However, as a general exception,
payment of such contribution will not be applicable for inclusion of
children in case of twin/triplet birth in the second delivery even though
there is already one living child. Children beyond the age of 18 years and
upto 25 years will be eligible for continuation under the Scheme provided
they are not gainfully employed. However, in case of any hardship, in
individual cases, for justifiable reasons, a relaxation shall be made by the
Department, on the basis of recommendation of the Head of the Unit in
the matter of upper age limit.
Parents of the prime beneficiary who are wholly dependent on the
prime beneficiary and normally residing with the prime beneficiary and
further provided the monthly income of both the parents from all sources
does not exceed Rs.4000/-.
Recommendation
The Committee felt that the present restriction of upper age limit
upto 25 years in the case of dependent children is very much reasonable
in-as-much-as the children are expected to become matured for securing
employment at this stage. This is especially for the reason that there is

8
already a provision in the Scheme to relax the age limit beyond 25 years
in deserving cases. Life long coverage is also available to the children
who are physically/mentally challenged.
As regards the question of fixing an upper limit for computation of
income, it was noted that the present ceiling of Rs.4000/- p.m. was fixed
in the year 2000 and raising the same can be considered when the present
limit under the CGHS/CS(MA) Rules which is Rs.1500/- p.m. is revised.
The Committee felt that there is no necessity to change the stipulation
that dependent should stay together with the employee to continue as
family members.
Point 4. Removal of the restriction in regard to supply of artificial hearing aids to any one of the family members on one time basis. Existing Provision Testing of vision, treatment of eye-diseases and full dental-care
will be provided free of cost. Provision of goggles, etc. is not within the
purview of the Scheme. Artificial hearing-aids will be made available to
the employee or any one of his family members on a one-time basis, on
the recommendations of ENT specialist of BARC Hospital and on the
basis of audiogram given to him/her, identifying the degree and nature of
deafness. Payment will be made directly to the manufacturer identified
by BARC Hospital. Reimbursement can be made only if the referral note
is counter-signed by the ENT specialist of BARC Hospital and duly
approved by the Head, Medical Division, BARC.
Recommendation The Committee felt that restricting supply of artificial hearing aids
to any one of the dependent family members or the employees may

9
operate harshly on the beneficiaries and it would be reasonable to extend
the facility to all the family members and the employees as may be
needed from medical view point. However, the Committee decided to fix
periodicity and ceiling limit on the amount reimbursable in respect of the
same. Director, BARC may decide the periodicity and ceiling limit in
this regard in consultation with Head, Medical Division.
Point 5. Shifting of prime beneficiary membership to the employed spouse in the event of the employee taking voluntary retirement with the liability of paying enhanced contribution.
Existing provision (letter no.7/14/98-CHSS/IR&W/317 dated November 12, 2002)
When the spouse who is the prime beneficiary by virtue of drawing
higher pay retires from service on superannuation, the option to become
the prime beneficiary may be allowed either to the retiring employee or to
the spouse who is in service even if the pay of the latter is lower. When
the retiring employee becomes prime beneficiary the option to pay one
time contribution for life long registration will also be available to him /
her.
Recommendation
The Committee noted that the facility of shifting of prime
beneficiary membership to the employed spouse exists only in the case of
superannuation and that no specific provision exists in the event of an
employee taking voluntary retirement with the liability to pay enhanced
contribution, i.e. before completion of 30 years of service. The husband
and wife team being an integral unit within the definition of family for
any benefits, the Committee felt that if either of them quits service
whether by way of resignation, superannuation or voluntary retirement,
the event should be treated on the same footing. The Committee noted
10
that even where one of the spouses is employed in the private sector, the
entire family is eligible to CHSS cover without any extra contribution.
The recommendation, therefore, is that the facility of change over of the
prime beneficiary membership to the employed spouse should be
extended without extra liability even if the concerned employee resigns or
takes voluntary retirement before completion of 30 years of service.
Point 6. Reviewing the provisions relating to registration of parents.
Existing Provision (Clause 4.1 (b)
Parents of the prime beneficiary who are wholly dependent on the
prime beneficiary and normally residing with the prime beneficiary and
further provided the monthly income of both the parents from all sources
does not exceed Rs.4000/-
Recommendation
It was observed that in a large number of cases parents who are
staying with the Scientific Officers/Engineers working in remote places
are presently not being covered under the Scheme since their income has
just crossed the prescribed limit of Rs.4,000/- p.m. This results in
hardship to the officers adversely affecting their performance. Further,
exclusion of dependent parents from such a vital facility also contributes
to the reluctance of the officers in moving to the remotely located units
where they are posted. In the circumstances, it was felt that not only there
is no necessity to change the present provision in regard to registration of
parents on the basis of income limit but it was also decided that the
ceiling limit of Rs.4000/- p.m. could be relaxed in respect of the cases as
indicated above for extension of the treatment to the parents. However,
the parents so included would be entitled to get treatment only from the
dispensaries/departmental hospitals and not from the referral hospitals.

11
Further, the facility would cease to exist when the concerned employees
are transferred from the remote locations.
Point 7. Registration after retirement within a time gap.
Existing provision
Retired employees of the Department who opt for the benefits of
the Scheme and members of their families as defined under the Scheme,
subject to the following conditions:
(i) Employees should have put in a minimum of five years service in
the Department before his/her retirement.
(ii) Employees should pay the contribution in advance for a minimum
period of one calendar year and the contribution shall be with
reference to the pay drawn by him/her prior to
retirement/invalidation. Employees may also have an option to pay
one time contribution for ten years to be eligible for life long
registration. The option to join the Scheme any time after the
retirement will be available to the employees subject to the
payment of one time contribution for life long registration as
indicated or arrears of contribution from the date of retirement.
Recommendation
The Committee recommends that an option should be given to the
retiring employees to be exercised within one month from the date of
retirement whether to continue in the medical facility or otherwise. The
option once exercised shall be final and would not be reviewed. For
those who have already retired, the existing practice of allowing them
upto 3 years to come to the CHSS fold can continue.
12
Point 8. Specifying terms and conditions for extending the CHSS facility to NPCIL and aided institutions including adjustment of expenditure.
Existing provision (Clause 2.1.16)
The scheme can be extended to the employees of such
organizations under the administrative control/responsibility of the DAE
at its discretion on such terms and conditions as may be prescribed.
Recommendation
The Committee noted that CHSS facility to employees of NPCIL
and aided institutions has been extended under the above provision and is
governed by specific instructions and as such no re-look at the same is
necessary. However, the Committee noted that the percentage of
overhead charges as being included presently in the per capita
expenditure is totally inadequate and as such the same needs to be
revised. The Committee felt that a common formula can be worked out
for calculating the per-capita expenditure to bring uniformity. There
should not be any “hidden subsidy” provided by Government, while
extending the facility to NPCIL and aided institutions. It was also
decided that the system of making payment of per capita expenditure
could be changed so as to make the same on quarterly basis instead of
yearly basis as is the practice being followed now.

