chronic ear disease as a possible reason for trephination
TRANSCRIPT
Internafional Iournal of Osteoarrhaeology, Vol 1: 165-168 /I9911
Chronic Ear Disease as a Possible Reason for Trephination GEORGEMANN 25 Chesterton Hall Crescent, Cambridge CB4 lAW, UK
ABSTRACT It is rare for any reason to be deduced for the operation of trephination. A Peruvian skull is presented with three trephine holes on one side and evidence of the chronic ear infection known as cholesteatoma on the other. This infection would have produced a facial paralysis on the same side. It is suggested that there would have been an awareness of the connection between the motor area of the brain on one side and the movement of the opposite side of the body, and that a trephination might have been carried out in an atternptto relievea supposed brain lesion, albeit on the wrong side.
Keywords: Trephination, Cholesteatoma, Paralysis
Introduction
Numerous examples of trephination have been reported from world-wide sites, but apart from an occasional association with a fractured skull it is rare that any reason can be deduced for this hazardous procedure. The skull described here shows, in addition to three trephinations, evidence on the right side of the chronic ear infection known to otologists as cholesteatoma. It is suggested that this might have provided a reason for the operation.
Cholesteatoma is a condition in which, for reasons which are still under discussion, the columnar epithelium of the middle ear air spaces becomes replaced by a stratified keratinizing type. This results in a gradual accumulation of keratinous debris, which becomes infected by low-grade pathogenic organisms. As a result of local pressure and low-grade osteitis the surrounding bone is slowly eroded with the possibility of damage to the many important structures that surround the middle ear cleft. There is no macroscopic evidence of bony reac- tion to this erosive process, and often the only external evidence is a small erosion of the tympanic ring in the upper posterior part of the deep external meatus. Spread of the infection may take place superiorly and enter the middle cranial fossa; posteriorly to enter the posterior
