christian sonnier m.d. lsu family medicine alexandria pgy-2 6/16/15 this is supplemental information...
TRANSCRIPT
Christian Sonnier M.D.LSU Family Medicine Alexandria PGY-2
6/16/15
This is supplemental information and is not intended to replace the information presented on the AFMB review lecture. In the event of any discrepancy between the information here and the AFMB review, you should err on the side of the AFMB review.

goals/learning pointsDefinition of acute abdomen
Differential Diagonosis
Clinical manifestation and diagnosis
Treatment
Atypical abdominal pain

DEFINITIONThe term acute abdomen refers to a
sudden, severe abdominal pain that is less than 24 hours in duration.
Abdominal pain can be Visceral Somatic Referred/neurological

CLINICAL ASSESSMENT: Characterizing the pain is the key
Visceral pain Stretching of
peritoneum or organ capsules by distension or edema
Diffuse Poorly localized May be perceived at
remote locations related to organ’s sensory innervation
Somatic pain Inflammation of parietal
peritoneum or diaphragm Sharp Well-localized Referred pain Perceived at distance
from diseased organ Pneumonia Acute MI Male GU problems Right shoulder pain can
be gall bladder or pancrease

CLINICAL ASSESSMENTLocation
Upper abdomen → PUD, cholecystitis, pancreatitisLower abdomen → Diverticulitis, ovary cyst, TOAMid abdomen → early appendicitis, SBO
Migratory pattern Epigastric → Peri-umbil → RLQ = Acute appendicitis Localized pain → Diffuse = Diffuse peritonitis
“Referred pain”Biliary disease → R shoulder or backSub-left diaphragm abscess → L shoulderAbove diaphragm(lungs) → Neck/shoulder
Acute onset & unrelenting pain = bad/consider sugical emergency Other red flags: rebound, rigidity, hemodynamic instability
Pain which resolves usually. not surgical

Clinical Assessment : Other History
GI symptomsNausea, emesis ( bilious
or bloody)Constipation,
obstipation (last BM or flatus)
Diarrhea (? bloody)Both Nausea/Diarrhea
present usu. medicalChange in sx w eating?
NSAID use (perf DU)Jaundice, acholic
stools, dark urine
Drinking history (pancreas)
Prior surgeries (adhesions → SBO, ?still have gallbladder & appendix)
History of herniasUrine output
(dehydrated)Constituational Sx
Fevers/chillsSexual history

Clinical DiagnosisLocation of pain by
organ*RUQ
GallbladderEpigastrum
StomachPancreas
Mid abdomenSmall intestine
Lower abdomenColon, GYN pathology

