choosing wisely task force hypoglycemia safety initiative (hsi) october 2014 susan kirsh, md, mph...
TRANSCRIPT
Choosing Wisely Task ForceHypoglycemia Safety Initiative (HSI)
October 2014Susan Kirsh, MD, MPHMark McConnell, MDStorm Morgan, RN, MSN, MBA
October 2012
Bernie Good, MDDonna Leslie, PharmDChartered May, 2014
Under auspices of Dr Leonard Pogach (Specialty Care) and Dr. Gordon Schectman (Primary Care
VETERANS HEALTH ADMINISTRATION 2
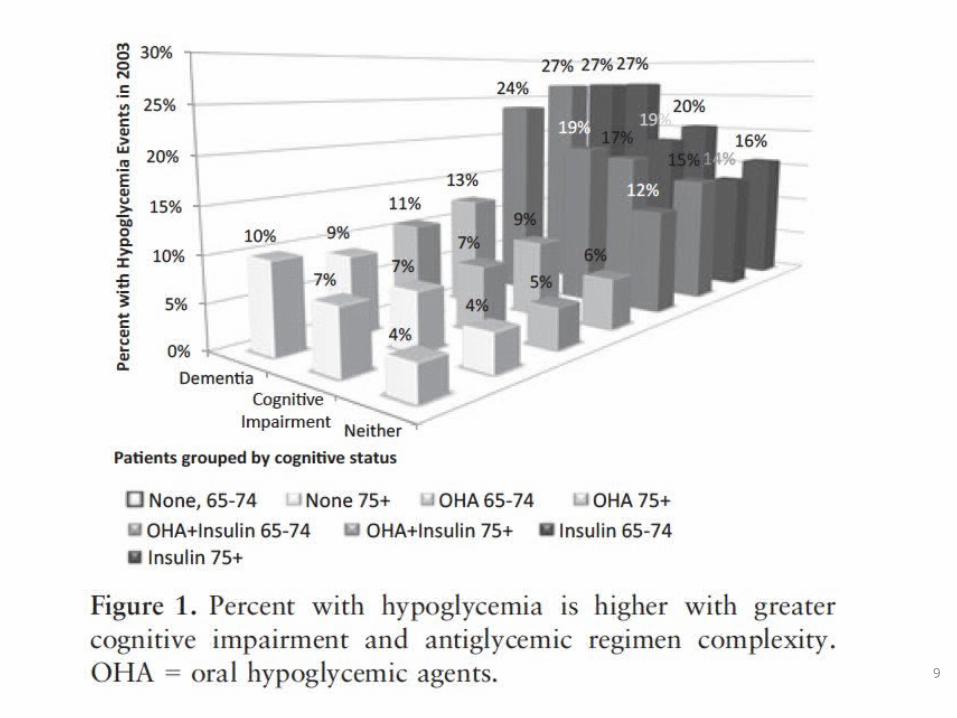
Recommendation: “There is no evidence that using medications to achieve tight glycemic control in older adults (65 and older) with type 2 diabetes is beneficial.”
VETERANS HEALTH ADMINISTRATION
DIVIDER PAGE
“Changing long-held beliefs is never easy, even when the need for change is based on strong evidence. Change is
especially difficult when prior beliefs are firmly embedded in culture, accepted as dogma, and codified in books,
articles, guidelines, public service announcements, and performance measures.”
Hayward and KrumholzCirc Cardiovasc Qual Outcomes, 2012;5:2-5
VETERANS HEALTH ADMINISTRATION 4
Choosing Wisely:VA Hypoglycemia Safety Initiative (HSI)
Ultimate Goal:To foster shared decision making between clinicians and Veterans that is informed by
the best available evidence and reduce unnecessary care.
VETERANS HEALTH ADMINISTRATION 5
Objectives
• Describe the HSI: – VA voluntary effort to identify and reduce
hypoglycemia• Describe the tools available for use• Invite any site or VISN to join!
