chronic care program - care coordination service€¦ · web viewthe clinical care coordinator and...
TRANSCRIPT

CHHS18/022
Canberra Hospital and Health ServicesOperational Procedure Chronic Care Program - Care Coordination ServiceContents
Contents....................................................................................................................................1
Purpose.....................................................................................................................................2
Scope........................................................................................................................................ 2
Section 1 – Care Coordination Service Model – Chronic Care Program....................................2
Section 2 – Referral...................................................................................................................5
Section 3 – Triage categories....................................................................................................5
Implementation........................................................................................................................ 6
Related Policies, Procedures, Guidelines and Legislation.........................................................6
References................................................................................................................................ 7
Definition of Terms...................................................................................................................7
Search Terms............................................................................................................................ 8
Attachments..............................................................................................................................8
Attachment 1: Care Coordination Service Flowchart............................................................9
Attachment 2: Care Coordination Service information for clinicians..................................10
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases1 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/022
Purpose
The purpose of this procedure is to define the process for care coordination: triaging, assessing and managing referrals and graduation from the service to ensure consistent, equitable and transparent care.
This document outlines the model of care coordination and the clinical management processes followed by the Care Coordination Service, a part of the Chronic Care Program in the ACT Health Division of Medicine.
Back to Table of Contents
Scope
This procedure applies to staff and patients of the Care Coordination Service.
This document applies to the following staff working within their scope of practice: Medical Officers Nurses and Midwives Allied Health Professionals Students under direct supervision.
Back to Table of Contents
Section 1 – Care Coordination Service Model – Chronic Care Program
There are a range of models available for the management and care coordination of those living with chronic disease. Amongst these are the Flinders Chronic Condition Management Program, Stanford Chronic Disease Self-Management Program, Hospital Admission Risk program (HARP) and the Wagner Chronic Care Model. However, one model of self-management support may not be appropriate to meet all the needs of a person (Department of Human Services, Victoria). Ideally, a range of self-management support options is needed. This is particularly so when providing clinical coordination services for patients with chronic disease and complex needs. Support is also required for families (as defined by the patient) in order to harness their ability to make positive contributions to the health and wellbeing of the patient.
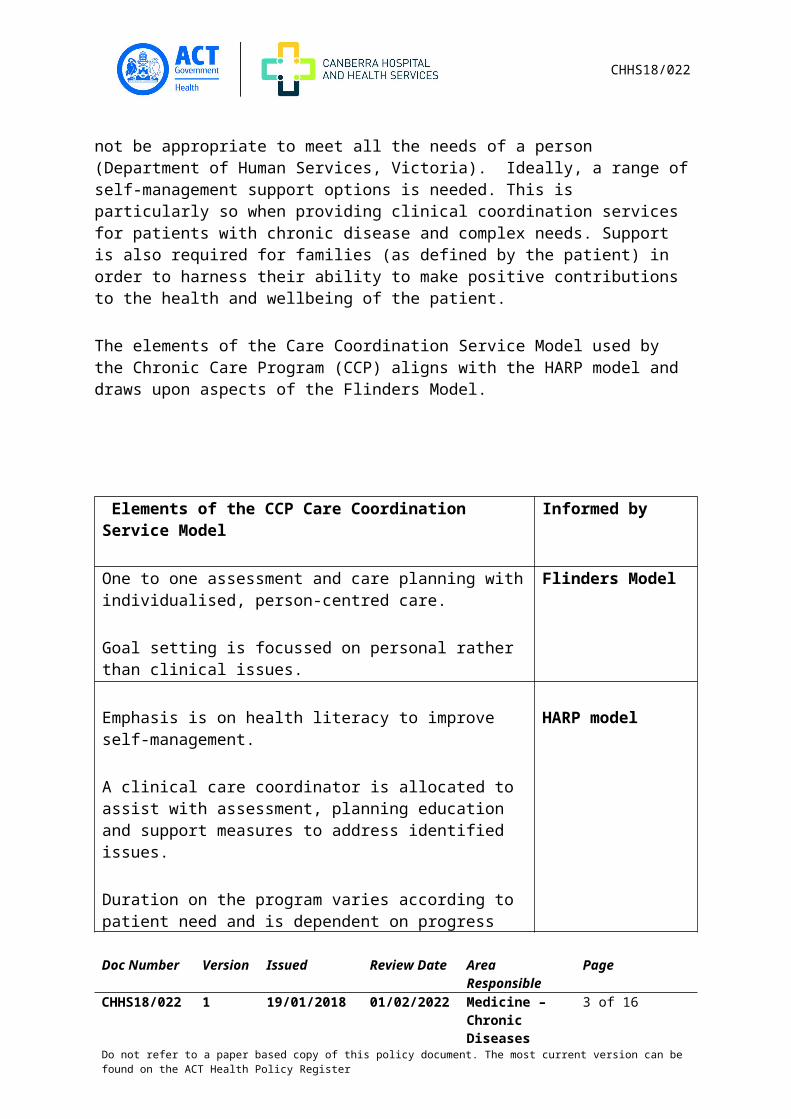
The elements of the Care Coordination Service Model used by the Chronic Care Program (CCP) aligns with the HARP model and draws upon aspects of the Flinders Model.
