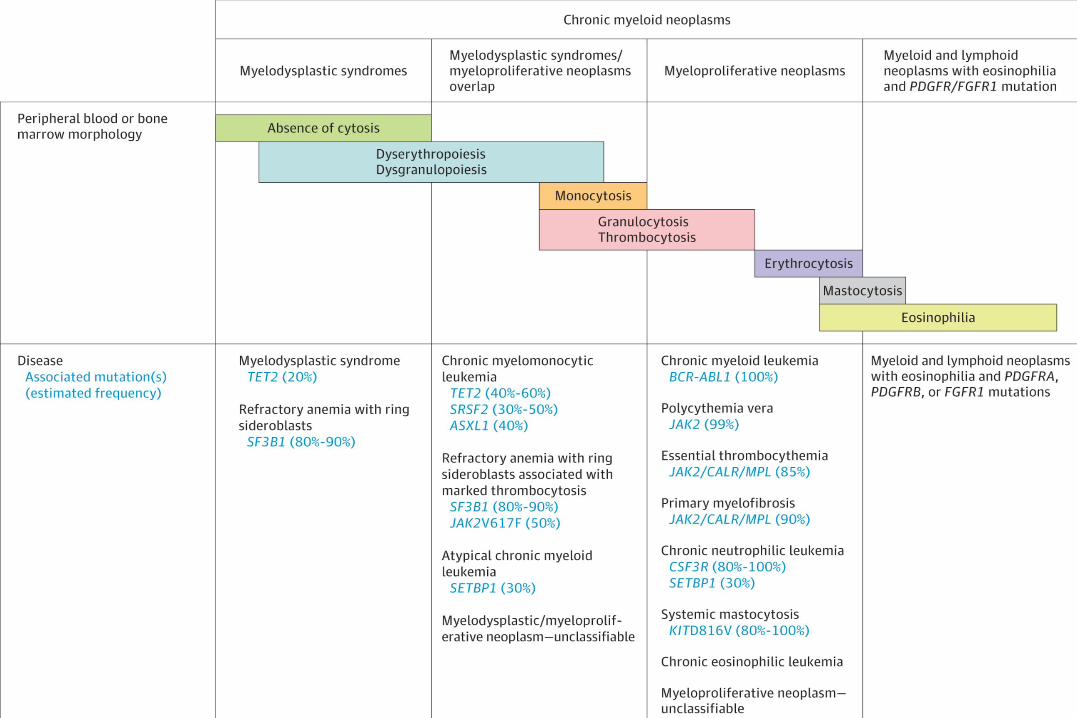
chronic myeloproliferative neoplasms · spurious polycythemia ... myelodysplastic syndromes; pmf,...
TRANSCRIPT

1
CHRONIC MYELOPROLIFERATIVE
NEOPLASMS
M. Kazmierczak 2016


4
CHRONIC MYELOPROLIFERATIVE
NEOPLASMS (MPN)
MPN are clonal diseases originating in pluripotential
haematopoietic stem cell. The clonal expansion results in
increased and abnormal haematopoiesis and produces a group of
interrelated syndromes, classified according to the predominant
phenotypic expression of the myeloproliferative clone.

5
ERYTHROCYTOSIS (Classification)
(1)
I. Relative erythrocytosis (pseudopolycythemia):
1. Hemoconcentration
2. Spurious polycythemia (Gaisboek syndrome)
II. Absolute erythrocytosis (Polycythemia):
A. Primery erythrocytosis
1. Polycythemia vera
2. Familial erythrocytosis
B. Secondary erythrocytosis (abnormal increase of serum erythropoietin level)

6
ERYTHROCYTOSIS (Classification)
(2)
1. Erythrocytosis secondary to decreased tissue oxygenation:
a) chronic lung diseases
b) cyanotic congenital heart diseases
c) high-altitude erythrocytosis (Monge disease)
d) hypoventilation syndromes (Sleep apnoe)
e) hemoglobin-oxygen dissociation abnormalities
- hemoglobinopathies associated with high oxygen affinity
- carboxyhemoglobin in „smoker’s polycythemia”
2. Secondary to aberrant erythropoietin production or response:
a) Erythropoietin-producting tumors: hepatoma, uterine leiomyoma,
cerebellar hemangioblastoma, ovarian carcinoma, pheochromocytoma
b) Renal diseases: renal cell carcinoma, kidney cysts and
hydronephrosis, renal transplantation.