13
Point 9. Specifying the places covered under CHSS in Mumbai so as to ensure inclusion of those who are staying outside the limit of the Brihan Mumbai/Navi Mumbai and also giving second option to those opted out of the Scheme in the past;
& Point 10. Providing 2
nd option to those opted out of the Scheme
earlier under changed circumstances like opening of new dispensaries, etc. Existing provision Employees of the Department of Atomic Energy who are staying
outside the limits of Brihan Mumbai and who have been exempted once
from the Scheme shall not be re-admitted to the scheme unless they shift
their residence to Brihan Mumbai. Similarly, an employee, who has been
a resident in Brihan Mumbai but shifts his/her residence outside the limits
of Brihan Mumbai may opt out of the Scheme consequent upon which
he/she will cease to be a member of the scheme with effect from the date
of receipt of such intimation by the Medical Division, BARC.
Contribution towards the Scheme will not be recoverable from him from
the succeeding month. A new entrant to the service of the Department
with Headquarters at Mumbai who stays outside Brihan Mumbai will be
given choice to opt out of the Scheme. The option once exercised shall
be final and he/she will not be allowed to rejoin the scheme unless he/she
shifts his residence to Brihan Mumbai.
Recommendation As per the above provision while membership is compulsory for
those who are staying within the Brihan Mumbai/Navi Mumbai, for those
staying outside, there is an option for availing the facility which is final
once exercised. However, it was noted that an opportunity was given in
the year 1995 to come within the fold of the Scheme on the basis of the

14
request of those who had opted out in the past and remained outside the
Scheme. Now, that with the setting up of dispensaries in places like
Dombivili, etc. a number of persons are interested to become members.
The Committee felt that it would be appropriate to give one more option
to come under the Scheme to these persons in the changed circumstances.
Point 11. Reviewing eligibility of beneficiaries for different classes of accommodation in referral hospitals.
Class of accommodation
Existing Provision
Sl.No. Category Classification of staff according to pay range
Type of accommodation
1 A Rs.4590/- or below General Ward 2 B More than Rs.4590/- but below
Rs.8000/- Room with four
beds 3 C Rs.8000/- to Rs.11500/- Room with two
beds 4 D Rs.11501/- and above Semi Private
Ward
Recommendation
After a detailed discussion on the issue of reviewing the eligibility
in the wake of increase in subscription on account of merger of DP with
basic pay, the Committee recommended that revised eligibility criteria
would be as under:
Sl.No. Category Classification of staff according to pay range
Type of accommodation
1 A Rs.6885/- or below General Ward 2 B More than Rs.6885/- but
below Rs.12000/- Room with four
beds 3 C Rs.12000/- to Rs.17250/- Room with two
beds 4 D Rs.17251/- and above Semi Private Ward

15
Point 12. Expanding the liberalized emergency scheme and reviewing the ceiling limit for confinement and maternity benefits including revising the flat rates, and also treatment for infertility etc.
Existing provision (Clause 15.5)
The reimbursable amount for outdoor and domicile treatment shall
be restricted to Rs.1500/- and for in patient treatment the reimbursable
amount shall be the actual restricted to Rs.5000/-. However, in deserving
cases, Director, BARC may authorize reimbursement of charges over and
above those indicated above.
Recommendation
It was noticed that the suggestions received from the Units favour
an increase in the ceiling for reimbursement as fixed above. The
Committee, therefore, felt that an upward revision in respect of the
reimbursable charges from the existing rates as indicated below which
were fixed in the year 1998 would be reasonable:-
Existing Proposed Outdoor & Domiciliary Rs.1500/- Rs.3000/-
In-patient Rs.5000/- Rs.15000/-
Confinement charges Rs.750/- Rs.2500/-
Since infertility is not considered as a disease, there is no scope for
bringing the same under the ambit of treatment in the Scheme especially
looking at the prohibitive cost involved for the purpose.

16
Point 13. Reviewing the reciprocal arrangements made with Department of Space and making reciprocal arrangements with other Departments.
Existing provision
No provision exists in this regard in the Scheme but arrangement
for the purpose was made separately.
Recommendation
The Committee felt that the existing reciprocal arrangement as
finalized in the year 1995 with the Department of Space is working well.
However, there is no scope for establishing similar arrangement with
other Departments.
Point 14. Provisions regarding extending the facility to transferees/ deputationists/persons on Foreign Service, etc. to and from the Units.
Existing provision (Clauses 2.1.4 (a) & (b)
(a) Employees of the Department temporarily transferred to other
organizations at Mumbai under the administrative control/
responsibility of the Department and members of their families
residing with them provided they pay contribution to the scheme and
are not beneficiaries of any other Health Scheme. Specific orders
will, however, have to be issued by the Department in each case.
(b) Employees of the Department while on deputation or on foreign
service to Government Departments/Undertakings at Mumbai and
members of their families residing with them provided they pay
contribution and are not beneficiaries of any other health scheme.
An option shall be exercised by the Government Servant concerned

17
for availing of the CHSS facilities. Specific orders will, however,
have to be issued by the Department in each case.
Recommendation
The Committee noted that provisions exist in the Scheme to take
care of the needs of such categories of persons as indicated above and as
such there is no need to add anything further specifically in this regard.
Point 15. Extending the CHSS facility to the persons working at Tarapur but staying in Mumbai and vice-versa.
Existing provision
No specific provision exists in this regard in the Scheme.
Recommendation
Since the employees residing in Mumbai and working at Tarapur
and vice versa are covered under the Scheme based on the place of
residence, there is no need for making any specific provision in this
regard.
Point 16. Provision for Ayurvedic and Homeopathy treatment both for serving and retired employees.
Existing Provision
CHSS is concerned with extending treatment under Allopathic
system only. However, treatment under Indian system of medicines viz.
Ayurvedic and Homeopathy are extended to serving employees and their
dependents under CS (MA) Rules 1944. CS(MA) Rules 1944 is not
applicable to retired employees.
Recommendation
The Scheme does not envisage treatment under Ayurvedic and
Homeopathy systems. Hence, no action seems to be necessary.