VETERANS HEALTH ADMINISTRATION 6
Background
• Approximately 25.8 million Americans have diabetes — 8.3 percent of the U.S. population
• Total health care and related costs for the treatment of diabetes run about $174 billion annually
• Complications are costly and decrease quality of life• Treatment largely focuses on lowering A1c• QUESTION: Should we individualize A1c goals in order to
reduce hypoglycemia in those at risk?
http://ndep.nih.gov – Diabetes Snapshot
VETERANS HEALTH ADMINISTRATION 7
Background
• Reducing Hypoglycemia is part of the National Action Plan developed by multiple Federal Agencies
• Sulfonylureas and insulin are 2 of the top 4 medications associated with ER visits or hospitalizations
• In one VISN, 4400 of 54,000 (8%) patients with DM comprise a high risk cohort for serious hypoglycemia ─ (VISN Data Warehouse)
• Nationally there are 4600 patients at VERY high risk of hypoglycemia: Age, A1c, on Cholinesterase Inhibitor ─ (PBM Data)
Budnitz DS, et al. NEJM 2011
VETERANS HEALTH ADMINISTRATION 8
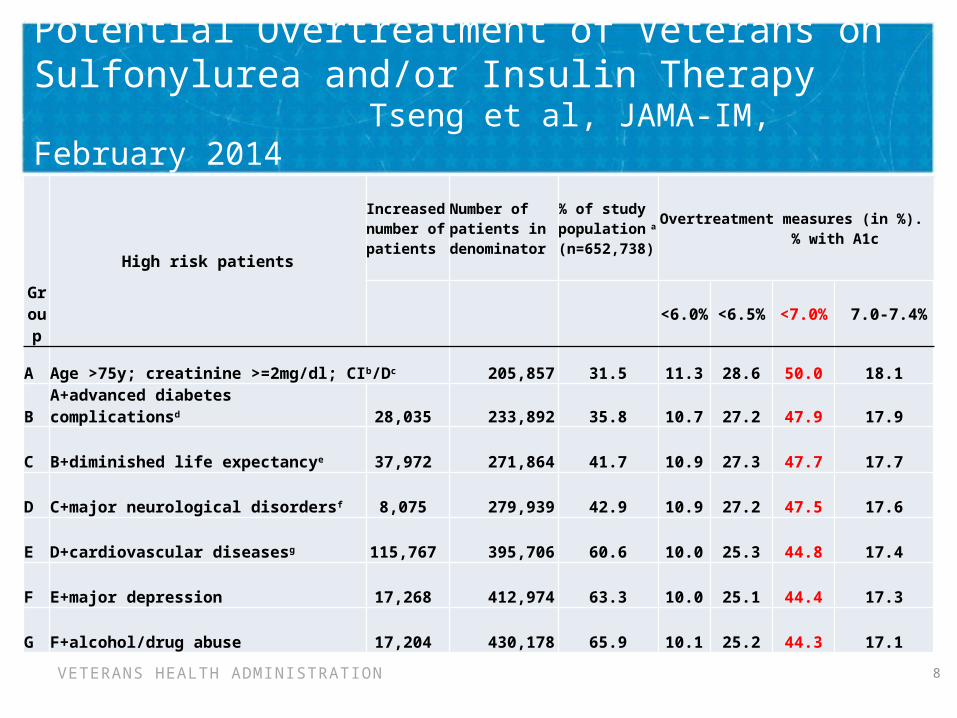
Potential Overtreatment of Veterans on Sulfonylurea and/or Insulin Therapy
Tseng et al, JAMA-IM, February 2014
Group
High risk patients
Increased number of patients
Number of patients in denominator
% of study population a (n=652,738)
Overtreatment measures (in %). % with A1c
<6.0% <6.5% <7.0% 7.0-7.4%
A Age >75y; creatinine >=2mg/dl; CIb/Dc 205,857 31.5 11.3 28.6 50.0 18.1
B A+advanced diabetes complicationsd 28,035 233,892 35.8 10.7 27.2 47.9 17.9
C B+diminished life expectancye 37,972 271,864 41.7 10.9 27.3 47.7 17.7
D C+major neurological disordersf 8,075 279,939 42.9 10.9 27.2 47.5 17.6
E D+cardiovascular diseasesg 115,767 395,706 60.6 10.0 25.3 44.8 17.4
F E+major depression 17,268 412,974 63.3 10.0 25.1 44.4 17.3
G F+alcohol/drug abuse 17,204 430,178 65.9 10.1 25.2 44.3 17.1
9
VETERANS HEALTH ADMINISTRATION 10
Federal Alignment
• September 29th: The Federal Diabetes Mellitus Interagency Coordinating Committee (DMICC) has a one day meeting at NIH to present the HHS National Action Plan for Hypoglycemic Safety and elicit Federal Collaboration
• October 30th: Health and Human Services (Office of the Assistant Secretary) sponsoring a conference for representatives from about 100 Federal Agencies and Private Sector Organizations to kick off a National Action Plan to decrease adverse drug events (opioids, anticoagulation, hypoglycemia)
VETERANS HEALTH ADMINISTRATION 11
How do WE help lower the risk?