Clinical Diagnosis

Think Broad categories for DDxInflammationObstructionIschemiaTraumainfectionPerforation (any of above can end here)
Offended organ becomes distendedLymphatic/venous obstrux due to ↑pressureArterial pressure exceeded → ischemiaProlonged ischemia → perforation
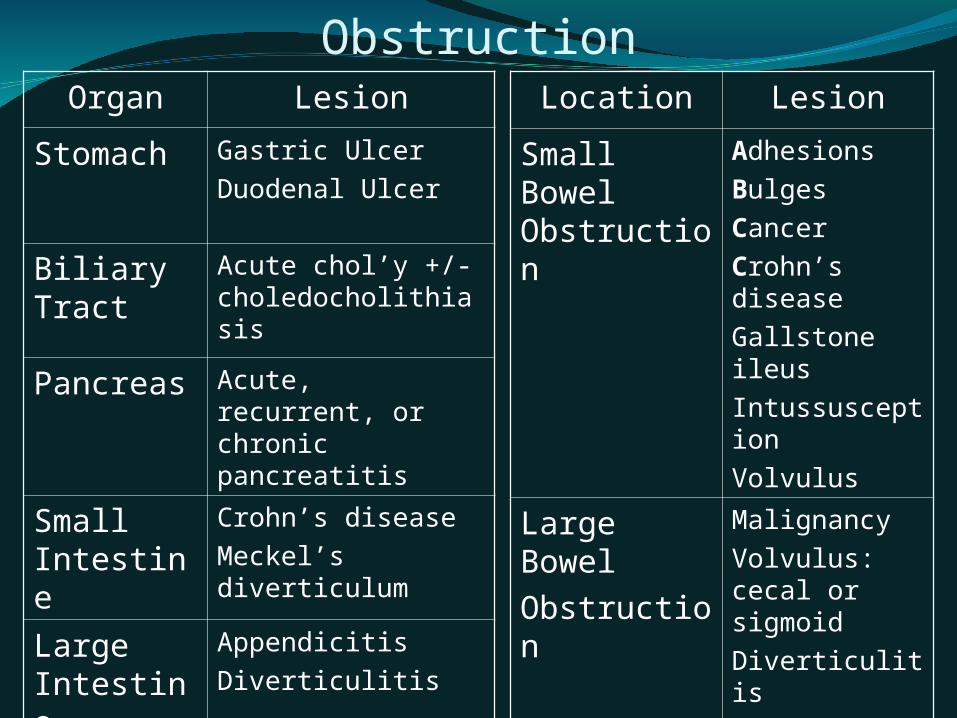
Inflammation versus ObstructionOrgan Lesion
Stomach Gastric Ulcer
Duodenal Ulcer
Biliary Tract
Acute chol’y +/-choledocholithiasis
Pancreas Acute, recurrent, or chronic pancreatitis
Small Intestine
Crohn’s disease
Meckel’s diverticulum
Large Intestine
Appendicitis
Diverticulitis
Location Lesion
Small Bowel Obstruction
Adhesions
Bulges
Cancer
Crohn’s disease
Gallstone ileus
Intussusception
Volvulus
Large Bowel
Obstruction
Malignancy
Volvulus: cecal or sigmoid
Diverticulitis

Ischemia / PerforationAcute mesenteric ischemia
Usually acute occlusion of the SMA from thrombus or embolism
“cramping/tight/pressure feeling of abdomen”Think the acs of the bowels
Chronic mesenteric ischemiaTypically smoker, vasculopath with severe
atherosclerotic vessel diseaseIschemic colitisAny inflammation, obstructive, or ischemic
process can progress to perforationRuptured abdominal aortic aneurysm
Profound hemodynamic instability

GYN EtiologiesOrgan Lesion
Ovary Ruptured graafian follicle
Torsion of ovary
Tubo-ovarian abscess (TOA)
Fallopian tube Ectopic pregnancy
Acute salpingitis
Pyosalpinx
Uterus Uterine rupture
Endometritis

Labs & ImagingTest Reason
CBC w diff Left shift can be very telling
CMP N/V, lytes, acidosis, dehydration
Amylase Pancreatitis, perf DU, bowel ischemia
LFT Jaundice,hepatitis
UA GU- UTI, stone, hematuria
Beta-hCG Ectopic
Test ReasonKUBFlat & Upright
SBO/LBO, free air, stones
Ultrasound Cholecystitis, jaundice,
GYN pathology
CT scan-Diagnostic
accuracy
Anatomic dx,
Case not straightforward

CT scan
What is the diagnosis? Acute appendicitis

Non-Surgical Causes by Systems
System Disease System DiseaseCardiac Myocardial infarction
Acute pericarditisEndocrine Diab ketoacidosis
Addisonian crisis
Pulmonary Pneumonia
Pulmonary infarction
PE
Metabolic Acute porphyria
Mediterranean fever
Hyperlipidemia
GI Acute pancreatitis
Gastroenteritis
Acute hepatitis
Musculo- skeletal
Rectus muscle hematoma
GU Pyelonephritis CNS
PNS
Tabes dorsalis (syph)
Nerve root compression
Vascular Aortic dissection Heme Sickle cell crisis

Special Circumstances[Atypical presentations]
Situations making diagnosis difficultStroke or spinal cord injuryInfluence of drugs or alcohol
Severity of disease can be masked by:SteroidsImmunosuppression (i.e. AIDS)Threshold to operate must be even lower