c) Androgen abuse: adrenal cortical hypersecretion, exogenous androgens
7
POLYCYTHEMIA VERA (PV)
Patogenesis
PV is a clonal disorder involving the hematopoietic stem cells; it leads to an
autonomous proliferation of the erythroid, myeloid, and megakaryocytic cell
lines. Increased erythroid proliferation is usually more prominent than that of the
other cell lines and occurs independently of erythropoietin levels (which are
usually very low in PV)
Epidemiology
The incidence rate of PV is approximately 2 per 100.000 population.
PV is slightly more prevalent in males with male/female ratio ranging from 1,2
to 2:1. Median age at diagnosis was 60 years in men and 62 years in women.
8
POLYCYTHEMIA VERA
symptoms
1. Erythrocytosis and hyperviscosity, leading to impaired oxygen delivery:
• Poor CNS circulation: headaches, dizziness, vertigo, tinnitus and visual disturbances
• Poor coronary circulation: angina pectoris
• Peripheral circulation intermittent claudication
2. Venous thrombosis or thromboembolism
3. Hemorrhage: epistaxis, gingival bleeding, ecchymoses, gastrointestinal bleeding
4. Abdominal pain secondary to peptic ulcer
5. Early satiety due to splenomegaly
6. Pruritus is secondary to increased histamine release from the basophils and mast cells

9
POLYCYTHEMIA VERA
physical examination
1. Splenomegaly – is present in 75% of patients at the time of
