chronic shoulder disorders - wikispacesshoulder+disorders.pdfchronic shoulder disorders. contents....
TRANSCRIPT

Dr. Mustafa ElsingergyConsultant orthopedic surgeon Dallah Hospita
Prof. Mamoun KremliAlmaarefa Medical College
Chronic Shoulder Disorders

Contents

Shoulder Pain• INTRINSIC
• Due to causes in the shoulder region
• EXTRINSIC
• Due to referred pain from outside the shoulder

Shoulder Pain• INTRINSIC
• Due to causes in the shoulder region

Shoulder Pain• EXTRINSIC
• Due to referred pain from outside the shoulder

Shoulder Disorders• Due to causes related to :
1. Rotator cuff2. Shoulder capsule3. Glenohumeral joint4. Scapular problems 5. Acromioclavicular joint

Rotator Cuff - Anatomy• Originate from the scapula
• Insert in the Greater Lesser tuberosities
• Pass under coraco-acromial arch
• Separate from the ligament by bursa
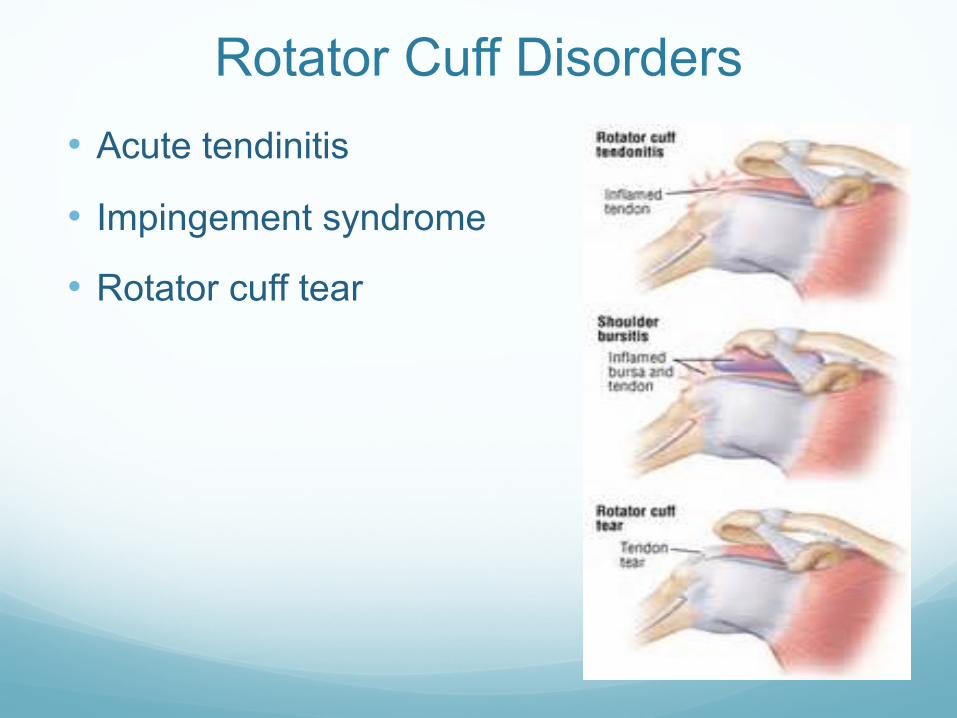
Rotator Cuff Disorders• Acute tendinitis
• Impingement syndrome
• Rotator cuff tear

R.C.D - Acute TendinitisClinical features:• Pain / Tenderness / Painful abduction range
X-ray:• Normal
• Area of calcification
Treatment:• Rest
• NSAID
• Local injection

R.C.D - Impingement SyndromeCausesClinical features• Pain
• Shoulder looks normal or wasted
• Tenderness
• Disturbed glenohumeral rhythm
• Painful abduction ( 6oo TO 120o )
• Neer’s test (+VE)
• Hawkin’s test (+ve)

R.C.D - Impingement SyndromeX-ray:• Calcification
• Degenerated AC jt.
MRI:• Bursitis
• Thickening of the tendon
Treatment:• Mild: NSAID, local injection
• Severe: arthroscopy vs acrmoioplasty

R.C.D - Impingement SyndromePredisposing factors
• Degeneration: middle age
• Chronic irritation by osteophyte
• Underlying disease:• eg. Rheumatoid
• Precipitating factor: trauma
Types:
• Incomplete
• Complete

R.C.D - Impingement SyndromeClinical features:
• Trauma, pain, limited abduction
• After few weeks:• Incomplete tear: improvement of pain and rom• Complete tear: improvement of pain and decrease of active range
Look:
• Early; normal appearance
• Late; wasting of supraspinatus and infraspinatus muscles
Feel:
• Tender greater tuberosity