1) Be able to identify what causes hypoglycemia2) Be aware of the symptoms3) Be able to counsel on management (15-15 rule)4) Act!– Be sure we have the right goal– Identify and intervene for patients at risk
5) Recognize that WE created the risk6) Each PACT Teamlet the key!7) Outreach to Veterans and Families
http://diabetes.niddk.nih.gov
VETERANS HEALTH ADMINISTRATION 12
Individual goal setting is needed to find an appropriate, safe, A1c goal
• We need an appropriate A1c goal• VA/DoD Diabetes Guideline 2010– Individualized A1C goals based on patient preferences,
complications, and co-morbidities– Based on best available evidence– Avoids “one size fits all” approach
• PACT: emphasis on shared decision making
VETERANS HEALTH ADMINISTRATION 13
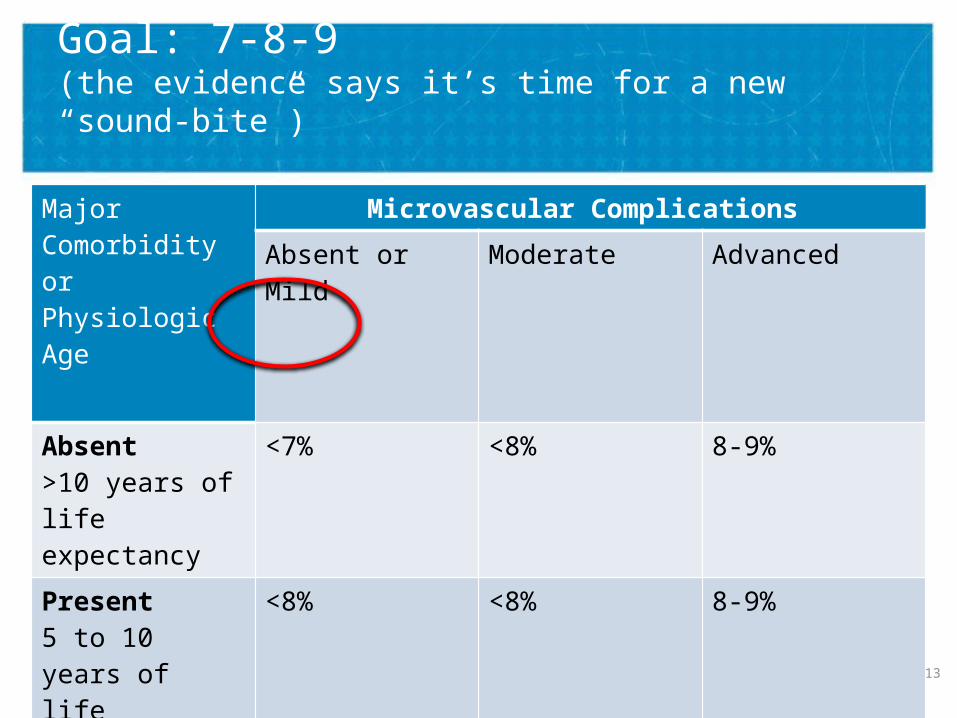
Goal: 7-8-9(the evidence says it’s time for a new “sound-bite”)