cranial fossa and the sigmoid sinus; or medially to enter the inner ear. It may also erode the canal carrying the facial nerve across the medial wall of the middle ear. The ossicles, particularly the incus, are involved early causing partial deaf- ness. In spite of the severe consequences of these intracranial complications, the initial symptoms are slight, consisting only of partial deafness and a thin, foul-smelling discharge.
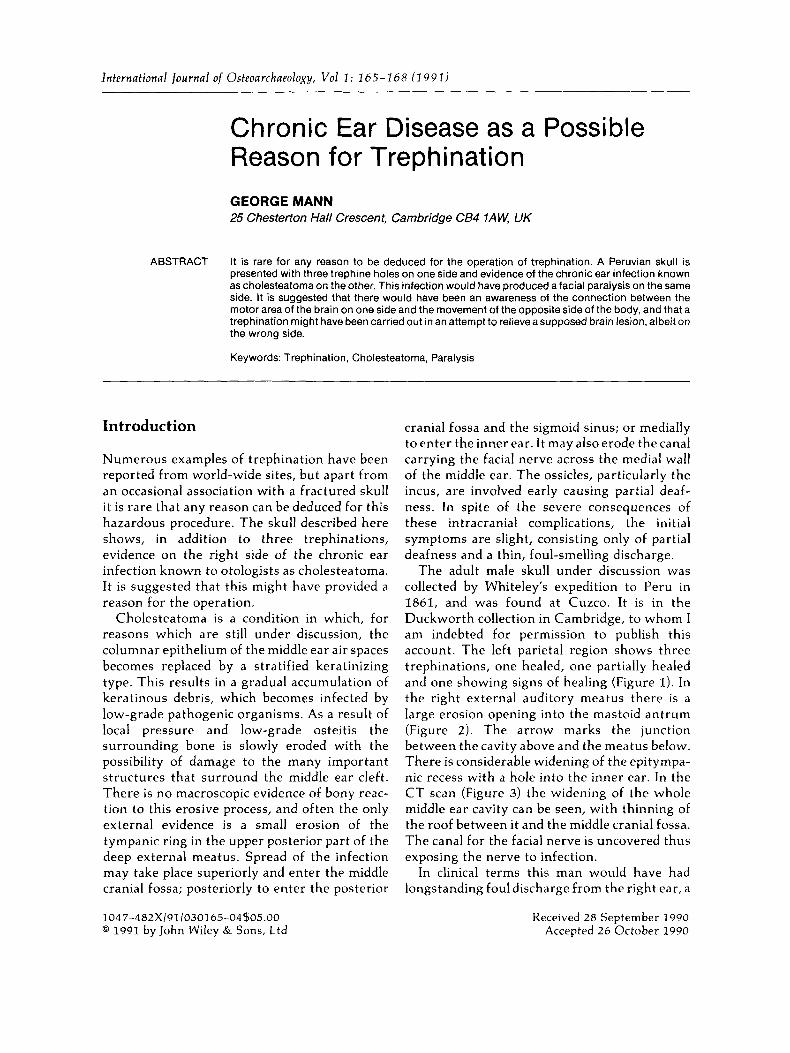
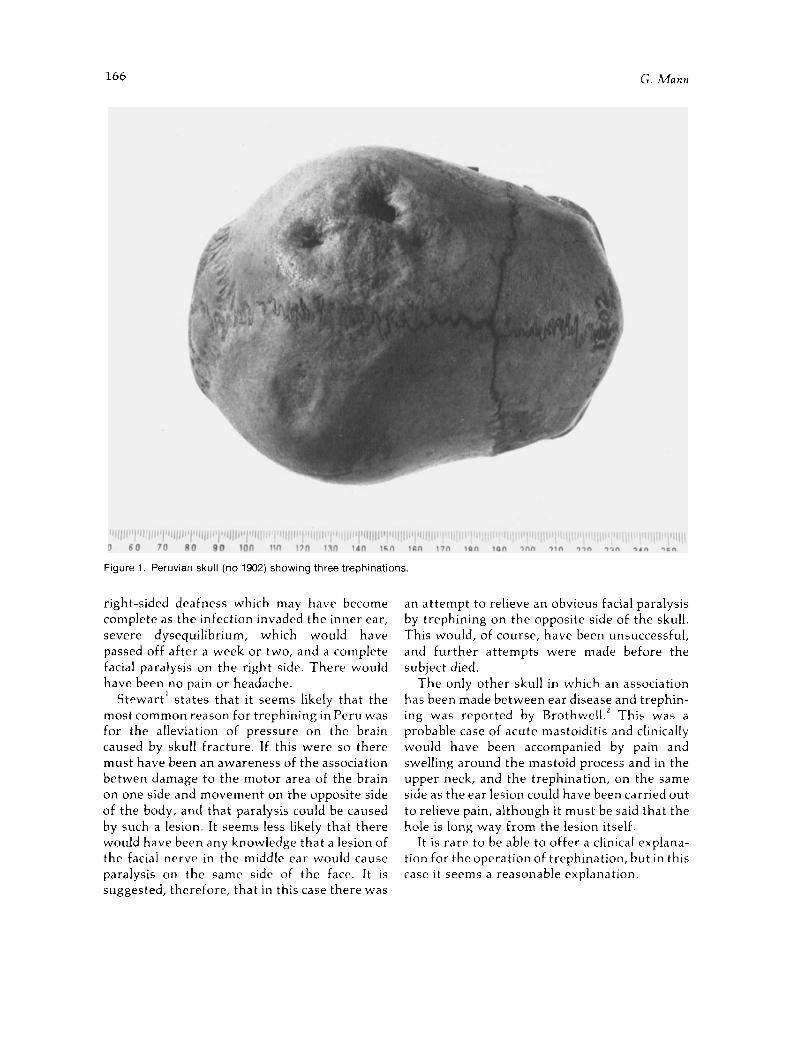
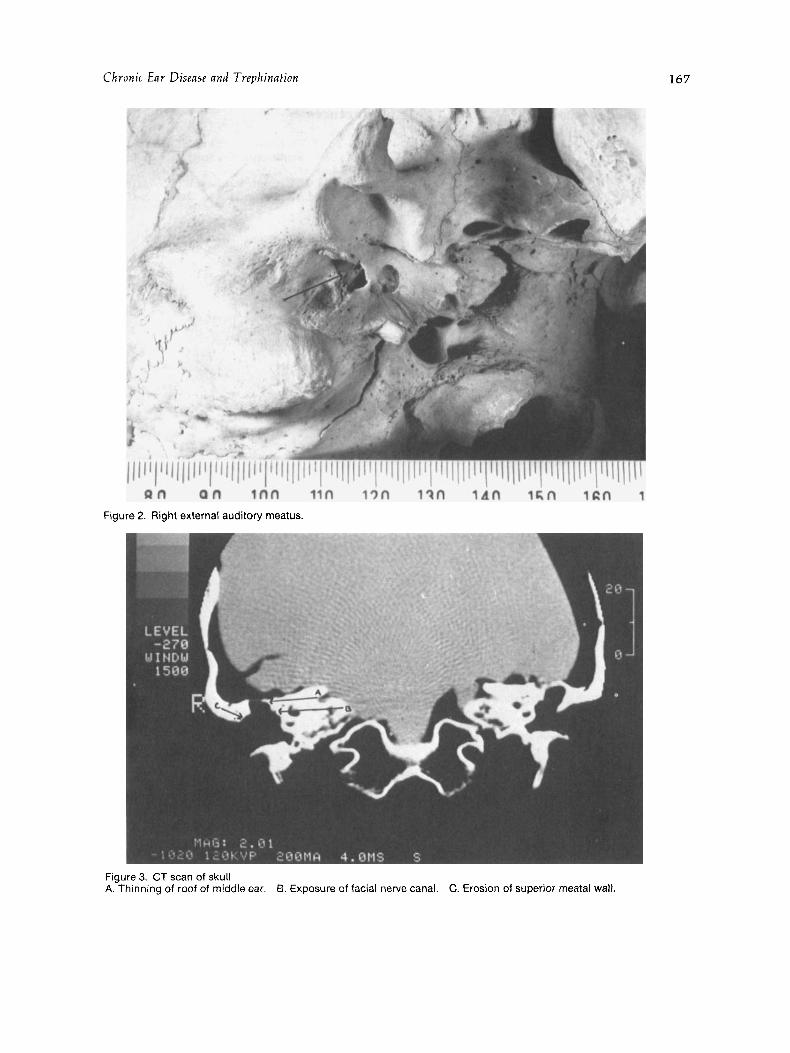
The adult male skull under discussion was collected by Whiteley's expedition to Peru in 1861, and was found at Cuzco. It is in the Duckworth collection in Cambridge, to whom I am indebted for permission to publish this account. The left parietal region shows three trephinations, one healed, one partially healed and one showing signs of healing (Figure I). In the right external auditory meatus there is a large erosion opening into the mastoid antrum (Figure 2 ) . The arrow marks the junction between the cavity above and the meatus below. There is considerable widening of the epitympa- nic recess with a hole into the inner ear. In the CT scan (Figure 3 ) the widening of the whole middle ear cavity can be seen, with thinning of the roof between it and the middle cranial fossa. The canal for the facial nerve is uncovered thus exposing the nerve to infection.
In clinical terms this man would have had longstanding foul discharge from the right ear, a
1047-482x/91/030165-04$05.00 @ 1991 by John Wiley & Sons, Ltd
Received 28 September 1990 Accepted 26 October 1990
166 G. Mann
Figure 1. Peruvian skull (no 1902) showing three trephinations.
right-sided deafness which may have become complete as the infection invaded the inner ear, severe dysequilibrium, which would have passed off after a week or two, and a complete facial paralysis on the right side. There would have been no pain or headache.