diagnosis.
2. Hepatomegaly - is present in approximately 30% of patients at
the time of diagnosis.
3. Hypertension
4. On examination of the eye grounds, the vessels may be
engorged, tortuous, and irregular in diameter; the veins may be dark purple.( fundus policythaemicus)
• Facial plethora
10
ESSENTIAL THROMBOCYTHEMIA
(ET)
ET is a clonal myeloproliferative neoplasms
characterized by bone marrow hyperplasia
with excessive proliferation of megakaryocytes
and sustained elevation of the platelet count.
11
ESSENTIAL THROMBOCYTHEMIA
clinical picture1. Thrombotic complications (intermittent or permanent
occlusion of small blood vessels)
• transient cerebral and ocular ischemic episodes that may
progress to infarction
• peripheral arterial occlusive disease associated with
„erythromelalgia”(intermittent, painful errythema and
cyanosis of the fingers and toes
2. Hemorrhagic complications
bleeding after surgery and spontaneus upper gastrointestinal bleeding (the
hemorrhagic tendency is worsened if nonsteroidal anti-inflammatory
agent are administered)
3. Splenomegaly - 20-50% patients
4. Hepatomegaly - rarely

MPN symptoms by subtype
Geyer HL, et al. Hematology 2014;277
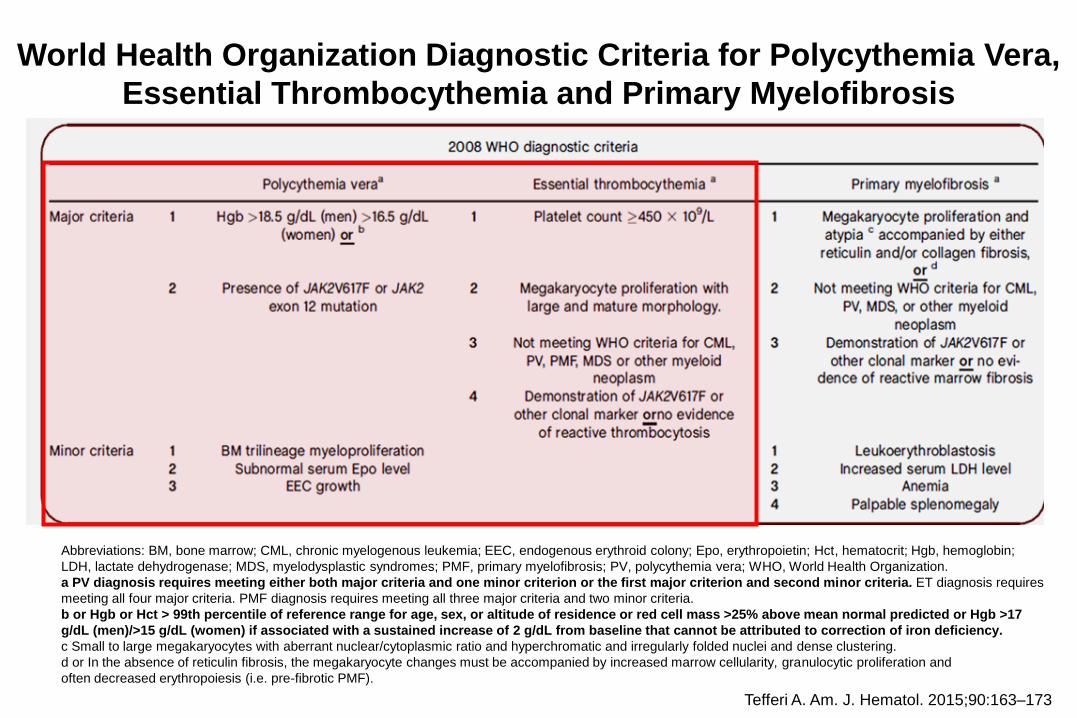
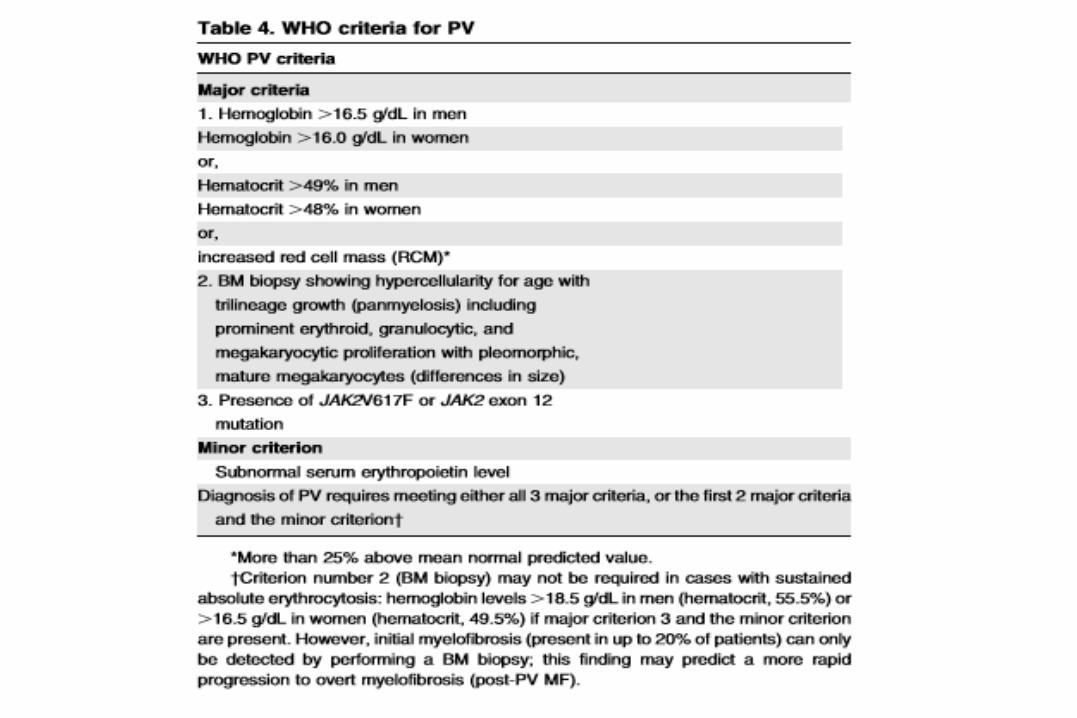
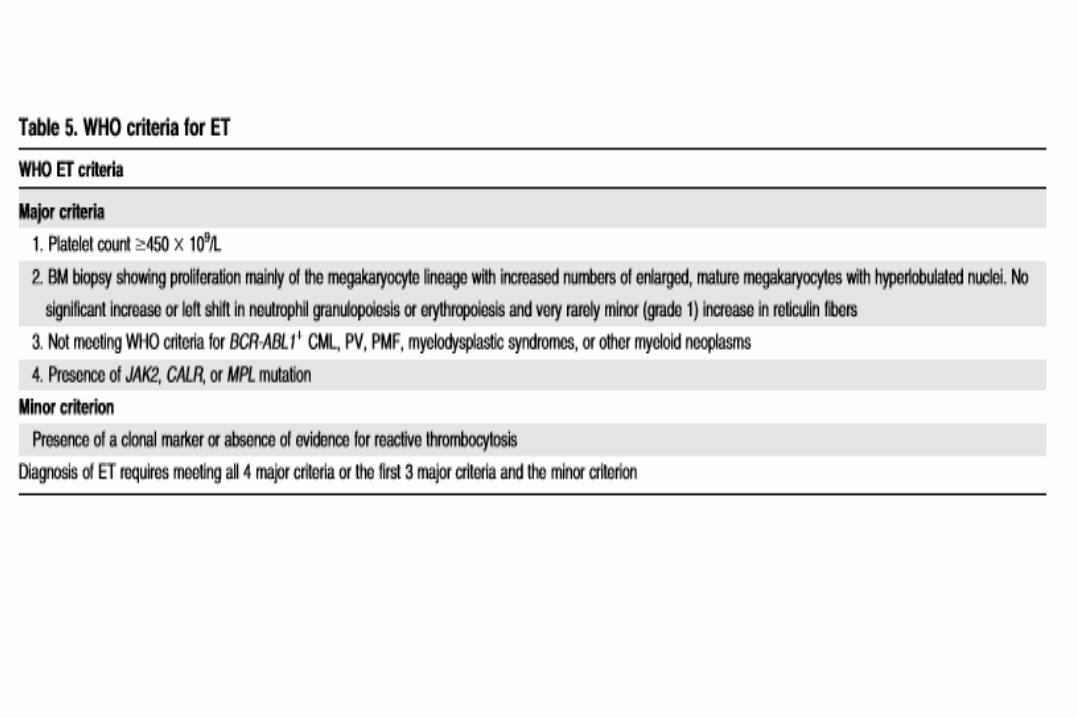