Major Comorbidity or Physiologic Age
Microvascular Complications
Absent or Mild Moderate Advanced
Absent >10 years of life expectancy
<7% <8% 8-9%
Present 5 to 10 years of life expectancy
<8% <8% 8-9%
Marked <5 years of life expectancy
8-9% 8-9% 8-9%
VETERANS HEALTH ADMINISTRATION 14
The “7-8-9” Approach
Using VA/DoD Diabetes Guidelines “The target range for glycemic control should be
individualized, based on the provider’s appraisal of the risk-benefit ratio and discussion of the target
with the individual patient. “
(Preventing A1c Craziness or Laziness)
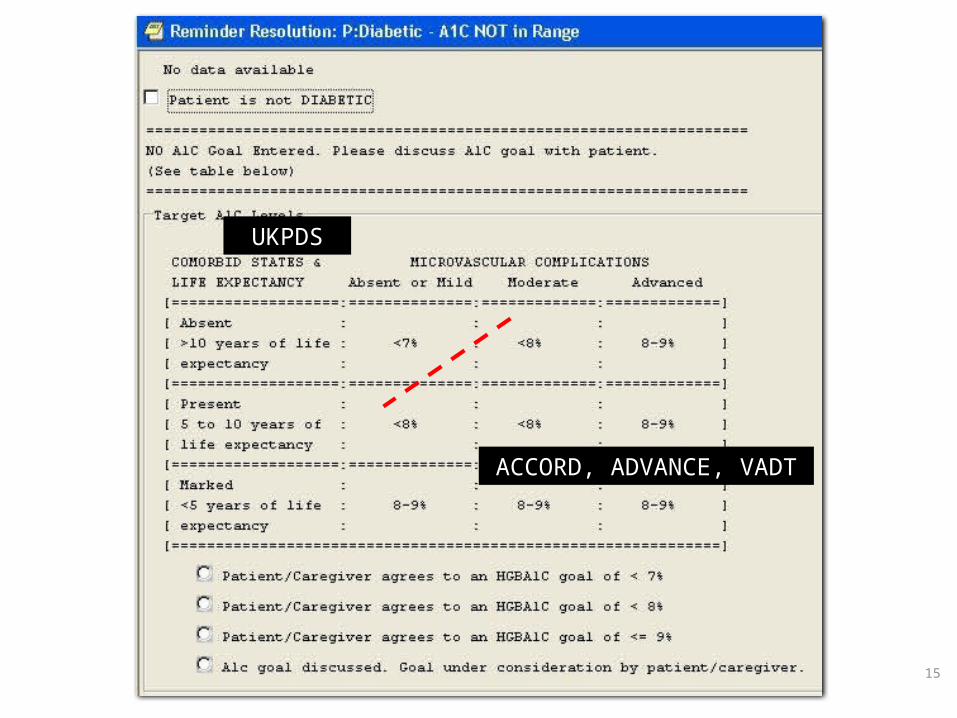
15
UKPDS
ACCORD, ADVANCE, VADT
VETERANS HEALTH ADMINISTRATION 16
Inappropriate Targets - Consequences
• Hassle (“the four P’s”)– Patients– Providers– Pharmacy– Phones
• TIME• Distraction (opportunity costs)• And...hypoglycemia...
