chronic inflammtion
TRANSCRIPT

Tehseen Anwar 03450743978 13-Arid-1112 Pir Mehr Ali Shah Arid Agriculture University
By
Chronic Inflammation
INFLAMMATION
Inflammation is part of the complex biological response of vascular tissues to harmful stimuli, such as pathogens damaged cells, or irritants.
CARDINAL SIGNS OF INFLAMMATION
There are five cardinal signs:
1. Calor 2. Rubor 3. Dolar4. Tumor 5. Funcito leasa
Major types of inflammation on basis of duration are:
1. ACUTE
2. CHRONIC
Acute inflammation is rapid in onset and of short duration, lasting from a few minutes to as long as a few days, and is characterized by fluid and plasma protein exudation and a predominantly neutrophilic leukocyte accumulation.
Chronic inflammationmay be more insidious, is of longer duration (days to years), and is characterized by influx of lymphocytes and macrophages with associated vascular proliferation and fibrosis (scarring).
Tehseen Anwar 13-Arid-1112 03450743978

CHRONIC INFLMMATION
It is inflammation of prolonged duration(weeks to years) in which continuing inflammation, tissue injury,and healing, often by fibrosis, proceed simultaneously.
It is characterized by different set of reactions involved
Infiltration with mononuclear cells, including macrophages, lymphocytes, and plasma cells.
Tissue destruction, largely induced by the products of theinflammatory cells.
Repair, involving new vessel proliferation (angiogenesis)and fibrosis.
Tehseen Anwar 13-Arid-1112 03450743978
CAUSES OF CHRONIC INFLAMMATION
Persistent infections
Microbes that are difficult to eradicate e.g. Mycobacterium tuberculosis, Treponema pallidum (the causative organism of syphilis) and viruses and fungi.
These all cause persistent infections and evoke T lymphocyte–mediated immune response called delayed-type hypersensitivity.
Immune-mediated inflammatory diseases (hypersensitivity
Diseases)
Diseases that are caused by excessive and inappropriate activation of the immune system.
Under certain conditions, immune reactionsdevelop against the affected person’s own tissues, leading to autoimmune diseases.
Prolonged exposure to potentially toxic agents
Exogenous agents include silica which causes silicosis. Endogenous causes include atherosclerosis caused by
toxic plasma lipid componentssuch as cholesterol crystals.
Autoimmunity
Auto-antigens provoke self-perpetuating immune responses that cause chronic inflammatory diseases like RA, MS.
Responses against common environmental substances cause chronic allergic diseases, such as bronchial asthma.
Tehseen Anwar 13-Arid-1112 03450743978
CHRONIC INFLMMATORY CELLS AND MEDIATORS
Macrophages
These are dominant cells in chronic inflammation.
Macrophages are normally diffusely scattered in most connective tissues and are also found in organs
Kupffer cells – liver Sinus Histiocytes - spleen and lymph nodes Alveolar Macrophages – Lungs Microglia – brain
Together these cells constitute the so-called mononuclear phagocyte system, also known by the older name of reticuloendothelial system.
Mononuclear phagocytes arise from a common precursor in the bone marrow.
From the blood, monocytes migrate into various tissues and differentiate into macrophages.
The half-life of blood monocytes is about 1 day. The life span of tissue macrophages is several
months or years.
Tissue macrophages are activated by two major pathways:
1. Classical macrophage activation
Tehseen Anwar 13-Arid-1112 03450743978
2. Alternative macrophage activation
Macrophages are initially activated by the classical pathway, designed to destroy the offending agents, and this is followed by alternative activation, which initiates tissue repair.
LYMPHOCYTE
The activation of T and B lymphocytes is part of the adaptive immune response in infections and immunologic diseases. Both classes of lymphocytes migrate into inflammatory sites using some of the same adhesion molecule pairs and chemokines that
Tehseen Anwar 13-Arid-1112 03450743978