18
Point 17. Liberalization of the provisions for eye treatment in the matter of replacement of spectacles, dental treatment/artificial dentures and provision for supply of artificial appliances, hearing aids, etc.
Existing provision (Clauses 8.3, 8.4 and 8.5)
Employees whose pay does not exceed Rs.7000/- p.m. and
members of their families will be eligible for reimbursement for purchase
of spectacles from registered opticians upto Rs.100/- only. Replacements
shall be at the cost of the employee concerned.
Recommendation
Since the existing rate of Rs.100/- for the reimbursement of cost of
spectacles was fixed in the year 1998, it is recommended to raise the
ceiling to Rs.300/-. The Committee also recommends an increase in the
existing ceiling of artificial dentures (by 3 times) as indicated below:
Concessional Rates chargeable for Artificial Dentures supplied under the CHSS of the Department of Atomic Energy
----------------------------------------------------------------------------------------------- Sl.No. Type of dentures Upto Between Between Over Rs.4590/- Rs.4591/- Rs.8001/- Rs.11501/- p.m. to to Rs.8000/- Rs.11500/- ----------------------------------------------------------------------------------------------- Rs. Rs. Rs. Rs. 1. Full dentures 300/- 600/- 900/- 1200/- (artificial set of teeth, upper and lower) 2. Full dentures 150 300 600 900 (artificial set of teeth upper) 3. Partial dentures one 30 60 90 120 tooth 4. Partial dentures 15 30 60 90 additional teeth -----------------------------------------------------------------------------------------------

19
Point 18. Listing out the inadmissible treatments, medicines, preparations, food and other auxiliary items.
Recommendation
The Committee felt that it is neither necessary nor practicable to
identify in an exhaustive manner the inadmissible medicines / treatment,
food and other auxiliary items in a health care scheme like CHSS. Not
only that, wherever doubts arises concerning these issues, the relevant
provisions of CS(MA) Rules could be invoked.
Point 19. Specifying the delegation of powers including payment to referral hospitals.
Recommendation
The Committee noted that adequate powers have been delegated to
the administering authorities or at lower levels in this regard and this
system is working satisfactorily.
Point 20. Deleting provisions relating to discretionary relaxations and making them more specific.
Recommendation
The CHSS being a medi-care system to take care of a large number
of beneficiaries, certain relaxations should be essential in a discretionary
way either in the matter of treatment or implementation of various
provisions as may be necessary so as to make the same flexible. Such
discretions are exercised with due caution by the concerned authorities as
demanded by circumstances and necessity so as to ensure proper care and

20
benefits to the concerned. The Committee, therefore, felt that no change
in the provisions in the Scheme in this regard is necessary.
Point 21. Reviewing the provision for registration of family members on the death of the employee.
Existing Provision
The spouse of a deceased employee and other family members of
the deceased employee registered under the CHS Scheme may continue
to avail of the benefits, provided the deceased employee had completed a
minimum of one year’s service in the Department and the spouse pays the
contribution last paid by the deceased employee and provided further, the
spouse and other members of the family are otherwise eligible for the
continued registration under the scheme. The scale of pay of the post last
held by the employee will be the basis for determining the entitlement.
Recommendation
The Committee noted that the existing provisions are adequate to
take care of the family of a deceased employee. However, it was felt that
the facility of lifelong membership as in the case of retired employees can
be extended to the family as a matter of option.
Point 23. Provision of periodical increase in contribution.
Existing provision (Clause 13.2)
For the medical service provided under the scheme a monthly
contribution shall be recovered. Contribution will be recoverable at the
following rates:
(a) member of AEC and their family Rs.260/-
(b) visiting Scientists / Fellows / Professors Rs.260/- and their family

21
(c) Employees and their family 1% of the basic pay + DP (d) All trainees 1% of stipend/ scholarship/fellowship
Recommendation
The Committee noted that presently contribution towards the
scheme is recovered at the rate of 1% of Pay + DP. The contribution
received is automatically increased on account of the accrual of increment
every year and subsequently on promotion to higher grades.
The Committee noted the income and expenditure under the
scheme for the last six years and carefully perused the Statistics presented
in Annexures VII, VIII, IX and X. It is clear that the annual expenditure
under the scheme is rising rather steeply. The expenditure has doubled in
the last five years, indicating an average 14% annual rate of growth in
expenditure. 92 to 93 percent of the expenditure is borne by the
Government Budget, while the contribution from the employees is only 7
to 8 percent.
The Committee noted that the increased expenditure is because of a
variety of factors, notable amongst them being
- The increasing age – profile of the beneficiaries.
- The ever growing new medical-treatment technologies and
medical diagnostic technologies
- Increased number of referrals.
While the Committee is in favour of continuous improvement in
the Health care facilities provided to employees, a question which
cropped up again and again was “whether the present system of

22
contribution leads to cost-effective health care? or can better systems be
though of ? ”
One thing was quite clear to the Committee “who pays for medical
care”, does influence both the quality of medical care and its cost-
effectiveness. Often a given medical problem can be treated in more than
one way. Choices among these depend not only on how serious the
problem is, but also on “who picks up the bill.” When CHSS
(Government) picks up the bill, the more expensive treatment becomes
more likely, than when the individual pays. Comprehensive health care
coverage – like the CHSS – reduces the price that people pay for routine
health care. The law of demand states that this will increase people’s use
of it.
When patients pay for their own medical treatments, they are more
apt to establish priorities, so that someone with a fractured leg is far more
likely to go to a doctor, than someone with a minor headache. But, when
both are treated free of charge to the patient, these people with minor
ailments may take up as much of doctor’s time and medical resources that
those with more serious medical conditions must be forced to wait. The
Anushakti Nagar dispensaries and the BARC Hospital is a case in point.
The everyday familiar scene is a crowd of retired employees and their
dependants (many with minor ailments), crowding out the more urgent
cases which require greater time of the Doctors.
Yet another issue discussed by the Committee was the issue of
“Moral Hazard” with reference to CHSS, “Moral Hazard” means that if
beneficiaries believe that major expenses are covered under CHSS, they
have less incentive to go in for preventive health. In order to mitigate,
moral hazard, CHSS could make it mandatory for beneficiaries to have

23
annual medical check-ups and perhaps link contribution to the medical
SHAPE of individual employees.
Keeping all the above considerations in mind, the Committee felt
that besides a certain mandatory contribution from all employees, a
mixture of Government payment and private payment by the patient may
mitigate to some extent the “Free Rider Problem” and the “Moral Hazard
Problem” inherent in the operation of scheme like the CHSS.
Beneficiaries can be charged some extra amount in the case of the
employees/families who make frequent visits to the dispensary/hospital.
This would not only reduce the crowd but also curb the tendency of
unnecessarily taking advantage of the facility. The Committee also felt
that a certain percentage of expenditure incurred towards treatment at
referral hospital in respect of dependent relatives/ parents beyond certain
age could be worked out and recovered from the prime beneficiary. The
exact extra amounts and percentage to be paid needs to be worked out.
Once such a system is worked out, and an estimate of the extra
income that will accrue to the CHSS is computed, one can consider
reducing the mandatory contribution from the present rate of 1% to a
suitable figure (say 0.75 percent or so), so that the net kitty of
contribution to CHSS remains at the same level as it exists at present.
After trying this out for a couple of years, one will get data to establish
whether the proposed changes have significantly contributed to increasing
cost-effectivenss of CHSS. Thereafter the question of making further
changes in the contribution can be re-examined.