VETERANS HEALTH ADMINISTRATION 17
HSI – VISN 12 attempt to reduce risk
• Utilize VISN Data Warehouse (VDW)• Generate lists for each PC Team– A1c < 7 and on Insulin or Sulfonylurea who:
• Are age 75 or greater• OR cognitive impairment regardless of age• OR renal impairment (creatinine >2.0)
• Use CPRS shared template to gather data• Approach:
1. Proactive: call patients2. Clinical reminder for face-to-face visits
• Easily Measured! (by uniform health factors)
VETERANS HEALTH ADMINISTRATION 18
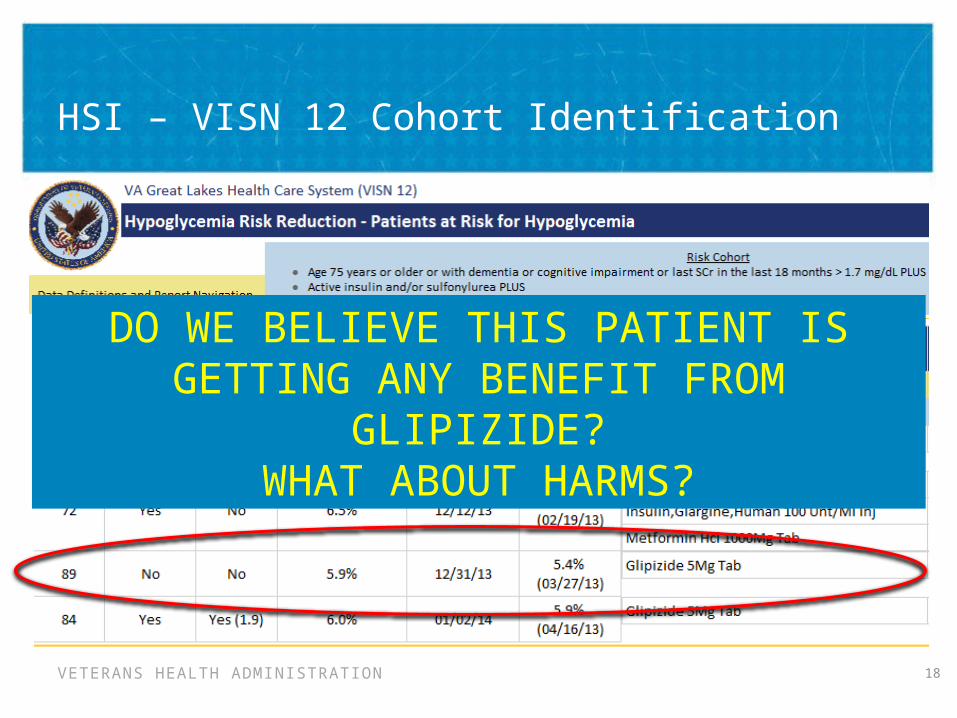
HSI – VISN 12 Cohort Identification
DO WE BELIEVE THIS PATIENT IS GETTING ANY BENEFIT FROM GLIPIZIDE?
WHAT ABOUT HARMS?
VETERANS HEALTH ADMINISTRATION 19
Patient Case #1
• 70 year old male with CKD (SCr 3.7)• Seen for routine care, at which time PCP noted his
Clinical Reminder saying he was due for hypoglycemia screening.