R.C.D - Rotator Cuff TearClinical features:
• Move:• Incomplete tear; painful weak• Complete; passive not painful, active
drop arm sign
X-rays:
• Early normal
• Late degenerative changes
MRI: image of choice
Treatment:
• Incomplete tear: PT, NSAID
• Complete tear: surgery
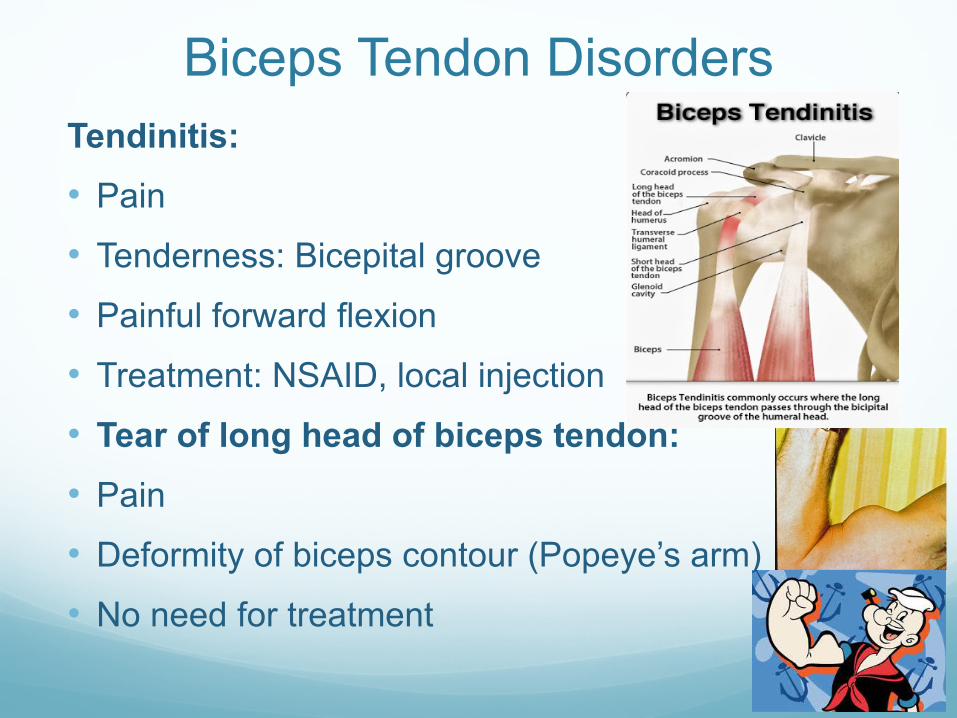
Biceps Tendon DisordersTendinitis:• Pain
• Tenderness: Bicepital groove
• Painful forward flexion
• Treatment: NSAID, local injection
• Tear of long head of biceps tendon:• Pain
• Deformity of biceps contour (Popeye’s arm)
• No need for treatment

Adhesive Capsulitis (Frozen Shoulder)• Unknown pathogenesis leads to pain and limitation of
movement
• Trauma or RCD may be causes
Clinical features:
• Pain
• Limitation of movement in all directions of GH range
Natural history:
• Pain and limitation of movement gradually increase then gradually decrease, takes 18 months
Treatment:
• Conservative vs arthroscopy

Recurrent Shoulder InstabilityTypes:
• Recurrent anterior dislocation (RAD)
• Recurrent posterior subluxation (rare)
• Multidirectional instability (MDI)
Type RAD MDI
Cause Traumatic Atraumatic
Clinical feature Apprehension test +ve Sulcus sign positive
Treatment Surgical PT

Recurrent Shoulder InstabilityMultidirectional instability:
• Generalized ligamentous laxity
• Sulcus sign (+ve)

Recurrent Shoulder InstabilityRecurrent anterior dislocation (RAD)
• Most common
• H/O acute dislocation
• Apprehension test (+ve)
Image:
• Hill Sach’s lesion
• Bankart’s lesion

Recurrent Shoulder Instability• Recurrent anterior dislocation (RAD)
• Multidirectional instability (MDI)
Type RAD MDICause Traumatic AtraumaticClinical feature Apprehension test +ve Sulcus sign positiveTreatment Surgery PT

Gleno-humeral Joint Disorder• Osteoarthritis
• Rheumatoid
• TB
• Milwaukee

Gleno-humeral Osteoarthritis• Usually follows other pathology
• eg. Trauma, rheumatoid artheritis or rc tears
Clinical features:
• Painful movement
• Wasting the shoulder muscle
• Tender joint line, Limited ROM
X-ray:
• Loss of joint space
• Subchondral sclerosis
Treatment: Conservative / Replacement

Gleno-humeral Rheumatoid ArthritisClinical features:
• Generalized arthritis affecting other joints
• Pain and limitation of movement
• Painful passive movement and limited active movement
Lab investigation:
• +ve rheumatoid factor
X-ray:
• Loss of articular space
• Peri-articular erosion

Acromioclavicular Disorders• Instability
• Arthritis

Scapular DisordersSprengel’s shoulder:
• Congenital
Winging of scapula:
• Weak serratus ant muscle

Shoulder Summary• Shoulder Symptoms:
• Pain• Stiffness• Instability• Deformity• Loss of Function
• Shoulder Examination• Look• Feel• Move• Special Tests
• Investigations• Lab• X-ray• MRI
• Treatment• Conservative• Surgical