Elements of the CCP Care Coordination Service Model Informed by
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases2 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/022
One to one assessment and care planning with individualised, person-centred care.
Goal setting is focussed on personal rather than clinical issues.
Flinders Model
Emphasis is on health literacy to improve self-management.
A clinical care coordinator is allocated to assist with assessment, planning education and support measures to address identified issues.
Duration on the program varies according to patient need and is dependent on progress made towards goal achievement.
Targets patients living with chronic disease, co-morbidities and who have complex needs.
HARP model
AimThe aim of the Care Coordination Service Model used by CCP is to increase the patient’s capacity to self-manage and enable their support systems to reduce presentations to emergency departments and unnecessary admission to hospital.
Application of the Care Coordination Service ModelThe CCP is located in Ambulatory Services within the Division of Medicine. This is provided by a multidisciplinary team comprising allied health professionals, nurses and medical practitioners. The clinical settings for care coordination are those based around a primary health care approach and include outpatient clinics, general practice, community health and the patient’s place of residence. Support is provided by clinical care coordinators to patients on the program who present to emergency department or who are admitted to hospital.
Care Coordination Service Model in Action Assessment Initial assessments are based on physical, environmental, psychosocial,
spiritual and social factors. Assessment may include discussion and addressing losses which affect meaning and purpose in life.
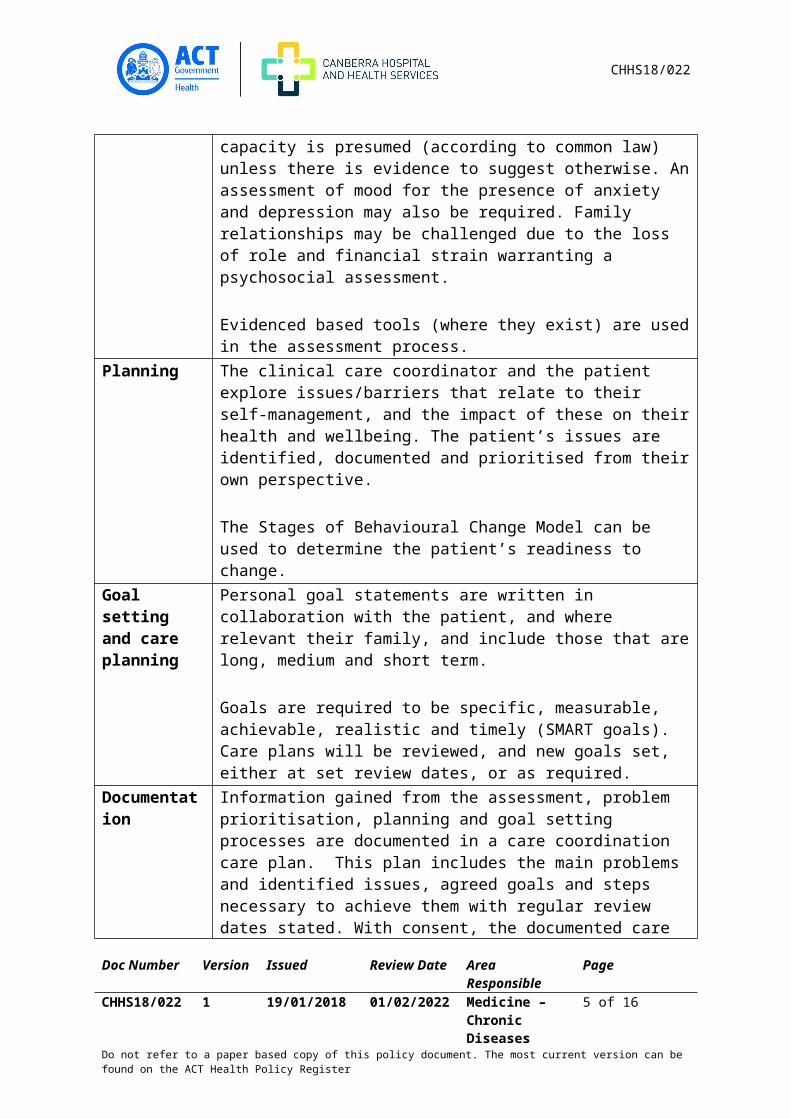
Risk factor assessment is undertaken relating to the ability to self-manage condition, access services, maintain environmental safety, conduct activities of daily living, and make healthy lifestyle choices including diet, physical activity, alcohol and smoking. Cognitive capacity is presumed (according to common law) unless there is evidence to suggest otherwise. An assessment of mood for the presence of anxiety
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases3 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/022
and depression may also be required. Family relationships may be challenged due to the loss of role and financial strain warranting a psychosocial assessment.