• Taking NPH 10 units daily• A1c 6.1%• Denies hypoglycemia• PCP stopped insulin – A1c remains well below goal at 6.4% (8-9 per CPG)
VETERANS HEALTH ADMINISTRATION 20
Patient Case #2
• 81 year old frail man and his wife• On insulin NPH/REG 70/30 35 units twice daily and 2
units of Aspart with each meal• A1c = 6.7• Hypoglycemic episodes about twice/week• PCP stopped Aspart & reduced 70/30 insulin to 30 units
in AM/20 units in PM– 3 months later: A1c = 8.4– “He feels SO much better”
VETERANS HEALTH ADMINISTRATION 21
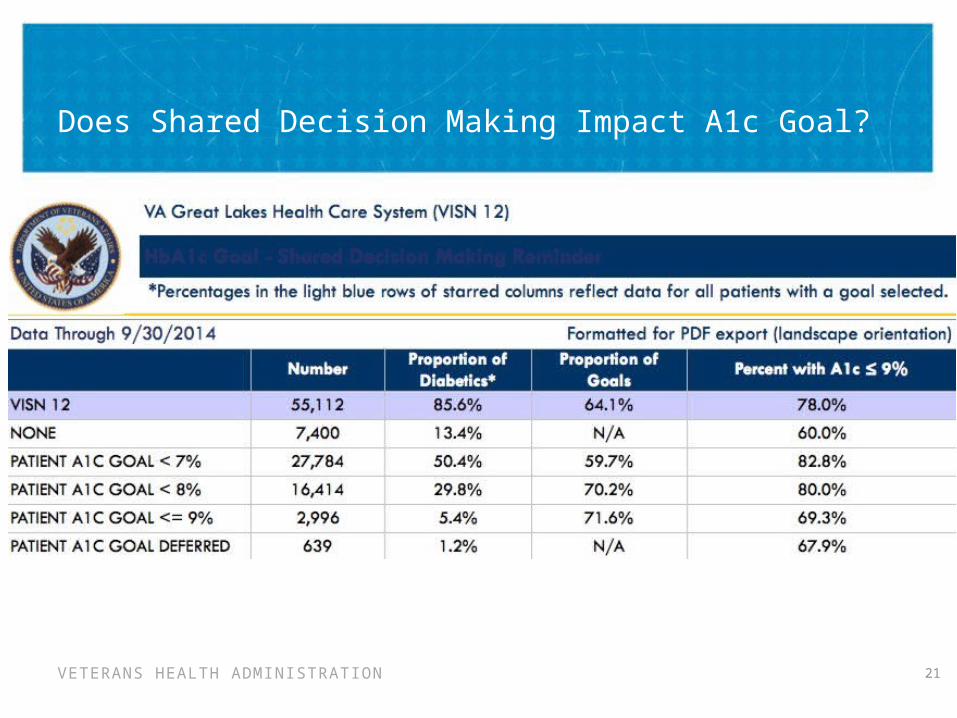
Does Shared Decision Making Impact A1c Goal?
VETERANS HEALTH ADMINISTRATION 22
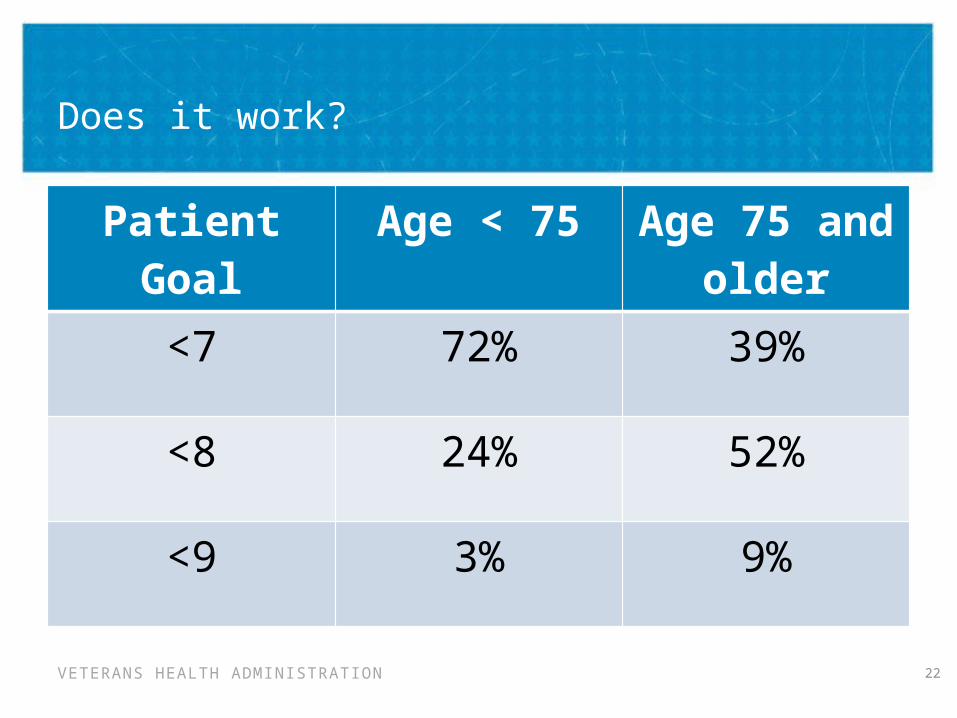
Does it work?