24
Point 24. Reducing the gap between subscription and expenditure &
Point 25. Checks to avert misuse of the facilities under CHS Scheme.
Recommendation
It was generally seen that under the Scheme in Mumbai, referrals
are being made to various hospitals costing about Rs.20 crores per annum
on an average but at the same time this does not fetch a commensurate
discount. It came to the notice of the Committee that one of the reasons
for the reluctance on the part of the hospitals to allow discount at the
expected level is because of the delay in settling the bills. It also came to
the notice that as per the existing procedure the bills when received from
the concerned hospitals in CHSS office have to essentially move to
various authorities before it finally reaches Accounts for making
payment. The bills are usually sent by hospitals in a consolidated way
for treatment in respect of a set of patients for different ailments and on
receipt, the same are first distributed among the concerned Medical
Officers for certification and thereafter submitted for approval to the
Head, Medical Division or Director, Bio-Medical Group or Director,
BARC according to the value. The bills as approved are then received
back in the BARC Hospital and from there sent to Accounts Division for
scrutiny and payment with the approval of the appropriate authority.
Quite often there is an upward revision in the charges in respect of certain
facilities or services in some of the hospitals and unless the new charges
are approved by the appropriate authority such bills will have to be kept
pending. This apart, duplication or inaccuracy of charges are also
common and these are to be checked and rectified before payment. After
going through the above process sometimes it takes 3 to 9 months before
the cheque is actually released. Since timely payment is the essence of
any such dealings and it is vital to ensure that the bills are promptly

25
settled so as to sustain the demand for appropriate discount from the
hospitals, BARC would be undertaking an in-depth study of the problems
involved in a holistic way and suggest ways and means to cut down the
undue delay in the matter of release of payment. Entering into an MOU
with the hospitals would be one of the measures to avoid unexpected
increase in the charges. Similarly, the Committee felt that the areas
where higher rate of discount would be feasible could be identified while
procuring medicines and other items, by way of directly procuring the
items from the manufacturers consolidating orders for commonly stocked
medicines etc. The Committee observed that although the BARC
Hospital is set up with multi-disciplinary medical facilities, lack of
trained doctors in certain core fields like Cardiology, Nephrology, Gastro,
etc. is a major handicap in affording proper treatment with the result that
the patients are required to be referred to hospitals of specialization. If a
cadre of trained Medical Officers in the essential fields as indicated above
is built up with a scaled-up in-house infrastructure as existing in Army or
Railway Hospitals, outside referrals could be considerably reduced
bringing about a substantial saving in the expenditure. Similarly
outsourcing the services of doctors at the Dispensary level is also one of
the measures for effecting economy in expenditure.
Another reason for the very high expenditure on referrals is the
cost of “defensive medicine” – namely asking a patient to undergo a large
number of unnecessary diagnostic tests only to “rule out such and such
possibility”. This practice has perhaps entered the medical profession in
India from the American practice (where the threat of lawsuits forces
doctors to take up costly ‘malpractice insurance’). To keep some kind of
check on the referral hospitals, BARC Medical Division, should institute
a annual review of “total payments” made to various hospitals every year
and replace one or two hospitals based on some well thought out

26
parameters (from which it can be concluded that a particular hospital was
not relatively speaking cost-effective). Such a practice will hopefully
“send a message” to the hospitals that no hospital can take the “BARC
Account” for granted.
Point 26. Conversion of CHSS as an autonomous body.
Recommendation
It is felt that this is not a practicable proposition.
Point 27. Checks & Balances
It has been noticed that the number of AMAs appointed under the
scheme wherever Department Hospitals/Dispensaries are not available
appears to be on higher side. It is seen from a report submitted by a
Committee that in some cases the average visit of the patients to each
AMAs are very low in general and in certain cases it is as low as two in a
year. The retention of large number of AMAs is not justifiable and
should be drastically pruned in a phased manner. Presently, AMAs are
paid retainer fee @ Rs.400/- p.m (only at Hyderabad). The annual
expenditure incurred on account of fees to these AMAs is around Rs.4.25
lakhs in one of the centres. Once the number of AMAs is reduced, the
expenditure will also stand reduced to that extent.
As per the existing practice in Hyderabad, a beneficiary can
directly approach either an AMA or Zonal Hospital with the CHSS card
without any referral letter from the Medical Officer of the concerned
DAE unit and can avail inpatient facilities from the approved hospital
under the scheme. Further, the beneficiary can also avail medical
treatment for the same disease from different hospitals located in the
27
same locality according to his choice. This is possible because there is no
mechanism to check the treatment being availed from multiple hospitals.
It is necessary to introduce some mechanism which will show the details
of the medical treatment availed by the individual when he approaches
different hospitals for various treatments. It is also noticed that
sometimes more than 3 – 4 zonal hospitals are approved in the same
location. It is possible that the number of approved zonal hospitals in
such localities can be reduced. It is understood that charges towards
supply of medicines from the medical shops of the zonal hospitals and
referral hospitals are at MRP. There is ample scope for availing discount
from the medical shops if negotiations are made with them.
Point 28. Any other points - Exploring the possibility for introduction
of Health Insurance Scheme.
The Committee had an indepth discussion on the possibility of
introducing health insurance scheme in order to ensure long term
sustainability of the current subscription based CHSS and possibility of
its replacement with medical insurance scheme. The suggestions in
regard to introduction of the Insurance Scheme would need a careful
assessment of such schemes and the experience of others to ascertain that
the character and benefits provided under CHSS are not altered. The
aim should be to improve the quality of medical services provided under
CHSS. In fact the scheme should be one of the attractions (perks) to
young scientists/engineers to join the department. While achieving this
aim, there should be innovative checks and balances to curb leakages in
the Scheme, to prevent abuses/misuse of the Scheme and to make the
scheme cost-effective.