World Health Organization Diagnostic Criteria for Polycythemia Vera,
Essential Thrombocythemia and Primary Myelofibrosis
Abbreviations: BM, bone marrow; CML, chronic myelogenous leukemia; EEC, endogenous erythroid colony; Epo, erythropoietin; Hct, hematocrit; Hgb, hemoglobin;
LDH, lactate dehydrogenase; MDS, myelodysplastic syndromes; PMF, primary myelofibrosis; PV, polycythemia vera; WHO, World Health Organization.
a PV diagnosis requires meeting either both major criteria and one minor criterion or the first major criterion and second minor criteria. ET diagnosis requires
meeting all four major criteria. PMF diagnosis requires meeting all three major criteria and two minor criteria.
b or Hgb or Hct > 99th percentile of reference range for age, sex, or altitude of residence or red cell mass >25% above mean normal predicted or Hgb >17
g/dL (men)/>15 g/dL (women) if associated with a sustained increase of 2 g/dL from baseline that cannot be attributed to correction of iron deficiency.
c Small to large megakaryocytes with aberrant nuclear/cytoplasmic ratio and hyperchromatic and irregularly folded nuclei and dense clustering.
d or In the absence of reticulin fibrosis, the megakaryocyte changes must be accompanied by increased marrow cellularity, granulocytic proliferation and
often decreased erythropoiesis (i.e. pre-fibrotic PMF).