Patient Goal Age < 75 Age 75 and older
<7 72% 39%
<8 24% 52%
<9 3% 9%
VETERANS HEALTH ADMINISTRATION 23
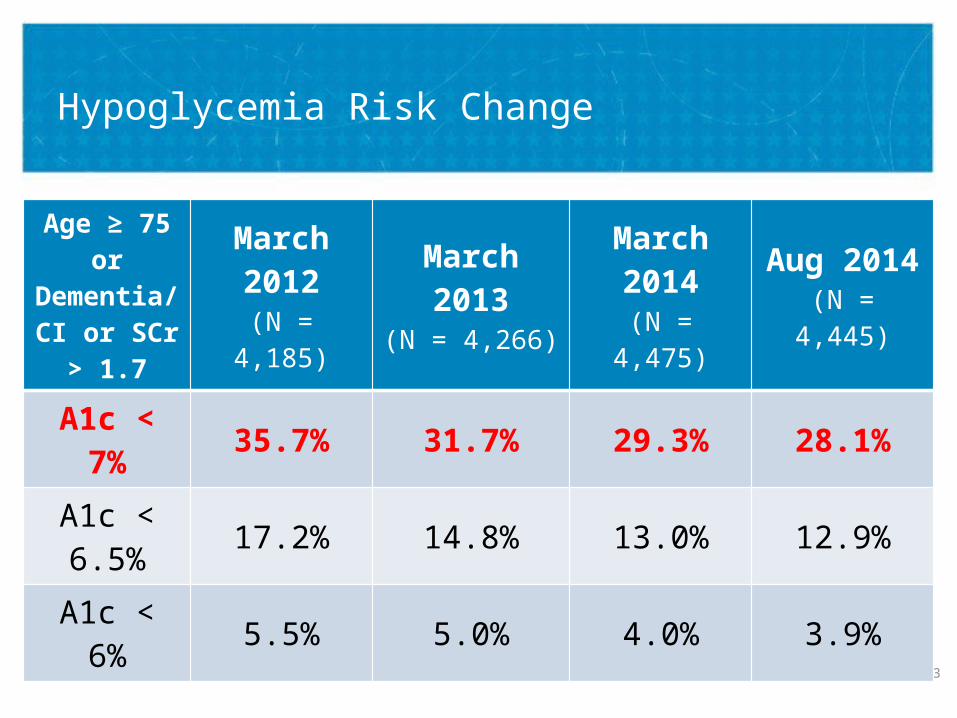
Hypoglycemia Risk Change
Age ≥ 75 or Dementia/CI or SCr > 1.7
March 2012(N = 4,185)
March 2013(N = 4,266)
March 2014(N = 4,475)
Aug 2014(N = 4,445)
A1c < 7% 35.7% 31.7% 29.3% 28.1%
A1c < 6.5% 17.2% 14.8% 13.0% 12.9%
A1c < 6% 5.5% 5.0% 4.0% 3.9%
VETERANS HEALTH ADMINISTRATION 24
Choosing Wisely: VA HSI
• National voluntary opportunity, similar to VISN 12• Lists– High risk: A1c < 7 and on Insulin or Sulfonylurea• Are age 75 or greater• OR renal impairment (creatinine >2.0)
– Ultra high risk: A1c <7 and on Insulin or Sulfonylurea who are on Cholinesterase Inhibitor
• Any VISN/site interested in participating can receive
VETERANS HEALTH ADMINISTRATION 25
Choosing Wisely: VA HSI Toolkit
• QSV Tool kit (coming soon)– Lists of patients at high risk– How to Implement• Who is involved?• How to discuss with patients
– Clinician facing education– Patient facing education
VETERANS HEALTH ADMINISTRATION 26
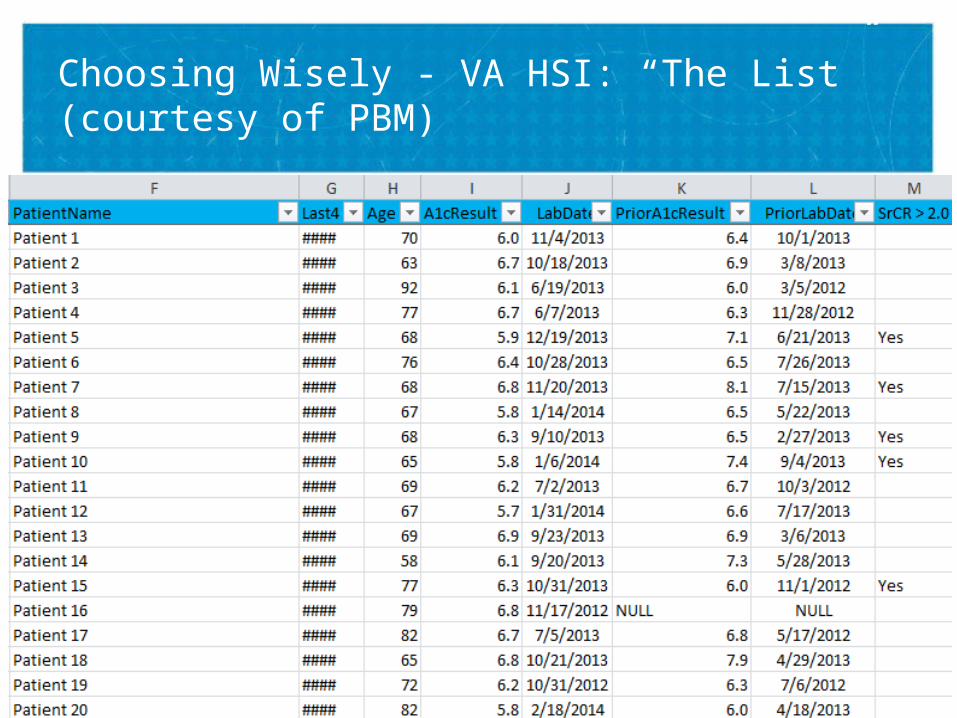
Choosing Wisely - VA HSI: “The List” (courtesy of PBM)
VETERANS HEALTH ADMINISTRATION 27
Choosing Wisely: VA HSI: Implementation
• Pro-active assessment of these patients using “non face-to-face” care (telephone encounters)
• The addition of a coversheet Clinical Reminder prompts face-to-face evaluation when these patients have a clinic visit.