28
Hence, the committee recommended that for the time being the
present CHS Scheme should continue with the modifications
recommended.
The Committee also felt that the report should contain its
recommendations on following points:
1. Existing infrastructure facilities in the Departmental Hospitals/ dispensaries.
2. Decentralisation of some of the services at dispensary level. 3. Preventive health care programme. 4. Health Promotion scheme. 5. Health Economics.
The BARC Hospital was constructed and commissioned in the
mid-70’s. The capacity of the Hospital was planned to take care of about
30000 beneficiaries under the Contributory Health Services Scheme. The
number of beneficiaries have increased substantially and at present stands
around 80000. Though some minor expansions had been undertaken
some time back, the infrastructure available is insufficient to take care of
the present load on the system.
With the advances in medical field, a large number of innovative
therapeutic procedure diagnostic techniques, modern drugs and their
delivery systems and advanced monitoring & critical-care equipment
have become available to the doctors in the management of various
diseases. These advancements in the present day concept of holistic
Medicare have permitted the doctors to alter the course of the disease
process, halt its progress or cure the disease, thus improving the quality of
life.

29
The increase in the number of beneficiaries, the rise in the average
age, the development of modern methods, both in diagnosis and treatment
have all resulted in heavy pressure on the present infrastructure.
It is therefore necessary to provide additional facilities to the
existing infrastructure in the form of new technology in the medical field,
latest machinery and equipments, manpower, additional buildings etc in
the XI th Plan in order to keep pace with the changing trend and
methodology in the field of medicine and also to take care of the
increasing load on the long waiting list for appointments for various
Outdoor Patient Departments.
Decentralization : It is necessary to decentralize the health care
arrangements to the maximum extent feasible. It should be possible to
have poly clinic type of arrangement at least in some of the major
dispensaries, say one in western suburbs, another in the central suburbs
and one in the Navi Mumbai area, where the dispensaries should also
have facilities for pathology, dental, X-ray, etc. This will reduce the
number of patients referred to the Hospital at Anushaktinagar for availing
these services. It may also be possible to outsource the service like
pathology, X-ray etc. Once a dental chair is provided in a dispensary it
may be possible to enlist the services of part time private consultants in
dental care.
Health Promotion Scheme : Due to increase in colony population and
lack of understanding in basic public hygiene and sanitation, there
remains a constant threat of an epidemic out break. Maintaining the
hygiene and sanitation of the DAE colonies play very important role in
health promotion scheme sponsored by the Department. Medical
Division extends the logistic and reporting attributes to this agency.
30
Hospital and dispensaries also inform about the notifiable diseases to
BMC and in return receive vaccines and advices. To target and promote
good health it will be wise to promote health education among school
going children and young mothers. It is not an expensive idea to provide
professionally managed gymnasia, yoga centers, health clubs and
swimming pools in the colony which would promote positive health. In
this context statement on morbidity details prepared by Head Medical
Division is very informative and useful. It gives an idea about disease
pattern prevailing in the departmental housing colony in Anushaktinagar.
Health Economics and Auditing : Different health care systems world
over use their resources in many different ways. Some systems are
hospital orientated i.e. highly technology dependent while others give
more emphasis on preventive aspects of the medicine i.e. community
orientated. Auditing makes us aware of the direction of the main focus of
our health expenditure, i.e. whether the major chunk of our budget goes
to cater too few patients suffering from chronic ailments of liver, kidney,
brain or congenital/genetic defects requiring long term medical coverage
or whether the focus is on common seasonal/preventable/lifestyle
diseases like malaria, tuberculosis, gastroenteritis, conjunctivitis, dengue,
chikangunia, diabetes, alcoholism, smoking and hypertension. A periodic
evaluation of the expenditure on both preventive and curative health and
questioning its cost-effectiveness should get institutionalized as one of
the functions of the Medical Division of BARC.
* * *

Annexure-I
UNIT-WISE CHSS REGISTRATIONS AS ON 1st OCTOBER, 2006
Unit Prime Spouses Children Parents Dependents Total
AEES 396 246 438 74 - 1154
AERB 163 118 150 41 - 472
BARC 12063 8942 14057 3473 21 38556
BRIT 426 348 590 135 1 1500
CISF 262 35 42 - - 339
DAE 334 247 437 101 - 1119
DCS&EM 1008 866 1640 316 - 3830
DPS 641 423 795 177 - 2036
HWB 254 193 333 56 - 836
IRE 3 3 4 1 - 11
ISRO 36 25 34 8 - 103
NFC 6 5 7 3 - 21
NPCIL 1884 1454 2251 555 4 6148
RAPS 2 1 1 1 - 5
TIFR 1484 968 1384 443 1 4280
TMC 1557 856 1548 184 - 4145
Total 20519 14730 23711 5568 27 64555
RETIRED POPULATION
Retired 6444 5670 1069 304 - 13487
V. Retired 747 598 214 51 - 1610
Late Employee 1334 - 372 36 - 1742
Total 8525 6268 1655 391 0 16839
Grand Total 29044 20998 25366 5959 27 81394

Annexure-II
CHSS REGISTRATION AS ON
1st OCTOBER, 2006 IN MUMBAI
PRIME 29044
SPOUSES 20998
CHILDREN 25366
PARENTS 5959
DEPENDENTS 27
TOTAL 81394

Annexure-III
CHSS BENEFICIARIES AS ON 01.11.2005 - MUMBAI
Age Group Exployees - Age-wise
00 –– 1177 1188003366 UUppttoo 3355 66667766
1188--2255 1100778888 3366--4455 55776633
2266--3355 1100007744 4466--5555 55006699
3366--4455 1111229933 5566--6600 22776655
4466--5555 99996633
5566--6655 1100332266 Total
6666--7755 66770066
AAbboovvee 7755 33000033 EEmmppllooyyeeeess 2288447766
SSppoouusseess 2200667722
CChhiillddrreenn 2255114455
PPaarreennttss 55887711
DDeeppeennddeennttss 2266

Annexure-IV
CHSS REGISTRATION AS ON 01.12.2005 – MUMBAI
Disp. No. Disp. Name Prime Spouses Children Parents Deps. Total
1 * OYC 597 370 404 54 1 1426
2 * A. Bhavan 795 524 500 186 0 2005
3&5 * Mistry Ngr. 1506 908 1013 366 1 3794
4 •Bandra 649 436 333 115 1 1534
6 Chembur 2069 1442 1361 353 0 5225
7 •Ghatkopar 3270 2183 2594 763 2 8812
8 Deonar (W) 4920 3968 6003 1145 6 16042
9 Deonar (E) 4119 2809 3497 706 8 11139
10 Vashi 3712 2818 2494 607 4 9635
11 Andheri 2554 1779 1683 496 0 6512
12 Mandala 3088 2592 4239 880 3 10802
14 •Dombivili 1275 985 1135 279 0 3674
TOTAL 28554 20814 25256 5950 26 80600
* Dispensaries working in "Single Shift"