recruit other leukocytes.In the tissues, B lymphocytes may develop into plasma cells, which secrete antibodies, and CD4 + T lymphocytes are activated to secrete cytokines.
There are three subsets of CD4 + helper T cells thatsecrete different sets of cytokines and elicit different typesof inflammation:
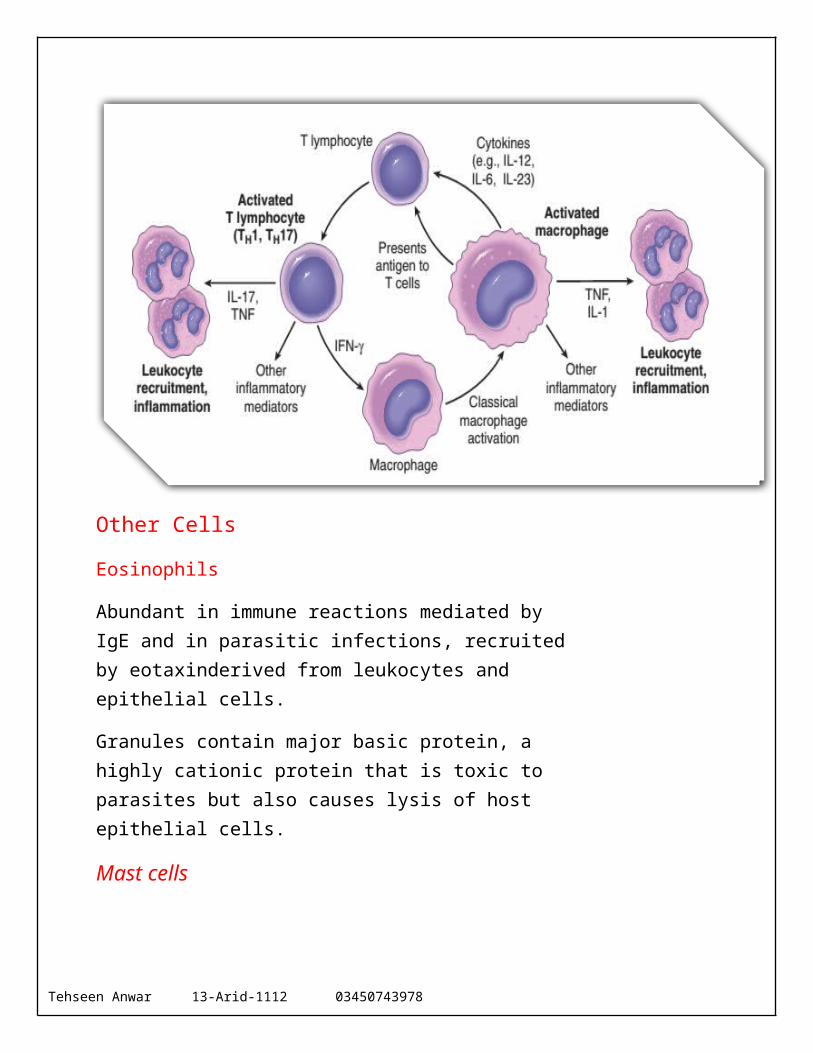
TH1 cells produce the cytokine IFN- γ, which activatesmacrophages in the classical pathway.
TH2 cells secrete IL-4, IL-5, and IL-13, which recruit and activate eosinophils and are responsible for the alternative pathway of macrophage activation.
TH17 cells secrete IL-17 and other cytokines that inducethe secretion of chemokines responsible for recruitingneutrophils and monocytes into the reaction.
Both TH1 and TH17 cells are involved in defense against many types of bacteria and viruses and in autoimmune diseases. TH2 cells are important in defense against helminthic parasites and in allergic inflammation.
Macrophages display antigens to T cells and produce membrane molecules (costimulators) and cytokines (notably IL-12) that stimulate T-cell responses.
Tehseen Anwar 13-Arid-1112 03450743978
Other Cells
Eosinophils
Abundant in immune reactions mediated by IgE and in parasitic infections, recruited by eotaxinderived from leukocytes and epithelial cells.
Granules contain major basic protein, a highly cationic protein that is toxic to parasites but also causes lysis of host epithelial cells.
Mast cells
Mast cells are “armed” with IgE antibody specific for certainenvironmental antigens. When these antigens are subsequently encountered, the IgE-coated mast cells are triggered to release histamines and AA metabolites that elicitthe early vascular changes of acute inflammation. IgEarmed mast
Tehseen Anwar 13-Arid-1112 03450743978
cells are central players in allergic reactions, including anaphylactic shock.
Neutrophils
Induced either by persistent microbes or by mediators produced by activated macrophages and T lymphocytes.
Neutrophil exudate can persist for many months in osteomyelitis. Cause chronic damage induced in lungs by smoking and other irritant stimuli.
GRANULOMATOUS INFLAMMATION
Granulomatous inflammation is a distinctive pattern of chronicinflammation characterized by aggregates of activated
macrophages with scattered lymphocytes.Granulomas can form under three settings:
With persistent T-cell responses to certain microbes(Such as Mycobacterium tuberculosis, T. pallidum, or fungi), in which T cell–derived cytokines are responsible for chronic macrophage activation. Tuberculosis is the prototype of a granulomatous disease caused by infection and should always be excluded as the cause when granulomas are identified.
Granulomas may also develop in some immune mediated inflammatory diseases, notably Crohn disease,which is one type of inflammatory bowel disease and animportant cause of granulomatous inflammation in theUnited States.
They are also seen in a disease of unknown etiologycalled sarcoidosis, and they develop in response to relatively inert foreign bodies (e.g., suture or splinter),forming so-called foreign body granulomas.
Tehseen Anwar 13-Arid-1112 03450743978
Examples of Diseases with Granulomatous Inflammation
SYSTEMIC EFFECTS OFINFLAMMATION
The systemic effects of inflammation, collectively called the acute-phase reaction, or the systemic inflammatory response syndrome. The cytokines TNF, IL-1, and IL-6 are the most important mediators of the acute-phase reaction. These cytokines are produced by leukocytes (and other cell types) in response to infection or in immune reactions and are released systemically.
The acute-phase response consists of several clinical andpathologic changes.
Fever
It is characterized by an elevation of body temperature, is one of the most prominent manifestations of the acute-phase
Tehseen Anwar 13-Arid-1112 03450743978