MANAGEMENTO2 by ncmaskcpap/bipapmechanical
ventilationIV LR or NSEmperic antibiotic treatment as appropriateManagement of sepsis as neededDetermine if need for surgical consult as well
as need for ICU care

MANAGEMENT [contd.]Monitor EKG
CONSIDER POSSIBLE MI WITH PAIN REFERRED TO ABDOMEN IN PTs >30 YEARS OLD
Keep pt NPOAnalgesia – controversial, Demerol has some limited
evidence of being superior however goal is to relieve pain so may require opiods
PASG* J Trauma. 1993 May;34(5)
This stands for Pneumatic Abdominal Anti-Shock Garment. An inflated abdominal wrapping designed to place pressure on
the abdomen in the setting of intra-abdominal hemorrhage. Fallen out of use but you may still see it

Decision to operatePeritonitis
Tenderness w/ rebound, involuntary guardingSevere / unrelenting pain“Unstable” (hemodynamically, or septic)
Tachycardic, hypotensive, white countIntestinal ischemia, including strangulationPneumoperitoneumComplete or “high grade” obstruction
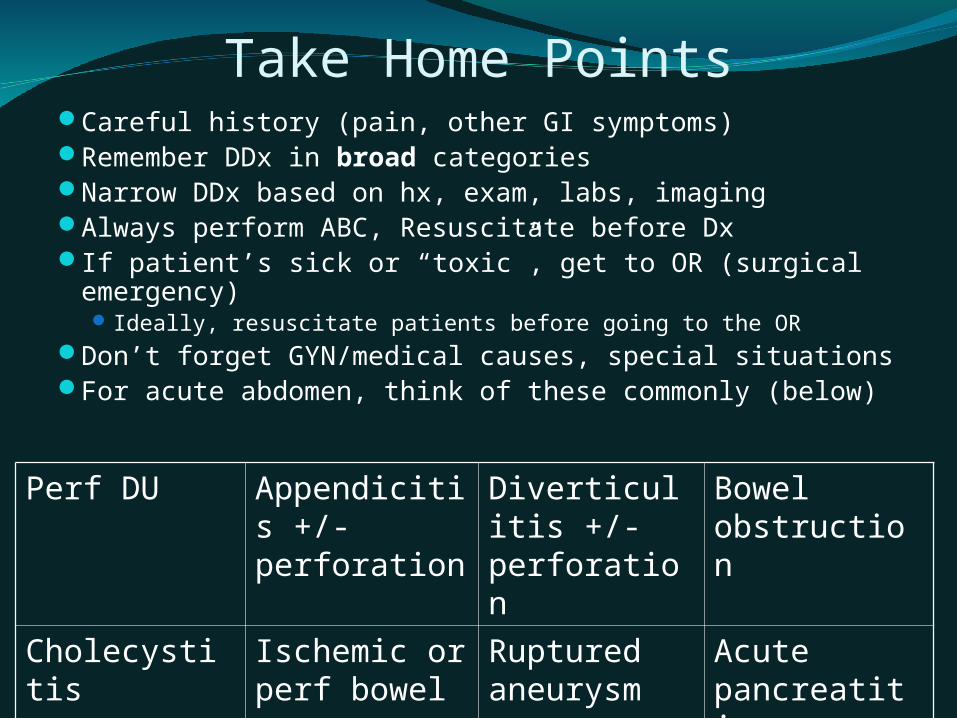
Take Home PointsCareful history (pain, other GI symptoms)Remember DDx in broad categoriesNarrow DDx based on hx, exam, labs, imagingAlways perform ABC, Resuscitate before DxIf patient’s sick or “toxic”, get to OR (surgical
emergency) Ideally, resuscitate patients before going to the OR
Don’t forget GYN/medical causes, special situationsFor acute abdomen, think of these commonly (below)
Perf DU Appendicitis +/- perforation
Diverticulitis +/- perforation
Bowel obstruction
Cholecystitis Ischemic or perf bowel
Ruptured aneurysm
Acute pancreatitis