Annexure-V
CHSS BENEFICIARIES - 2004-05
Unit No. of Beneficiaries No. of Beneficiares Total
Retired Dependents Serving Dependents
BARC (M) 8023 9853 19696 45304 82876
GSO-K 798 1124 6484 18133 26539
VECCQ 135 232 634 1668 2669
RMP 23 31 778 2188 3020
NFC 320 467 4452 13707 18946
HWP(B) 113 125 522 1353 2113
CAT 44 67 1337 3974 5422
RAPS-K 584 656 4200 13638 19078
TAPS 336 587 3843 10539 15305
HWP (TH) 2 4 244 722 972
HWP (M) 19 54 1919 7381 9373
HWP (TU) 84 105 477 1434 2100
10481 13305 44586 120041 188413
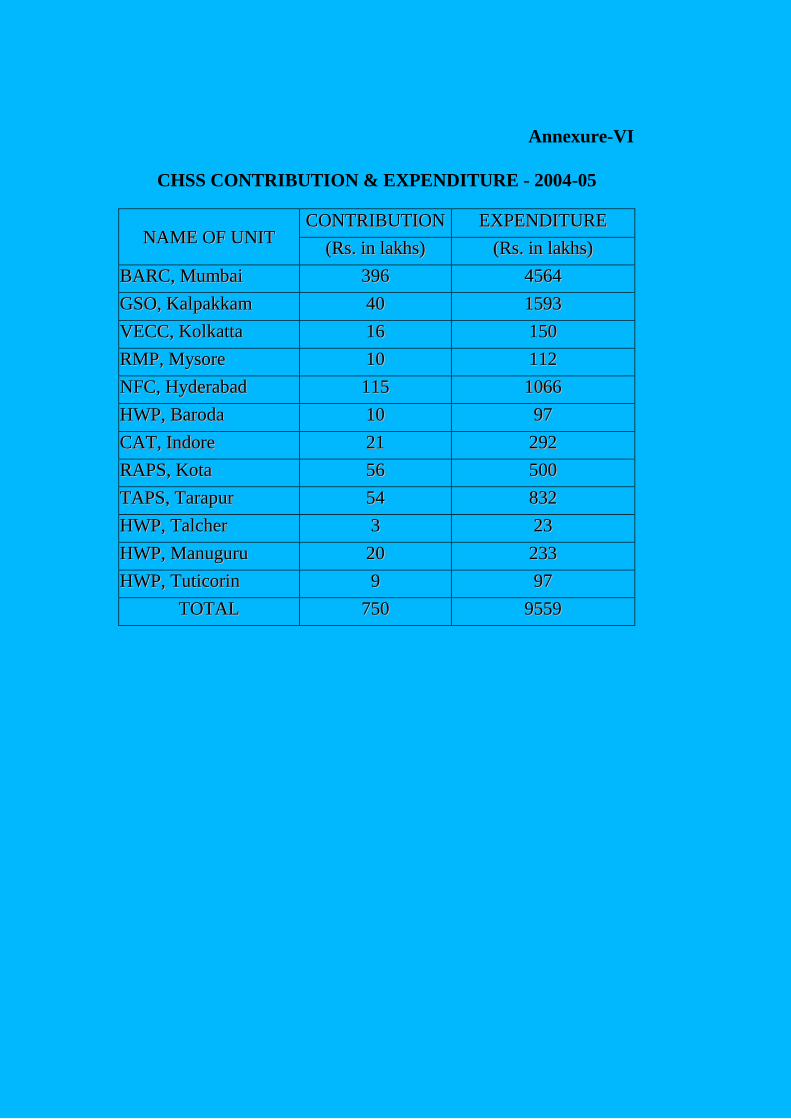
Annexure-VI
CHSS CONTRIBUTION & EXPENDITURE - 2004-05
NNAAMMEE OOFF UUNNIITT CCOONNTTRRIIBBUUTTIIOONN EEXXPPEENNDDIITTUURREE
((RRss.. iinn llaakkhhss)) ((RRss.. iinn llaakkhhss))
BBAARRCC,, MMuummbbaaii 339966 44556644
GGSSOO,, KKaallppaakkkkaamm 4400 11559933
VVEECCCC,, KKoollkkaattttaa 1166 115500
RRMMPP,, MMyyssoorree 1100 111122
NNFFCC,, HHyyddeerraabbaadd 111155 11006666
HHWWPP,, BBaarrooddaa 1100 9977
CCAATT,, IInnddoorree 2211 229922
RRAAPPSS,, KKoottaa 5566 550000
TTAAPPSS,, TTaarraappuurr 5544 883322
HHWWPP,, TTaallcchheerr 33 2233
HHWWPP,, MMaannuugguurruu 2200 223333
HHWWPP,, TTuuttiiccoorriinn 99 9977
TTOOTTAALL 775500 99555599
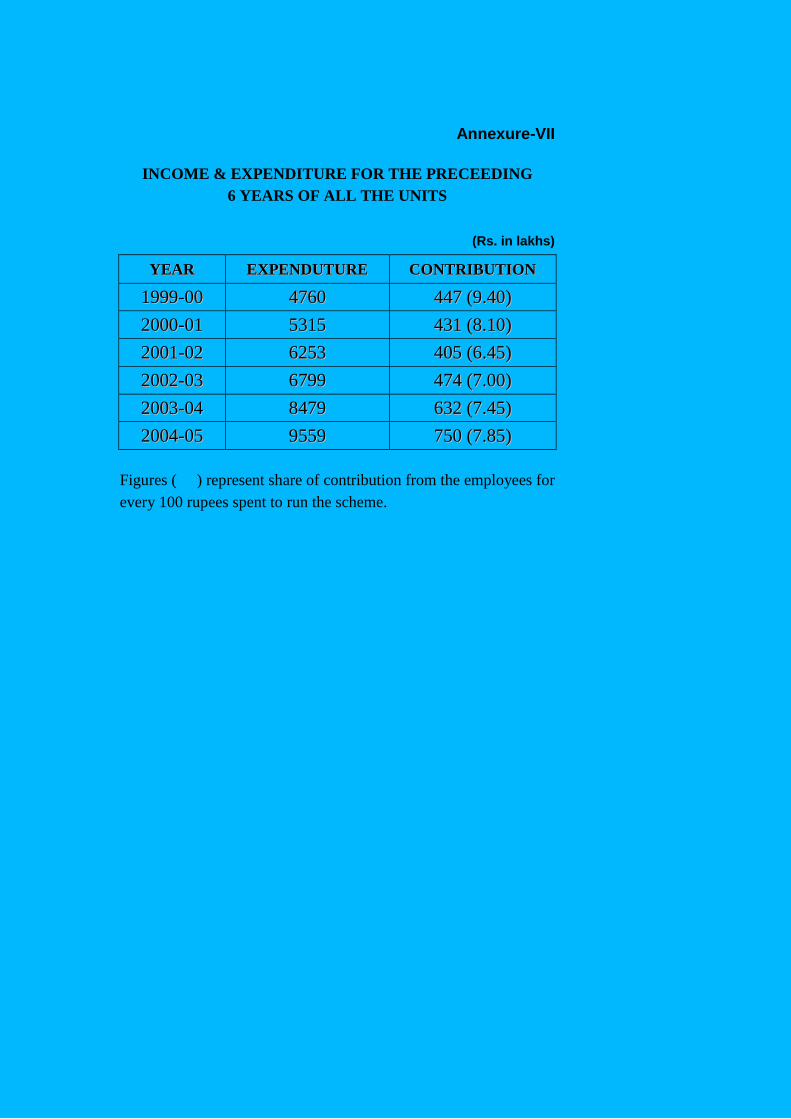
Annexure-VII