response. Fever is produced in response to substances called pyrogens that act by stimulating prostaglandin synthesis in the vascular and perivascular cells of the hypothalamus.
Mechanism
Bacterial products such as lipopolysaccharide (LPS) (called exogenous pyrogens) stimulate leukocytes to release cytokines such as IL-1 and TNF (called endogenous pyrogens) which increase thelevels of cyclooxygenases that convert AA into prostaglandins. In the hypothalamus the prostaglandins, especially PGE2, stimulate the production of neurotransmitters, which function to reset the temperature set point at ahigher level.
NSAIDs (Nonsteroidal anti-inflammatory drug) including aspirin, reduce fever by inhibiting cyclooxygenase and thus blocking prostaglandin synthesis.
Elevated plasma levels of acute-phase proteins
These plasma proteins are mostly synthesized in the liver. Three of the best known of these proteins are:
1. C-reactive protein (CRP, 2. fibrinogen3. serum amyloid A (SAA) protein
Synthesis of these molecules by hepatocytes is stimulated by cytokines, especially IL-6.
Tehseen Anwar 13-Arid-1112 03450743978
Function
Many acute-phase proteins, such as CRP and SAA, bind to microbial cell walls, and they may act as opsonins and fix complement.Fibrinogen binds to erythrocytes and causes them to form stacks (rouleaux) that sediment more rapidly at unit gravity than individual erythrocytes. This is the basis for measuring the erythrocyte sedimentation rate (ESR) as a simple test for the systemic inflammatory response, caused by anynumber of stimuli, including LPS.
Serial measurements of ESR and CRP are used to assess therapeutic responses in patients with inflammatory disorders such as rheumatoid arthritis. Elevated serum levels of CRP are now used as a marker for increased risk of myocardial infarction or stroke in patients with atherosclerotic vasculardisease. It is believed that inflammation is involved inthe development of atherosclerosis and increased CRP is a measure of inflammation.
Leukocytosis
It means production of leukocytes.Cytokines (CSFs) stimulate production of leukocytes from precursors in the bone marrow.
Leukemoid Reactions
Normal level of leukocyte is 15,000 to 20,000 cells/mL, but in some extraordinary cases it may reach 40,000 to 100,000 cells/mL. These extreme elevations are referred to as leukemiareactions because they are similar to those seen in leukemia.
Neutrophilia
Most bacterial infections induce an increase in the blood neutrophil count, called neutrophilia.
Tehseen Anwar 13-Arid-1112 03450743978

Lymphocytosis
Viral infections, such as infectious mononucleosis, mumps, and German measles, are associated with increased numbers of lymphocytes (lymphocytosis).
Eosinophilia
Bronchial asthma, hay fever, and parasite infestations all involve an increase in the absolute number of eosinophils, creating aneosinophilia.
Leukopenia
In typhoid fever and infections caused by some viruses, rickettsia, and certain Protozoa are usually associated with a decreased number of circulating white cells (leukopenia).
Because of cytokine-induced sequestration of lymphocytes in lymph nodes.
In some severe infections, septic shock: fall in blood pressure, disseminated intravascular coagulation, metabolic abnormalities; induced by high levels of TNF including IL-12 and IL-1.
OVERVIEW OF TISSUE REPAIR
Cells involved:
Labile cells: normally continuous turn over (e.g. epithelial and bone marrow cells) chances of regeneration are excellent.
Permanent cells: Not capable of proliferation (e.g. adult neurons) HEALING BY SCARRING(no regeneration).
Stable cells: normally little proliferation but remain capable of more rapid cell division following injury
Tehseen Anwar 13-Arid-1112 03450743978
(liver, renal tubular epithelium) Chances of regeneration are GOOD.
Tissue and healing
Granulation tissue: mixture of proliferating capillaries (angioblasts), fibroblasts, macrophages and plasma cells. Granulation tissue is formed by the action of different cytokines and growth factors released by blood platelets and macrophages.
Healing by primary (first) intention: In simple skin incisions where the edges are in close apposition and actual defect is minimal, healing occur quickly with small amount of granulation tissue.
Healing by secondary (second) intention: in other situations when wound edges are far apart and tissue defect is large and filed with blood clot and variable amount of debris, here organization and filling of defect with extensive granulation take place a long time.
Tehseen Anwar 13-Arid-1112 03450743978