• Teams are encouraged to review their lists of patients and decide on a strategy for contacting them: – Providers, Nurses (RN), Diabetes Educators (CDE), and
Clinical Pharmacy Specialists (CPS)
VETERANS HEALTH ADMINISTRATION 28
Choosing Wisely: VA HSI: Teamlet Implementation
• The Team decides who will contact patients:– If a Provider or CPS with Scope of Practice: the entire
process can be completed in one encounter– If an RN or CDE: a “huddle” will be needed after
evaluation to determine action• Patient contact can be made using a phone encounter
– Consider a standardized template– Using health factors in a standard ‘reminder dialog’ CPRS
template would allow for data collection if desired
VETERANS HEALTH ADMINISTRATION 29
Summary
• Hypoglycemia is a severe and significant risk• Everyone in VA can help by being aware of
causes/symptoms/management of hypoglycemia• We can easily identify a high-risk cohort• We have the ability to proactively reach out to these
patients and potentially lower their risk
VETERANS HEALTH ADMINISTRATION 30
What Can YOU do?
• Encourage your leaders/site to join the effort!–Remember, it’s voluntary: NOT a “Directive”–So, Veterans NEED you to volunteer!
• Sign up for the “HSI Listserv”–We will regularly update everyone on this email group about activities related to HSI
• Contact us if you want lists of your patients sent to you for action