INCOME & EXPENDITURE FOR THE PRECEEDING
6 YEARS OF ALL THE UNITS
(Rs. in lakhs)
YYEEAARR EEXXPPEENNDDUUTTUURREE CCOONNTTRRIIBBUUTTIIOONN
11999999--0000 44776600 444477 ((99..4400))
22000000--0011 55331155 443311 ((88..1100))
22000011--0022 66225533 440055 ((66..4455))
22000022--0033 66779999 447744 ((77..0000))
22000033--0044 88447799 663322 ((77..4455))
22000044--0055 99555599 775500 ((77..8855))
Figures ( ) represent share of contribution from the employees for
every 100 rupees spent to run the scheme.
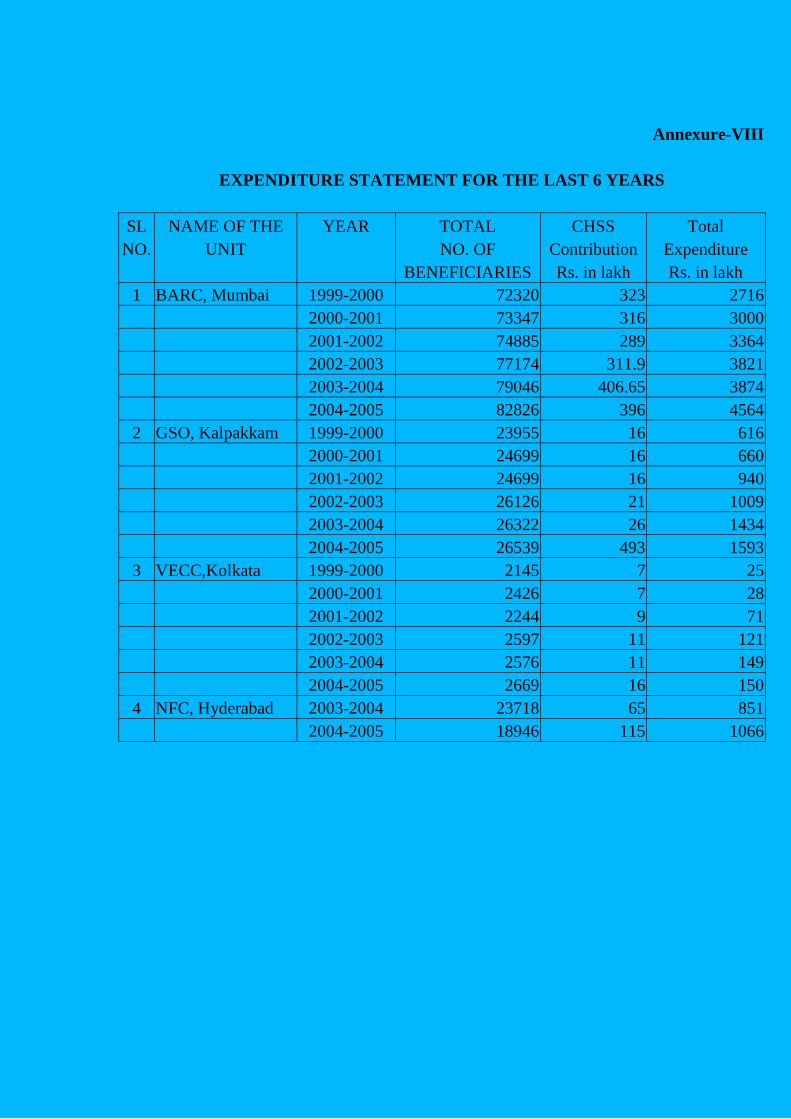
Annexure-VIII
EXPENDITURE STATEMENT FOR THE LAST 6 YEARS
SL NAME OF THE YEAR TOTAL CHSS Total
NO. UNIT NO. OF Contribution Expenditure
BENEFICIARIES Rs. in lakh Rs. in lakh
1 BARC, Mumbai 1999-2000 72320 323 2716
2000-2001 73347 316 3000
2001-2002 74885 289 3364
2002-2003 77174 311.9 3821
2003-2004 79046 406.65 3874
2004-2005 82826 396 4564
2 GSO, Kalpakkam 1999-2000 23955 16 616
2000-2001 24699 16 660
2001-2002 24699 16 940
2002-2003 26126 21 1009
2003-2004 26322 26 1434
2004-2005 26539 493 1593
3 VECC,Kolkata 1999-2000 2145 7 25
2000-2001 2426 7 28
2001-2002 2244 9 71
2002-2003 2597 11 121
2003-2004 2576 11 149
2004-2005 2669 16 150
4 NFC, Hyderabad 2003-2004 23718 65 851
2004-2005 18946 115 1066