Evidenced based tools (where they exist) are used in the assessment process.
Planning The clinical care coordinator and the patient explore issues/barriers that relate to their self-management, and the impact of these on their health and wellbeing. The patient’s issues are identified, documented and prioritised from their own perspective.
The Stages of Behavioural Change Model can be used to determine the patient’s readiness to change.
Goal setting and care planning
Personal goal statements are written in collaboration with the patient, and where relevant their family, and include those that are long, medium and short term.
Goals are required to be specific, measurable, achievable, realistic and timely (SMART goals). Care plans will be reviewed, and new goals set, either at set review dates, or as required.
Documentation Information gained from the assessment, problem prioritisation, planning and goal setting processes are documented in a care coordination care plan. This plan includes the main problems and identified issues, agreed goals and steps necessary to achieve them with regular review dates stated. With consent, the documented care plan is shared with the patient’s General Practitioner (GP), and relevant health professionals involved in their care.
Review During the assessment, planning and goal setting processes a range of techniques may be used by clinical care coordinators including motivational interviewing, counselling and health coaching to assist patients achieve their goals. Regular reviews are conducted to assess progress towards goal attainment.
Time to discharge from the care coordination service is contingent on goals being achieved. Duration on the program varies with each individual.
Back to Table of Contents
Section 2 – Referral
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases4 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/022
The CCP process for managing referrals is outlined in the Care Coordination Service Flowchart at attachment 1. To make a referral, complete the Care Coordination Service Chronic Care Program - Care Coordination Service. This form is available from the Clinical Forms register on the intranet.
Referring clinicians should review the eligibility criteria on the referral form. Further information is contained in the flyer ‘Care Coordination Service - information for clinicians’ at attachment 2.
A consumer handout ‘Care Coordination Service - information for consumers’ is available on the intranet from the Policy and Clinical Guidance Register.
Back to Table of Contents
Section 3 – Triage categories
All patients who are referred to the service for care coordination will be triaged initially as Category 1 (high intensity). This is because an initial assessment and care planning is required which may take several weeks to a month to finalise depending on the patient’s general wellbeing.
Category 1 applies to patients who have multiple issues that require regular and frequent home visits and/or phone calls (more than once a month) whilst services and/or supports are put in place. The goal is to gradually help patients progress to Category 2 when and if appropriate and safe to do so. Some patients will remain on Category 1 throughout the duration of their time on the care coordination service.
Category 2 applies to patients on the program who have progressed from Category 1 and only require phone contact once a month. These patients are generally able to self-manage, have appropriate supports in place and are clinically stable. If they remain stable and their goals are reached, they may be discharged from the care coordination service. The patient may be referred back to the care coordination service, if required at a later date. This will require a new referral form from the clinician.
Some patients will move between high (category 1) and low intensity support (category 2) from clinical care coordinators. Patients should be informed of how they are likely to progress through the program at the time written consent is obtained. The goal of care coordination is for all patients to focus on self-management strategies and to progress along the continuum from Category 1 to Category 2 and discharge.
Back to Table of Contents
Implementation
This procedure will be: Available to all staff on the Policy register on SharePoint.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases5 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS18/022
Included in the orientation of new staff to the care coordination program. Communicated to staff through an all staff email and via team meetings.
Back to Table of Contents
Related Policies, Procedures, Guidelines and Legislation
Policies Health Directorate Nursing and Midwifery Continuing Competence Policy Consent and Treatment ACT Health Work Health and Safety Management System (WHSMS) Risk Management Policy Violence and Aggression by Patients Consumers or Visitors Prevention and Management
Policy Work Health and Safety Management System – Section 7.7 Work Health and Safety Policy Approval to Use Private Vehicles for Official Purposes Policy and Procedure
Procedures CHHS Healthcare Associated Infections Clinical Procedure CHHS Patient Identification and Procedure Matching Policy Clinical Record Documentation procedure Significant Incident procedure Violence and Aggression by Patients Consumers or Visitors Procedure Home Visiting operation Procedure
Guidelines Standards of Practice for ACT Allied Health Professionals Risk Management Guidelines Risk Management Framework The Australian Charter of Healthcare Rights: A guide for patients, consumers, carers and
families ACT Charter of Rights for people who experience mental health issues ACT Health Reconciliation Action Plan 2015 - 2018 ACT Chronic Conditions Strategy- Improving Care and Support 2013-2018 Multicultural Co-ordinating Framework – Towards Culturally Appropriate and Inclusive
Services 2014-2018
Legislation Health Records (Privacy and Access) Act 1997 Human Rights Act 2004 Work Health and Safety Act 2011 Carers Recognition Act 2010 Safety Rehabilitation and Compensation Act 1988 Mental Health Act 2015
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases6 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/022
Work Health and Safety Regulation 2011
Back to Table of Contents
References
1. Australian Health Ministers’ Advisory Council, 2017, National Strategic Framework for Chronic Conditions. Australian Government. Canberra.