Stewart' states that i t seems likely that the most common reason for trephining in Peru was for the alleviation of pressure on the brain caused by skull fracture. If this were so there must have been an awareness of the association betwen damage to the motor area of the brain on one side and movement on the opposite side of the body, and that paralysis could be caused by such a lesion. It seems less likely that there would have been any knowledge that a lesion of the facial nerve in the middle ear would cause paralysis on the same side of the face. It is suggested, therefore, that in this case there was
an attempt to relieve an obvious facial paralysis by trephining on the opposite side of the skull. This would, of course, have been unsuccessful, and further attempts were made before the subject died.
The only other skull in which an association has been made between ear disease and trephin- ing was reported by Brothwell.' This was a probable case of acute mastoiditis and clinically would have been accompanied by pain and swelling around the mastoid process and in the upper neck, and the trephination, on the same side as the ear lesion could have been carried out to relieve pain, although it must be said that the hole is long way from the lesion itself.
It is rare to be able to offer a clinical explana- tion for the operation of trephination, but in this case it seems a reasonable explanation.
Chronic Ear Disense and Trephination
Figure 2. Right external auditory meatus.
Figure 3. CT scan of skull A. Thinning of roof of middle ear. B. Exposure of facial nerve canal. C. Erosion of superior meatal wall.
167

168 G. Mann
Acknowledgements References
My thanks are due to Dr Desrnond Hawkins of Addenbrookes Hospital, Cambridge for the CT scant and to Mr G. Owen Of the Of
Archaeology for the photographs.
1. Stewart, T. D. Stone Age Skull Surgery. Wash- ington, DC: Smithsonian Institute Reports (1957),
2. Brothwell, D. R. Contributions on trephination in ancient and modern times. Man, 1959; 59: 95.
1958: 469-491.