Annexure-IX
Statement showing year-wise cases referred
to panel Hospital and Expenditure thereon (CHSS Mumbai)
(Rs. in lakhs)
Year No. of cases Total
2002-03 6226 1082.19
2003-04 6304 1331.81
2004-05 9426 1946.81 @
2005-06 10410 2176.20 @
@ Steep increase due to upward revision of rates by Panel Hospitals
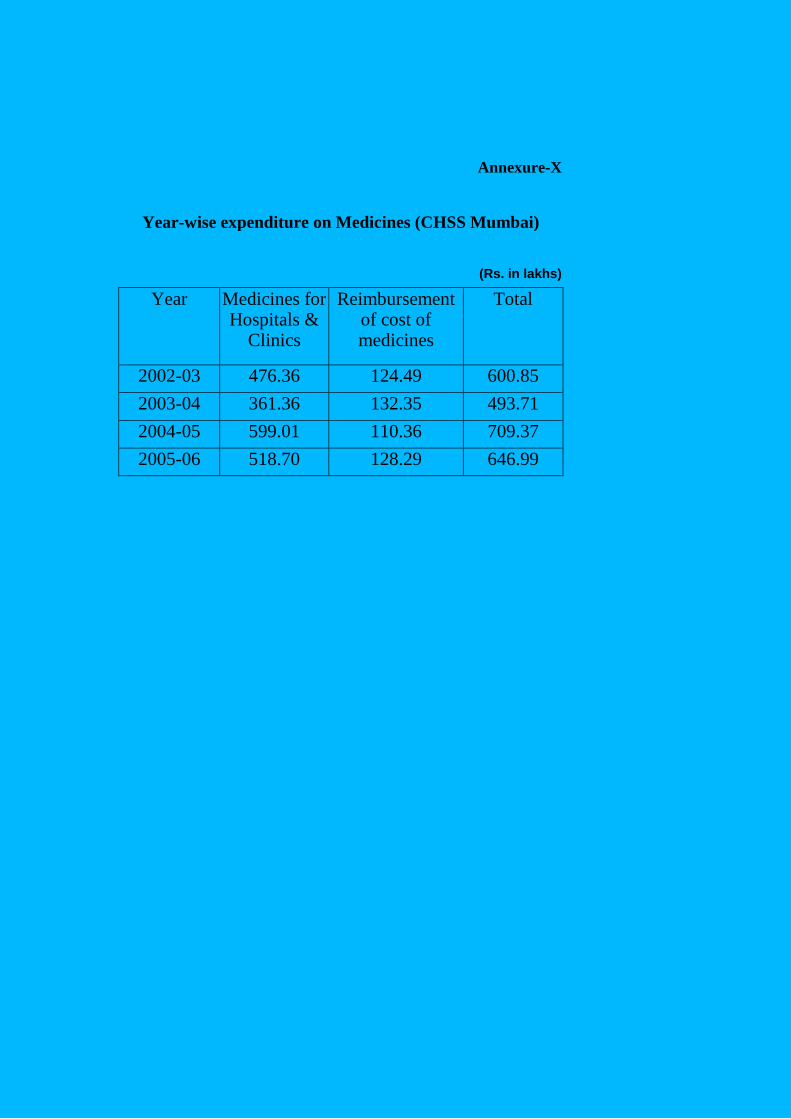
Annexure-X
Year-wise expenditure on Medicines (CHSS Mumbai)
(Rs. in lakhs)
Year Medicines for Hospitals &
Clinics
Reimbursement of cost of medicines
Total
2002-03 476.36 124.49 600.85
2003-04 361.36 132.35 493.71
2004-05 599.01 110.36 709.37
2005-06 518.70 128.29 646.99
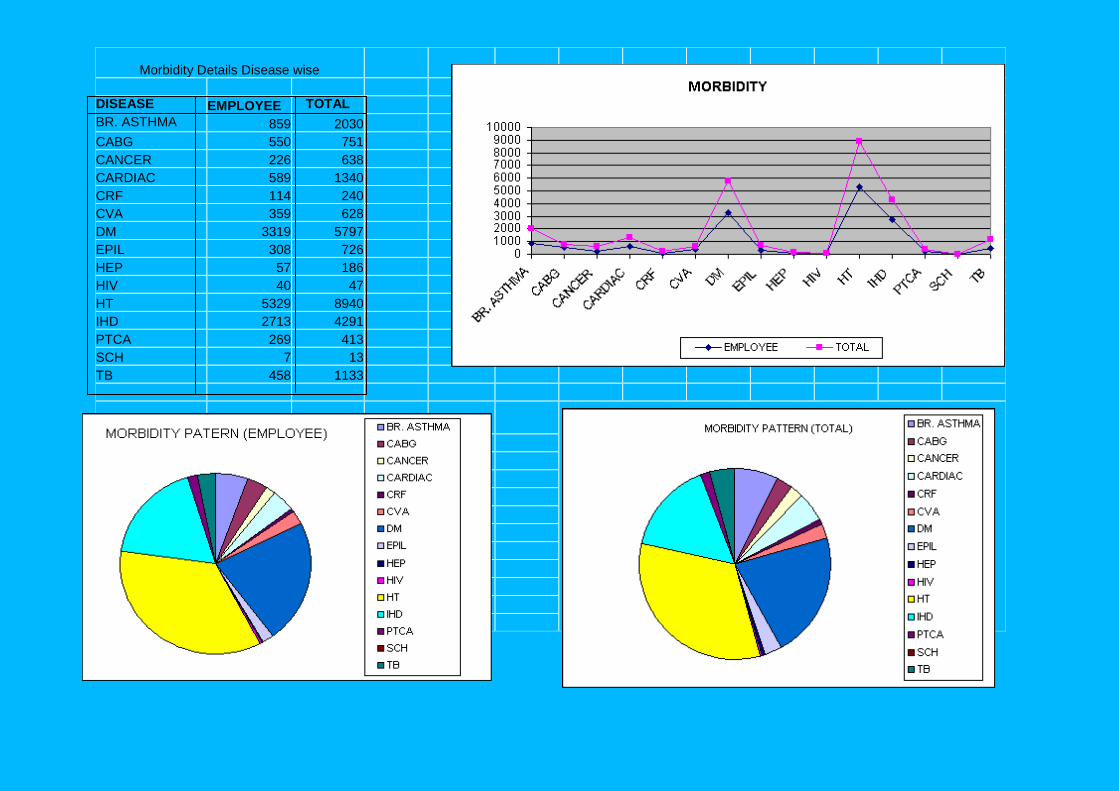
Morbidity Details Disease wise
DISEASE EMPLOYEE TOTAL
BR. ASTHMA 859 2030
CABG 550 751
CANCER 226 638
CARDIAC 589 1340
CRF 114 240
CVA 359 628
DM 3319 5797
EPIL 308 726
HEP 57 186
HIV 40 47
HT 5329 8940
IHD 2713 4291
PTCA 269 413
SCH 7 13
TB 458 1133