Tefferi A. Am. J. Hematol. 2015;90:163–173
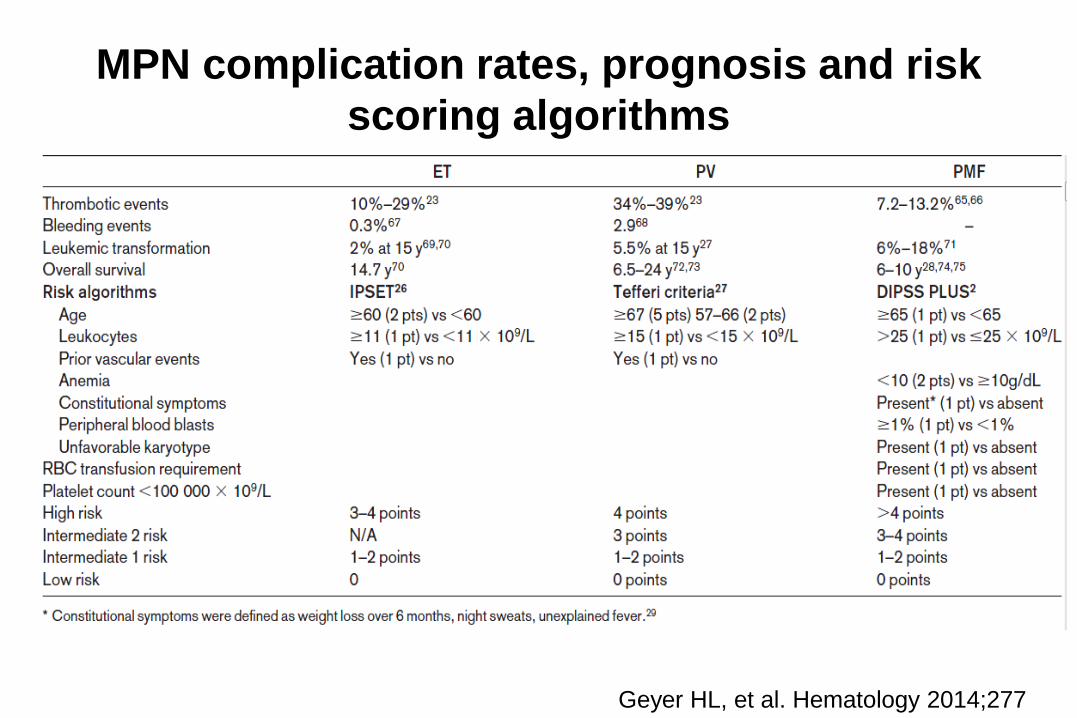
MPN complication rates, prognosis and risk
scoring algorithms
Geyer HL, et al. Hematology 2014;277
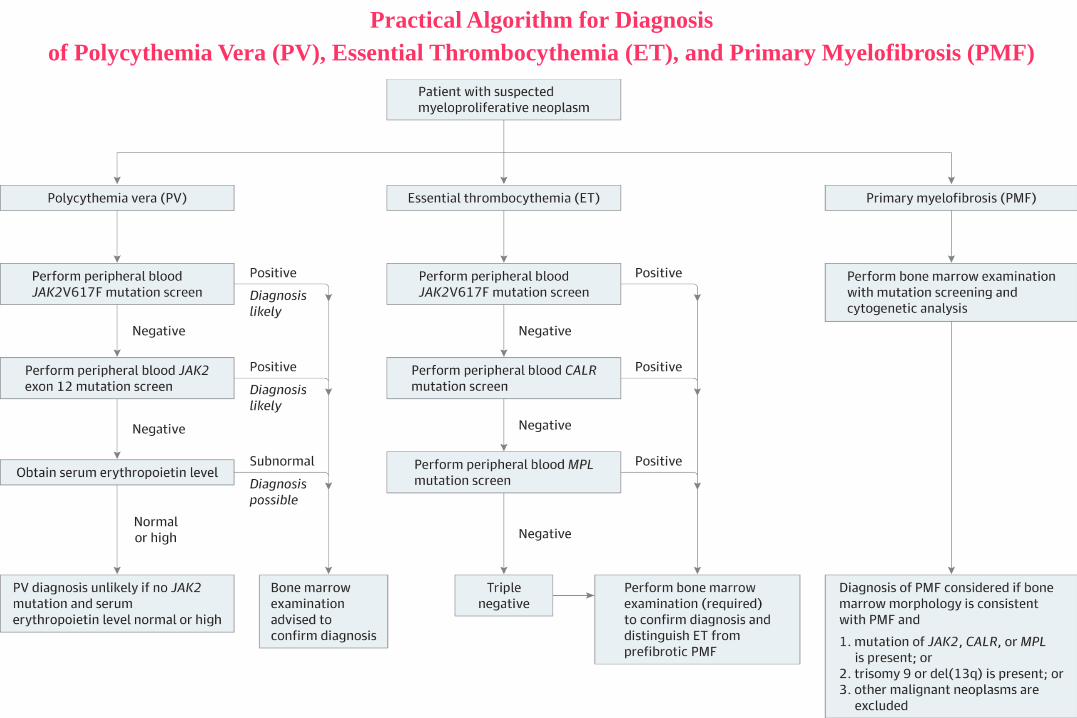
Practical Algorithm for Diagnosis
of Polycythemia Vera (PV), Essential Thrombocythemia (ET), and Primary Myelofibrosis (PMF)
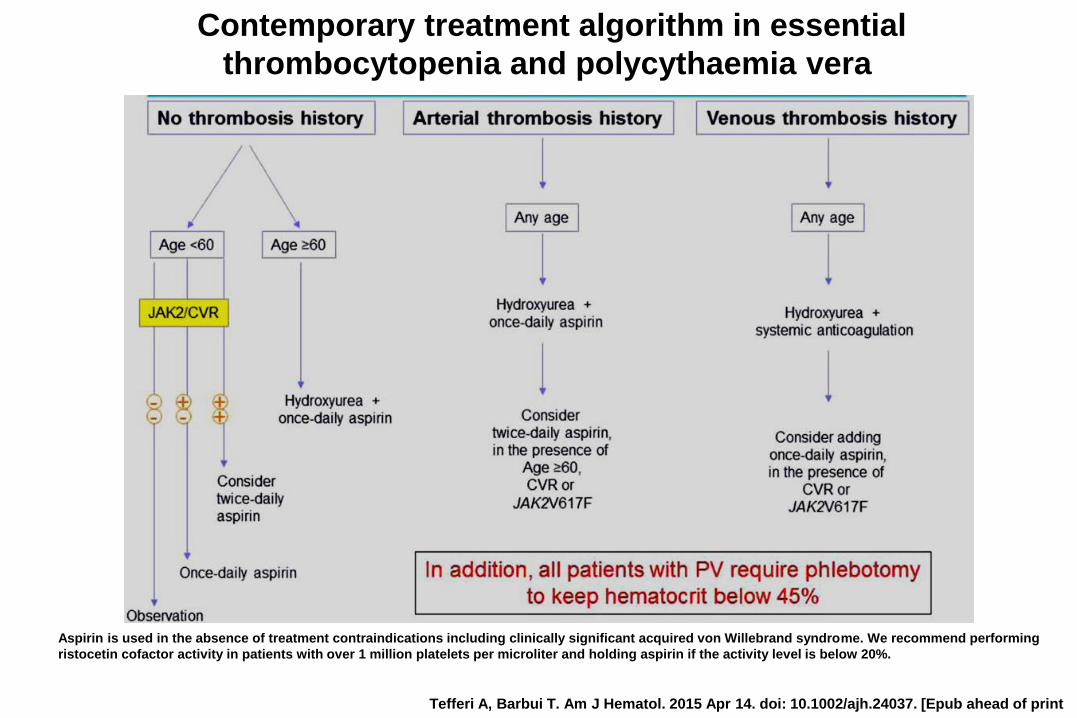
Tefferi A, Barbui T. Am J Hematol. 2015 Apr 14. doi: 10.1002/ajh.24037. [Epub ahead of print
Aspirin is used in the absence of treatment contraindications including clinically significant acquired von Willebrand syndrome. We recommend performing
ristocetin cofactor activity in patients with over 1 million platelets per microliter and holding aspirin if the activity level is below 20%.
Contemporary treatment algorithm in essential
thrombocytopenia and polycythaemia vera

17
POLYCYTHEMIA VERA
Phlebotomy
- initially 450-500 ml phlebotomy every other day until the
hematocrit is less than 45% (M), 42% (F)
- older patients or these with underlying cardiovascular disase should
undergo smaller phlebotomies 200-300mL twice weekly or
100-150mL every day until Ht<45%
- fluid replacement so that the patients remains isovolemic

POLYCYTHEMIA VERA - supportive care
Severe itching (pruritus) — antihistamines, H2-receptor blockers, serotonin
reuptake inhibitors, interferon alpha, and in resistant cases, myelosuppression.
Hyperuricemia — allopurinol 300mg/day
Erythromelalgia (a burning pain in the feet or hands accompanied by erythema,
pallor or cyanosis) — low-dose aspirin (Grade 1C). Erythromelalgia
unresponsive to treatment with low-dose aspirin should be treated with
myelosuppression.
Bleeding — Extraneous causes for bleeding (eg, use of high-dose aspirin,
antiplatelet agents, anticoagulants) should be stopped. Patients should be
evaluated for acquired von Willebrand disease and treated accordingly.