2. Bird S, Noronha M, Sinnott H. An integrated care facilitation model improves quality of life and reduces use of hospital resources by patients with chronic obstructive pulmonary disease and chronic heart failure. Australian Journal of Primary Health. 2010 (16) 326- 333p
3. Department of Health, 2015, Victoria Common models of chronic disease self-management support: A factsheet for primary care partnerships available from: http://vicpcp.org/wp-content/uploads/2015/10/Common-models-of-chronic-disease.pdf
4. Fiandt, Karen. The chronic care model: description and application for practice. Topics in Advance Practice Nursing eJournal. 2006; 6(4)
5. Flinders Program Information paper (2017) available from: http://www.flinders.edu.au/medicine/fms/sites/FHBHRU/Flinders%20Program%20Information%20Paper.pdf
6. http://www.ihi.org/resources/Pages/Changes/ ChangestoImproveChronicCare.aspx
7. Wagner EH. Chronic disease management: What will it take to improve care for chronic illness? Effective Clinical Practice. 1998 (1) 2-4p
Back to Table of Contents
Definition of Terms
ACTPAS - Australian Capital Territory Patient Administration System CCP - Chronic Care ProgramCHF - Chronic Heart Failure COPD - Chronic Obstructive Pulmonary DiseaseCRIS - Clinical Record Information SystemPD - Parkinson’s disease
Back to Table of Contents
Search Terms
Chronic care program, Care coordination
Back to Table of Contents
Attachments
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases7 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/022
Attachment 1: Care Coordination Service FlowchartAttachment 2: Care Coordination Service information for clinicians
Disclaimer: This document has been developed by ACT Health, Canberra Hospital and Health Services specifically for its own use. Use of this document and any reliance on the information contained therein by any third party is at his or her own risk and Health Directorate assumes no responsibility whatsoever.
Policy Team ONLY to complete the following:Date Amended Section Amended Divisional Approval Final Approval 10/01/2018 Complete review ED Medicine CHHS Policy Committee
This document supersedes the following: Document Number Document NameCHHS13/393 Chronic Care Program -Triaging Assessment and Management of Referrals
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases8 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/022
Attachment 1: Care Coordination Service Flowchart
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases9 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
CHHS18/022
Attachment 2: Care Coordination Service information for clinicians
The Care Coordination Service provides support services for people living in the community who have had several hospital admissions or ED presentations related to their chronic condition. These conditions include chronic heart failure (CHF), chronic obstructive pulmonary disease (COPD), Parkinson’s disease (PD) or other conditions by arrangement.
Clinical care coordinators perform a comprehensive person-centred assessment. Goal setting interventions are developed with the patient and the health professionals involved in their care. The aim is to achieve a coordinated approach to the management of the patient’s condition. Care is person-centred, focussing on the development and/or support of self-management skills to improve quality of life and adaptation to living with a chronic condition. This may also include a palliative approach. The Care Coordination Service assists the patient to remain well in the community, and to navigate and engage with the health system. This may result in prevention of unnecessary hospital presentations and admissions. To achieve this clinical care coordinators may:
Arrange support services for the patient in the community to assist health management Provide patient education and strategies to help them self-manage their condition Provide ongoing patient contact via home visits and phone consultation Liaise and advocate with patient’s GP, specialist and other health care
professionals/service providers regarding appointments and health management Discuss and document Advance Care Planning conversations/decisions in line with
patients’ wishes.
Eligibility criteria: Adult (> 18 years old) ACT resident Under the care of a relevant specialist (cardiologist, neurologist/geriatrician or respiratory
specialist) with a documented medical management plan for their Heart Failure, Chronic Obstructive Pulmonary Disease, Parkinson’s Disease or other conditions by arrangement with the Chronic Care Program Manager
Has a need for psychosocial or clinical assistance to overcome barriers that may be affecting the patient from self-managing their chronic condition
More than 2 presentations per annum to hospital related to their chronic condition
How to refer? Ensure patient/EPOA consent is obtained for referral Complete the Care Coordination Service Referral Form (25018) listed on the Clinical
Forms Register Include a documented medical plan with the Care Coordination Service Referral Form
For further information, call the Chronic Care Program on 02 6244 2273.
Doc Number Version Issued Review Date Area Responsible PageCHHS18/022 1 19/01/2018 01/02/2022 Medicine –
Chronic Diseases10 of 10
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register