Pt is a 55 year old male with history of 30 pack year smoking, prior MI with stents, and long term heavy alcohol abuse. Presents to the ED following MVC one hour ago. The patient has stable vital signs and is complaining of intense abdominal pain diffusely . Labs show wbc of 25 with left shift. CMP is wnl with a metabolic acidosis. EKG, CT abdomen/pelvis and cxr as well as other labs are pending. What should be included on differential dx?
A) acute MIB) GastroenteritisC) PancreatitisD) Bowel perforationE) Aortic AneurysmF) Ischemic coltis

Answer:
All of the above.
Rational: -Acute MI: patient has prior MI and has significant CAD history-Gastroenteritis: should always been on the differential of abdominal pain as it is one of the most common reasons for abdominal pain-Pancreatitis: patient has significant alcohol abuse history-Bowel perforation: any acute abdominal process can lead to perforation if inflammation or trauma is bad enough. Trauma from mvc-Aortic Aneurysm: patient has significant cad history-ischemic Colitis: significant CAD history
Take home point: acute severe abdominal pain under the right circumstances has a very broad ddx

Suppose the same patient has the following:
Sudden acute hemodynamic instability and on exam patient has intense abdominal pain with light palpation and shaking of bed or legs as well as percussion of the abdomen. During exam and interview the patient suddenly develops hypotension and respiratory distress and a decrease in GCS from 15 to 6 as he becomes somulent. The patient has not made it to the CT scanner yet.
What is the best next course of action?
A)Stabilize patient with intubation as needed and cvc with rapid fluid infusionB)Obtain stat surgical consultC)Apply PASG D)Perform diagnostic peritoneal lavage and FAST ScanE)Admit to SICU F)Wait for ct scan of abdomen and pelvis before further action
Answer:
All of the above with exception of waiting for ct scan are valid option. The patient is becoming rapidly unstable and needs stabilization and stat surgical consult. The differential diagnosis is still very broad as he may have aortic dissection, perforation or intra-abdominal hemorrhage.
Fast Scan if available can remove need for diagnostic perotoneal lavage and per ATLS is replacing this as the prefered diagnostic modality however it is still an option if ultrasound is not available however it would be best to run this by the surgical consult first.
PASG: Pneumatic Abdominal Anti-Shock Garment is a pressurized air wrapping which is used to apply pressure to intra-abdominal space to stabilize hemmorrage

27 yo female G2P2 with history of PUD, c-section x2, and smoking history presents to ED with sudden onset abdominal pain described as sharp and 10/10 with n/v for the past 1 day. The patient reports her entire abdomen is sore with pain worse in the RLQ. She is sexually active with a new partner. She reports vague history of attending outdoor picnic and eating room temperature potato salad yesterday, she also reports the pain was worse in the middle of her abdomen and the most intense pain is now over the RLQ. Vitals are wnl as is cbc and cmp. The patient has further imaging studies pending and you are called by the ED to evaluate the patient.
What should be included on the DDxA)AppendicitisB)Food poisoningC)PID D)Ectopic pregnancyE)Perforated gastric ulcer
Follow up question: what else would you like to order?

Answer: all of the above and more
As stated previously the ddx for acute abdominal pain is very broad an this patient has several things in her history which cloud the picture
Appendicitis: the history of sudden onset with pain over umbilicus then moving to the RLQ is suspicious however in females of reproductive age ectopic pregnancy should always be considered. Also remember even in early appendicitis cbc can be normal
PID: new sexual partner increases risk of this
Food poisoning: while this should be lower on the list the hx of recent picnic and exposed food should be kept in mind
Gastric ulcer: patient has history of PUD in the past, no mention of what treatment she received therefore it is conceivable she could have another

Other things to consider ordering:
1)Pregnancy test2)Ultrasound of abdomen such as fast scan3)Ua to look for uti4)Perform pelvic exam with culture5)Blood cultures or urine cultures6)Egd (history of PUD)7)Fobt8)Stool studies

Questions?

Sources
UptodateAAFP notebookHarrisons textbook of medicineCecils textbook of medicineNIH archives