20
Myelofibrosis=agnogenic myeloid metaplasia(primary myelofibrosis, osteomyelofibrosis, idiopathic myelofibrosis,
myelofibrosis with myeloid metaplasia )
Myelofibrosis is a chronic myeloproliferative neoplasms with
clonal hematopoesis and secondary(non-clonal) hyperproliferation
of fibroblasts (stimulated by PDGF, EGF, TGF- released from
myeloid cells, mainly from neoplastic megakaryocytes) with
increased collagen synthesis. It produces bone marrow fibrosis and
to extramedullary hematopoesis in the spleen or in multiple organs.
21
MYELOFIBROSIS
• The incidence of Myelofibrosis is about 0,5/100.000. The median
age at diagnosis was approximately 65 years.
• Common complaints: fatigue, weight loss, night sweats, bone pain,
abdominal pain, fever
• Physical findings: splenomegaly (often huge), hepatomegaly (in
about 50% of patients), symptoms of anaemia and
thrombocytopenia

22
MYELOFIBROSIS
- laboratory findings (1)
• Anemia - Hb<10g/dL in 60% of patients
• Leukocytosis with counts generally below 50G/L (in about 50%), leukopenia
(in about 25% at the time of diagnosis)
• thrombocytosis in 50% at the time of diagnosis, with disease progression
thrombocytopenia becomes common
• eosinophilia and basophilia may be present
• retikulocytosis
• LAP score is usually elevaatedd
• Increased level of lactate dehydrogenase
• uric acid level is increased in most patients
23
MYELOFIBROSIS
- laboratory findings(2)• Peripheral blood smear: anisocytosis and poikilocytosis with the
presence of teardrop-shaped and nucleated red cells, immature
neutrophils but myeloblasts not always
• Aspiration of bone marrow is usually ansuccessful (dry tap).
Smears from successful aspirates usually show neutrophilic and
megakaryocytic hyperplasia
• Trephine biopsy often shows a hypercellular marrow with increased
reticulin fibers and variable collagen deposition . Increased numbers of
megakaryocytes are frequently seen.

Practical Algorithm for Diagnosis
of Polycythemia Vera (PV), Essential Thrombocythemia (ET), and Primary Myelofibrosis (PMF)

World Health Organization Diagnostic Criteria for Polycythemia Vera,
Essential Thrombocythemia and Primary Myelofibrosis
Abbreviations: BM, bone marrow; CML, chronic myelogenous leukemia; EEC, endogenous erythroid colony; Epo, erythropoietin; Hct, hematocrit; Hgb, hemoglobin;
LDH, lactate dehydrogenase; MDS, myelodysplastic syndromes; PMF, primary myelofibrosis; PV, polycythemia vera; WHO, World Health Organization.
a PV diagnosis requires meeting either both major criteria and one minor criterion or the first major criterion and second minor criteria. ET diagnosis requires
meeting all four major criteria. PMF diagnosis requires meeting all three major criteria and two minor criteria.
b or Hgb or Hct > 99th percentile of reference range for age, sex, or altitude of residence or red cell mass >25% above mean normal predicted or Hgb >17
g/dL (men)/>15 g/dL (women) if associated with a sustained increase of 2 g/dL from baseline that cannot be attributed to correction of iron deficiency.
c Small to large megakaryocytes with aberrant nuclear/cytoplasmic ratio and hyperchromatic and irregularly folded nuclei and dense clustering.
d or In the absence of reticulin fibrosis, the megakaryocyte changes must be accompanied by increased marrow cellularity, granulocytic proliferation and
often decreased erythropoiesis (i.e. pre-fibrotic PMF).
Tefferi A. Am. J. Hematol. 2015;90:163–173

MPN complication rates, prognosis and risk
scoring algorithms
Geyer HL, et al. Hematology 2014;277
27
Dynamic IPSS :
· Age >65 years: 1 point
· Leukocyte count >25,000/microL: 1 point
· Hemoglobin <10 g/dL: 2 points
· Circulating blast cells ≥1 percent: 1 point
· Presence of constitutional symptoms: 1 point
Subjects with zero, one to two, three to four, or 5 to 6 points were considered low,
intermediate-1, intermediate-2, or high risk, respectively.
DIPSS Plus — IPSS-independent prognostic factors for survival in PMF have been
identified, such as unfavorable karyotype (complex karyotype or sole or two abnormalities
that include +8, -7/7q-, i(17q), -5/5q-, 12p-, inv(3), or 11q23 rearrangements),
red cell transfusion need, and thrombocytopenia
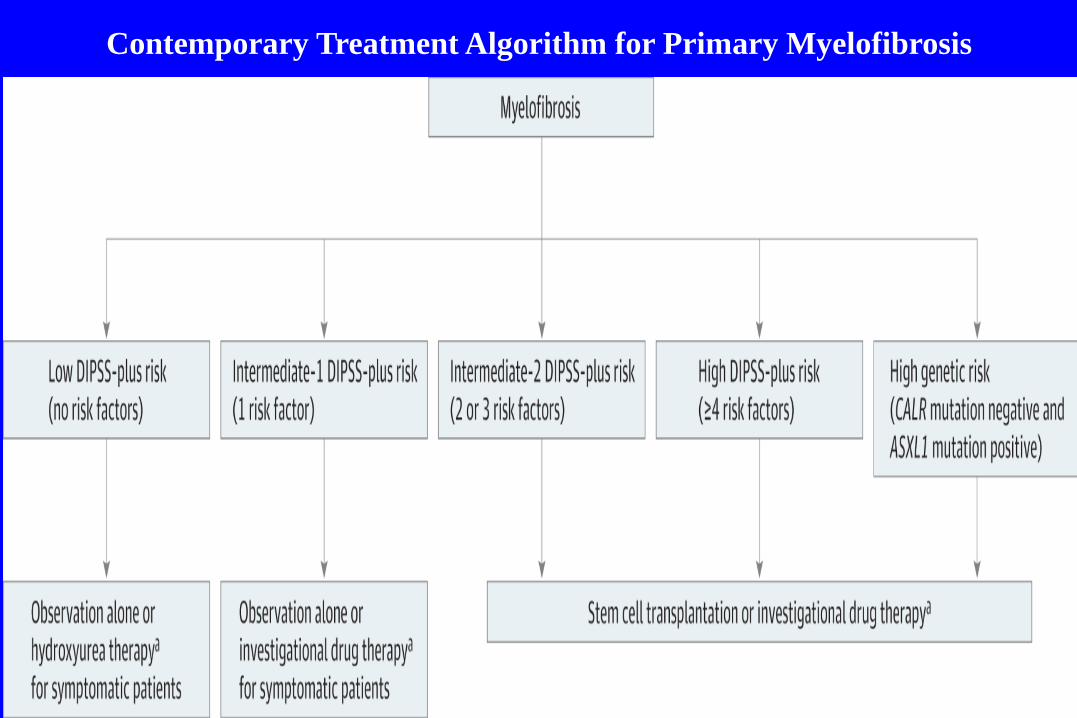
Contemporary Treatment Algorithm for Primary Myelofibrosis

MYELOFIBROSIS - therapy (1)
Drug used for the control of leukocytosis, thrombocytosis:
hydroxyurea
Drugs used for treatment of splenomegaly and constitutional symptoms:
hydroxyurea, ruxolitinib.
Drugs used for treatment of anemia include:
androgen preparations, prednisone, danazol, thalidomide, lenalidomide (in the
presence of del(5q).

30
MYELOFIBROSIS - therapy (2)
Splenectomy should be considered for: portal hypertension, painful
splenomegaly, refractory anemia and thrombocytopenia, or
exccessive transfusion requirement. However,the procedere is
hazardous (an operative mortality is up to 10%).
Splenic irradiation: when there is a contrindication to splenectomy
Allogeneic stem-cell transplantation: for young patients who have a
poor prognosis and have a suitable donor identified.
Supportive care: Allopurinol-to prevent hyperuricaemia.
Transfusions of packed red cells for anemia or platelets for
thrombocytopenia with bleeding
MYELOFIBROSIS - therapy (3)
Clinical trials:
- potentially disease-modifying agents such as inhibitors of mutated isocitrate
dehydrogenase protein and telomerase,
- immune conjugates directed at leukemic stem cells,
- another Janus kinase (JAK) inhibitor (momelotinib) - currently in a phase-3 study, in
improving anemia, in addition to its demonstrated efficacy in controlling splenomegaly and constitutional
symptoms.